 Seyed Hamid Borsi1Gholamreza Goudarzi2,3Gholamreza Sarizadeh3Maryam Dastoorpoor2,4
Seyed Hamid Borsi1Gholamreza Goudarzi2,3Gholamreza Sarizadeh3Maryam Dastoorpoor2,4 Sahar Geravandi5Habib Allah Shahriyari4Zahra Akhlagh Mohammadi6
Sahar Geravandi5Habib Allah Shahriyari4Zahra Akhlagh Mohammadi6 Mohammad Javad Mohammadi2,3*
Mohammad Javad Mohammadi2,3*- 1Department of Internal Medicine, Air Pollution and Respiratory Diseases Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 2Air Pollution and Respiratory Diseases Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 3Department of Environmental Health Engineering and Environmental Technologies Research Center (ETRC), Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 4Department of Biostatistics and Epidemiology, School of Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 5School of Public Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
- 6Department of Environmental Health Engineering, School of Public Health, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
The presence of criteria air pollutants (CAP) in the ambient air of a populated inhalation region is one of the main serious public health concerns. The present study evaluated the number of cardiovascular mortalities (CM), hospital admissions with cardiovascular disease (HACD), and hospital admissions for respiratory disease (HARD) due to CAP exposure between 2010 and 2014. The study used the Air Q model and descriptive analysis to investigate the health endpoint attributed to the ground level of ozone (O3), nitrogen dioxide (NO2), sulfide dioxide (SO2), and particle matter (PM10). Baseline incidence (BI) and relative risk (RR) are the most important factors in the evaluation of health outcomes from exposure to CAP in the ambient air of a populated area according to EPA and the World Health Organization (WHO) guidelines. Our study showed that annual cases of cardiovascular mortality during the period 2010–2014 relating to particle mater were 478, 506, 469, 427, and 371; ozone was 19, 24, 43, 56, and 49; nitrogen dioxide was 18, 20, 23, 27, and 21; and sulfide dioxide was 26, 31, 37, 43 and 11, in the years 2010 to 2014, respectively. These results indicate that the number of hospital admissions for respiratory disease attributed to PM were 2054, 2277, 2675, 2042, and 1895; O3 was 27, 35, 58, 73, and 63; NO2 was 23, 24, 15, 25, and 18; and SO2 was 23, 24, 25, 30, and 20, in the years from 2010 to 2014, respectively. The results also showed that the number of hospital admissions for cardiovascular disease related to particle mater was 560, 586, 529, 503, and 472; ozone was 22, 32, 38, 55, and 51; nitrogen dioxide was 19, 18, 13, 21, and 14; and sulfide dioxide was 12, 14, 16, 22, and 9, in the same period, respectively. Observations showed that most of the pollution was from outdoor air and in the human respiratory tract. Increased levels of sulfide dioxide, particle matter, nitrogen dioxide, and ozone can cause additional morbidity and mortality for exposed populations. According to the results, it is possible to help increase the level of public health. The use of these findings could also be of great help to health professionals and facilitators at regional and national levels.
Highlights
- Ahvaz city is one of the most polluted cities in the Middle East and the world.
- PM10, NO2, SO2 and O3 significantly increased cardiovascular hospital admissions among human.
- Data shown here may motivate further studies would allow assessing the development in health status more precisely.
- Air pollution has had hazardous cardiovascular effects in Ahvaz city.
Introduction
In recent years, the production and emission of air pollutants due to severe climate change, the uncontrolled increase of urbanization, increasing consumerism, high waste production, reducing rainfall, increasing desertification, as a result of the occurrence of dust phenomenon, the conversion of forest areas into agricultural fields, increasing pollution from industry and increasing emissions from transportation have been among the most serious problems. These factors cause heavy damage to human societies by increasing the number of hospitalizations and the cost of treatment, increasing the number of deaths, and intensification of economic and social damage caused by closures due to air pollution events (1, 2). The most important influencing factors are the type, size, and concentration of inhaled pollutants (3). Man-made pollutants are emitted from fixed sources (such as power plants, petrochemicals, chemical plants) and mobile sources (including transportation, cars, aircraft, trains, and growth of people) that increase the risk of disease in humans (4–6).
Respiratory diseases, pulmonary diseases, cardiovascular diseases, and deaths due to the high concentration of air pollutants and deeper penetration into the respiratory system are the main complications for human health (7, 8). In both developed and developing countries in recent decades, air pollution (ground level of ozone, nitrogen dioxide, sulfide dioxide, and particle matter) has become one of the most important factors that cause many health effects such as asthma, bronchitis, respiratory and cardiovascular disease, and different cancers (stomach, blood, liver, lung, kidney, brain) and death (7). Based on a report by the World Health Organization (WHO) and another health organization, ~6.4 million people have Disability-Adjusted Life Year (DALY) and 7 million people have died due to exposure to pollutants in indoor and outdoor air (9–11). The main factors that determine the severity of health consequences depend on the concentration of pollutants in ambient air and the duration of exposure to polluted air (12, 13). The most important way air pollutants enter the body are through the respiratory system, digestion, swallowing, skin, nasal mucosa, and eyes, which cause various diseases including cataracts, skin diseases (itching, redness, and dry skin), cardiovascular disease, the upper and lower respiratory system, gastrointestinal diseases, various cancers (stomach, intestines, brain, lungs, ovaries, and prostate), infertility and unwanted abortion, especially in groups sensitive to air pollution (children, the elderly, heart and respiratory patients) and eventually death (4, 14–16).
The concentration and number of pollutants are influenced by several parameters such as aerosol composition, aerosol charge, particle dryness, division power, wind velocity, and sampling volume (17). Exposure to air pollutants during exercise has more negative effects on lung health due to higher exposure to pollutants. Decreasing the use of fossil fuels, modifying the industrial production process, improving the fuel quality of conveyors and increasing public transportation can be effective in diminishing the detrimental effects on the economy and health because of breathing in air pollutants. If the methods are followed properly and seriously, it is possible to prevent the inhalation of polluted air, which can cause a lot of destructive and irreparable damage to the environment, animals, and humans (18). Extreme exercise increases the number of breaths per minute. In many cases, athletes breathe through the mouth instead of the nose when exercising, meaning that many air pollutants such as bioaerosols can easily penetrate the lungs (19).
The main risks that threaten the environment, animal, and human health include rapid population growth, wastewater, climate change, dust storms, and the development of industries such as petroleum, gas, oil, and steel in regions of Iran (20). This study aimed to investigate the consequences of exposure to ozone, nitrogen dioxide, particle matter, and sulfide dioxide and evaluate cardiovascular mortality, hospital admission respiratory disease, and hospital admission cardiovascular disease in Ahvaz megacity from 2010 to 2014.
Materials and Methods
Study Design
This is a cross-sectional study undertaken in Ahvaz megacity. In this study, the number of deaths (per 100,000 population) includes all-cause mortality cardiovascular in people, HACD in residents of Ahvaz, and HARD in adults attributable to exposure to PM10, O3, NO2, and SO2 in Ahvaz will be assessed over the period (2010–2014). Table 1 shows the number of populations at risk for health effect assessment of CAP.

Table 1. Criteria air pollutants concentrations (μg/m3) and Health effects assessment of CAP on Ahvaz megacity inhabitants, 2010-2014.
Ahvaz with an area of 185 km2 at the center of Khuzestan province, located in the southwest of Iran and to the north of the Persian Gulf, located at 31° 19′ 13″ N, 48° 40′ 9″ E. Ahvaz is one of the largest cities in Iran (26). The population of Ahvaz is 1,300,000. The climate is warm most of the time, with warm summers and long and moderate winters, and temperatures reaching as high as 50°C. The land area is 140 km2 (27). PM10, O3, NO2, and SO2 data from the Department of Environment and Meteorological Organization were collected from the Deputy of Health (Ahvaz city). Based on these criteria, four monitoring stations were selected. The geographical location of the area under study (Ahvaz city) is shown in Figure 1.

Figure 1. Located of sampling stations in Ahvaz megacity.
Air Q Software
Quantification of PM10, O3, NO2, and SO2 pollutants for health impact assessment (HIA) was performed by employing Air Q modeling software.
Air Q software consists of two models of quantification and life tables. These life tables and health effects were used in this study. Population contact data including demographics, health outcomes, and air quality data were fed into the software. The relative risk (RR) in formula 1 was used to calculate the Attributable proportion (AP) value (4, 27–29).
In which AP is equal to the proportion of the population exposed to the pollutant over a specified period of time (attributed ratio), RR (c) is the relative risk of health effects on the target population in the contact group c and P (c) equals the population ratio of the exposure group c.
The number of cases per 100,000 population at risk (BE) can be calculated by Formula 2.
B represents the number of health outcomes per 100,000 populations at risk. Due to the inaccessibility of hospital data, baseline incidence (BI) values were used from other studies (28, 30, 31). AP can calculate through the following formula (32):
The total number of cases attributable (NE) was calculated using Formula 4 to evaluate the health effects on the number of at-risk populations (N) (shown in Table 1).
Data Collection
The present study is an epidemiological study that correlated the concentration of PM10, O3, NO2, and SO2 to the number of CM, HARD, and HACD during the period 2010-2014. The hourly concentrations of CAP were obtained from the Department of Environment (DOE) Ahvaz.
Classification of health endpoint in this study is based on the International Classification of Diseases (ICD-10) indication for total mortality (TM- J95.150), hospital admission respiratory disease (HARD- J44.8), hospital admission cardiovascular disease (HACD- I51.6), and cardiovascular mortality (CM- I25.8) (33–35). The health effect in this study was investigated with used baseline incidence, relative risk, and proportion attributed to CAP by the Air-Q model.
Results
Investigation of cardiovascular mortality, hospital admission cardiovascular disease, hospital admission respiratory disease and the relationship between criteria air pollutants and needs to gather information exposed population and concentration of O3, PM10, SO2, and NO2.
Table 1 shows the number of health endpoints related to the criteria air pollutant concentrations on Ahvaz citizens during 2010-2014. It shows that the trend of yearly concentration of particle matter was decreased and related to ozone and that nitrogen dioxide and sulfide dioxide increased during 2010-2014.
As shown in Table 1, the level of sulfide dioxide, nitrogen dioxide, and ozone in 2013 was at a maximum. In this study central relative risk according to sulfide dioxide, particle matter, nitrogen dioxide, and ozone were used to calculate the number of cases (Table 1).
Based on the result, the annual level of CAP during the same period were SO2: 78.92, 91.07, 92.75, 112.3, and 88.57 μg/m3; NO2: 28.7, 31, 37, 41, and 34 μg/m3; PM10: 281.98, 288.38, 278.12, 242.29, and 205.52 μg/m3; O3: 66.52, 72.67, 102.27, 223, and 187 μg/m3, respectively.
Finding showed that, the number of CM attributed to particle mater were (478, 506, 469, 427, and 371); ozone (19, 24, 43, 56, and 49); nitrogen dioxide (18, 20, 23, 27, and 21); and sulfide dioxide (26, 31, 37, 43, and 11), in 2010 until 2014, respectively (Table 1). The number of HARD attributed to PM were (2,054, 2,277, 2,675, 2,042, and 1,895); O3 (27, 35, 58, 73, and 63); NO2 (23, 24, 15, 25, and 18); and SO2 (23, 24, 25, 30, and 20), during 2010-2014, respectively (Table 1).
Table 1 shows that the number of HACD related to particle mater were (560, 586, 529, 503, and 472); ozone (22, 32, 38, 55, and 51); nitrogen dioxide (19, 18, 13, 21, and 14); and sulfide dioxide (12, 14, 16, 22, and 9), in 2010 until 2014, respectively.
Figure 2 presents the annual average of the criteria air pollutants in ambient air of Ahvaz City, Iran. As depicted in Figure 2, particle matter was a decreasing trend and other pollutants including ozone, sulfide dioxide and nitrogen dioxide had an increasing and then a decreasing trend.
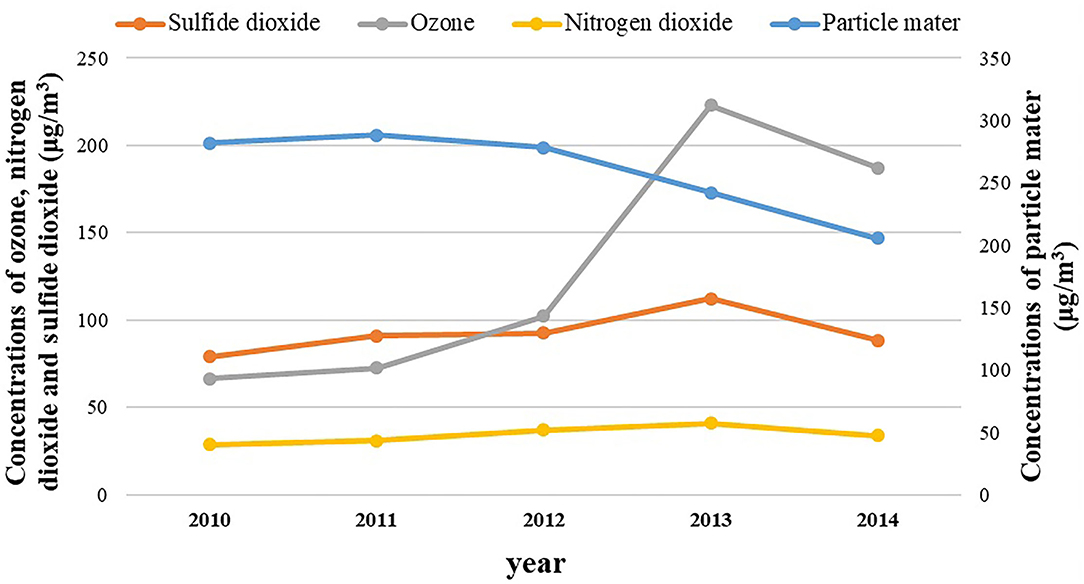
Figure 2. Annual averages of the criteria air pollutants during the study period in ambient air of Ahvaz City, Iran.
The cumulative number of cardiovascular mortality, hospital admission respiratory disease, hospital admission cardiovascular disease related to criteria air pollutants during 2010 to 2014 is illustrated in Figure 3. Figure 3 shows that the number of health endpoints of exposure to criteria air pollutants were characterized by a sinusoidal process (first increasing and then decreasing).
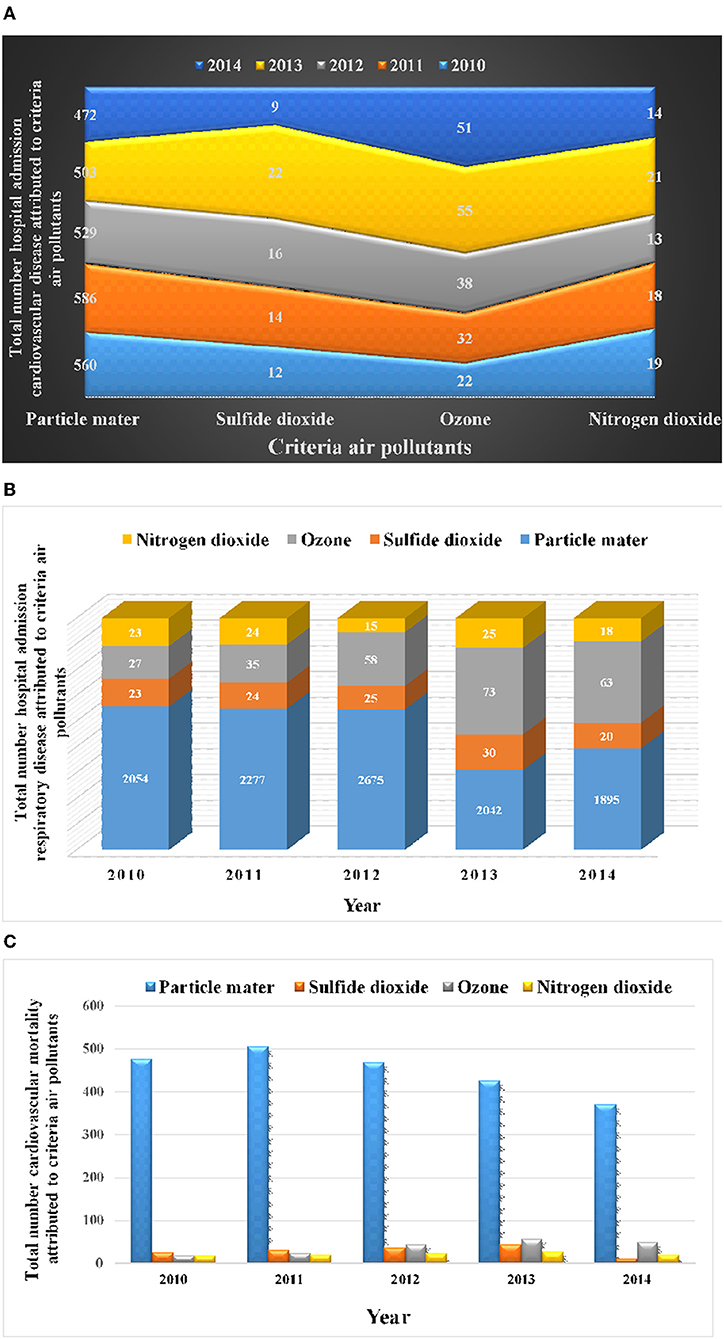
Figure 3. Cumulative number of cardiovascular mortality, hospital admission respiratory disease, hospital admission cardiovascular disease related to criteria air pollutants. (A) Number of hospital admission cardiovascular disease. (B) Number of hospital admission respiratory disease. (C) Number of cardiovascular mortality.
Discussion
Recently the disadvantages of ozone, nitrogen dioxide, particle matter, and sulfide dioxide on physical and mental health have attracted the attention of many researchers. According to the result of this study most cases of CM, HACD and HARD were related to O3, PM10, SO2, and NO2 during the year 2013. The results also showed that the highest calculated number of cases health endpoint regarding PM10 was from 2010 to 2011.
Based on these findings, the annual level of average ozone, nitrogen dioxide, particle mater and sulfide dioxide concentrations during the same period were 66.52, 72.67, 102.27, 223, and 187 μg/m3; 28.7, 31, 37, 41, and 34 μg/m3; 281.98, 288.38, 278.12, 242.29, and 205.52 μg/m3; 78.92, 91.07, 92.75, 112.3, and 88.57 μg/m3, respectively.
These results indicated that the number of CM attributed to particle mater were (478, 506, 469, 427, and 371); ozone (19, 24, 43, 56, and 49); nitrogen dioxide (18, 20, 23, 27 and 21); and sulfide dioxide (26, 31, 37, 43, and 11), in the years 2010 to 2014, respectively. The number of HACD related to particle mater were (560, 586, 529, 503, and 472); ozone (22, 32, 38, 55, and 51); nitrogen dioxide (19, 18, 13, 21, and 14); and sulfide dioxide (12, 14, 16, 22, and 9), in 2010 until 2014, respectively. The number of HARD attributed to PM were (2054, 2277, 2675, 2042, and 1895); O3 (27, 35, 58, 73 and 63); NO2 (23, 24, 15, 25, and 18); and SO2 (23, 24, 25, 30, and 20), during 2010-2014, respectively.
Table 1 shows the trends of level nitrogen dioxide, sulfide dioxide, ozone, and particle matter and the health endpoint of exposure to criteria air pollutants in ambient air of on a populated in Ahvaz city, Iran.
Also, the result specified that the mean concentration of air pollutants was higher than WHO guidelines standard. As can be seen in Figure 2, cases of cardiovascular mortality, hospital admission respiratory disease, and hospital admission cardiovascular disease related to PM10, SO2, NO2, and O3 in the period of the study had an increasing and then a decreasing trend.
Yao et al. (36) undertook a China evaluation of health burden related to exposure to air pollutants. They reported that exposure to air pollutants cause cardiovascular and respiratory disease in 7.8 million people (36). They reported that the premature mortality, contributions of PM2.5, PM10, NO2, SO2, O3, and CO were11.1, 5.2, 28.9, 9.6, 23.0, and 22.2%, respectively (36).
In 2013, Jeong undertook a study of Suwon, Korea, which examined the health effects of air pollution on people. The study observed that the annual PM10 average was equal to 52 μg/m3. The results of the study suggest that the summer season with a concentration of 2,563 μg/m3 was the highest amount of PM10 μg/m3 (37).
In Egypt Shakour et al. reported that for every 10 μg/m3 in PM10 concentration, there would be a 4.1% increase in hospital admission cardiovascular disease (HARD) (38), which is lower compared to other studies. A 2013 study by Habeebullah et al. (39) in Makkah, Saudi Arabia found that the annual average and maximum PM10 were 195.5 and 782.1 μg/m3, which were lower than the levels of PM10 in our study. Particle concentrations in the present study also had the highest concentrations in summer, which is the main reason this increase could be due to the occurrence of dust storms in the Middle East areas because of wind speed and higher temperature.
DeFlorio-Barker et al. (40) estimated the air pollution levels and population influence interaction of exposure to air pollution. They showed that exercise intensifies the ill effects of air pollution for those with chronic conditions (40).
Kumarathasan et al. (41) in the vicinity of a steel mill assessment of healthy humans between cardiovascular and inflammatory mechanisms and exposure to air pollution in healthy humans. The results showed that the mean CO, SO2 and ultrafine particle (UFP) levels on the day of biological sampling were higher at the Bayview site compared to the College site (41). They reported that the steel mill site can influence inflammatory and vascular mechanisms (41).
In studies performed by Yarahmadi et al. (42) in Tehran on mortality related to exposure to fine particles, the results showed that mortality was related to a corresponding reduction in PM concentrations. The annual mean cases of chronic obstructive pulmonary disease and lung cancer deaths related to exposure to PM2.5 were 158 and 142, respectively (42).
The results of this study showed that the level of pollutants in Ahvaz was a great deal higher compared to standards outlined in heavy industries such as oil, gas, petrochemical, and steel. The reasons for this might include dust storms, a decrease in rainfall, and an increase in drought.
Biggeri et al. (43) studied the relationship between the health effects attributed to long-term exposure to sulfur dioxide and health endpoint on citizens in Italy. This study reported a significant relationship between health effects and SO2 (43). The result of this study showed that an increase of 10 μg/m3 in sulfur dioxide was associated with an increase of 2.4% in hospital admissions (43).
High emissions of high sulfur from heavy industries could be related to the high percentage of hospital admissions for respiratory and cardiovascular disease in Ahvaz.
Bell et al. (44) in the U.S undertook similar work, in 2004, they studied the relationship between health effects and ground-level ozone. Results showed that a high level of ground-level ozone increased the risk of daily deaths, hospital admissions, and respiratory and cardiovascular diseases (10-ppb increase in the concentration of ground-level ozone was attributed to a 0.52% increase in daily deaths) (44). The most important reasons that can be mentioned for the difference between the results of this study and other studies is the existence of climatic characteristics, geography and meteorological changes in the city of Ahvaz.
Samoli et al. (45) conducted a study in 30 European cities, outlining that there was a relation between NO2 levels and cardiovascular and respiratory mortality. According to their results, a significant association was found between cardiovascular and respiratory mortality and the level of nitrogen dioxide (45). They indicate that cities with a larger proportion of elderly persons in the population were observed to have a higher number of respiratory mortality (45).
In 2016, Dijkema et al. (46) studied the relation between cardiopulmonary hospital admissions and variation in concentrations of nitrogen dioxide. They found that there is a higher risk of cardiopulmonary hospital admissions in areas with a higher concentration of nitrogen dioxide (46). Findings showed that positive associations were found between the levels of nitrogen dioxide and hospital admission rates for asthma, chronic obstructive pulmonary disease (COPD), all cardiovascular causes, ischemic heart disease, and for the second to fourth quartile relative to the first quartile of exposure were 1.87 (1.46–2.40), 2.34 (1.83–3.01), and 2.81 (2.16–3.65) for asthma; 1.44 (1.19–1.74), 1.50 (1.24–1.82), and 1.60 (1.31–1.96) for COPD) (46).
The city of Ahvaz has also been significantly affected by rapid population growth, heavy industry, lack of proper transportation, and dust storms. Since air is the main factor in the life of humans, breathing large amounts of pollutants can pose health risks to the people in the region. Activities related to the development of oil and gas fields and petrochemical and steel project industries and pipelines have increased the concentration of other pollutants. Therefore, continuous monitoring of the air pollutant content in indoor and outdoor air quality is a priority. The trend of yearly concentration of air pollutants was decreasing and showed that the action taken to reduce the emission of these contaminants through corrective actions such as improving the quality of fuel in vehicles, increasing the planting of trees, improving the quality of services provided in the public transport sector, reducing the production and emission by industries are effective.
Limitations and Strengths
The main limitations of this study were a lack of epidemiological studies and calculations of relative risk (RR) and baseline incidence (BI) attributed to cardiovascular mortality, hospital admission respiratory and cardiovascular disease in humans due to criteria air pollutants in the study area. To solve this problem, it is necessary to conduct cohort studies for several years to calculate RR and BI. In recent years, a study of the Hoveyzeh cohort has started in the southwest of Iran. It is hoped that in a few years, important indicators such as baseline incidence and relative risk in this region will be calculated and this problem will be solved in future studies.
The most important strengths of the study were the investigation of the health endpoint of exposure to criteria air pollutants in ambient air for this area (Ahvaz City, Iran). Estimating the risks of air pollutants on human health can play an important role in raising public awareness. They can also help health policymakers by providing a practical guide for policy. In future studies, examination of time series analysis will be done with the help of statistics experts.
Conclusion
We evaluated the consequences of exposure to particle matter (PM10), ground level of ozone (O3), sulfide dioxide (SO2), and nitrogen dioxide (NO2) in the ambient air of a populated area in Ahvaz City, Iran. Considering that Ahvaz is one of the largest cities in Iran and the region from the aspect of urbanization, industry, and population, these findings could be useful for decision-makers in other parts of the country and the world, especially in the Middle East. According to the findings, there is a significant relationship between cardiovascular mortality (CM), hospital admissions cardiovascular disease (HACD), hospital admission respiratory disease (HARD), and increased exposure to air pollutants.
The results of this study showed that the concentration of PM10, O3, SO2, and NO2 was higher than the WHO guideline value. The main agents of cases health effects of exposure to PM10 were because of the high level of this pollutant. Paying attention to decreasing emissions and levels of particle matter, the ground level of ozone, sulfide dioxide, and nitrogen dioxide for the reduction of cases of CM, HACD, and HARD attributed to particle matter, nitrogen dioxide, sulfide dioxide, and ozone b are important.
Observing modern urban planning patterns in urban development, developing public transportation (especially metro), increasing green space per capita by planting trees and creating parks in different areas of the city, carrying out effective activities in desertification, car replacement (worn and old), creating green belts around cities, reducing emissions due to the activities of heavy industries (oil and gas), improving production processes in important industries (steel, refineries, and cement), the establishment of monitoring and measuring stations, careful monitoring and increasing the general literacy of society are the most important control activities that will reduce the concentration of pollutants and harmful effects of inhaling these substances.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
SB, GG, GS, MD, SG, HS, ZA, and MM: study concept, design, and critical revision of the manuscript for important intellectual content. MM: drafting of the manuscript and advisor. MD, SG, HS, and ZA: performing the experiments. SB, GG, MM, GS, and MD: revised the manuscript and finalizing. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Air Pollution and Respiratory Diseases Research Center of Ahvaz Jundishapur University of Medical Sciences (APRD-9906). The authors are grateful to the Department of Environment of Ahvaz city for providing data as well as the Air Pollution and Respiratory Diseases Research Center of Ahvaz Jundishapur University of Medical Sciences (with code IR.AJUMS.REC.1399.444) for providing the necessary facilities to perform this research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Goudarzi G, Alavi N, Geravandi S, Idani E, Behrooz HRA, Babaei AA, et al. Health risk assessment on human exposed to heavy metals in the ambient air PM 10 in Ahvaz, southwest Iran. Int J Biometeorol. (2018) 62:1075–83. doi: 10.1007/s00484-018-1510-x
2. Morovati P, Valipour A, Geravandi S, Karimyan A, Behrooz HRA, Mohammadi MJ. Association of air quality index related to criteria air pollutants in Abadan, Iran. Fresenius Environmental Bulletin. (2018) 27:4023–8. Available online at: http://eprints.asaums.ac.ir/id/eprint/57
3. Momtazan M, Geravandi S, Rastegarimehr B, Valipour A, Ranjbarzadeh A, Yari AR, et al. An investigation of particulate matter and relevant cardiovascular risks in abadan and khorramshahr in 2014–2016. Toxin Rev. (2018) 1–8. doi: 10.1080/15569543.2018.1463266
4. Dobaradaran S, Geravandi S, Goudarzi G, Idani E, Salmanzadeh S, Soltani F, et al. Determination of cardiovascular and respiratory diseases caused by PM10 Exposure in Bushehr, 2013. J Mazandaran Univ Med Sci. (2016) 26:42–52. Available online at: http://jmums.mazums.ac.ir/article-1-8154-en.html
5. Geravandi S, Sicard P, Khaniabadi YO, De Marco A, Ghomeishi A, Goudarzi G, et al. A comparative study of hospital admissions for respiratory diseases during normal and dusty days in Iran. Environ Sci Pollut Res. (2017) 24:18152–9. doi: 10.1007/s11356-017-9270-4
6. Hashemzadeh B, Idani E, Goudarzi G, Ankali KA, Sakhvidi MJZ, Babaei AA, et al. Effects of PM 2.5 and NO 2 on the 8-isoprostane and lung function indices of FVC and FEV 1 in students of Ahvaz city, Iran. Saudi J Biol Sci. (2019) 26:473–80. doi: 10.1016/j.sjbs.2016.11.008
7. Mirhoseini SH, Nikaeen M, Hatamzadeh M, Hassanzadeh A. Assessment of bioaerosol concentration in the indoor environments. Health Syst Res. (2014) 10:376–85.
8. Massoudinejad MR, Ghajari A, Hezarkhani N, Aliyari A. Survey of fungi bioaerosols in icu ward of taleghani hospital in tehran by petri-dish trapping technique and bioaerosol sampler in 2013. Safety Promot Inj Prev. (2015) 3:147–54. doi: 10.22037/meipm.v3i3.8800
9. Hay S, GRF Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. (2017) 390:1345–422. doi: 10.1016/S0140-6736(17)32366-8
10. Prüss-Üstün A, Wolf J, Corvalán C, Bos R, Neira M. Preventing Disease Through Healthy Environments: A Global Assessment of the Burden of Disease From Environmental Risks: World Health Organization (2016).
11. Neira M. The 2014 WHO conference on health and climate. SciELO Public Health. (2014) 546. doi: 10.2471/BLT.14.143891
12. Dehghanzadeh R, Ansarian K, Aslani H. Concentrations of carbon monoxide in indoor and outdoor air of residential buildings. J Health. (2013) 3:29–40. Available online at: http://healthjournal.arums.ac.ir/article-1-55-en.html
13. Bhatia L. Impact of bioaerosols on indoor air quality-a growing concern. Adv Biores. (2011) 2:120–3.
14. Kim K-H, Kabir E, Kabir S. A review on the human health impact of airborne particulate matter. Environ Int. (2015) 74:136–43. doi: 10.1016/j.envint.2014.10.005
15. Taylor M, Retalis A, Flocas HA. Particulate matter estimation from photochemistry: a modelling approach using neural networks and synoptic clustering. Aerosol Air Qual Res. (2016) 16:2067–84. doi: 10.4209/aaqr.2015.07.0481
16. Lin C-C, Tsai J-H, Huang K-L, Yeh CK-J, Chen H-L, Chen S-J, et al. Characteristics of respirable particulate metals emitted by a beehive firework display in yanshuei area of southern Taiwan. Aerosol Air Qual Res. (2016) 16:2227–36. doi: 10.4209/aaqr.2016.08.0346
17. Dehdashti A, Sahranavard N, Rostami R, Barkhordari A, Banayi Z. Survey of bioaerosols type and concentration in the ambient air of hospitals in Damghan, Iran. Occup Med Quart J. (2013) 4:41–51.
18. Carlisle A, Sharp N. Exercise and outdoor ambient air pollution. Br J Sport Med. (2001) 35:214–22. doi: 10.1136/bjsm.35.4.214
19. Kargarfard M, Rouzbahani R, Rezanejad S, Poursafa P. The effect of air pollution on cardio respiratory perfor-mance of active individuals. Arya Atheroscler. (2009) 5:71–7. Available online at: https://arya.mui.ac.ir/article_10038.html
20. Hassani GBA, Takdastan A, Shirmardi M, Yousefian F, Mohammadi MJ. Occurrence and fate of 17β-estradiol in water resources and wastewater in Ahvaz, Iran. Glob NEST J. (2016) 18:855–66. doi: 10.30955/gnj.002053
21. Tahery N, Geravandi S, Goudarzi G, Shahriyari HA, Jalali S, Mohammadi MJ. Estimation of PM 10 pollutant and its effect on total mortality (TM), hospitalizations due to cardiovascular diseases (HACD), and respiratory disease (HARD) outcome. Environ Sci Pollut Res Int. (2021) 28:22123–30. doi: 10.1007/s11356-020-12052-9
22. Khaefi M, Geravandi S, Hassani G, Yari AR, Soltani F, Dobaradaran S, et al. Association of particulate matter impact on prevalence of chronic obstructive pulmonary disease in Ahvaz, southwest Iran during 2009–2013. Aerosol Air Qual Res. (2017) 17:230–7. doi: 10.4209/aaqr.2015.11.0628
23. Goudarzi G, Geravandi S, Foruozandeh H, Babaei AA, Alavi N, Niri MV, et al. Cardiovascular and respiratory mortality attributed to ground-level ozone in Ahvaz, Iran. Environ Monit Assess. (2015) 187:487. doi: 10.1007/s10661-015-4674-4
24. Khaefi M, Goudarzi G, Yari AR, Geravandi S, Dobaradaran S, Idani E, et al. An association between ambient pollutants and hospital admitted respiratory cases in Ahvaz, Iran. Fresenius Environ Bull. (2016) 25:3955–61.
25. Goudarzi G, Geravandi S, Idani E, Hosseini SA, Baneshi MM, Yari AR, et al. An evaluation of hospital admission respiratory disease attributed to sulfur dioxide ambient concentration in Ahvaz from 2011 through 2013. Environ Sci Pollut Res Int. (2016) 23:22001–7. doi: 10.1007/s11356-016-7447-x
26. Effatpanah M, Effatpanah H, Jalali S, Parseh I, Goudarzi G, Barzegar G, et al. Hospital admission of exposure to air pollution in Ahvaz megacity during 2010–2013. Clin Epidemiol Glob Health. (2020) 8:550–6. doi: 10.1016/j.cegh.2019.12.001
27. Yari AR, Goudarzi G, Geravandi S, Dobaradaran S, Yousefi F, Idani E, et al. Study of ground-level ozone and its health risk assessment in residents in Ahvaz City, Iran during 2013. Toxin Rev. (2016) 35:201–6. doi: 10.1080/15569543.2016.1225769
28. Khaniabadi YO, Polosa R, Chuturkova RZ, Daryanoosh M, Goudarzi G, Borgini A, et al. Human health risk assessment due to ambient PM10 and SO2 by an air quality modeling technique. Process Saf Environ Protect. (2017) 111:346–54. doi: 10.1016/j.psep.2017.07.018
29. Fattore E, Paiano V, Borgini A, Tittarelli A, Bertoldi M, Crosignani P, et al. Human health risk in relation to air quality in two municipalities in an industrialized area of Northern Italy. Environ Res. (2011) 111:1321–7. doi: 10.1016/j.envres.2011.06.012
30. Faridi S, Shamsipour M, Krzyzanowski M, Künzli N, Amini H, Azimi F, et al. Long-term trends and health impact of PM2. 5 and O3 in Tehran, Iran, 2006–2015. Environ Int. (2018) 114:37-49. doi: 10.1016/j.envint.2018.02.026
31. Karimi A, Shirmardi M, Hadei M, Birgani YT, Neisi A, Takdastan A, et al. Concentrations and health effects of short-and long-term exposure to PM2. 5, NO2, and O3 in ambient air of Ahvaz city, Iran (2014–2017). Ecotoxicol Environ Saf. (2019) 180:542-8. doi: 10.1016/j.ecoenv.2019.05.026
32. Nourmoradi H, Goudarzi G, Daryanoosh SM, Omidi-Khaniabadi F, Jourvand M, Omidi-Khaniabadi Y. Health impacts of particulate matter in air by airQ model in Khorramabad city, Iran. J Bas Res Med Sci. (2015) 2:44–52. Available online at: http://jbrms.medilam.ac.ir/article-1-157-en.html
33. Treede R-D, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. (2019) 160:19–27. doi: 10.1097/j.pain.0000000000001384
34. Chung K-F, Yeung W-F, Ho FY-Y, Yung K-P, Yu Y-M, Kwok C-W. Cross-cultural and comparative epidemiology of insomnia: the Diagnostic and statistical manual (DSM), International classification of diseases (ICD) and International classification of sleep disorders (ICSD). Sleep Med. (2015) 16:477–82. doi: 10.1016/j.sleep.2014.10.018
35. Organization WH. ICD-10: International Statistical Classification Of Diseases And Health-Related Problems. Geneva: WHO (2010). p. 64–7.
36. Yao M, Wu G, Zhao X, Zhang J. Estimating health burden and economic loss attributable to short-term exposure to multiple air pollutants in China. Environ Res. (2020) 183:109184. doi: 10.1016/j.envres.2020.109184
37. Jeong S. The impact of air pollution on human health in suwon city. Asian J Atmos Environ. (2013) 7:227–33. doi: 10.5572/ajae.2013.7.4.227
38. Shakour A, El-Shahat M, El-Taieb N, Hassanein M, Mohamed A. Health impacts of particulate matter in greater Cairo, Egypt. J Am Sci. (2011) 7:840–8. Available online at: http://hdl.handle.net/10986/35810
39. Habeebullah T. Health impacts of PM10 using AirQ2.2.3 model in Makkah. J Basic Appl Sci. (2013) 9:259–68. doi: 10.6000/1927-5129.2013.09.34
40. DeFlorio-Barker S, Lobdelle DT, Stone SL, Boehmer T, Rappazzo KM. Acute effects of short-term exposure to air pollution while being physically active, the potential for modification: a review of the literature. Prev Med. (2020) 106195. doi: 10.1016/j.ypmed.2020.106195
41. Kumarathasan P, Vincent R, Blais E, Bielecki A, Guénette J, Filiatreault A, et al. Cardiovascular and inflammatory mechanisms in healthy humans exposed to air pollution in the vicinity of a steel mill. Part Fibre Toxicol. (2018) 15:1–17. doi: 10.1186/s12989-018-0270-4
42. Yarahmadi M, Hadei M, Nazari SSH, Conti GO, Alipour MR, Ferrante M, et al. Mortality assessment attributed to long-term exposure to fine particles in ambient air of the megacity of Tehran, Iran. Environ Sci Pollut Res. (2018) 25:14254–62. doi: 10.1007/s11356-018-1680-4
43. Biggeri A, Bellini P, Terracini B, Italian MG. [Meta-analysis of the Italian studies on short-term effects of air pollution]. Epidemiol Prev. (2001) 25:1–71.
44. Bell ML, McDermott A, Zeger SL, Samet JM, Dominici F. Ozone and short-term mortality in 95 US urban communities, 1987-2000. JAMA. (2004) 292:2372–8. doi: 10.1001/jama.292.19.2372
45. Samoli E, Aga E, Touloumi G, Nisiotis K, Forsberg B, Lefranc A, et al. Short-term effects of nitrogen dioxide on mortality: an analysis within the APHEA project. Eur Resp J. (2006) 27:1129–38. doi: 10.1183/09031936.06.00143905
Keywords: air pollutants, health endpoint, cardiovascular mortality, respiratory disease, cardiovascular disease, Iran
Citation: Borsi SH, Goudarzi G, Sarizadeh G, Dastoorpoor M, Geravandi S, Shahriyari HA, Akhlagh Mohammadi Z and Mohammadi MJ (2022) Health Endpoint of Exposure to Criteria Air Pollutants in Ambient Air of on a Populated in Ahvaz City, Iran. Front. Public Health 10:869656. doi: 10.3389/fpubh.2022.869656
Received: 04 February 2022; Accepted: 21 February 2022;
Published: 29 March 2022.
Edited by:
Luigi Angelo Vaira, Azienda Ospedaliero Universitaria Sassari, ItalyReviewed by:
Mostafa Hadei, Tehran University of Medical Sciences, IranMarija Jevtic, University of Novi Sad, Serbia
Copyright © 2022 Borsi, Goudarzi, Sarizadeh, Dastoorpoor, Geravandi, Shahriyari, Akhlagh Mohammadi and Mohammadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Javad Mohammadi, amF2YWQuc2FtMjAwQGdtYWlsLmNvbQ==; bW9oYW1hZGkubUBhanVtcy5hYy5pcg==