 Felipe Teixeira Lopes1Renata Santos de Sousa1Jayanne L. Carvalho Gomes1
Felipe Teixeira Lopes1Renata Santos de Sousa1Jayanne L. Carvalho Gomes1 Mariana Cayres Vallinoto1Aline Cecy Rocha de Lima1
Mariana Cayres Vallinoto1Aline Cecy Rocha de Lima1 Sandra Souza Lima1Felipe Bonfim Freitas2
Sandra Souza Lima1Felipe Bonfim Freitas2 Rosimar N. Martins Feitosa1
Rosimar N. Martins Feitosa1 Andrea Nazaré M. Rangel da Silva1
Andrea Nazaré M. Rangel da Silva1 Luiz Fernando A. Machado1Cintia Y. P. Aben-Athar1Eduardo Leitão Maia da Silva1
Luiz Fernando A. Machado1Cintia Y. P. Aben-Athar1Eduardo Leitão Maia da Silva1 Izaura M. V. Cayres Vallinoto1
Izaura M. V. Cayres Vallinoto1 Antonio Carlos R. Vallinoto1*
Antonio Carlos R. Vallinoto1*- 1Laboratory of Virology, Institute of Biological Sciences, Federal University of Pará, Belém, Brazil
- 2Virology Section, Evandro Chagas Institute, Ananindeua, Brazil
Introduction: To identify the prevalence of infection in the urban area of the capital city of Belém, Brazil, the Laboratory of Virology of the Federal University of Pará implemented, as a public service, serological screening for human T-lymphotropic viruses 1 and 2 (HTLV-1/2) infection and, if necessary, counseling service and referral to specialized medical care. The project is funded by the National Council of Science and Technology, the Ministry of Health of Brazil and the Pan American Health Organization.
Methods: From January 2020 to June 2021, 1,572 individuals of both sexes were approached to answer a questionnaire and were tested using an enzyme immunoassay (Murex HTLV-I+II, DiaSorin, Dartford, UK). Seropositive samples were confirmed as HTLV-1 and HTLV-2 infection by line immunoassay (INNO-LIA® HTLV I/II Score, Fujirebio, Japan) and/or by real-time polymerase chain reaction. G and Fisher's exact tests were applied to identify the association between epidemiological characteristics and HTLV-1/2 infection.
Results: Of the 1,572 screened individuals, 63.74% were females between the ages of 30 and 59 years (49.04%). Infection was confirmed in six individuals (0.38%), among whom three (0.19%) were infected with HTLV-1 and three with HTLV-2 (0.19%). Blood transfusion before 1993 was the main risk factor associated with the route of exposure to the virus (p = 0.0442). The infected individuals were referred to a counseling session with a nursing professional, and two patients who manifested signs and symptoms suggestive of myelopathy associated with HTLV were referred to a neurologist.
Conclusion: The implementation of the screening service revealed the occurrence of moderate endemicity of HTLV-1/2 in Belém, reinforcing the importance of continuing the service as a means of establishing an early diagnosis and providing counseling as a measure to prevent and control viral transmission in the general population.
Introduction
Human T-lymphotropic viruses 1 and 2 (HTLV-1 and HTLV-2) belong to the family Retroviridae, subfamily Orthoretrovirinae, and genus Deltaretrovirus (1), and both were isolated in the early 1980s (2, 3). HTLV-1/2 is characterized by the ability to cause a persistent and silent infection, and its forms of transmission are contact with contaminated organic fluids through sexual intercourse, syringe and needle sharing and breastfeeding (4, 5).
Although most individuals infected with the virus show no symptoms, HTLV-1 is associated with serious diseases, such as HTLV-1-associated myelopathy (HAM) and adult T-cell leukemia/lymphoma (ATL), pathologies that may occur in ~2–3% of people living with HTLV (PLHTLV) (2, 6, 7). HTLV-1 is also associated with other diseases, such as uveitis, infectious dermatitis, bronchitis, bronchiectasis, arthropathies, myositis, urinary dysfunction, and strongyloidiasis (8–10). For HTLV-2, there are reports that correlate it to cases of neurological disorders similar to HAM; however, there are no precise indications of the clinical manifestations of these disorders (11, 12).
The diagnosis of infection is initially performed using an enzyme-linked immunosorbent assay (ELISA) as a screening method for the detection of anti-HTLV-1/2 antibodies. Positive cases are referred for infection confirmation by Western blot, INNO-LIA and/or conventional (PCR) or real-time (qPCR) polymerase chain reaction assays (13). The first two tests are used for the detection of specific antibodies to different virus proteins, and PCR is used for the detection of proviral DNA, to differentiate between viral types and subtypes, and to quantify the proviral load (13–15).
Globally, it is estimated that 5 to 10 million individuals are infected with HTLV, with the distribution varying based on ethnic group, behavioral risk factors for infection and geographic location; southwestern Japan, sub-Saharan Africa and South America have the highest endemicity of the virus (16). In Brazil, there are an estimated 2.5 million PLHTLV (17), and Brazil is considered the country with the highest absolute number of HTLV-1/2 seropositive individuals in the world (18). The infection is endemic, being heterogeneously distributed among the different Brazilian regions and states, with Bahia, Maranhão and Pará recording the highest prevalence rates in Brazil (6, 17, 18).
Previous studies conducted in the state of Pará have reported high prevalence rates of HTLV infection in specific groups, such as blood donors (18, 19), pregnant women (20), indigenous populations (21), the Quilombola people (22) and people living with human immunodeficiency virus (PLHIV) (23). The prevalence of the virus in the metropolitan region of Belém, the most population-dense area in the state of Pará, is still unknown because of a lack of the early diagnosis of infection and diseases associated with HTLV (24), reinforcing the fact that the epidemiology of this viral agent should be better described for the capital of Pará.
It is of paramount importance the counseling of asymptomatic HTLV-1-infected subjects, to perform a clinical follow-up of the individual aiming to detect early the symptoms of diseases associated with the virus. Additionally, the lack of public policies for the active identification of cases of infection and subsequent counseling and screening for intrafamilial transmission results in a loss of productivity for those affected and their families. In addition, the absence of policies for preventing new infections and for providing adequate care for those living with HTLV-1 contributes to the increase in socioeconomic disparity between and within countries (25). Given this, the Laboratory of Virology of the Institute of Biological Sciences of Federal University of Pará (Universidade Federal do Pará—UFPA), with support from the Brazilian National Council for Scientific and Technological Development (CNPq, acronym in Portuguese) and the Pan American Health Organization (PAHO), implemented a public HTLV-1/2 serological screening and confirmation service for the general population of the city of Belém (metropolis of the Brazilian Amazon) and, if necessary, provided counseling and follow-up by a nurse and a referral for care by various health professionals (nurse, occupational therapist and doctor). In the present study, we aimed to describe the main results after the first year of service implementation.
Methods
Study Design
In the period from January 2020 to June 2021, the Laboratory of Virology of the Federal University of Pará began the HTLV-1/2 serological screening project in the city of Belém, the capital of the state of Pará, and tested a total of 1,572 individuals of both sexes who were categorized into the following age groups: children (7 to 11 years); adolescents (12 to 17 years); adults (18 to 59 years); and elderly individuals (>60 years).
The individuals were approached through an active search via the promotion of social actions in health, carried out primarily in community and religious centers in different neighborhoods in the capital. A portion of the sample consisted of people who voluntarily sought the Laboratory of Virology of UFPA, seeking a diagnosis for an infection, after extensive posts and dissemination on social networks and in a newspaper (printed and online) with high circulation in the state.
The participants were given basic information about HTLV and educated on the importance of diagnosing the infection and implementing prevention methods. All participants answered an epidemiological survey, after which peripheral venous blood was collected into 4-mL EDTA tubes. Subsequently, the samples were centrifuged to separate the plasma and cells (erythrocytes and leukocytes) and stored at −20°C until serological and molecular tests were performed at the UFPA Laboratory of Virology. The participants were informed that if they presented reactive or indeterminate results, blood would be collected again to confirm the infection and that if infection was confirmed, they would be referred to counseling and follow-up with a nurse. Individuals who manifested clinical signs suggestive of diseases associated with HTLV were referred to specialized medical care.
Serological Screening
Plasma detection of total anti-HTLV-1/2 antibodies was performed using an ELISA (Murex HTLV-I+II, DiaSorin, Dartford, UK) following the manufacturer's protocol. Samples with reactive or indeterminate results (cut-off = 0.284) were subjected to confirmatory tests (INNO-LIA and/or qPCR).
Line Immunoassay
LIA was used as a supplementary confirmation method for HTLV infection and used to differentiate viral types. An INNO-LIA® HTLV I/II Score kit (Fujirebio, Japan) was used to detect anti-HTLV-1 and/or HTLV-2 antibodies following the manufacturer's protocol.
DNA Extraction
For the analysis of HTLV proviral DNA, DNA was extracted from 200 μL of cell mass (leukocytes) with a QiaAmp DNA mini kit (Qiagen, Germany) following the manufacturer's protocol.
Real-Time PCR
Samples with positive ELISA results that were subsequently confirmed by INNO-LIA were subjected to qPCR using the TaqMan system (Applied Biosystems, Foster City, CA) on the Applied Biosystems StepOne Plus Real Time PCR platform. The human albumin gene was used as an endogenous reaction control, and the viral gene regions pol (186 bp) of HTLV-1 and tax (75 bp) of HTLV-2 were used as viral confirmation and molecular differentiation targets (26). Each reaction contained 12.5 μL of TaqMan Universal PCR Master Mix (2X) (Applied Biosystems, Foster City, USA), 6.0 μL of ultrapure water, 0.5 μL of each primer, 0.5 μL of each probe and 5.0 μL of DNA, resulting in a total volume of 25 μL. The following temperature cycles were used: 95 °C for 10 mins, followed by 45 cycles of 95 °C for 15 secs and 60°C for 1 min for primer and probe binding.
The following primers were used in the reactions: 5′-CCCTACAATCCAACCAGCTCAG-3′ (HTLV-1F), 5′-GTGGTGAAGCTGCCATCGGGTTTT-3′ (HTLV-1R), 5′-CGATTGTGTACAGGCCGATTG-3′ (HTLV-2F), 5′-CAGGAGGGCATGTCGATGTAG-3′ (HTLV-2R), 5′-GCTGTCATCTCTTGTGGGCTGT-3′ (Albumin F), and 5′-AAACTCATGGGAGCTGCTGGTT-3′ (Albumin R). The probe sequences were as follows: FAM-5′- CTTTACTGACAAACCCGACCTACCCATGGA-3′-MGB (HTLV-1), FAM-5′- TGTCCCGTCTCAGGTGGTCTATGTTCCA-3′-MGB (HLTV-2) and FAM-5′- CCTGTCATGCCCACACAAATCTC-3′-MGB (Albumin) (26).
Statistical Analysis
The data obtained from the epidemiological survey answered by the participants was input in a database in Epi-Info 7.2. Statistical analyses were performed using BioEstat 5.3 (27) and GraphPad Prism 6.0. The studied variables were analyzed using descriptive statistics, and the estimated prevalence was analyzed by point and confidence interval (95% confidence interval [CI]) estimators. To identify the epidemiological characteristics associated with HTLV infection, the chi-square and Fisher's exact tests were applied, adopting a significance level of 95% (p < 0.05).
Ethical Aspects
This study complied with ethical precepts and was submitted to and approved by the Human Research Ethics Committee of the Health Sciences Institute of UFPA and by the National Research Ethics Committee (CAAE No. 27290619.2.0000.0018; opinion: 4.351.470), in accordance with Resolution no. 466/12 of the Ministry of Health of Brazil. Individuals over 18 years of age who agreed to participate signed an informed consent form. Children under 18 years of age signed an informed assent form, and their legal representatives signed an informed consent form, authorizing their participation in the study.
Results
Serological Screening and Infection Confirmation
Of the 1,572 individuals evaluated, 63.74% were female, with a mean age of 41 years, ranging from 30 to 59 years (49.04%). Among the other characteristics identified in the epidemiological survey, 54.03% self-reported being mixed race, 33.81% reported having a higher education, and 38.69% reported having a family income equal to or greater than five times the minimum wage, with no significant differences between infected and non-infected individuals (Table 1).
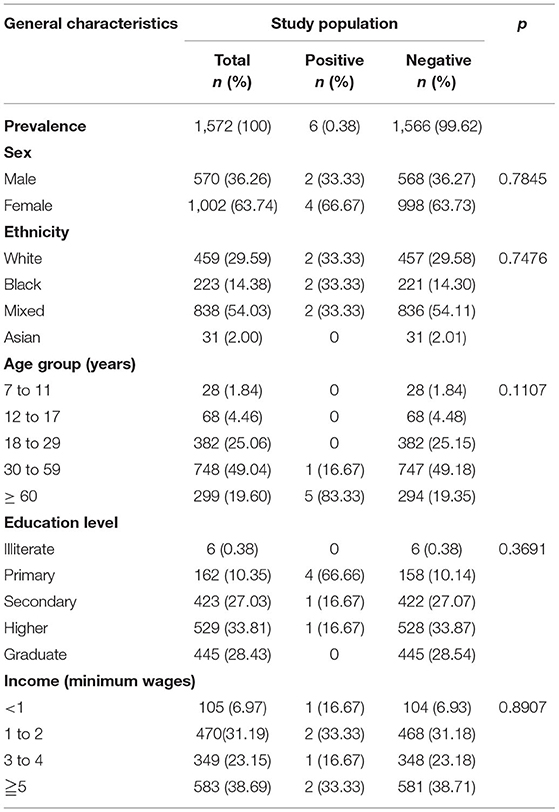
Table 1. General characteristics of the study population.
After obtaining the serology results for anti-HTLV-1/2 antibodies, six individuals were positive and were contacted by telephone to schedule an appointment for blood collection to confirm the viral infection. The new samples were subjected to the same testing sequence, and ELISA and INNO-LIA were performed again. Additionally, qPCR was performed as previously described. Infection was confirmed in six individuals (0.38%; CI: 0.07–0.69%), with 3 (0.19%) infected by HTLV-1 and 3 infected by HTLV-2 (0.19%). Among those infected, 66.7% were women aged 49 to 87 years (Table 2).

Table 2. Results of tests performed for the screening and confirmation of HTLV infection.
INNO-LIA indicated two cases of an HTLV profile without defining the viral type, and qPCR confirmed the presence of proviral DNA of HTLV-1 and HTLV-2. One HTLV-1-positive individual, as determined by INNO-LIA, did not have proviral DNA detected by qPCR (Table 2).
Clinical and Epidemiological Characteristics of Individuals Seropositive for HTLV-1/2
When evaluating the responses obtained in the epidemiological survey answered by the six HTLV carriers, blood transfusion was the main risk factor associated with the virus exposure route (p = 0.0442) (Table 3). However, when this result was stratified into “before” and “after” 1993, the year in which screening for HTLV in blood bags became mandatory in blood centers in Brazil, statistical significance was not maintained (Table 3).
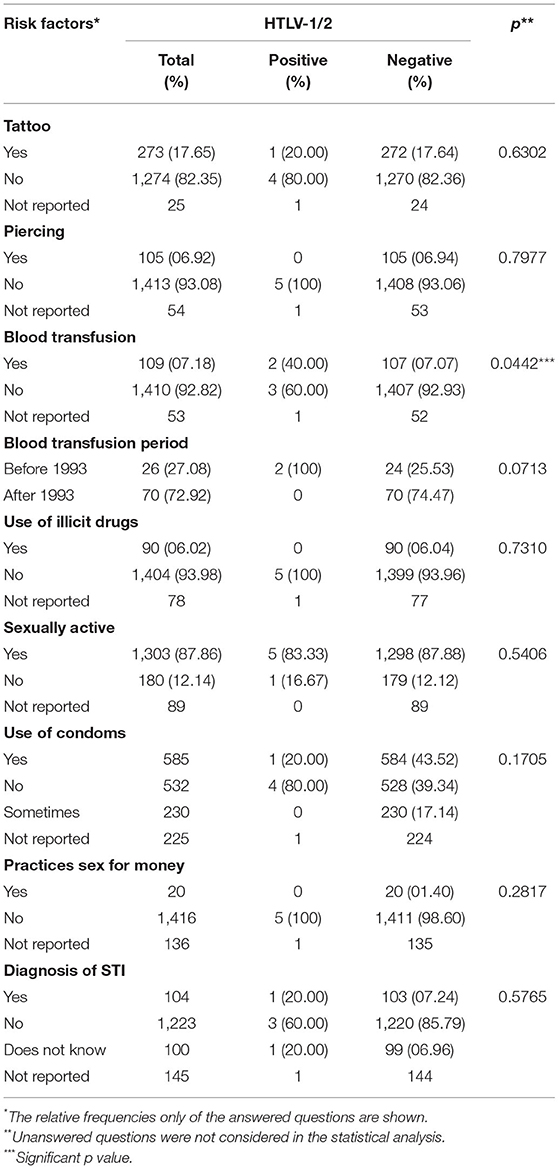
Table 3. Risk factors associated with HTLV infection.
The infected individuals received their respective laboratory diagnostic for the infection and were referred for a first counseling session with a nurse who took the medical history of the patients and talks about some virus' aspects, such as transmission modes, diseases associated, intrafamilial segregation, prevention, and treatment. The close relatives (parents, spouses and children) of the six patients were invited to undergo testing for possible intrafamilial transmission; however, to date, they have not yet responded to our first call.
Of the six individuals with confirmed cases, four were asymptomatic. Two female HTLV-2-positive individuals had clinical signs suggestive of neurological disorders and were referred for evaluations by a neurologist, as described below.
Patient #04 (HTLV-2), female, single, 49 years old, had incomplete primary education and reported in the survey that she had been pregnant three times and breastfed for more than 6 months. At the time of the interview, she reported not having an active sex life. During counseling with a nurse, she reported feeling hand tremors, urinary urgency, swelling and joint pain, with restricted movements and gait changes.
Patient #06, widower, 87 years old, was hospitalized during the study with severe pulmonary fibrosis and presented with alternating consciousness, which prevented a complete neurological evaluation. It was possible to observe only the absence of clear signs of HAM, but there was a history of urinary incontinence associated with motor deficit (leg weakness) but without signs suggestive of a pyramidal corticospinal tract injury.
Discussion
Investigations of the prevalence of HTLV-1/2 infection in the state of Pará have been conducted in specific population groups, such as blood donors, indigenous populations, the Quilombola people, PLHIV and Japanese immigrants (22, 28–30). The present study provides seroepidemiological information on the prevalence of HTLV-1 and HTLV-2 in the general population of Belém, the capital of the state of Pará.
A study by Silva et al. (24), conducted between 2014 and 2015, showed a 2% prevalence of HTLV infection (1.4% for HTLV-1 and 0.5% for HTLV-2) in a sample from the city of Belém, classifying this location as an area of moderate endemicity. The prevalence found in the present study of 0.38% was well below that described by Silva et al. (24); this difference may be due to (i) a possible reduction in prevalence over the 6 years separating the studies; (ii) the fact that Silva et al. (24) sampled adult individuals who were passing public places such as the Ver-o-Peso Complex, a location with a high circulation of people from other municipalities of the metropolitan region of Belém, which differs from the present study, which evaluated only people residing in Belém; (iii) sample size; or (iv) differences in the sensitivity of the different ELISAs used in the two studies. Currently, we are collecting seroepidemiological information from neighboring municipalities that compose the metropolitan region of Belém, for example, Ananindeua, Marituba and Benevides, with the objective of separately evaluating prevalence and thus identifying the overall occurrence of infection in the region. Our results did not differ from those observed by Maneschy et al. (31) in a study conducted between 2015 and 2019 in a blood center in the state of Pará; the results indicated an HTLV prevalence of 0.3% (1476/453,626) among blood donors, among whom most positive individuals were from the metropolitan region of Belém. In another study conducted with pregnant women, the estimated prevalence of HTLV was 0.6% (32).
During the screening and confirmation analyses, two individuals were identified by INNO-LIA with a serological profile of HTLV, and qPCR molecular analysis confirmed the presence of HTLV-1 proviral DNA in one individual and HTLV-2 proviral DNA the other. Another individual was positive for HTLV-1 based on INNO-LIA diagnostic criteria, but proviral DNA was not detected by qPCR. These serological (INNO-LIA) and molecular (qPCR) methods have been used and endorsed for the confirmatory and differential diagnosis of HTLV-1 and HTLV-2 infections (13). Differences in results between serological and molecular methods are frequent and result from differences in the sensitivity and specificity of the tests (26). Furthermore, Caterino-de-Araújo and Rodrigues Campos (33) described difficulties in the laboratory diagnosis of the infection, including the presence of incomplete HTLV viral particles (characterized by the absence of a viral gene, such as the tax gene), low quality of extracted DNA, mutations and a low proviral load, which can potentially lead to the absence of gene amplification and thus result in a false-negative diagnosis for infection. Therefore, the use of a single laboratory method to confirm and differentiate HTLV-1/2 infection is not recommended; it is necessary to adopt complementary confirmatory assays to minimize diagnostic and prevalence estimate errors.
In addition to an accurate laboratory diagnosis that allows identifying the prevalence of infection in a given geographic area, it is necessary to implement a counseling and follow-up service for PLHTLV to provide efficient clinical, laboratory and psychological monitoring. Rosadas et al. (34) emphasize the importance of including the multiprofessional screening of HTLV in the routine care provided in services for people infected with HIV and other STIs. For this reason, all individuals diagnosed in our study were referred to initial counseling with a nurse, at which time they were informed about HTLV, its modes of transmission and prevention, associated diseases and supportive therapies for infection-related symptoms. Subsequently, those individuals who, in counseling, complained of neurological changes were referred to a neurologist. Of the six individuals with confirmed cases of infection, four individuals were asymptomatic. Interestingly, the two individuals who presented complaints suggestive of neurological disorders were infected with HTLV-2. Although there is some rare evidence in the literature associating this viral type with neurological diseases similar to HAM (11, 12), the initial evaluation by the neurologist did not identify the presence of clinical changes that confirmed a diagnosis of HAM.
Conclusions
The results presented here are part of the first year of a screening, confirmation, counseling and multiprofessional follow-up service for PLHTLV offered through the Laboratory of Virology of the Federal University of Pará and implemented as part of a National Network of laboratories, funded by the Ministry of Health and PAHO. The main limitation of the study can be considered the difficulty of convincing the seropositive individual to perform a new blood collection in order to carry out the confirmatory tests. On the other hand, the main strength of the study is to contribute with the prevention and control measures for HTLV infection to reduce transmission and to identify the main risk factors associated with infection, characterizing the individuals or groups that may be more vulnerable to HTLV, and thus provide information that will support the development of public health policy strategies to combat the spread of this virus in Brazil.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of the Health Sciences Institute of the Federal University of Pará and by the National Research Ethics Committee (CAAE No. 27290619.2.0000.0018). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
AV and IC conceived and designed the study. FL, MV, AL, and FF performed the laboratory experiments. FL, RS, JC, MV, AL, RF, AR, and LM performed the fieldwork. CA-A and EM performed clinical follow-ups. FL and AV wrote the manuscript. All authors read and approved the final version of the manuscript.
Funding
This study received financial support from the National Council of Science and Technology (CNPq # 442522/2019-3 and CNPQ # 302935/2021-5) and the Ministry of Health of Brazil and the Pan American Health Organization (#SCON2021-00310).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all the volunteers for their participation in the study.
References
1. ICTV - International Committee on Taxonomy of Viruses. Taxonomy. (2019). Disponível em: https://ictvonline.org. Acesso em: 19/12/2020.
2. Poiesz BJ, Ruscetti FW, Gazdar AF, BUNN PA, Minna JD, Gallo RC. Detection and isolation of type c retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous t-cell lymphoma. Proceed Nat Acad Sci. (1980) 77:7415. doi: 10.1073/pnas.77.12.7415
3. Kalyanaraman VS, Sarngadharan MG, Robert-Guroff M, Miyoshi I, Golde D, Gallo RC. A new Subtype of Human T-Cell Leukemia Virus (HTLV-II) Associated With a T-Cell Variant of Hairy Cell Leukemia. Science. (1982) 218:571. doi: 10.1126/science.6981847
4. Hu CY, Lin MT, Yang YC, Tang JL, Tseng LH, Wang CH, et al. Familial Transmission of Human T-Lymphocyte Virus Type (HTLV-1) in Patients With Adult T-Cell Leukemia/Lymphoma or HTLV-1-Associated Myelopathy. J Formosan Med Assoc. (1998) 97:101.
5. Gotuzzo E, Arango C, De Queiroz-Campos A, Istúriz RE. Human T- Cell Lymphotropic Vírus-I in Latin America. Infect Dis Clin North Am. (2000) 14:211. doi: 10.1016/S0891-5520(05)70225-7
6. Catalan-Soares BC, Proietti FA, Carneiro-Proietti ABF. Os Vírus Linfotrópicos de Células T Humanos (HTLV) na Última Década (1990-2000): Aspectos Epidemiológicos. Revista Brasileira de Epidemiologia. (2001) 4:81. doi: 10.1590/S1415-790X2001000200003
7. Nagasaka M, Yamagishi M, Yagishita N, Araya N, Kobayashi S, Makiyama J, et al. Mortality and Risk of Progression to Adult T Cell Leukemia/Lymphoma in HTLV-1-Associated Myelopathy/Tropical Spastic Paraparesis. Proc Natl Acad Sci U S A. (2020) 117:11685–91. doi: 10.1073/pnas.1920346117
8. Romanelli LCF, Caramelli P, Carneiro Proietti ABF. O Vírus Linfotrópico de Células T Humanos Tipo 1 (HTLV1): Quando Suspeitar da Infecção? Rev Assoc Med Bras. (2010) 56:340. S0104-42302010000300021. doi: 10.1590/S0104-42302010000300021
9. Einsiedel L, Chiong F, Jersmann H, Taylor GP. Human T-Cell Leukaemia virus type 1 associated pulmonary disease: clinical and pathological features of an under-recognised complication of HTLV-1 infection. Retrovirology. (2021) 18:1. Erratum in: Retrovirology. (2021). Feb 22;18(1):5. doi: 10.1186/s12977-020-00543-z
10. Schierhout G, McGregor S, Gessain A, Einsiedel L, Martinello M, Kaldor J. Association Between HTLV-1 Infection and Adverse Health Outcomes: A Systematic Review and Meta-Analysis of Epidemiological Studies. Lancet Infect Dis. (2020) 20:133–43. doi: 10.1016/S1473-3099(19)30402-5
11. Araujo A, Hall WW. Human T-Lymphotropic Virus Type II and Neurological Disease. Ann Neurol. (2004) 56:10. doi: 10.1002/ana.20126
12. Hall WW, Ishak R, Zhu SW, Novoa P, Eiraku N, Takahashi H, et al. Human T Lymphotropic Virus Type II (HTLV-II): Epidemiology, Molecular Properties, and Clinical Features of Infection. J Acquir Immune Defic Syndr Hum Retrovirol. (1996) 13:204. doi: 10.1097/00042560-199600001-00031
13. Caterino-De-Araujo A, Barbosa-Stancioli EF, Alonso Neto JB, Aragón MG, Galvão-Castro B, Ishak R, et al. Laboratory Diagnosis of Human T-Lymphotropic Virus in Brazil: Assays, Flowcharts, Challenges, and Perspectives. Rev Soc Bras Med Trop. (2021) 54:E01752021. doi: 10.1590/0037-8682-0175-2021
14. Santos FLN, Lima FWM. Epidemiologia, Fisiopatogenia e Diagnóstico Laboratorial da Infecção Pelo HTLV-I. J Bras Patol Med Lab. (2005) 41:105. doi: 10.1590/S1676-24442005000200008
15. BRASIL. Ministério da Saúde. Relatório de Recomendação: Western Blot e PCR em Tempo Real em Pacientes com Leucemia/Linfoma de Células T Do Adulto Associado ao HTLV-1. Brasília: Secretaria de Ciência, Tecnologia e Insumos Estratégicos. (2016), p. 14.
16. Gessain A, Cassar O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front Microbiol. (2012) 3:1. doi: 10.3389/fmicb.2012.00388
17. Carneiro-Proietti ABF, Ribas JGR, Catalan-Soares BC, Martins ML, Brito-Melo GEA, Martins-Filho AO, et al. Infecção e Doença Pelos Vírus Linfotrópicos Humanos de Células T (HTLV-I/II) no Brasil. Revista da Sociedade Brasileira de Medicina Tropical. (2002) 35:499. doi: 10.1590/S0037-86822002000500013
18. Catalan-Soares BC, Carneiro-Proietti ABF, Proietti FA. Heterogeneous Geographic Distribution of Human T-Cell Lymphotropic Viruses I and II (HTLV-I/II): Serological Screening Prevalence Rates in Blood Donors From Large Urban Areas in Brazil. Cadernos de Saúde Pública. (2005) 21:926. doi: 10.1590/S0102-311X2005000300027
19. Galvão-Castro B, Loures L, Rodriques LG, Sereno A, Ferreira Júnior OC, Franco LG, et al. Distribution of Human T-Lymphotropic Virus Type I Among Blood Donors: A Nationwide Brazilian Study. Transfusion. (1997) 37:242. doi: 10.1046/j.1537-2995.1997.37297203532.x
20. Sequeira CG, Tamegão-Lopes BP, Santos EJM, Ventura AMR, Moraes-Pinto MI, Succi RCM. Descriptive Study of HTLV Infection in a Population of Pregnant Women From the State of Pará, Northern Brazil. Rev Soc Bras Med Trop. (2012) 45:453–6. doi: 10.1590/S0037-86822012005000007
21. Braço ILJ, Sá KSG, Waqasi M, Queiroz MAF, Silva ANR, Cayres- Vallinoto IMV, et al. High Prevalence of Human T-Lymphotropic Virus 2 (HTLV-2) Infection in Villages of the Xikrin Tribe (Kayapo), Brazilian Amazon Region. BMC Infect Dis. (2019) 19:1–8. doi: 10.1186/s12879-019-4041-0
22. Vallinoto ACR, Pontes GS, Muto NA, Lopes IGL, Machado LFA, Azevedo VN, et al. Identification of Human T-Cell Lymphotropic Virus Infection in a Semi-Isolated Afro-Brazilian Quilombo Located in the Marajó Island (Pará, Brazil). Memórias Do Instituto Oswaldo Cruz. (2006) 101:103. doi: 10.1590/S0074-02762006000100020
23. Vallinoto ACR, Azevedo VN, Santos DEM, Carniceiro S, Mesquita FCL, Hall WW, et al. Serological Evidence of HTLV-I and HTLV-II Coinfections in HIV-1 Positive Patients in Belém, State of Pará, Brazil. Memórias Do Instituto Oswaldo Cruz. (1998) 93:407. doi: 10.1590/S0074-02761998000300026
24. Silva IC, Pinheiro BT, Nobre AFS, Coelho JL, Pereira CCC, Ferreira LDSC, et al. Moderate Endemicity of the Human T-Lymphotropic Virus Infection in the Metropolitan Region of Belém, Pará, Brazil. Revista Brasileira de Epidemiologia. (2018) 21:1. doi: 10.1590/1980-549720180018
25. Rosadas and Graham. Health Inequities and HTLV-1. Lancet Microbe. (2022) 22:56. doi: 10.1016/S2666-5247(21)00330-X
26. Waters A, Oliveira AL, Coughlan S, de Venecia C, Schor D, Leite AC, et al. Multiplex Real-Time PCR for the Detection and Quantitation of HTLV-1 and HTLV-2 Proviral Load: Addressing the Issue of Indeterminate HTLV Results. J Clin Virol. (2011) doi: 10.1016/j.jcv.2011.05.022
27. Ayres M, Ayres Jr M, Ayres DL, Santos AS. BioEstat 5.3: Aplicações Estatísticas nas Áreas das Ciências Biológicas e Médicas. Belém. (2011) 364p.
28. Ishak R, Ishak MO, Azevedo VN, Santos DE, Vallinoto AC, Saraiva JC, et al. Detection of HTLV-IIa Blood Donors in an Urban Area of the Amazon Region of Brazil (Belém, PA). Rev Soc Bras Med Trop. (1998) 31:193–7. doi: 10.1590/S0037-86821998000200005
29. Ishak R, Vallinoto AC, Azevedo VN, Ishak Mde O. Epidemiological Aspects of Retrovirus (HTLV) Infection Among Indian Populations in the Amazon Region of Brazil. Cad Saude Publica. (2003)19:901–14. doi: 10.1590/S0102-311X2003000400013
30. Vallinoto AC, Muto NA, Pontes GS, Machado LF, Azevedo VN, dos Santos SE, et al. Serological and Molecular Evidence of HTLV-I Infection Among Japanese Immigrants Living in the Amazon Region of Brazil. Jpn J Infect Dis. (2004) 57:156-9.
31. Maneschy CA, Barile KAS, Castro JAA. Epidemiological and Molecular Profile of Blood Donors Infected With HTLV-1/2 in the State of Pará, Northern Brazil. Braz J Microbiol. (2021) 52, 2001–6. doi: 10.1007/s42770-021-00609-w
32. Guerra AB, Siravenha LQ, Laurentino RV, Feitosa RNM, Azecedo VN, Vallinoto ACR, et al. Seroprevalence of HIV, HTLV, CMV, HBV and Rubella Virus Infections in Pregnant Adolescents who Received Care in the City of Belém, Pará, Northern Brazil. BMC Pregnancy Childbirth. (2018) 18:169. doi: 10.1186/s12884-018-1753-x
33. Caterino-De-Araujo A; Rodrigues Campos K. Defective Particles of Human T-Lymphotropic Virus and Negative Results in Molecular Assays. Infect Genet Evol. (2021) 96:1. doi: 10.1016/j.meegid.2021.105141
Keywords: HTLV-1, HTLV-2, epidemiology, Belém, Amazonia
Citation: Lopes FT, de Sousa RS, Carvalho Gomes JL, Vallinoto MC, de Lima ACR, Lima SS, Freitas FB, Feitosa RNM, Rangel da Silva ANM, Machado LFA, Aben-Athar CYP, Maia da Silva EL, Cayres Vallinoto IMV and Vallinoto ACR (2022) The Relevance of a Diagnostic and Counseling Service for People Living With HTLV-1/2 in a Metropolis of the Brazilian Amazon. Front. Public Health 10:864861. doi: 10.3389/fpubh.2022.864861
Received: 28 January 2022; Accepted: 16 February 2022;
Published: 28 March 2022.
Edited by:
Juarez Antonio Simões Quaresma, Universidade do Estado do Pará, BrazilReviewed by:
Marizete Argolo Teixeira, Universidade Estadual do Sudoeste da Bahia, BrazilDenise Utsch Gonçalves, Federal University of Minas Gerais, Brazil
Marcos Antonio Custódio Neto Da Silva, Federal University of Maranhão, Brazil
Copyright © 2022 Lopes, de Sousa, Carvalho Gomes, Vallinoto, de Lima, Lima, Freitas, Feitosa, Rangel da Silva, Machado, Aben-Athar, Maia da Silva, Cayres Vallinoto and Vallinoto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Carlos R. Vallinoto, dmFsbGlub3RvQHVmcGEuYnI=