
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 13 July 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.862978
This article is part of the Research TopicCOVID-19 Pandemic: Mental Health, Life Habit Changes and Social PhenomenaView all 70 articles
 Sabine Felser1*
Sabine Felser1* Corinna Sewtz1Ursula Kriesen1Brigitte Kragl1
Corinna Sewtz1Ursula Kriesen1Brigitte Kragl1 Till Hamann2Felix Bock3
Till Hamann2Felix Bock3 Daniel Fabian Strüder4Clemens Schafmayer5Désirée-Louise Dräger6
Daniel Fabian Strüder4Clemens Schafmayer5Désirée-Louise Dräger6 Christian Junghanss1
Christian Junghanss1Background: The COVID-19 pandemic led to visiting restrictions (VRs) of patients in hospitals. Social contacts between patients' relatives play an important role in convalescence. Isolation may cause new psychological comorbidity. The present study investigated the psychological distress of VR in in-patients and their relatives.
Methods: From April 1, 2020 to May 20, 2020, 313 in-patients (≥14 years) of the University Medical Center Rostock were interviewed by questionnaires and 51 relatives by phone. Subjective psychological distress was assessed by a distress thermometer [0 (not at all)−100 (extreme)]. The study also investigated stressors due to VR, psychological distress in dependence on demographic or disease-related data, currently used communication channels and desired alternatives and support.
Results: Relatives were more psychologically distressed by VR than in-patients (59 ± 34 vs. 38 ± 30, p = 0.002). Loss of direct physical contact and facial expressions/gestures resulted in the most distress. Psychological distress due to VR was independent of demographics and indicates small positive correlations with the severity of physical restriction and the general psychological distress of in-patients. The most frequent ways of communication were via phone and social media. Frequently requested alternatives for patients were other interlocutors and free phone/tablet use, for relatives visiting rooms with partitions.
Conclusion: VRs are a stressor for patients and their relatives. The establishment of visiting rooms with partitions and the free use of phones/tablets could reduce the additional distress.
As social beings, humans depend on interactions with others in group bonds and relationships. Especially during states of exception as hospitalization social contacts and clear targeted communication are of great relevance; however, depending on the situation often limited.
Information exchange regarding disease and therapy between physician, patient, and relatives has been shown to influence patient satisfaction, treatment outcome, the healing process, and compliance (1–4). Contact with family members and close friends has positive effects on the health, everyday experience, and wellbeing of hospital in-patients (5). Relatives are not only supporters, but also affected persons and caregiver, which leads to a multiple burden (6). As a result of the knowledge of the importance and positive effects of the patient-relative relationship, hospitals have established visiting hours. Visitation restrictions (VR) have existed since the first hospitals were founded in the early 1800's. These were to reduce the spread of diseases and protect patients and their families from stress (7). In 2020, severe restrictions on visiting hours and bans on visiting occurred as a result of the COVID-19 pandemic. WHO and the European Center for Disease Prevention and Control published strict public health measures and guidelines to reduce the spread of the Coronavirus (8). The German Bundestag declared an “epidemic situation of national significance” in March 2020 (9) and enacted legal Corona protection measures based on the WHO guidelines. In the middle of March 2020, severe VRs in hospitals were determined (10). Based on the evidence that isolation/quarantine for the prevention of infectious diseases can cause mental health problems, such as depression, anxiety, and insomnia, there has been intense debate about VR (11, 12). The psychological impact of VR resulting from the COVID-19 pandemic on hospitalized patients and their families is largely unknown. Preliminary study results on investigations in vulnerable groups (nursing home residents, patients in palliative and intensive care units including neonatology), relatives of hospitalized children, and those who tested positive for COVID-19 and their relatives showed increased lonesomeness, depressive symptoms, agitation, aggression, decreased cognitive abilities, and general dissatisfaction for patients. For relatives, concerns, fears, and insecurities occurred (13–19). The present study aimed to investigate prospectively: (I) Whether hospitalized patients and their relatives experience different levels of psychological distress as a result of COVID-19-related VR? (II) Which items are particularly distressing? (III) Whether demographic and disease-related data provide information about psychological distress? and (IV) Which communication channels alternative to personal contact are currently used and which additions in terms of communication channels are desirable?
The prospective study was designed as a two-arm cross-sectional study. A survey of in-patients and their relatives (relative was defined as the most important contact person) was conducted by questionnaire in person (patients) or by telephone interview (relatives).
From April 1st until May 20th, 2020, a self-designed questionnaire survey of in-patients (age ≥14 years) was conducted at 17 somatic clinics of the University Medical Center Rostock (UMR) with various areas of care. Questionnaires were only handed out to patients once during their stay with a length of stay ≥ 2 days. Further inclusion criteria were: ability to consent, German-speaking, and physical and cognitive ability to complete a questionnaire. For underage patients (14–17 years), these criteria applied with regard to the legal guardians. The patient questionnaire was administered during the informed consent interview to minimize the number of contacts. Questionnaires were distributed and collected by medical staff, nursing staff, and study center staff.
Patients were asked to provide a relative with contact details. If a relative was named, the study center staff contacted that person by telephone. After consent was given, the interview was conducted according to a standardized interview template. The interviews had an approximate duration of 10 min.
Participation in the survey was voluntary, and all patient/relative data were analyzed in a pseudonymous manner. The study was reviewed and approved by the ethics committee of the University of Rostock (A2020-68).
From March 13th, 2020, strict visiting restrictions to the in-patient areas of the Rostock University Medical Center applied. In individual cases, it was possible to deviate from this procedure. This resulted in inconsistent procedures for different areas. In wards with primarily cure-oriented intentions, patients with palliative diseases were under certain circumstances allowed to receive visitors. On the palliative ward, a maximum of two visitors per day were allowed to visit dying patients, only. Minor children were allowed to be accompanied by a healthy caregiver. The procedure in each individual case was determined by the facility manager of the respective department. The senior physicians in charge of the wards ensured implementation in consultation with the nursing teams. From May 20th, 2020, the strict visitation restrictions were abolished. Patients were then allowed to receive visits from caregivers again under strict conditions. This marked the end of this survey.
Assessed were age, gender, living situation, and the patient-relative relationship (e.g., spouses).
The following questions were asked of the patient: reason (diagnosis) for hospitalization, duration of illness to date, whether first hospitalization/in-patient stay, number of days spent as an in-patient, and expected length of stay.
Patients and relatives were asked to indicate on a distress thermometer (0 not at all and 100 extremely) how much they are currently physically restricted and under psychological pressure.
All participants were asked by means of 5-level Likert scales how important communication is in everyday life and direct communication with relatives, friends, etc. to them.
Patients and relatives recorded: preferred frequency of visits, missed communication elements (e.g., facial expressions/gestures), understanding of the visitation restrictions, the general and personal perception of the VR on 5-point Likert scales, and the severity of the communication restriction. The strength of subjective psychological distress as a result of the VR was recorded using a distress thermometer (0 not at all−100 extremely). To be able to assess which proportion of the patients/relatives were distressed and to what extent, the following grouping was performed: Value “0” on the visual analog scale (VAS) = “not stressed,” VAS > 0 ≤ 30 = “slightly stressed,” VAS > 30 ≤ 70 = “moderately stressed,” VAS > 70 ≤ 90 = “highly stressed,” and VAS > 90 = “very highly stressed.”
Patients and relatives were asked to provide information about the technologies used and ways of communication under the given conditions. In addition to given answer options, the respondents had the opportunity to add further technologies. Furthermore, wishes and possibilities for improvement in communication were surveyed. In addition to the predefined answer options, there was also the possibility of free-text options.
In addition to descriptive analysis, interval-scaled data were tested for normal distribution using the Shapiro–Wilk test. Depending on the scale level, correlations and mean differences were tested using the Pearson chi-square test, Spearman correlation, and Mann–Whitney U test, respectively. The level of significance was set at p ≤ 0.05. Cramer's V (CV), effect size (ES), and correlation coefficient r, respectively, were used to interpret the strength of the relationships depending on the scale level. SPSS 22.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis of the data.
A total of 313 patients participated in the survey. These provided eligible 85 relatives, 51 of whom agreed to the interviews.
The questionnaires were completed by 120 (38%) women and 191 (61%) men (no sex n = 2). The mean age of the total cohort was 60 ± 16 years. Two hundred and seventeen (69%) of the patients lived with partner(s) and/or child(ren) at the time of hospitalization (Table 2).
Interviews were conducted with 51 relatives (40 (78%) women and 11 (22%) men) with an average age of 60 ± 13 years. Seventy-eight percent of the relatives were married to the patients (Table 1). The relatives-patients groups differed in gender distribution (p < 0.001, ES = 0.508).
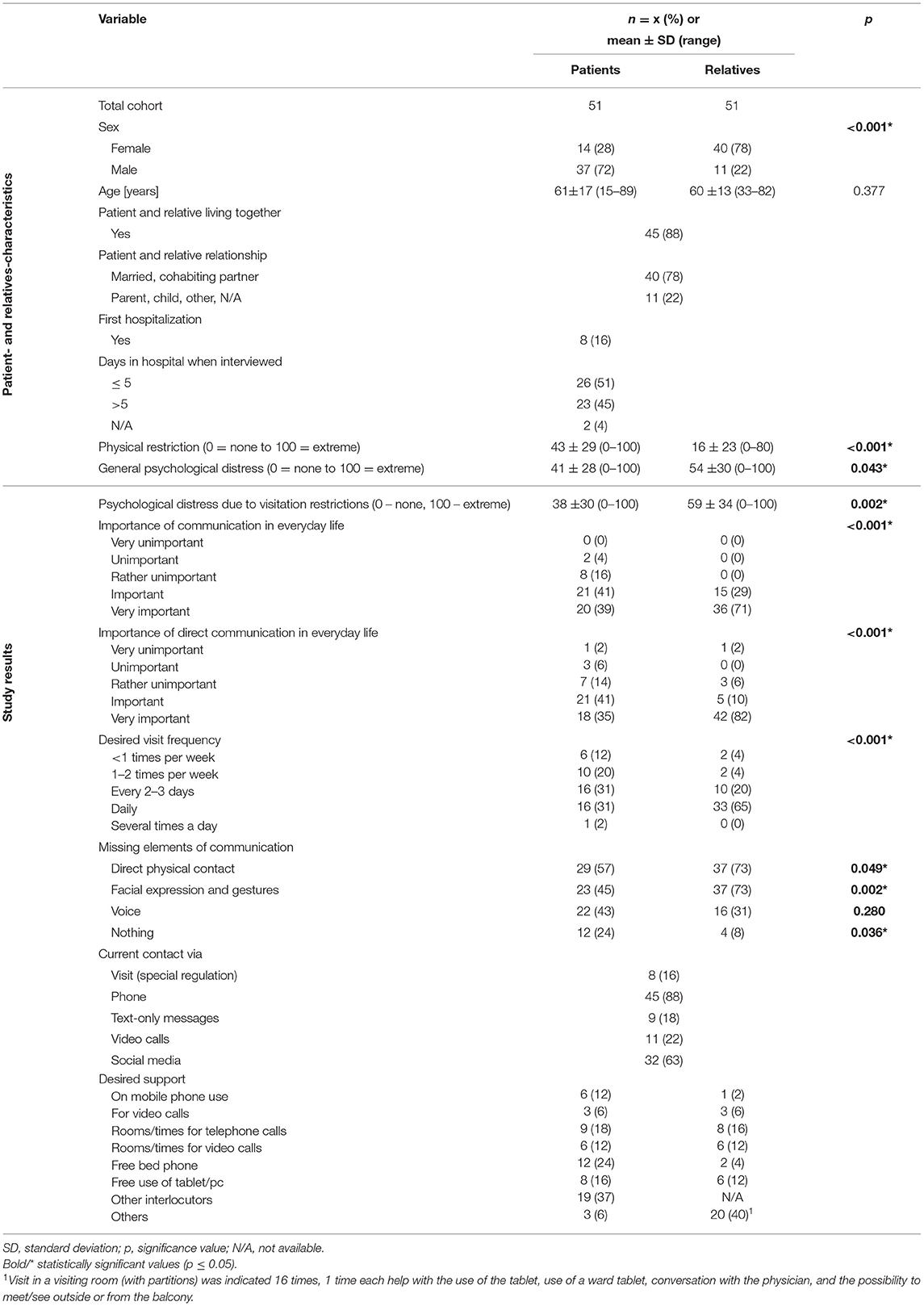
Table 1. Patient- and relatives-characteristics, study results.
Information on disease-related data can be found in Table 2. One-quarter of the patients each were assigned to neurological, surgical, or internal medicine institutions. Patients in the palliative care unit and patients hospitalized for COVID-19 infection were grouped under “palli/infect” (8%). “Other” facilities (18%) included radiation therapy, psychosomatics, dermatology, and pediatric and adolescent clinics. Approximately one-third of the patients surveyed were in-patients due to oncological disease.
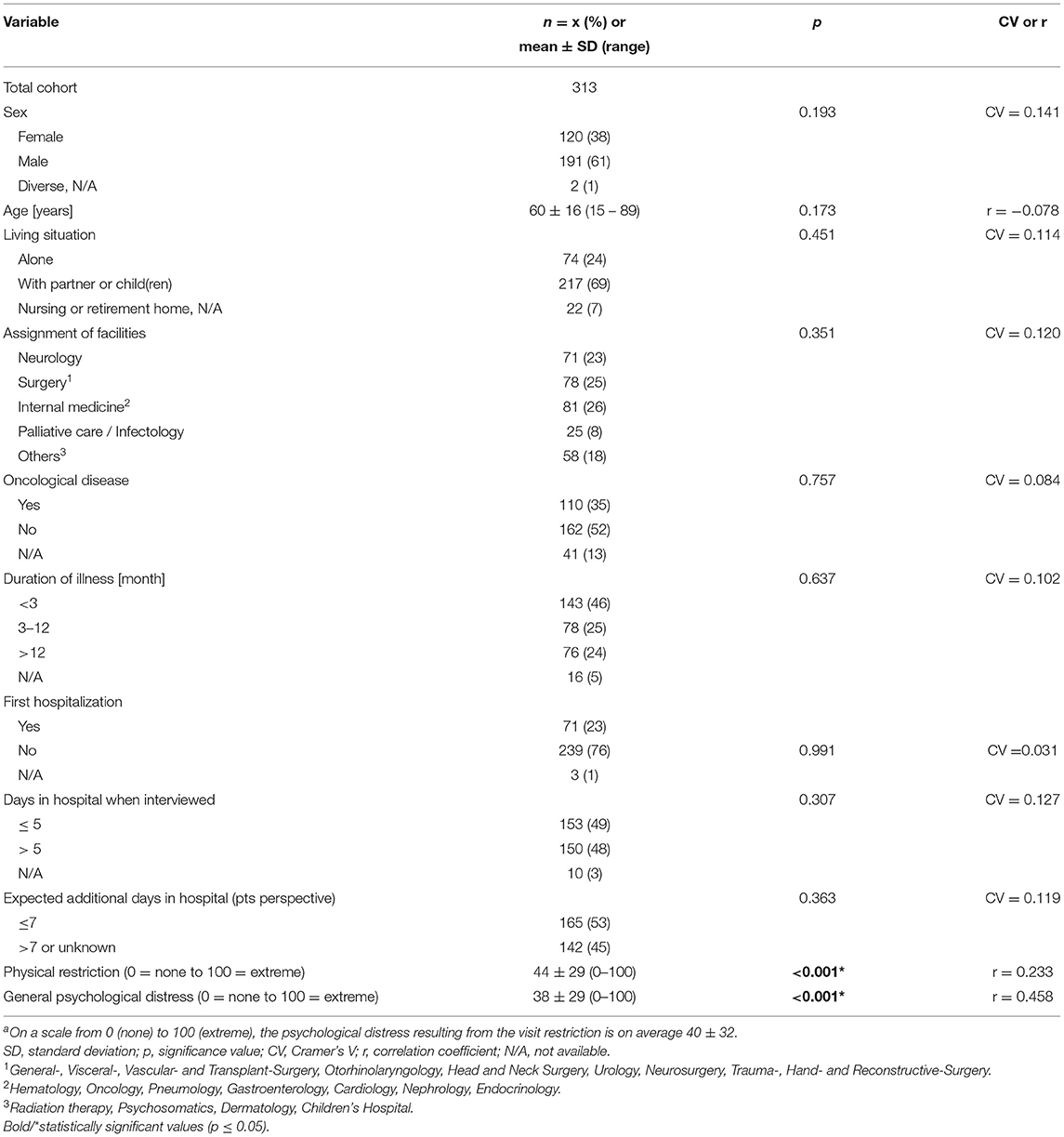
Table 2. Patient characteristics and association with psychological distress as a result of visit restrictiona.
Of all patients, physical impairment with a mean of 44 ± 29 was reported, and the current psychological distress with 38 ± 29.
The 51 family members reported a mean of 16 ± 23 for physical limitation and 54 ± 30 for current psychological distress. There were significant mean differences between patients and relatives for both factors (p < 0.001, ES = 0.466 and p = 0.043, ES = 0.200, respectively; Table 1).
Daily communication was considered important to very important by 80% of the patients and 100% of the relatives (p < 0.001, ES = 0.360). Direct communication with relatives, friends, etc. was considered (very) important by 76% of patients and 92% of relatives (p < 0.001, ES = 0.442; Table 1).
Desired visit frequencies and missed communication elements are shown in Table 1. While 33% of the patients wanted daily visits, 65% of the relatives did (p < 0.001, ES = 0.345). Most frequently, both, patients and relatives, missed direct physical contact and nonverbal communication by means of facial expressions and gestures.
Comprehension of the VRs was 96% for each of the patients and relatives, respectively.
Figure 1 gives a graphical overview of the psychological distress and the perception of VR in patients compared to relatives. On average, patients reported psychological distress due to VR as 40 ± 32, whereas relatives reported it as 59 ± 34. The proportion of severely and very severely distressed was higher among relatives (p = 0.002). The sex-stratified analysis shows a higher psychological distress of the relatives in both genders compared to the patients (male: patients vs. relatives 40 ± 32 vs. 66 ±29, p = 0.012, ES = 0.179; female: patients vs. relatives 41 ± 33 vs. 56 ± 35, p = 0.014, ES = 0.196).

Figure 1. Psychological distress and perception of visit restrictions by patients and relatives. *Statistically significant mean differences are indicated with *p < 0.05.
As shown in Table 2, there are no associations between the severity of psychological distress due to VR and demographic characteristics. In relation to the disease-related data, there were small or medium associations between psychological distress due to VR and the degree of physical impairment (p < 0.001) or general psychological distress (p < 0.001). These associations did not become apparent to relatives. The variance resolution between the parameters “general psychological distress” and “psychological distress due to VR” was 21% (patients) and 8% (relatives).
Of the 51 relatives, eight (16 %) had special visitation rights during the study period. The most frequently used means of communication were telephony and social media, which were used by 45 (88 %) and 32 (63 %) patient/relative pairs, respectively. Videotelephony was used to communicate by 11 (22%) patients/relatives pairs (Table 1).
Of all in-patients, 19 (37%) wished for other interlocutors (e.g., other in-patients and caregivers) as alternative visitors. Twelve (24%) wanted free bed phones and eight (16%) free use of tablet/PC. Relatives primarily used free text when indicating desired alternatives. Analysis of responses revealed that 16 (32%) desired patient visitations and suggested visitation rooms with partitions (e.g., glass partitions) as an option.
The study revealed that VR in hospitals to control the COVID-19 pandemic is an additional stressor for patients and their relatives. In the investigated cohort of in-patients and their relatives regardless of gender, relatives were more psychologically stressed by VR than patients. Direct physical contact and facial expressions/gestures were missed most by patients and relatives. Visitor rooms with partitions are a potential alternative to reduce psychological distress due to VR, especially for relatives. In the following, the causes and possible consequences of psychological distress due to VR and recommendations for action are discussed.
Almost all patients and relatives had an understanding of the VR and generally considered them to be (very) good. This is consequently considering the aim and reason for the VR was to protect these groups of people from infection, among other things. Nevertheless, the consequences of the VR had an impact on the mental conditions of patients and relatives. The collected data show that patients and relatives felt the psychological distress due to VR comparable to the general psychological distress they were exposed to in the actual situation. Both parameters, “general psychological distress” and “psychological distress due to VR” correlate only slightly with each other. The low variance resolution indicates that the VR is an additional stressor that is largely independent of other parameters. Consequently, VR places additional stress on the mental status of patients and relatives, as described by Meesters, among others, in mothers of infants (14).
Since the study presented here is cross-sectional, no concrete statements can be made about the medium- and long-term consequences among the respondents. In addition, the psychological distress due to VR was not assessed qualitatively. But based on the fact that elective procedures were severely restricted during the study period as part of the provision of ICU capacity in the context of the COVID-19 pandemic, it can be assumed that patients were confronted with more serious medical conditions (more than one-third were hospitalized due to cancer). The impact of VR during the COVID-19 pandemic on the wellbeing of hospitalized patients and their visitors, particularly in vulnerable populations, was examined by Inees et al. (20). Overall, the VRs were associated with negative emotions and detrimental effects on most in-patients and their families, especially in the context of end-of-life care (21). In end-of-life care, limiting visits or prohibiting visits resulted in inadequate emotional and spiritual care/support for patients and anxiety and despair among family members (22, 23). Patients were afraid of dying alone (24). In patients in the postoperative period, VR affected satisfaction with the hospital experience, and patients without visitors reported social isolation due to a lack of psychosocial support (25).
We suspect that the greater psychological distress on relatives results in part from the fact that they could not form their own impression of the patient's condition. It is known that inadequate information is a stressor for negative psychological effects such as posttraumatic stress symptoms, confusion, and anger (26). Furthermore, relatives feel helpless and guilty, because they cannot support their beloved ones (24). In addition, due to the extensive Corona protection measures, the relatives were exposed to additional restrictions (e.g., quarantine, contact blocks, and distance regulations) in everyday life, which have direct negative psychological consequences (11, 12, 26, 27). Furthermore, the data suggest that patients, although more physically limited than their relatives, felt cared for well in the hospital. Different data show that an in-patient environment with appropriate medical presence and participatory decision-making processes can contribute to anxiety reduction and higher satisfaction (2, 3, 28).
Even if VR contribute to a reduction of surgical site infections in postoperative patients (29), this does not outweigh the sum of the mentioned serious consequences for patients and their relative. Urgent action is needed to reduce or prevent the negative psychological effects and psychiatric symptoms resulting from VR.
No predictors of the severity of psychological distress were identified within the demographic parameters analyzed. Also, length of hospitalization, single or repeated hospitalization, or cause of hospitalization (e.g., neurologic, surgical, and palliative) did not provide information on the severity of psychological distress due to VR. Only the severity of physical limitations and/or the general psychological distress the patients were under, showed a small positive correlation with psychological distress due to VR. For this reason, all patients should be given the necessary attention and offered help in dealing with VR.
Relatives, independent of the gender, claimed to have more distress than in-patient due to VR. This can partly be explained by the higher importance of communication and interpersonal relationships among the relatives. Thus, the desire to visit the in-patients was more pronounced among the relatives than the desire to get visited among the patients. During the study period, patients and relatives communicated most frequently via phone and social media. Consequently, direct physical contact and facial expressions/gestures were missed the most. While patients mentioned other interlocutors (e.g., other patients and caregivers) as a possible alternative, the establishment of visiting rooms with protective measures (e.g., partition walls/glasses) was most frequently desired by relatives. Video calls were used by only a few and were also mentioned as an alternative by only a few. We suspect that lack of experience, technical difficulty, and lack of access to a device are barriers. However, unsuitability for patients, e.g., due to sedation, could also be a reason (30). According to the answers, especially patients could benefit from free phone, tablet, and/or PC use. In addition, the patients' and relatives' requests for rooms/times for phone and video calls indicate a desire for more privacy.
To protect mental health, the establishment of visiting rooms with partitions and free phone/chat rooms as alternative communication channels for patients and relatives in clinics should be examined and implemented. These measures could reduce psychological distress, especially for the relatives of in-patients, due to visual contact, an improved flow of information, and more privacy. Special attention should be paid to bed-ridden patients with limited communication skills (e.g., sedation, mechanical ventilation, and tracheostomy) and their relatives (31).
Since the Corona case numbers in the federal state, where the investigation was performed (Mecklenburg-Vorpommern) during the study period were rather low compared to other federal states (from mid-March to the end of May 2020, 15 Corona patients were treated at UMR, three of them intensively; all patients were discharged), it can be assumed that the psychological distress of patients and their relatives was even higher in risk areas. Further research is needed to take targeted measures to benefit the mental health of patients and relatives during pandemic periods.
The survey was successfully conducted prospectively on a large cohort, despite the difficult baseline conditions, even for the study investigators. The service volumes and elective procedures were reduced at some hospitals during the survey period. The high number of oncological patients may be explained first by the fact that the study was led by the Department of Hematology, Oncology and Palliative Medicine (bias). Second, the treatments of these patients cannot be electively discharged. At the same time, this represents a strength, since specifically oncological patients were affected by VR.
Due to the involvement of a large number of clinics in the survey and the applicable contact restrictions, it was not possible to record exactly how many patients refused to participate, despite the coding of the questionnaires. A statement on the response rate is therefore not possible. As a result, a bias of the answers in the direction of socially desirable answers cannot be ruled out.
To keep the questionnaire and the interview duration short despite the complexity of the survey (aim: to increase the number of participants), only a visual analog scale and no standard psychological questionnaires were used to record psychological stress. As a consequence, no statements can be made about qualitative psychological stress. Whether and to what extent the visit restrictions had serious health consequences and which coping strategies were used should be investigated in further studies. Whether and to what extent the patients/relatives used psychotherapeutic services was not recorded and represents a further limitation of this study.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the University of Rostock. The patients consented to participate in the study by filling out the questionnaire. The relatives verbally agreed to be interviewed before the interview.
SF and CJ: conception of the work, data analysis and interpretation, and drafting the article. UK: conception of the work, data collection, and drafting the article. CSe: conception of the work and data collection. BK: data collection and head of study office. TH, FB, DS, CSc, and D-LD: data collection and critical revision of the article. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank all patients and relatives who participated in the survey. The authors want to thank the staff of all recruiting departments: Prof. Dr. med. Carsten Spitzer—Psychosomatic, Prof. Dr. med. Johann Christian Virchow—Pneumology, Prof. Dr. med. Georg Lamprecht—Gastroenterology, PD Dr. med. Alper Öner—Cardiology, Prof. Dr. med. Steffen Emmert—Dermatology, Prof. Dr. med. Emil Reisinger—Infectious Diseases, Prof. Dr. med. Steffen Mitzner—Nephrology, Dr. med. Steffen Sola—Neurosurgery, Prof. Dr. med. H. S. Willenberg—Endocrinology, Prof. Dr. med. Thomas Mittlmeier—Trauma, hand, reconstructive surgery, Dr. med. Hanne Lademann—Clinic for Pediatric and Adolescent Medicine and to the study nurse Carolin Schneider and the staff of the study center of the Medical Clinic III: Julia Grün and Silke Stellmacher-Kaiser.
1. Di Blasi Z, Harkness E, Ernst E, Georgiou A, Kleijnen J. Influence of context effects on health outcomes: a systematic review. Lancet. (2001) 357:757–62. doi: 10.1016/S0140-6736(00)04169-6
2. Geßner K. Wann Patienten zufrieden sind. Deutsches Ärzteblatt. (2017) 114:2–4. Available online at: https://www.aerzteblatt.de/archiv/185989/Kommunikation-Wann-Patienten-zufrieden-sind
3. Klemperer D. Partizipation der Patienten an medizinischen Entscheidungen. Manag Care. (2003) 7:9–11.
5. Pflegende Angehörige – Probleme, Belastungen und Unterstützungen |, Gesundheitsportal. (2020). Available online at: https://www.gesundheit.gv.at/leben/altern/wohnen-im-alter/pflegende-angehoerige-entlastungen-unterstuetzungen (accessed June 23, 2020).
6. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche, Krebshilfe, AWMF). Palliativmedizin für Patienten mit einer nicht heilbaren Krebserkrankung: Langversion 1.1, 2015, AWMF-Registernummer: 128/001OL. (2015). p. 268. Available online at: http://leitlinienprogramm-onkologie.de/Palliativmedizin.80.0.html (accessed June 25, 2020).
7. Smith L, Medves J, Harrison MB, Tranmer J, Waytuck B. The impact of hospital visiting hour policies on pediatric and adult patients and their visitors. JBI Lib Syst Rev. (2009) 7:38–79. doi: 10.11124/jbisrir-2009-181
8. World Health Organization. Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19: Interim Guidance. Geneva: World Health Organization (2020).
9. Bundesministerium für Gesundheit. Bundesrat stimmt Gesetzespaketen zur Unterstützung des Gesundheitswesens bei der Bewältigung der Corona-Epidemie zu. (2020). Available online at: https://www.bundesgesundheitsministerium.de/presse/pressemitteilungen/2020/1-quartal/corona-gesetzespaket-im-bundesrat.html (accessed June 25, 2020).
10. Deutscher Ärzteverlag GmbH, Redaktion Deutsches, Ärzteblatt. Corona: Krankenhäuser sollen ab Montag alle planbaren Eingriffe verschieben. (2020). Available online at: https://www.aerzteblatt.de/nachrichten/111034/Corona-Krankenhaeuser-sollen-ab-Montag-alle-planbaren-Eingriffe-verschieben (accessed June 25, 2020).
11. Hossain MM, Sultana A, Purohit N. Mental health outcomes of quarantine and isolation for infection prevention: a systematic umbrella review of the global evidence. Epidemiol Health. (2020) 42:e2020038. doi: 10.4178/epih.e2020038
12. Deutsche Gesellschaft für Psychiatrie und Psychotherapie, Psychosomatik und Nervenheilkunde, e,. V. Soziale Isolation kann psychisch krank Machen. (2020). Available online at: https://www.dgppn.de/presse/pressemitteilungen/pressemitteilungen-2020/soziale-isolation.html (accessed July 17, 2020).
13. Hugelius K, Harada N, Marutani M. Consequences of visiting restrictions during the COVID-19 pandemic: an integrative review. Int J Nurs Stud. (2021) 121:104000. doi: 10.1016/j.ijnurstu.2021.104000
14. Meesters N, van Dijk M, Sampaio de Carvalho F, Haverman L, Reiss IK, Simons SH, et al. COVID-19 lockdown impacts the wellbeing of parents with infants on a Dutch neonatal intensive care unit. J Pediatr Nurs. (2021). 62:106–12. doi: 10.1016/j.pedn.2021.09.024
15. Polloni L, Cavallin F, Lolli E, Schiavo R, Bua M, Volpe B, et al. Psychological Wellbeing of Parents with Infants Admitted to the Neonatal Intensive Care Unit during SARS-CoV-2 Pandemic. Children. (2021) 8:755. doi: 10.3390/children8090755
16. O'Caoimh R, O'Donovan MR, Monahan MP, Dalton O'Connor C, Buckley C, Kilty C, et al. Psychosocial impact of COVID-19 nursing home restrictions on visitors of residents with cognitive impairment: a cross-sectional study as part of the Engaging Remotely in Care (ERiC) project. Front Psychiatry. (2020) 11:585373. doi: 10.3389/fpsyt.2020.585373
17. Sizoo EM, Monnier AA, Bloemen M, Hertogh CM, Smalbrugge M. Dilemmas with restrictive visiting policies in dutch nursing homes during the COVID-19 Pandemic: a qualitative analysis of an open-ended questionnaire with elderly care physicians. J Am Med Dir Assoc. (2020) 21:1774–81.e2. doi: 10.1016/j.jamda.2020.10.024
18. Wammes JD, Kolk D, van den Besselaar JH, MacNeil-Vroomen JL, Buurman-van BM, van Rijn M. Evaluating perspectives of relatives of nursing home residents on the nursing home visiting restrictions during the COVID-19 crisis: a dutch cross-sectional survey study. J Am Med Dir Assoc. (2020) 21:1746–50.e3. doi: 10.1016/j.jamda.2020.09.031
19. Hyczko AV, Fu C, Graf Z, Perkowski CD, Whyte-Nesfield MM, Zhou S, et al. Evaluating Pediatric Families' Understanding of and Reactions to COVID-19 Visitor Restrictions. J Patient Exp. (2022) 9:23743735221077547. doi: 10.1177/23743735221077547
20. Iness AN, Abaricia JO, Sawadogo W, Iness CM, Duesberg M, Cyrus J, et al. The Effect of hospital visitor policies on patients, their visitors, and health care providers during the COVID-19 pandemic: a systematic review. Am J Med. (2022). doi: 10.1016/j.amjmed.2022.04.005. [Epub ahead of print].
21. Boulton AJ, Jordan H, Adams CE, Polgarova P, Morris AC, Arora N. Intensive care unit visiting and family communication during the COVID-19 pandemic: A UK survey. J Intens Care Soc. (2021). doi: 10.1177/17511437211007779. [Epub ahead of print].
22. Onwuteaka-Philipsen BD, Pasman HR, Korfage IJ, Witkamp E, Zee M, van Lent LG, et al. Dying in times of the coronavirus: an online survey among healthcare professionals about end-of-life care for patients dying with and without COVID-19 (the CO-LIVE study). Palliat Med. (2021) 35:830–42. doi: 10.1177/02692163211003778
23. Feder S, Smith D, Griffin H, Shreve ST, Kinder D, Kutney-Lee A, et al. “Why Couldn't I Go in To See Him?” bereaved families' perceptions of end-of-life communication during COVID-19. J Am Geriatr Soc. (2021) 69:587–92. doi: 10.1111/jgs.16993
24. Sudai M. Not dying alone: the need to democratize hospital visitation policies during COVID-19. Med Law Rev. (2021) 29:613–38. doi: 10.1093/medlaw/fwab033
25. Zeh RD, Santry HP, Monsour C, Sumski AA, Bridges JF, Tsung A, et al. Impact of visitor restriction rules on the postoperative experience of COVID-19 negative patients undergoing surgery. Surgery. (2020) 168:770–6. doi: 10.1016/j.surg.2020.08.010
26. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
27. Czeisler MÉ, Wiley JF, Facer-Childs ER, Robbins R, Weaver MD, Barger LK, et al. Mental health, substance use, and suicidal ideation during a prolonged COVID-19-related lockdown in a region with low SARS-CoV-2 prevalence. J Psychiatr Res. (2021) 140:533–44. doi: 10.1016/j.jpsychires.2021.05.080
28. Sewtz C, Muscheites W, Grosse-Thie C, Kriesen U, Leithaeuser M, Glaeser D, et al. Longitudinal observation of anxiety and depression among palliative care cancer patients. Ann Palliat Med. (2021) 10:3836–46. doi: 10.21037/apm-20-1346
29. Losurdo P, Paiano L, Samardzic N, Germani P, Bernardi L, Borelli M, et al. Impact of lockdown for SARS-CoV-2 (COVID-19) on surgical site infection rates: a monocentric observational cohort study. Updates Surg. (2020) 72:1263–71. doi: 10.1007/s13304-020-00884-6
30. Rose L, Yu L, Casey J, Cook A, Metaxa V, Pattison N, et al. Communication and Virtual Visiting for Families of Patients in Intensive Care during the COVID-19 Pandemic: A UK National Survey. Ann Am Thorac Soc. (2021) 18:1685–92. doi: 10.1513/AnnalsATS.202012-1500OC
Keywords: communication, COVID-19, psychological distress, stress, visit restriction
Citation: Felser S, Sewtz C, Kriesen U, Kragl B, Hamann T, Bock F, Strüder DF, Schafmayer C, Dräger D-L and Junghanss C (2022) Relatives Experience More Psychological Distress Due to COVID-19 Pandemic-Related Visitation Restrictions Than In-Patients. Front. Public Health 10:862978. doi: 10.3389/fpubh.2022.862978
Received: 26 January 2022; Accepted: 06 June 2022;
Published: 13 July 2022.
Edited by:
Xenia Gonda, Semmelweis University, HungaryReviewed by:
Peter Nydahl, University Medical Center Schleswig-Holstein, GermanyCopyright © 2022 Felser, Sewtz, Kriesen, Kragl, Hamann, Bock, Strüder, Schafmayer, Dräger and Junghanss. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabine Felser, c2FiaW5lLmZlbHNlckBtZWQudW5pLXJvc3RvY2suZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.