 Xue-Bing Wang1
Xue-Bing Wang1 Gordon Chih Ming Ku
Gordon Chih Ming Ku Chin Hsien Hsu
Chin Hsien Hsu- 1School of Tourism Management, Wuhan Business University, Wuhan, China
- 2Department of Leisure and Recreation Management, Asia University, Taichung, Taiwan
- 3Department of Sport Management, National Taiwan University of Sport, Taichung, Taiwan
- 4Department of Sport Performance, National Taiwan University of Sport, Taichung, Taiwan
- 5Department of Leisure Industry Management, National Chin-Yi University of Technology, Taichung, Taiwan
- 6Department of Business Administration, National Yunlin University of Science and Technology, Douliu, Taiwan
The COVID-19 global pandemic and the uneven distribution of vaccines have resulted in alternative medical tourism, vaccine tourism. The purpose of this study is to identify the antecedents of vaccine tourists' travel intention. The Stimulus-organism-response model was used as a framework to understand the relationship between risk perception (stimulus), pandemic prevention attitude (organism), decision making (organism), and travel intention (response) in vaccine tourism. An online questionnaire survey method was adopted to address the purpose of the research. Purposive and snowball sampling were used to select eligible respondents who were over 18 years old and had experience in vaccine tourism. A total of 520 online questionnaires were collected, and description analysis, confirmatory factor analysis, and structural equation modeling were utilized to analyze the collected data. The findings indicated that pandemic prevention attitude is a full mediator between risk perception and travel intention. There is a significant causal relationship between risk perception and pandemic prevention attitude and between pandemic prevention attitude and travel intention. Furthermore, tourists' travel decision-making also significantly influences their travel intention. However, the relationship between tourists' risk perception and travel decision-making has no significant effect. Vaccine tourism was created based on the COVID-19 context. Therefore, in order to avoid vaccine travel becoming an infection control breach, pandemic prevention planning and the medical quality of the destination, and the prevention policies between the countries should be completely assessed and conducted.
Introduction
Background and problem statement
Medical tourism is an international or long-distance tourism activity that aims to obtain medical services and combines leisure, business, and other purposes (1, 2). In the COVID-19 context, the global pandemic and the uneven distribution of vaccines have resulted in the prevalence of alternative medical tourism, vaccine tourism. Taiwan faces the problem of vaccine shortage during the pandemic, which has led to people traveling abroad for vaccination. According to statistics from the Tourism Bureau (3), since the United States opened the vaccine system for foreign tourists, many Taiwanese tourists to the United States have increased every month. For example, in May 2021, the number of Taiwan tourists to the United States reached 7,188, an increase of 428.53% over the same period last year. Thus, it can be seen that, even though there are certain risks in going abroad for vaccination, the uncertainty of pandemic control and vaccine supply is one of the main reasons for Taiwanese people to travel abroad for vaccination.
Tourism risk perception is one issue that influences tourists' attitude and decision-making process toward tourism, which hinders tourists' travel intentions (4, 5). Tourists usually assess the risks they may encounter during their travel, including the risks between the origin and destination and the destination itself, and determine their travel intention or change the destination according to the perceived risks (6, 7). Zhu and Deng (8) found that, during the COVID-19 pandemic, there has been a significant negative relationship between the risk perception and travel intention of rural tourism tourists. However, the journey, especially during aircraft travel, is one of the common ways to be infected with COVID-19 (9), and while the control of the pandemic abroad is not explicit, Taiwanese still choose to go abroad to get vaccinated. Therefore, whether the relationship between risk perception, attitude, and decision-making regarding vaccine tourism in the COVID-19 context is different from that of other tourism activities is one of the focuses of this study.
The pandemic prevention attitude is an essential factor directly affecting tourists' travel intention in the COVID-19 context (4, 5). The pandemic prevention attitude of tourists represents their confidence in pandemic control, which is related to the integrity and implementation of pandemic prevention measures taken by government departments (10). The more positive the pandemic prevention attitude of tourists, the higher their travel intention (4). However, the relationship between pandemic prevention attitude and travel intention may vary with different tourism activities. In terms of vaccine tourism in Taiwan, most Taiwanese tourists traveling abroad for vaccination will consider the uncontrolled pandemic situation and lack of access to vaccines locally, which has indirectly contributed to the development of vaccine tourism and is different from other tourism situations. Therefore, the relationship between the pandemic prevention attitude of vaccine tourists and their travel intention is worthy of further study.
Consumer behavior, decision-making factors are essential mechanisms affecting tourists' behavior (11, 12). The decision-making process of tourists is influenced by tourists' demand cognition, information search, scheme evaluation, consumption behavior, post-consumption evaluation, and feedback (13). Therefore, tourists' travel attitudes, activities, ideas, and experiences are all factors that affect their travel decision-making process (14). Many previous studies have shown that the factors influencing tourists' decision making have a significant impact on their choice of tourist destinations and their behaviors (15), and the research topics were mainly mass tourism, outbound tourism (16), domestic tourism (17), marine tourism (18), and medical tourism (19–21). Although many studies focused on exploring the factors influencing the decision-making of medical tourism, most types of medical tourism were mainly for health care, such as health examinations. Therefore, they were usually under the condition that they were allowed to travel abroad usually. In the context of COVID-19, vaccine tourism is another way to ensure life safety for countries with a shortage of vaccines, rather than promoting physical health. Moreover, when traveling abroad for vaccine tourism, it is no longer enough just to consider the quality of local medical services, reputation, and destination image, meaning the personal pandemic prevention attitude and risk of infection are the priority factors affecting tourists' travel decisions (22) when determining whether or not to travel abroad for vaccination.
A stimulus-organism-response (SOR) model can be seen as a framework for exploring the vaccine tourism behavior in the context of COVID-19. The SOR model has been used to measure the link between the input (stimulus), process (organism), and output (response) of the tourism behavior and to understand the factors and processes that influence tourists' behavior (23, 24). In retrospect, the related topics of SOR model application in tourism include virtual reality tourism (23), honeymoon tourism (25), nature-based tourism (26), and sports tourism (27). These studies found a variety of different stimulus variables and process variables to predict tourist behavior. Their results provide an effective way to further understand the behavior of tourists during different types of tourism; however, no studies are using the SOR model to understand tourists' behavior in vaccine tourism. Especially during the global COVID-19 pandemic, the risk perception of tourists (stimulus) may affect their pandemic prevention attitude (organism), which in turn affects their decision making to travel abroad for vaccination, and finally, leads to their behavioral intention of vaccine tourism (response). Accordingly, in this study, the SOR model was used as the framework to explore the relationship between the risk perception, pandemic prevention attitude, decision making, and travel intention of vaccine tourists traveling abroad for vaccination.
Stimulus-organism-response model
The SOR model is proposed by Mehrabian and Russell (28) and is used to understand the impact of external environmental stimulus (S) on individual emotions (O), and finally, form specific behaviors (R). In tourism, the SOR model is used to explain the impact of a tourist destination environment on tourists' inner emotions and the generation of their behaviors (26). The SOR model is composed of antecedent variables, intervening variables, and outcome variables (28). The antecedent variable refers to the external environment attributes. Tourists will stimulate their psychological state through their five senses. The intervening variables refer to the process of the internal psychological responses produced by external stimuli, representing tourists' emotional state. The outcome variables refer to the behavioral responses of tourists, which emotions may influence to produce the approach behavior and avoidance behavior (28). From the perspective of consumer behavior, the approach behavior refers to the positive behavioral response of consumers caused by the stimuli of the external environment, which can be regarded as consumers' desire to stay, look around, explore, and socialize in a specific environment (29). On the contrary, avoidance behavior refers to the negative behavioral response produced by consumers after receiving environmental stimuli, and their intention to stay in the environment is relatively low (29). Among them, the approach behavior can be divided into actual approach behavior and intended approach behavior; the actual approach behavior refers to the behavior that has been realized, while the intended approach behavior refers to the intention of the behavior (30, 31). In tourism research, travel intention is usually used to measure the intended approach behavior of tourists (23). According to the SOR model, this study set the risk of tourists to the external environment of tourism as an antecedent variable (S), which may have an impact on their pandemic prevention attitude (O1) and decision-making process (O2). It will ultimately determine the intention to travel abroad for vaccination (R).
Stimulus: Risk perception
Risk perception refers to the possibility of negative results (32). Tourism risk perception can be regarded as the negative result or process that tourists' subjective judgment may produce in the tourism environment, mainly due to the asymmetry between tourism safety information and subjective perception (8, 33). Tourism risk perception is based on tourists' environmental knowledge of the destination and generated through subjective and objective assessment, beyond the critical point of negative impact in the journey (24). Therefore, tourism risk perception can be regarded as the risk awareness generated by external environmental stimuli in tourism. However, the risk perception of vaccine tourism is different from that of other types of tourism activities, and there is a certain degree of risk in treatment. Therefore, in addition to medical treatment and tourism costs for tourists, the risk of nosocomial infection caused by different sanitary conditions is also one of the major risks of medical tourism in other countries (34, 35). Similarly, in addition to the high cost of travel, medical treatment, and quarantine when traveling abroad for vaccination, the most critical risk of vaccine tourism is the possibility of catching the disease. However, due to the shortage of vaccines in Taiwan, even if the pandemic situation in foreign countries has not been controlled, people are still traveling abroad for vaccination to protect their lives. Therefore, it is worth exploring whether tourism risk perception will affect tourists' intention to medical tourism, as well as their pandemic prevention attitude and travel decision-making.
Tourists' attitude is related to their risk perception in the COVID-19 context (5). As risk perception represents a loss to some extent, it has a negative impact on tourists' behavior and attitude (36); for example, Rather (5) found that tourists' risk perception had a significant negative impact on their attitude. However, a study on untact travel by Bae and Chang (36) found that tourism risk perception had a significant positive impact on attitude, as they considered untact travel as a health promotion behavior to reduce tourism risk. Similarly, vaccination is also a health promotion behavior; the higher tourists' risk perception, the more positive their pandemic prevention attitude. Accordingly, this study proposes the following hypothesis:
H1: Vaccine tourists' risk perception significantly influences their pandemic prevention attitude.
The risk perception of tourists has a significant impact on their travel decision-making (37). When tourists believe that tourism satisfaction will be reduced due to risk perception, they usually change the process of travel decision making and the choice of destination (7); the higher the risk perception, the higher the chance to change the decision. Polas et al. (37) found that the risk perception of medical tourism had a significant positive impact on travel decision-making. Therefore, the travel decision-making process of vaccine tourists may also be affected by risk perception. Thus, this study proposes the following hypothesis:
H2: Vaccine tourists' risk perception significantly influences their travel decision-making.
High-risk perception is the main reason for reducing tourists' travel intention (38). Although many studies have explored the relationship between tourists' risk perception and travel intention, the research results showed that the relationship between the two variables was not very stable. For example, Qi et al. (39) found no significant correlation between the perception of financial risk, physical risk, psychological risk, social risk, and time risk of mega-event tourists and their travel intention. On the contrary, in their research on tourism after the nuclear disaster in Japan, Chew and Jahari (38) found that financial risk, physical risk, psychological risk, and social risk all had a significant negative impact on travel intention; therefore, the relationship between risk perception and travel intention will vary according to the different types of tourism activities. The relationship between the risk perception and travel intention of vaccine tourists has not been explored, and it is worth further understanding, especially in the context of COVID-19. Based on the above literature review, this study proposes the following hypothesis:
H3: Vaccine tourists' risk perception significantly influences their travel intention.
Organism: Pandemic prevention attitude and decision-making
The pandemic prevention attitude and travel decision-making can be regarded as the psychological state generated by tourists' perception of the external physical risking the COVID-19 context. The pandemic prevention attitude refers to people's perception of the decisions or beliefs about implementing pandemic prevention policies (4). The perception of the pandemic prevention attitude is based on the effectiveness of the government in controlling the pandemic, which affects people's confidence in participating in tourism activities (3). Luan et al. (40) suggested that pandemic prevention strategies can be divided into primary and secondary strategies. The primary strategy is a direct pandemic prevention method, meaning vaccination. The second strategy is indirect pandemic prevention, including wearing masks, isolation from infected persons and close contacts, regular disinfection of public places, mass screening, and strengthening public awareness health education. Effective pandemic prevention strategies and knowledge advocacy can help to increase civic behavior among tourists, ensure travel safety, and strengthen social forces against the COVID-19 pandemic (41). Tseng et al. (4) found that the pandemic prevention attitude of tourists had a significant positive impact on their travel intention; therefore, the more positive the pandemic prevention attitude of vaccine tourists, the higher their intention to travel abroad for vaccination. Accordingly, this study proposes the following two hypotheses:
H4: Vaccine tourists' epidemic prevention significantly influences their travel intention.
H5: Vaccine tourists' risk perception indirectly influences travel intention through pandemic prevention attitude.
Travel decision-making is a factor that directly affects tourists' travel intention. Travel intention can be regarded as the result of tourists' psychological decision-making process, which leads to the actual tourism behavior and transforms perceived value into actual behavior (42). Risk perception is one of the critical factors affecting the decision-making process of tourists. Especially in the COVID-19 context, understanding the relationship between tourists' tourism risk perception and travel decision-making can help the tourism industry draw up restart and recovery plants in the post-pandemic era and provide clear supply management strategies for the tourism industry (42). Many studies have confirmed a significant relationship between risk perception, travel decision-making, and travel intention (42–44). This study focused on the relationship between tourism risk perception, decision making, and travel intention of vaccine tourists. Accordingly, this study proposes the following two hypotheses:
H6: Vaccine tourists' travel decision-making significant influences their travel intention.
H7: Vaccine tourists' risk perception indirectly influences travel intention via travel decision-making.
Response: Travel intention
Travel intention is the intention of tourists to transform the results and motivation of the psychological process into actual behavior, which can also be regarded as a form of behavior intention (45). Travel intention is generated by rationally evaluating the potential benefits and costs of a series of alternative tourist destinations through external information (46). Thus, medical tourism intention can be regarded as tourists' rational evaluation of medical and tourism information, and then, they transfer the decision-making and motivation into the intention of actual behavior. A review of relevant studies on the travel intention of medical tourism shows that the factors affecting travel intention include electronic word-of-mouth (47, 48), destination trust (47), motivation (49), risk perception (49), destination image (48–50), attitude (50), subjective norms (50), and perceived behavioral control (50). However, in the COVID-19 context, there is a lack of research on tourists' risk perception, pandemic prevention attitude, travel decision making, and travel intention in medical tourism with vaccination as the main purpose, especially in countries with a shortage of vaccines. Based on the above literature review and the SOR model framework, this study proposes the following research framework (Figure 1).
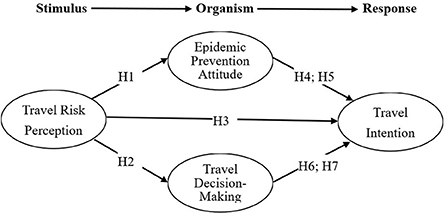
Figure 1. Research framework of medical tourists' intention.
Methods
Research design
This study used the SOR model to explore the relationship between tourism risk perception, pandemic prevention attitude, travel decision-making, and travel intention of vaccine tourism among Taiwanese people traveling abroad for vaccination. After determining the research topic, a quantitative research method was selected as the basis of the overall research design to meet the research issue. This study collected data through a questionnaire survey, and the questionnaire was prepared by referring to relevant literature. Before the formal distribution of the questionnaire, this study adopted a pre-test and invited two experts in related fields to review the questionnaire content to ensure its surface validity and content validity. Furthermore, this study selected adults over 18 years of age as the subjects for the formal distribution of the questionnaire, and questionnaire data were collected through online questionnaires. Finally, statistical software was used to analyze the data and present the results.
Data collection
This study used purposive and snowball sampling to select tourists over 18 who had traveled abroad for vaccination as the research objects. Tourists under the age of 18 and those who had not traveled abroad for vaccination were excluded. This study used google forms as the platform for questionnaire data collection (https://docs.google.com/forms). Eligible respondents were invited to fill out the questionnaire through online social network platforms, Line and Facebook, and were asked to share the online questionnaire with their acquaintances. Snowball sampling assisted this study in reaching the respondents who were impossible or prohibitively expensive (51). Especially in the COVID-19 context, social distance is a huge constraint for investigation. Snowball sampling increased the efficiency and quality of questionnaire distribution. The questionnaires were collected from July 1 to July 31, 2021. During this period, five hundred and fifty online questionnaires were collected, and 520 valid questionnaires were obtained after excluding the invalid questionnaires (the answers were all the same and the IP addresses of the online questionnaires were repeated) for a valid questionnaire rate of 94.5%.
Measures
The questionnaire of this study consists of three parts. The first part is the content of informed consent, including the description of the purpose of this study and the related rights of the research objects. The second part is the scale of tourism risk perception, pandemic prevention attitude, travel decision-making, and travel intention (Table 1). The tourism risk perception (17) included three dimensions, namely “social risk”, “psychological risk”, and” financial risk”, with seven items in total; the pandemic prevention attitude scale has consisted of three items. The travel decision-making scale (17) contained three dimensions, namely “commercial source”, “experiential source”, and “public source”, with six items in total; Travel intention scale was comprised of three items. A Likert 5-point scale was used to be the measurement benchmark, with “Strongly agree” to “Strongly disagree” represented by 5 to 1 points, respectively. The third part is the demographic, including gender, age, marriage, education level, occupation, average monthly income, and residence.
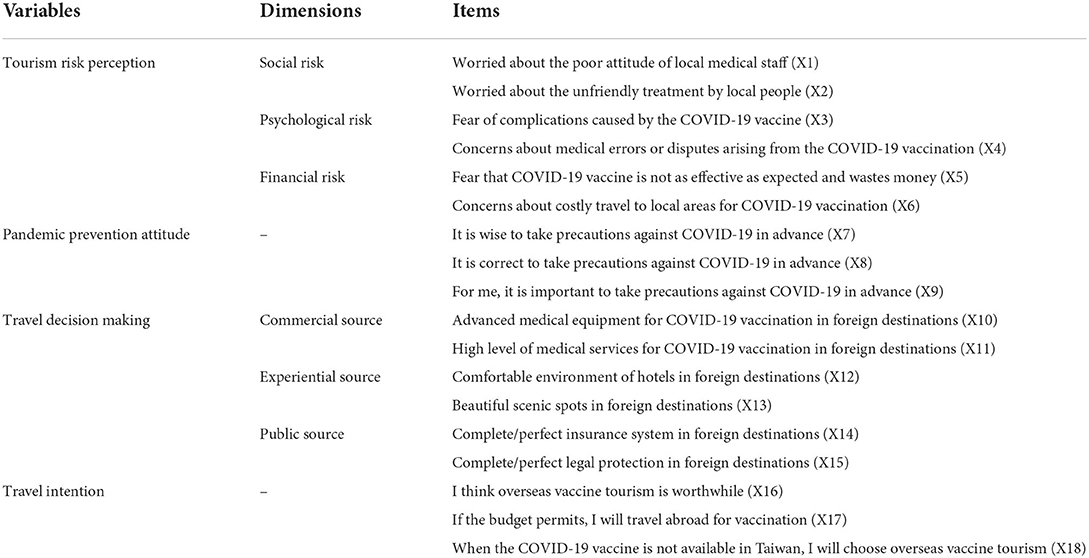
Table 1. Scale of tourism risk perception, pandemic prevention attitude, travel decision-making, and travel intention.
Ethical considerations
In order to comply with research ethics, an anonymous questionnaire survey was conducted in this study to ensure that the personal information of respondents could not be identified. The research respondents must be at least 18 years old to participate in this study, and those under 18 years old were excluded. This study provided the content of informed consent on the first page of the questionnaire to inform the purpose of the study and the respondents' rights. The respondents understood and agreed to participate in the survey voluntarily. If the respondents were not willing to participate in the survey or withdrew from this study during the completion, their rights and interests would not be affected, and the results would not be adverse. The collected data can only be reviewed and analyzed by the researchers and will not be used for any purpose other than academic research. The researchers will destroy the data themselves after the publication of this study.
Data analysis
This study used SPSS18.0statistical software to analyze the mean, standard deviation, skew, and kurtosis of the demographic background variables and questions. AMOS 23.0 structural equation was used to conduct confirmatory factor analysis (CFA) to test the reliability and validity of the variables in this study. Structural model analysis was used to test the relationship between tourism risk perception and pandemic prevention attitude, travel decision making, and travel intention.
Results and discussion
Demographic
According to the demographic of the samples in this study, men (55.0%) were slightly more than women (45.0%). Most of the samples were aged from 41 to 50 (29.8%). More than half of the samples were married (68.2%). Nearly half of the samples earned more than NTD 45001 per month on average (45.6%) 0.55.6% of the samples had a college or junior college degree. Most of the samples lived in the central part of Taiwan (68.8%). The samples engaged in the service industry (45.2%) were the largest in terms of occupation (Table 2).
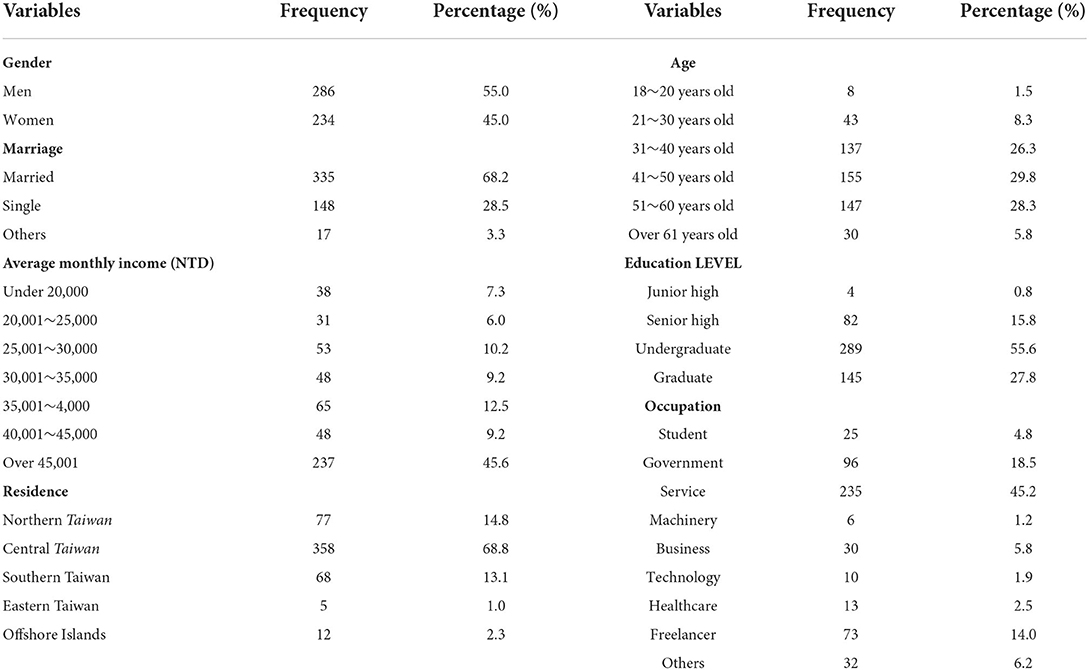
Table 2. Respondents' demographics (n = 520).
Confirmatory factor analysis
Confirmatory factor analysis was used to test the reliability and validity of tourism risk perception, pandemic prevention attitude, travel decision making, and travel intention scale. In order to avoid affecting the estimation and test results of the structural equation model, the sample data should be verified before the analysis. The absolute kurtosis values of the observed variables should be <10, and the absolute skew values should be <3. If the observed variables meet the above conditions, the maximum likelihood method can be used for model estimation (52). As can be seen from Table 3, tourism risk perception (skew: −0.173 to −0.803; kurtosis: −0.120 to −1.084), pandemic prevention attitude (skew: −0.601 to −0.918; kurtosis:-0.337 to 0.743), travel decision making (skew: −0.019 to −0.520; kurtosis: 0.002 to 0.964), and travel intention (skew: −0.433 to −0.650; kurtosis: −0.102 to 0.178), the absolute skew values of all observed variables are <3, and the absolute kurtosis values are <10. Thus, the structural equation in this study is suitable for analysis by the maximum likelihood method.
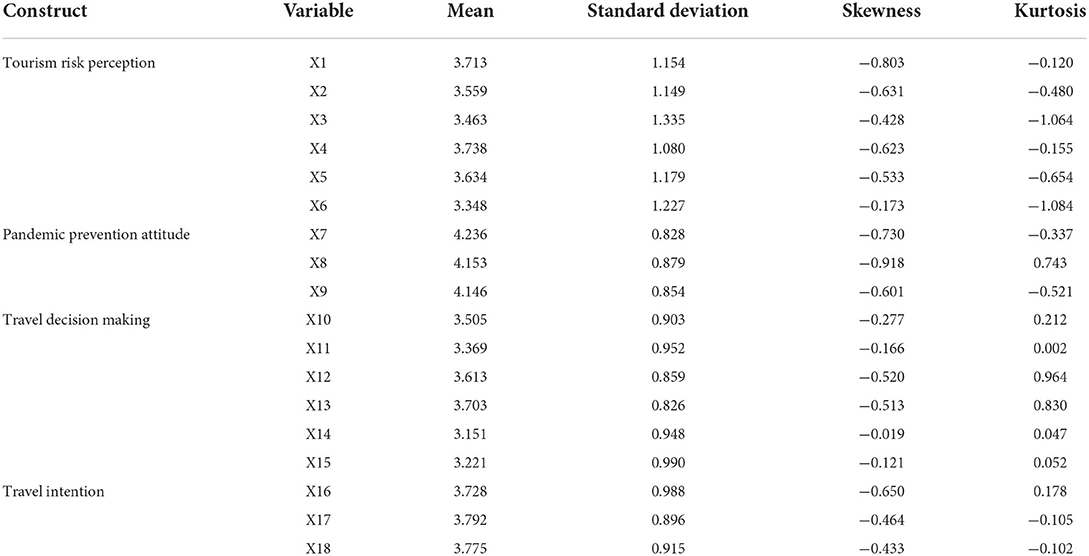
Table 3. Analysis of mean, standard deviation, skew, and kurtosis of variables.
Before analyzing the model fit, to avoid improper explanation, it is necessary to examine whether the measurement model has offending estimates or the parameter estimate exceeds the acceptable range. General offending estimates occur with negative standard errors, standardization coefficients exceeding or too close to 1 (usually 0.95 as the critical point), and substantial standard errors (52). As can be seen from the analysis results of model parameter estimation (Table 4), the standard error of the observed variables in this study ranges from 0.04 to 0.10, meaning without substantial standard error and negative value. In contrast, the standardization coefficient ranges from 0.65 to 0.95 without any standardization coefficient exceeding or approaching 1. Therefore, the measurement model in this study has no offending estimate and is suitable for the fit analysis of the measurement model.

Table 4. Model parameter estimation table of variables.
In this study, absolute and relative fit measures were used to measure the model fit of the measurement and structural models. The absolute fit measures include GFI, AGFI, and RMSEA (52), while the relative fit measures include NFI, TLI (NNFI), CFI, IFI, and RFI. The results of measurement model fit show that the absolute fit measures, meaning GFI (0.94) and AGFI (0.91), are both >0.90, and RMSEA was 0.06, while the relative fit measures, NFI (0.94), TLI (NNFI) (0.94), CFI (0.96), IFI (0.96), and RFI (0.91) are all >0.90, indicating that the measurement model in this study has a reasonable degree of fit (Table 5).
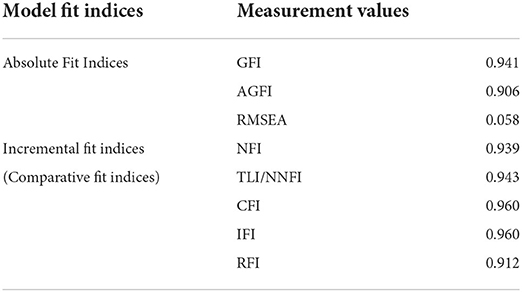
Table 5. CFA model.
In terms of the reliability and validity of the scale (Figure 2, Tables 6, 7), Cronbach's α, the reliability of individual observed variables, construction reliability, mean extraction variation, aggregation validity, and discriminant validity were used as the basis for measurement (52). The Cronbach's coefficients of all potential variables exceeded 0.70, indicating the good internal consistency of potential variables. The R2 coefficients (variation ratio) of the reliability of individual observed variables were all >0.20, indicating the good internal consistency of individual observed variables. The construction reliability coefficients were all >0.60, indicating a high correlation between the observed variables. The mean extraction variation was above 0.50, indicating that more than half of the explanatory variables of the dimensions were from the observed variables themselves. The factor loads of the observed variables were all higher than 0.50, indicating that the observed variables could effectively reflect the potential variables. The AVE square root coefficients of the discriminant validity of all potential variables were higher than the correlation coefficients between two variables, indicating that each potential variable could be effectively distinguished (52). According to the above findings, the measurement model in this study has good reliability and validity.
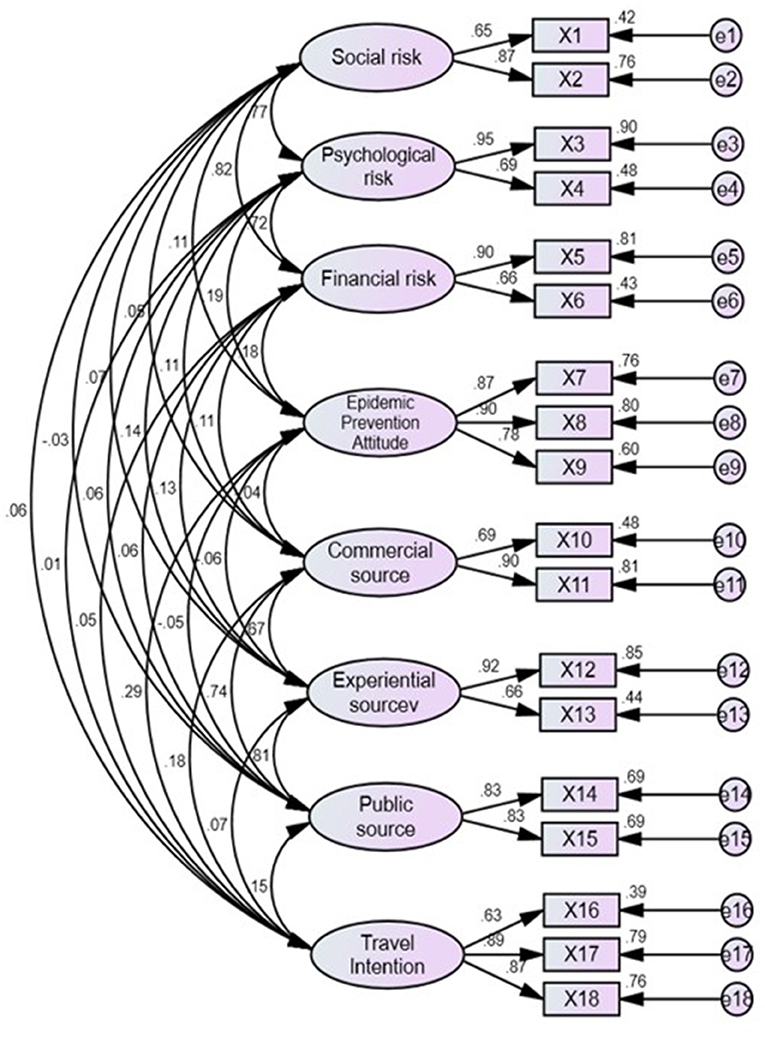
Figure 2. CFA model (Model fit indices: GFI = 0.941, AGFI = 0.906, RMSEA = 0.058, TLI/NNFI = 0.943, CFI = 0.960, IFI = 0.960, RFI = 0.912).
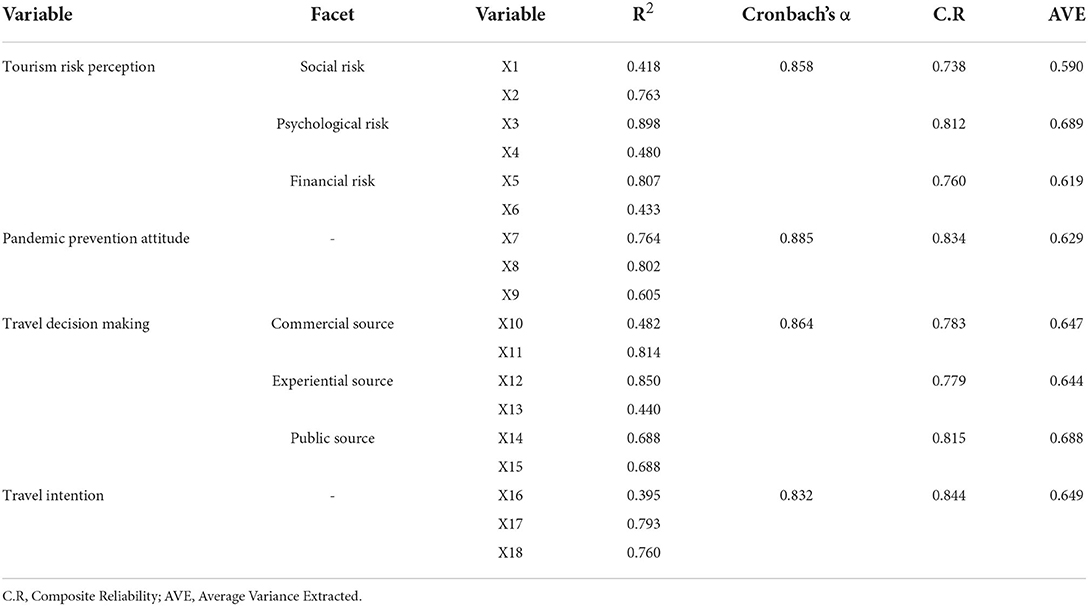
Table 6. Summary of the convergent validity and construct reliability.
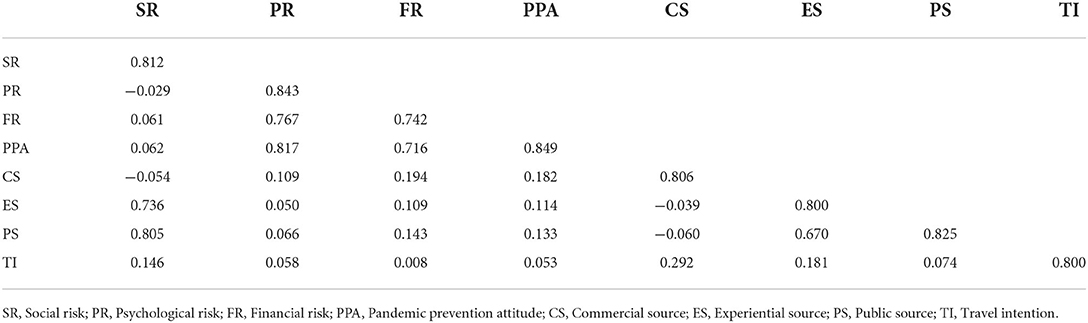
Table 7. Discriminant validity.
Structural model analysis
According to the measurement model, reliability and validity in this study reached the standard value. Thus, the structural model analyzed the relationship between tourism risk perception, pandemic prevention attitude, travel decision making, and travel intention. The fit detection results of the structural model show that both the absolute fit measures, GFI (0.933), AGFI (0.907), and RMSEA (0.056), and the relative fit measures, NFI (0.931), TLI (NNFI) (0.945), CFI (0.956), IFI (0.956), and RFI (0.915), meet the standard for model fit, which means that the model obtained in this study has a reasonable degree of fit (Table 8).
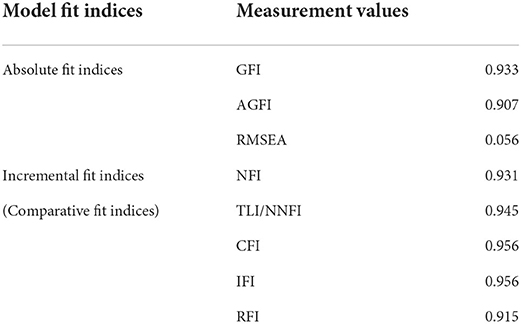
Table 8. Structural model.
The results of structural model analysis (Figure 3) show that tourism risk perception only has a significant impact on the pandemic prevention attitude (β = 0.18*, *p < 0.05); the higher the risk perception of tourists traveling abroad for vaccination, the higher their pandemic prevention attitude. On the contrary, tourism risk perception has no significant impact on travel decision making (β = −0.02, p > 0.05) or travel intention (β = 0.09, p > 0.05), and the risk perception of tourists traveling abroad for vaccination has no impact on their travel decision-making or travel intention.
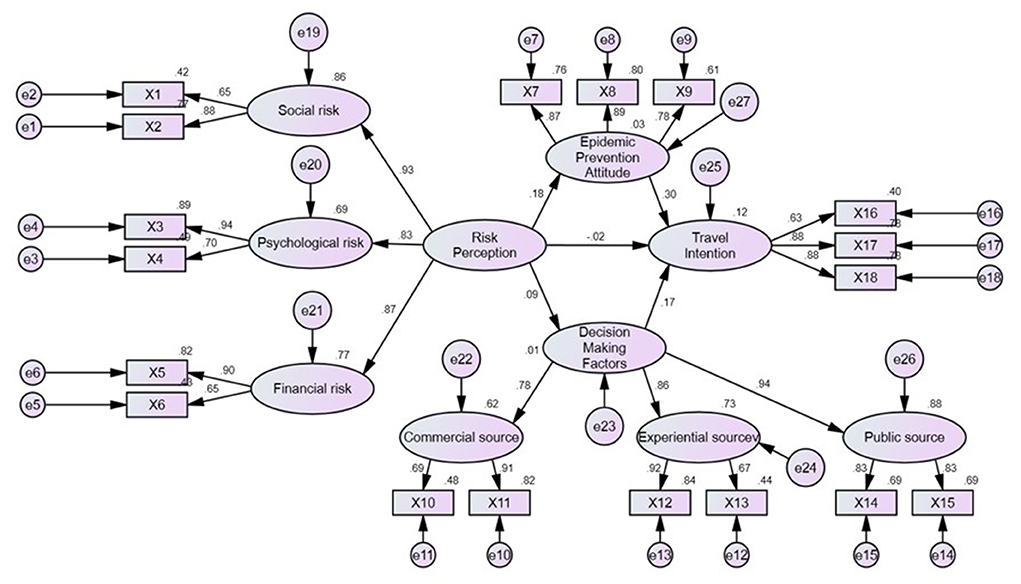
Figure 3. Structural model of the relationship between risk perception, pandemic prevention attitude, travel decision making, and travel intention (Model fit indices: GFI = 0.933, AGFI = 0.907, RMSEA = 0.056, TLI/NNFI = 0.931, CFI = 0.945, IFI = 0.956, RFI = 0.915).
Furthermore, there is a significant positive relationship between the pandemic prevention attitude (β = 0.30*, *p < 0.05) and travel decision making (β = 0.17*, *p < 0.05) of tourists and their intention to travel abroad for vaccination; the more positive the pandemic prevention attitude and travel decision making of tourists, the higher their intention to travel abroad for vaccination. Moreover, tourists' risk perception has a significant indirect impact on their travel intention through the pandemic prevention attitude, and the pandemic prevention attitude plays a complete intervening role between the two. In other words, only when the risk perception of tourists traveling abroad for vaccination effectively strengthens their pandemic prevention attitude will there be a significant impact on their vaccine travel intention.
Discussion
This study used the SOR model as the framework to explore the relationship between the risk perception, pandemic prevention attitude, travel decision-making, and travel intention of vaccine tourists. The risk perception of tourists has a significant positive impact on their pandemic prevention attitude. Their pandemic prevention attitude significantly impacts their travel intention, and pandemic prevention attitude is a complete intervening variable between risk perception and travel intention. Therefore, the relationship between the risk perception, pandemic prevention attitude and travel intention of vaccine tourists corresponds to the SOR model mechanism proposed by Mehrabian and Russell (28). Due to the shortage of vaccines in Taiwan, vaccine tourists are stimulated by their risk perception, which positively affects their pandemic prevention attitude, and eventually leads to the intention to travel abroad for vaccination. Ram and Chand (53) argued that risk perception can improve people's attitudes toward safety. When the risk perception is higher, people's attitude toward safety will be more rigorous, and generate the behaviors for personal safety. Therefore, the tourists' higher risk perception of COVID-19 actually strengthens intention to vaccinate abroad to ensure their life security.
In addition, the findings of this study are consistent with the findings of Bae and Chang (36), meaning that vaccine tourists regard traveling abroad for vaccination as a health promotion behavior, which results in a reduction of the risk perception of tourists and has a positive impact on their travel attitude. The relationship between pandemic prevention attitude and travel intention is the same as the findings of Tseng et al. (4), meaning that the better the pandemic prevention attitude of vaccine tourists, the higher their intention to travel abroad for vaccination.
Tourists' attention to their life safety and their desire to travel exceed travel risk perception and decision making. This study found no significant relationship between the risk perception and travel intention of vaccine tourists, which is inconsistent with most previous research results (7, 37–39). There are two possible reasons to explain why vaccine tourists in Taiwan do not reduce their intention to travel abroad for vaccination or their decision to travel abroad, despite the risks of traveling abroad during COVID-19. First, there is a severe shortage of vaccines in Taiwan, and most people have not been vaccinated. However, to maintain their daily life, they have to take the risk of being infected without antibodies to go out to work and buy goods. Thus, they feel their lives are threatened and choose to go abroad for vaccination. Second, the impact of the long-term ban on travel caused by COVID-19 results in tourists' perceptions of the severity of the pandemic having no significant impact on their travel intention (54). Thus, people's desire to travel abroad continues to accumulate, and vaccine tourism maybe meets people's desire to travel abroad. Thus, in the short term, especially in countries with a shortage of vaccines, vaccine tourism can be regarded as a way to alleviate the shortage of vaccines and meet the desire to travel.
There is a significant relationship between vaccine tourists' travel decision-making and travel intention, corresponding to previous tourism-related research results (42–44). Vaccine tourists' confidence in the effectiveness of the government's pandemic prevention policies and the medical system of the destination are the main factors influencing tourists' intention to travel abroad for vaccination. Thus, the perceived value is transformed into the actual intention of tourism after receiving information about the destinations and conducting internal evaluation (42). The implementation of pandemic prevention policies and the supply of medical quality in the tourist destinations of vaccine tourism are the key factors that determine tourists' travel intention. Therefore, before implementing vaccine tourism, the pandemic prevention policies between the two countries must be consensus-based and thoroughly implemented. In addition, the local medical system must be sound enough to provide sufficient vaccinations and medical care for international tourists and meet the pandemic control measures in Taiwan.
Limitations of the study
While this study was carried out with a rigorous design, there are still several limitations to be further studied:
1. The research scope of this study is limited to Taiwan, and other cases with the same shortage of vaccines are not included in the scope of this study; therefore, future studies can verify whether there are similar findings in cases with similar situations.
2. The relationship between risk perception and travel intention in cases with abundant vaccines is worth exploring and comparing.
3. This study conducted quantitative research. Thus, qualitative research can be added to the research design in the future to enhance the understanding of vaccine tourists' travel intentions.
Conclusion
The risk perception of vaccine tourists has a significant impact on the pandemic prevention attitude, and the pandemic prevention attitude is a complete intervening variable between risk perception and travel intention. Due to the shortage of vaccines and a long-standing travel ban in Taiwan, tourists' risk perceptions do not have a significant impact on their travel intention or decision making. However, vaccine travel decision-making has a significant impact on tourists' travel intentions, which mainly depend on the local tourism destinations' pandemic prevention policy and medical quality. In the short term, as a product of COVID-19, vaccine tourism can alleviate the tourism economic dilemma for countries with sufficient medical supplies and ease the desire of tourists to travel. Therefore, the pandemic prevention planning and medical quality of the tourism destinations and the supportive measures in inbound and outbound destination must be carefully reviewed. The government can use direct and indirect management policy forcing vaccine tourists to obey the national pandemic prevention.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
X-BW contributions in the study included methodology, conceptualization, and original draft. C-CC contributions in the study were investigation, methodology, and original draft. GK contributions in the study were formal analysis, methodology, and review and editing. C-HC contributions in the study were investigation, project administration, and resources. CH contributions in the study were supervision and review and editing. P-YL contributions in the study were data curation and project administration. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Heung VC, Kucukusta D, Song H. A conceptual model of medical tourism: implications for future research. J Travel Tour Mark. (2010) 27:236–51. doi: 10.1080/10548401003744677
3. Tourism Bureau Outbound Departures of Nationals of the Republic of China. Statistics of Outbound Tourists. (2021). Available online at: https://admin.taiwan.net.tw/ (accessed July 21, 2021).
4. Tseng K-C, Lin H-H, Lin J-W, Chen I, Hsu C-H. Under the COVID-19 environment, will tourism decision making, environmental risks, and epidemic prevention attitudes affect the people's firm belief in participating in leisure tourism activities? Int J Env Res Public Health. (2021) 18:7539. doi: 10.3390/ijerph18147539
5. Rather RA. Monitoring the impacts of tourism-based social media, risk perception and fear on tourist's attitude and revisiting behaviour in the wake of COVID-19 pandemic. Curr Issues Tour. (2021) 1–9. doi: 10.1080/13683500.2021.1884666
6. Artuger S. The effect of risk perceptions on tourists' revisit intentions. Eur J Bus Manag. (2015) 7:36–43.
7. Garg A. Travel risks vs tourist decision making: a tourist perspective. Int J Hosp Tour Syst. (2015) 8:1–9. doi: 10.21863/ijhts/2015.8.1.004
8. Zhu H, Deng F. How to influence rural tourism intention by risk knowledge during COVID-19 containment in China: mediating role of risk perception and attitude. Int J Env Res Public Health. (2020) 17:3514. doi: 10.3390/ijerph17103514
9. Cotfas L-A, Delcea C, Milne RJ, Salari M. Evaluating classical airplane boarding methods considering COVID-19 flying restrictions. Symmetry. (2020) 12:1087. doi: 10.3390/sym12071087
10. Dai Y, Jia L. A Study on Tourists' Travel Intention Under the Situation of Novel Coronavirus Pneumonia Epidemic. 6th Annual International Conference on Social Science and Contemporary Humanity Development (SSCHD 2020). Atlantis Press. (2021) p. 942–947. doi: 10.2991/assehr.k.210121.183
11. Seyidov J, Adomaitiene R. Factors influencing local tourists' decision-making on choosing a destination: a case of Azerbaijan. Ekon. (2016) 95:112–27. doi: 10.15388/Ekon.2016.3.10332
12. Decrop A. Tourists' Decision-Making and Behavior Processes. Consumer Behavior in Travel and Tourism. (1999) p. 103–133.
14. Al-Tarawneh HA. The main factors beyond decision making. J Manag Res. (2012) 4:1–23. doi: 10.5296/jmr.v4i1.1184
15. Smallman C, Moore K. Process studies of tourists' decision-making. Ann Tour Res. (2010) 37:397–422. doi: 10.1016/j.annals.2009.10.014
16. Zhang W. The Motivations, Constraints and Decision-Making of Beijing Outbound Tourists. The University of Waikato. (2009).
17. Bae SY, Chang P-J. The effect of coronavirus disease-19 (COVID-19) risk perception on behavioural intention towards ‘untact'tourism in South Korea during the first wave of the pandemic (March 2020). Curr Issues Tour. (2021) 24:1017–35. doi: 10.1080/13683500.2020.1798895
18. Wang AI. Systematic literature review on health effects of playing Pokémon Go. Entertain Comput. (2021) 38:100411. doi: 10.1016/j.entcom.2021.100411
19. Isa SM, Ramli L. Factors influencing tourist visitation in marine tourism: lessons learned from FRI Aquarium Penang, Malaysia. Int J Cult Tour Hosp Res. (2014) 8:103–17. doi: 10.1108/IJCTHR-04-2013-0016
20. Smith PC, Forgione DA. Global outsourcing of healthcare: a medical tourism decision model. Case Appl Res. (2007) 9:19–30. doi: 10.1080/15228053.2007.10856117
21. Henson JN, Guy BS, Dotson MJ. Should I stay or should I go? Motivators, decision factors, and information sources influencing those predisposed to medical tourism. Int J Healthc Manag. (2015) 8:4–14. doi: 10.1179/2047971914Y.0000000083
22. Nilashi M, Samad S, Manaf AA, Ahmadi H, Rashid TA, Munshi A, et al. Factors influencing medical tourism adoption in Malaysia: A DEMATEL-Fuzzy TOPSIS approach. Comput Ind Eng. (2019) 137:106005. doi: 10.1016/j.cie.2019.106005
23. Luo JM, Lam CF. Travel anxiety, risk attitude and travel intentions towards “travel bubble” destinations in Hong Kong: Effect of the fear of COVID-19. Int J Env Res Public Health. (2020) 17:7859. doi: 10.3390/ijerph17217859
24. Kim MJ, Lee C-K, Jung T. Exploring consumer behavior in virtual reality tourism using an extended stimulus-organism-response model. J Travel Res. (2020) 59:69–89. doi: 10.1177/0047287518818915
25. Jani D, Han H. Influence of environmental stimuli on hotel customer emotional loyalty response: Testing the moderating effect of the big five personality factors. J Hosp Manag. (2015) 44:48–57. doi: 10.1016/j.ijhm.2014.10.006
26. Chen G, So KKF, Hu X, Poomchaisuwan M. Travel for affection: a stimulus-organism-response model of honeymoon tourism experiences. J Hosp Tour Res. (2021) 1–33. doi: 10.1177/10963480211011720
27. Jiang J. The role of natural soundscape in nature-based tourism experience: an extension of the stimulus–organism–response model. Curr Issues Tour. (2020) 1–20. doi: 10.1080/13683500.2020.1859995
28. Jeong Y, Kim E, Kim S-K. Understanding active sport tourist behaviors in small-scale sports events: stimulus-organism-response approach. Sustainability. (2020) 12:8192. doi: 10.3390/su12198192
30. Peng C, Kim YG. Application of the stimuli-organism-response (SOR) framework to online shopping behavior. J Internet Commer. (2014) 13:159–76. doi: 10.1080/15332861.2014.944437
31. Chen C-C, Yao J-Y. What drives impulse buying behaviors in a mobile auction? The perspective of the stimulus-organism-response model. Telemat Inform. (2018) 35:1249–62. doi: 10.1016/j.tele.2018.02.007
32. Ryu K, Jang SS. The effect of environmental perceptions on behavioral intentions through emotions: The case of upscale restaurants. J Hosp Tour Res. (2007) 31:56–72. doi: 10.1177/1096348006295506
33. Liu J, Gao J. Based tourism risk perception conceptual model—a case study of Shanghai residents. Tour Sci. (2008) 22:37–43.
34. Cui F, Liu Y, Chang Y, Duan J, Li J. An overview of tourism risk perception. Nat Hazards. (2016) 82:643–58. doi: 10.1007/s11069-016-2208-1
35. Menvielle L, Menvielle W, Tournois N. Medical tourism: A decision model in a service context. Tour Int Interdiscip J. (2011) 59:47–61.
37. Polas RH, Imtiaz M, Mahbub A, Khan AM. Antecedent and consequences of risk perception on tourist decision making towards the sustainable medical tourism development in Bangladesh. J Tour Manag Res. (2019) 6:93–108. doi: 10.18488/journal.31.2019.61.93.108
38. Chew EYT, Jahari SA. Destination image as a mediator between perceived risks and revisit intention: a case of post-disaster Japan. Tour Manag. (2014) 40:382–93. doi: 10.1016/j.tourman.2013.07.008
39. Qi CX, Gibson HJ, Zhang JJ. Perceptions of risk and travel intentions: the case of China and the Beijing Olympic Games. J Sport Manag Tour. (2009) 14:43–67. doi: 10.1080/14775080902847439
40. Luan R-S, Wang X, Sun X, Chen X-S, Zhou T, Liu Q-H, et al. Epidemiology, treatment, and epidemic prevention and control of the coronavirus disease 2019: a review. Med Sci Edi. (2020) 51:131–8. doi: 10.12182/20200360505
41. Shen J, Duan H, Zhang B, Wang J, Ji JS, Wang J, et al. Prevention and control of COVID-19 in public transportation: experience from China. Environ Pollut. (2020) 115291. doi: 10.1016/j.envpol.2020.115291
42. Zhang Y, Li J, Liu C-H, Shen Y, Li G. The effect of novelty on travel intention: the mediating effect of brand equity and travel motivation. Manag Decis. (2020) 59:1271–90. doi: 10.1108/MD-09-2018-1055
43. Karl M, Bauer A, Ritchie WB, Passauer M. The impact of travel constraints on travel decision-making: a comparative approach of travel frequencies and intended travel participation. J Dest Mark Manage. (2020) 18:100471. doi: 10.1016/j.jdmm.2020.100471
44. Girish V, Lee C-K, Kim MJ, Kim YS. Impacts of perception and perceived constraint on the travel decision-making process during the Hong Kong protests. Curr Issues Tour. (2021) 24:2093–6. doi: 10.1080/13683500.2020.1819971
45. Makhdoomi UM, Baba MM. Destination image and travel intention of travellers to Jammu & Kashmir: the mediating effect of risk perception. J Hosp Appli Res. (2019) 14:35.
46. Chen Y-C, Shang R-A, Li M-J. The effects of perceived relevance of travel blogs' content on the behavioral intention to visit a tourist destination. Comput Human Behav. (2014) 30:787–99. doi: 10.1016/j.chb.2013.05.019
47. Abubakar AM, Ilkan M. Impact of online WOM on destination trust and intention to travel: a medical tourism perspective. J Dest Mark Manage. (2016) 5:192–201. doi: 10.1016/j.jdmm.2015.12.005
48. Farrukh M, Shahzad IA, Sajid M, Sheikh MF. Revisiting the intention to travel framework in the perspective of medical tourism: The role of eWord-of-mouth and destination image. Int J Healthc Manag. (2020) 1–8. doi: 10.1080/20479700.2020.1836733
49. Khan MJ, Chelliah S, Haron MS, Ahmed S. Role of travel motivations, perceived risks and travel constraints on destination image and visit intention in medical tourism: theoretical model. Sultan Qaboos Univ Med J. 17:e11. doi: 10.18295/squmj.2016.17.01.003
50. Cham T-H, Lim Y-M, Sia B-C, Cheah J-H, Ting H. Medical tourism destination image and its relationship with the intention to revisit: a study of Chinese medical tourists in Malaysia. J China Tour Res. (2021) 17:163–91. doi: 10.1080/19388160.2020.1734514
51. Handcock MS, Gile KJ. Comment: On the concept of snowball sampling. Sociol Methodol. (2011) 41:367–71. doi: 10.1111/j.1467-9531.2011.01243.x
53. Ram T, Chand K. Effect of drivers' risk perception and perception of driving tasks on road safety attitude. Transp Res Part F Traffic Psychol Behav. (2016) 42:162–76. doi: 10.1016/j.trf.2016.07.012
Keywords: medical tourism, vaccine tourism, risk perception, pandemic prevention attitude, travel decision making, travel intention, COVID-19
Citation: Wang X-B, Chen C-C, Ku GCM, Chen C-H, Hsu CH and Lee P-Y (2022) Travel for survive! Identifying the antecedents of vaccine tourists' travel intention: Using a stimulus-organism-response model. Front. Public Health 10:850154. doi: 10.3389/fpubh.2022.850154
Received: 07 January 2022; Accepted: 05 July 2022;
Published: 29 July 2022.
Edited by:
Stefan Swartling Peterson, Karolinska Institutet (KI), SwedenReviewed by:
An-Shin Shia, Lingnan Normal University, ChinaWang Chien-Hua, Lingnan Normal University, China
Copyright © 2022 Wang, Chen, Ku, Chen, Hsu and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chin Hsien Hsu, aHN1NjI5MjAwMEB5YWhvby5jb20udHc=