
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 15 June 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.845015
This article is part of the Research TopicCOVID-19 Pandemic: Mental Health, Life Habit Changes and Social PhenomenaView all 70 articles
 Esmaeil Hoseinzadeh1
Esmaeil Hoseinzadeh1 Abbas Ebadi2,3
Abbas Ebadi2,3 Hamid Sharif Nia4,5
Hamid Sharif Nia4,5 Erika Sivarajan Froelicher6,7
Erika Sivarajan Froelicher6,7 Pardis Rahmatpour8*
Pardis Rahmatpour8*The crisis of the COVID-19 prevalence in Iran, as well as the world, caused mental disorders and anxiety syndrome. The COVID-19 anxiety syndrome scale (C-19ASS) assesses conceptually and psychometrically the nature of the COVID-19 threat experience instead of a response to the threat, fear, and COVID-19 anxiety. Therefore, the aim of this study is to evaluate the psychometric properties of the Persian version of the anxiety syndrome scale of COVID-19 in the population of Iran. The Persian version of C-19ASS was sent to Iranian adults via online social networking applications and finally, 932 adults responded to the questionnaire. The results of exploratory factor analysis revealed two-factor structures for C-19ASS, which explained 48.70% of the total variance. Given the confirmatory factor analysis findings, all goodness of fit indices confirmed the model fit. All coefficients of internal consistency were estimated as acceptable reliability. The results showed that the C-19ASS has good psychometric properties, and can be used by researchers, psychologists, and healthcare providers to assess the anxiety syndrome of the Iranian population during the COVID-19 pandemic.
In Iran, from 3 January 2020 to 15 March 2022, there have been 7,126,906 confirmed cases of COVID-19 with 139,063 deaths, according to WHO (1). It is well known that stressful life events can cause psychological symptoms (2). The public physical health, anxieties, and human safety are affected by this infectious disease that has caused numerous psychological health problems and psychological symptoms (3, 4). The COVID-19 outbreak is exacerbating the anxiety that many people feel. Anxiety is defined as distress or fear caused by the prediction of an event or a real or understandable threatening situation (3, 5). Anxiety syndrome may appear in a combination of avoidance, worrying, and monitoring of threat, such a set of incompatible contrasting forms may have an essential role in the stability of psychological depression (6).
The COVID-19 pandemic has exerted high pressures on health systems of countries where the virus is most prevalent (7). It has destructive and variable effects on all aspects of human life (8). It led to lockdowns that lasted over multiple months affecting educational and non-essential business activities in many countries. These lockdowns were implemented for the rapid reduction of COVID-19 transmission (9). All affected countries have a complete or partial cessation of social activities and a wide range of interventions. Examples include social isolation, individual isolation, social distancing, and quarantine to prevent the gathering of large numbers of people, beyond the immediate members of the household.
Many people who have been quarantined may feel lonely, bored, inactive, and insecure about food and economic issues as well as feel fear and anxiety about the infection caused by the disease (10). National polls show a severe increase of fear and anxiety about the virus (11). For example, a study of 44,000 participants in Belgium, conducted at the beginning of April 2020, reported that 20% of people had anxiety and 16% of them had a depressive disorder (11). Based on the model provided in Iranian study anxiety syndrome and fear of COVID-19 with mediation effects of perceived stress explained 70% of the total variance of psychological behavioral responses (4). According to the clinical manifestations of this disease such as respiratory failure, sepsis, shock, and various organ failures, it is understandable that medical professionals and public health specialists focus on caring for the sick people. While it is recognized that corona virus spreads to the general population, there is less attention given to the mental health consequences of the COVID-19 crisis (12). About 54%of the Chinese general population (n = 1,210) reported moderate or severe psychological effects of the disease outbreak, 16.5% reported moderate or severe depressive symptoms, and 28.8% reported moderate or severe anxiety symptoms (13). In the systematic review study of Salari et al. (14) the prevalence of stress, anxiety, and depression among the general population during the COVID-19 pandemic were 29.6% (sample size of 9,074), 31.9% (sample size of 63,439), and 33.7% (sample size of 44,531), respectively. Previous research has shown that people who suffer from pandemic anxiety tend to also show an increase in stress, anxiety, and suicide (15).
There are different scales such as the scale of the fear of COVID-19 (16), Coronavirus anxiety scale (17), scale of threat of Coronavirus (18), and COVID stress scale (19). These scales are intended to identify people who have been affected by anxiety, fear, and uncertainty over this growing epidemic crisis. However, the COVID-19 anxiety syndrome scale (C-19ASS) assesses conceptually and psychometrically the nature of the COVID-19 threat experience instead of a response to threat, fear, and COVID-19 anxiety. This scale has been developed and psychometrically tested by Nikcevic and Spada in the U.K. This scale identifies features of anxiety syndrome related to COVID-19 and assessed its validity and reliability (6).
Considering the prevalence of COVID-19 anxiety syndrome in Iran, and the lack of an accurate scale to measure it among the Iranian population, the aim of this study is to evaluate the psychometric properties of the Persian version of the anxiety syndrome scale of COVID-19 in the population of Iran.
This methodological study design was used to achieve the research objective. Data collection took place between October and November 2021.
The measurements consist of two parts: demographic information, and the Persian version of C-19ASS. The original version of C-19ASS consists of nine items and two factors including perseveration (six items) and avoidance (three items). The C-19ASS is a short easily administered scale that can be used with both healthy and frail individuals exposed to any specific traumatic event. The response options for the C-19ASS are scored on a 5-point Likert-type scale from 0 (not at all) to 4 (Nearly every day) (6).
At first, the written permission was obtained from the authors of the scale, Professor Marcantonio M. Spada via email. Then, two English-Persian translators translated the C-19ASS independently. The research team, as well as two professional translators, evaluated the two translations and created a Persian translation of C-19ASS. In the next step, two Persian to English translators who had no knowledge of the English version of the C-19ASS were asked to back-translate the Persian version of the C-19ASS scale into English. Then the panel of experts compiled and compared the results of the back-translation with the original instrument to detect any differences and similarities between the original instrument and the back-translated version.
All items translate into Persian and back-translated into English without any required modifications and Dr. Marcantonio M. Spada (The main developer scale) confirmed The Backward Scale. It is noteworthy that all the steps of this process were performed based on the World Health Organization protocol of forward-backward translation technique (20).
The Persian version of C-19ASS was sent to Iranian adults via an online data gathering and 932 adults responded to the questionnaire. The online scale was created via Google Forms and its URL link was sent by email or social networking applications such as a Telegram channel or WhatsApp to a group of adults. To prevent duplicate data, the Google Form was restricted to get the data from each individual once. The inclusion criteria for participants were adults (age > 18) who were willing to participate in this study. The sample size should be at least 200 cases for factor analysis (21). Of these, 466 subjects were used for the exploratory factor analysis (EFA) and a second group with 466 subjects serves as the confirmatory factor analysis (CFA).
The construct validity of the Persian version of C-19ASS was evaluated by exploratory and confirmatory factor analysis. Maximum likelihood EFA with Promax rotation was conducted. The Kaiser–Meyer–Olkin test (KMO > 0.7: acceptable) and Bartlett's test of sphericity were calculated. The number of factors was determined based on parallel analysis, scree plot. Items with absolute loading values of 0.3 or greater and communalities more than 0.2 were considered appropriate (21). For assessment of the extracted factors, CFA was conducted using the maximum-likelihood method and the most common goodness of fit indices.
According to Fornell and Larcker's criteria (22), the Average Variance Extracted (AVE), Maximum Shared Squared Variance (MSV), and Composite Reliability (CR) were estimated to assess the convergent and discriminant validity. In addition, discriminant validity was evaluated by heterotrait-monotrait ratio of correlations (HTMT) approach. All values in the HTMT matrix table should be <0.85 (23). The reliability of the scale was evaluated using internal consistency and construct reliability (CR). The average inter-item correlation (AIC) was in the range of 0.2 to 0.4, Cronbach's alpha and McDonald's omega was >0.7 and are considered acceptable internal consistency (24). The CR was calculated using the structural equation model analysis as an alternative to Cronbach's alpha coefficient – it was acceptable if it was >0.7 (25). The relationship between demographic information and level of C-19ASS were evaluated by independent t-test, one-way ANOVA, and Pearson correlation coefficient.
Both univariate and multivariate normality of the data was evaluated in this study. The univariate distributions were tested for outliers, skewness, and kurtosis. The normality of the multivariate distribution was assessed using Mardia's coefficient of multivariate kurtosis, and the Mardia's coefficient. Mardia's coefficient > 7.98 can be considered as indicative of departure from multivariate normality. Moreover, the outliers of the multivariate distribution were detected using Mahalanobis distance (P < 0.001) (21).
The SPSS26, SPSS-R menu2, AMOS26, and JASP0.15.0.0 software were used to perform all of the statistical calculations.
The Tehran Islamic Azad University of Medical Sciences Research Ethics Committee approved the protocol of this study (IR.IAU.TMU.REC.1400.315). While sending the online scale through social networking programs, the objectives of the study were fully explained to the participants. Subjects were informed that participation was voluntary and that their decision would not affect their care. Participants were reassured about the confidentiality of the data.
The mean and standard deviation for the age of 932 adults was 31.14 (SD = 7.81) years. Other demographic characteristics of participants are shown in Table 1. Also, the level of C-19ASS was estimated 31.68 (SD = 8.23, CI 95%: 31.14–32.21).
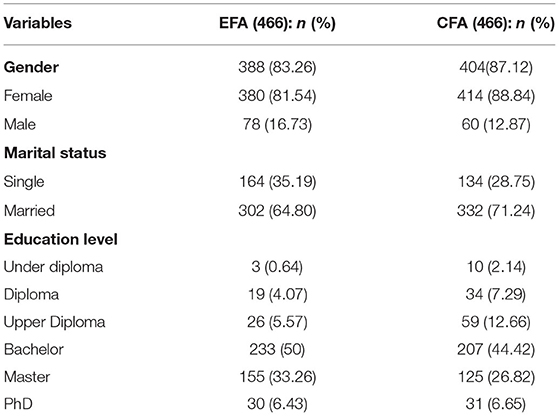
Table 1. Demographic characteristics of participants (n = 932).
In maximum likelihood EFA, the KMO test value was 0.852, and Bartlett's test value was 30,036.137 (P < 0.001). The EFA results revealed two factors with 48.70% explained variance for the C-19ASS (see Table 2, Figure 1).
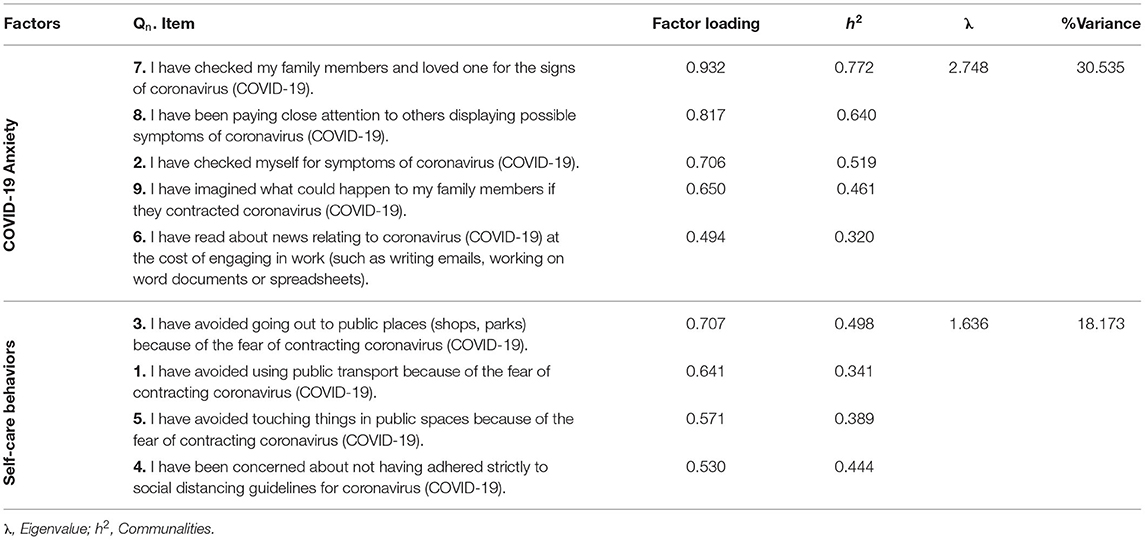
Table 2. Exploratory factors extracted of COVID-19 anxiety syndrome scale (C-19ASS; n = 466).
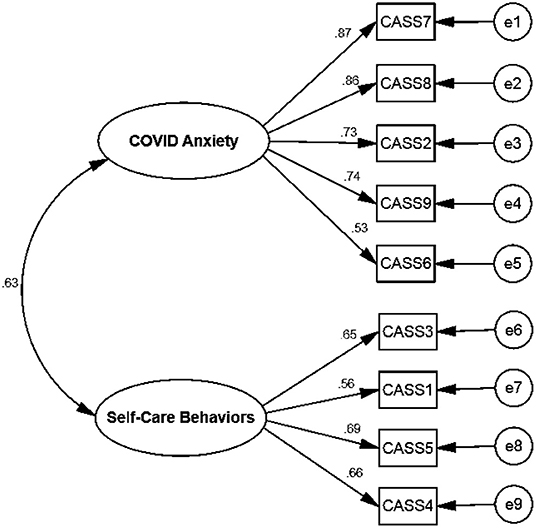
Figure 1. The CFA model of the C-19ASS.
The acceptable fit indices showed that the model was confirmed (see Table 3 and Figure 2). The convergent and discriminant validity for both factors were acceptable for the current study. The value in the HTMT matrix was <0.66, indicating discriminant validity was established in this study. All coefficients of internal consistency were estimated as acceptable reliability (see Table 4). There was no significant relationship between demographic variables and C-19ASS.

Table 3. Fit indices of the first order confirmatory factor analysis of the C-19ASS (n = 466).
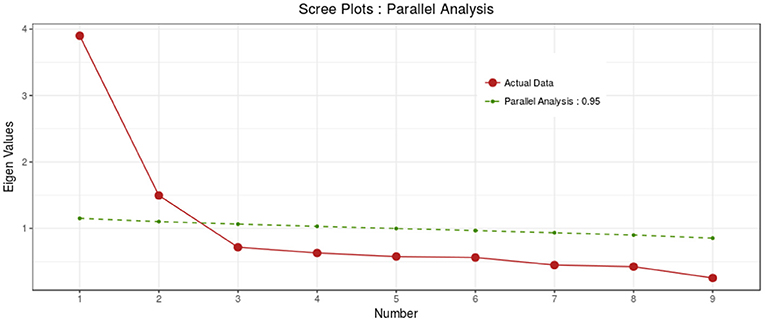
Figure 2. The scree plot of the C-19ASS.

Table 4. The indices of the convergent, discriminant validity, and internal consistency C-19ASS for the CFA (n = 466).
The results of this study demonstrated that the Persian version of C-19ASS has nine items in two subscales namely COVID-19 Anxiety and self-care behaviors, these two factors explained about the half of total variance of anxiety syndrome among the Iranian general population. Although one of the advantages of convenience sampling is that participants are readily available but at a disadvantage, a particular sample may be given more attention or, conversely, a group of the target population may not be included in the sample. Due to the fact that in this study, samples were collected through Google Form and social networks, people who were not members of social networks could not access the data collection form.
In the present study, the high level of Cronbach's alpha (>0.72), McDonald's omega (>0.72), and the average correlation between the items demonstrated that two factors of the scale had acceptable internal consistency. The results of internal consistency were almost similar to the original scale. The calculation of McDonald's omega is the advantage of this study because it does not depend on sample size and numbers of items. Also, based on the results of CR (>0.85) and Max-R, the Persian version of C-19ASS had good reliability. The CR is estimated by factor loading in CFA (26).
Based on the EFA results, two factors were identified, the first of which is COVID-19 anxiety which consists of five items. Anxiety is a mental disorder defined by excessive anxiety that leads to panic and is often accompanied by physical symptoms (27). People usually need more information about critical events to reduce anxiety caused by uncertainty in a critical event (27). For this reason, in examining COVID-19 anxiety syndrome in this study, people more than anything, are searching for the signs and symptoms of COVID-19 disease and news related to COVID-19.
The second factor is self-care behaviors. Behaviors that are performed with the aim of preventing disease and maintaining individual well-being is commonly defined as self-care behaviors. Self-care is a decision-making process with the aim of preventing COVID-19 and maintaining well-being in the COVID-19 pandemic (28).
The numbers of factors and items of the Persian version of C-19ASS were similar to the original. The only difference between the original version and the Persian version was an item “4) I have been concerned about not having adhered strictly to social distancing guidelines for COVID-19”. This item in the original version loaded into the first factor. But in the present study replaced in the second factor.
The findings of this study indicate that the Iranian version of the C-19ASS scale for evaluating COVID-19 anxiety syndrome is effective and useful in the general population to determine the prevalence of COVID-19. This scale helps the health-care providers, psychologists, and psychiatrists to identify and screen high-risk individuals and to offer preventive interventions to minimize the development of irreversible complications of anxiety syndrome.
The crisis of COVID-19 prevalence in the world, as well as Iran, caused mental disorders and COVID-19 anxiety syndrome, physical, psychological, and financial impacts on people and the government (29). The psychometric analysis of C-19ASS in the Iranian population in this situation showed that the concept of anxiety caused by COVID-19 was explained nearly 50% by the C-19ASS, which contained acceptable psychometric properties.
One of the limitations of this study was related to convenience sampling which is limited in its ability to reach all groups of the population (for example, the elderly population and individuals with no internet or without access to social media such as WhatsApp, Telegram, or email). Since the elderly are more affected by the COVID-19 pandemic due to their vulnerability and it was difficult to access them through social networks, it is recommended that this group be considered in evaluating the scale.
The Persian version of the C-19ASS scale had an acceptable construct validity and reliability. It has two factors with nine items that explained 48.70% of the total variance of the C-19ASS in the Iranian population during the COVID-19 pandemic. This scale could be beneficial for researchers, psychologists, and healthcare providers to assess anxiety syndrome during the COVID-19 pandemic.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
The Tehran Islamic Azad University of Medical Sciences Research Ethics Committee approved the protocol of this study (IR.IAU.TMU.REC.1400.315).
Informed consent was obtained from all individual participants included in the study.
AE, HS, ES, and EH contributed to the study conception and design. Material preparation and data collection were performed by EH and HS performed data analysis. The first draft of the manuscript was written by EH, PR, HS, and AE. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the Tehran Islamic Azad University of Medical Sciences and those participants who kindly helped us with this study.
1. WHO. The Current COVID-19 Situation 2022. Available online at: https://covid19.who.int/region/emro/country/ir (accessed March 15, 2022).
2. Aghakhani N, Sharif Nia H, Eghtedar S, Rahbar N, Jasemi M, Zadeh MM. Prevalence of depression among students of Urmia university of medical sciences (Iran). Iran J Psychiatry Behav Sci. (2011) 5:131.
3. Sharif Nia H, Akhlaghi E, Torkian S, Khosravi V, Etesami R, Froelicher ES, et al. Predictors of persistence of anxiety, hyperarousal stress, and resilience during the COVID-19 epidemic: a national study in Iran. Front Psychol. (2021) 12:671124. doi: 10.3389/fpsyg.2021.671124
4. Sharif Nia H, She L, Kaur H, Boyle C, Khoshnavay Fomani F, Hoseinzadeh E, et al. A predictive study between anxiety and fear of COVID-19 with psychological behavior response: the mediation role of perceived stress. Front Psychiatry. (2022) 13:851212. doi: 10.3389/fpsyt.2022.851212
5. Labrague LJ. De los Santos JAA. COVID-19 anxiety among front-line nurses: predictive role of organisational support, personal resilience and social support. J Nurs Manag. (2020) 28:1653–61. doi: 10.1111/jonm.13121
6. Nikčević AV, Spada MM. The COVID-19 anxiety syndrome scale: development and psychometric properties. Psychiatry Res. (2020) 292:113322. doi: 10.1016/j.psychres.2020.113322
7. Welt FG, Shah PB, Aronow HD, Bortnick AE, Henry TD, Sherwood MW, et al. Catheterization laboratory considerations during the coronavirus (COVID-19) pandemic: from the ACC's interventional council and SCAI. J Am Coll Cardiol. (2020) 75:2372–5. doi: 10.1016/j.jacc.2020.03.021
8. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. (2020) 78:185. doi: 10.1016/j.ijsu.2020.04.018
9. Soraci P, Ferrari A, Abbiati FA, Del Fante E, De Pace R, Urso A, et al. Validation and psychometric evaluation of the Italian version of the fear of COVID-19 scale. Int J Ment Health Addict. (2020) 1–10. doi: 10.1007/s11469-020-00277-1
10. Ahmed O, Faisal RA, Sharker T, Lee SA, Jobe MC. Adaptation of the Bangla version of the COVID-19 anxiety scale. Int J Ment Health Addict. (2020) 1–12. doi: 10.1007/s11469-020-00357-2
11. Mertens G, Gerritsen L, Duijndam S, Salemink E, Engelhard IM. Fear of the coronavirus (COVID-19): predictors in an online study conducted in March 2020. J Anxiety Disord. (2020) 74:102258. doi: 10.1016/j.janxdis.2020.102258
12. Sher L. The impact of the COVID-19 pandemic on suicide rates. QJM. (2020) 113:707–12. doi: 10.1093/qjmed/hcaa202
13. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. (2020) 17:1729. doi: 10.3390/ijerph17051729
14. Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. (2020) 16:1–11. doi: 10.1186/s12992-020-00589-w
15. Lee SA, Mathis AA, Jobe MC, Pappalardo EA. Clinically significant fear and anxiety of COVID-19: a psychometric examination of the coronavirus anxiety scale. Psychiatry Res. (2020) 290:113112. doi: 10.1016/j.psychres.2020.113112
16. Ahorsu DK, Lin C-Y, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. (2020). doi: 10.1007/s11469-020-00270-8
17. Lee SA. Coronavirus anxiety scale: a brief mental health screener for COVID-19 related anxiety. Death Stud. (2020) 44:393–401. doi: 10.1080/07481187.2020.1748481
18. Conway III. LG, Woodard SR, Zubrod A. Social psychological measurements of Covid-19: Coronavirus perceived threat, government response, impacts, and experiences questionnaires. (2020). doi: 10.31234/osf.io/z2x9a
19. Taylor S, Landry C, Paluszek M, Fergus TA, McKay D, Asmundson GJ. Development and initial validation of the COVID stress scales. J Anxiety Disord. (2020) 72:102232. doi: 10.1016/j.janxdis.2020.102232
20. Nilsson J, Gardulf A, Lepp M. Process of translation and adaptation of the nurse professional competence (NPC) scale. J Nurs Educ Pract. (2016) 6:100. doi: 10.5430/jnep.v6n1p100
21. Pahlevan Sharif S, Sharif Nia H. Factor Analysis and Structural Equation Modeling with SPSS-AMOS. Tehran: Jame-e-Negar (2021).
22. Fornell C, Larcker DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. (1981) 18:39–50. doi: 10.1177/002224378101800104
23. Henseler J, Ringle CM, Sarstedt M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J Acad Mark Sci. (2015) 43:115–35. doi: 10.1007/s11747-014-0403-8
24. Javali SB, Gudaganavar NV, Raj SM. Effect of Varying Sample Size in Estimation of Coefficients of Internal Consistency. (2011).
25. Sharif Nia H, Shafipour V, Allen K-A, Heidari MR, Yazdani-Charati J, Zareiyan A, et al. second-order confirmatory factor analysis of the moral distress scale-revised for nurses. Nurs Ethics. (2019) 26:1199–210. doi: 10.1177/0969733017742962
26. Vinzi VE, Chin WW, Henseler J, Wang H. Handbook of Partial Least Squares. Berlin/Heidelberg: Springer (2010).
27. Liu C, Liu Y. Media exposure and anxiety during COVID-19: the mediation effect of media vicarious traumatization. Int J Environ Res Public Health. (2020) 17:4720. doi: 10.3390/ijerph17134720
28. De Maria M, Ferro F, Ausili D, Alvaro R, De Marinis MG, Di Mauro S, et al. Development and psychometric testing of the self-care in COVID-19 (SCOVID) scale, an instrument for measuring self-care in the COVID-19 pandemic. Int J Environ Res Public Health. (2020) 17:7834. doi: 10.3390/ijerph17217834
Keywords: COVID-19, anxiety syndrome, Iran, validity, reliability
Citation: Hoseinzadeh E, Ebadi A, Sharif Nia H, Sivarajan Froelicher E and Rahmatpour P (2022) Validity and Reliability of the Persian Version of COVID-19 Anxiety Syndrome Scale Among the Iranian General Population. Front. Public Health 10:845015. doi: 10.3389/fpubh.2022.845015
Received: 29 December 2021; Accepted: 08 April 2022;
Published: 15 June 2022.
Edited by:
Xenia Gonda, Semmelweis University, HungaryReviewed by:
Hesham Fathy Gadelrab, Mansoura University, EgyptCopyright © 2022 Hoseinzadeh, Ebadi, Sharif Nia, Sivarajan Froelicher and Rahmatpour. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pardis Rahmatpour, cGFyLnJhaG1hdHBvdXJAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.