
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Public Health, 12 April 2022
Sec. Digital Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.839838
This article is part of the Research TopicExtracting Insights from Digital Public Health Data using Artificial IntelligenceView all 15 articles
 B. L. Radhakrishnan1*
B. L. Radhakrishnan1* E. Kirubakaran2
E. Kirubakaran2 Immanuel Johnraja Jebadurai1A. Immanuel Selvakumar3
Immanuel Johnraja Jebadurai1A. Immanuel Selvakumar3 J. Dinesh Peter1
J. Dinesh Peter1Sleep is a pivotal biological process and has generally been accepted as a critical factor in human health. Even though the whole function of sleep is not very well studied, it is associated with physical and mental wellness (1, 2). The transient disruptions in regular sleep patterns known as acute sleep deprivation impair cognitive skills. In contrast, long-term sleep abnormalities such as chronic sleep deprivation are related to disease development (3, 4).
Poor sleep quality (5) (as outlined by National Sleep Foundation recommended parameters sleep latency, wake after sleep onset, number of >5 minutes awakenings, and sleep efficiency) has an association with a slew of major medical conditions ranging from obesity and diabetes to neuropsychiatric disorders (6–8). Recent research findings also reveal the associations of poor sleep quality with cardiometabolic risk (9), diabetes (7), weight gain (6), impaired appetite (10), cognitive decline (11), mood changes (12), depression (13), immune function (14), and cancer (15). Global sleep trends indicate that average sleep time is diminishing (16, 17). Besides, sleep-related disorders are on the rise (18, 19). Considering these trends and the importance of sleep for health, a better understanding of sleep characteristics is a public health goal (20, 21).
Polysomnography (PSG) is the gold standard for objective sleep physiology evaluation and has proven to be the most helpful tool for diagnosing sleep-related breathing disorders such as obstructive sleep apnoea, central apnoea, hypopnea, and other respiratory disorders, and also for screening less common sleep disorders, including neurological disorders, such as narcolepsy, parasomnias and seizure disorders, restless legs syndrome and periodic limb movement disorder, depression with insomnia, and circadian rhythm sleep disorder in-clinic sleep assessment and sleep disturbances treatment (22, 23). A PSG study records distinct physiological signals, including electroencephalogram (EEG), electrooculogram (EOG), electromyography (EMG), electrocardiogram (ECG), respiration, pulse oximetry, and other parameters (24). After acquiring the PSG recordings, it is converted into 30-s epochs, and each epoch is mapped to a particular sleep stage (such as N1, N2, SWS, W, REM) manually by a sleep expert or technician, termed as sleep scoring (sleep staging/sleep stage classification). Traditionally more than one technician is involved in this process to avoid biases in marking sleep stages. The accuracy of sleep scoring depends on the expertise of the technicians (25). Although PSG use in clinical sleep medicine has significant benefits, the high cost is a barrier to its accessibility to many populations. Moreover, while undergoing an overnight PSG test, factors such as the unfamiliar sleeping environment with limited privacy, skin irritation due to electrode adhesion, and the numerous leads attached to the person, could obstruct sleep, undermining the accuracy of the recordings (26). Recent advancements in technology play an indispensable role in developing reliable portable monitors (PMs) that support the evaluation of sleep in-home and assist in overcoming the limitations of in-clinic PSG assessment (27). In general PMs are categorised as type 2 (at least seven channels), type 3 (minimum of four channels) and type 4 (either one or two channels) (28).
After considering the underpinning proof of a connection between sleep and wellness, challenges in the traditional sleep evaluation, the need for quality data for the sleep clinicians, this article discusses the significant importance of single-channel EEG in home-based sleep monitoring and analysis. Besides, to further explore the opportunities behind single-channel EEG this article highlights the need for in-home sleep monitoring and its challenges and the role of AI in sleep monitoring. Finally, the challenges in the presented technique and opportunities for future research are presented.
In-home sleep monitoring is gaining popularity because of its convenience, non-invasive, and self-administrable. In-home sleep monitoring usually uses type 4 sleep monitoring devices. These devices are either picked up by the patients from the clinic or delivered to their homes (29, 30).
A wearable sleep monitoring system (type 4) is widely used in-home sleep monitoring; these systems detect sleep stages based on any one or two of the signals such as brain waves, heart rate, pulse rate, respiration rate, movements, and other types of signals (body temperature, snoring, etc.) Even though different signals are used for sleep stage analysis, brain signals(EEG) provide more accuracy in specific sleep stage detection and analysis (27). For sleep professionals looking for a more trustworthy, long-term documented total sleep time evaluation, single-channel EEG could be a helpful tool (31). Affordable medical-grade EEG on a large scale is conceived by reducing the electrodes, making it more comfortable, miniaturised, and low-cost. Neurosky (single channel system), Muse and Melon (3-4 electrodes), iBrain, Zeo, and Ear-EEG are consumer-grade products available in the market (32–34).
Due to the COVID-19 pandemic, people are staying indoors; sleep habits have changed. Sleep disorders are common during the COVID-19 pandemic, affecting roughly 40% of the public and healthcare population (35, 36). Furthermore, non-emergency health services like sleep labs were shut to reduce the infection rate (37). During the pandemic, there has been a significant increase in the usage of PMs for sleep monitoring. Most healthcare providers are expecting this trend to continue in the future (38).
Sleep must be tracked in a free-living setting and in an unobtrusive manner to ensure that the sleep captured is as representative of regular sleep as feasible in order to understand the role of sleep in health and disease. Due to the limitations of PSG, most people are only monitored for a single night. Monitoring during one night, on the other hand, is insufficient to ascertain the actual sleep condition. Long-term, at-home monitoring is required to optimise effectiveness and obtain proper follow-up (29). There are currently various options available for sleep monitoring outside the laboratory using type 4 PM devices (39). Compared to the traditional PSG, the single-channel scheme will save money (40) and make data collection much more straightforward, and valuable in a situation like the COVID-19 pandemic (41, 42). A comparison work done by Lucey et al. (43) show that single-channel EEG can assess REM, combined Stages N2 and N3 sleep, and a variety of other indicators, including frontal slow-wave activity, in a way that is equivalent to polysomnography. Therefore, single-channel EEG based PMs can serve as a better alternative to traditional sleep monitoring, and a better solution for in-home monitoring (44). The significant advantage of in-home sleep monitoring is convenience, level of comfort, and less expensive (45).
A home sleep study records your breathing patterns while you sleep in your own bed using small, portable monitoring equipment (30). Even though in-home sleep study is convenient, comfortable, easily accessible and less expensive, it is having a set of challenges listed below.
An excellent in-home sleep monitoring system design must consider the way the sensor is connected to the body and its attachment method. Users may not prefer the inconvenient method (using adhesive) of connecting sensors to the body and connecting too many sensors. Hence, striking a better balance between user's requirements and acceptance is necessary to design an in-home sleep monitoring device (30, 46).
The capacity to do prolonged monitoring is essential for an effective sleep monitoring system. For reliable results and early detection of aberrant sleep abnormalities, long-term monitoring is required. In order to accomplish this, sleep monitoring devices should be low-cost, simple-to-use, and easily accessible (46). The capacity to do prolonged monitoring is essential for an effective sleep monitoring system. For reliable results and early detection of aberrant sleep abnormalities, long-term monitoring is required. In order to accomplish this, sleep monitoring devices should be low-cost, simple-to-use, and easily accessible. To this end, a bed based sensor (47), ear-based EEG (48), Wireless polysomnography system based on the Internet of Things (49), and posture recognition based sleep monitoring (50) proposed.
Sleep can be monitored using wearables for a wide range of physical and mental disorders. The majority of the studies relied on commercially accessible gadgets that are linked to smartphones or tablets (34, 51). Wearables can be used to track sleep data. Sleep data can be collected and sent over the internet to a remote clinical on-premise server or cloud server for further analysis, evaluation, decision-making, and treatment. In the captured data, applying machine or deep learning to evolving trends, and instantly alerting patients, nurses, and physicians is a powerful ability (46). Sharing data from a remote location is still a challenging task due to connectivity issues (52).
Long-term sleep data collection is more comprehensive and diverse. There is an increased chance of user personal information being leaked. Even though, informed consent is used before data collection; given the great value and growing popularity of big data apps, data sharing privacy is a big concern (29). Blockchain technology has the potential to address the issue of privacy and secure data sharing. Implementation of blockchain in real-life applications are in the inception stage and more understanding is needed (53).
Sleep technicians must verify each epoch manually to perform the sleep scoring, and it has limitations such as labour-intensive and time-consuming and inter-rater variability (25). Kappa (κ) measures the manual sleep scoring performance to estimate interrater reliability, representing an agreement between epoch-to-epoch. The benchmark κ value against human-AI algorithm agreement is 0.68–0.76 approximately (54). Analyzing hours of patient sleep records is not easy due to the aforementioned limitations. Therefore, researchers extensively use machine-learning (ML) and deep-learning (DL) techniques to score the sleep stages from the sleep data automatically (55).
ML models' performance depends on the representative features extracted from the EEG signals. The features are either extracted from 30-s data (epoch) or sub-bands of decomposed signals. Specific studies have extracted features from both the 30-s epochs as well as sub-bands or only from the decomposed signals. The commonly used EEG signal decomposition techniques used in the literature include EMD (empirical-mode decomposition), EEMD (ensemble-empirical-mode decomposition), wavelet-based, FFT (fast Fourier-transform), and frequency such as alpha, gamma, etc., based decomposition (56–58). Once the features are extracted from the EEG signal, it is given as an input (training/test data) to the ML model. Sleep scoring is a multi-class classification problem (mapping five/six sleep stages based on input features). Researchers have tested multiple ML models for automated sleep scoring systems viz.: tree-based models (Random forest, SVM, XGBoost, etc.), clustering (KNN), and an amalgamation of distinct models known as ensemble learning (stacking, boosting, bagging, and blending). These approaches achieved 74.5 to 91.9 % accuracy levels for a standard five-class classification (57, 59–63).
Data dimensionality is a notable concern in ML-based systems when dealing with high data-dimension like PSG, which overfit the ML model. Besides, ML-based sleep scoring systems have distinct phases, such as feature extraction, selection, and classification that run as separate tasks. Recent improvements in ML facilitate ways to run discrete tasks together. DL models provide encouraging results in sleep scoring using single-channel EEG based systems (64). The literature's proposed DL-based sleep scoring systems generate features from the input sequence or employ the manually extracted features. A few existing works have used 90- and 60-s epochs instead of traditional 30-second epochs for classification in order to represent the temporal relations between the sleep stages and enhance the sleep scoring results (65). Authors have explored many individual and cascaded DL models for automated sleep scoring systems. Some of the recently proposed DL based works are: convolutional neural network (CNN) (65, 66), IITNet, a CNN and Recurrent Neural Networks (RNN) based network (67), SingleChannelNet (SCNet), a CNN based model. The DL based approaches achieved 83.9 to 92.9% for a standard five-class classification (68), SleepStageNet (69), Long short-term memory (LSTM)-RNN (70). The Figure 1 illustrates the overview of sleep data extraction and analysis pipeline using cloud computing. The EEG signals are extracted from the individuals suspected of sleep-related issues. Then the signals are filtered to remove the noise and converted into 30-s epochs for identifying the specific sleep stages. Next, features are extracted manually using the methods mentioned above or fed the signals to the DL model for automatic feature extraction. The trained model is used to detect sleep stages automatically.
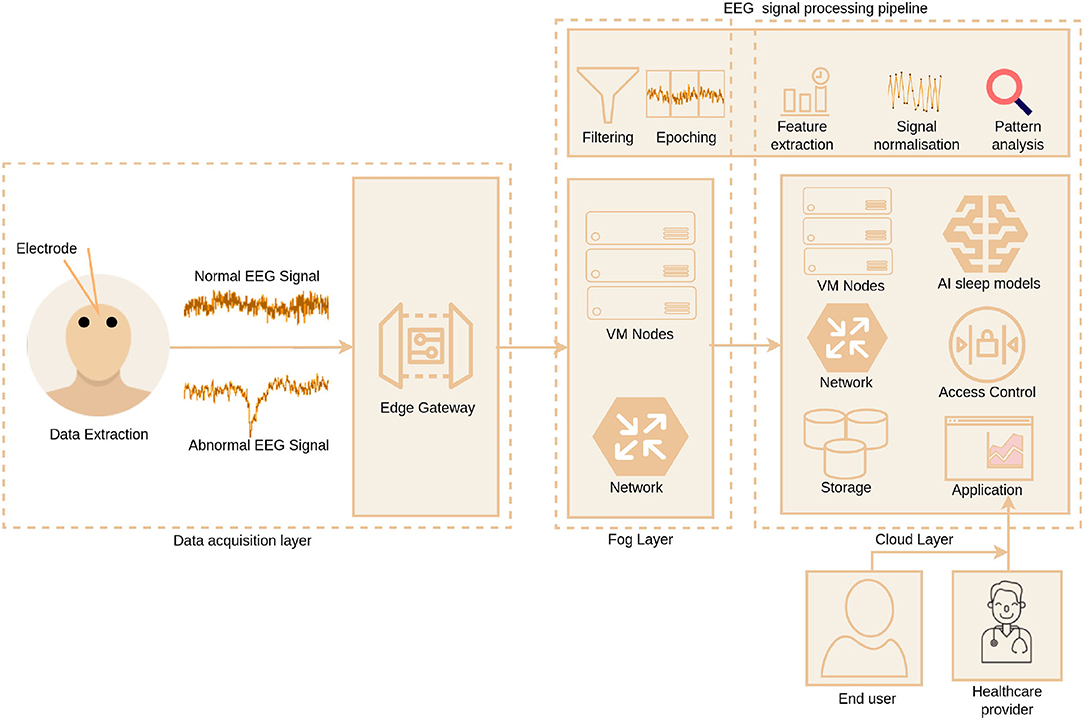
Figure 1. Overview of sleep data extraction and analysis using cloud computing.
Remote health monitoring is one of the key benefits of the digital era; it allows for remote tracking and monitoring of an individual's health-related factors, as well as sharing with healthcare specialists (71). Recent advancements in sensors, microcontrollers, and communication systems have made significant advances in remote healthcare, allowing for collecting health data from individuals. The Internet of Things (IoT) has pushed the healthcare industry to adopt completely digitised e-health systems and will undoubtedly play a role in remote healthcare (72). The application of wearable sensors to assess an individual's health or well-being status is most attractive in out-of-hospital circumstances (73).The IoT and Cloud integration is gaining traction in digital healthcare and is used for digital sleep monitoring and assessment. The modern digital sleep health applications comprise data acquisition, fog, and cloud layers depicted in Figure 1. The data acquisition layer uses wearable EEG devices for EEG data acquisition. The fog layer brings the cloud to the end-user devices to perform basic preprocessing of data and initial assessment at the user end. Also, It supplies the homogeneous data to the sleep application running in the cloud that simplifies the processing. The cloud layer provides the compute and storage for the applications. The data acquired by the wearable EEG devices needs to be accumulated and kept safely for future reference, trend analysis and retraining the deployed models. Cloud storage is the viable option to store the sleep data since it offers cost-efficiency, secure sharing, synchronisation and scalability. Healthcare providers leverage ML or DL models using the EEG data stored in the cloud to perform automated sleep stage analysis, resulting in more accurate insightful findings, visualisation, and diagnosis. Analysing EEG data and running sleep stage predictive models support real-time decision making. Despite the merits of the cloud, there are specific challenges when connecting EEG devices in real-time and storing data to the cloud. In the fog layer, EEG data may miss due to improper wearing of the device or malfunction of the sensor. Cloud layer stores and shares EEG data among applications; however, there is growing concern concerning privacy, security and data access (74–76).
In a technology-driven world, sleep is usually the first thing individuals compromise when they feel pressed against time. Chronic sleep deficiency is associated with cognitive skills, as well as health consequences, such as obesity, diabetes, neuropsychiatric disorders, cardiometabolic risk, impaired appetite, mood changes, depression, immune function, and cancer (6–10, 13–15). COVID-19 pandemic phenomenon increased the sleep-related issues and inaccessibility to sleep clinics. Despite continuous sleep monitoring having its benefits, COVID-19 highlighted its importance (35, 36). Contemporary advancements in sensing techniques, data analytics, and AI systems allow sleep monitoring ubiquitously and unobtrusively (38, 54, 65). Sleep monitoring research using single-channel EEG gains an excess of attraction and momentum since it supports continuous monitoring non-obstructive, aids detecting specific sleep stages accurately and is easy to employ at home (44, 45).
Many ML and DL-based models proposed in the literature achieved better accuracy and kappa (κ) values. Although ASSC systems produce better results, a set of specific challenges exist, such as database variability, channel mismatch, class imbalance, inter-class distinction, computational complexity, and scoring issues (63, 65). Most of the ML and DL-based models proposed in the literature used distinct datasets; these data had been collected from different individuals. Hence, this creates a bias during the comparison of results, and there is a need to investigate the robustness of the model (65). There has been a considerable interest among researchers to design sound in-home single-channel EEG-based sleep monitoring systems. Channel mismatch is another significant factor that hampers the performance of portable ASSC systems (65).
Effectively managing class imbalance (among stages of sleep) is an obligation of an ASSC system. All PSG recordings from healthy persons are generally imbalanced due to the less representation of the S1 stage. Consequently, both ML and DL models render limited performance in classifying the N1 stage (65). To handle this issue, researchers took different approaches. Zhou et al. (62) proposed a method that adjusts the class weights to achieve class balancing, and it has significantly improved the N1 stage recognition to 72.52%. Another author Jiang et al. (58) balanced only the training dataset to make all the classes equal. This approach improved the S1 stage detection from 0.44 to 0.58 (recall score). Moreover, this approach slightly improved the overall detection of less represented classes. In Sors et al. (66) class balancing is done using cost-sensitive learning. That improves N1 and N3 stage results significantly.
Sleep is referred to as a continuous event, and there is no clear-cut boundary between sleep stages. Therefore, different sleep stages, particularly transitioning stages, are tough to distinguish due to subtle inter-class distinctions (65). The sleep stages N1and N2 have similar features. Similarly, N1 and REM also have similar features. This similarity confuses the classifier and even human experts. Moreover, the S1 stage is the transitional stage between W and REM. Hence, among the tested classifiers in literature, N1 stage detection is still challenging (58). Some studies have combined the N1 and N2 stages as light sleep (LS), improving detection accuracy. This limitation can be further improved by incorporating EMG or EOG signals (69). The study by Michielli et al. (70) used a multi-class (N1 and REM combined) and binary class (N1 and REM) approach, this approach improving the N1 stage detection considerably. The performance of the ASSC systems depends on the ML/DL model's complexity. Hence, it is necessary to strike a balance between model complexity and performance (65). Training neural networks like RNN on GPU have tight memory size. This limitation is managed using lesser training sequences.
An in-home ASSC system based on single-channel EEG is required to alleviate the problems in manual scoring and enable the development of a convenient, comfortable, and less expensive in-home sleep monitoring system (63). Single-channel systems have excellent scope in terms of convenience and cost-effectiveness. When comparing the results of recent studies, single-channel EEG shows significant performance. However, there are fewer number studies that validate the results against PSG. Conducting more validation studies among the diverse group (including normal and person with a sleep disorder) using single-channel EEG and validating against PSG would improve the reliability and validity of the ASSC systems. A cloud-based trained and tested framework is necessary to provide accurate multi-model sleep scoring and analysis, seamless data sharing, and facilitate connecting health providers. The importance of continuous monitoring is evident in the literature. Continuous monitoring accumulates more data, detects sleep anomalies, and predicts health-related consequences. Cloud providers offer HIPPA compliance cloud storage that supports securely storing and sharing data. All the services offered by the cloud providers may not be HIPPA compliant. Therefore, before adopting a cloud service, it is essential to verify its HIPPA compliance. Convenience and accuracy is the prime objective of single-channel EEG systems. The missing data issue in the fog layer can be addressed by various methods such as tensor factorization (77). Some studies suggested that adding EMG or EOG sensors may improve the discrepancies in detecting accuracy among N1, N2, and REM stages. However, it causes inconvenience and obstructs regular sleep. Therefore, future research could incorporate heart rate and body movement signals (smartwatches or wearables) with single-channel EEG to improve sleep scoring.
BR, EK, IJ, AS, and JP contributed to the study conception and design, literature review, interpretation, and manuscript preparation. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Schwartz JR, Roth T. Neurophysiology of sleep and wakefulness: basic science and clinical implications. Curr Neuropharmacol. (2008) 6:367–78. doi: 10.2174/157015908787386050
2. Clement-Carbonell V, Portilla-Tamarit I, Rubio-Aparicio M, Madrid-Valero JJ. Sleep quality, mental and physical health: a differential relationship. Int J Environ Res Publ Health. (2021) 18:460. doi: 10.3390/ijerph18020460
4. Bertisch SM, Pollock BD, Mittleman MA, Buysse DJ, Bazzano LA, Gottlieb DJ, et al. Insomnia with objective short sleep duration and risk of incident cardiovascular disease and all-cause mortality: sleep heart health study. Sleep. (2018) 41:zsy047. doi: 10.1093/sleep/zsy047
5. Ohayon M, Wickwire EM, Hirshkowitz M, Albert SM, Avidan A, Daly FJ, et al. National Sleep Foundation's sleep quality recommendations: first report. Sleep Health. (2017) 3:6–19. doi: 10.1016/j.sleh.2016.11.006
6. Kim HO, Kang I, Choe W, Yoon KS. Sleep duration and risk of obesity: a genome and epidemiological study. World Acad Sci J. (2021) 3:1. doi: 10.3892/wasj.2021.91
7. Lu H, Yang Q, Tian F, Lyu Y, He H, Xin X, et al. A meta-analysis of a cohort study on the association between sleep duration and type 2 diabetes mellitus. J Diabetes Res. (2021) 2021, 8861038. doi: 10.1155/2021/8861038
8. Kammerer MK, Mehl S, Ludwig L, Lincoln TM. Sleep and circadian rhythm disruption predict persecutory symptom severity in day-to-day life: a combined actigraphy and experience sampling study. J Abnormal Psychol. (2021) 130:78. doi: 10.1037/abn0000645
9. Nagai M, Hoshide S, Kario K. Sleep duration as a risk factor for cardiovascular disease-a review of the recent literature. Curr Cardiol Rev. (2010) 6:54–61. doi: 10.2174/157340310790231635
10. Knutson KL, Spiegel K, Penev P, Van Cauter E. The metabolic consequences of sleep deprivation. Sleep Med Rev. (2007) 11:163–78. doi: 10.1016/j.smrv.2007.01.002
11. Spira AP, Chen-Edinboro LP, Wu MN, Yaffe K. Impact of sleep on the risk of cognitive decline and dementia. Curr Opin Psychiatry. (2014) 27:478. doi: 10.1097/YCO.0000000000000106
12. Selvi Y, Gulec M, Agargun MY, Besiroglu L. Mood changes after sleep deprivation in morningness–eveningness chronotypes in healthy individuals. J Sleep Res. (2007) 16:241–4. doi: 10.1111/j.1365-2869.2007.00596.x
13. Becker NB, de Jesus SN, Viseu JN, Stobäus CD, Guerreiro M, Domingues RB. Depression and quality of life in older adults: Mediation effect of sleep quality. Int J Clin Health Psychol. (2018) 18:8–17. doi: 10.1016/j.ijchp.2017.10.002
14. Tan HL, Kheirandish-Gozal L, Gozal D. Sleep, sleep disorders, and immune function. In: Allergy and Sleep. Cham: Springer (2019). p. 3–15.
15. Lu Y, Tian N, Yin J, Shi Y, Huang Z. Association between sleep duration and cancer risk: a meta-analysis of prospective cohort studies. PloS ONE. (2013) 8:e74723. doi: 10.1371/journal.pone.0074723
17. Fry C. Sleep deprived but socially connected: balancing the risks and benefits of adolescent screen time during COVID-19. J Children Media. (2021) 15:37–40. doi: 10.1080/17482798.2020.1858907
19. Zitting KM, Lammers-van der Holst HM, Yuan RK, Wang W, Quan SF, Duffy JF. Google Trends reveals increases in internet searches for insomnia during the 2019 coronavirus disease (COVID-19) global pandemic. J Clin Sleep Med. (2021) 17:177–84. doi: 10.5664/jcsm.8810
20. Stranges S, Tigbe W, Gómez-Olivé FX, Thorogood M, Kandala NB. Sleep problems: an emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep. (2012) 35:1173–81. doi: 10.5665/sleep.2012
21. Hafner M, Stepanek M, Taylor J, Troxel W, Stolk C. Why Sleep Matters – the Economic Costs of Insufficient Sleep: A Cross-Country Comparative Analysis. vol. 6. RAND Corporation. (2016). Available online at: https://circadiansleepcoaching.com/wp-content/uploads/sites/1753/2022/01/RAND-REPORT-2016.pdf
22. Thorpy M. International classification of sleep disorders. In: Sleep Disorders Medicine. Springer. (2017). p. 475–84. doi: 10.1007/978-1-4939-6578-6_27
23. Sharma M, Goyal D, Achuth P, Acharya UR. An accurate sleep stages classification system using a new class of optimally time-frequency localized three-band wavelet filter bank. Comput Biol Med. (2018) 98:58–75. doi: 10.1016/j.compbiomed.2018.04.025
24. Berthomier C, Drouot X, Herman-Stoïca M, Berthomier P, Prado J, Bokar-Thire D, et al. Automatic analysis of single-channel sleep EEG: validation in healthy individuals. Sleep. (2007) 30:1587–95. doi: 10.1093/sleep/30.11.1587
25. Cesari M, Stefani A, Penzel T, Ibrahim A, Hackner H, Heidbreder A, et al. Interrater sleep stage scoring reliability between manual scoring from two European sleep centers and automatic scoring performed by the artificial intelligence–based Stanford-STAGES algorithm. J Clin Sleep Med. (2021) 17:1237–47. doi: 10.5664/jcsm.9174
26. Zhang J, Tang Z, Gao J, Lin L, Liu Z, Wu H, et al. Automatic detection of obstructive sleep apnea events using a deep CNN-LSTM model. Comput. Intell Neurosci. (2021) 2021:5594733. doi: 10.1155/2021/5594733
27. Kwon S, Kim H, Yeo WH. Recent advances in wearable sensors and portable electronics for sleep monitoring. Iscience. (2021) 24:102461. doi: 10.1016/j.isci.2021.102461
28. Krishnaswamy U, Aneja A, Kumar RM, Kumar TP. Utility of portable monitoring in the diagnosis of obstructive sleep apnea. J Postgraduate Med. (2015) 61:223. doi: 10.4103/0022-3859.166509
29. Pan Q, Brulin D, Campo E. Current Status and Future Challenges of Sleep Monitoring Systems: Systematic Review. JMIR Biomed Eng. (2020) 5, e20921. doi: 10.2196/20921
30. Shustak S, Inzelberg L, Steinberg S, Rand D, Pur MD, Hillel I, et al. Home monitoring of sleep with a temporary-tattoo EEG, EOG and EMG electrode array: a feasibility study. J Neural Eng. (2019) 16:026024. doi: 10.1088/1741-2552/aafa05
31. Hof zum Berge A, Ferrauti A, Meyer T, Pfeiffer M, Kellmann M. Portable polysomnography for sleep monitoring in elite youth rowing: An athlete's gain or the sleep's thief? Transl Sports Med. (2021) 4:289–96. doi: 10.1002/tsm2.205
32. NeuroSky. EEG Sensors - EEG Headsets | NeuroSky. (2020). Available Online at: http://neurosky.com/biosensors/eeg-sensor/biosensors/
33. Muse. Muse™ - Meditation Made Easy With the Muse Headband. (2021). Available Online at: https://choosemuse.com/
34. Looney D, Goverdovsky V, Rosenzweig I, Morrell MJ, Mandic DP. Wearable in-ear encephalography sensor for monitoring sleep. preliminary observations from nap studies. Ann Am Thoracic Soc. (2016) 13:2229–33. doi: 10.1513/AnnalsATS.201605-342BC
35. Jahrami H, BaHammam AS, Bragazzi NL, Saif Z, Faris M, Vitiello MV. Sleep problems during the COVID-19 pandemic by population: a systematic review and meta-analysis. J Clin Sleep Med. (2021) 17 :299–313. doi: 10.5664/jcsm.8930
36. Radhakrishnan B, Kirubakaran E, Belfin R, Selvam S, Sagayam KM, Elngar AA. Mental health issues and sleep quality of Indian employees and higher education students during COVID-19 lockdown. Int J Intell Eng Inf. (2021) 9:193–210. doi: 10.1504/IJIEI.2021.10040086
37. Lee M, You M. Avoidance of healthcare utilization in south korea during the coronavirus disease 2019 (COVID-19) pandemic. Int J Environ Res Publ Health. (2021) 18:4363. doi: 10.3390/ijerph18084363
38. Johnson KG, Sullivan SS, Nti A, Rastegar V, Gurubhagavatula I. The impact of the COVID-19 pandemic on sleep medicine practices. J Clin Sleep Med. (2021) 17:79–87. doi: 10.5664/jcsm.8830
39. Baltrušaitis T, Ahuja C, Morency LP. Multimodal machine learning: a survey and taxonomy. IEEE Trans Pattern Anal Mach Intell. (2018) 41:423–43. doi: 10.1109/TPAMI.2018.2798607
40. Supratak A, Dong H, Wu C, Guo Y. DeepSleepNet: a model for automatic sleep stage scoring based on raw single-channel EEG. IEEE Trans Neural Syst Rehabil Eng. (2017) 25:1998–2008. doi: 10.1109/TNSRE.2017.2721116
41. Toedebusch CD, McLeland JS, Schaibley CM, Banks IR, Boyd J, Morris JC, et al. Multi-modal home sleep monitoring in older adults. J. Visual. Exp. JoVE. (2019) 143: 10.3791/58823. doi: 10.3791/58823
42. Faezipour M, Faezipour M. Efficacy of smart EEG monitoring amidst the COVID-19 pandemic. Electronics. (2021) 10:1001. doi: 10.3390/electronics10091001
43. Lucey BP, Mcleland JS, Toedebusch CD, Boyd J, Morris JC, Landsness EC, et al. Comparison of a single-channel EEG sleep study to polysomnography. J Sleep Res. (2016) 25:625–35. doi: 10.1111/jsr.12417
44. Hussain Z, Sheng QZ, Zhang WE, Ortiz J, Pouriyeh S. A review of the non-invasive techniques for monitoring different aspects of sleep. arXiv preprint arXiv:210412964. (2021).
45. Kundel V, Shah N. Impact of portable sleep testing. Sleep Med Clin. (2017) 12:137. doi: 10.1016/j.jsmc.2016.10.006
46. Guillodo E, Lemey C, Simonnet M, Walter M, Baca-García E, Masetti V, et al. Clinical applications of mobile health wearable–based sleep monitoring: systematic review. JMIR mHealth uHealth. (2020) 8:e10733. doi: 10.2196/10733
47. Shin J, Chee Y, Park K. Long-term sleep monitoring system and long-term sleep parameters using unconstrained method. In: Proceedings of Intl Special Topic Conf on Info Tech in BME. New York, NY (2006).
48. Nakamura T, Goverdovsky V, Morrell MJ, Mandic DP. Automatic sleep monitoring using ear-EEG. IEEE J Transl Eng Health Med. (2017) 5:1–8. doi: 10.1109/JTEHM.2017.2702558
49. Lin CT, Prasad M, Chung CH, Puthal D, El-Sayed H, Sankar S, et al. IoT-based wireless polysomnography intelligent system for sleep monitoring. IEEE Access. (2017) 6:405–14. doi: 10.1109/ACCESS.2017.2765702
50. Matar G, Lina JM, Carrier J, Riley A, Kaddoum G. Internet of Things in sleep monitoring: an application for posture recognition using supervised learning. In: 2016 IEEE 18th International Conference on e-Health Networking, Applications and Services (Healthcom). Munich: IEEE. (2016). p. 1–6.
51. Koydemir HC, Ozcan A. Wearable and implantable sensors for biomedical applications. Ann Rev Anal Chem. (2018) 11:127–46. doi: 10.1146/annurev-anchem-061417-125956
52. Radhakrishnan B, Kirubakaran E, Ebenezer V, Belfin R, Ting DI, et al. Remote sleep monitoring and 5G. In:Secure Communication for 5G and IoT Networks. Springer. (2022). p. 173–95. doi: 10.1007/978-3-030-79766-9_11
53. Yaeger K, Martini M, Rasouli J, Costa A. Emerging blockchain technology solutions for modern healthcare infrastructure. J Sci Innov Med. (2019) 2:1. doi: 10.29024/jsim.7
54. Danker-hopfe H, Anderer P, Zeitlhofer J, Boeck M, Dorn H, Gruber G, et al. Interrater reliability for sleep scoring according to the Rechtschaffen & Kales and the new AASM standard. J Sleep Res. (2009) 18:74–84. doi: 10.1111/j.1365-2869.2008.00700.x
55. Stephansen JB, Olesen AN, Olsen M, Ambati A, Leary EB, Moore HE, et al. Neural network analysis of sleep stages enables efficient diagnosis of narcolepsy. Nat Commun. (2018) 9:1–15. doi: 10.1038/s41467-018-07229-3
56. Boostani R, Karimzadeh F, Nami M. A comparative review on sleep stage classification methods in patients and healthy individuals. Comput Methods Programs Biomed. (2017) 140:77–91. doi: 10.1016/j.cmpb.2016.12.004
57. Memar P, Faradji F. A novel multi-class EEG-based sleep stage classification system. IEEE Trans Neural Syst Rehabil Eng. (2017) 26:84–95. doi: 10.1109/TNSRE.2017.2776149
58. Jiang D, Lu Yn, Yu M, Yuanyuan W. Robust sleep stage classification with single-channel EEG signals using multimodal decomposition and HMM-based refinement. Exp Syst Appl. (2019) 121:188–203. doi: 10.1016/j.eswa.2018.12.023
59. Hassan AR, Bhuiyan MIH. Automatic sleep scoring using statistical features in the EMD domain and ensemble methods. Biocybern Biomed Eng. (2016) 36:248–55. doi: 10.1016/j.bbe.2015.11.001
60. Hassan AR, Bhuiyan MIH. Computer-aided sleep staging using complete ensemble empirical mode decomposition with adaptive noise and bootstrap aggregating. Biomed Signal Process Control. (2016) 24:1–10. doi: 10.1016/j.bspc.2015.09.002
61. Seifpour S, Niknazar H, Mikaeili M, Nasrabadi AM. A new automatic sleep staging system based on statistical behavior of local extrema using single channel EEG signal. Exp Syst Appl. (2018) 104:277–93. doi: 10.1016/j.eswa.2018.03.020
62. Zhou J, Wang G, Liu J, Wu D, Xu W, Wang Z, et al. Automatic sleep stage classification with single channel EEG signal based on two-layer stacked ensemble model. IEEE Access. (2020) 8:57283–97. doi: 10.1109/ACCESS.2020.2982434
63. Liu C, Tan B, Fu M, Li J, Wang J, Hou F, et al. Automatic sleep staging with a single-channel EEG based on ensemble empirical mode decomposition. Phys A Stat Mech Appl. (2021) 567:125685. doi: 10.1016/j.physa.2020.125685
64. Loh HW, Ooi CP, Vicnesh J, Oh SL, Faust O, Gertych A, et al. Automated detection of sleep stages using deep learning techniques: a systematic review of the last decade (2010–2020). Appl Sci. (2020) 10:8963. doi: 10.3390/app10248963
65. Li F, Yan R, Mahini R, Wei L, Wang Z, Mathiak K, et al. End-to-end sleep staging using convolutional neural network in raw single-channel EEG. Biomed Signal Process Control. (2021) 63:102203. doi: 10.1016/j.bspc.2020.102203
66. Sors A, Bonnet S, Mirek S, Vercueil L, Payen JF. A convolutional neural network for sleep stage scoring from raw single-channel EEG. Biomed Signal Process Control. (2018) 42:107–14. doi: 10.1016/j.bspc.2017.12.001
67. Seo H, Back S, Lee S, Park D, Kim T, Lee K. Intra-and inter-epoch temporal context network (IITNet) using sub-epoch features for automatic sleep scoring on raw single-channel EEG. Biomed Signal Process Control. (2020) 61:102037. doi: 10.1016/j.bspc.2020.102037
68. Zhou D, Hu G, Zhang J, Wang J, Yan R, Li F, et al. SingleChannelNet: a model for automatic sleep stage classification with raw single-channel EEG. bioRxiv. (2021) p. 2020–09.
69. Chen K, Zhang C, Ma J, Wang G, Zhang J. Sleep staging from single-channel EEG with multi-scale feature and contextual information. Sleep Breath. (2019) 23:1159–67. doi: 10.1007/s11325-019-01789-4
70. Michielli N, Acharya UR, Molinari F. Cascaded LSTM recurrent neural network for automated sleep stage classification using single-channel EEG signals. Comput Biol Med. (2019) 106:71–81. doi: 10.1016/j.compbiomed.2019.01.013
71. Albahri OS, Albahri AS, Mohammed K, Zaidan A, Zaidan B, Hashim M, et al. Systematic review of real-time remote health monitoring system in triage and priority-based sensor technology: taxonomy, open challenges, motivation and recommendations. J Med Syst. (2018) 42:1–27. doi: 10.1007/s10916-018-0943-4
72. Ray PP, Dash D, Kumar N. Sensors for internet of medical things: State-of-the-art, security and privacy issues, challenges and future directions. Comput Commun. (2020) 160:111–31. doi: 10.1016/j.comcom.2020.05.029
73. Korhonen I, Parkka J, Van Gils M. Health monitoring in the home of the future. IEEE Eng Med Biol Mag. (2003) 22:66–73. doi: 10.1109/MEMB.2003.1213628
74. Aazam M, Huh EN. Fog computing and smart gateway based communication for cloud of things. In: 2014 International Conference on Future Internet of Things and Cloud. Barcelona: IEEE (2014). p. 464–70.
75. Sangat P, Indrawan-Santiago M, Taniar D. Sensor data management in the cloud: data storage, data ingestion, and data retrieval. Concurr Comput Pract Exp. (2018) 30:e4354. doi: 10.1002/cpe.4354
76. Yacchirema DC, Sarabia-Jácome D, Palau CE, Esteve M. A smart system for sleep monitoring by integrating IoT with big data analytics. IEEE Access. (2018) 6:35988–6001. doi: 10.1109/ACCESS.2018.2849822
Keywords: sleep, sleep disorders, sleep monitoring, remote sleep monitoring, sleep quality, sleep stage classification, single-channel EEG
Citation: Radhakrishnan BL, Kirubakaran E, Jebadurai IJ, Selvakumar AI and Peter JD (2022) Efficacy of Single-Channel EEG: A Propitious Approach for In-home Sleep Monitoring. Front. Public Health 10:839838. doi: 10.3389/fpubh.2022.839838
Received: 20 December 2021; Accepted: 21 March 2022;
Published: 12 April 2022.
Edited by:
Steven Fernandes, Creighton University, United StatesReviewed by:
Venkatesan Rajinikanth, St. Joseph's College of Engineering, IndiaCopyright © 2022 Radhakrishnan, Kirubakaran, Jebadurai, Selvakumar and Peter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: B. L. Radhakrishnan, Ymxyay5yZXNlYXJjaEBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.