 Rafaela Simon Myra1†
Rafaela Simon Myra1† Micheline Henrique Araújo da Luz Koerich2†‡
Micheline Henrique Araújo da Luz Koerich2†‡ Elaine Cristina Gregório1
Elaine Cristina Gregório1 Alessandra Swarowsky3*
Alessandra Swarowsky3*- 1Brazilian Parkinson's Disease Rehabilitation Initiative (BPaRkI), Center for Health and Sports Sciences (CEFID), Santa Catarina State University (UDESC), Florianópolis, Brazil
- 2Center for Health and Sports Sciences (CEFID), Santa Catarina State University (UDESC), Florianópolis, Brazil
- 3Physical Therapy Program, AdventHealth University, Orlando, FL, United States
Background: People with Parkinson's disease (PD) need to exercise to have a better quality of life. The risk of falling needs to be considered when choosing and implementing exercise interventions. Flowcharts are used to facilitate referrals in Brazilian primary care network, but there is no specific one for PD.
Aim: To develop a referral flowchart for people with PD in Brazilian primary care based on the risk of falls and scientific evidence in the context of a multidisciplinary approach.
Methods: The development of the referral flowchart was accomplished in three steps; (1) relevant literature was reviewed (2) semi-structured interviews (in focus groups) were conducted with primary health care professionals to investigate the current care for people with Parkinson's disease, and (3) the information obtained from the previous steps were analyzed to inform the development of the referral flowchart.
Results: The fall risk-based flowchart uses the 3-step-fall-prediction tool. The primary health care professional should refer the person with a low risk of falls to activities with minimal supervision and those with a higher risk of falls to specialized neurology services. Neurology services are also the referral target for persons presenting significant mobility restrictions (i.e., restricted to a wheelchair or bed). The referral occurs according to what is available in Brazilian primary care.
Conclusion: This flowchart might be the first step to build a multidisciplinary approach for people with Parkinson's disease in Brazilian primary care. The next stage of this study is the validation and subsequent implementation of the flowchart through the primary care at Unified Health System in Brazil.
Background
The progressive nature of Parkinson's disease (PD) and the range of symptoms accompanying PD is a complex challenge for the Health System to manage successfully (1–3). As PD progresses, falling can present as an early symptom, and it becomes increasingly frequent in advanced PD, as is the presence of dementia and severe dysphagia (4).
Fall often have deleterious consequences for people with PD, their caregiver, and the quality of life of both (1–3). Falls and fear of falling in PD can lead to (1) significant limitations to daily-life activities (5); (2) pain and decreased independence (6); (3) upper and lower limb fractures (7); (4) increased morbidity (1). The most common causes of hospitalization in people with PD are pneumonia, motor decline, urinary tract infection, and hip fractures. Also, increasing age and presence of dementia were commonly associated with increased mortality (8).With that information we can assume the relationship between the falls and the increase in mortality (1).
Many hospitalizations and attending primary medical care following a fall will have a significant cost impact on the health system (9). Such cost impact may be minimized if the primary care (PC) pathway for prevention and management of falls in PD people was integrated and standardized (10). Fall prevention programs have also been carried out in some other alterations, such as diabetes (11), diabetic neuropathy (12), osteoporosis (13), elderly people (14), and it obtained satisfactory results. Integrated models of multidisciplinary care have been proposed to improve the quality of care for people with PD (15, 16). These types of integrated models could be adapted for low to middle-income countries (16). Brazil has a well-established Unified Health System (UHS), which offers an integrated care model, especially in PC (17). PC comprises the Family Health Strategy (FHS) with allied-health professionals' teams who work collaboratively to develop and deliver care plans that best suit each patient, the presenting symptoms and achieve the expected patient outcomes (17).
Even with an integrated model of care, the Brazilian PC UHS does not have a standardized approach for preventing, treating, and managing falls in people with PD. Brazil primary care is generalist and focused on prevalent diseases, which means that some diseases do not receive as much attention and care. Recent data show that 57% of the people with PD from different regions of Brazil, in general, were not prescribed physiotherapy, and 75% did not do other therapeutic activities, such as speech therapy, occupational therapy, and psychology treatment. This fact may be related to the lack of information and experience in treating PD (18). Despite evidence that exercise reduces falls in people with PD (19, 20), referred patients encountered a variable and ad-hoc approach to falls' care and management, with minimal multidisciplinary care provided (21). This situation can be explained by the lack of an explicit policy for referrals and subsequent fall management in the Brazilian PC UHS.
Given the increasing life expectancy of Brazilians (22), the number of people presenting with PD tends to increase, resulting in higher demand for care. As falls represent a significant determinant of quality of life, our study aimed to create a referral flowchart based on the fall risk in people with PD to guide the PC's health professionals.
Methods
The flowchart development occurred in three steps: (1) literature review, (2) focus group interviews with professionals from the Family Health Strategy (FHS) and (3) refinement of the flowchart elements. The Ethics Committee for Human Beings (CESPH) of the State University of Santa Catarina approved this study under number 2,950,524.
Literature review
A detailed non-systematic literature review sought the highest level of evidence specific to PD (Guidelines, Meta-analyzes, Systematic Reviews, and Randomized Controlled Trials). We searched for information regarding the recommended treatment according to disease severity, the occurrence of falls, and fall risk. We used the following databases - PubMed, SciELO, Lilacs, Medline, Cinahal, PEDRO - with the keywords Parkinson's disease AND falling OR fall OR falls. We included articles in English and Portuguese without the restriction of date.
Focus groups interviews
The study was conducted at the Health Centers (HC) of the four health districts (Center, Continent, North, and South) of Florianópolis - Santa Catarina, Brazil, that offered PC services. There are 45 HC spread across the health districts and 125 FHS teams working in them. The FHS teams, work in the HC and are the first contact with people with PD arriving at PC.
The FHS teams are formed primarily by a general practitioner, or specialist in Family Health, or a Family and Community physician; generalist nurse or specialist in Family Health; nursing assistant or technician; and community health agents. It is relevant to say that rehabilitation professionals work in the HC but don't integrate the FHS teams and people who need the rehabilitation service must be referred by FHS professionals.
Florianópolis is the capital city of Santa Catarina State and is the second largest in the number of inhabitants, with approximately 508,826 individuals (22). Also, it is the Brazilian reference (model) for structuring the UHS due to excellent health indicators and population coverage of 90% (23).
Before recruiting FHS teams between January 2016 and December 2017, a survey of people diagnosed with PD was carried out through a municipality's information system management (GeI - Geinfo / DIPLAN). A list of people with PD who engaged in PC services was used to determine those health units with the highest PD caseloads. The FHS were recruited by e-mail, and the focus groups (FG) were formed.
The Consolidated criteria for the REporting Qualitative research Checklist (COREQ) were used to guide FG interviews. The COREQ is a 32-item checklist to assist researchers in reporting essential aspects of the research team, study methods, context of the study, findings, analysis, and interpretations (24). We conducted the FG interview with the FHS teams to determine how they approach and manage people with PD at the PC. It includes the opinions of professionals on the role of PC in the treatment of people with PD and the main barriers and strengths faced in their care. We also examined existing specialized services (polyclinics and rehabilitation centers) and identified the services offered in HC (walking, physical activity, and nutrition groups) to propose the referral flowchart.
After agreeing to participate, the FG meetings were scheduled and held in the HC of each district. A total of eight focus groups took place between January and June 2019, conducted by a moderator, member of the research team, who took detailed interview notes. The FG health professionals number ranged from two to nine, and the interviews lasted from 20 min to 40 min (average of 30 min). There were no conflicts of interest between the researchers and FGs.
A semi-structured interview guided the questions and was recorded by audio. Researchers identified possible central themes, phrases, and impressions. The following issues were framed into questions that each FG discussed: (I) Experience with PD; (II) Diagnosis and Management for people with PD, (III) Referrals, (IV) Specialized Care; and (V) Options for multi-professional activities available at the health unit. Two researchers read the transcribed data and created codes using open coding to themes and subthemes. When differences in interpretation occurred, a third researcher was consulted, and the majority view was prevailing. After the eighth FG, no new information and themes emerged, and we identified the saturation point of the interviews. To assist the organization of the collected data, we used the software package ATLAS.ti8.
Flowchart elaboration
The data obtained from the qualitative research was used to build and scaffold the referral flowchart based on the risk of falls for people with PD. In addition, the services that were available in PC in the city of Florianopolis and the data from the literature review were incorporated and assisted in the development, structure, and sequencing of the flowchart. The proposal for structuring the PC services for people with PD was structured into: (1) PD care recommendations – Crucial points based on the literature review and (2) The referral flowchart based on the risk of falls - How does it work?
Results
The results are organized in three steps: (1) Literature review results: in this section, we will aboard the PD care recommendations and show the crucial points for treating people with and without risk of falling. (2) Focus group results: Here we present the qualitative data and its contribution to the construction of the flowchart. (3) The referral flowchart structure and how to employ it: in this section, we present the creative process of the flowchart and a manual for using it.
PD care recommendations—crucial points based on the literature review
PD is a multisystemic disease with several motor and non-motor symptoms. The drug treatment available is only partially effective, requiring multidisciplinary care to complete the approach. The involvement of professionals such as physiotherapists, speech therapists, nurses, psychologists, nutritionists, among others, is as significant as the physician's attention (21). The European Physiotherapy Guideline for Parkinson's Disease (2014) states that ideally, a neurologist and a nurse (or other professional with experience in managing PD to access the disease) should always be involved in treating people with PD, corroborating with different specialties to improve their physical well-being (25).
Worldwide, several guidelines recommend multidisciplinary care for the treatment of persons with PD. These include the guidelines produced by the Dutch National Professional Allied Health Associations on speech therapy, occupational therapy, and nutrition (26–30). In addition, a multidisciplinary approach is considered more favorable for PD managing motor and non-motor symptoms (31).
Currently, it is recognized that when performing an exercise, people with PD benefit in different physical (32, 33) and mental aspects (34). Recent evidence also suggests that aerobic exercise may slow the progression of PD symptoms (35). However, special care is required to prescribe exercise for people with PD, accounting for the ' 'individual's mobility status, as well as motor and non-motor impairments. People at risk of falling should be observed more carefully to avoid accidents.
The Brazilian UHS recognizes health as a right for the people and a duty for the state (36). The government must ensure it through social and economic politics, reduce disease risks, and give equal access to health services (36). Specifically, for neurological diseases, in 2005, the Ministry of Health created the National Policy for Attention to Patients with Neurological Disease targeted at people with these health conditions (37). In 2017, the Clinical Protocol and Therapeutic Guidelines for Parkinson's Disease were approved. It aimed to structure the care network, define care services, and establish flowcharts for people with PD. However, it emphasized only clinical aspects of the disease-related medication and surgery, leaving aside other health-related therapies and practices, including physical therapy or any multidisciplinary referral services. In addition, to date, the implementation of this Protocol is still being structured. Thus, it is noted that PD care in the Brazilian UHS presents opportunities for improvement (38).
Approach to people with PD—with or without risk of falling
When taking the clinical decision about exercise prescription and the need for referring people with PD with accuracy, it is necessary to consider the high rate of falls in this population. PD falls are heterogeneous, recurrent, causing morbidity (1), and might be present since the early stages of the disease (2, 3). Falls can lead to activity limitations (5), pain (6), decreased independence, fear of falling (39), injuries, disabling fractures, among others (5).
Falls may be associated with generic (aging-related) or PD-related factors (21). Generic risk factors include advanced age, polypharmacy and sedative use, cardiac arrhythmia, hypotension, depression, female gender, osteoporosis, weakness due to inactivity, use of visual aids and, anxiety. PD-related risk factors include: (1) disease severity, (2) axial stiffness, (3) cognitive impairment, (4) dyskinesias, (5) history of falls, (6) abnormal posture, (7) high dose of levodopa, (8) use of dopamine agonists, (9) reduced mobility (10) postural instability, (11) freezing of gait (FOG) or festination, and (12) urinary incontinence (21, 40). Environmental risk factors (quality of sidewalks and streets, lack of home adaptations, type of footwear used) also contribute to the high rate of falls (40).
Although falls can occur in the early stages of the disease, falls are not frequent, with a low level of association with the person's daily activities (19). With disease progression, the number of falls increases due to postural and gait changes while the people are still active (19). Although people with PD have an increased risk of falls in the later stages, they are less mobile, so the number of falls tends to be lower (19). Therefore, falls and their complications need to be considered when choosing the best treatment. And as mentioned earlier, physical exercise and physical therapy are essential for improving the quality of life of people with PD (19, 25, 32, 33, 41, 42).
Currently, several tools help to predict falls in PD. Scales as Functional Gait Assessment (37, 43) and Mini-Balance Evaluation Systems Test (44) are well structured but are lengthy and challenging to be applied by the primary health care network health professional who is unlikely to be a physiotherapist. An alternative is the 3-step fall prediction test, which assesses falls in the past year (Yes/No), freezing of gait in the past month (Yes/No), and comfortable gait speed (Yes/No) (Table 1) (45–47).
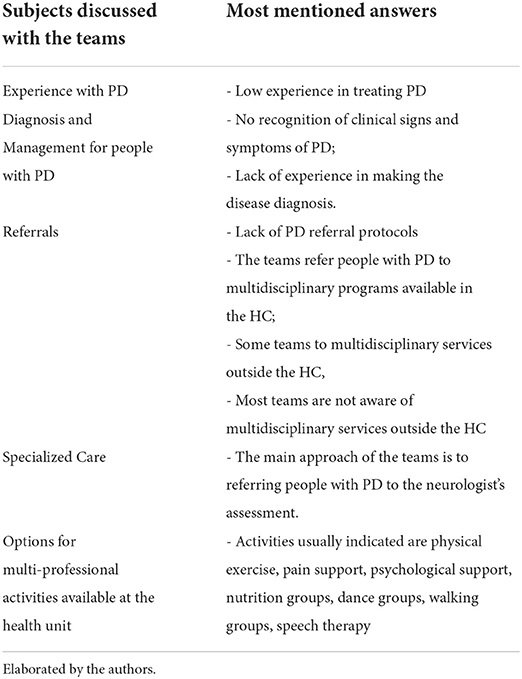
Table 1. Subjects and answers of the qualitative interviews.
The 3-step-fall-prediction test is objective and accessible to daily use, and it is validated for people with PD (46, 47). It determines the probability of falling in the next 6 months and rates it as a low (17%), moderate (51%), or high (85%) risk of falls, based on the weighted sum of scores for the 3 questions. (46). The test requires periodic reevaluations (in six months) and is crucial for establishing care routines, (45, 46). Although no training is required for physical therapists, it is recommended that other health professionals learn how to measure gait speed.
The 3-step-fall prediction test has been externally validated in 171 PD people showing accuracy to discriminate fallers from non-fallers (AUC = 0.83; 95% CI 0.76–0.89) (46). The test has recently been administered using a self-report measure for gait speed with similar accuracy to the original 3-step clinical prediction tool (47). The self-reported 3-step-fall prediction test may be useful to identify people with PD at risk of falls in e/tele-health settings (47), or to use in HC with no space to test for gait speed and then referral to other services accordingly.
Those people with PD who are at low risk of falls could engage in group activities available at the PC and require less attention from the health professional. On the other hand, fallers require more outstanding care and may be referred to rehabilitation services such as Specialized Rehabilitation Centers (RECs). Another critical point to remember is the need for more focused attention for lower-mobility people. Those who are mobility-restricted and recurrent fallers also need to be referred to RECs for treatment.
Qualitative data and its contribution to the flowchart
Approximately 120 e-mails were sent to the coordinators of HC in Florianópolis. Six HC declined to participate, and ten HC agreed. Two were excluded from the final analysis due to unpredicted events occurring on the spot (lack of professionals), totaling eight HC and eight FHS interviewed. We interviewed 37 FHS professionals-−12 community health agents, 10 nurses, 10 physicians, two nurse residents, two medical residents, and one dentist.
The results of the interviews presented in Table 1 and it shows that professionals have little experience in treating people with PD. In their view, referring people with PD to the neurologist's assessment (specialized care) should be one of the main approaches. However, despite knowing the referral protocol, most have never done it, as they claim not to receive high demand from people with PD who seek the service for specific disease treatment. Also, the lack of PD referral protocols for other services is one of the barriers in caring for these people at this level of care.
Medical practitioners report that the correct diagnosis of PD is an essential requirement for appropriate treatment. But, as it is a specific condition and not so frequent (or not correctly identified by them), they report a lack of experience in making the diagnosis. They prefer to refer them to neurologists. Thus, the proposed flowchart is intended to assist professionals with PD cases already diagnosed and confirmed by specialized neurologists. In addition, the lack of experience of these professionals also hampers the recognition of clinical signs and symptoms (such as the frequency of falls) that can be used to indicate/recommend activities and trigger referral to other professionals (such as physiotherapists and physical educator professionals)
FHS professionals recognize the need for multidisciplinary care and, likewise, the need to refer people with PD to other professionals and activities offered by PC. When they do, the activities usually indicated are physical exercise, pain support, psychological support, nutrition groups, dance groups, walking groups, speech therapy, among others that occur within the HC. Usually, these groups are carried out by professionals in the indicated area. Some teams also refer people with PD to multidisciplinary services outside the HC, although most report not being aware of these services.
Some professionals interviewed also believe that their role in treating people with PD is related to support / adjustment of medications and providing documents (medical certificates, expert / judicial reports, request for exams, and consultations). In their perception, most people with PD use the service for renewing medical prescriptions for their disease control, failing to other possible treatments. In this way, the flowchart can help professionals visualize what is available in the primary health care network and quickly refer people with PD to multidisciplinary services.
The referral flowchart based on the risk of falls—how does it work?
Flowcharts are practical tools for patient assessment, maintenance, and management; thus, they assist the health professional with the management and care proposal (involving risk and vulnerability assessment) (48) This flowchart is a suggestion to direct the FHS teams in the PC and enhance the quality of care offered to people with PD (Figure 1).
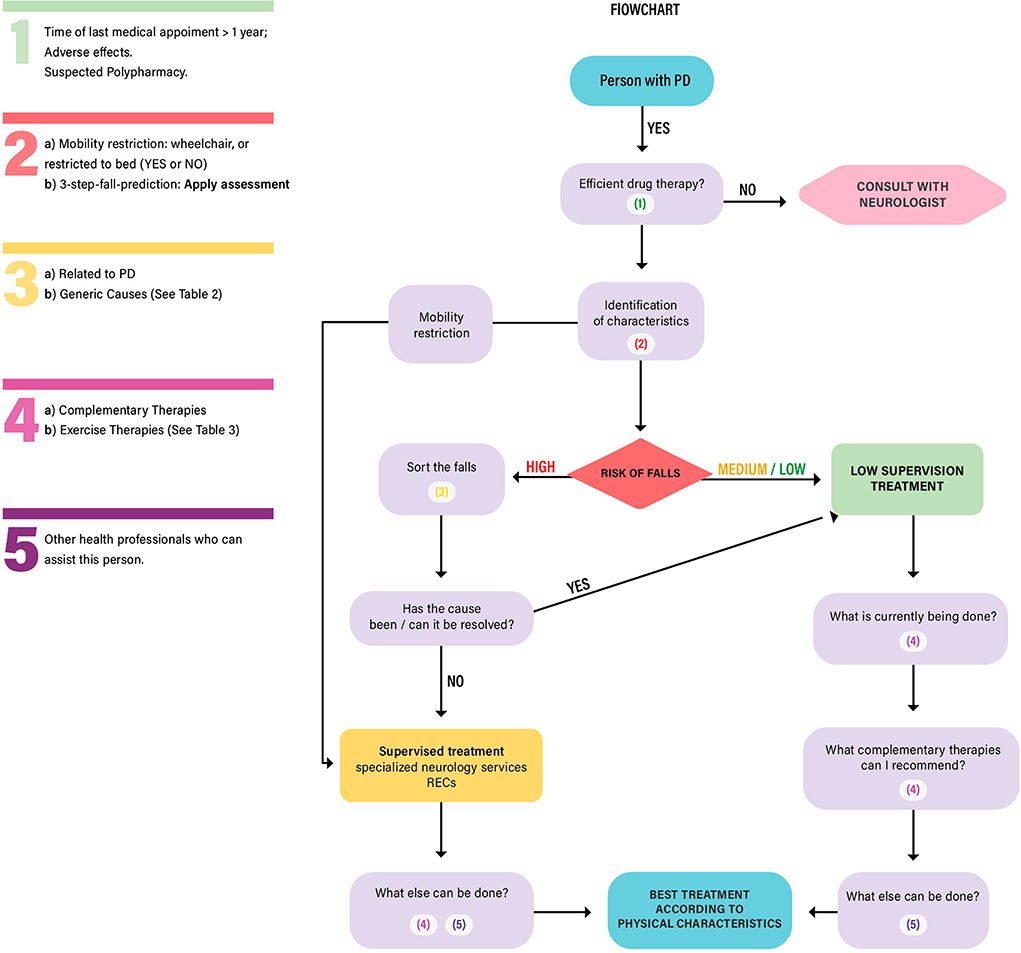
Figure 1. Elaborated by the authors. RECs: Specialized Rehabilitation Centers. PD: Parkinson's Disease.
The following tables must be used within the referral flowchart. The Table 2 is a 3-step-fall-prediction test (46, 47). This test is crucial for performing the flowchart. The evaluator should take the measurements, mark which option the person fits, and then continue with the flowchart.
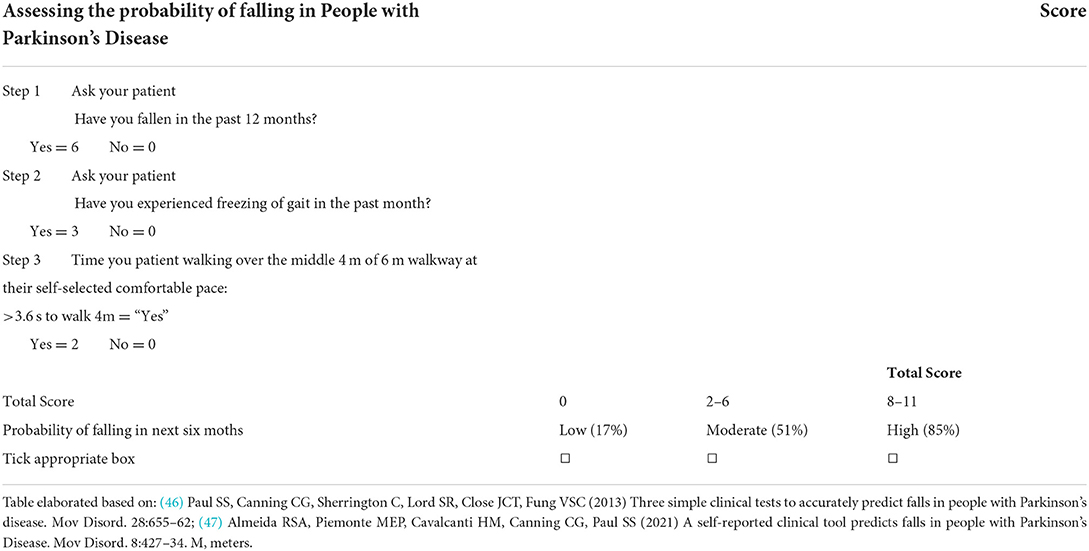
Table 2. 3-Step-fall-prediction.
After performing the test, and in case of falls, the health professionals should go to Table 3, which refers to PD's fall classification (40), based on modifiable and non-modifiable factors. Modifiable factors may be related to an inappropriate environment - for example, the person's type of shoe can be switched to a safer option that avoids falls. Another example is the high dosage of levodopa or polypharmacy. In this case, the person can be referred to a pharmacist or neurologist to update the medication. Non-modifiable factors may be related to genetic factors (gender), disease severity, among others (40). From that table, the evaluator can check the possible reasons for the falls, manage them, or refer to specialized neurology services, which offer a supervised physiotherapy approach.
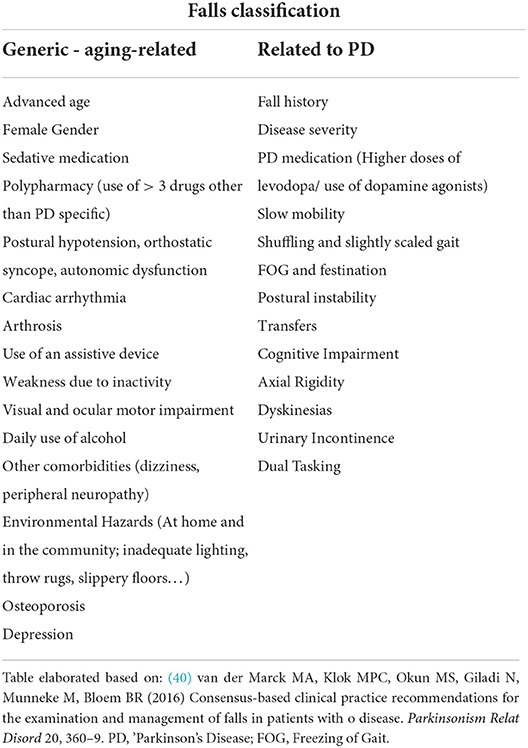
Table 3. Fall classification in Parkinson's disease.
Table 4 refers to complimentary and exercise therapies indicated for people with PD. (31, 40).
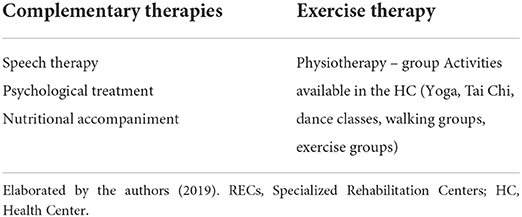
Table 4. Complementary and exercise therapy for people with PD.
Conclusion
This study aimed to develop a referral flowchart based on the risk of falls for people with PD at the Brazilian PC. Brazil does not require mandatory reporting of PD. However, the Brazilian population of 60 years of age and over (approx. 28 million) and the increasing life expectancy of Brazilians suggest that PD and resulting falls are a significant health issue for older people.
We suggest that this flowchart might be the first step to build a multidisciplinary approach for people with PD in PC in Brazil. The next stage of this study might be the validation and subsequent implementation of the flowchart through PC at the UHS in Brazil.
Limitations and future directions
Although prevention and management of falls of people with PD emerge in the qualitative research, we did not address specific questions for the FHS teams in the qualitative interview about this subject. Another limitation of our study was that we did not address the cognitive issues of people with PD. And this can influence the rate of falls in this population, so this must be considered when using the flowchart.
Also, the quality and quantity of the services offered at the PC varies among Brazilian regions. Like any standard, this flowchart cannot be taken as an absolute character, even if it applies to many situations. Therefore, a pilot study is needed for further improvements and to warrant the implementation in different regions.
As future directions, continuing education programs must be offered to health professionals at Primary Care. These professionals are the first contact with the PD patients through the Brazilian Health System. Hence, knowing how to identify, treat, and refer a person with PD could improve the quality of care and potentially increase the quality of life of those who live with the disease. Also, to use the flowchart its validation must occur, so the next step of this study might be its validation through the Primary Care at Unified Health System in Brazil.
Data Availability Statement
The raw data supporting the conclusions of this manuscipt will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee for Human Beings of the State University of Santa Catarina. The patients/participants provided their written informed consent to participate in this study.
Author contributions
RSM, ECG, AS, and MHALK contributed to conception and design of the study. RSM organized the database, performed the statistical analysis, and wrote the first draft of the manuscript. AS and MHLAK revised the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Acknowledgments
We would like to acknowledge Florianópolis city hall and the health department and all the professionals of FHS. They made their time available and shared their opinions and knowledge with the researchers.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Canning CG, Paul SS. Nieuwboer. A prevention of falls in Parkinson's disease: a review of fall risk factors and the role of physical interventions. Neurodegenener Dis Manag. (2014) 4:203–21. doi: 10.2217/nmt.14.22
2. Kerr GK, Worringham CJ, Cole MH, Lacherez PF, Wood JM, Silburn PA. Predictors of future falls in Parkinson's disease. Neurology. (2010) 75:116–24. doi: 10.1212/WNL.0b013e3181e7b688
3. Voss TS, Elm JJ, Wielinski CL, Aminoff MJ, Bandyopadhyay D, Chou KL, et al. Fall frequency and risk assessment in early Parkinson's disease. Parkinsonism Relat Disord. (2012) 18:837–41. doi: 10.1016/j.parkreldis.2012.04.004
4. Luquin MR, Kulisevsky J, Martinez-Martin P, Mir P, Tolosa ES. Consensus on the definition of advanced Parkinson's disease: a neurologists-based delphi study (CEPA Study). Parkinsons Dis. (2017) 2017:4047392. doi: 10.1155/2017/4047392
5. Bloem BR, Grimbergen YA, Cramer M, Willemsen M, Zwinderman AH. Prospective assessment of falls in Parkinson's disease. J Neurol. (2001) 248:950–8. doi: 10.1007/s004150170047
6. Temlett JA, Thompson PD. Reasons for admission to hospital for Parkinson's disease. Intern Med J. (2006) 36:524–6. doi: 10.1111/j.1445-5994.2006.01123.x
7. Wielinski CL, Erickson-Davis C, Wichmann R, Walde-Douglas M, Parashos SA. Falls and injuries resulting from falls among patients with Parkinson's disease and other parkinsonian syndromes. Mov Dis. (2005) 20:410–5. doi: 10.1002/mds.20347
8. Macleod AD, Taylor KS, Counsell CE. Mortality in Parkinson's disease: a systematic review and meta-analysis. Mov Disord. (2014) 29:1615–22. doi: 10.1002/mds.25898
9. Abreu DROM, Novaes ES, Oliveira RR, Mathias TAF, Marcon SS. Internação e mortalidade por quedas em idosos no Brasil: análise de tendência. Ciênc Saúde Colet. (2018) 23:1131–41. doi: 10.1590/1413-81232018234.09962016
10. Grimbergen Y, Munneke M, Bloem B. Falls in Parkinson's disease. Curr Opin Neurol. (2004) 17:405–15. doi: 10.1097/01.wco.0000137530.68867.93
11. Gu Y, Denni SM. Are falls prevention programs effective at reducing the risk factors for falls in people with type-2 diabetes mellitus and peripheral neuropathy: a systematic review with narrative synthesis. J Diabetes Complications. (2017) 312:504–16. doi: 10.1016/j.jdiacomp.2016.10.00
12. Wettasinghea AH, Dissanayake DWN, Allet L, Katulanda P, Lord SR. Falls in older people with diabetes: identification of simple screening measures and explanatory risk factors. Prim Care Diabetes. (2020) 14:723–8. doi: 10.1016/j.pcd.2020.05.006
13. Anam AK, Insogna K. Update on osteoporosis screening and management. Med Clin North Am. (2021) 105:1117–34. doi: 10.1016/j.mcna.2021.05.016
14. Ang GC, Low SL, How CH. Approach to falls among the elderly in the community. Singapore Med J. (2020) 61:116–21. doi: 10.11622/smedj.2020029
15. Kessler D, Hauteclocque J, Grimes D, Mestre T, Côtéd D, Liddy C. Development of the integrated Parkinson's care network (IPCN): using co-design to plan collaborative care for people with Parkinson's disease. Qual Life Res. (2019) 28:1355–64. doi: 10.1007/s11136-018-2092-0
16. Rajan R, Brennan L, Bloem BR, Dahodwala N, Gardner J, Goldman JG, et al. Integrated care in Parkinson's disease: a systematic review and meta-analysis. Mov Disord. (2020) 35:1509–31. doi: 10.1002/mds.28097
17. Brasil. Portaria no 1.559, de 10 de agosto de 2008. Institui a Política Nacional de Regulação do Sistema Único de Saúde – SUS. Ministério da Saúde (2008). Available Online at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2008/prt1559_01_08_2008.html (accessed January 29, 2020).
18. Lana RC, Lopes LKR, Cardoso F, Lindquist ARR, Piemonte MEP, et al. Determinants of the use of physiotherapy services among individuals with Parkinson's disease living in Brazil. Arq Neuro-Psiquiatr. (2018) 76:592–8. doi: 10.1590/0004-282X20180087
19. Fasano A, Canning CG, Hausdorff JM, Lord S, Rochester L. Falls in Parkinson's disease: a complex and evolving picture. Mov Disord. (2017) 32:1524–36. doi: 10.1002/mds.27195
20. Shen X, Wong-Yu ISK, Mak MKY. Effects of exercise on falls, balance, and gait ability in Parkinson's disease: a meta-analysis. Neurorehabil Neural Repair. (2016) 30:512–27. doi: 10.1177/1545968315613447
21. Qmar MA, Harington G, Trump S, Johnson J, Roberts F, Frost E. Multidisciplinary care in Parkinson's disease. Int Rev Neurobiol. (2017) 132:511–23. doi: 10.1016/bs.irn.2017.02.001
22. IBGE – Instituto Brasileiro de Geografia e Estatística (2020). Available Online at: https://www.ibge.gov.br/cidades-e-estados/sc/florianopolis.html (accessed July 5, 2020).
23. Florianópolis. Protocolo de atenção à saúde do idoso. Editora Copiart, Tubarão. (2010). Available Online at: http://portal.pmf.sc.gov.br/arquivos/arquivos/pdf/14_05_2012_8.47.51.ea16b1f5291407e4d39d30837dfc2809 (accessed July 05, 2020).
24. Tong A, Sainsbury P, Grayg J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
25. Keus SHJ, Munneke M, Graziano M, Pelosin E, Domingos J, Bruhlmann S, et al. European Physiotherapy Guideline for Parkinson's Disease. KNGF/ParkinsonNet. (2014).
26. Kalf JG, de Swart BJM, Bonnier M, Hofman M, Kanters J, Kocken J, et al. Guidelines for Speech-Language Therapy in Parkinson's Disease. Miami, FL: ParkinsonNet. (2011).
27. Sturkenboom I, Thijssen M, Elsacker JG, Jansen I, Maasdam A, Schulten M, et al. Guidelines for Occupational Therapy in Parkinson's Disease Rehabilitation. ParkinsonNet. (2018).
28. van Asseldonk MJMD, Dicke HC, van den Beemt BJW, van den Berg DJ, ter Borg S, Duin GM, et al. Dietetics Guideline for Parkinson's Disease. The Hague. Lemma Publisher (2012).
29. Robinson K, Picton R, Harries S, Bruce A. Best practice guideline for dietitians on the management of Parkinson's. BDA consensus on the nutritional management of Parkinson's (2021). Available Online at: https://www.parkinsons.org.uk/sites/default/files/2017-12/dietitians_bestpracticeguideline.pdf (accessed February 22, 2021).
30. Bloem BR, Van Laar T, Keus SHJ, De Beer H, Poot E, Buskens E, et al. Multidisciplinaire Richtlijn Ziekte van Parkinson. Alphen aan den Rijn: Van Zuiden Communications (2010).
31. van der Marck MA, Bloem BR. Borm GF, Overeem S, Munneke MP, Guttman M. Effectiveness of multidisciplinary care for Parkinson's disease: a randomized, controlled trial. Mov Disord. (2013) 28:605–11. doi: 10.1002/mds.25194
32. Tomlinson CL, Patel S, Meek C, Herd CP, Clarke CE, Stowe R, et al. Physiotherapy versus placebo or no intervention in Parkinson's disease. Cochrane Database Sys Rev. (2013) 10:1–111. doi: 10.1002/14651858.CD002817.pub4
33. Uhrbrand A, Stenager E, Pedersen MS, Dalgas U. Parkinson's disease and intensive exercise therapy- A systematic review and meta-analysis of randomized controlled trials. J Neurol Sci. (2015) 353:9–19. doi: 10.1016/j.jns.2015.04.004
34. Wu PL, Lee M, Huang TT. Effectiveness of physical activity on patients with depression and Parkinson's disease: a systematic review. PLoS ONE. (2017) 12:1–14. doi: 10.1371/journal.pone.0181515
35. Ahlskog JE. Aerobic exercise: evidence for a direct brain effect to slow Parkinson disease progression. Mayo Clin Proc. (2018) 93:360–72. doi: 10.1016/j.mayocp.2017.12.015
36. Brasil. Constituição da República Federativa do Brasil. Brasí; Senado Federal (1988). Available Online at: https://www2.senado.leg.br/bdsf/bitstream/handle/id/518231/CF88_Livro_EC91_2016.pdf (accessed January 12, 2020).
37. Brasil. Portaria no 1.161, de 07 de Julho de 2005. Institui a Política Nacional de Atenção ao Portador de Doença Neurológica, a ser implantada em todas as unidades federadas, respeitadas as competências das três esferas de gestão. Governo Federal Do Brasil (2005). Available Online at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2005/prt1161_07_07_2005.html (accessed March 12, 2020).
38. Brasil. Portaria Conjunta N° 10, de 31 de Outubro de 2017. Aprova o Protocolo Clínico e Diretrizes Terapêuticas da Doença de Parkinson (2017). Available Online at: http://portalarquivos2.saude.gov.br/images/pdf/2017/novembro/14/Portaria-Conjunta-PCDT-Doenca-de-Parkinson.pdf (accessed March 12, 2020).
39. Kader M, Iwarsson S, Odin P, Nilsson MH. Fall-related activity avoidance in relation to a history of falls or near falls, fear of falling and disease severity in people with Parkinson's disease. BMC Neurol. (2016) 2:16–84. doi: 10.1186/s12883-016-0612-5
40. van der Marck MA, Klok MPC, Okun MS, Giladi N, Munneke M, Bloem BR. Consensus-based clinical practice recommendations for the examination and management of falls in patients with o disease. Parkinsonism Relat Disord. (2016) 20:360–9. doi: 10.1016/j.parkreldis.2013.10.030
41. Ellis T, Rork T, Dalton DD, Venne J. Be active & beyond: a guide to exercise and wellness for people with Parkinson's disease. American Parkinson Disease Association (2016). Available Online at: https://www.apdaparkinson.org/wp-content/uploads/pdf_publications/Be-Active-Book_For-Web-90o.pdf (accessed December 11, 2020).
42. Flach A, Jaegers L, Krieger M, Bixler E, Kelly P, Weiss EP, et al. Endurance exercise improves function in individuals with Parkinson's disease: a meta-analysis. Neurosci Lett. (2017) 659:115–9. doi: 10.1016/j.neulet.2017.08.076
43. Yang Y, Wang Y, Zhou Y, Chen C, Xing D, Wang C. Validity of the functional gait assessment in patients with Parkinson disease: construct, concurrent, and predictive validity. Phys Ther. (2014) 94:392–400. doi: 10.2522/ptj.20130019
44. Benka Wallén M, Sorjonen K, Löfgren N, Franzén E. Structural validity of the mini-balance evaluation systems test (mini-BESTest) in people with mild to moderate Parkinson disease. Phys Ther. (2016) 96:1799–806. doi: 10.2522/ptj.20150334
45. Duncan RP, Cavanaugh JT, Earhart GM, Ellis TD, Ford MP, Foreman KB, et al. External validation of a simple clinical tool used to predict falls in people with Parkinson disease. Parkinsonism Relat Disord. (2015) 21:960–3. doi: 10.1016/j.parkreldis.2015.05.008
46. Paul SS, Canning CG, Sherrington C, Lord SR, Close JCT, Fung VSC. Three simple clinical tests to accurately predict falls in people with Parkinson's disease. Mov Disord. (2013) 28:655–62. doi: 10.1002/mds.25404
47. Almeida LR, Piemonte MEP, Cavalcanti HM, Canning CG, Paul SS. A self-reported clinical tool predicts falls in people with Parkinson's Disease. Mov Disord Clin Pract. (2021) 8:427–34. doi: 10.1002/mdc3.13170
48. Brasil. Humanized reception of patients without an appointment: the most common complaints in spontaneous demand of basic attention. Cad Aten Básica. (2013) 28:1–56. Available online at: https://bvsms.saude.gov.br/bvs/publicacoes/acolhimento_demanda_espontanea_queixas_comuns_cab28v2.pdf (accessed February 22, 2021).
Keywords: Parkinson's disease, workflow, community health planning, primary health care, South America, Brazil
Citation: Myra RS, Koerich MHAdL, Gregório EC and Swarowsky A (2022) Primary care for people with Parkinson's disease in Brazil: A referral flowchart based on risk of falls. Front. Public Health 10:836633. doi: 10.3389/fpubh.2022.836633
Received: 15 December 2021; Accepted: 29 June 2022;
Published: 25 July 2022.
Edited by:
Iva Stankovic, University of Belgrade, SerbiaReviewed by:
Naoya Hasegawa, Hokkaido University, JapanLiza Das, Post Graduate Institute of Medical Education and Research (PGIMER), India
Copyright © 2022 Myra, Koerich, Gregório and Swarowsky. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandra Swarowsky, YWxlc3NhbmRyYS5zd2Fyb3dza3ltYXJ0aW5AYWh1LmVkdQ==
†These authors share first authorship
‡Senior author