 Gerrit Stassen
Gerrit Stassen Lukas Baulig
Lukas Baulig Andrea Schaller
Andrea Schaller
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 25 March 2022
Sec. Occupational Health and Safety
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.832523
This article is part of the Research TopicWorkplace Health Promotion, Volume IIView all 14 articles
Background: The workplace is an important setting for adult health promotion including exercise training such as resistance training (RT). Since the reporting of exercise training interventions is generally inconsistent, the objective of this systematic review was to investigate the attention to principles of RT progression and variables of RT exercise prescription in workplace-related RT interventions.
Methods: A systematic literature search was conducted in the databases LIVIVO, PubMed, SPORTDiscus, and Web of Science (2000–2020). Controlled trials with apparently healthy “employees” and a main focus on RT were included. RT principles and variables were extracted and rated by two reviewers (reported, not reported, or unclear). Sum scores for each RT intervention and percentages regarding each principle and variable were calculated.
Results: Overall, 21 articles were included (18 primary studies, 3 protocols). Summarized narratively, the interventions showed different positive effects on strength- or performance-related and/or health- or complaint-related outcomes. The reporting of the RT principles and variables was varied [progressive overload: 94% of the studies, specificity: 78%, variation (periodization): 39%, muscle action: 94%, loading: 94%, volume; 67%, exercise selection: 89%, exercise order: 47%, rest periods between sets: 33%, rest periods between exercises: 27%, repetition velocity: 44%, and frequency: 100%].
Conclusion: Several key RT principles and variables were reported inconsistently, reducing reproducibility and pointing to the need for standardized RT intervention reporting in workplace-related interventions. Exercise science and workplace promotion should be further linked, since accurate reporting is a prerequisite for transferring robust findings into practice.
For years, the workplace has developed into an important setting regarding adult health promotion, as it is one setting of everyday life where health is created and lived (1). Since working adults spend almost half of their waking hours at work (2), large and diverse groups of the population can be reached there. Accordingly, the workplace also offers an environment for health-promoting exercise training (3).
In general, the multiple positive health benefits of physical activity (PA) and fitness training are well documented (4–8). In this respect, workplace-related PA interventions conducted directly at the workplace and, where appropriate, also during working hours, have shown positive effects on, e.g., activity behavior, physical fitness and cardio-metabolic health, musculoskeletal disorders, and the prevention of work-related pain (9–13). They improve overall well-being and work ability, reduce sickness absenteeism and sick leave, and can generate a positive financial return (14–16).
Besides the general health-promoting effects of PA, scientific findings emphasize the independent positive effects of resistance training (RT) on health (17, 18). RT attenuates the age-related decrease in muscle mass and strength (19, 20), improves health-related quality of life (21), and there is an inverse association of muscular strength and fitness with all-cause mortality, even after adjusting for cardiorespiratory fitness or proven risk factors (22–25). Considering the workplace setting, the “medicine” RT (26, 27) shows inter alia positive effects on physical (e.g., pain reduction) and work-related (e.g., productivity) factors of employees (28–33).
However, the mode of exercise training seems to be decisive for achieving positive effects, which is why optimal planning is essential (33). The proper application of training principles leads to improvements of components of fitness or health through physical adaptions. In order to optimize effectiveness so that improvements occur, targeted (resistance) training is supposed to be designed according to basic principles (34–36). A RT program should be systematically altered according to the foremost principles of RT progression to make the body adapt to changing stimuli: progressive overload, specificity, and variation (periodization) (37, 38). Furthermore, proper RT exercise prescription involves several key variables: muscle action, loading, volume, exercise selection, exercise order, rest periods between sets and exercises, repetition velocity, and frequency (37–39). Nevertheless, systematic reviews show that the application and reporting of principles and guidelines of exercise training is inconsistent and could be improved in intervention studies in general (40–45) and in RT studies in particular (46–48).
Given the great potential of workplace-related interventions to reach diverse adult target groups in the context of health promotion, RT interventions in this setting should be reported as comprehensively as possible to facilitate replicability and thus transfer of promising approaches. Thus, based on the outlined state of research, the question of this systematic review was: How are the principles of RT progression and variables of RT exercise prescription applied in studies involving workplace-related RT interventions?
This systematic review was conducted in accordance with the PRISMA-recommendations (49, 50).
The studies were selected according to the PICOS criteria (participants, interventions, comparators, outcomes, study design) (50) as well as setting, language and time frame.
Intervention studies with apparently healthy “employees” (defined as working-age adults in full- or part-time-employment) without restrictions regarding sex or job/type of occupation were taken into account, while studies with specific patient populations or populations focusing on specific diseases or comorbidities were not. To be included, studies must have examined an intervention with at least one study arm with main focus on RT (mentioned in the rationale, hypothesis and/or methods section) conducted within the workplace-context and/or at the workplace (“workplace-related”) and had other training forms included for warm-up or cool-down only. Studies with alternative PA interventions without a main RT focus (general fitness training, other training forms, mixed PA interventions) and multicomponent interventions were excluded. Due to the review focus, no restrictions were placed on the comparison groups (no intervention, non-RT intervention, minimal intervention, waitlist control etc.) and the outcome measurements.
Therefore, any prospective research study (experimental design) with a workplace-related RT intervention and a comparator group [randomized controlled trials (RCTs), Cluster RCTs, controlled trials] with no limitation on the length of the intervention or a follow-up was considered. RCTs are generally the most powerful experimental design but to include them alone may be too restrictive to investigate workplace-related RT interventions as many studies occur in naturalistic workplace settings where RCTs are not always possible (51). The language limitation was English or German and the time limitation was from January 2000 to December 2020 due to past developments in the field of health promotion and especially workplace health promotion [e.g., Jakarta Declaration on Leading Health Promotion into the 21st Century (52) and Luxembourg Declaration on Workplace Health Promotion (53)].
A computerized systematic literature search was conducted in LIVIVO, PubMed, SPORTDiscus, and Web of Science at the end of January 2021. Search terms related to workplace interventions (e.g., “worker*,” “employe*,” and “workplace”), RT (e.g., “resistance,” “weight,” or “strength” and “training” or “exercise”) and controlled trials (e.g., “controlled study” OR “RCT”) were used with operators (“OR,” “AND,” and “NOT) and truncations (“*”) with appropriate adjustments for each database (Supplementary Table 1).
Articles were imported into the literature management program Rayyan (54). After removing all duplicates, two reviewers (GS and LB) independently screened all titles/abstracts in a first step and full texts in a second step based on the inclusion/exclusion criteria. Any disagreements were resolved by consensus or consulting with a third reviewer (OM). If the full texts were secondary analyses, the corresponding primary studies were additionally searched for and included instead (if eligible and not already included). If underlying study protocols were mentioned, these were additionally used for data collection regarding the RT intervention.
On a first constructed form, the following study characteristics were extracted: name of first author and year, study design, study sample [including occupation description, baseline sample size, sex, and age (years)], RT intervention (general description of all study interventions and period, frequency and duration, location, and supervision of the RT study arm). In addition, significant effects of the included RT interventions were listed with respect to the control group with a focus on the intervention period only (without considering possible follow-ups).
Using a second constructed form, principles of RT progression (37, 38) and variables of RT exercise prescription (37–39) were extracted from the methods sections of the included articles or additionally from the underlying study protocols, respectively, and rated independently by two reviewers (GS and LB) according to the working understandings (Tables 1, 2). Principles and variables were rated as follows: yes (+) “reported/applied,” no (−) “not reported/not applied,” or unclear (?) if it was unclear or inconsistent whether a principle/variable was reported/applied. “Not applicable” (na) was recorded for “exercise order” and “rest between exercises” if only one exercise was used and for “rest between sets” if only single sets were used. Disagreements were resolved through personal communication or consulting with a third reviewer (OM).
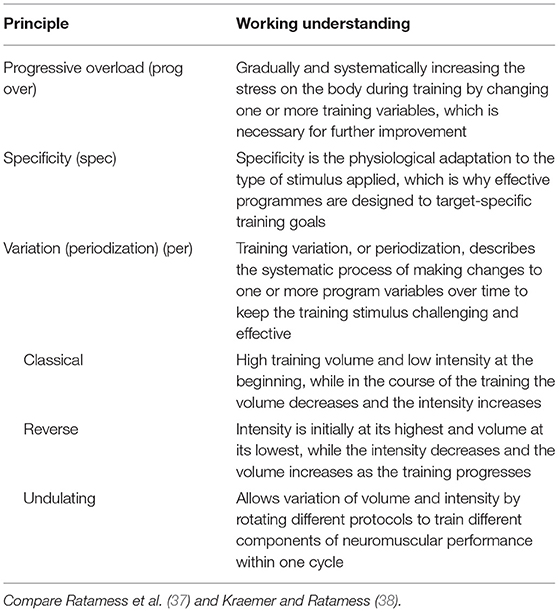
Table 1. Principles of resistance training progression (working understandings).
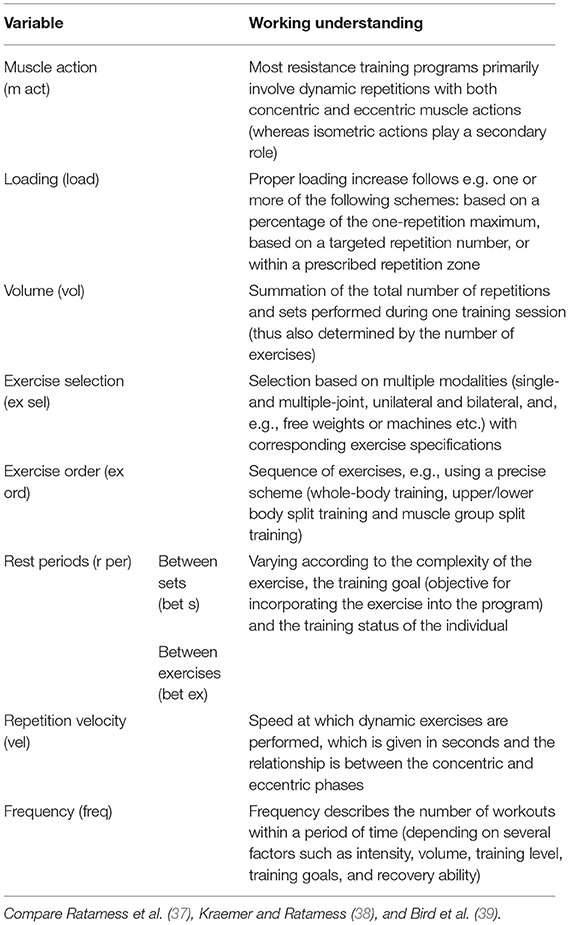
Table 2. Variables of resistance training exercise prescription (working understandings).
All included studies were subjected to the Effective Public Health Practice Project's (EPHPP) quality assessment tool for quantitative studies (55, 56). Two reviewers (LB and OM) independently assessed the quality of the studies reaching consensus through discussion [consulting a third reviewer in case of uncertainties (GS)]. According to the EPHPP dictionary (57), the first six components were included in the assessment (selection bias, study design, confounders, blinding, data collection methods, and withdrawals and dropouts) and rated as weak, moderate or strong. Since it is impossible to blind participants and instructors in RT studies, blinding according to the EPHPP is assessed on two levels: whether the outcome assessor(s) were aware of the intervention or exposure status of participants and whether the study participants were aware of the research question (55). The assessment is based on the extent to which both, one or none are fulfilled (57).
The significant effects of the study arm(s) with RT in the intervention studies (pre-post, compared to the control group) were summarized narratively.
Reported/applied (+) principles of RT progression and variables of RT exercise prescription were given a score of “1,” not reported/not applied (−) and unclear (?) a “0,” and not applicable (na) no score. Sum scores of progression principles and exercise prescription variables were calculated and corrected for the number of “na.” Percentages of RT intervention descriptions reporting/applying each principle and variable were also calculated (proportion relative to the total number).
The systematic search resulted in 7.427 articles and after removing duplicates and screening titles/abstracts a total of 105 potentially relevant articles were assessed for eligibility. Based on the full-text assessments, 1 additional primary study and 3 study protocols were added, resulting in 21 articles remaining for the qualitative synthesis (18 studies, 3 protocols) (Figure 1).
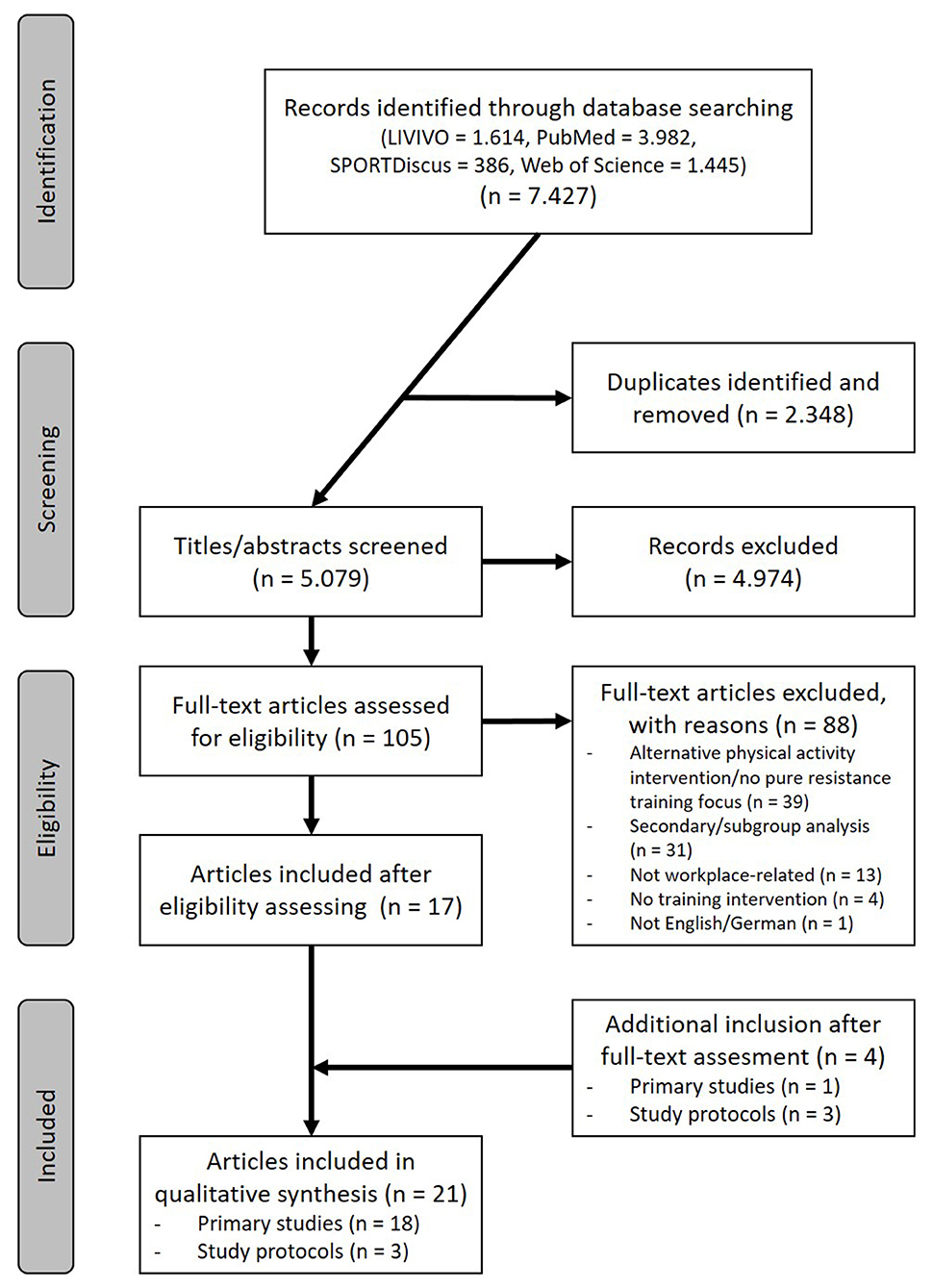
Figure 1. Flow diagram illustrating the search and selection process.
Table 3 presents the characteristics of the 18 included primary studies. The majority were RCTs [9 studies (58, 59, 64–67, 69, 70, 73, 74)] and another described as feasibility study (71). Furthermore, there was one non-randomized CT (62) and 6 cluster RCTs (60, 61, 63, 68, 72, 75), with 2 each evaluating a subgroup of the intervention groups in an overarching study (60, 63).
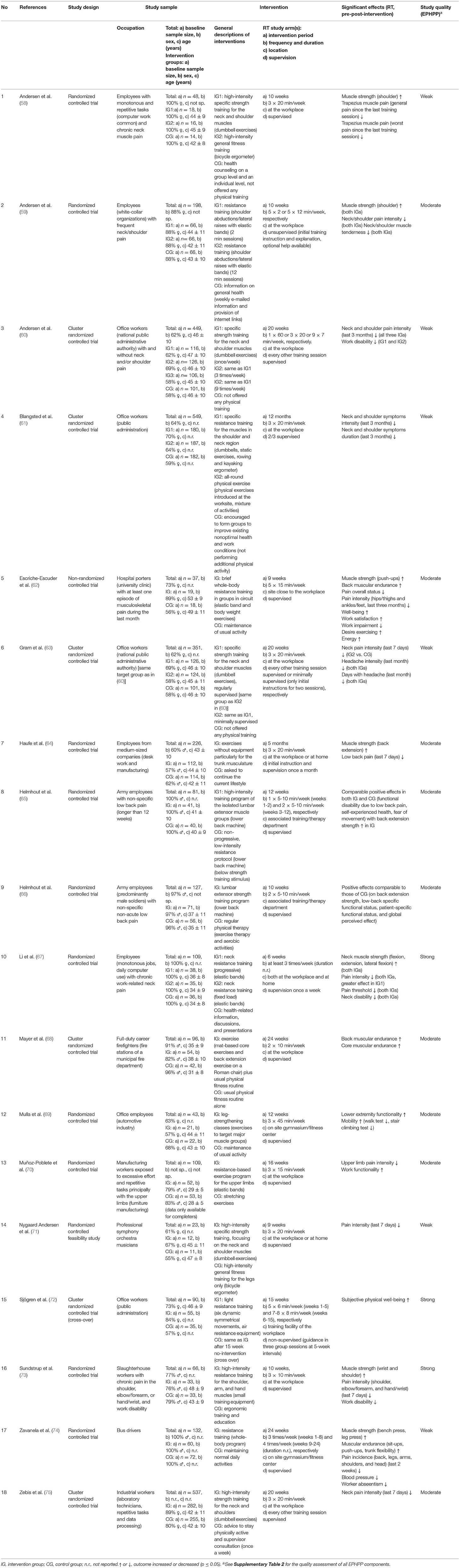
Table 3. Included primary studies.
The target groups were diverse in terms of types of occupation, with employees in inactive work environments (e.g., white collar/office desk work, laboratory technicians), physically active jobs (hospital porters, firefighters, army employees, musicians) or also blue collar workers (manufacturing, slaughterhouse, bus drivers). Some studies specified eligible participants in terms of health status or physical complaints (e.g., neck/shoulder or low back pain) whereas others targeted employees generally. The baseline sample size in the studies ranged from 23 (71) to and 549 (61) participants, with four studies including females only (58, 67) or predominantly females (>80%) (59, 75) and 5 studies males only (65, 74) or predominantly males (66, 68, 70), respectively. The majority of studies had, on average, middle-aged samples.
The RT interventions used different materials or equipment, such as dumbbells, elastic bands or machines, in different organizational forms [ranging from, e.g., training consisting of only one exercise or even one single set (59, 65, 66) to circuit training in groups (62)] with the sessions being supervised to varying extents (fully, alternating to minimal, and not at all). The majority of studies were conducted directly at the workplace, although three studies had the option of exercising at home (64, 67, 71). Interventions that included training in groups and/or used larger equipment took place in associated training/therapy departments (65, 66) or in fitness centers/training facilities within the workplace (69, 72, 74) or in close proximity (62), respectively. The intervention periods were between 6 weeks (67) and 12 months (61) with a frequency of at least 1-2 times/week (60, 65) up to sometimes several times/day (60, 72), with most interventions conducting RT 2-3 times/week.
Overall, with 9 out of 18 studies, the majority of studies were rated as moderate (59, 62, 64–66, 68–70, 75), six studies were again rated as weak (58, 60, 61, 63, 71, 74), and the remaining three studies were rated as strong (67, 72, 73) (Table 3). In summary, study design and data collection methods were rated as the strongest across all studies, while the distribution of the other components was more varied (weak/moderate/strong) (Supplementary Table 2).
Within the workplace-related RT interventions, different positive effects (pre-post-intervention) were reported (Table 3).
Significant improvements in (muscular) strength- or performance-related outcomes as a result of RT intervention were reported in 10 studies. Upper limb strength (neck, shoulder, or wrist) after an specific RT program was examined in four studies (58, 59, 67, 73). Comparable to this, four studies examined the strength/endurance of the back or trunk (64–66, 68). The other two studies performed multi-joint exercises to assess strength/performance effects to correspond to the whole-body training conducted in the interventions (62, 74).
Significant improvements regarding pain- or complaint-related outcomes were reported in 13 studies. Most frequently, the intensity and/or duration of neck or upper back/limb pain or headache was examined (eight studies) (58–61, 63, 70, 73, 75), often using variants of a visual analog scale. The other studies assessed either complaints in the lower back or lower extremities or a general pain condition without specifying more precisely the body region (62, 64, 67, 71, 74).
Further different outcomes assessed for which significant improvements were shown included muscle tenderness (59), functional status or mobility (65, 66, 69), well-being (62, 72), work-related outcomes such as disability, functionality, satisfaction, impairment, or abseentism (60, 62, 70, 73, 74).
In two studies, pre-post improvements also occurred in the control groups, as these were a comparison with regular physiotherapy (66) or a comparison with low-intensity strength training, respectively, although in the latter study, only the high-intensity intervention group also showed significant effects regarding strength (65).
The rating of the RT interventions in terms of attention to principles of progression and variables of exercise prescription is listed in Table 4 and reported in detail in Supplementary Table 3. For the assessment, protocols could also be taken into account for 4 of the 18 primary studies, as one protocol (76) refers to the two aforementioned studies that each evaluate a subset of the intervention groups in an overarching study (60, 63).

Table 4. Application of principles of progression and variables of exercise prescription.
Overall, 70 % of the principles of RT progression (Table 1) were reported in the included studies (38/54), ranging from 1 to 3 principles with 6 of the 18 studies reporting all 3 principles (58, 60, 63, 71, 73, 75) (Table 4). The principle of progressive overload was explicitly stated in all but one study (94%, 17/18). Specificity, in turn, was documented for 78% (14/18), whereby the four studies classified as “unspecific” were rated as “unclear” as they reasoned whole-body trainings with its impact on, among other things, musculoskeletal pain (62), subjective physical well-being (72) or absenteeism (74), or investigated a specific osteoarthritis training in a general target group (69). The least documented principle is variation understood as systematic variation of both intensity and volume over the course of training (periodization) (Table 1) with 39% (7/18) describing classical (58, 62, 71, 73) or classical/undulating (60, 63, 75) models, respectively. Two studies were rated as unclear because in the first case, training was only performed at a lower intensity and a higher volume in the first 2 of the 12 intervention weeks and the change after week 3 does not appear to be systematic (65) [moreover, the same research group did not apply any periodization in another included subsequent study (66)] and in the second case, although an increase in volume is indicated to some extent by increased duration and number of repetitions, no change in intensity is described (69).
Overall, 69% of all variables of resistance training exercise prescription (Table 2) were reported in the included studies (103/150, corrected for the number of “not applicable”) (Table 4). The variable muscle action is reported in 94% (17/18), describing concentric, eccentric as well as isometric muscle action, with the only missing studies most likely using dynamic exercises but not explicitly stating this (74). Loading is applied in 94% (17/18) and was predefined as, e.g., prescribed repetition range for an exercise or a session (59, 65, 66, 68), as a percentage of a certain repetition maximum or the maximal strength (58, 60–63, 67, 71, 73–75), based on a rating of perceived exertion (69, 72), or as a fixed weight during a defined intervention phase (70). The only “unclear” study indicated load adjustments by therapists on site without explaining the procedure in more detail (64). The training volume, which can be recognized by an indication of the number of exercises, sets and repetitions, was given in 67% (12/18). The exercise selection was named in 89% (16/18) of the studies, while the exact exercise order was only clearly described in 47% (7/15) (corrected for single exercise interventions), as in some cases it remained unclear whether the order or numbering in the article texts remained the same throughout the intervention phase. Corrected for single exercise interventions and single set interventions, rest periods between exercises and between sets were also reported comparatively infrequently at 33% (4/12) and 27% (4/15) respectively, which also applies to the repetition velocity (given in seconds) [44% (8/18)]. Finally, all studies 100 % (18/18) applied the frequency of the training sessions (compare also Table 3).
To the best of our knowledge, this review is the first to specifically address attention to progression principles and variables of exercise prescription in workplace-related RT interventions. The main finding of the analysis was that several important RT principles and variables were inconsistently reported. While the goal of this systematic review was not to evaluate whether general RT recommendations were followed, the results do highlight some gaps in reporting (and potential for intervention planning).
The principle of progressive overload was mentioned in almost all studies indicating that there is agreement on the importance of increasing the stress to achieve adaptations and improvements. Due to the often limited time available for interventions at the workplace (79, 80), progressive overload provides the foremost basis for effective but also efficient interventions.
The principle of specificity was rated as unclear in four studies, as these (62, 69, 72, 74) used a more general training approach. Specific training should ensure that the most optimal type of exercise is chosen for a desired outcome (e.g., specific neck and shoulder training to prevent or reduce pain). Nonetheless, non-specific whole-body training could be reasoned from a primary prevention perspective since regular RT has a wide range of health-enhancing effects (17, 26, 81, 82). Depending on possibly rather broader intervention goals in the context of workplace health promotion (such as increasing well-being, reducing physical complaints, increasing or maintaining work ability), the exact specificity of RT may seem less necessary than, e.g., in rehabilitation or high-performance sports.
It is noticeable that the majority of the studies did not specify a periodization model, which not only represents a reporting gap but also a potential for intervention optimization from the perspective of exercise science. Research shows that systematic variation in both intensity and volume leads to increased adaptation over time (83–85), which is therefore relevant in recreational or health promotion contexts. Additionally, changing one or more variables over time could have a motivating effect (86) and might have a positive influence on adherence, especially in rather less training-experienced target groups in the workplace context.
Commonly reported variables of RT exercise prescription in the included studies were muscle action, load, volume, and frequency. Therefore, in general, it was reported what was exercised, how often and with what load. Especially the determination (and continuous realization) of an appropriate load is the prerequisite for training progression. Although the load is generally specified in almost all studies (Supplementary Table 3), the exact procedures for load determination often remain rather unclear. A more precise description of the protocols or test methods used, e.g., to determine the RM or the maximal strength, would increase transparency beyond the mere mention of load and provide added value in terms of practice transfer. Moreover, with regard to training conduction, it would be critical to question the extent to which study participants are able to continuously manage the load when interventions consist of (sometimes predominantly) unsupervised training sessions (59–61, 63, 64, 67, 72, 75). As an example, the included study by Andersen et al. in which the two intervention groups performed lateral raises with elastic bands (one single-set and one multi-set group) can be referred to (59). In the associated process evaluation, 40% of participants with low adherence responded, among other things, that they felt the load progression was too fast (87). Particularly in conjunction with lower adherence, this could influence the effectiveness. For workers—some of whom may have little experience with exercise training—it may be difficult to self-direct load to, e.g., predefined repetition ranges in such a way that a constant impactful stress is ensured over the course of the intervention.
The selection of exercises was usually shown in the corresponding descriptions and illustrations, while the order of the exercises remained unclear in some studies. As complex exercises were not performed in all studies, a specific sequence, e.g., multi-joint to single-joint exercises within a session (37, 39), appears negligible in some cases, although research suggests that the exercise order should be based on priority with respect to the program goal and regardless of whether the exercise involves a relatively large or small muscle group (88). However, the intervention transparency could easily be improved by a short textual reference. Moreover, the more precise implementation (rest periods between the exercises and the sets and repetition velocity) remained partly unclear. From an exercise science perspective, rest periods in particular are important for both training planning and management (89, 90). Also, rest periods are relevant from a transfer point of view, as they determine the detailed implementation in practice, and already brief descriptions (e.g., timing or autoregulatory) would facilitate intervention replication.
In summary, reporting of RT in workplace-related interventions appears inconsistent, which is in line with reviews in, e.g., rehabilitative contexts (46–48), hindering both the replication and validation of results in follow-up studies and the implementation of successful interventions. Therefore, the use of standardized exercise-reporting tools should be further encouraged. Current guidelines from the equator network, such as the consensus on exercise reporting template (CERT) (91) or the template for intervention description and replication (TIDieR) (92), provide comprehensive guidance and were developed to address the issues outlined above. The CERT, e.g., does not only refer to the intervention itself, but also to the actual conduction (including individualization or adverse events) and implementation (including teaching/supervising expertise or setting in which exercise training is performed) (93). Thus, further important contextual factors would be captured in a more comprehensive description.
Regardless of the reporting analysis, the included studies illustrate the multifaceted nature of potential workplace-related RT interventions for adult health promotion. RT represents a promising health promotion intervention component in many respects for a wide variety of target populations (27, 33, 82, 94, 95) (for employees with, e.g., different gender, age, occupational background, or exercise experience). Most of the included studies used only small equipment such as elastic bands or dumbbells, which basically allows exercise to be performed on site (or at home) without major organizational hurdles. For interventions again with group trainings or using machines, facilities are needed to keep distances short (fitness center or training facility in the building or in close proximity). However, given the small number of exercises in most studies (Supplementary Table 3) and the small amount of time required (session duration) combined with reduced or minimal supervision, the possibility of implementing RT interventions at the workplace is generally emphasized.
The main strength of the present review is the emphasis on the fundamentals of RT progression and exercise prescription (37–39). The assessment approach—oriented on a protocol by Westra et al. on the quality of RT description in COPD trials (96)—is comparatively comprehensive in terms of analyzing the reporting of RT interventions and provides a more detailed insight than, e.g., analyzing according to the so-called FITT-VP components (frequency, intensity, time, type of exercise, volume, and progression).
Since the main purpose of the review was not to investigate whether the reporting influences the intervention effects, the narrative analysis of the significant effects can be seen as a limitation. Determining the extent to which progression principles and variables of exercise prescription are attended is a critical first step in advancing knowledge of workplace-related RT interventions. Their impact on effectiveness should be explored in future analyses.
The main limitation of the review was the strict limitation to studies with a main focus on RT. During the full-text assessments, 28 studies alone were excluded that had a RT component within an intentionally mixed or multicomponent intervention. These studies would have required detailed analysis of all components (e.g., training principles for other training forms, theoretical basis for educational programs), which would have exceeded the review focus. Nevertheless, the present results should raise awareness for improved reporting not only for interventions with a main focus on RT. Future challenges will lie in the comparable reporting of training principles in more individualized or tailored approaches (33, 97) that take into account individual prerequisites and workloads in training planning and management. In addition, some studies did not definitively identify the extent to which they were workplace-related indicating the need for a better contextual description (such as location and integration into the working day).
Based on the great health-promoting potential of workplace-related interventions and the often limited time available for interventions at the workplace, RT interventions in this setting should be designed to be as effective as possible. However, without comprehensive information on the actual design of workplace-related RT interventions, it remains difficult to implement optimally dosed interventions for a desired benefit in different employee target groups. Therefore, a detailed description is also relevant from a transfer perspective.
In order to increase the reproducibility of RT interventions, exercise-reporting tools should be applied more frequently (98). Furthermore, findings from exercise science should be increasingly incorporated into RT interventions in the context of workplace-related health promotion. There is still potential, especially in the integration of periodization models and the reporting of rest periods.
All data generated or analyzed during this study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
GS: conceptualization, writing—original draft, visualization, and project administration. GS and LB: methodology. GS, LB, and OM: formal analysis and investigation. AS: resources and supervision. LB, OM, and AS: writing—review and editing. All authors have read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.832523/full#supplementary-material
1. World Health Organization. Ottawa Charter for Health Promotion. World Health Organization (1986).
2. Tudor-Locke C, Leonardi C, Johnson WD, Katzmarzyk PT. Time spent in physical activity and sedentary behaviors on the working day: the American time use survey. J Occup Environ Med. (2011) 53:1382–7. doi: 10.1097/JOM.0b013e31823c1402
3. Søgaard K, Sjøgaard G. Physical activity as cause and cure of muscular pain: evidence of underlying mechanisms. Exerc Sport Sci Rev. (2017) 45:136–45. doi: 10.1249/JES.0000000000000112
4. Löllgen H, Böckenhoff A, Knapp G. Physical activity and all-cause mortality: an updated meta-analysis with different intensity categories. Int J Sports Med. (2009) 30:213–24. doi: 10.1055/s-0028-1128150
5. Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380:219–29. doi: 10.1016/S0140-6736(12)61031-9
6. Sassen B, Cornelissen VA, Kiers H, Wittink H, Kok G, Vanhees L. Physical fitness matters more than physical activity in controlling cardiovascular disease risk factors. Eur J Cardiovasc Prev Rehabil. (2009) 16:677–83. doi: 10.1097/HJR.0b013e3283312e94
7. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. (2009) 301:2024–35. doi: 10.1001/jama.2009.681
8. Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. (2015) 25(Suppl 3):1–72. doi: 10.1111/sms.12581
9. Proper KI, Koning M, van der Beek AJ, Hildebrandt VH, Bosscher RJ, van Mechelen W. The effectiveness of worksite physical activity programs on physical activity, physical fitness, and health. Clin J Sport Med. (2003) 13:106–17. doi: 10.1097/00042752-200303000-00008
10. Prieske O, Dalager T, Herz M, Hortobagyi T, Sjøgaard G, Søgaard K, et al. Effects of physical exercise training in the workplace on physical fitness: a systematic review and meta-analysis. Sports Med. (2019) 49:1903–21. doi: 10.1007/s40279-019-01179-6
11. Mulchandani R, Chandrasekaran AM, Shivashankar R, Kondal D, Agrawal A, Panniyammakal J, et al. Effect of workplace physical activity interventions on the cardio-metabolic health of working adults: systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2019) 16:134. doi: 10.1186/s12966-019-0896-0
12. Maher CG. A systematic review of workplace interventions to prevent low back pain. Austral J Physiother. (2000) 46:259–69. doi: 10.1016/S0004-9514(14)60287-7
13. Burn NL, Weston M, Maguire N, Atkinson G, Weston KL. Effects of workplace-based physical activity interventions on cardiorespiratory fitness: a systematic review and meta-analysis of controlled trials. Sports Med. (2019) 49:1255–74. doi: 10.1007/s40279-019-01125-6
14. Pronk NP. Physical activity promotion in business and industry: evidence, context, and recommendations for a national plan. J Phys Activity Health. (2009) 6(Suppl 2):S220-35. doi: 10.1123/jpah.6.s2.s220
15. Kuoppala J, Lamminpää A, Husman P. Work health promotion, job well-being, and sickness absences - a systematic review and meta-analysis. J Occup Environ Med. (2008) 50:1216–27. doi: 10.1097/JOM.0b013e31818dbf92
16. Abdin S, Welch RK, Byron-Daniel J, Meyrick J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: a systematic review. Public Health. (2018) 160:70–6. doi: 10.1016/j.puhe.2018.03.029
17. Feigenbaum MS, Pollock ML. Prescription of resistance training for health and disease. Med Sci Sports Exerc. (1999) 31:38–45. doi: 10.1097/00005768-199901000-00008
18. Stamatakis E, Lee I-M, Bennie J, Freeston J, Hamer M, O'Donovan G, et al. Does strength-promoting exercise confer unique health benefits? A pooled analysis of data on 11 population cohorts with all-cause, cancer, and cardiovascular mortality endpoints. Am J Epidemiol. (2018) 187:1102–12. doi: 10.1093/aje/kwx345
19. Distefano G, Goodpaster BH. Effects of exercise and aging on skeletal muscle. Cold Spring Harb Perspect Med. (2018) 8:a029785. doi: 10.1101/cshperspect.a029785
21. Hart PD, Buck DJ. The effect of resistance training on health-related quality of life in older adults: Systematic review and meta-analysis. Health Promot Perspect. (2019) 9:1–12. doi: 10.15171/hpp.2019.01
22. Volaklis KA, Halle M, Meisinger C. Muscular strength as a strong predictor of mortality: a narrative review. Eur J Intern Med. (2015) 26:303–10. doi: 10.1016/j.ejim.2015.04.013
23. FitzGerald SJ, Barlow CE, Kampert JB, Morrow JR, Jackson AW, Blair SN. Muscular fitness and all-cause mortality: prospective observations. J Phys Activity Health. (2004) 1:7–18. doi: 10.1123/jpah.1.1.7
24. Abramowitz MK, Hall CB, Amodu A, Sharma D, Androga L, Hawkins M. Muscle mass, BMI, and mortality among adults in the United States: a population-based cohort study. PLoS ONE. (2018) 13:1-16. doi: 10.1371/journal.pone.0198318
25. Jochem C, Leitzmann M, Volaklis K, Aune D, Strasser B. Association between muscular strength and mortality in clinical populations: a systematic review and meta-analysis. J Am Med Dir Assoc. (2019) 20:1213–23. doi: 10.1016/j.jamda.2019.05.015
26. Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep. (2012) 11:209–16. doi: 10.1249/JSR.0b013e31825dabb8
27. Shaw BS, Shaw I, Brown GA. Resistance exercise is medicine: strength training in health promotion and rehabilitation. Int J Ther Rehabil. (2015) 22:385–9. doi: 10.12968/ijtr.2015.22.8.385
28. van Eerd D, Munhall C, Irvin E, Rempel D, Brewer S, van der Beek AJ, et al. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: an update of the evidence. Occup Environ Med. (2016) 73:62–70. doi: 10.1136/oemed-2015-102992
29. Skamagki G, King A, Duncan M, Wåhlin C. A systematic review on workplace interventions to manage chronic musculoskeletal conditions. Physiother Res Int. (2018) 23:e1738. doi: 10.1002/pri.1738
30. Sundstrup E, Seeberg KG, Bengtsen E, Andersen LL. A systematic review of workplace interventions to rehabilitate musculoskeletal disorders among employees with physical demanding work. J Occup Rehabil. (2020) 30:588-612. doi: 10.1007/s10926-020-09879-x
31. Proper KI, van Oostrom SH. The effectiveness of workplace health promotion interventions on physical and mental health outcomes - a systematic review of reviews. Scand J Work Environ Health. (2019) 45:546–59. doi: 10.5271/sjweh.3833
32. Frutiger M, Borotkanics R. Systematic review and meta-analysis suggest strength training and workplace modifications may reduce neck pain in office workers. Pain Pract. (2020) 21:100-31. doi: 10.1111/papr.12940
33. Sjøgaard G, Christensen JR, Justesen JB, Murray M, Dalager T, Fredslund GH, et al. Exercise is more than medicine: The working age population's well-being and productivity. J Sport Health Sci. (2016) 5:159–65. doi: 10.1016/j.jshs.2016.04.004
34. Baechle TR, Earle RW, Wathen D. Resistance training. In: Baechle TR, Earle RW, editors. Essentials of Strength Training and Conditioning. Champaign, IL: Human Kinetics (2008). p. 381–412.
35. Fleck SJ, Kraemer WJ. Designing Resistance Training Programs. Champaign, Ill.: Human Kinetics (2014). p. 507.
36. Kasper K. Sports training principles. Curr Sports Med Rep. (2019) 18:95–6. doi: 10.1249/JSR.0000000000000576
37. Ratamess NA, Alvar BA, Evetoch TK, Housh TJ, Kibler WB, Kraemer WJ, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. (2009) 41:687–708. doi: 10.1249/MSS.0b013e3181915670
38. Kraemer WJ, Ratamess NA. Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc. (2004) 36:674–88. doi: 10.1249/01.MSS.0000121945.36635.61
39. Bird SP, Tarpenning KM, Marino FE. Designing resistance training programmes to enhance muscular fitness: a review of the acute programme variables. Sports Med. (2005) 35:841–51. doi: 10.2165/00007256-200535100-00002
40. Ammann BC, Knols RH, Baschung P, Bie RA de, Bruin ED de. Application of principles of exercise training in sub-acute and chronic stroke survivors: a systematic review. BMC Neurol. (2014) 14:167. doi: 10.1186/s12883-014-0167-2
41. Baschung Pfister P, Bruin ED de, Tobler-Ammann BC, Maurer B, Knols RH. The relevance of applying exercise training principles when designing therapeutic interventions for patients with inflammatory myopathies: a systematic review. Rheumatol Int. (2015) 35:1641–54. doi: 10.1007/s00296-015-3343-9
42. Campbell KL, Neil SE, Winters-Stone KM. Review of exercise studies in breast cancer survivors: attention to principles of exercise training. Br J Sports Med. (2012) 46:909–16. doi: 10.1136/bjsports-2010-082719
43. Winters-Stone KM, Neil SE, Campbell KL. Attention to principles of exercise training: a review of exercise studies for survivors of cancers other than breast. Br J Sports Med. (2014) 48:987–95. doi: 10.1136/bjsports-2012-091732
44. Neil-Sztramko SE, Winters-Stone KM, Bland KA, Campbell KL. Updated systematic review of exercise studies in breast cancer survivors: attention to the principles of exercise training. Br J Sports Med. (2019) 53:504–12. doi: 10.1136/bjsports-2017-098389
45. Neil-Sztramko SE, Medysky ME, Campbell KL, Bland KA, Winters-Stone KM. Attention to the principles of exercise training in exercise studies on prostate cancer survivors: a systematic review. BMC Cancer. (2019) 19:321. doi: 10.1186/s12885-019-5520-9
46. Fairman CM, Hyde PN, Focht BC. Resistance training interventions across the cancer control continuum: a systematic review of the implementation of resistance training principles. Br J Sports Med. (2017) 51:677–85. doi: 10.1136/bjsports-2016-096537
47. Minshull C, Gleeson N. Considerations of the principles of resistance training in exercise studies for the management of knee osteoarthritis: a systematic review. Arch Phys Med Rehabil. (2017) 98:1842–51. doi: 10.1016/j.apmr.2017.02.026
48. Hendrey G, Holland AE, Mentiplay BF, Clark RA, Williams G. Do trials of resistance training to improve mobility after stroke adhere to the American College of Sports Medicine Guidelines? A systematic review. Arch Phys Med Rehabil. (2018) 99:584-97.e13. doi: 10.1016/j.apmr.2017.06.021
49. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. (2009) 339:b2535. doi: 10.1136/bmj.b2535
50. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) 339:b2700. doi: 10.1136/bmj.b2700
51. Schelvis RM, Oude Hengel KM, Burdorf A, Blatter BM, Strijk JE, van der Beek AJ. Evaluation of occupational health interventions using a randomized controlled trial: challenges and alternative research designs. Scand J Work Environ Health. (2015) 41:491–503. doi: 10.5271/sjweh.3505
52. World Health Organization. Jakarta Declaration on Leading Health Promotion into the 21st Century. World Health Organization (1997).
53. European Network for Workplace Health Promotion. Luxembourg Declaration on Workplace Health Promotion in the European Union. European Network for Workplace Health Promotion (1997).
54. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
55. Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies. Available online at: https://www.ephpp.ca/PDF/Quality%20Assessment%20Tool_2010_2.pdf (accessed September 30, 2021).
56. Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews Evid Based Nurs. (2004) 1:176–84. doi: 10.1111/j.1524-475X.2004.04006.x
57. Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies Dictionary. Available online at: https://www.ephpp.ca/PDF/QADictionary_dec2009.pdf (accessed September 30, 2021).
58. Andersen LL, Kjaer M, Søgaard K, Hansen L, Kryger AI, Sjøgaard G. Effect of two contrasting types of physical exercise on chronic neck muscle pain. Arthritis Rheum. (2008) 59:84–91. doi: 10.1002/art.23256
59. Andersen LL, Saervoll CA, Mortensen OS, Poulsen OM, Hannerz H, Zebis MK. Effectiveness of small daily amounts of progressive resistance training for frequent neck/shoulder pain: randomised controlled trial. Pain. (2011) 152:440–6. doi: 10.1016/j.pain.2010.11.016
60. Andersen CH, Andersen LL, Gram B, Pedersen MT, Mortensen OS, Zebis MK, et al. Influence of frequency and duration of strength training for effective management of neck and shoulder pain: a randomised controlled trial. Br J Sports Med. (2012) 46:1004–10. doi: 10.1136/bjsports-2011-090813
61. Blangsted AK, Søgaard K, Hansen EA, Hannerz H, Sjøgaard G. One-year randomized controlled trial with different physical-activity programs to reduce musculoskeletal symptoms in the neck and shoulders among office workers. Scand J Work Environ Health. (2008) 34:55–65. doi: 10.5271/sjweh.1192
62. Escriche-Escuder A, Calatayud J, Andersen LL, Ezzatvar Y, Aiguadé R, Casaña J. Effect of a brief progressive resistance training program in hospital porters on pain, work ability, and physical function. Musculoskelet Sci Pract. (2020) 48:102162. doi: 10.1016/j.msksp.2020.102162
63. Gram B, Andersen C, Zebis MK, Bredahl T, Pedersen MT, Mortensen OS, et al. Effect of training supervision on effectiveness of strength training for reducing neck/shoulder pain and headache in office workers: cluster randomized controlled trial. Biomed Res Int. (2014) 2014:693013. doi: 10.1155/2014/693013
64. Haufe S, Wiechmann K, Stein L, Kück M, Smith A, Meineke S, et al. Low-dose, non-supervised, health insurance initiated exercise for the treatment and prevention of chronic low back pain in employees. Results from a randomized controlled trial. PLoS ONE. (2017) 12:e0178585. doi: 10.1371/journal.pone.0178585
65. Helmhout PH, Harts CC, Staal JB, Candel MJ, Bie RA de. Comparison of a high-intensity and a low-intensity lumbar extensor training program as minimal intervention treatment in low back pain: a randomized trial. Eur Spine J. (2004) 13:537–47. doi: 10.1007/s00586-004-0671-y
66. Helmhout PH, Harts CC, Viechtbauer W, Staal JB, Bie RA de. Isolated lumbar extensor strengthening versus regular physical therapy in an army working population with nonacute low back pain: a randomized controlled trial. Arch Phys Med Rehabil. (2008) 89:1675–85. doi: 10.1016/j.apmr.2007.12.050
67. Li X, Lin C, Liu C, Ke S, Wan Q, Luo H, et al. Comparison of the effectiveness of resistance training in women with chronic computer-related neck pain: a randomized controlled study. Int Arch Occup Environ Health. (2017) 90:673–83. doi: 10.1007/s00420-017-1230-2
68. Mayer JM, Quillen WS, Verna JL, Chen R, Lunseth P, Dagenais S. Impact of a supervised worksite exercise program on back and core muscular endurance in firefighters. Am J Health Promot. (2015) 29:165–72. doi: 10.4278/ajhp.130228-QUAN-89
69. Mulla DM, Wiebenga EG, Chopp-Hurley JN, Kaip L, Jarvis RS, Stephens A, et al. The effects of lower extremity strengthening delivered in the workplace on physical function and work-related outcomes among desk-based workers: a randomized controlled trial. J Occup Environ Med. (2018) 60:1005–14. doi: 10.1097/JOM.0000000000001408
70. Muñoz-Poblete C, Bascour-Sandoval C, Inostroza-Quiroz J, Solano-López R, Soto-Rodríguez F. Effectiveness of workplace-based muscle resistance training exercise program in preventing musculoskeletal dysfunction of the upper limbs in manufacturing workers. J Occup Rehabil. (2019) 29:810–21. doi: 10.1007/s10926-019-09840-7
71. Nygaard Andersen L, Mann S, Juul-Kristensen B, Søgaard K. Comparing the impact of specific strength training vs general fitness training on professional symphony orchestra musicians: a feasibility study. Med Probl Perform Art. (2017) 32:94–100. doi: 10.21091/mppa.2017.2016
72. Sjögren T, Nissinen KJ, Järvenpää SK, Ojanen MT, Vanharanta H, Mälkiä EA. Effects of a physical exercise intervention on subjective physical well-being, psychosocial functioning and general well-being among office workers: a cluster randomized-controlled cross-over design. Scand J Med Sci Sports. (2006) 16:381–90. doi: 10.1111/j.1600-0838.2005.00516.x
73. Sundstrup E, Jakobsen MD, Andersen CH, Jay K, Persson R, Aagaard P, et al. Effect of two contrasting interventions on upper limb chronic pain and disability: a randomized controlled trial. Pain Phys. (2014) 17:145–54. doi: 10.36076/ppj.2014/17/145
74. Zavanela PM, Crewther BT, Lodo L, Florindo AA, Miyabara EH, Aoki MS. Health and fitness benefits of a resistance training intervention performed in the workplace. J Strength Cond Res. (2012) 26:811–7. doi: 10.1519/JSC.0b013e318225ff4d
75. Zebis MK, Andersen LL, Pedersen MT, Mortensen P, Andersen CH, Pedersen MM, et al. Implementation of neck/shoulder exercises for pain relief among industrial workers: a randomized controlled trial. BMC Musculoskelet Disord. (2011) 12:205. doi: 10.1186/1471-2474-12-205
76. Andersen LL, Zebis MK, Pedersen MT, Roessler KK, Andersen CH, Pedersen MM, et al. Protocol for work place adjusted intelligent physical exercise reducing musculoskeletal pain in shoulder and neck (VIMS): a cluster randomized controlled trial. BMC Musculoskelet Disord. (2010) 11:173. doi: 10.1186/1471-2474-11-173
77. Helmhout PH, Harts CC, Staal JB, Bie RA de. Rationale and design of a multicenter randomized controlled trial on a 'minimal intervention' in Dutch army personnel with nonspecific low back pain [ISRCTN19334317]. BMC Musculoskelet Disord. (2004) 5:40. doi: 10.1186/1471-2474-5-40
78. Sundstrup E, Jakobsen MD, Andersen CH, Jay K, Persson R, Aagaard P, et al. Participatory ergonomic intervention versus strength training on chronic pain and work disability in slaughterhouse workers: study protocol for a single-blind, randomized controlled trial. BMC Musculoskelet Disord. (2013) 14:67. doi: 10.1186/1471-2474-14-67
79. Hunter JR, Gordon BA, Bird SR, Benson AC. Perceived barriers and facilitators to workplace exercise participation. IJWHM. (2018) 11:349–63. doi: 10.1108/IJWHM-04-2018-0055
80. Kruger J, Yore MM, Bauer DR, Kohl HW. Selected barriers and incentives for worksite health promotion services and policies. Am J Health Promot. (2007) 21:439–47. doi: 10.4278/0890-1171-21.5.439
81. Kraemer WJ, Ratamess NA, French DN. Resistance training for health and performance. Curr Sports Med Rep. (2002) 1:165–71. doi: 10.1249/00149619-200206000-00007
82. Mcleod JC, Stokes T, Phillips SM. Resistance exercise training as a primary countermeasure to age-related chronic disease. Front Physiol. (2019) 10:645. doi: 10.3389/fphys.2019.00645
83. Rhea MR, Alderman BL. A meta-analysis of periodized versus nonperiodized strength and power training programs. Res Q Exerc Sport. (2004) 75:413–22. doi: 10.1080/02701367.2004.10609174
84. Williams TD, Tolusso DV, Fedewa MV, Esco MR. Comparison of periodized and non-periodized resistance training on maximal strength: a meta-analysis. Sports Med. (2017) 47:2083–100. doi: 10.1007/s40279-017-0734-y
85. Lorenz DS, Reiman MP, Walker JC. Periodization: current review and suggested implementation for athletic rehabilitation. Sports Health. (2010) 2:509–18. doi: 10.1177/1941738110375910
86. Baz-Valle E, Schoenfeld BJ, Torres-Unda J, Santos-Concejero J, Balsalobre-Fernández C. The effects of exercise variation in muscle thickness, maximal strength and motivation in resistance trained men. PLoS ONE. (2019) 14:e0226989. doi: 10.1371/journal.pone.0226989
87. Andersen LL, Zebis MK. Process evaluation of workplace interventions with physical exercise to reduce musculoskeletal disorders. Int J Rheumatol. (2014) 2014:761363. doi: 10.1155/2014/761363
88. Simão R, Salles BF de, Figueiredo T, Dias I, Willardson JM. Exercise order in resistance training. Sports Med. (2012) 42:251–65. doi: 10.2165/11597240-000000000-00000
89. Salles BF de, Simão R, Miranda F, Novaes Jd, Lemos A, Willardson JM. Rest interval between sets in strength training. Sports Med. (2009) 39:765–77. doi: 10.2165/11315230-000000000-00000
90. Grgic J, Schoenfeld BJ, Skrepnik M, Davies TB, Mikulic P. Effects of rest interval duration in resistance training on measures of muscular strength: a systematic review. Sports Med. (2018) 48:137–51. doi: 10.1007/s40279-017-0788-x
91. Slade SC, Dionne CE, Underwood M, Buchbinder R. Consensus on exercise reporting template (CERT): explanation and elaboration statement. Br J Sports Med. (2016) 50:1428–37. doi: 10.1136/bjsports-2016-096651
92. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
93. Slade SC, Dionne CE, Underwood M, Buchbinder R, Beck B, Bennell K, et al. Consensus on exercise reporting template (CERT): modified delphi study. Phys Ther. (2016) 96:1514–24. doi: 10.2522/ptj.20150668
94. Winett RA, Carpinelli RN. Potential health-related benefits of resistance training. Prev Med. (2001) 33:503–13. doi: 10.1006/pmed.2001.0909
95. Hass CJ, Feigenbaum MS, Franklin BA. Prescription of resistance training for healthy populations. Sports Med. (2001) 31:953–64. doi: 10.2165/00007256-200131140-00001
96. Westra B, Wolf S de, Bij de Vaate E, Legemaat M, Nyberg A, Klijn P. Quality of resistance training description in COPD trials: study protocol for a systematic review. BMJ Open. (2019) 9:e025030. doi: 10.1136/bmjopen-2018-025030
97. Sjøgaard G, Justesen JB, Murray M, Dalager T, Søgaard K. A conceptual model for worksite intelligent physical exercise training–IPET–intervention for decreasing life style health risk indicators among employees: a randomized controlled trial. BMC Public Health. (2014) 14:652. doi: 10.1186/1471-2458-14-652
Keywords: health promotion, workplace, resistance training, reporting, transfer
Citation: Stassen G, Baulig L, Müller O and Schaller A (2022) Attention to Progression Principles and Variables of Exercise Prescription in Workplace-Related Resistance Training Interventions: A Systematic Review of Controlled Trials. Front. Public Health 10:832523. doi: 10.3389/fpubh.2022.832523
Received: 09 December 2021; Accepted: 08 February 2022;
Published: 25 March 2022.
Edited by:
Danijela Gasevic, Monash University, AustraliaReviewed by:
Karen Søgaard, University of Southern Denmark, DenmarkCopyright © 2022 Stassen, Baulig, Müller and Schaller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gerrit Stassen, Zy5zdGFzc2VuQGRzaHMta29lbG4uZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.