 Siyu Xu1
Siyu Xu1 Ya Wang
Ya Wang Mengmeng Wang
Mengmeng Wang Hao Huang
Hao Huang- 1West China Second University Hospital, Sichuan University, Chengdu, China
- 2West China School of Nursing, Sichuan University, Chengdu, China
- 3West China Hospital, Sichuan University, Chengdu, China
- 4Department of Nursing, West China Hospital, Sichuan University, Chengdu, China
- 5Mental Health Center, West China Hospital, Sichuan University, Chengdu, China
Introduction: Hospital-at-home (HaH) services have become increasingly popular. However, the experience of HaH implementation in Asia is inadequate. Therefore, the purpose of this study was to investigate individuals' willingness to accept HaH services and the potential related factors.
Methods: The researchers visited households to select appropriate participants. An online questionnaire survey was conducted among the inhabitants of selected communities. An individual's awareness, willingness to accept HaH services, and demands such as ideal service providers and more detailed information to accept HaH care were investigated. The outcome measure was the willingness to accept HaH services. Chi-square tests and logistic regression models were used to analyze the factors.
Results: A total of 622 subjects participated in this study. The findings indicate that 55.9% of the participants were not aware of HaH services, while most of the subjects (88.4%) were willing to accept them. Regression models indicated that having health insurance (OR = 2.170, 95% CI: 1.003–4.697), an awareness of the necessity of HaH services (OR = 4.721, 95% CI: 2.471–9.019), very much hoping staff from central hospitals would be service providers (OR = 20.299, 95% CI: 5.718–72.068), and somewhat hoping that staff from central hospitals would be service providers (OR = 9.139, 95% CI: 2.714–30.775) were the factors associated with a greater willingness to accept HaH services.
Conclusion: The study indicates that compared to the awareness of HaH care, residents had a greater willingness to accept such care. The willingness to utilize HaH services among individuals was associated with enabling factors, predisposing factors, and HaH-related demand factors.
Introduction
With increasing health care demand and shortage of hospital beds around the world, the health care system is currently facing the challenge of decreased quality of care (1). The high incidence rate of chronic diseases such as diabetes, cancer, and hypertension (2) has caused many hospitals to be unable to provide sufficient care to satisfy their clients' needs. Moreover, the increasing number of elderly individuals as the population ages contributes to the challenges facing current health systems to satisfy consumers' demands (3, 4). As the proportion of chronic diseases has increased with population aging, the availability of hospital beds has decreased. Even more noteworthy, since the outbreak of the COVID-19 epidemic, according to the World Health Statistics 2021 launch by the World Health Organization (WHO), the number of confirmed cases of COVID-19 has topped 0.153 billion, which has exacerbated the conflict between the supply and demand for medical resources and made it more difficult for people to obtain medical services1.
To overcome these complex challenges, an innovative solution that can offer an alternative model of care is needed. With hospital-at-home (HaH) services, originated in 1958, health care professionals provide hospital-level care in patients' homes (1). Gogan suggested that receiving health care at home could help patients recover more rapidly (5). In recent years, HaH care has become increasingly popular as a substitute for inpatient care, and many diseases have been treated through HaH services, including chronic obstructive pulmonary disease and chronic kidney disease (5–10). Compared to inpatient care, HaH services represent substantial cost savings, alleviate the increasing pressures on the inpatient bed supply, and reduce the risks associated with prolonged inpatient care, such as delirium and hospital-acquired infections (11). Mortality and readmission rates do not differ significantly between HaH and inpatient care (6, 7).
The Chinese government has also paid close attention to the implementation of HaH services. The Interim Regulations on HaH Management in Sichuan Province were launched in 2019 and defined the mission, target diseases, leadership, methods, and regulations for HaH services (12). However, compared to several Western countries, such as the United States, United Kingdom, Australia, and Canada, HaH services in China are developing slowly (13). For example, in 2012 a total of 12,200 home health agencies provided home hospital beds in the United States. Insurance coverage for this service was available to 3.43 million patients. A total of 98.6% of these facilities were authorized by Medicare (federal health insurance) and 77.5% were authorized by Medicaid (medical assistance). Home care services were subsidized by Medicare for almost $1.79 billion in 2015 (14, 15). In Canada, health care is mainly provided by a family physician primary care system. Family physicians accompanied by their teams handle more than 80% of disease treatments, and refer patients to appropriate specialists through a referral mechanism when necessary. The Canadian model significantly improves the utilization of medical resources for hospital specialties (16). Due to different cultures, financial development, and compensatory policies, attitudes toward accepting HaH care vary among countries. Despite the prevalence of HaH services in Western countries, studies that explore individuals' willingness to accept HaH services in Asia are limited, and the public perception of HaH services has yet to be well established (13). A deeper comprehension of individuals' attitudes toward HaH care is essential before implementing it in any new setting (17). Moreover, more detailed issues, such as ideal service providers, the proportion of compensation, and the frequency of ward rounds are yet to be determined, and taking individual demands into consideration is crucial in the promotion of HaH development (18).
Therefore, this study adopted the Andersen–Newman behavioral model to explore the willingness of residents to accept HaH services and the potential factors of agreement to HaH services in Asian countries such as China (18), which will be helpful for obtaining a deeper understanding of residents' opinions concerning HaH services and in providing reliable evidence for HaH promotion and service improvement to ensure that targeted services can be offered.
Methods
Study Design
This was a cross-sectional study carried out with 622 residents of Chengdu City by using a personal characteristics questionnaire and a questionnaire that assessed respondents' awareness of and willingness to accept HaH services.
Participants
The initial sample size (n = 600) was calculated by the formula N = Z2× {P× (1−P)}÷E2(Z = 1.96, E = 4%, and P = 0.5). Participants were selected through convenience sampling. Because of the possibility of survey dropout, 700 participants were invited to finish the survey. Volunteers who met the following criteria were enrolled in this study: (1) >18 years old; (2) no cognitive impairment or psychiatric disorder; and (3) permanent residents of Chengdu City. Of the 700 residents invited to participate, 650 answered the questionnaire, and of these, 622 (88.9%) provided complete and usable data to be included in the data analysis. Only complete data were analyzed.
Sample Collection
To ensure that the process of data collection would go smoothly, the researchers discussed with several community leaders in Chengdu. With the consent of the people in charge, the surveys were administered to subjects from five communities in Chengdu City. Through lectures, the researchers explained the HaH concept and function, as well as the proposal and precautions of the survey. After the lectures were completed, three researchers visited households in the community to select subjects who met the inclusion criteria. After the link to the online questionnaire was sent to the subjects by a WeChat QR code, the subjects completed the questionnaires by themselves. During this process, the researchers always answered the subjects' questions to ensure that the subjects fully understood each item of the questionnaire to improve the accuracy of each answer. Through an online questionnaire, the processes of data collection and entry were integrated. The software package WJX (www.wjx.com) was used to collect data. WJX is a professional online platform widely used in several fields that includes data collection, custom reports, and survey result analysis. More than 0.1 billion individuals in China have registered with WJX software. To ensure rigor in the sample collection process and reduce bias, strict quality control measures were adopted. Misfillinging or omission of filling the questions was avoided by preset single-choice, multiple-choice, and fill-in-the-blank questions. The questionnaires could not be submitted unless they were completed. One person could only fill in the questionnaire once after all the topics were completed. Each questionnaire was screened by automatic screening rules and manually checked by the researchers after submission. Any answer that did not meet the requirements, such as only one option was selected or the questionnaire was finished within 60 s, was marked as invalid and removed.
Instruments
Personal Characteristics Questionnaire
A personal characteristics questionnaire was designed to collect data on the participants' general characteristics, including their gender, age, educational background, occupation, income, family income, and health status, such as whether they currently or previously had any chronic disease, type of chronic disease, family's health status, medication usage, family's medication usage, and family's visual acuity status.
Questionnaire on Residents' Awareness of, Willingness to Accept, and Demands Regarding HaH Services
The researchers designed a questionnaire consisting of 12 multiple-choice items to investigate Chengdu residents' willingness to accept HaH services and potential related factors. This questionnaire was constructed after reading related literature and was revised by many experts; Cronbach's α coefficient (0.821) and Kaiser–Meyer–Olkin measure (0.948) were calculated as reliability and validity indicators. The variables were as follows: whether the subject had heard about HaH services; whether the subject had accepted any HaH services; the necessity of launching HaH services; the reasons why the subject believed that HaH services were important; an awareness of the extent of HaH service reimbursement; the ideal service provider; the frequency of ward rounds by doctors; the frequency of nursing ward rounds; the ideal expense account for family income; the attitude toward doctors and nurses from the central hospitals that provide the services; and willingness to accept HaH services. The primary dependent variable was the willingness of residents to accept HaH services.
Independent and Dependent Variables
The Andersen–Newman behavioral model was constructed by Professor Ronald in 1968 and is one of the classic models for studying the utilization of health services. The model involves three types of determining factors that affect an individual's utilization, namely, predisposing, enabling, and need factors. Predisposing factors refer to personal sociocultural position prior to health service utilization, which consist of demographic characteristics, social structure, and health beliefs. Demographic characteristics indicate one's basic condition, such as age and gender. Social structure includes one's educational background, occupation, social network, and perception of the health service system (18). Therefore, we inquired about individuals' age, gender, educational background, occupation, whether they had heard about HaH care, whether they had accepted HaH services, the necessity of launching HaH services, and their awareness of the extent of HaH service reimbursement as predisposing factors. Enabling factors include the capacity to obtain health services and the availability of health services, such as income and health insurance (18). Therefore, an individual's monthly income, family monthly income, and health insurance status were defined as enabling factors. Need factors indicate the cognitive requirements of individuals for health services, including their health status and disease conditions (18). As for service demands, service provider requirements were also taken into consideration and were defined as the HaH-related demand factor. The dependent variable of the study was willingness to accept HaH services.
Statistical Analysis
The data were analyzed with the SPSS 21.0 software package. Frequency and percentage statistics were used to analyze the participants' predisposing, enabling, need, and HaH-related factors. The results of the questionnaire on the participants' awareness of, willingness to accept, and demands regarding HaH are also presented as frequencies and percentages. The associations among the independent variables and dependent variable were evaluated by using the chi-square test, with P < 0.05 considered to be statistically significant. Before a logistic regression was performed, the correlations among the independent variables were also analyzed. To bypass the impact of collinearity between the independent variables on the final findings, stepwise (forward) logistic regression models were run to minimize the effect of the correlation between variables, including only the independent variables associated with the dependent variable.
Ethics
The study was approved by the Ethics Committee of West China Hospital, Sichuan University (No. 848). All participants were informed of the details of this study and agreed to participate in the survey. Written informed consents were provided by each participants.
Results
Participant Characteristics
A total of 622 residents of Chengdu City participated in this study (including 166 males and 456 females). Most were between 30 and 50 years old (mean ± SD: 40.22 ± 12.95). Of the respondents, 36.35% had a bachelor's degree or above, 47.9% were managers, public servants, or professional personnel, and 90.0% had health insurance. A total of 17.4% currently or previously had a chronic disease, while 46.5% of participants' relatives currently or previously had a chronic disease.
Residents' Awareness of, Willingness to Accept, and Demands Regarding HaH Services
The data from this study indicate that 55.9% of participants were not aware of HaH services, while most of the subjects (88.4%) were willing to accept them. Only 2.4% of residents had accepted HaH care before this survey. In this study, 418 (67.2%) of individuals thought that HaH services were necessary. A total of 360 (57.9%) residents were willing to accept better companionship, and 253 (40.7%) were willing to accept this for convenience. Details are shown in Table 1.

Table 1. Participant characteristics, awareness of, willingness to accept, and demands regarding HaH services.
Chi-Test of the Willingness to Accept HaH Services by Predisposing Variables, Enabling Variables, Need Factors, and HaH-Related Demands
The chi-square test detected the potential factors that affected the likelihood of agreeing to HaH services. The participants' educational background, occupation, health insurance status, source of revenue, monthly income, family monthly income, awareness of HaH services, ideal frequency of ward rounds, ideal service providers, and attitudes toward doctors and nurses from the central hospitals that provided services may affect their willingness to accept HaH care (Table 2).
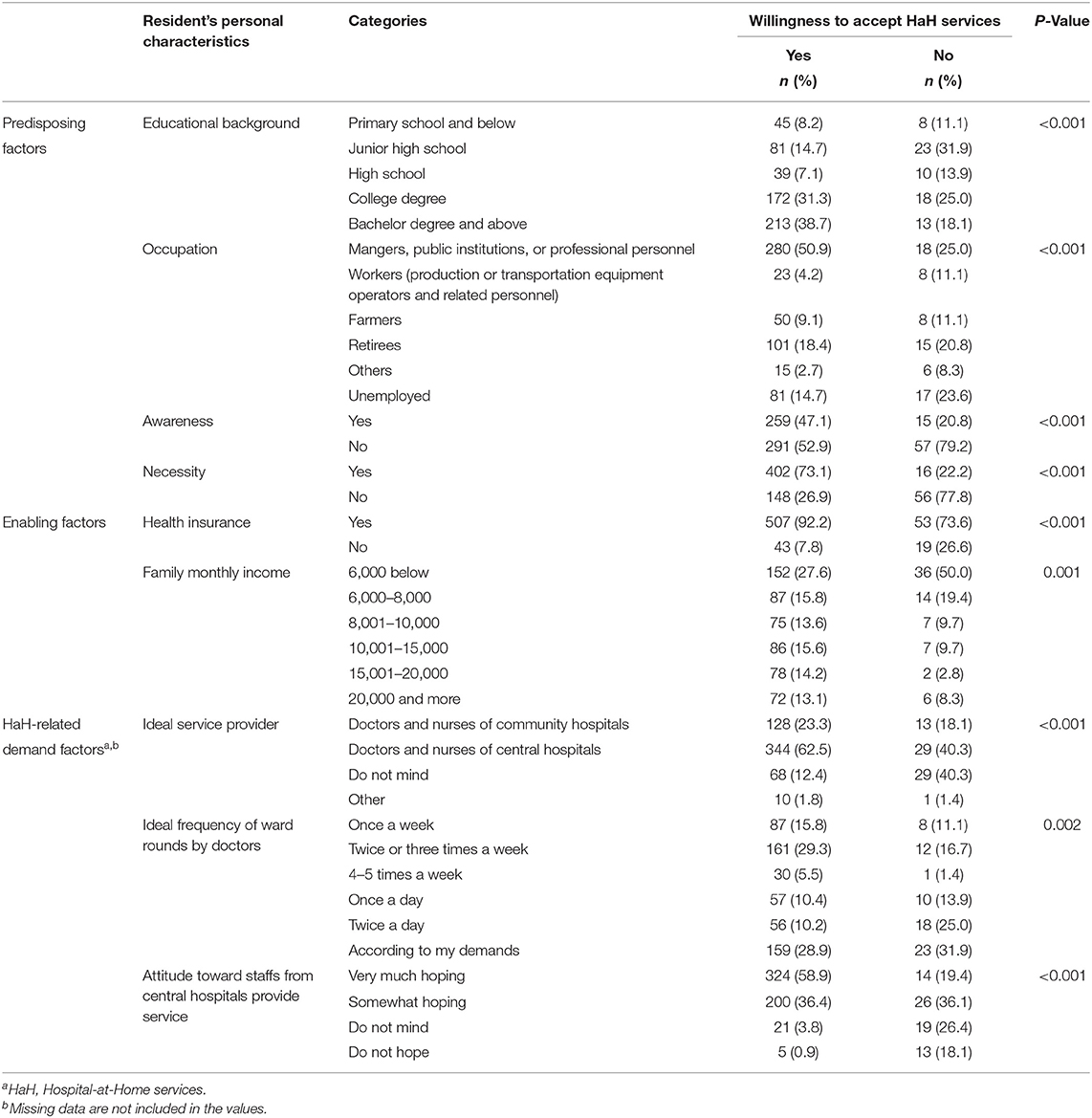
Table 2. Chi-test of the willingness to accept HaH services.
Correlation Analysis Among the Independent Variables
The results of the correlation analysis tested the collinearity between the independent variables. The results indicated that there are significant correlations between the variables, especially between demographic variables such as educational background, occupation, and health insurance, which may affect the research results. Therefore, rigorous statistical methods were required. Stepwise (forward) logistic regression models were run to minimize the effect of the correlation between variables (Table 3).
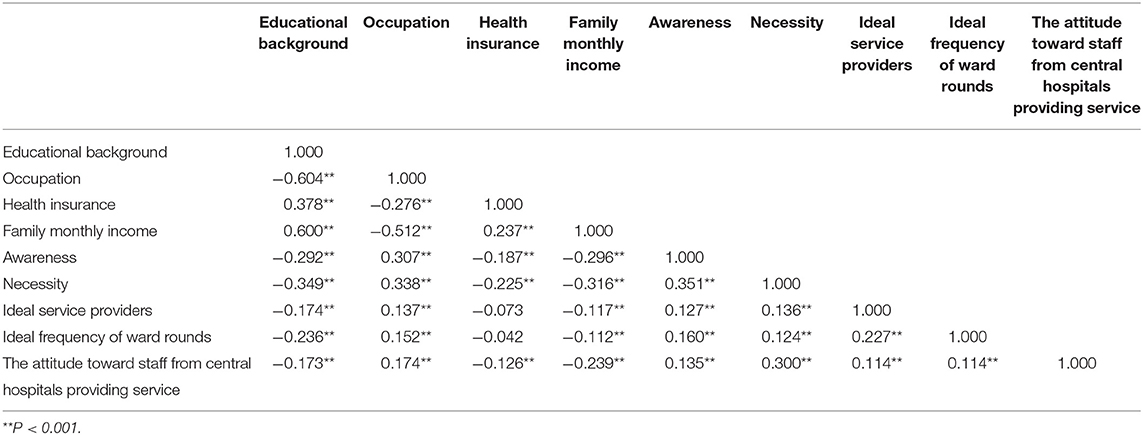
Table 3. Correlation between the independent variables.
Comparison of the Willingness to Accept HaH Services by Predisposing Variables, Enabling Variables, Need Factors, and HaH-Related Demands
A stepwise logistic regression model was used to identify the variables associated with the willingness to accept HaH services, and the final regression model indicated that being enrolled in health insurance (OR = 2.170, 95% CI: 1.003–4.697), an awareness of the necessity of HaH services (OR = 4.721, 95% CI: 2.471–9.019), very much hoping that staff from central hospitals would be the service providers (OR = 20.299, 95% CI: 5.718–72.068), and somewhat hoping that staff from central hospitals would be the service providers (OR = 9.139, 95% CI: 2.714–30.775) were the factors associated with a greater willingness to accept HaH services (Table 4).
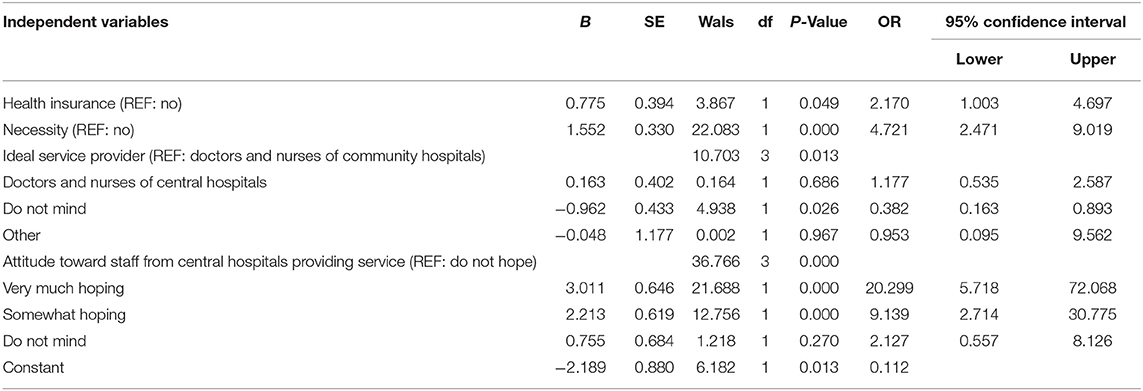
Table 4. Comparison of the willingness to accept HaH services by predisposing variables, enabling variables, need factors, and HaH-related demands.
Discussion
To our knowledge, this study is the first to explore individuals' awareness of and willingness to accept HaH services that focuses on the demands related to HaH services based on the Andersen–Newman behavior model. The findings might serve as guidelines for future HaH promotion and implementation. Our findings emphasize the impact of HaH-related variables such as the awareness of HaH services, service demands, and reimbursement demands on the acceptance of HaH services among individuals in Chengdu City. In contrast to a similar study conducted in Singapore, the vast number of subjects in this study would accept HaH services (13). This phenomenon can be explained by the differing health care service models and resource allocation between China and Singapore. Singapore not only has a dual system of health care services, with a public system provided by the government and a private system provided by the private sector but also has 24.60 medical doctors and 62.43 nursing personnel per 10,000 people (19). In China, medical and health institutions are divided into public and socially run categories. Public medical institutions are the main medical service providers, and they are supplemented by socially run medical institutions, with 22.27 medical doctors and 30.83 nursing personnel per 10,000 people, which are both lower than in Singapore (19). Therefore, we infer that Chinese residents may have to spend more time waiting for effective treatment, as China's health care human resources are more limited. HaH services have been proven to be effective in saving time and alleviating the shortage of medical resources; therefore, Chinese residents are more willing to accept them. Individuals' willingness to accept HaH services is connected to their health insurance status, awareness of their necessity, and attitudes toward staff from the central hospitals that offer HaH services.
The findings of this study indicate that compared to the awareness of HaH services, there was a greater willingness to accept HaH care among the subjects. Because of the shortage of medical resources in recent years, healthcare professionals cannot provide adequate medical services to every patient, which results in patients' needs not being fully met and leads to poor healthcare experiences (20, 21). In addition, the unfamiliarity of the hospital environment can harm patients' mental health, which is not conducive to their recovery (22). Prolonged hospitalization can lead to additional risks, such as delirium and infections (23–28). These problems are mitigated by HaH services, which might be why most of the subjects were willing to accept them. However, there is inadequate advertising and utilization of HaH services. Therefore, the awareness of HaH care is not high. Accordingly, concrete measures are needed to raise awareness of the concept, strengths, and functions of HaH services, such as information disseminated through television, newspapers, and applications, to increase residents' understanding of these services. Individuals' awareness of the necessity of HaH services is related to their willingness to accept HaH services. According to the Andersen–Newman behavioral model, an individual's perception of a medical service before receiving it can influence his or her willingness to accept this service (18). After hearing an explanation of the concept and function of HaH services, subjects might be more aware of the necessity of developing HaH care to ameliorate the shortage of medical resources. Therefore, those who are more aware of the necessity of HaH services might perceive more benefits and exhibit a higher willingness to accept HaH services.
As an enabling factor, health insurance coverage is associated with the willingness to accept HaH services. This result is similar to a study that argued that individuals enrolled in health insurance are more willing to maintain contact with family doctors (29). A previous study confirmed that health insurance status varies by socioeconomic status. Individuals not enrolled in health insurance may have a lower socioeconomic status; therefore, they cannot afford the full cost of HaH care (30, 31). Being covered by health insurance can reduce the cost of medical services and alleviate patients' stress, which enables them to be available to accept health services (29). Accordingly, individuals not enrolled in health insurance cannot afford the fees for HaH services. Therefore, wider enrollment in health insurance is key to the promotion of HaH services. More mature compensatory policies are needed, and the experience of developed countries is enlightening. For instance, in Norway, home care is free for patients, and in Canada, it is funded by the government (32). Moreover, the results of this study showed that 391 participants were not clear about the cost of HaH services, and most hoped that it would be <20% of their monthly family income. Many countries where HaH services have been widely implemented, such as Australia and the UK, have single-payer systems and strong imperatives to keep medical costs low; related systems need to control the overall cost of HaH care and set proper charging standards (33).
The vast number of the subjects in this study (54.3%) hoped that staff from central hospitals would offer HaH services. This study also found that the participants who very much or somewhat hoped that staff from central hospitals would be service providers were inclined to be more accepting of HaH services. However, in China, HaH care is mostly performed by community staff with only a college degree or below and limited medical skills to meet client requirements (34, 35). Moreover, highly qualified health staff in China always work in central hospitals and do not have time to provide HaH services (35). This phenomenon can be explained by the siphon effect of high-grade hospitals in China; these hospitals attract both large numbers of patients, which gives them a strong “resource siphon” ability, and qualified doctors to actively practice there for more opportunities and career resources (36). However, the workload in central hospitals in China is too heavy for these staff to provide extra HaH services (35). In Spain, each HaH unit consists of at least an internal medicine specialist and a general physician who incorporate specialists such as pulmonologists, geriatricians, and general surgeons. Nurses who provide HaH services must also be trained in hospital specialties and obtain a qualification certificate (37). In Sweden, nurses who provide home care services are required to have at least a bachelor's degree, and a master's degree is preferable (38). Therefore, related departments should make efforts to encourage health systems to develop HaH services and provide adequate resources for this development to inspire well-trained professionals to participate (13). The experiences of other countries can be studied to understand how to launch HaH services. For instance, it would be useful to develop a curriculum on medical care at home, promote practical home care skills, and train students on the use of portable medical devices to cultivate talent with at least a bachelor's degree in home care (35).
Interestingly, one of the findings of this research contradicts previous literature: socioeconomic factors were not associated with an individual's willingness to accept HaH care (30, 31). As there is a linkage between enrollment in health insurance and an individual's educational background, occupation, and income, it appears that enrollment in health insurance might act as a mediating variable between socioeconomic factors and willingness to accept HaH services. People who have high earnings with higher educational backgrounds care a great deal about their health; therefore, they pay health insurance enrollment fees (39). However, further analysis is needed to better explain this phenomenon. Individuals' health status was also not associated with their willingness to accept HaH services, which might be explained by the fact that there were only 622 participants in this study, and most did not have a chronic disease. Further investigation is also needed on this issue.
China has a total of 1.4 billion people, which accounts for nearly one-third of the total population of Asia, and there are similarities between the health care delivery systems in mainland China and both Japan and South Korea. Therefore, because of the similar health care systems and population ratios in China, we believe that the results of this study may have some generalizable implications. However, due to the differences in the per capita medical human resources and economic development levels, whether the results of this study are representative of Asia requires further discussion.
This study has certain limitations. First, it used a convenience sampling method, not random sampling, which may have resulted in bias. Second, the sample size was only 622, which may lead to the sample being unrepresentative. For example, the gender ratio in Chengdu is nearly 1:1 (50.54%:49.46%) (40); however, male respondents accounted for only 26.7% of the sample in this study. A smaller sample size might fail to reflect the real willingness of the male population. In addition to the male population, the other groups that accounted for a minor proportion, such as workers' estimated willingness (e.g., production or transportation equipment operators and related personnel), may be affected. Third, this study was a cross-sectional study that was unable to explore how individuals' willingness to accept HaH care is shaped. Therefore, longitudinal studies are needed. Fourth, the survey utilized an online method to collect data, and those who were not familiar with the internet may be under-represented. Thus, this study's participants might not represent elderly individuals with more healthcare needs, whose views are also important. However, this study investigated the willingness of residents to accept HaH services and demonstrated the gap between residents' actual demands and willingness to accept HaH services. The results of this study are significant for both the medical system and residents. In terms of the medical systems' viewpoints, a better understanding of residents' perceptions and demands can help develop more targeted services and effective advertising policies to lead to a higher willingness to accept HaH services. Therefore, HaH services can be widely accepted to alleviate medical resource insufficiency. In terms of residents' viewpoints, a better understanding of their opinions and demands can result in better service, more reasonable charging standards, and regular work procedures of HaH care to ensure that people can truly benefit from HaH services.
Conclusion
This study shows that there was a lower awareness of but higher willingness to accept HaH services among the participants, which indicates that the awareness of HaH services among the residents of Chengdu City has room for growth. The willingness to accept HaH services among individuals was associated with enabling factors such as health insurance enrollment, predisposing factors such as an awareness of the necessity of HaH services, and HaH-related demand factors such as attitudes toward staff from central hospitals as service providers. Therefore, effective policies and practical measures must be created to motivate the development of HaH services.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethics Committee of West China Hospital, Sichuan University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
JW and YW were involved in the design of the study, acquisition of data, and development of the statistical framework, and they reviewed the manuscript. MW and XH were involved in the study design and development of the analysis framework. SX and HH developed the statistical framework for data analysis, conducted the statistical analysis, interpreted the data, and drafted the manuscript. All authors read and approved the final manuscript.
Funding
This research was supported by the Science and Technology Department of Sichuan Province Fund Project (Program Nos: 2021YFS0151 and 2021JDR0188) and the West China School of Nursing, Sichuan University (HXHL19012).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank the study participants for their contribution to the research and current and past investigators and staff. We would like to thank Na Meng for providing methodological feedback in preparing the manuscript.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.823384/full#supplementary-material
Footnotes
References
1. Leong MQ, Lim CW, Lai YF. Comparison of Hospital-at-Home models: a systematic review of reviews. BMJ Open. (2021) 11:e043285. doi: 10.1136/bmjopen-2020-043285
2. Lyu J, Zhang W, Li W, Wang S, Zhang J. Epidemic of chronic diseases and the related healthy lifestyle interventions in rural areas of Shandong Province, China. BMC Public Health. (2020) 20:606. doi: 10.1186/s12889-020-08729-y
3. Liu Y, Qu Z, Meng Z, Wang S. Relationship between loneliness and quality of life in elderly empty nesters from the Wolong Panda Nature Reserve in Sichuan province, China, from the perspective of rural population and social sustainability. Phys A Stat Mech Appl. (2020) 551:124154. doi: 10.1016/j.physa.2020.124154
4. Zhang C, Hou L, Zheng X, Zhu R, Zhao H, Lu J, et al. Risk factors of mental disorders among empty and non-empty nesters in Shanxi, China: a cross-sectional study. Health Qual Life Outcomes. (2019) 17:18. doi: 10.1186/s12955-019-1088-y
5. Makela P, Stott D, Godfrey M, Ellis G, Schiff R, Shepperd S. The work of older people and their informal caregivers in managing an acute health event in a hospital at home or hospital inpatient setting. Age Ageing. (2020) 49:856–64. doi: 10.1093/ageing/afaa085
6. Hughes SL, Ulasevich A, Weaver FM, Henderson W, Manheim L, Kubal JD, et al. Impact of home care on hospital days: a meta analysis. Health Serv Res. (1997) 32:415–32.
7. Ram FSF. Hospital at home for patients with acute exacerbations of chronic obstructive pulmonary disease: systematic review of evidence. Br Med J. (2004) 329:315. doi: 10.1136/bmj.38159.650347.55
8. Hecimovic A, Matijasevic V, Frost SA. Characteristics and outcomes of patients receiving Hospital at Home Services in the South West of Sydney. BMC Health Serv Res. (2020) 20:1090. doi: 10.1186/s12913-020-05941-9
9. Caplan GA, Sulaiman NS, Mangin DA, Ricauda NA, Wilson AD, Barclay L, et al. Meta-analysis of “hospital in the home”. Med J Aust. (2012) 197:512–9. doi: 10.5694/mja12.10480
10. Elliott MJ, Love S, Donald M, Manns B, Donald T, Premji Z, et al. Outpatient interventions for managing acute complications of chronic diseases: a scoping review and implications for patients with CKD. Am J Kidney Dis. (2020) 76:794–805. doi: 10.1053/j.ajkd.2020.04.006
11. Levine DM, Pian J, Mahendrakumar K, Patel A, Saenz A, Schnipper JL. Hospital-level care at home for acutely ill adults: a qualitative evaluation of a randomized controlled trial. J Gen Intern Med. (2021) 36:1965–73. doi: 10.1007/s11606-020-06416-7
12. Province HcoS,. The Interim Regulations On hospital-at-home management in Sichuan province. (2019). Available online at: http://wsjkw.sc.gov.cn/scwsjkw/zcwj11/2019/11/27/996f53681194442a9b4a7fee192ba902.shtml (accessed November 27, 2019).
13. Lai YF, Lim YW, Sen Kuan W, Goh J, Soong JTY, Shorey S, et al. Asian attitudes and perceptions toward hospital-at-home: a cross-sectional study. Front Public Health. (2021) 9:704465. doi: 10.3389/fpubh.2021.704465
14. Harris-Kojetin L, Sengupta M, Park-Lee E, Valverde R, Caffrey C, Rome V, et al. Long-term care providers and services users in the United States: data from the National Study of Long-Term Care Providers, 2013-2014. Vital Health Stat 3. (2016) 14:38;x–xii; 1–105.
15. Centers for Medicare and Medicaid Services. Medicare and Medicaid Statistical Supplement. (2012).
16. Gutkin C. Supporting Canada's family physicians - the public has spoken; is anybody listening? Can Fam Physician. (2006) 52:548.
17. Chua CMS, Ko SQ, Lai YF, Lim YW, Shorey S. Perceptions of stakeholders toward “hospital at home” program in Singapore: a descriptive qualitative study. J Patient Saf. (2022) 18:e606–12. doi: 10.1097/PTS.0000000000000890
18. Andersen R, Newman JF. Societal and individual determinants of medical care utilization in United-States. Milbank Mem Fund Q Health Soc. (1973) 51:95–124. doi: 10.2307/3349613
20. Nguyen M, Cerasani M, Dinka LA, Rodriguez JA, Omoruan M, Acosta E, et al. Association of demographic factors and medical school experiences with students' intention to pursue a surgical specialty and practice in underserved areas. JAMA Surg. (2021). doi: 10.1001/jamasurg.2021.4898
21. Yu G, Chen Z, Wu J, Tan Y. Medical decision support system for cancer treatment in precision medicine in developing countries. Expert Syst Appl. (2021) 186:115725. doi: 10.1016/j.eswa.2021.115725
22. Moitra S, Foraster M, Arbillaga-Etxarri A, Marin A, Barberan-Garcia A, Rodriguez-Chiaradia DA, et al. Roles of the physical environment in health-related quality of life in with chronic obstructive disease. Environ Res. (2022) 203:111828. doi: 10.1016/j.envres.2021.111828
23. Heinik J, Avnon M, Hes JP. Length of hospitalization and disposition of elderly vs younger delirium patients in psychiatric hospitals. Isr J Psychiatry Relat Sci. (1997) 34:115–8.
25. Tkacheva ON, Runikhina AK, Vertkin AL, Voronina IV, Sharashkina AV, Mkhitaryan LA, et al. The diagnosis of delirium in an acute-care hospital in Moscow: what does the Pandora's box contain. Clin Interv Aging. (2017) 12:343–9. doi: 10.2147/CIA.S123177
26. Bi S-H, Tang W, Rigodanzo-Massey N, Young BA, Blagg CR, Wang T, et al. Infection-related hospitalizations in home hemodialysis patients. Blood Purif. (2015) 40:187–93. doi: 10.1159/000433517
27. Drozd M, Garland E, Walker AMN, Slater TA, Koshy A, Straw S, et al. Infection-related hospitalization in heart failure with reduced ejection fraction a prospective observational cohort study. Circ Heart Fail. (2020) 13:e006746. doi: 10.1161/CIRCHEARTFAILURE.119.006746
28. Zare M, Ghodsbin F, Jahanbin I, Ariafar A, Keshavarzi S, Izadi T. The effect of health belief model-based education on knowledge and prostate cancer screening behaviors: a randomized controlled trial. Int J Community Based Nurs Midwifery. (2016) 4:57–68.
29. Wang C, Yan S, Jiang H, Nie Z, Miller M, He Y, et al. Residents' willingness to maintain contracts with family doctors: a cross-sectional study in China. J Gen Intern Med. (2021) 36:622–31. doi: 10.1007/s11606-020-06306-y
30. Munoz CA. Socioeconomic determinants of health insurance status among Puerto Ricans. P R Health Sci J. (1988) 7:27–30.
31. Ross CE, Mirowsky J. Does medical insurance contribute to socioeconomic differentials in health? Milbank Q. (2000) 78:291–321. doi: 10.1111/1468-0009.00171
32. Hoel K-A, Rokstad AMM, Feiring IH, Lichtwarck B, Selbaek G, Bergh S. Person-centered dementia care in home care services - highly recommended but still challenging to obtain: a qualitative interview study. BMC Health Serv Res. (2021) 21:723. doi: 10.1186/s12913-021-06722-8
33. Marsteller JA, Burton L, Mader SL, Naughton B, Burl J, Guido S, et al. Health care provider evaluation of a substitutive model of hospital at home. Med Care. (2009) 47:979–85. doi: 10.1097/MLR.0b013e31819c93fc
34. Zhao W. The research progress of domestic sickbed management norms and system. Chin J Urban Rural Enterp Hyg. (2016) 3:13–5. doi: 10.16286/j/1003-5052.2016.03.006
35. Tao C, Nengliang Y, Mingzhu S, Sheng N, Meng B, Ziyuan M. Challenges of home-based medical care in China: a telephone interview from the perspectives of home care providers. Chin Gen Pract. (2020) 23:1459–65. doi: 10.12114/j.issn.1007-9572.2020.00.214
36. Lv G, Zhao M. The more the rating, the more the imbalance? Research on hospital rating and human resource allocation of doctors in China. Bus Manag J. (2018) 40:110–27. doi: 10.19616/j.cnki.bmj.2018.0.007
37. Vale JS, Franco AI, Oliveira CV, Araujo I, Sousa D. Hospital at home: an overview of literature. Home Health Care Manag Pract. (2020) 32:118–23. doi: 10.1177/1084822319880930
38. Claesson M, Josefsson K, Jonasson L-L. 'My registered nurse': Older people's experiences of registered nurses' leadership close to them in community home care in Sweden. Int J Older People Nurs. (2021) 16:e12399. doi: 10.1111/opn.12399
39. Winkleby MA, Jatulis DE, Frank E, Fortmann SP. Socioeconomic-status and health - how education, income, and occupation contribute to risk-factors for cardiovascular-disease. Am J Public Health. (1992) 82:816–20. doi: 10.2105/AJPH.82.6.816
40. Province TPsGoS,. Press Conference on Main Data Results of the Seventh National Population Census in Sichuan Province. (2021). Available online at: https://www.sc.gov.cn/10462/705/707/2021/5/27/3ef3323416694f98a236021554b82406.shtml (accessed May 27, 2021).
Keywords: home care, hospital-based, home care service, willingness, attitude, awareness
Citation: Xu S, Wang J, Wang Y, Wang M, Huang X and Huang H (2022) Individuals' Awareness of and Willingness to Accept Hospital-at-Home Services and Related Factors: A Cross-Sectional Study. Front. Public Health 10:823384. doi: 10.3389/fpubh.2022.823384
Received: 27 November 2021; Accepted: 03 May 2022;
Published: 27 May 2022.
Edited by:
Simiao Chen, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Qiushi Chen, The Pennsylvania State University (PSU), United StatesXiaoxv Yin, Huazhong University of Science and Technology, China
Copyright © 2022 Xu, Wang, Wang, Wang, Huang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hao Huang, aGFvaHVhbmcyMDIxQDEyNi5jb20=