 Yi-Chen Chiang
Yi-Chen Chiang Xian Li
Xian Li Chun-Yang Lee
Chun-Yang Lee Chi-Chen Wu
Chi-Chen Wu Hsing-Yi Chang
Hsing-Yi Chang Shuoxun Zhang
Shuoxun Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 29 March 2022
Sec. Public Health Education and Promotion
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.818894
Background: Drug use among adolescents are still crucial issues that endanger their lifetime health. Evidence concerning the interpersonal-related factors influencing youngsters' experimental drug use behavior, especially from longitudinal and school-based prospective cohort studies, is insufficient. We aimed to describe the annual incidence rate and mean annual incidence rate of experimental drug use from childhood to adolescence by education stage, clarify the risk in childhood and examine the longitudinal relationship between social attachment factors and experimental drug use.
Materials and Methods: The data were derived from the 1st to 11th wave of the longitudinal study. In total, 1,106 respondents aged 19–20-year-old were followed up for 11 years (from 9 to 10-year-old) in Taiwan. A survival analysis was used to analyze the time-invarying/time-dependent effects of social attachment factors on experimental drug use.
Results: The mean annual incidence rate of experimental drug use from childhood to adolescence was 6.8‰. The incidence increased over time and was the highest in the first year of university (19.3‰). Boys were more likely to use drugs than girls. A low degree of self-perceived likeability in childhood was a risk factor influencing experimental drug use. On average, a low degree of parental supervision and a high degree of family conflict were both influential risk factors. According to the time-dependent models, a high degree of parental supervision, a high degree of family support and a low degree of family conflict in the current year can protect children and adolescents from drug use, whereas a sustained low degree of parental supervision and a high degree of family conflict may promote students' experimental drug use.
Conclusion: Parents should be informed and educated to avoid family conflict during childhood, maintain consistent supervision of their children's behavior, provide adequate family support, and pay attention to their children's interpersonal relationships in school. Teachers should focus on the social attachment status of their students while considering their attachments to their families and peers.
Drug use is increasing worldwide, which can be manifested by the augmenting total number and proportion of drug users. In 2018, an estimated 269 million people worldwide used drugs at least once in the previous year, corresponding to 5.4% of the global population aged 15–64 years (1). The estimated number of any drug users in the past year globally rose from 210 million to 269 million during the period between 2009 and 2018; thus, the growth rate of drug consumption was more than a quarter (28%) (1). In 2018, an estimated 35.6 million people suffered from drug use disorders globally (2). There is a strong link between drug use disorders and psychiatric comorbidities, and these conditions often share common risk factors (3–6), such as family structure and functioning, family psychiatric and substance abuse history, traumatic events, peer relations and peer group characteristics (5). In addition, the COVID-19 pandemic has raised huge concerns for the mental health of an entire generation of children and young people (7), which may be related to the adoption of anti-epidemic measures such as lockdown, school closure, and social distancing. Mandatory social distancing policies have reduced the accessibility of drugs, and adolescents' drug use has decreased (8, 9); while subsequent small-scale unblocking might bring about experimental drug use among adolescents. Drug use have become a public health issue with a serious impact on people's development and social security. It is therefore necessary to further explore the prevalence and negative effects of drug use among children and adolescents.
Adolescence is an important transitional period during people's lifespan characterized by physical and psychological development. For some adolescents, adolescence is also a time of increased vulnerability to the initiation of drug use. In 2018, it was estimated that there were 13 million past-year users of any drug among students aged 15–16 years globally (10). According to studies in the United States, New Zealand and Australia, this rate increased to 17% among lifetime users who started using cannabis in adolescence (11). Based on the Monitoring the Future Survey (MTF) of America, 26.4, 40.8, and 51.8% of the respondents had tried an illicit drug in 8th grade, 10th grade, and 12th grade, respectively (12). A study conducted in Canada followed 4,885 adolescents throughout secondary school and found that 17.6% of these adolescents reported using illicit drugs in 7th grade (13). In a survey involving 2,974 Japanese junior and senior high school students, 3.8% reported using illicit drugs (14). A national survey of drug use in China found that among the 2.553 million reported drug users, 0.6% were under the age of 18 (15). A 3-year survey conducted in Taiwan indicated that 1.5% of the 2,375 students previously used drugs (16). This difference in the prevalence of drug use may be due to cultural differences or prevention policies. For example, students in Taiwan complete a series of drug prevention courses at various stages since elementary school. However, research focusing on the onset of drug use behavior among children and adolescents is insufficient, thus deserving further attention.
The long-term use of drugs can lead to physiological tolerance and psychological dependence, resulting in addiction. Adolescent drug use entails health risks (17). It is significantly associated with other leading causes of morbidity and mortality during adolescence, including depression, anxiety, unprotected sex, suicide attempts, and accidents (18–21). Drug use during adolescent was associated with their cognitive control and emotion regulation (22). The results of a nationally representative sample survey of 10th graders in the United States showed that polysubstance users reported elevated levels of somatic and depressive symptoms (23). Hence, this study further explored the influencing factors of drug use among children and adolescents.
Humans depend on social relationships for survival and wellbeing throughout life (24). Social control theory indicates that “social attachment” is the earliest social connection in children. “Attachment” refers to the affective relationships that one has with other people (25). Social attachment has the basic attributes and functions of attachment, which focuses on the emotional characteristics and behavioral tendencies that individuals form with specific objects during their growth (26). Social attachment can be considered as a social bond, and this bond can be either secure or insecure (27, 28). A secure bond can be described as a balanced interaction in which the interactors are neither too distant nor too close (29). It provides a sense of wellbeing, intimacy, or security to interactors (30). Positive bonds to society deter adolescents from substance use (31).
Attachment theory, which is formulated by Bowlby (32–34), conceptualizes the tendency of individuals to build strong emotional bonds with specific others and understands varied forms of affective disturbance (e.g., anger, despair, and detachment). Attachment relationships are usually formed during infancy and tend to be relatively stable after adolescence (35). Hence, attachment relationships from childhood to adolescence are extremely important (32). As social attachments increase, participation in health protective behaviors increases (36). Notably, social attachments in childhood and adolescence are mainly derived from family and friends (37). Like social attachments, social learning theory emphasizes that cognition affecting behaviors stem from observing others (38, 39). For children and adolescents, the most influential role models are parents, peers, and siblings (40). Vicarious learning requires an identification process when the students match or identify themselves with the punishment/reward target so that they will subsequently have contiguous association of the sensory event. Their self-controlling responses can be modified and reinforced by models' self-evaluative and self-punitive reactions to deviation (41). During the identification process, the child/adolescent decides which actions should and should not be done based on the perceived consequences of the actions. In order to reinforce constructive parent-child/peer interaction and dynamic, students tend to enhance their positive behaviors and inhibit non-expected behaviors.
Family environment and atmosphere have an impact on the development and behavior of children and adolescents (42). Children may model parents' behaviors which have greater or lesser access to health-harming substances, receive specific encouragement or discouragement to participate in certain behaviors, and receive family support to attempt and alter behaviors (43). Research has documented that poor family interactions, low levels of family supervision, and parental use of punishment for discipline all increase the risk of future substance use (44–46). Similarly, peer influence was a significant factor on adolescents' participation in health-related behaviors such as substance abuse (47, 48) and drinking behavior (49). Youngsters who were popular and liked within their peer group were rated as more competent within their closest friendship (50). Students who lack supportive friendship network and have low adaptability to school are more likely to be exposed to drugs (36, 51, 52). In particular, perceived likeability impacts children's subsequent substance abuse and dependence (53). Therefore, the social attachment of this study includes four aspects: parental supervision, family support, family conflict and perceived likability. Clearly, social attachment is critical to children's and adolescents' healthy development. However, previous studies did not examine the impact of social attachment on children's or adolescents' substance use from long-term perspectives, especially in multiyear prospective cohort studies.
The prevalence of drug use among children and adolescents reviewed in the above literature is primarily based on cross-sectional data, and it is difficult to see changes in drug use at different consecutive stages. Based on 11-year longitudinal data, the present study was meant to determine the new incidence of experimental drug use among students by year and education stage. According to the continuous tracking of periodic fluctuations in drug use among children and adolescents, we hypothesized that adolescents with weaker social connections were more likely to start drug use than their counterparts. This study further examined the impact of students' social attachment factors on experimental drug use by longitudinal cohort. Social attachment factors involved their parents and peers (in childhood and time-dependent contexts), i.e., parental supervision, family support, family conflict, and perceived likeability. Therefore, our objectives were to (a) describe the annual incidence rate and mean annual incidence rate of experimental drug use from childhood to adolescence by education stage; and (b) examine the longitudinal relationship between social attachment factors and experimental drug use behavior throughout the education duration, including early/average exposure and simultaneous/lag effects.
The data were derived from the 1st to 11th wave of the longitudinal study Child and Adolescent Behaviors in Long-term Evolution (CABLE), which was initiated in 2001 (54). There were 152 primary schools in urban area and 79 primary schools in rural area. There were only a few private primary schools in these two areas (10/152 in urban and 1/79 in rural). Differing from students attending public schools, those who attended private schools have relatively good family conditions. In addition, the overall teaching mode in private schools might differ from the compulsory education system of public schools. Furthermore, most students attended public schools. Thus, these private schools were excluded from the sample population in the cohort study after considering the comparability of the study subjects. Based on the number of first-grade students, the schools were divided into small (50–199 students), medium-sized (200–399 students) and large (more than 400 students) schools. Schools with fewer than 50 students were not included in the sample population due to insufficient numbers. Then, the schools were randomly selected to participate in the survey. To ensure that the numbers of children chosen from each type of school were approximately equal, six small schools, two medium-sized schools and one large school were selected from each location. Finally, eighteen public elementary schools from urban area and rural area were randomly selected. The school/parents/students were informed of the purpose of the cohort study, and written informed consent for the annual follow-up survey was obtained from the students' parents before the baseline survey. Since this article presents a secondary analysis, the data were released with deidentification to protect the privacy of the children. The study team did not intervene or inform the teachers/parents of the students' actual answers.
All 3,612 fourth graders aged 9–10 years were selected. Among them, 2,125 students provided parental permission in 1st wave (58.83% agreed to participate). Moreover, 2,076 students completed their questionnaires (response rate = 97.69%). The annual losses to follow-ups were due to absences from school, illnesses, refusals to participate, etc. (annual response rate = ~78.37–98.17%, Figure 1). Eventually, in total, 1,106 respondents aged 19–20 years completed an annual survey (11-year follow-up rate = 53.28%). Fortunately, when comparing the distributions of the students' sex, parents' education levels and students' drug use behaviors between “the first-wave data” and “the 11-year follow-up data”, the results were non-significant. We assumed that cohort data were randomly missing. Further details of the sampling procedures of the cohort study have been previously described (55). Furthermore, participants completed a follow-up questionnaire in classes/schools before their senior high school years. Trained interviewers answered questions posed by the students, which verified that they understood each question. As the participants grew up during senior-high-school/college years, they were followed up face-to-face at home/school. Because the students were enrolled in different middle schools and universities after their elementary school years and because they could have different experiences, the clustering effect was expected to be at a minimal level.
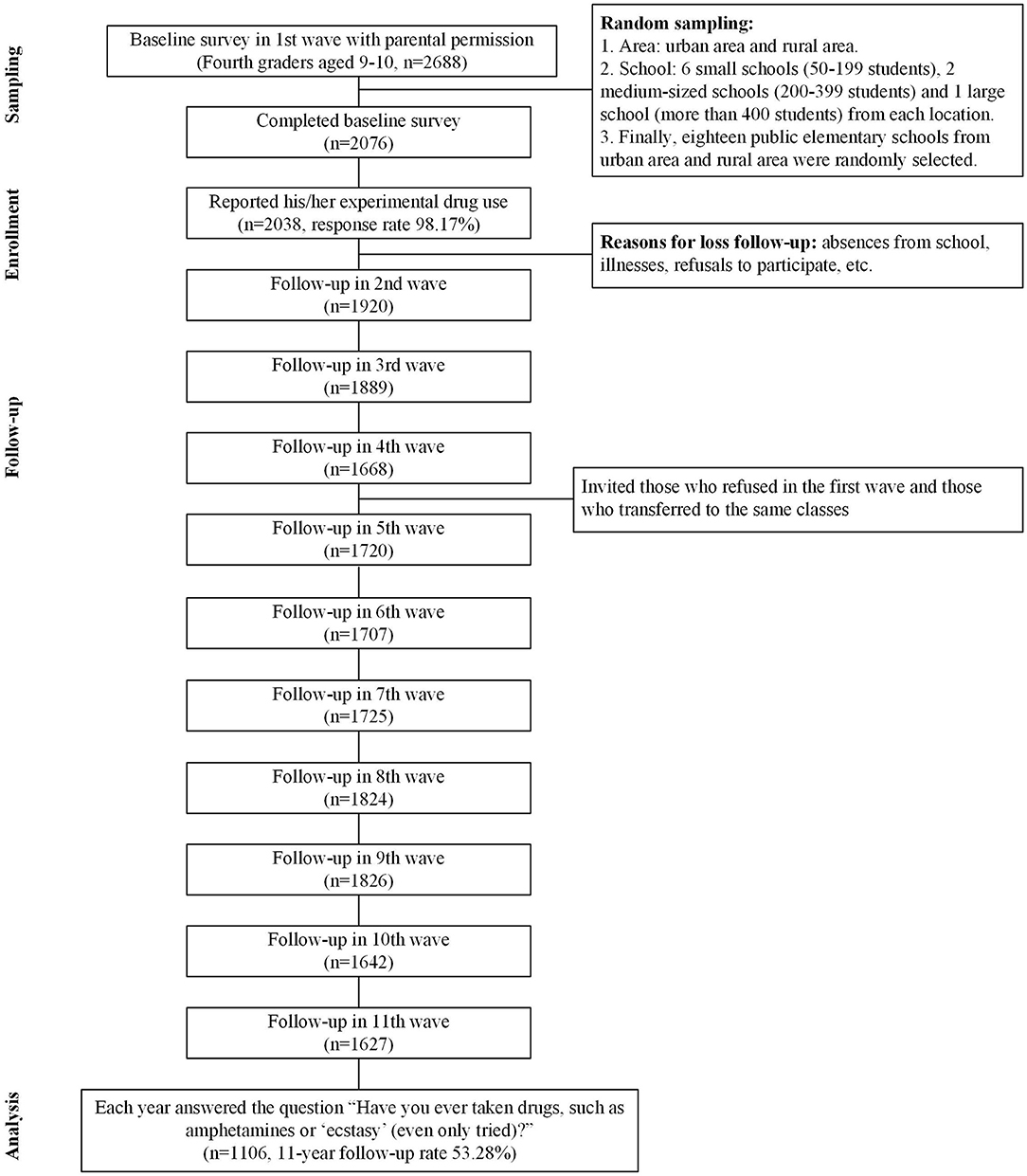
Figure 1. Flowchart.
Drug use refer to the use of substances controlled under the international drug control conventions for non-medical (56). Experimental drug use is defined as having tried a drug, which may develop into habitual drug use through enduring exposure to drugs, or may be reversed with timely intervention (57, 58). This variable was measured by asking the students “Have you ever taken drugs, such as amphetamines or “ecstasy” (even only tried)?”. Among the annual surveys, the response options differed depending on the age of the respondents: (a) The students in elementary school grade 4 or grade 5 responded using a five-point scale with “never” = 1, “not recently but in the past” = 2, “once or twice in the past month” = 3, “many times in the past month” = 4, and “every day in the past month” = 5, and (b) the students from grade 6 to grade 14 responded using a six-point scale with “never” = 1, “not in the past year but before” = 2, “not in the past month but before” = 3, “once or twice in the past month” = 4, “many times in the past month” = 5, and “every day in the past month” = 6. The time (school grade) of experimental drug use was used as an outcome variable in the survival analysis. Experimental drug use at baseline included students before the fourth grade. Therefore, these students were asked the exact year of the experimental drug use that occurred before grade 4.
The independent variables included parental supervision, family support, family conflict, and perceived likeability. These four factors were measured consistently in most of the 11 years, for they can be used to test their long-term influence on the students' experimental drug use. The measurement and scoring of each item were conducted as follows.
Parental supervision was measured from grade 6 to grade 9 using a scale with three items, including “Does your mom or dad know what you do after school before returning home every day/who you usually go out with/what you do in your free time?”. These items were scored on a four-point scale with higher scores indicating higher levels of parental supervision.
Family support was measured annually in our 11-year data set by using six items, including “Does your mom or dad care for you when you are feeling unwell?” and “Does your mom or dad comfort you when you are feeling unhappy or sad?” These items were scored on a four-point scale with higher overall scores indicating higher levels of family support.
Family conflict was measured from grade 4 to grade 9 by using five items, including “In the past month, did your parents hit each other when they were fighting?”. These items were scored on a four-point scale with higher overall scores indicating higher levels of family conflict.
Perceived likeability was measured annually in our 11-year data set by using five items, including “In the past two weeks, were you afraid that your friends or other people don't like you/people are making fun of you”. These items were scored on a three-point scale with higher scores indicating that the respondent was more likely to perceive that they were not well-liked (i.e., low likeability).
These scales all demonstrated acceptable reliability with Cronbach's α values of 0.69–0.83 for parental supervision, Cronbach's α values of 0.80–0.92 for family support, and Cronbach's α values of 0.65–0.84 for perceived likeability. In the confirmatory factor analysis (CFA), parental supervision only includes three items, so degrees of freedom (df) = 0, which cannot provide the index of the goodness-of-fi; the factor loading values of the three items are 0.90–1.00 for parental supervision. The CFA results of family support showed: Adjusted Goodness of Fit Index (AGFI) = 0.99, Comparative Fit Index (CFI) = 0.99, Incremental Fit Index (IFI) = 0.99, Critical N (CN) = 809.45. The CFA results of perceived likeability showed: AGFI = 0.97, CFI = 0.94, IFI = 0.94, CN = 277.96. The above CFA results show that the scale is valid (59–61).
Although previous studies have suggested that students' drug use was associated with sex (62), subjective academic performance (63, 64), parents' education levels (65, 66), etc., these factors were not the focus of this study and were deemed as control variables.
Experimental drug use in the sample is described using frequencies and percentages. For the incidence of experimental drug use, the annual incidence rate refers to the number of newly reported experimental drug users in each year out of the total number of students who never used drugs up until the previous year, except for the annual incidence of experimental drug use in the first year, which represents the cumulative incidence (i.e., includes the frequency of drug use prior to grade 4). The independent variables are described using means and standard deviations. In this study, for those participants who answered more than half of the questions on a scale, we measured the individual average values of the remaining questions to replace the missing values (67, 68). Otherwise, these values were treated as completely missing. A Cox regression was used to examine the relationship between each variable and experimental drug use, which helped to figure out the causal relationship between the independent and dependent variables over time. We examined the proportional hazards assumption using the Schoenfeld test, and the results showed no violation of proportionality (Appendix 1). Thus, the proportional hazard model was used in this study.
To examine early/average exposure or the long-term effect, Cox proportional hazards models were created using the following two different approaches: (a) for the time-invarying covariates, model 1-1 assessed the hazards of early exposure in childhood, whereas model 1-2 assessed the hazards of the average exposure during the 11 years of follow-up, and (b) for the time-dependent covariates, model 2-1 examined the simultaneous effects, whereas model 2-2 examined the lag effects. Regarding those variables that were only assessed at early ages, we measured the average values. When considering only those variables that were measured in all years, we modeled these variables as time-dependent covariates. In addition, instead of replacing each missing value with a single value, a multiple imputation (MI) model replaced each missing value with a set of plausible values that represented the uncertainty of the correct value to impute (69, 70). Via comparisons between our analyzed data collected before and after the MI procedures (with the comparisons assessed via R software using the Amelia II strategy to replace the missing values), we found the results were similar (i.e., the differences in each HR value assessed before and after the MI were almost lower than 0.02). SAS software version 9.2 was employed for the statistical analysis.
As shown in Table 1, the respondents aged 9–10 years old were approximately half boys (51.4%) and half girls (48.6%). In total, 53.8% of the participants were from urban areas, and 46.2% of the participants were from rural areas.
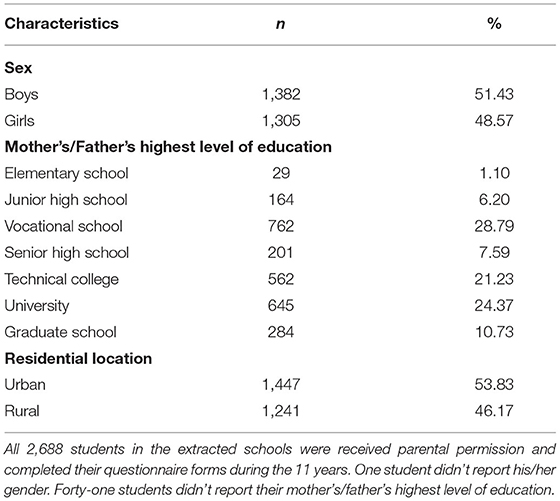
Table 1. Characteristics of the sample of fourth graders (aged 9–10 years) in the baseline survey (n = 2,688).
As shown in Table 2, the rate of drug use in 1st wave (21.7 per 1,000 persons) represents a cumulative incidence and includes the frequency of using drugs prior to 4th grade aged 9–10 years old. The highest mean annual incidence rates from 5th grade (aged 10–11 years old) to 14th grade (aged 19–20 years old) were observed in 13th grade (aged 18–19 years old), was 19.3‰. This finding indicates that new cases of experimental drug use were the highest upon attending university. The mean annual incidence rates gradually increased by education stage. In addition, there were two peaks of students' experimental drug use: 9th grade aged 14–15 years old (the third year of junior high school) and 13th grade aged 18–19 years old (the first year of university) (Figure 2). Experimental drug use in senior high school and university was much higher than that in the other stages (Table 2).
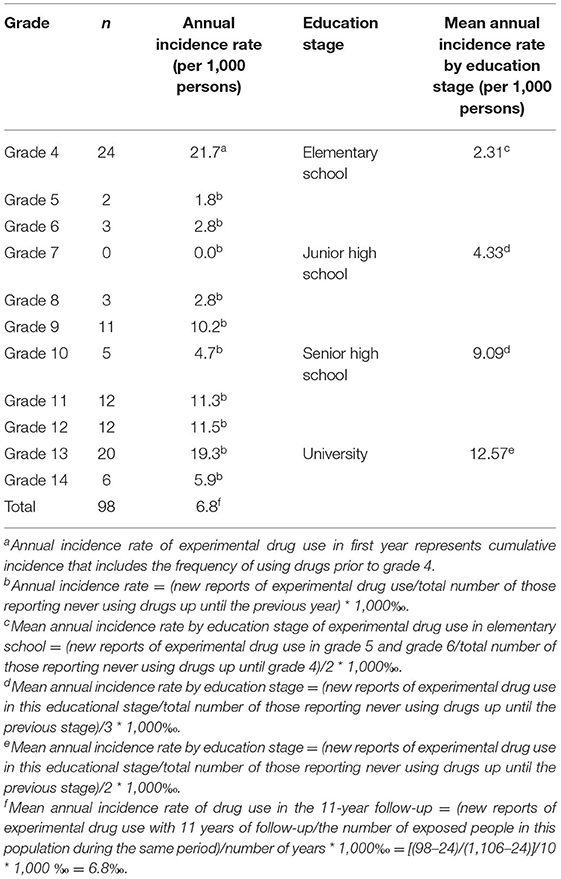
Table 2. Frequency, annual incidence rate and mean stage incidence rate per 1,000 persons of experimental drug use among 11-year follow-up participants.
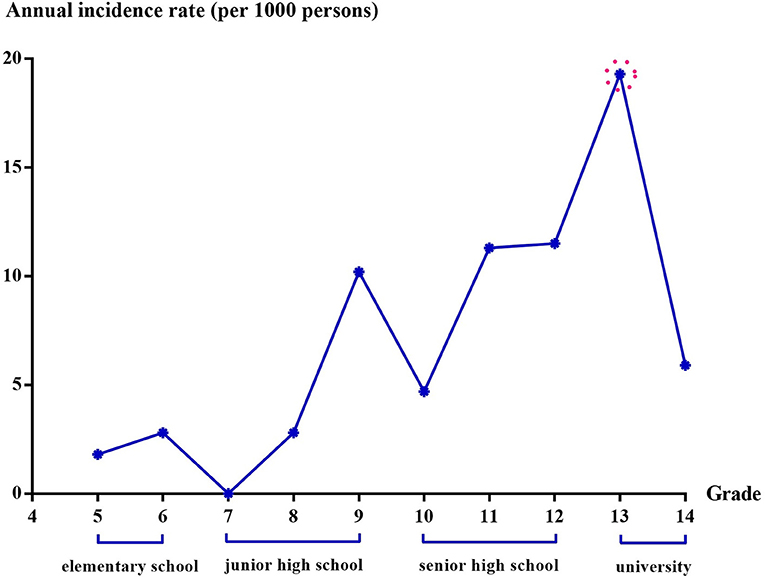
Figure 2. Annual incidence rate of experimental drug use.
As shown in Table 3, boys were significantly more likely to start using drugs during the follow-up than girls, and students living in urban areas were more likely to consume drugs than students living in rural areas. Model 1-1 revealed that a low perceived likeability in childhood was a risk factor influencing experimental drug use [hazard ratio (HR) = 1.15, 95% CI = 1.02–1.30]. Students with worse subjective academic performance (HR = 0.73, 95% CI = 0.51–1.04) in elementary school were marginally and significantly more likely to start using drugs. Besides, model 1-2 indicated that low parental supervision (HR = 0.83, 95% CI = 0.71–0.98) and high family conflict (HR = 1.24, 95% CI = 1.01–1.52) on average were both risk factors influencing experimental drug use.
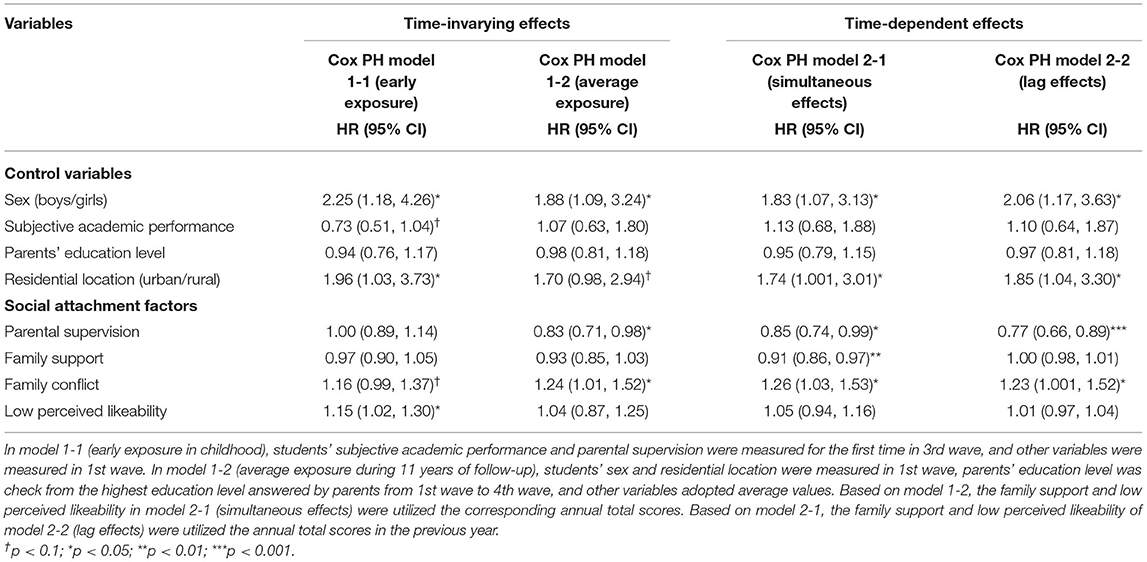
Table 3. Relationship between social attachment factors at different time points and experimental drug use: survival analysis results.
According to the time-dependent models, model 2-1 implied that high parental supervision (HR = 0.85, 95% CI = 0.74–0.99), high family support (HR = 0.91, 95% CI = 0.86–0.97) and low family conflict (HR = 1.26, 95% CI = 1.03–1.53) in the current year could protect children and adolescents from drug-use activities. In model 2-2, we considered the lag effects of social attachment factors on experimental drug use and discovered that sustained high parental supervision (HR = 0.77, 95% CI = 0.66–0.89) and low family conflict (HR = 1.23, 95% CI = 1.001–1.52) may reduce students' experimental drug use rates.
Based on the above analysis, sex as a control variable was significant in each model. Given the possible differential risk/protective effects of sex, time-dependent effects were further examined by a gender-stratified analysis. The model with simultaneous effects showed that boys who were less supported by their family were more likely to have experimental drug use, while girls who were less supervised by their parents were more likely to have experimental drug use. The results of the lag effects model showed that both boys and girls were more likely to develop experimental drug use in the next year if they had low degree of parental supervision, but the significance of the model was p = 0.001 for girls and p = 0.048 for boys.
Based on our 11-year prospective cohort study, the new incidences of experimental drug use among students (both annually and during each educational stage), and the time-dependent effects could be assessed. There were two peaks of students' experimental drug use: in grades 9 (i.e., students' first experience with entrance examinations) and 13 (i.e., the first-time students left their family and enjoyed life/freedom alone). Notably, experimental drug use in senior high school and university was much higher than before. Moreover, our findings revealed the importance of social attachment for preventing students from experimentally consuming drugs. It was essential to avoid family conflict/low perceived likeability during childhood and to emphasize the necessity of sustained parental supervision and sustained family support.
Most research suggests that early (12–14 years old) to late (15–17 years old) adolescence is a critical risk period for the initiation of substance use (71). Some researchers indicated that adolescents first start using drugs between the ages of 13 and 17 years (72). In this study, we found that both the third year of junior high school and the first year of university were the time points when experimental drug use increased. There is excessive academic pressure in the third year of junior high school, and a few students may use drugs to escape the pressure (i.e., there may be other related reasons). A qualitative study of 38 adolescents using focus interviews found that academic pressure is a major source of stress. These adolescents attempted to relieve stress by using substances, especially when they felt that they could not succeed (73). Furthermore, with decreased parental supervision and increased autonomy, a small number of students who enter university may exhibit more participation in high-risk behaviors such as drug use (74, 75). In this study, students' drug use decreased in the first years of junior and senior high school likely because during these two periods, students are entering a new stage of learning, are adapting to the environment and do not yet feel great pressure due to learning or peer relationship distress. Hence, it suggests that we should pay more attention to the status of students at each stage to protect them from exposure to drugs.
As is currently known, social attachments are important (including attachment relationships between family members/peers and adolescents) in shaping adolescents' behaviors. Because youths enjoy maintaining social relationships with their families and friends, the risk behaviors of children and adolescents are especially affected by or imitated from their parents and peers. For example, studies have shown that the usage of amphetamine, cocaine and cannabis among adolescents before attending university was mostly associated with illicit drug use by their parents and friends (76). Stronger social attachments may lead to the avoidance of illegal and heavy substance use (31). Some studies pointed out that the strongest protective factors against substance use among senior high school students are individual factors (such as substance use refusal self-efficacy and self-control), peer factors (such as attitudes against substance use and peer drug use), and family support (such as the ability of parents to listen) (77, 78). Among these factors, the factors related to the family environment are particularly important (79). The results of this study confirmed the importance of sustained family support/parental supervision in reducing substance use among children and adolescents. The negative impact of poor parental involvement in children's education on adolescents' substance use before they attend university should not be ignored (76). Parents should participate more in their children's studies and life before they attend university to prevent their children's hedonism, which can reduce their opportunity to access illicit drugs.
Moreover, our study revealed that low perceived likeability from peers was an influential factor of experimental drug use, especially for exposure in childhood. Those with high levels of family conflict in grade 4 were at an increased risk of experimental drug use during the follow-up, which was consistent with previous research findings (62). Regarding the measurement of family conflict, the types covered in this study included parents fighting with each other verbally, siblings fighting with each other verbally or physically, and adolescents fighting with parents or other adults in the family. Future research could further investigate this relationship by grouping family conflict. Past research has suggested that girls with low perceived likeability are more likely to develop future substance use as adults (52). Similarly, our study discovered that low perceived likeability in grade 4 was associated with an increased risk of experimental drug use during the follow-up. Therefore, high levels of family conflict and low perceived likeability are risk factors for experimental drug use in students.
Parents may raise their children differently by gender because of the stereotype and social expectations for boys/girls. Studies have found that compared with girls, boys are more likely to engage in high-risk behaviors, such as aggressive behavior and drinking (80–82); while girls tend to show empathic behaviors and prosocial behaviors. Similarly, our study revealed that boys were more likely than girls to consume drugs. In addition, continuous parental supervision of students, including both boys and girls, from childhood to adolescence is necessary to reduce their possibility of exposure to drugs and then decrease the likelihood of experimental drug use. For boys, appropriate family support is also a key protective factor in avoiding experimental drug use. This study separated different social attachment factors for experimental drug use behaviors among boys and girls, which suggested that we should take gender-specific measures to prevent students' experimental drug use behaviors in the beginning.
While drug use may cause harm and further addiction, it is a gradual process and it is not absolute. It should be taken into account that many people who have ever consumed drugs a time may not do this again, only use occasionally or use casually without developing any significant issues. Based on the findings of the Monitoring the Future Survey (MTF) of America from 1975 to 2016, most 12th graders disapproved of the regular use of any illicit drugs, and fewer respondents uncovered disapproval of experimental or occasional use than of regular use (83), which may be related to their change trends in the perceived risk of use (84). A previous study revealed that compared to students who reported “often” drug use, those who reported “once or twice” or “sometimes” use and those who never endorsed use were more similar to each other (85), such as both reported high levels of hope for the future (86). Because the cohort study just reported children's and adolescents' experimental drug use, those who initiated the use of illicit drugs might not continue use, not necessarily become an addictive behavior. Therefore, the results of the current study should be interpreted with caution.
The main strength of this study is its long-term prospective cohort design, which allowed us to discover the annual incidence rate and mean annual incidence rate of experimental drug use from childhood to adolescence by education stage, and examine the longitudinal effects of social attachment factors on experimental drug use behavior. Particularly, this cohort study was based on a school-based survey focusing on non-clinical samples. Our findings are noteworthy. However, some limitations still exist. First, cohort studies inevitably experience a loss to follow-up over more than 10 years of visits. Fortunately, the differences in the distributions of several important variables (as previously mentioned between “the first-wave data” and “the 11-year follow-up data”) were non-significant, and there were no differences in the HRs before and after the MI procedures. Second, the questionnaire used in the present study focused on general problems faced by children and adolescents in campus and family lifestyles. The questionnaire was not specific to drug problems; thus, we were unable to obtain more covariates and provide further explanation. Third, because the questionnaire asks about children's behavior over time, recall bias could occur possibly due to incorrect long-term memory. We believe that recall bias is likely minimal since drug use is a rare behavior that is not easily forgotten. As drug use is a sensitive issue, students might not report it honestly. Therefore, reporting bias could exist. In this regard, our well-trained interviewers established good communication with the interviewees at the beginning of the questionnaire to reduce their defensiveness, informed them that their privacy would be fully protected and that the content of the questionnaire would not reflect personal information, and placed some sensitive questions at the back of the questionnaire. Fourth, this study is a school-based longitudinal follow-up study, and there may be attrition bias due to students dropping out. This limitation needs to be taken into account when interpreting the results. Finally, this study is also limited by the different measurement approaches used to assess particular items across the years. Therefore, when using time-independent covariates, if the items were not measured in 1st wave, variable values from the closest available year were used. When using time-dependent covariates, the values of the variables from the preceding year were used.
Based on the findings of this study concerning the importance of social attachment, we should fully mobilize the positive forces of family, peers and school to create a healthy environment for children and adolescents and even create a positive social climate. For every dollar spent on prevention, at least ten dollars can be saved in future health, social and crime costs (87). In terms of family, according to the United Nations Office on Drugs and Crime (UNODC), parents are important because families are a primary source of socialization and parental opinion can either reinforce or countermand the messages conveyed by drug abuse prevention programmes (88). Parents should be encouraged to use a warm child-rearing style with the help of parenting skills programmes which support parents in being better parents (89). What's more, parents should take the initiative to disseminate correct health information to their children and ensure adequate parent-child communication to enhance family bonding. Regarding peers, children and adolescents are encouraged to monitor and support each other through mutual help groups to maximize the positive influence of peers in their social network. Regarding school, drug-related learning outcomes should be addressed in the context of the health curriculum or other appropriate learning areas (90). Starting with the ongoing comprehensive and developmental elements that encourage the development of personal and social skills and values, the designed curriculum should cover adolescent development, stress coping, sexuality, and collaboration between home and school and personal relationships.
In summary, the risk of experimental drug use increases with age but may decrease due to protective factors. Additional prevention resources for young people exposed to multiple contextual risk factors (even in the absence of risk behaviors) from childhood to adolescence were offered by Wang et al. (91). Hence, preventative strategies should be implemented at early stages to avoid the onset of drug-use behaviors among students. Firstly, we recommend that parents expand efforts to lower conflict among families or relatives and provide children with sustained support and behavioral supervision. It is also necessary to understand their child's acceptance from others, to provide emotional support and effective communication skills when their child experiences difficulties. Secondly, teachers should focus on the social attachment status of their students while considering their attachments to their families and peers. Particularly, it is crucial to launch continuous and cross-stage drug-use denial campaigns aiming to prevent drugs from entering school campuses. Thirdly, relevant government departments should formulate corresponding policies, such as advocating health education courses or activities becoming compulsory credits, establishing a support association or counseling services aiming to sustain increases in students' drug refusal efficacy as well as health consciousness, and nurturing conflict resolution and stress management skills in children and families. Finally, although the first attempt at drugs does not mean that they will become dependent or drug abusers in the future, as far as the prevention of drug use by children and adolescents is concerned, it is still necessary to avoid the opportunity of the first try. Stigma is not as important as providing supportive environment to help children who want to get out of drug use.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The studies involving human participants were reviewed and approved by Institutional Review Board in National Health Research Institutes in Taiwan (No. EC9009003). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Y-CC, XL, C-CW, and H-YC were major contributors in conception and design of the study. Y-CC, C-CW, and H-YC participated in the data collection. Y-CC, XL, C-YL, SZ, and H-YC made contributions to data analysis and interpretation. Y-CC, XL, and C-YL drafted the manuscript. SZ, H-YC, and Y-CC supervised the study and critically reviewed the manuscript several times. Y-CC provides funding acquisition. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved and read and approved the final manuscript.
This article was funded by the Scientific Research Grant of Fujian Province of China (No. Z0230104). The sponsors of the project had no role in the study design, data collection, data analysis, data interpretation and in writing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to express sincere appreciation to all research assistants and investigators in CABLE for their assistance. Miss Yen-Ying Tsai is acknowledged for collation and preliminary analysis of data. The authors would especially like to thank the participants in the study for their time and willingness to participate.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.818894/full#supplementary-material
1. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2020: Drug Use and Health Consequences. Vienna: United Nations Publication, Sales No. E.20.XI.6 (Booklet 2) (2020). 10 p.
2. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2020: Drug Use and Health Consequences. Vienna: United Nations Publication, Sales No. E.20.XI.6 (Booklet 2), (2020). 11 p.
3. National Institute on Drug Abuse (NIDA). Common Comorbidities with Substance Use Disorders. Advancing Addiction Science. (2020) 1–45. Available online at: https://nida.nih.gov/download/1155/common-comorbidities-substance-use-disorders-research-report.pdf?v=5d6a5983e0e9353d46d01767fb20354b (accessed October 22, 2021).
4. Ross S, Peselow E. Co-occurring psychotic and addictive disorders. Clin Neuropharmacol. (2012) 35:235–43. doi: 10.1097/WNF.0b013e318261e193
5. Armstrong TD, Costello EJ. Community studies on adolescent substance use, abuse, or dependence and psychiatric comorbidity. J Consult Clin Psychol. (2002) 70:1224–39. doi: 10.1037/0022-006X.70.6.1224
6. Mueser KT, Gottlieb JD, Cather C, Glynn SM, Zarate R, Smith MF, et al. Antisocial personality disorder in people with co-occurring severe mental illness and substance use disorders: clinical, functional, and family relationship correlates. Psychosis. (2012) 4:52–62. doi: 10.1080/17522439.2011.639901
7. United Nations International Children's Fund (UNICEF). The State of the World's Children 2021. (2021). Available online at: https://data.unicef.org/resources/sowc-2021/ (accessed November 11, 2021).
8. Maurino MD, Eymann A, Santarsieri N, Vainman S, Krauss M, Catsicaris C, et al. Adolescent behaviors during the preventive and mandatory social isolation in Argentina in 2020. Arch Argent Pediatr. (2022) 120:39–45. doi: 10.5546/aap.2022.eng.39
9. Miech R, Patrick ME, Keyes K, O'Malley PM, Johnston L. Adolescent drug use before and during U.S. national COVID-19 social distancing policies. Drug Alcohol Depend. (2021) 226:108822. doi: 10.1016/j.drugalcdep.2021.108822
10. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2020: Drug Use and Health Consequences. Vienna: United Nations Publication, Sales No. E.20.XI.6 (Booklet 2) (2020). 14 p.
11. Anthony JC. The epidemiology of cannabis dependence. In: Roffman RA, Stephens RS, editors. Cannabis Dependence: Its Nature, Consequences and Treatment. Cambridge: Cambridge University Press (2006). p. 58–105.
12. Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future National Results on Adolescent Drug Use: Overview of Key Findings, 2011. Ann Arbor, MI: Institute for Social Research, University of Michigan (2012).
13. Briere FN, Fallu JS, Morizot J, Janosz M. Adolescent illicit drug use and subsequent academic and psychosocial adjustment: an examination of socially-mediated pathways. Drug Alcohol Depend. (2014) 135:45–51. doi: 10.1016/j.drugalcdep.2013.10.029
14. Matsumoto T, Imamura F. Self-injury in Japanese junior and senior high-school students: prevalence and association with substance use. Psychiatry Clin Neurosci. (2008) 62:123–5. doi: 10.1111/j.1440-1819.2007.01783.x
15. China National Narcotics Control Commission. Report on the Drug situation in China in 2017. (2018). Available online at: http://www.nncc626.com/2018-06/25/c_129900461.htm (accessed September 16, 2021).
16. Yang SL, Tzeng S, Tai SF, Ku YC. Illegal drug use among adolescents in schools and facilities: 3-year surveys in Taiwan. Asian J Criminol. (2020) 15:45–63. doi: 10.1007/s11417-019-09292-1
17. Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, et al. Youth Risk Behavior Surveillance - United States, 2007. MMWR Surveill Summaries. (2008) 57:1–131. Available online at: https://www.cdc.gov/mmwr/preview/mmwrhtml/ss5704a1.htm (accessed October 22, 2021).
18. Hingson RW, Edwards EM, Heeren T, Rosenbloom D. Age of drinking onset and injuries, motor vehicle crashes, and physical fights after drinking and when not drinking. Alcohol Clin Exp Res. (2009) 33:783–90. doi: 10.1111/j.1530-0277.2009.00896.x
19. National Institute on Drug Abuse. Drug Facts— Comorbidity: Addiction and Other Mental Disorders. (2021). Available online at: https://www.drugabuse.gov/publications/drugfacts/comorbidity-addiction-other-mental-disorders (accessed November 11, 2021).
20. Shrier LA, Harris SK, Sternberg M, Beardslee WR. Associations of depression, self-esteem, and substance use with sexual risk among adolescents. Prev Med. (2001) 33:179–89. doi: 10.1006/pmed.2001.0869
21. Swahn MH, Bossarte RM, Sullivent EE. Age of alcohol use initiation, suicidal behavior, and peer and dating violence victimization and perpetration among high-risk, seventh-grade adolescents. Pediatrics. (2008) 121:297–305. doi: 10.1542/peds.2006-2348
22. Shollenbarger S, Thomas AM, Wade NE, Gruber SA, Tapert SF, Filbey FM, et al. Intrinsic frontolimbic connectivity and mood symptoms in young adult cannabis users. Front Public Health. (2019) 7:311. doi: 10.3389/fpubh.2019.00311
23. Conway KP, Vullo GC, Nichter B, Wang J, Compton WM, Iannotti RJ, et al. Prevalence and patterns of polysubstance use in a nationally representative sample of 10th graders in the United States. J Adolesc Health. (2013) 52:716–23. doi: 10.1016/j.jadohealth.2012.12.006
24. Chumbley J, Steinhoff A. A computational perspective on social attachment. Infant Behav Dev. (2019) 54:85–98. doi: 10.1016/j.infbeh.2018.12.001
25. Oygard L, Klepp KI. Influences of social groups on eating patterns: a study among young adults. J Behav Med. (1996) 19:1–15. doi: 10.1007/BF01858171
26. Zhao X, Zhou M, Yu L, Liu Q. An attachment perspective conceptual model of virtual community continuance: surpass the cognitive judgment paradigm. Prediction. (2012) 31:14–20.
27. Scheff TJ. The emotional/relational world: shame and the social bond. In Turner JH, editor. Handbook of Sociological Theory. Boston, MA: Springer US (2001). p. 255–68.
28. Scheff TJ. Goffman Unbound! A New Paradigm for Social Science (Advancing the Sociological Imagination). London: Routledge (2006).
29. Mikkelsen BE, Romani AQ, Bo IG, Sudzina F, Brandão MP. Does it run in the family? How family background affects attachment styles for students in higher education. Int J Environ Res Public Health. (2021) 18:5135. doi: 10.3390/ijerph18105135
30. Lutgendorf SK, De Geest K, Bender D, Ahmed A, Goodheart MJ, Dahmoush L, et al. Social influences on clinical outcomes of patients with ovarian cancer. J Clin Oncol. (2012) 30:2885–90. doi: 10.1200/JCO.2011.39.4411
31. Wray-Lake L, Maggs JL, Johnston LD, Bachman JG, O'Malley PM, Schulenberg JE. Associations between community attachments and adolescent substance use in nationally representative samples. J Adolesc Health. (2012) 51:325–31. doi: 10.1016/j.jadohealth.2011.12.030
33. Bowlby J. Attachment and Loss: Vol. 2. Separation Anxiety and Anger. New York, NY: Basic Books (1973).
35. Biringen Z. Attachment theory and research: application to clinical practice. Am J Orthopsychiatry. (1994) 64:404–20. doi: 10.1037/h0079540
36. Weiss GL, Larsen DL, Kevin Baker W. The development of health protective behaviors among college students. J Behav Med. (1996) 19:143–61. doi: 10.1007/BF01857604
37. Holt MK, Espelage DL. Perceived social support among bullies, victims, and bully-victims. J Youth Adolesc. (2007) 36:984–94. doi: 10.1007/s10964-006-9153-3
38. Akers RL, Cochran JK. Adolescent marijuana use: a test of three theories of deviant behavior. Deviant Behav. (1985) 6:323–46. doi: 10.1080/01639625.1985.9967683
39. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
40. Collins RL, Ellickson PL. Integrating four theories of adolescent smoking. Substance Use Misuse. (2004) 39:179–209. doi: 10.1081/JA-120028487
41. Bandura A. Social-learning theory of identificatory processes. In Goslin DA, editor. Handbook of Socialization Theory and Research. Chicago, IL: Rand McNally (1969). p. 213–62.
42. Kit LM, Wu CI. Bad parents, bad kids? The linkages of adolescence violent behavior. Taiwan Soc. (2004) 7:1–46.
43. Sallis JF, Nader PR. Family determinants of health behavior. In Gochman DS, editor. Health Behavior: Emerging Research Perspectives. New York, NY: Plenum Press (1988). p. 103–24.
44. Wu GHM, Chong MY, Cheng ATA, Chen THH. Correlates of family, school, and peer variables with adolescent substance use in Taiwan. So Sci Med. (2007) 64:2594–600. doi: 10.1016/j.socscimed.2007.03.006
45. Piko BF, Kovács E. Do parents and school matter? Protective factors for adolescent substance use. Addict Behav. (2010) 35:53–6. doi: 10.1016/j.addbeh.2009.08.004
46. Chou P. Drug abuse prevalence and risk factors among adolescents in Taiwan. Chin J Drug Depend. (2001) 1:20–2. doi: 10.3969/j.issn.1007-9718.2001.01.010 (in Chinese).
47. Hansen WB, Graham JW, Sobel JL, Shelton DR, Flay BR, Johnson CA. The consistency of peer and parent influences on tobacco, alcohol, and marijuana use among young adolescents. J Behav Med. (1987) 10:559–79. doi: 10.1007/BF00846655
48. Stacy AW, Newcomb MD, Bentler PM. Interactive and higher-order effects of social influences on drug use. J Health Soc Behav. (1992) 33:226–41. doi: 10.2307/2137353
49. Kline RB, Canter WA, Robin A. Parameters of teenage alcohol use: a path analytic conceptual model. J Consult Clin Psychol. (1987) 55:521–8. doi: 10.1037/0022-006X.55.4.521
50. Allen JP, Porter MR, McFarland FC, Marsh P, McElhaney KB. The two faces of adolescents' success with peers: adolescent popularity, social adaptation, and deviant behavior. Child Dev. (2005) 76:747–60. doi: 10.1111/j.1467-8624.2005.00875.x
51. Kandel DB, Davies M. High school students who use crack and other drugs. Arch Gen Psychiatry. (1996) 53:71–80. doi: 10.1001/archpsyc.1996.01830010073010
52. Temcheff CE, Serbin LA, Martin-Storey A, Stack DM, Ledingham J, Schwartzman AE. Predicting adult physical health outcomes from childhood aggression, social withdrawal and likeability: a 30-year prospective, longitudinal study. Int J Behav Med. (2010) 18:5–12. doi: 10.1007/s12529-010-9082-0
53. Martin-Storey A, Serbin LA, Stack DM, Ledingham JE, Schwartzman AE. Self and peer perceptions of childhood aggression, social withdrawal and likeability predict adult substance abuse and dependence in men and women: a 30-year prospective longitudinal study. Addict Behav. (2011) 36:1267–74. doi: 10.1016/j.addbeh.2011.07.043
54. Yen LL, Chang HY, Wu WC, Wu CC, Chiang YC. CABLE Annual Report 2012. (2013). Available online at: http://cable.nhri.org.tw/ (accessed November 12, 2020).
55. Yen LL, Chen L, Lee SH, Hsiao C, Pan LY. Child and adolescent behaviors in long-term evolution (CABLE): a school-based health lifestyle study. Promot Educ. (2002) 1:33–40. doi: 10.1177/10253823020090010115
56. United Nations Office on Drugs and Crime (UNODC). World Drug Report 2021. Vienna: United Nations publication, Sales No. E.21.XI.8 (Booklet 2), (2021). 7 p.
57. Jones R. What paediatricians should know about young people and drugs in the UK. Arch Dis Childhood Educ Pract. (2006) 91:ep81–6. doi: 10.1136/adc.2005.072702
58. Chernobrovkina TV, Nikiforov IA. Medical Social Factors Determining Early Poly-Drug Dependence. (2005). Available online at: https://xueshu.baidu.com/usercenter/paper/show?paperid=706722a9ac5b70ef3f4180bfae5a85b4&site=xueshu_se (accessed July 11, 2021).
59. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. (1990) 107:238–46. doi: 10.1037/0033-2909.107.2.238
60. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Eq Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
61. Hoelter JW. The analysis of covariance structures. Sociol Methods Res. (1983) 11:325–44. doi: 10.1177/0049124183011003003
62. Lin CY. The Illegal Behaviors Drug Resources of Initial Drug-Abuse Offenders. (2015). Available online at: http://www.moj.gov.tw/mp001.html (accessed October 10, 2021).
63. Kim HH, Kim HJ, Kim EM. Exploring the association between suicidality and smoking behavior among school-based children in Lao People's Democratic Republic (PDR). J Psychoact Drugs. (2020) 52:46–55. doi: 10.1080/02791072.2019.1707914
64. Kebbe M, Sampasa-Kanyinga H, Hamilton HA, Colman I, Chaput JP. Correlates of nonmedical use of prescription opioids among a cohort of adolescents in Ontario, Canada. J Psychiatr Res. (2020) 120:175–84. doi: 10.1016/j.jpsychires.2019.10.021
65. Ayvasik HB, Sümer HC. Individual differences as predictors of illicit drug use among turkish college students. J Psychol. (2010) 144:489–505. doi: 10.1080/00223980.2010.496671
66. Charitonidi E, Studer J, Gaume J, Gmel G, Daeppen JB, Bertholet N. Socioeconomic status and substance use among Swiss young men: a population-based cross-sectional study. BMC Public Health. (2016) 16:333. doi: 10.1186/s12889-016-2949-5
67. Bernaards CA, Sijtsma K. Factor analysis of multidimensional polytomous item response data suffering from ignorable item nonresponse. Multivariate Behav Res. (1999) 34:277–13. doi: 10.1207/S15327906MBR3403_1
68. Bernaards CA, Sijtsma K. Influence of imputation and EM methods on factor analysis when item nonresponse in questionnaire data is nonignorable. Multivariate Behav Res. (2000) 35:321–64. doi: 10.1207/S15327906MBR3503_03
69. Rubin DB. Inference and missing data. Biometrika. (1976) 63:581–92. doi: 10.1093/biomet/63.3.581
70. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York, NY: John Wiley & Sons (1987).
71. United States Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality. Age of Substance Use Initiation Among Treatment Admissions Aged 18 to 30. Rockville, MD: The TEDS Report (2014).
72. Yen LL, Hung PH, Yang HH, Tung SC, Yen HW. Addictive drug use in vocational high school students. J Med Educ. (1997) 1:69–80.
73. Doraiswamy P, Nattala P, Murthy P. How can today's substance-using youth be helped to quit? Perspectives of college students from Bangalore, India. Int J Soc Psychiatry. (2020) 66:469–75. doi: 10.1177/0020764020916745
74. Zamboanga BL, Tomaso CC, Cloutier RM, Blumenthal H, Kenney SR, Borsari B. Drinking game participation among high school and incoming college students. J Addict Nurs. (2016) 27:24–31. doi: 10.1097/JAN.0000000000000108
75. Adelekan ML, Abiodun OA, Imouokhome-Obayan AO, Oni GA, Ogunremi OO. Psychosocial correlates of alcohol, tobacco and cannabis use: findings from a Nigerian university. Drug Alcohol Depend. (1993) 33:247–56. doi: 10.1016/0376-8716(93)90111-3
76. Kpozehouen A, Ahanhanzo YG, Paraïso MN, Munezero F, Saizonou JZ, Makoutodé M, et al. Facteurs associés à l'usage de substances psychoactives chez les adolescents au Bénin. Santé Publique. (2015) 27:871–80. doi: 10.3917/spub.156.0871
77. Lee CM, Chang FC, Lai HR, Chiang JT, Lee PH, Chen WJ. A prospective study of the risk and protective factors of substance use among vocational high school students in Taipei. Taiwan J Public Health. (2008) 27:399–410. doi: 10.6288/TJPH2008-27-05-05 (in Chinese).
78. Lee JY, Kim W, Brook JS, Finch SJ, Brook DW. Adolescent risk and protective factors predicting triple trajectories of substance use from adolescence into adulthood. J Child Fam Stud. (2019) 29:403–12. doi: 10.1007/s10826-019-01629-9
79. Scholes-Balog KE, Hemphill SA, Heerde JA, Toumbourou JW, Patton GC. Childhood social environmental and behavioural predictors of early adolescent onset cannabis use. Drug Alcohol Rev. (2020) 39:384–93. doi: 10.1111/dar.13077
80. Marsh TY, Cornell DG. The contribution of student experiences to understanding ethnic differences in high-risk behaviors at school. Behav Disord. (2001) 26:152–63. doi: 10.1177/019874290102600204
81. Hoffman ML. Sex differences in empathy and related behaviors. Psychol Bull. (1977) 84:712–22. doi: 10.1037/0033-2909.84.4.712
82. Feldman L, Harvey B, Holowaty P, Shortt L. Alcohol use beliefs and behaviors among high school students. J Adolesc Health. (1999) 24:48–58. doi: 10.1016/S1054-139X(98)00026-3
83. Miech RA, Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future National Survey Results on Drug Use, 1975-2016: Volume I, Secondary School Students. Ann Arbor, MI: Institute for Social Research, The University of Michigan (2017).
84. Pacek LR, Mauro PM, Martins SS. Perceived risk of regular cannabis use in the United States from 2002 to 2012: differences by sex, age, and race/ethnicity. Drug Alcohol Depend. (2015) 149:232–44. doi: 10.1016/j.drugalcdep.2015.02.009
85. Brener ND, Collins JL. Co-occurrence of health-risk behaviors among adolescents in the United States. J Adolesc Health. (1998) 22:209–13. doi: 10.1016/S1054-139X(97)00161-4
86. Topolski TD, Patrick DL, Edwards TC, Huebner CE, Connell FA, Mount KK. Quality of life and health-risk behaviors among adolescents. J Adolesc Health. (2001) 29:426–35. doi: 10.1016/S1054-139X(01)00305-6
87. United Nations Office on Drugs Crime (UNODC). UNODC/WHO International Standards on Drug Use Prevention Second Updated Edition. (2018). Available online at: https://www.unodc.org/unodc/en/prevention/prevention-standards.html (accessed December 18, 2020).
88. United Nations Office on Drugs and Crime (UNODC). SCHOOLS: School-Based Education for Drug Abuse Prevention. Vienna: United Nations Publication, Sales No. E.04.XI.21 (2020). 46 p.
89. United Nations Office on Drugs Crime (UNODC). UNODC/WHO International Standards on Drug Use Prevention Second Updated Edition. (2018). Available online at: https://www.unodc.org/documents/prevention/UNODC-WHO_2018_prevention_standards_E.pdf (accessed December 18, 2020).
90. United Nations Office on Drugs and Crime (UNODC). SCHOOLS: School-Based Education for Drug Abuse Prevention. Vienna: United Nations Publication, Sales No. E.04.XI.21 (2020). 16 p.
Keywords: experimental drug use, social attachment, cohort study, childhood, adolescence, survival analysis
Citation: Chiang Y-C, Li X, Lee C-Y, Wu C-C, Chang H-Y and Zhang S (2022) Effects of Social Attachment on Experimental Drug Use From Childhood to Adolescence: An 11-Year Prospective Cohort Study. Front. Public Health 10:818894. doi: 10.3389/fpubh.2022.818894
Received: 02 December 2021; Accepted: 11 February 2022;
Published: 29 March 2022.
Edited by:
Chung-Ying Lin, National Cheng Kung University, TaiwanReviewed by:
Meng-Che Tsai, National Cheng Kung University Hospital, TaiwanCopyright © 2022 Chiang, Li, Lee, Wu, Chang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi-Chen Chiang, anlqQHhtdS5lZHUuY24=; Hsing-Yi Chang, aHNpbmd5aUBuaHJpLm9yZy50dw==; Shuoxun Zhang, aGVsbGVuenN4QGdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.