 Kathryn Harris
Kathryn Harris Francine Overcash
Francine Overcash Damien Belobrajdic
Damien Belobrajdic Joanne Slavin
Joanne Slavin- 1Bay State Milling, Quincy, MA, United States
- 2Department of Food Science and Nutrition, University of Minnesota, St. Paul, MN, United States
- 3Commonwealth Scientific and Industrial Research Organization (CSIRO), Canberra, ACT, Australia
Children and adolescents have consistently failed to meet recommended levels of dietary fiber consumption, thus making fiber a nutrient of concern. The importance of adequate dietary fiber intake to attain a healthy diet necessitates the identification of fiber-rich and readily consumed food sources by youth. Grain-based foods derived from whole grains represent a strategic initiative to increase dietary fiber consumption and is consistent with the American diet pattern. Increased intake of foods made from whole grains have been positively associated with improved health outcomes but are also less preferred among youth compared to refined grain products, which make up the majority of their carbohydrate intake. Advances in the commercialization and availability of high amylose wheat flour, a source of resistant starch fiber, provides an opportunity to remedy the suggested acceptability issues of whole grain products indicative of sensory factors, without compromising the amount of fiber ingested. Resistant starch fiber consumption has been associated with health benefits including improved blood sugar management, improved markers of digestive and gut health, increased satiety, and a reduced inflammatory response among adults. The limited studies that indicate fiber's direct benefit among youth are largely observational, thereby necessitating the need for more controlled trials for these age groups. Replacing traditional refined wheat flour with refined high amylose wheat flour has the unique ability to increase dietary fiber consumption without compromising desired sensory and finished product characteristics and thus can help increase dietary fiber consumption in children and adolescents who struggle to meet adequate intakes of fiber.
Introduction
Children and adolescents have consistently failed to meet minimum levels of fiber intake, leading it to be an official nutrient of concern (1, 2). Current recommendations set forth in the 2020–2025 Dietary Guidelines for Americans are based on adequate intakes of fiber that range from 17 g/d (ages 4–8 years) to 31 g/d (ages 14–18 years) (3). The extant literature is peppered with epidemiological evidence that continuously shows alarmingly low intake levels for all ages of youth (≤ 18 years). One study reported that nine out of 10 children failed to meet the National Academy of Medicine's Dietary Reference Intake (DRI) recommendation for fiber while another found both children and adolescents only consume half of the DRI recommendation for fiber (4). This fiber gap is even more pronounced in low-income and minority children (5) and appears to widen in adolescence (6).
Dietary Fiber in Children and Adolescents
The importance of fiber to dietary quality necessitates the identification of fiber-rich and readily consumed food sources. Given an estimated 60 and 93% of youth aged 1–18 years do not meet recommended intake levels of fruit and vegetables respectively (7), dietary research has justifiably focused on fruits and vegetables as fiber-rich food sources (8–10). However, fruits and vegetables contribute <30% of the overall dietary fiber intake in children and adolescents, whereas cereal grains and their food sources contribute over 50% (11). Youth consume more than the recommended daily amount of grains (11), thus demonstrating the opportunity to make dietary modifications that incorporate whole grains and/or novel high amylose grains as a means for increasing dietary fiber intake in children and adolescents. A concerted effort to improve intake of nutrient dense grain-based foods fits within the American diet pattern (12), which may be advantageous for children and adolescents who are notoriously more selective in their food choices (13–15).
The recently released 2020–2025 Dietary Guidelines for Americans recommend at least half of the daily grain intake should be whole grains (16). Unfortunately, children and adolescents have consistently failed to meet these recommended levels. A study from a large representative sample of the US population (NHANES), found almost 40% of children and adolescents do not consume any whole grains (oz eq/d) and only 2.9% of children/adolescents (ages 2–18 years) met the minimum recommended intake of three whole grain oz equivalent servings per day (11). These whole grain deficiencies persisted in other studies that examined continuous years (≥10 years) of NHANES data from ~15,000 children/adolescents (6, 17).
High-Amylose Wheat
While it is recommended that children and adolescents consume 2–5 ounce-equivalents of whole grains per day, the majority of their carbohydrate intake comes from refined grains (3). Consumer preference for refined bread is often cited as a reason for the relatively low consumption of whole wheat breads (18). Wheat is an important cereal grain that is a sustainable source of energy and is a staple food in the diets of most individuals around the world, but the way it is processed often determines its associated health outcome (19). When whole wheat kernels are processed into refined wheat flour, the fiber-rich bran and phytonutrient-rich germ layer are removed, and the starchy endosperm is milled to a fine particle size and used as the base ingredient for a broad range of processed foods such as breads, pastas/noodles, and tortillas (20). Products made with refined wheat flour do contain small amounts of dietary fiber, but these products generally elicit a high glycemic load due to the readily available, high digestible starch content in refined wheat flour, and thus their consumption has been associated with a number of chronic diseases (21). Wheat starch typically contains >70% amylopectin, a highly branched and rapidly digestible polymer, and <30% amylose, a linear polymer that is less digestible in the human small intestine. To address the nutritional inadequacies of refined wheat flour, high amylose wheat (HAW) varieties have been developed to deliver >80% amylose (22). The substantial increase in amylose within the endosperm of the wheat kernel delivers a higher resistant starch (RS) content, which is a form of non-digestible starch (23). Because wheat flour is the primary ingredient in a broad range of commonly consumed cereal products, any improvements to the nutritional value of wheat, like those achieved with this novel wheat variety, could have a positive impact of public health.
An alternate approach to increasing the dietary fiber content of cereal foods is to use these novel HAW varieties that yield refined flours naturally high in RS. Important products of intestinal fermentation are short chain fatty acids, which help to decrease colonic pH and maintain a healthy bacterial population in the large bowel (24). RS fermentation specifically favors the production of butyrate which is the primary energy source for colonic epithelial cells and it has antineoplastic effects in the colon (25). Consumption of foods high in RS have been shown to lower postprandial glucose responses in comparison to conventional starch-based foods and a sustained high intake of RS improves insulin sensitivity through mechanisms believed to be both dependent and independent of the byproducts of bacterial fermentation (26–28). Additionally, RS consumption has been associated with a number of health benefits including improved markers of digestive and gut health, increased satiety, and a reduced inflammatory response (29, 30).
Emerging clinical trials are demonstrating the functional health effects of foods made from HAW (31). This includes a lowered glycemic response for bread, noodles and pasta when conventional wheat flour is replaced with HAW (32–34). In particular the HAW breads, irrespective of whether they were made with whole wheat or refined flour, had a glycemic response that was 39% less than that achieved with conventional wheat breads and an insulinemic and incretin responses that were 24–30% less for HAW breads than for conventional wheat breads (33). Furthermore, foods containing refined HAW, but not whole wheat HAW showed favorable changes in fecal metabolites and bacteria species indicative of greater carbohydrate and lower protein fermentation compared to conventional wheat (35). Importantly, substituting conventional wheat flour with HAW in commonly consumed foods such as bread and biscuits enabled adults to increase their fiber intake (from a low background level of 20 g/d above the recommended level of 37 g/d) which was then well tolerated by the study participants (35, 36). Although these clinical trials on HAW have only used a healthy adult population (32–35) similar improvements in metabolic and gastrointestinal endpoints are expected in other age groups, including children and adolescents.
Dietary Fiber Studies
The impact of fiber on children and adolescents' health has relied heavily on observational studies, while studies that show fiber's direct health benefits are limited at best. As such, the aforementioned recommendations for fiber intake among youth are extrapolated from studies among adult populations that showed improved outcomes with higher dietary fiber intake, namely cardiovascular disease and colon cancer (37, 38). Intervention studies among youth are often hampered by ethical and practical challenges in study design and methodologies (4). Constipation may be one of the more researched morbidities affected by fiber among youth, in part due to its inverse associations with quality-of-life scores and academic performance (39–42). In general, the correlations between fiber and obesogenic conditions have resulted in inconsistent findings. For example, two large-scale cross-sectional studies of American and British children found increased fiber was associated with reduced risk for overweight/obesity and lower body fatness, respectively (43, 44). On the other hand, another study found a null association between dietary fiber and adiposity in a sample of overweight Latino adolescents aged 10–17 years (45). Increased fiber intake was associated with reduced prevalence of metabolic syndrome, a grouping of multiple cardiometabolic risk factors including hyperglycemia/insulin resistance, obesity, and dyslipidemia in a study of 12 continuous years of NHANES data consisting of over 16,000 13–18 year olds (46).
Discussion
While policy leaders have continuously pushed for increased whole grain consumption due to the higher vitamin, mineral, phytoestrogen, antioxidant, and dietary fiber content compared to its refined grain counterpart (12), refined grains continue to be the major contributor of dietary carbohydrates due to sensory preferences (18, 20). Because the most commonly cited reason for not consuming whole grain products is related to sensory attributes, it is important to ensure that the replacement of conventional refined flour with high amylose flour does not impart any differences in finished product quality. While there are other cereal-based ingredients that are high in resistant starch made from bananas (green banana flour) and corn (Hi-Maize®) there are considerable limitations to the amount of these ingredients that can be added to conventional cereal-based foods. For instance, adding 15% Hi-maize® to a bread recipe increased the RS content of the bread to 5% but the bread had a worse appearance to the control and had a lower volume, and a lighter crust (47). While the addition of green banana flour can increase the RS content of bread to upwards of 6%, significantly lower loaf volumes, higher bread hardness, and darker crumb and crust colors have been reported at inclusion levels as low as a 10% replacement of wheat flour (48, 49).
Unlike other isolated fiber ingredients in high in resistant starch, HAW can replace upwards of 50% of conventional wheat flour without any deleterious effects in bread quality despite a 6X increase in resistant starch (50). In a recently conducted study, flour tortillas made with a 50% replacement of common wheat flour with HAW delivered 2.5 times more dietary fiber and had significantly higher rollability and foldability scores compared to flour tortillas made with conventional wheat (p < 0.05 for both, unpublished) even after 9 weeks of storage, demonstrating that the inclusion of HAW in this commonly consumed processed cereal food improved two important aspects of product quality with no deleterious effects on finished product quality. Consistent with these findings, a trained sensory panel reported that despite delivering three times more fiber, pasta made with 50% HAW flour and 50% semolina had no discernable differences in flavor, aroma, or texture (hardness, cohesiveness) when compared to standard pasta made with 100% semolina (unpublished data).
The effective incorporation of HAW flour into commonly consumed foods (i.e., breads/rolls, tortillas, pasta) supports the potential incorporation into other wheat-flour based foods including commonly consumed snack foods (i.e., crackers, biscuits/cookies), cereals, and pastries without adversely affecting the taste attributes of these products. While most of the research conducted on HAW has been done using bread, tortillas, and pasta as the delivery mode, refined HAW flour can readily replace common refined wheat flour in any of these wheat-based products to deliver higher amounts of dietary fiber, see Table 1. Given the well-known understanding that children like what they know and eat what they like (51), HAW has the unique potential to vastly increase dietary fiber consumption without compromising the desired sensory and finished product characteristics in commonly consumed foods and thus can serve as a platform for increasing dietary fiber consumption in children and adolescents who struggle to meet adequate intakes of fiber.
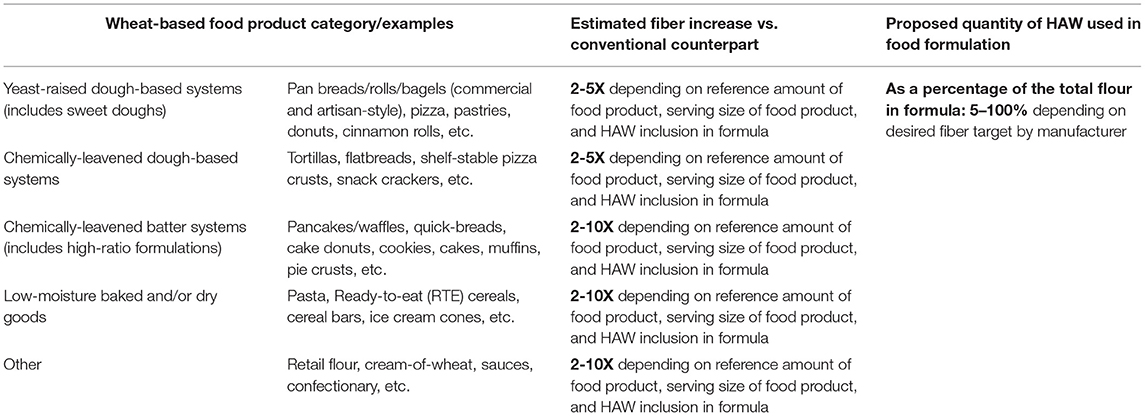
Table 1. Potential wheat-based foods that can be made with HAW and the subsequent impact on their fiber level.
As HAW has great potential to increase a child's fiber consumption, it is important to address the cost disparity that often comes with healthier food choices. A recently conducted meta-analysis concluded that healthier versions of grains and snacks/sweets were more expensive per serving, with an increase in $0.03/serving and $0.12/serving respectively (52). One reason healthier versions of grains and sweets/snacks can be more expensive is because of the addition of higher cost ingredients needed to meet superior nutritional targets such as whole grains, fiber isolates, and protein isolates. In addition to the compromised product performance, the cost of these ingredients may be prohibitive for food manufacturers due to their increased cost and ingredient declaration. Other cereal-based ingredients high in resistant starch undergo various manufacturing processes (separation and/or chemical modification) which drive higher raw material costs compared to HAW which is manufactured similarly to conventional wheat flour and thus is lower in cost. It is estimated that replacement of wheat flour with HAW may not have the same impact on price as it is a flour substitute. Using pasta as an example, replacement of 25% of standard wheat flour with HAW will increase fiber content by 3-fold, yet only increase the manufacturing cost by ~$0.05/1 lb. box, or ~$0.006/serving. Conversely, a standard pasta containing an isolated fiber additive providing an equivalent increase in dietary fiber would result in a larger increase in the manufacturing cost ~$0.10/1 lb. box, or ~$0.01/serving. However, it is unknown how the increased cost per serving will translate to a consumer because different food manufacturers will have different pricing models based on desired margin targets and revenue growth. Additionally, the cost of raw materials (i.e., HAW, isolated fibers, isolated proteins, etc.) vary depending on manufacturers, processing requirements, crop years, and/or crop quality. The commercial availability of cereal-based foods that contain HAW is currently limited to bread, tortillas, dry pasta, fresh noodles, pizza/pizza bases, ice cream cones, and cookies, this is anticipated to expand dramatically as the production of HAW increases and mainstream food manufacturers replace conventional wheat flour in existing cereal-based foods with HAW.
Closing the fiber gap among children and adolescents will remain a critical public health concern until new strategies and/or food products succeed where whole wheat has fallen short. A panel of leaders and experts in fiber research and industry took the official position that grain-based foods represent a pragmatic and “small step strategy” to increase total dietary fiber with reduced risk of increasing energy intake (12). The promising, albeit limited, results from the trials of high-amylose wheat products in adults make for a strong case to conduct controlled trials in youth that test the hypothesis of its mass appeal to increase fiber intake and deliver improved health outcomes, all without sacrificing desired sensory characteristics and thus ensuring consumption among children and youth.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
KH, FO, DB, and JS have contributed significantly to the writing and editing of this manuscript and have approved the final version of the manuscript.
Funding
Bay State Milling, Inc. financially supports FO.
Conflict of Interest
FO is employed by the University of Minnesota but is financially supported by Bay State Milling for her time in writing this Perspective Manuscript. KH is a Research Food Scientist employed by Bay State Milling.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Brauchla M, McCabe GP, Miller KB, Kranz S. The effect of high fiber snacks on digestive function and diet quality in a sample of school-age children. Nutr J. (2013) 12:153. doi: 10.1186/1475-2891-12-153
2. Korczak R, Kamil A, Fleige L, Donovan SM, Slavin JL. Dietary fiber and digestive health in children. Nutr Rev. (2017) 75:241–59. doi: 10.1093/nutrit/nuw068
3. U.S. Department of Agriculture (USDA) ARS. 2020–2025 Dietary Guidelines for Americans. Washington, DC. (2019). Available online at: https://www.dietaryguidelines.gov/
4. Kranz S, Brauchla M, Slavin JL, Miller KB, Paul S, Kellogg WK. What do we know about dietary fiber intake in children and health? The effects of fiber intake on constipation, obesity, and diabetes in children. Adv Nutr. (2012) 3:47–53. doi: 10.3945/an.111.001362
5. Banfield EC, Liu Y, Davis JS, Chang S, Frazier-Wood AC. Poor adherence to US dietary guidelines for children and adolescents in the national health and nutrition examination survey population. J Acad Nutr Diet. (2016) 116:21–7. doi: 10.1016/j.jand.2015.08.010
6. McGill CR, Fulgoni VL, Devareddy L. Ten-year trends in fiber and whole grain intakes and food sources for the United States population: national health and nutrition examination survey 2001–2010. Nutrients. (2015) 7:1119–30. doi: 10.3390/nu7021119
7. NCI. Usual dietary intakes: food intakes, U.S. population, 2007–10. Epidemiol Genomics Res Progr. (2015). Available online at: http://epi.grants.cancer.gov/diet/usualintakes/pop/2007-10/ (accessed May 16, 2016).
8. Appleton KM, Hemingway A, Saulais L, Dinnella C, Monteleone E, Depezay L, et al. Increasing vegetable intakes: rationale and systematic review of published interventions. Eur J Nutr. (2016) 55:869–96. doi: 10.1007/s00394-015-1130-8
9. Hiza HAB, Casavale KO, Guenther PM, Davis CA. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J Acad Nutr Diet. (2013) 113:297–306. doi: 10.1016/j.jand.2012.08.011
10. Overcash FM, Vickers Z, Ritter AE, Mann T, Mykerezi E, Redden J, et al. An in-home intervention of parent-implemented strategies to increase child vegetable intake: results from a non-randomized cluster-allocated community trial. BMC Public Health. (2019) 19:881. doi: 10.1186/s12889-019-7079-4
11. Reicks M, Jonnalagadda S, Albertson AM, Joshi N. Total dietary fiber intakes in the US population are related to whole grain consumption: results from the national health and nutrition examination survey 2009 to 2010. Nutr Res. (2014) 34:226–34. doi: 10.1016/j.nutres.2014.01.002
12. Clemens R, Kranz S, Mobley AR, Nicklas TA, Raimondi MP, Rodriguez JC, et al. Filling America's fiber intake gap: summary of a roundtable to probe realistic solutions with a focus on grain-based foods. J Nutr. (2012) 142:1390S−401S. doi: 10.3945/jn.112.160176
13. Wardle J, Herrera M-L, Cooke L, Gibson EL. Modifying children's food preferences: the effects of exposure and reward on acceptance of an unfamiliar vegetable. Eur J Clin Nutr. (2003) 57:341–8. doi: 10.1038/sj.ejcn.1601541
14. Birch LL. Development of food preferences. Annu Rev Nutr. (1999) 19:41–62. doi: 10.1146/annurev.nutr.19.1.41
15. Brug J, Tak NI, te Velde SJ, Bere E, de Bourdeaudhuij I. Taste preferences, liking and other factors related to fruit and vegetable intakes among schoolchildren: results from observational studies. Br J Nutr. (2008) 99:S7–14. doi: 10.1017/S0007114508892458
17. Albertson AM, Reicks M, Joshi N, Gugger CK. Whole grain consumption trends and associations with body weight measures in the United States: results from the cross sectional national health and nutrition examination survey 2001-2012. Nutr J. (2016) 15:8. doi: 10.1186/s12937-016-0126-4
18. Bakke A, Vickers Z. Consumer liking of refined and whole wheat breads. J Food Sci. (2007) 72:S473–80. doi: 10.1111/j.1750-3841.2007.00440.x
19. Jones JM, Peña RJ, Korczak R, Braun HJ. Carbohydrates, grains, and wheat in nutrition and health: an overview part I. Role of carbohydrates in health. Cereal Foods World. (2015) 60:224–33. doi: 10.1094/CFW-60-5-0224
20. Jensen MK, Koh-Banerjee P, Hu FB, Franz M, Sampson L, Grønbœk M, et al. Intakes of whole grains, bran, and germ and the risk of coronary heart disease in men. Am J Clin Nutr. (2004) 80:1492–9. doi: 10.1093/ajcn/80.6.1492
21. Liu S. Intake of refined carbohydrates and whole grain foods in relation to risk of type 2 diabetes mellitus and coronary heart disease. J Am Coll Nutr. (2002) 21:298–306. doi: 10.1080/07315724.2002.10719227
22. Regina A, Berbezy P, Kosar-Hashemi B, Li S, Cmiel M, Larroque O, et al. A genetic strategy generating wheat with very high amylose content. Plant Biotechnol J. (2015) 13:1276–86. doi: 10.1111/pbi.12345
23. Cummings JH, Beatty ER, Kingman SM, Bingham SA, Englyst HN. Digestion and physiological properties of resistant starch in the human large bowel. Br J Nutr. (1996) 75:733–47. doi: 10.1079/BJN19960177
24. Den Besten G, Van Eunen K, Groen AK, Venema K, Reijngoud DJ, Bakker BM. The role of short-chain fatty acids in the interplay between diet, gut microbiota, and host energy metabolism. J Lipid Res. (2013) 54:2325–40. doi: 10.1194/jlr.R036012
25. Siavoshian S, Segain JP, Kornprobst M, Bonnet C, Cherbut C, Galmiche JP, et al. Butyrate and trichostatin a effects on the proliferation/differentiation of human intestinal epithelial cells: induction of cyclin D3 and p21 expression. Gut. (2000) 46:507–14. doi: 10.1136/gut.46.4.507
26. Bindels LB, Segura Munoz RR, Gomes-Neto JC, Mutemberezi V, Martínez I, Salazar N, et al. Resistant starch can improve insulin sensitivity independently of the gut microbiota. Microbiome. (2017) 5:12. doi: 10.1186/s40168-017-0230-5
27. De Vadder F, Kovatcheva-Datchary P, Goncalves D, Vinera J, Zitoun C, Duchampt A, et al. Microbiota-generated metabolites promote metabolic benefits via gut-brain neural circuits. Cell. (2014) 156:84–96. doi: 10.1016/j.cell.2013.12.016
28. Robertson MD, Bickerton AS, Dennis AL, Vidal H, Frayn KN. Insulin-sensitizing effects of dietary resistant starch and effects on skeletal muscle and adipose tissue metabolism. Am J Clin Nutr. (2005) 82:559–67. doi: 10.1093/ajcn/82.3.559
29. Vahdat M, Hosseini SA, Khalatbari Mohseni G, Heshmati J, Rahimlou M. Effects of resistant starch interventions on circulating inflammatory biomarkers: a systematic review and meta-analysis of randomized controlled trials. Nutr J. (2020) 19:33. doi: 10.1186/s12937-020-00548-6
30. McOrist AL, Miller RB, Bird AR, Keogh JB, Noakes M, Topping DL, et al. Fecal butyrate levels vary widely among individuals but are usually increased by a diet high in resistant starch. J Nutr. (2011) 141:883–9. doi: 10.3945/jn.110.128504
31. Belobrajdic DP, Bird AR. Evaluation of an ileorectostomised rat model for resistant starch determination. Nutrients. (2021) 13:1–13. doi: 10.3390/nu13010091
32. Ang K, Bourgy C, Fenton H, Regina A, Newberry M, Diepeveen D, et al. Noodles made from high amylose wheat flour attenuate postprandial glycaemia in healthy adults. Nutrients. (2020) 12:1–14. doi: 10.3390/nu12082171
33. Belobrajdic DP, Regina A, Klingner B, Zajac I, Chapron S, Berbezy P, et al. High-amylose wheat lowers the postprandial glycemic response to bread in healthy adults: a randomized controlled crossover trial. J Nutr. (2019) 149:1335–45. doi: 10.1093/jn/nxz067
34. Sissons M, Sestili F, Botticella E, Masci S, Lafiandra D. Can manipulation of durum wheat amylose content reduce the glycaemic index of spaghetti? Foods. (2020) 9:693. doi: 10.3390/foods9060693
35. Gondalia SV, Wymond B, Benassi-Evans B, Berbezy P, Bird A, Belobrajdic D. Substitution of refined conventional wheat flour with high amylose wheat modulates the intestinal microbiome and improves fecal metabolites in healthy adults: a randomized, controlled trial. J Nutr. (2022). doi: 10.1093/jn/nxac021. [Epub ahead of print].
36. Hughes RL, Horn WH, Finnegan P, Newman JW, Marco ML, Keim NL, et al. Resistant starch type 2 from wheat reduces postprandial glycemic response with concurrent alterations in gut microbiota composition. Nutrients. (2021) 13:1–20. doi: 10.3390/nu13020645
37. Murphy N, Norat T, Ferrari P, Jenab M, Bueno-de-Mesquita B, Skeie G, et al. Dietary fibre intake and risks of cancers of the colon and rectum in the European prospective investigation into cancer and nutrition (EPIC). PLoS ONE. (2012) 7:e39361. doi: 10.1371/journal.pone.0039361
38. Threapleton DE, Greenwood DC, Evans CEL, Cleghorn CL, Nykjaer C, Woodhead C, et al. Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis. BMJ. (2013) 347:f6879. doi: 10.1017/S0029665113002784
39. Elkhayat HA, Shehata MH, Nada A, Deifalla SM, Ammar MS. Impact of functional constipation on psychosocial functioning and quality of life of children: a cross sectional study. Egypt Pediatr Assoc Gaz. (2016) 64:136–41. doi: 10.1016/j.epag.2016.05.003
40. Kovacic K, Sood MR, Mugie S, Di Lorenzo C, Nurko S, Heinz N, et al. A multicenter study on childhood constipation and fecal incontinence: effects on quality of life. J Pediatr. (2015) 166:1482–7.e1. doi: 10.1016/j.jpeds.2015.03.016
41. Rajindrajith S, Devanarayana NM, Perera BJC, Benninga MA. Childhood constipation as an emerging public health problem. World J Gastroenterol. (2016) 22:6864–75. doi: 10.3748/wjg.v22.i30.6864
42. Youssef NN, Langseder AL, Verga BJ, Mones RL, Rosh JR. Chronic childhood constipation is associated with impaired quality of life: a case-controlled study. J Pediatr Gastroenterol Nutr. (2005) 41:56–60. doi: 10.1097/01.mpg.0000167500.34236.6a
43. Johnson L, Mander AP, Jones LR, Emmett PM, Jebb SA. Energy-dense, low-fiber, high-fat dietary pattern is associated with increased fatness in childhood. Am J Clin Nutr. (2008) 87:846–54. doi: 10.1093/ajcn/87.4.846
44. Oneil CE, Nicklas TA, Zanovec M, Cho SS, Kleinman R. Consumption of whole grains is associated with improved diet quality and nutrient intake in children and adolescents: the national health and nutrition examination survey 1999-2004. Public Health Nutr. (2011) 14:347–55. doi: 10.1017/S1368980010002466
45. Davis JN, Alexander KE, Ventura EE, Kelly LA, Lane CJ, Byrd-Williams CE, et al. Associations of dietary sugar and glycemic index with adiposity and insulin dynamics in overweight Latino youth. Am J Clin Nutr. (2007) 86:1331–8. doi: 10.1093/ajcn/86.5.1331
46. Fulgoni VL, Brauchla M, Fleige L, Chu YF. Association of whole-grain and dietary fiber intake with cardiometabolic risk in children and adolescents. Nutr Health. (2020) 26:243–51. doi: 10.1177/0260106020928664
47. Šárka E, Kubová M, Wiege I, Horák P, Smrčková P, Dvoráček V, et al. Two resistant starches applied in bread. Czech J Food Sci. (2017) 35:67–72. doi: 10.17221/343/2016-CJFS
48. Khoozani AA, Kebede B, Birch J, El-Din Ahmed Bekhit A. The effect of bread fortification with whole green banana flour on its physicochemical, nutritional and in vitro digestibility. Foods. (2020) 9:152. doi: 10.3390/foods9020152
49. Thakaeng P, Boonloom T, Rawdkuen S. Physicochemical properties of bread partially substituted with unripe green banana (Cavendish spp.) flour. Molecules. (2021) 26:2070. doi: 10.3390/molecules26072070
50. Li C, Dhital S, Gidley MJ. High-amylose wheat bread with reduced in vitro digestion rate and enhanced resistant starch content. Food Hydrocoll. (2022) 123:107181. doi: 10.1016/j.foodhyd.2021.107181
51. Cooke L. The importance of exposure for healthy eating in childhood: a review. J Hum Nutr Diet. (2007) 20:294–301. doi: 10.1111/j.1365-277X.2007.00804.x
Keywords: fiber, resistant starch, high amylose wheat, adolescents, children
Citation: Harris K, Overcash F, Belobrajdic D and Slavin J (2022) Perspective: Utilizing High Amylose Wheat Flour to Increase Dietary Fiber Intake of Children and Adolescents: A Health by Stealth Approach. Front. Public Health 10:817967. doi: 10.3389/fpubh.2022.817967
Received: 18 November 2021; Accepted: 14 February 2022;
Published: 31 March 2022.
Edited by:
Terry Huang, City University of New York, United StatesReviewed by:
Jagmeet Madan, SNDT Women's University, IndiaCopyright © 2022 Harris, Overcash, Belobrajdic and Slavin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francine Overcash, b3ZlcmMwMDYmI3gwMDA0MDt1bW4uZWR1
†These authors share first authorship