 Gustavo Vega-Fernández
Gustavo Vega-Fernández Enrique Olave3
Enrique Olave3 Pablo A. Lizana
Pablo A. Lizana- 1Laboratory of Epidemiology and Morphological Sciences, Instituto de Biología, Pontificia Universidad Católica de Valparaíso, Valparaíso, Chile
- 2Programa de Magister en Ciencias Mención Morfología, Universidad de La Frontera, Temuco, Chile
- 3Facultad de Medicina, Universidad de La Frontera, Temuco, Chile
Introduction: Teaching professionals have reported multiple conditions associated with low quality of life (QoL) perception. Various studies have also reported high prevalence of musculoskeletal disorders (MSD). In this context, there are few studies regarding the association between low QoL perception and MSD suffering in teachers.
Objective: Therefore, in this study the aim was evaluate MSD prevalence and its association with teachers' QoL perception.
Participants and Methods: A total sample of 544 Chilean teachers were included in a cross-sectional study. MSD prevalence was evaluated via the Standardized Nordic Questionnaire and QoL perception via the Short-Form 36 Health Survey Instrument. Multinomial logistic regression was applied to evaluate the association between MSD and QoL perception adjusted for gender and age.
Results: A total of 91% of teachers have had some MSD in the last 12 months, and 28.86% have had 6 or more painful regions. Females showed greater MSD prevalence than males. Teachers who reported no MSD had higher QoL scores compared to teachers with MSD. The group of teachers with the most MSD (≥p75) saw significant increases in the risk of having low scores in the physical (OR: 2.82) and mental components (OR: 2.65) of QoL. By contrast, teachers without MSD have a buffer effect for their QoL (physical OR: 0.2; mental OR: 0.44).
Conclusions: High MSD prevalence suggest that preventive and informative actions must be taken regarding these disorders to protect teachers' mental and physical health, considering the multiple risk factors to which teachers are exposed given their work conditions in Chile and worldwide.
Introduction
Musculoskeletal disorders (MSD) are musculoskeletal system pathologies which produce pain and are sometimes accompanied by mobility limitations (1, 2). They are also some of the most prevalent public health problems among the working population and the general global population (1), representing one of the main causes of work absenteeism (3) and causing major economic costs for national health systems worldwide (4–6). Regarding physical health, MSD have been associated with workplace ergonomics and infrastructure (7), chronic health conditions including obesity and type 2 diabetes (8), repetitive movements, bad posture, lifting heavy objects and general physical stress (9–11). In mental health, MSD have been associated with high psychosocial demands, high mental workplace stress and workplace harassment (12–15), and feelings of depression, anxiety, and job dissatisfaction (10, 16, 17). All of these health conditions significantly im-pact the Quality of Life (QoL) of working groups and the general population (18, 19).
The teaching sector has reported various occupational ailments due to high physical and mental demands (20–22), along with various diseases related to MSD (23, 24). Worldwide MSD reports among teachers indicate that these symptoms' prevalence fluctuates between 30 and 90% in this work group (24) and are related with various sociodemographic factors and certain health conditions among teachers (25–27). For example, some studies report high prevalence of pain in the lower back, neck and shoulders associated with depressive conditions, anxiety, and high psychosocial demands at work (25, 28), and high foot pain prevalence associated with age, body mass index (BMI), inappropriate footwear and long hours standing (29), along with teachers with high lower back pain rates associated with sleep disorders, irregular physical activity and staying on their feet at work (30).
MSD are also associated with low QoL perception in various working groups worldwide (31, 32), as well as in general population studies (33, 34). Among teachers, those suffering from MSD have also reported low QoL scores, impacting their physical and mental health (20, 35, 36).
Chilean teachers have reported that some chronic health conditions generate significant QoL impact, especially on the Mental Component Summary (20). However, reports associating MSD with QoL in Chilean teachers are scarce. Therefore, the objective of this study is to determine MSD prevalence among teachers and its association with QoL mental and physical components.
Materials and Methods
Participants
The target population was all Chilean teachers [N = 2,49,865; (37)]. To calculate the sample size, the variable with the greatest variance for this group was selected according to the literature published. The sample was determined with the variable MSD for Chilean workers [49.8%; (38)]. The sample was calculated with 95% confidence and a 5% error. In addition, the sample size was increased by 25% due to possible dropouts. Minimum sample was 511.
This cross-sectional study was done among currently active teachers working in various types of schools. The schools were randomly selected. There were 697 initial participants in the study. Of these, 132 did not complete some of the surveys and 21 had missing data. In total, we analyzed 544 teachers from 28 urban schools in three Chilean regions, namely: northern zone: Arica and Parinacota Region (41%); central zone: Valparaíso Region (36%); and southern zone: Araucanía Region (23%). Measurements were applied between October 2018 and October 2019.
Instruments
Musculoskeletal Disorders
To evaluate MSD, we used the Spanish version of the Standardized Nordic Questionnaire adapted and validated for various countries including Chile (39–41). This instrument grants information about teachers' pain prevalence in 12 body areas: neck, right shoulder, left shoulder, right forearm/elbow, left forearm/elbow, right hand/wrist, left hand/wrist, upper back, lower back, hips/buttocks/thighs, knees, feet/ankles. The first part of the questionnaire consisted in detecting whether or not pain was present in any of the 12 previously mentioned areas, within the last 12 months. The second part of the questionnaire investigated whether incapacitating pain happened within any of the 12 body areas in the last 12 months. The instrument uses short answers (yes/no) to prevent self-report from having inaccuracies and subjective biases regarding pain scale and TME durations in painful regions.
Quality of Life
To evaluate teachers' QoL, we used the Spanish version with syntactic and semantic adjustments for Chilean expressions (42, 43) of the “Short-Form 36 Health Survey Instrument (SF-36)” questionnaire created and standardized in the USA (44). This instrument evaluates QoL in individuals using 36 Likert-form questions, calibrated to obtain a diagnosis in eight health dimensions: physical function, physical role, body pain, general health perception, vitality, social function, emotional role, and mental health. These 8 scales are gathered in two components: Physical Component Summary (PCS) and Mental Component Summary (MCS). The questions for each of the eight dimensions add up to a score on a scale of 0 to 100, which is then standardized via a T-Score value for each scale and PCS and MCS summary measures, calculated according to the standardization indicated by the creator (44). Values greater than T-Score 50 indicate good QoL perception while scores below T-Score 50 indicate poor QoL perception. Regarding the reliability of the scale, the Cronbach's alpha coefficient was α = 0.883 for the physical function scale, α = 0.860 for the limitations due to physical problems scale, α = 0.868 for the bodily pain scale, α = 0.859 for the general health perceptions scale, α = 0.854 for the vitality scale, α = 0.853 for the social functioning scale, α = 0.858 for the role limitations due to emotional problems scale, α = 0.852 for the mental health scale, α = 0.874 for the Physical Component Summary and α = 0.861 for the Mental Component Summary.
Proceedings
Instruments were previously explained to the teachers by the researchers in person. Teachers also had to sign informed consent indicating their voluntary participation, without payment or incentives in any point of the study. All procedures in this study met with bioethical standards according to the Helsinki Declaration (45) and were approved by the Ethics Committee at Pontificia Universidad de Valparaíso, Chile (n°BIOEPUCV-H 160-2017).
Statistical Analysis
In statistical analysis, we used STATA MP2 V.16 software for Windows. For associations between categorical variables, the chi-squared test and Fisher's exact test (frequencies below 5) were used. In mean comparisons, the t-test was used for parametric variables while the Wilcoxon's test was used for non-parametric variables according to the Shapiro-Wilk normality test. Differences and associations between sociodemographic variables were analyzed according to gender. Two age categories were used (≤44 years old and ≥45 years old) according to the cut-off scores used in the Chilean National Health Survey 2009/2010 (46). MSD prevalence in each region and body segment were described according to gender and age category in the last 12 months without movement limitations and in the last 12 months with movement limitations. We applied ANOVA to evaluate differences between scores on each of the eight QoL dimensions regarding MSD prevalence grouped in 3 categories as a response variable (without symptoms, ≥ p10– <p75 [1 to 5 regions], and ≥p75 [6 or more regions]), followed by a post-hoc test (Bonferroni). Finally, two logistic regression models were done with the highest and lowest T-Score 50 scores on the Physical Component Summary and Mental Component Summary QoL measurements as dependent variables, while for independent variables we used the group without pains (0 painful regions), and the group with high pain prevalence (≥p75–6 or more regions without limitations) adjusted for gender and age. The goodness of fit calculation for each model was done with a Hosmer-Lemeshow test (a value above 0.05 indicates that the model fits the data).
Results
The sociodemographic characteristics of the teachers participating in this study are presented in Table 1, compared by gender. In total, 544 teachers were analyzed, of which 390 were women (72%). Mean age of the total sample was 40.3 ± 12 years; 66% of participants fell in the first age category (≤44 years). There was a significant association (p < 0.05) between the female gender and the presence of 4 or more musculoskeletal pains (≥p50) and low scores on the physical component of QoL (<T-Score). In addition, it is observed that younger teachers have significantly greater MSD (>5 regions with pain). On the other hand, a significant association is observed between the high prevalence of MSD and the components of QoL scores (PCS and MCS; see Table 2).
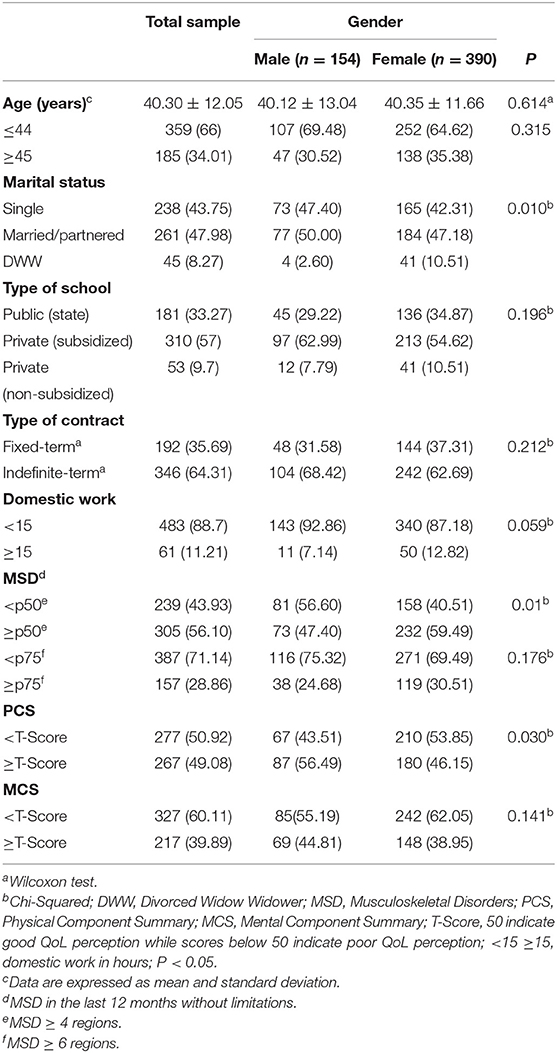
Table 1. Sociodemographic characteristics, presence of musculoskeletal disorders and quality of life, evaluated by gender in Chilean teachers.
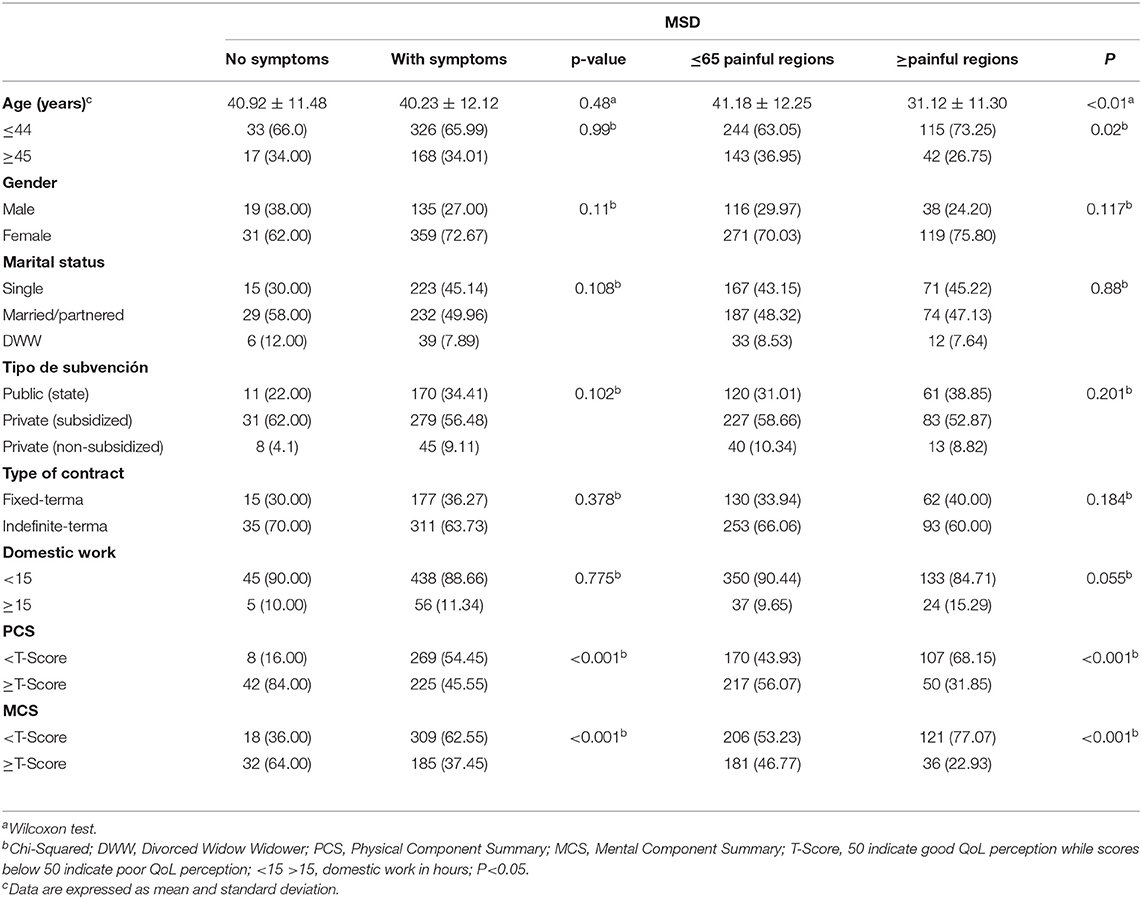
Table 2. Sociodemographic characteristics and quality of life, evaluated by the presence of musculoskeletal disorders in Chilean teachers.
Table 3 shows MSD prevalence in each body region in the total sample and according to age categories during the previous 12 months (with and without movement limitations). Around 91% reported some musculoskeletal pain in the previous 12 months without limitations. The region with the highest pain prevalence was the lower back at 80.85%, followed by the neck/shoulder segment at 67%. The ≤44 years group also presented greater prevalence of pain in the upper limbs and back, while in the lower limbs the highest prevalence was found among older teachers (≥45 years). Furthermore, when evaluating pain with mobility limitations somewhere within the body, the general prevalence was 75.18% in the total sample, with the most common regions being the neck/shoulders (52.39%) and lower back (50.5%). 64.5% of teachers ≤44 years also mentioned having over 5 painful regions with mobility limitations in the previous 12 months.
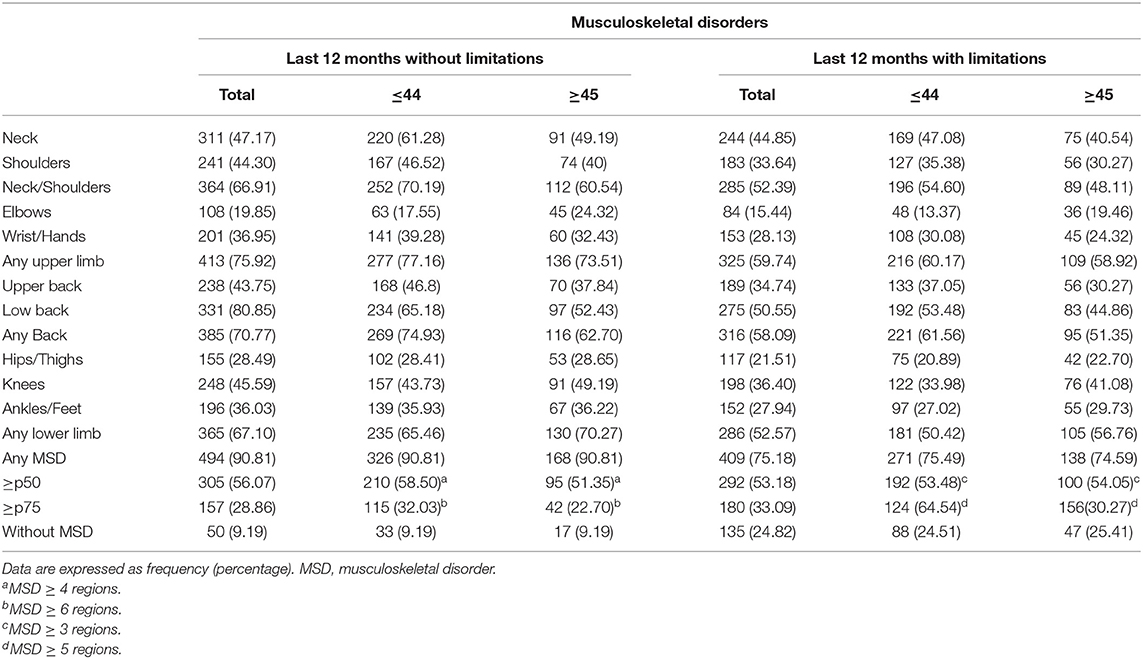
Table 3. Prevalence of musculoskeletal disorders in the last 12 months with and without movement limitations according to age ranges.
MSD prevalence in the previous 12 months without mobility limitations and with limitations presented by gender appear in Table 4. Pain prevalence in at least one body region were greater among women, with 92% reporting pain without limitations and 76.92% presenting pain with limitations. The body segments with the highest prevalence without limitations were the upper limbs (78.72%) and neck/shoulders (69.49%) corresponding to women. The only body region with a slightly higher pain prevalence in men was the ankle/foot in both survey segments (with and without limitations). Females had a higher prevalence of presenting 4 painful regions with limitations (36.15%).
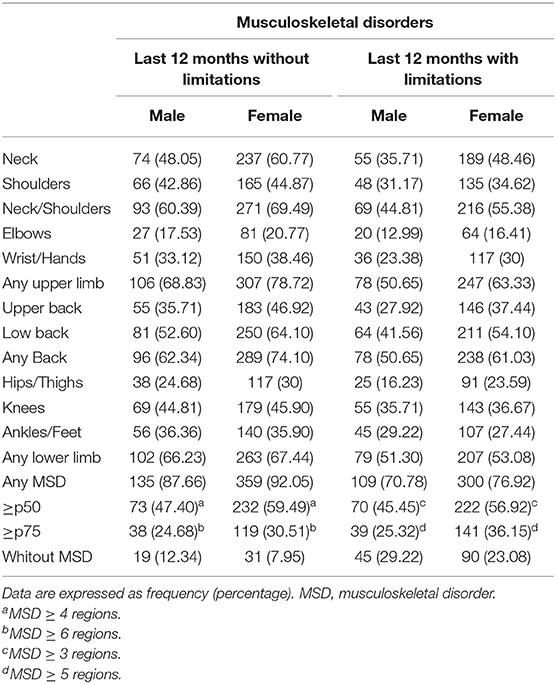
Table 4. Prevalence of musculoskeletal disorders in the last 12 months with and without movement limitations according to gender.
Table 5 shows comparisons of scores in each QoL dimension with three MSD prevalence categories. The results show that all teachers who reported no MSD had significantly higher QoL scores (better QoL) than other categories, especially compared with the group of teachers with prevalence above p75 (6 or more regions without limitations and 5 or more with limitations; p < 0.05).
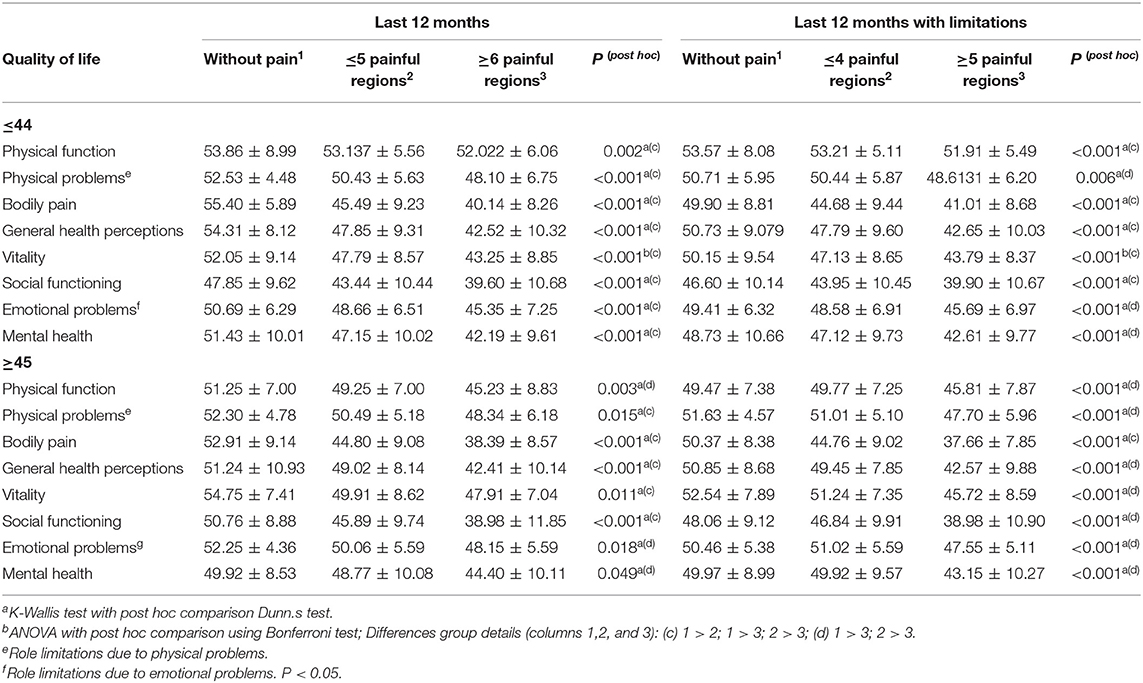
Table 5. Evaluation of the differences in the scores of the eight quality of life scales between three categories of MSD according to age ranges.
Table 6 presents the logistic regression models. Teachers who reported no painful regions are significantly associated (p < 0.05) with a decreased risk of low scores on the physical (OR: 0.20) and mental QoL components (OR: 0.44). By contrast, individuals with 6 or more painful regions (≥p75) had a greater risk of low scores on the mental (OR: 2.56, p < 0.05) and physical components (OR: 2.53, p < 0.05). Regarding age, younger teachers (≤44 years) were associated with a significantly lower risk than teachers ≥45 years of having low scores on the Physical Component Summary (OR: 0.45, p < 0.01). By contrast, younger teachers had a significantly greater risk than the second age group (≥45 years), of having low scores on the Mental Component Summary (OR: 1.66, p < 0.05).
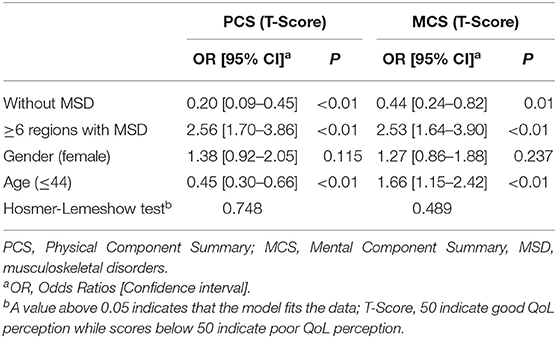
Table 6. Logistic regression to evaluate the association between the physical and mental health components of quality of life with the absence of MSD and greater equal to six painful regions (≥p75).
Discussion
The objective of this cross-sectional study was to evaluate the association of MSD with QoL in Chilean teachers. The principal results show high MSD prevalence among participants (90.81%). In this regard, teachers with more painful regions had significantly lower scores in all QoL scales, with risks of low scores on both Physical and Mental QoL scales. Age and gender according to their categories were reported as risk factors, where young teachers had a significant risk of low scores on the Mental Component Summary, while teachers in the second age category had a significant risk of low scores on the Physical Component Summary.
MSD Prevalence
Regarding MSD, 90.81% of teachers in this study reported having felt pain some-where in their body in the previous 12 months, similar to Italian teachers' reported prevalence of 91.5% (47). This MSD prevalence is relatively high considering that the maximum found in literature review about MSD among teachers was 95% prevalence in a Chinese study (23, 48). High MSD prevalence have also been reported among Latin American teachers. For instance, in Bolivia 86% reported pain in at least one part of their body in the previous 12 months (26); other studies in Brazil reported that 55% of teachers mentioned pain in at least one body segment, as well as in Chile where 88.9% of teachers reported MSD in a body region (35, 49).
Regarding MSD in each body region, lower back pain is the most common (80.85%) followed by the neck (47.17%) and knees (45.19%). These regions have already had high prevalence reported among teachers worldwide (50). For example, in Saudi Arabia 81% reported lower back pain, 58% in the neck and 62% in the knees (51); while for teachers in Turkey the prevalence were lower back 74.9%, neck 47.9% and knees 30.9% (36). In this sense, studies among teachers reveal that lower back pain is significantly associated to job provisions, work environment satisfaction (52) and the female gender (53). Additionally, a study during the health crisis by COVID-19 indicates that more than 60% of teachers have some back pain associated with non-performance of PA, non-compliance with ergonomic recommendations, and stress (54). In that vein, the highest pain associations have been reported with extremely severe depression, extremely severe anxiety and high psycho-social work demands among secondary teachers (28). In this regard, this study did not evaluate depressive states. However, teachers with higher MSD prevalence had lower QoL scores on mental health-related scales.
Regarding MSD according to the age variable, each age group in this study presented the same pain prevalence in at least one part of the body in the previous 12 months. These results have no counterpart in the literature, considering that some studies report no MSD associated with the age variable or with any sociodemographic variable in teachers (55). Other studies report greater MSD prevalence among older teachers (56, 57), while some even specifically indicate that ages 40–49 present the greatest MSD prevalence (58). Regarding gender, in this study the highest prevalence were found among women, which coincides with MSD prevalence reported in most studies done on teachers (24). However, a study in Malaysia reported a higher MSD prevalence among women but without significant associations between both genders (56). This contrasts with a study among Turkish teachers, where more MSD presented among men but without significant gender associations (19).
In Chile, there are reports that 42.6% of the general working population has chronic work-related MSD, with symptoms presenting as risk factors strongly associated with low QoL scores, especially on the physical and mental health components (33). Therefore, the organizational context of teaching work in Chile and the world presents various physical and psychosocial deficiencies resulting in the presence of MSD and a concomitant deterioration in the mental and physical health of people.
MSD and Quality of Life
The findings of this study indicate that scores on all QoL scales present significant differences among teachers, especially between those who report no MSD and those with six or more painful regions (≥p75). Furthermore, having six or more painful regions (≥p75) was reported as a significant risk associated with low scores on the Physical Component Summary and Mental Component Summary. These results are similar to reports from teachers in Turkey where MSD presence was linked with negative QoL impact, especially on the Physical Component Summary (19) and which indicated that teachers with MSD have significantly lower QoL scores and greater presence of depression (36). Similarly, studies on the working population in the USA report high muscle pain prevalence related to low QoL scores (34); and studies on dockworkers in Brazil showed similar significantly lower scores on at least 5 of the 8 QoL scales on the SF-36 instrument among individuals with MSD (32). In the Chilean general population, people with chronic musculoskeletal pain have reported physical and mental QoL impacts, especially among women (33). Studies on the working population of Chilean teachers report high MSD prevalence in urban and rural teachers with significant QoL impact (35). Some chronic health conditions impacting teachers' QoL have already been reported in Chile, a background reinforcing the fact that teachers are an at-risk group for low QoL scores de-pending on the health disorders they may present (20, 35).
Limitations
This study has several limitations. First, given the nature of this research as a cross-sectional study, only a moment of the interviewees' lives can be observed, which can influence the answer at the time of the interview and prevent studying cause-effect relations. Second, although a representative sample of teachers was obtained, it does not necessarily represent all teachers. However, it has the strength of covering three zones of Chile (north, center, and south) which helps reach a broader vision of MSD and QoL is-sues among teachers.
Conclusion
This study determined a high prevalence of MSD among Chilean teachers, with significantly greater prevalence among women than men. We also determined the impact of MSD on teachers' QoL, where younger teachers with high MSD had a greater risk of low mental component QoL scores and older teachers with high MSD had a greater risk of low physical component QoL scores. These findings should be useful for generating policies to protect teachers' physical and mental health in order to protect the people who pro-vide education to the youth of the nation.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee at Pontificia Universidad de Valparaíso, Chile (n°BIOEPUCV-H 160-2017). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
PL designed the study. PL and GV-F performed the measurements and statistical analysis, processed the data, drafted the manuscript, designed the tables, writing review, and editing. All authors discussed the results and commented on the manuscript, contributed to the article, and approved the submitted version.
Funding
This research was supported by FONDECYT Grant No. 11170716 (FONDECYT-ANID, Chile) and Vicerrectoría de Investigación y Estudios Avanzados of the Pontificia Universidad Católica de Valparaíso through project 039.346/2016–039.460/2021.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors of this work thank the directors and teachers for their willingness to participate in this study.
References
1. World Health Organization. Musculoskeletal Conditions. (2019). Available online at: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed February 02, 2020).
2. Coggon D, Ntani G, Palmer KT, Felli VE, Harari R, Barrero LH, et al. Disabling musculoskeletal pain in working populations: Is it the job, the person, or the culture? Pain. (2013) 154:856–63. doi: 10.1016/j.pain.2013.02.008
3. OIT. Prevención De Las Lesiones Y Enfermedades Profesionales a Través De La Ergonomía. Organ Int Del Trab. (2008) 21:6–8.
4. Lentz TA, Harman JS, Marlow NM, Beneciuk JM, Fillingim RB, George SZ. Factors associated with persistently high-cost health care utilization for musculoskeletal pain. PLoS One. (2019) 14:1–23. doi: 10.1371/journal.pone.0225125
5. Vargas C, Bilbeny N, Balmaceda C, Rodríguez MF, Zitko P, Rojas R, et al. Costs and consequences of chronic pain due to musculoskeletal disorders from a health system perspective in Chile. Pain Rep. (2018) 3:1–10. doi: 10.1097/PR9.0000000000000656
6. Bone Joint Initative. The Hiden Impact of Musculoskeletal on AMERICANS. (2018). Available online at: https://www.boneandjointburden.org/docs/BMUSImpactofMSKonAmericansbooklet_4thEdition%282018%29.pdf (accessed January 18, 2021).
7. Mohammadipour F, Pourranjbar M, Naderi S, Rafie F. Work-related musculoskeletal disorders in Iranian office workers: prevalence and risk factors. J Med Life. (2018) 11:328–33. doi: 10.25122/jml-2018-0054
8. Mendonça CR, Noll M, De Carvalho Santos ASEA, Dos Santos Rodrigues AP, Silveira EA. High prevalence of musculoskeletal pain in individuals with severe obesity: Sites, intensity, and associated factors. Korean J Pain. (2020) 33:245–57. doi: 10.3344/kjp.2020.33.3.245
9. Atlas A, Bondoc RG, Garrovillas RA, Lo RD, Recinto J, Yu KJ. Prevalence of low back pain among public high school teachers in the City of Manila. Philipp J Allied Heal Sci. (2007) 2:34-40. doi: 10.36413/pjahs.0201.004
10. Da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med. (2010) 53:285–323. doi: 10.1002/ajim.20750
11. Kozak A, Wirth T, Verhamme M, Nienhaus A. Musculoskeletal health, work-related risk factors and preventive measures in hairdressing: a scoping review. J Occup Med Toxicol. (2019) 14:1–14. doi: 10.1186/s12995-019-0244-y
12. Smith DR, Mihashi M, Adachi Y, Koga H, Ishitake T. A detailed analysis of musculoskeletal disorder risk factors among Japanese nurses. J Safety Res. (2006) 37:195–200. doi: 10.1016/j.jsr.2006.01.004
13. Vignoli M, Dina G, Cristian B, Bonfiglioli R. Workplace bullying as a risk factor for musculoskeletal disorders: the mediating role of job-related psychological strain. Biomed Res Int. (2015) 2015:8. doi: 10.1155/2015/712642
14. Taibi Y, Metzler YA, Bellingrath S, Müller A. A systematic overview on the risk effects of psychosocial work characteristics on musculoskeletal disorders, absenteeism, and workplace accidents. Appl Ergon. (2021) 95:103434. doi: 10.1016/j.apergo.2021.103434
15. Lizana PA, Vega-Fernadez G. Teacher teleworking during the covid-19 pandemic: Association between work hours, work–family balance and quality of life. Int J Environ Res Public Health. (2021) 18:7566. doi: 10.3390/ijerph18147566
16. Heikkinen J, Honkanen R, Williams L, Leung J, Rauma P, Quirk S, et al. Depressive disorders, anxiety disorders and subjective mental health in common musculoskeletal diseases: a review. Maturitas. (2019) 127:18–25. doi: 10.1016/j.maturitas.2019.05.011
17. Menzel NN. Psychosocial factors in musculoskeletal disorders. Crit Care Nurs Clin North Am. (2007) 19:145–53. doi: 10.1016/j.ccell.2007.02.006
18. Beaudart C, Biver E, Bruyère O, Cooper C, Al-Daghri N, Reginster JY, et al. Quality of life assessment in musculo-skeletal health. Aging Clin Exp Res. (2018) 30:413–8. doi: 10.1007/s40520-017-0794-8
19. Karakaya IÇ, Karakaya MG, Tunç E, Kihtir M. Musculoskeletal problems and quality of life of elementary school teachers. Int J Occup Saf Ergon. (2015) 21:344–50. doi: 10.1080/10803548.2015.1035921
20. Lizana PA, Vega-Fernandez G, Lera L. Association between chronic health conditions and quality of life in rural teachers. Front Psychol. (2020) 10:1–8. doi: 10.3389/fpsyg.2019.02898
21. Robalino M, Körner A. Condiciones de trabajo y salud docente: estudios de casos en Argentina, Chile, Ecuador, México, Perú y Uruguay. (2005).
22. Portilla A, Meza MF, Lizana PA. Association between emotional exhaustion and tobacco consumption in teachers. Int J Environ Res Public Health. (2022) 19:2022. doi: 10.3390/ijerph19052606
23. Erick PN, Smith DR. A systematic review of musculoskeletal disorders among school teachers. BMC Musculoskelet Disord. (2011) 12:260. doi: 10.1186/1471-2474-12-260
24. Patience E, Derek S. Musculoskeletal disorder risk factors in the teaching profession: a critical review. OA Musculoskelet Med. (2013) 1:1–10.
25. Ng YM, Voo P, Maakip I. Psychosocial factors, depression, and musculoskeletal disorders among teachers. BMC Public Health. (2019) 19:1–10. doi: 10.1186/s12889-019-6553-3
26. Solis-Soto MT, Schön A, Solis-Soto A, Parra M, Radon K. Prevalence of musculoskeletal disorders among school teachers from urban and rural areas in Chuquisaca, Bolivia: a cross-sectional study. BMC Musculoskelet Disord. (2017) 18:1–7. doi: 10.1186/s12891-017-1785-9
27. Smith DR. The prevalence and risk factors for musculoskeletal disorders among school teachers in Botswana. Occup Med Health Aff. (2014) 2:178. doi: 10.4172/2329-6879.1000178
28. Zamri EN, Moy FM, Hoe VCW. Association of psychological distress and work psychosocial factors with self-reported musculoskeletal pain among secondary school teachers in Malaysia. PLoS ONE. (2017) 12:1–15. doi: 10.1371/journal.pone.0172195
29. Alias AN, Karuppiah K, How V, Perumal V. Prevalence of musculoskeletal disorders (MSDS) among primary school female teachers in Terengganu, Malaysia. Int J Ind Ergon. (2020) 77:102957. doi: 10.1016/j.ergon.2020.102957
30. Kebede A, Abebe SM, Woldie H, Yenit MK. Low back pain and associated factors among primary school teachers in Mekele City, North Ethiopia: a cross-sectional study. Occup Ther Int. (2019) 2019:3862946. doi: 10.1155/2019/3862946
31. Algarni FS, Alkhaldi HA, Zafar H, Kachanathu SJ, Al-Shenqiti AM, Altowaijri AM. Self-reported musculoskeletal disorders and quality of life in supermarket cashiers. Int J Environ Res Public Health. (2020) 17:1–14. doi: 10.3390/ijerph17249256
32. De Carvalho MP, Schmidt LG, Soares MCF. Musculoskeletal disorders and their influence on the quality of life of the dockworker: a cross-sectional study. Work. (2016) 53:805–12. doi: 10.3233/WOR-162249
33. Mena-Iturriaga MJ, Mauri-Stecca MV, Sizer PS, Leppe J. Quality of life in chronic musculoskeletal symptomatic Chilean population: secondary analysis of National Health Survey 2009-2010. BMC Musculoskelet Disord. (2020) 21:1–7. doi: 10.1186/s12891-020-03261-x
34. McDonald M, Dibonaventura MD, Ullman S. Musculoskeletal pain in the workforce: the effects of back, arthritis, and fibromyalgia pain on quality of life and work productivity. J Occup Environ Med. (2011) 53:765–70. doi: 10.1097/JOM.0b013e318222af81
35. Vega-Fernández G, Lera L, Leyton B, Cortés P, Lizana PA. Musculoskeletal disorders associated with quality of life and body composition in urban and rural public school teachers. Front Public Health. (2021) 9:607318. doi: 10.3389/fpubh.2021.607318
36. Durmus D, Ilhanli I. Are there work-related musculoskeletal problems among teachers in Samsun, Turkey? J Back Musculoskelet Rehabil. (2012) 25:5–12. doi: 10.3233/BMR-2012-0304
37. Ministerio de Educación. Bases de datos oficiales del Centro de Estudios MINEDUC. Cent Estud MINEDUC. Available online at: http://centroestudios.mineduc.cl/index.php?t=96&i=2&cc=2519&tm=2 (accessed April 30, 2021).
38. Vidal Gamboa C, Hoffmeister Arce L, Benadof D. Factores asociados al dolor musculoesquelético en población trabajadora chilena. Cienc Trab. (2016) 18:23–7. doi: 10.4067/S0718-24492016000100005
39. Kahraman T, Genç A, Göz E. The Nordic Musculoskeletal Questionnaire: cross-cultural adaptation into Turkish assessing its psychometric properties. Disabil Rehabil. (2016) 38:2153–60. doi: 10.3109/09638288.2015.1114034
40. Martínez M, Muñoz R. Validación Del Cuestionario Nórdico Estandarizado De Síntomas Musculoesqueléticos Para La Población Trabajadora Chilena, Adicionando Una Escala De Dolor. Rev Salud Pública. (2017) 19:41–51. doi: 10.31052/1853.1180.v21.n2.16889
41. Pugh JD, Gelder L, Williams AM, Twigg DE, Wilkinson AM, Blazevich AJ. Validity and reliability of an online extended version of the Nordic Musculoskeletal Questionnaire (NMQ-E2) to measure nurses' fitness. J Clin Nurs. (2015) 24:3550–63. doi: 10.1111/jocn.12971
42. Olivares-Tirado P. Beneficiarios de Isapres: Informe Preliminar. Superintendencia de Isapres, Gobierno de Chile (2005). Available online at: www.supersalud.gob.cl/documentacion/666/articles-1062_recurso_1.pdf (accessed February 02, 2021).
43. Lizana PA, Vega-Fernadez G, Gomez-Bruton A, Leyton B, Lera L. Impact of the covid-19 pandemic on teacher quality of life: a longitudinal study from before and during the health crisis. Int J Environ Res Public Health. (2021) 18:3764. doi: 10.3390/ijerph18073764
44. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (Sf-36): I. conceptual framework and item selection. Med Care. (1992) 30:473–83. doi: 10.1097/00005650-199206000-00002
45. The World Medical Association. Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects (Declaration of Helsinki). Seoul: 59th WMA General Assembly (2008). doi: 10.1515/9783110208856.233
46. Ministerio de Salud de Chile. Encuesta Nacional de Salud 2009 – 2010. Chile: Ministerio de Salud de Chile. Available online at: https://www.minsal.cl/portal/url/item/bcb03d7bc28b64dfe040010165012d23.pdf (accessed May 10, 2021).
47. Scopa P., Pasqua di Bisceglie A, De Lotto F, Alfano A, Faiferri S, Regazzo A. Musculoskeletal disorders and work-related musculoskeletal diseases among nursery school teachers: analysis in a sample in the city of Venice. G Ital Med Lav Ergon. (2020) 42:82–6.
48. Chong EYL, Chan AHS. Subjective health complaints of teachers from primary and secondary schools in Hong Kong. Int J Occup Saf Ergon. (2010) 16:23–39. doi: 10.1080/10803548.2010.11076825
49. Paixão J, Batista I, Tânia DA, Carvalho F, Farias E. Prevalence of musculoskeletal pain among teachers. Rev Bras Epidemiol. (2009) 12:1–10.
50. Erick PN, Smith DR. Low back pain among school teachers in Botswana, prevalence and risk factors. BMC Musculoskelet Disord. (2014) 15:359. doi: 10.1186/1471-2474-15-359
51. Alqahtani T. The prevalence of foot pain and its associated factors among Saudi school teachers in Abha sector, Saudi Arabia. J Fam Med Prim Care. (2020) 9:4641. doi: 10.4103/jfmpc.jfmpc_898_20
52. Mengestu MY. Low back pain and associated factors among teachers in Gondar Town, North Gondar, Amhara Region, Ethiopia. Occup Med Health Aff. (2013) 01:1–8. doi: 10.4172/2329-6879.1000127
53. Hussein E, Raymond D, Mwangi A. Low back pain among primary school teachers in Rural Kenya: prevalence and contributing factors. Afr J Prim Health Care Fam Med. (2019) 11:1–7. doi: 10.4102/phcfm.v11i1.1819
54. Prieto-González P, Šutvajov M, Les A, Bart P. Back pain prevalence, intensity, and associated risk factors among female teachers in Slovakia during the COVID-19 pandemic : a cross-sectional study. Healthcare. (2021) 9:860. doi: 10.3390/healthcare9070860
55. Constantino Coledam DH, Júnior RP, Ribeiro EAG, de Oliveira AR. Factors associated with musculoskeletal disorders and disability in elementary teachers: a cross-sectional study. J Bodyw Mov Ther. (2019) 23:658–65. doi: 10.1016/j.jbmt.2018.05.009
56. Amit LM, Malabarbas GT. Prevalence and risk-factors of musculoskeletal disorders among provincial high school teachers in the Philippines. J UOEH. (2020) 42:151–60. doi: 10.7888/juoeh.42.151
57. Maakip I. Prevalence and risk factors of musculoskeletal disorders (MSDs) among primary and secondary school teachers : a narrative review. Austin J Musculoskelet Disord. (2017) 4:1046.
Keywords: mental health, physical health, quality of life, school teachers, gender, musculoskeletal disorders
Citation: Vega-Fernández G, Olave E and Lizana PA (2022) Musculoskeletal Disorders and Quality of Life in Chilean Teachers: A Cross-Sectional Study. Front. Public Health 10:810036. doi: 10.3389/fpubh.2022.810036
Received: 05 November 2021; Accepted: 07 March 2022;
Published: 29 March 2022.
Edited by:
Somnath Gangopadhyay, University of Calcutta, IndiaReviewed by:
Alexis Descatha, Univ Angers Inserm CHU Angers, FranceMałgorzata Grabara, Jerzy Kukuczka Academy of Physical Education in Katowice, Poland
Copyright © 2022 Vega-Fernández, Olave and Lizana. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo A. Lizana, cGFibG8ubGl6YW5hQHB1Y3YuY2w=