 Lixian Ren
Lixian Ren Jianping Ren
Jianping Ren Chaojie Liu
Chaojie Liu Mengyan He1
Mengyan He1
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 02 May 2022
Sec. Family Medicine and Primary Care
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.800612
This article is part of the Research Topic Insights in Family Medicine and Primary Care: 2021 View all 20 articles
Objective: China is attempting to establish a voluntary contracting system in primary care. This study aimed to determine the degree of consumer satisfaction with the entitlements of contract arrangements and its associated factors.
Methods: A stratified cluster sampling strategy was adopted to recruit study participants from three administrative districts of Hangzhou municipality, each containing six residential communities. In each community, 50 households were recruited. A questionnaire was administered through face-to-face interviews with members of the households who signed a contract with community health centers, to collect data regarding their sociodemographic characteristics, health conditions, and knowledge of and attitudes toward the contract entitlements. Consumer satisfaction was measured using six items rated on a five-point Likert scale ranging from “1=very dissatisfied” to “5=very satisfied” and a summed score was calculated. A mixed linear regression model was established to identify individual predictors of consumer satisfaction after adjustment of the random (intercept) effect of household clusters.
Results: Overall, the respondents reported low levels of awareness and understanding of the contract entitlements, with an average knowledge score of 8.21 (SD = 3.74) out of a maximum possible of 19. The respondents had relatively lower levels of satisfaction (satisfied or very satisfied) with their prioritized entitlements (51.5%) and hospitals at home and telemedicine services (31.3%), compared with the contract and insurance policies (85.5%) and medical services provided (87.0%). Female gender, older age, chronic conditions, and perceived better health were associated with higher levels of satisfaction, while poor awareness and knowledge were associated with lower levels of satisfaction.
Conclusion: The study participants perceived limited benefits from the contract arrangements in primary care, which may jeopardize the policy purpose of the arrangements to encourage patients to use primary care as the first contact point in accessing health care services. It is evident that consumer satisfaction with the contract entitlements varies by healthcare needs. Lower levels of satisfaction are associated with poor awareness and knowledge of the entitlements.
Internationally, there is consensus that 90% of health problems can be appropriately managed in primary care settings, while the rest require specialist consultations (1). Since the 1960s, the important role and functions of general practitioners (also known as family doctors in some countries) in the development of an efficient and quality health system have been increasingly recognized. They are the backbone of the primary care sector, aiming at maintaining and promoting both individual and population health. Empirical evidence shows that a primary-care-dominant health system outperforms the others in population health outcomes (2).
In a primary-care-dominated health care system, general practice is usually a predominant stream of medical specialization. General practitioners (GPs) are often assigned a gate-keeping role and serve as the first contact point for consumers to access health care services. Some countries even go further by introducing contract arrangements to ensure that GPs also look after the entire group of patients, not just individuals. The UK national health system (NHS) is deemed an exemplar (3). It is a publicly-funded system in which each GP is responsible for managing about 2,000 contracted patients. Specialist consultations and hospital services except for emergency care require a referral from the GPs (4). Contract arrangements have the advantage of promoting continuity and coordination of patient care despite some compromise to patient freedom of choice (2). Evidence shows that the UK system is characterized by a relatively low investment with high returns (5). Under such a system, GPs attach great importance to preventive services (6). Despite the stark contrast with the UK system, in the largely market-driven health system in the US, contract arrangements have also demonstrated their potential to reduce hospitalization and readmission of hospital patients (7), although it is often considered as a cost containment measure (8, 9).
Many countries have not introduced a contract system for various reasons. Germany, for example, has a strong tradition of corporatism and consumers enjoy freedom in choosing their first contact doctors, as well as in negotiating referred doctors (8). Contract arrangements are usually absent in low- and middle-income countries simply because they do not have enough skilled primary care professionals. This has resulted in a serious shortage of research into the potential effects of contract arrangements in low- and middle-income countries (10).
China is an upper middle-income country. Over the past two decades, China has been attempting to establish a GP-led health system. However, general practice is still in its early stage of development. Despite a serious shortage of GPs, there is both an under-use of primary care facilities and an over-use of hospital facilities in China (11, 12). The freedom of patients to bypass primary care in seeking hospital services is often blamed for the irrational distribution of health resources and services. For historical reasons, primary care facilities in China employ a large number of physicians without a university medical degree. Concerns over quality have deterred the Chinese government from introducing a gate-keeping and referral mechanism similar to the UK and several other countries (13). As an alternative option, a voluntary contracting system was introduced (14). In May 2016, the national government issued guidelines to promote primary care contract arrangements. Local governments were also encouraged to develop and use contract entitlements to incentivize patients to increase their use of primary care facilities (15). These may involve certain free services, prioritized medical appointments and referrals, and favorable policies for social health insurance programs (16). Although the contract is usually signed between a GP and a patient, the entitlements go beyond the scope of the services delivered by the GP (14).
The existing studies on China have focused on documenting the coverage of the contract arrangements (14), with a prior assumption that such arrangements are beneficial to the patients and the health care system. However, little is known about the experience of the community residents who enter into the contracts. This study contributes to the literature by measuring the satisfaction of those who signed a contract with their local community health centers. Internationally, measuring consumer satisfaction has become an important step for quality improvement (17).
A cross-sectional questionnaire survey of community residents was conducted in Hangzhou. Ethics approval was obtained from Hangzhou Normal University (Reference number 20190070). The survey was anonymous and oral informed consent was sought from the study participants prior to the survey.
Hangzhou is the capital city of Zhejiang province, one of the most developed regions in China. More than 10 million people reside in Hangzhou permanently and about 23% are older than 60 years. There are 5,925 health institutions in Hangzhou, including 2,626 community health centers (CHCs) (18). Community health services are available to all Hangzhou residents, including voluntary contract arrangements with local CHCs. Hangzhou started the voluntary contract initiative in 2014 and scaled it up across all CHCs in 2016. A total of 40.551 million patient visits to CHCs were recorded in Hangzhou in 2019 (18).
A multi-stage stratified sampling strategy was adopted. Administrative districts were sorted in order according to their local gross domestic products and evenly divided into high-, middle-, and low-income districts. One district in each category was selected: Xiacheng (high income), Jianggan (middle income), and Gongshu (low income). Six residential communities were then conveniently selected from each participating district. In each residential community, 50 households were randomly selected. All adult (>18 years) household members were eligible to participate in the study. The households that rejected invitations or were not approachable were replaced by neighboring households.
Data were collected through household visits and face-to-face interviews in November 2018. Interviewers were recruited from local CHC health workers. A total of 36 interviewers were trained and grouped into six teams. Each team visited one residential community at a time. Each eligible household member was interviewed separately and completed the questionnaire independently. Those who were absent or refused to give informed consent were excluded. This resulted in a final sample of 2,315 individuals from 906 households. After excluding those who did not enter into a contract arrangement with local CHCs, 1,304 (56.33%) respondents from 673 households were included in data analyses for the purpose of this study. This sample size was at least 25 times the number of independent variables for regression modeling, far exceeding the minimal requirement (19).
Satisfaction was defined as a subjective perception, reflecting the gap between one's expectation and actual experience (20). It was measured using a six-item scale in this study, covering six aspects of the contract entitlements, namely (1) favorable contract and insurance policies; (2) free services covered by the contract; (3) free personal inquiries and appointments; (4) prioritized consultations and referral; (5) hospitals at home and telemedicine; and (6) free prescription services for chronic diseases. The participants were asked to rate their degree of satisfaction with each of the six items on a five-point Likert scale, ranging from 1 (very dissatisfied) to 5 (very satisfied). Satisfaction ratings on the six items were summed for each respondent. The respondents were then divided into two groups using a cut-off point of 24 (exceeding the neutral total): low satisfaction (<24) and high satisfaction (≥24).
Knowledge has a significant impact on individual expectations (21). In this study, an eleven-item scale was developed to measure awareness of the respondents about their contracting institution (item 1) and GPs (item 2), and the benefits they were entitled to in line with the contract policy, which included discounts in out-of-pocket payments for insurance-covered services delivered in the contracting institution (300 Yuan reduction in deductibles–item three; 3% increase in reimbursement rates–item four); prioritized (free of charge) medical appointments (item five), consultations (item six) and referrals (item seven); free access to inquiries on personal records (item eight); and free prescribing services for chronic diseases (item nine). A score of one was assigned to a correct answer or a recognized benefit; 0 was recorded otherwise (including answer of unsure). The respondents were then asked to rate their overall understanding of the contract arrangements (item 10) and their entitlement to free prescribing services for chronic diseases (item 11) on a five-point Likert scale, ranging from 1 (very poorly) to 5 (very well). A summed score (ranging from 2 to 19) for each respondent was calculated. The respondents were subsequently divided into three knowledge groups: low (2–6, the lowest one quarter of the score range), medium (7–10, the lower middle range of score) and high (11–19, the higher middle and upper range of score), for the purpose of regression analyses since no linear correlation between knowledge and satisfaction could be assumed.
Health insurance benefits are an important component of the contract entitlement package. Although China has achieved almost universal coverage of social health insurance, multiple insurance programs with great disparities exist (22). In this study, we asked the respondents to report their membership of the two major social insurance programs: basic medical insurance for urban employees (BMIUE) and basic medical insurance for urban/rural residents (BMIUR). Both insurance programs require individual monetary contributions through premiums and copayments. The BMIUE usually has a larger funding pool and offers more generous financial benefits to enrollees than the BMIUR (23).
Previous research shows that consumer satisfaction with health care services often varies by sociodemographic characteristics of the consumers (20). In this study, we collected data in relation to the respondents' age (years), gender (male, female), marital status (unmarried, married, widowed), education (≤ primary school, middle school, high school, ≥university), employment status (employed, retired, unemployed), and occupation (management, professional, office clerical staff, company sales and services, self-employed, industrial worker, farming, other). We also asked the respondents to report their health status measured by chronic diseases (yes, no) and self-rated general health (poor, good, excellent).
The characteristics of the study participants were described through frequency distributions. Their knowledge of the contract arrangements (with a normal distribution) was described using mean scores and standard deviations, as well as percentage distributions across the high, medium and low knowledge groups.
Consumer satisfaction was described using mean and standard deviation of the satisfaction score (with a normal distribution), and the percentage of high satisfaction. Student t-tests (or ANOVA) and chi-squared tests were performed to identify the differences in the satisfaction score and the level of satisfaction, respectively, among respondents with different characteristics. The household cluster effect on consumer satisfaction was significant (ICC > 0.8). Therefore, a mixed linear regression model was established to determine individual predictors of patient satisfaction after adjustment of the random effect (intercept) of the family clusters. Independent variables were entered into the model in a block (enter approach) and all were coded as categorical measurements.
Data were managed using Epidata 3.1. Double data entry was conducted to ensure the accuracy of the data. Statistical analyses were performed using SPSS 21.0 software. A p < 0.05 was considered statistically significant.
Slightly over half (54%) of the study participants were women. The respondents had a mean age of 59 years: more than 60% were older than 60 years. The majority had not completed high school (62%), were married (86%) and retired (71%) at the time of the survey. More than 53% of respondents reported chronic diseases, but most self-rated their health as good (49%) or excellent (28%) (Table 1).
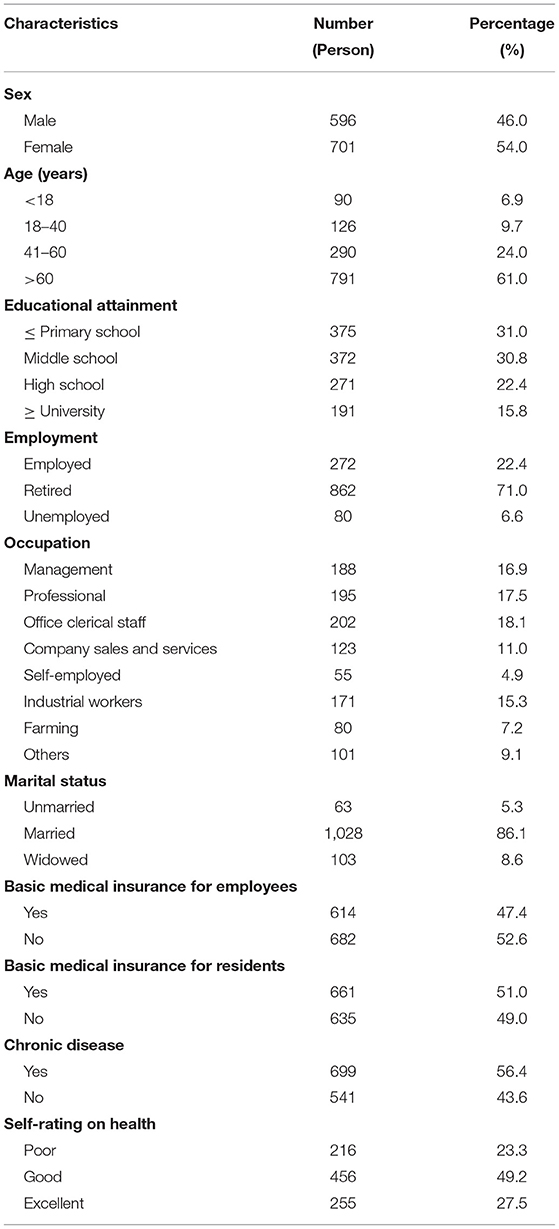
Table 1. Characteristics of study participants.
The respondents had low levels of knowledge about their contract entitlements (Table 2). More than 72.8% fell into the low (34.0%) and medium (38.7%) knowledge groups, resulting in an average score of 8.21 (SD = 3.74) out of a maximum possible of 19. Less than half of the respondents could name their contracting doctors (38.2%) or institutions (34.5%) correctly. About 59.4% only identified one or two benefits to which they were entitled. The most noticeable benefit was the 300 Yuan (US$50) reduction in deductibles for insurance-covered outpatient services (54.4%), followed by prioritized medical appointments (29.6%), 3% increase in insurance reimbursement rates (26.1%), and free access to inquiries on personal records (26.1%). Most respondents (56%) were not aware of the free prescribing services for chronic diseases.
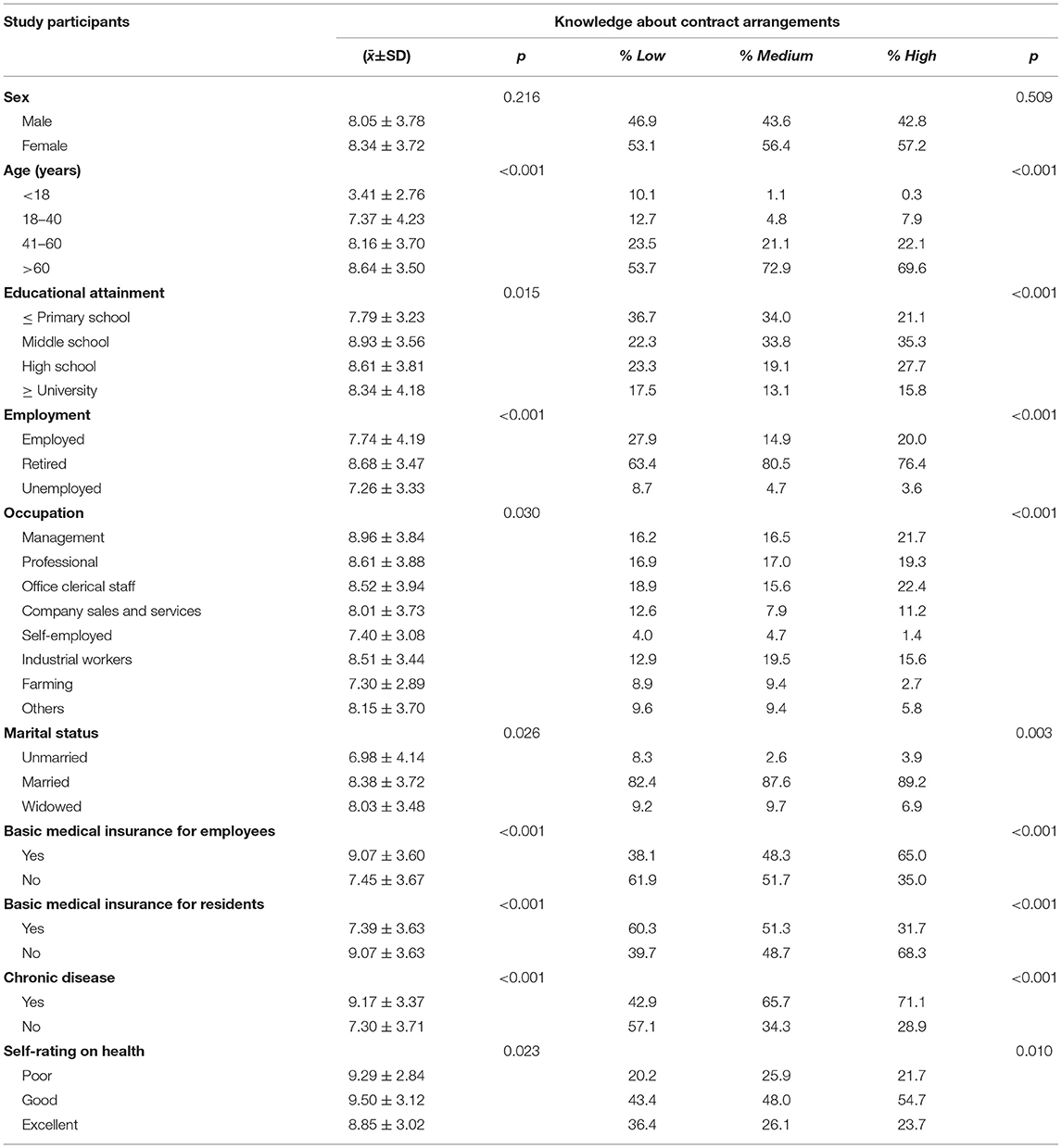
Table 2. Knowledge of study participants about contract arrangements.
Overall, the respondents had a mean satisfaction score of 22.24 (SD = 3.98), falling short of the cut-off point of 24. Variations in satisfaction with the different aspects of contract arrangements were evident. The respondents reported relatively lower levels of satisfaction with prioritized entitlements (51.5%, p < 0.001) and hospitals at home and telemedicine services (31.3%, p < 0.001), compared with favorable contract and insurance policies (85.5%) and fee discounts in the medical services provided (87.0%). The mean scores on prioritized entitlements and hospitals at home and telemedicine services fell below 4 (satisfied) (Table 3).

Table 3. Consumer satisfaction with contract arrangements.
The respondents who were older, retired, reported chronic conditions, and had a higher knowledge score on contract entitlements reported significantly (p < 0.001) higher degrees of satisfaction than the others. Similarly, those respondents were also more likely to fall into the high satisfaction group. Women were more likely to report higher satisfaction than men (Table 4).
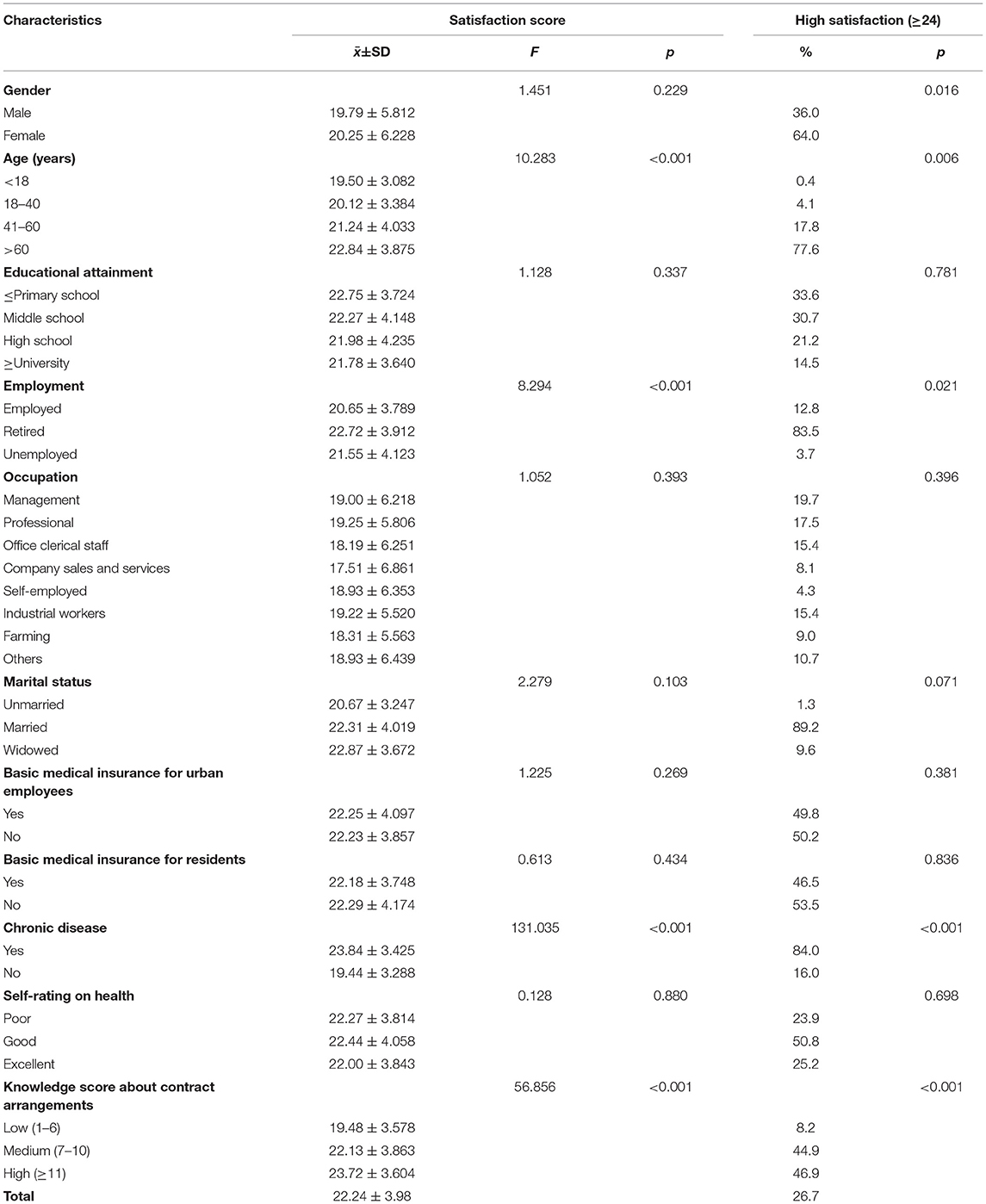
Table 4. Satisfaction with contract arrangements of respondents with different characteristics.
The high ICC values of the null model indicated a significant cluster effect of households on consumer satisfaction. The two-level mixed effect linear model generated consistent results after adjustment for variations in the random effect of family clusters (p < 0.001) as compared with those of the individual-level fixed effect model. High levels of knowledge on contract entitlements (β = 2.184–4.858, p < 0.01) and self-rated excellent health (β = 0.980, p = 0.016) were associated with higher levels of satisfaction with contract arrangements, while the absence of chronic conditions (β = −4.034, p < 0.001) was associated with lower levels of satisfaction with contract arrangements (Table 5).
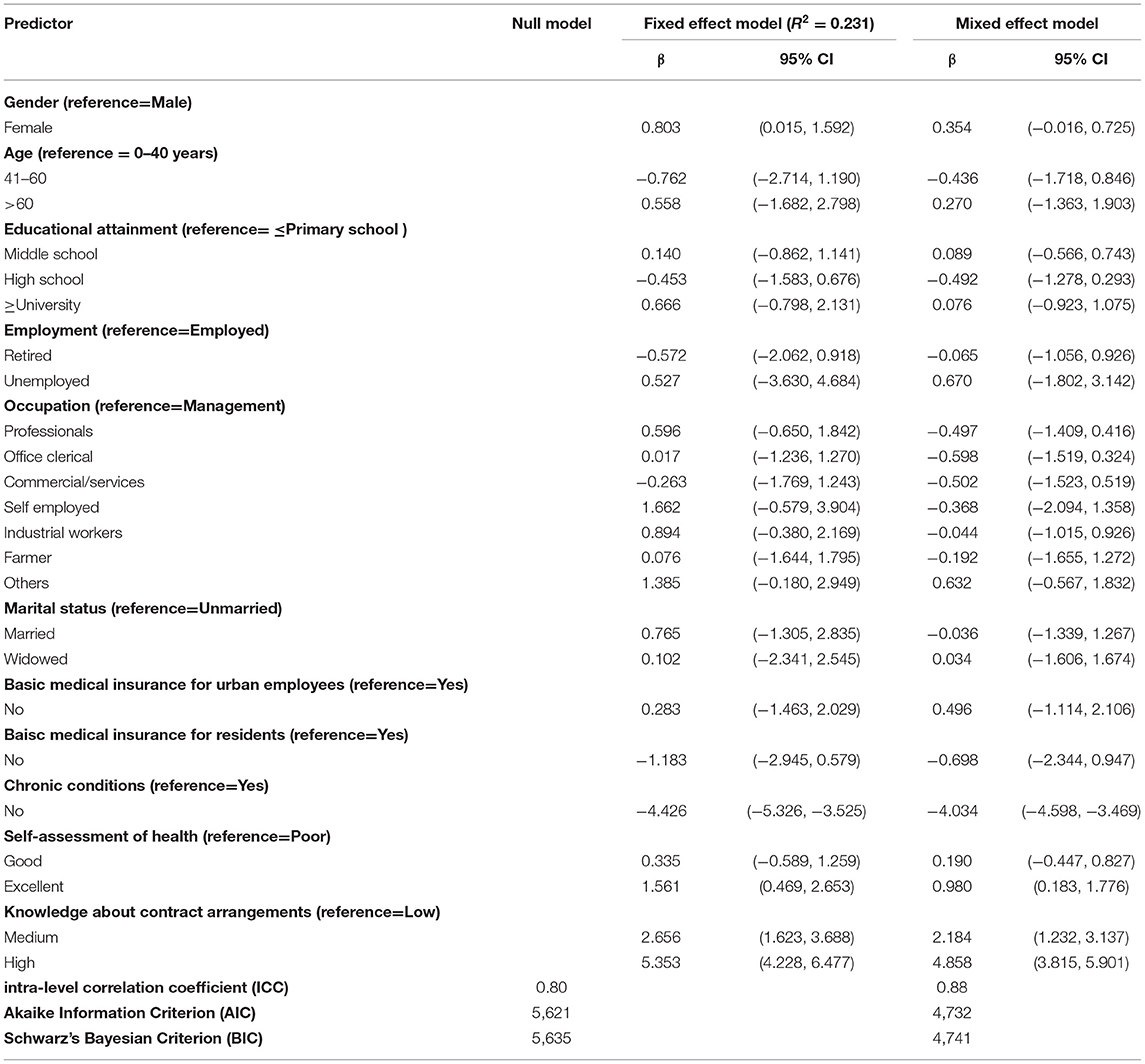
Table 5. Multivariate linear regression analysis on factors associated with consumer satisfaction.
The level of awareness and knowledge of contract entitlements of the study participants was very low, although they had all entered into a contract arrangement with their local CHC and the system has been fully implemented since 2016 (24). Less than half of the respondents could correctly identify two or more entitlements. The satisfaction rates with the contract entitlements ranged from 31 to 87%. Higher awareness, better perceived health, and living with chronic conditions are significant predictors of higher levels of satisfaction after adjustment for variations in other variables and the random effect of family clusters.
The low level of awareness and knowledge of the contract entitlements is concerning as it can jeopardize the attainment of the intended goals. We found that the financial benefit of discounts in out-of-pocket payments was most acknowledged, with 54.4% of respondents noticing the sizable 300 Yuan reduction in deductibles. Similar financial benefits are widely available across China despite variations in policy designs. In Shanghai, for example, contracted patients could be prescribed up to 2 months of medications for chronic conditions which saves costs on medical appointments and consultation fees, a benefit which is not readily available to non-contracted patients (25). However, it is not clear whether these financial benefits provide sufficient incentives to encourage consumers to seek medical attention from primary care facilities. Over the past decade, the volume of patient visits to primary care facilities has increased significantly; but patient visits to primary care as a proportion of the total volume of outpatient services has actually been declining in China (26). It appears that a lack of trust in primary care imposes a great barrier to diverting hospital patients to primary care. The perceived quality of medical services in primary care is often deemed inferior to those provided in hospitals (27). Although primary care has the advantage of maintaining continuous relationships with patients and GPs are well positioned to coordinate care on behalf of their patients (2), these benefits are not well endorsed by the patients, according to the findings of this study. Indeed, <30% of the participants in our study realized the benefits of prioritized medical appointments and referrals and free access to inquiries on personal records. Previous studies showed that many people do not trust the competency of primary care providers in disease diagnosis and management. The legacy of the barefoot doctors led them to believe that primary care doctors nowadays are still inferior to hospital specialists (28).
In this study, we found that 56.33% of Hangzhou residents entered into contract arrangements with local CHCs, which is slightly higher than the average of 50.43% in China (29). Although Hangzhou did not lead in the contract rate (30), it outperformed some other developed regions in China such as Shanghai Changning District (52.8%) (31) and Guangdong province (52.9%) (32). Perceived financial benefits may be a major contributor to encourage consumers to sign a contract with CHCs in China. We found that the contracted patients were predominantly elderly and retirees. It is important to note that consumers do not need to pay a fee to enter into a contract arrangement. The contract arrangement system operates as part of the essential public health package funded by the government. Those who enter into contract arrangements still maintain freedom in their choice of providers. They are not obligated to abide by any conditions imposed by the contracts. Because “contract coverage” is one of the performance indicators of the essential public health package, CHCs often implement very aggressive strategies to incentivize residents to sign contracts. From the perspective of consumers, there is little to lose from entering into a contract with a CHC (29).
Our study revealed that consumer satisfaction with the contract arrangements fell short of expectations. We found that only 26.7% of the study participants obtained a summed satisfaction score of higher than 24, exceeding the neutral total. Although over 85% of the respondents were satisfied with the financial benefits of discounts in medical services, only slightly more than half of our study participants were satisfied with their entitlements for prioritized medical appointments and referrals and less than one third were satisfied with hospitals at home and telemedicine services. Specialist and hospital services can become more efficient and more effective by liaising with primary care workers (28). However, it is not possible for GPs to fulfill such a role without the trust and acceptance of consumers.
However, there are some positive signs. We found in this study that 79% of respondents were satisfied with the free prescription services for chronic diseases under the contract arrangements. This may ease some of the burdens on overcrowded hospitals (33). Further evidence needs to be gathered to support such a claim. In theory, the better management of chronic conditions through primary care is critical, not only to improve the quality of life of patients but also to reduce preventable hospital admissions (28). GPs are best positioned to manage chronic conditions as they can establish a long-term continuing relationship with their patients and they understand the multiple needs of their patients best (34). Interestingly, less than half the respondents in our study could name their contracting doctors. Liu et al. (35) found that patients in China favor a concept of continuity centered around team efforts facilitated by information technologies.
The Chinese government is determined to continue to expand the initiative of contract arrangements with primary care. Our study shows that consumers' lack of awareness and understanding of contract entitlements may jeopardize such an effort. The findings have some policy implications. Firstly, the CHC approach to entering into contracts with community residents does not provide any mechanism or incentives to ensure the effective provision and materialization of contract entitlements. Secondly, contracting by itself is not the ultimate goal. A systems approach is needed to enable contract arrangements to serve as an instrument to improve the continuity and coordination of patient care. Thirdly, more radical system restructuring in China, such as the introduction of a gatekeeping mechanism through primary care, can be hindered by the low confidence from the government and trust from the public (27). Finally, the fragmentations in policy development across sectors in China need to be addressed (36) so that various incentives can be better aligned (37) and public trust in primary care can be regained (15). Unlike many developed countries, where a “gatekeeper” role has been assigned to GPs through social health insurance policies (38, 39), the Chinese system currently depends on voluntary contract arrangements. A systems approach is needed to achieve the policy goals of the contract arrangement system. These will include, but are not limited to, a strong commitment from the government, better aligned policies across sectors, the strong capacity of GPs, and public endorsement and support (40, 41).
There are several limitations in this study. We assessed patient satisfaction with the contract entitlements, but did not evaluate its impacts on the entire healthcare delivery system. Further studies are needed to systematically examine the impacts of the contracting system. The study adopted a cross-sectional design, which prevents causal conclusions. The study sample was drawn from Hangzhou, one of the most developed regions in China. Any attempts to extrapolate the findings need to be cautious.
Contract arrangements for community residents with local primary care institutions represent the Chinese government's effort to reverse the hospital-dominant system in healthcare service delivery. Despite the rapid expansion of contracting rates, consumer awareness and understanding of contract entitlements is low, according to the findings of this study. Higher awareness, better perceived health, and living with chronic conditions are significant predictors of higher levels of satisfaction with the contract arrangements. Although the current system may bring certain benefits to consumers living with chronic conditions, a better design of contract arrangements, if not a fundamental change in the health care system, will be required to further advance the contracting system. Improving consumers' awareness and understanding of contract entitlements may help, but alone it is not enough.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics approval for the study protocol was obtained from the Hangzhou Normal University (Reference Number 20190070). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JR and CL contributed to the conceptualization and methodological design. LR, MH, and XQ contributed to the collection and analysis of data. LR, JR, and CL contributed to the interpretation of the results and the drafting of the manuscript. All authors mentioned contributed to technical enrichment, the writing and also reviewed, and then approved the final manuscript.
This work was supported by National Natural Science Foundation of China (71874047) and Basic Public Welfare Research Program of Zhejiang Province (LGF21G030003).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Liu Z, Tan Y, Liang H, Gu Y, Wang X, Hao Y, et al. Factors influencing residents' willingness to contract with general practitioners in Guangzhou, China, during the GP policy trial phase: a cross-sectional study based on Andersen's behavioral model of health services use. Inquiry. (2019) 56:46958019845484. doi: 10.1177/0046958019845484
2. Shi L, Lee D-C, Liang H, Zhang L, Makinen M, Blanchet N, et al. Community health centers and primary care access and quality for chronically-ill patients - a case-comparison study of urban Guangdong Province, China. Int J Equity Health. (2015) 14:90. doi: 10.1186/s12939-015-0222-7
3. Koperski M. The state of primary care in the United States of America and lessons for primary care groups in the United Kingdom. Br J Gen Pract. (2000) 50:319–22.
4. Ting S, Ou-min S HW. Foreign family physician service model and its enlightenment on China. Heilongjiang Med. (2015) 39:852–3. doi: 10.3969/j.issn.1004-5775.2015.07.059
5. Yuan-yuan T, Xiao-yao W DG. Foreign Family Doctor Service Mode. Chinese Prim Heal Care. (2015) 29:9–11. doi: 10.3969/j.issn.1001-568X.2015.02.0004
6. Peckham S. The new general practice contract and reform of primary care in the United Kingdom. Health Policy. (2007) 2:34–48. doi: 10.12927/hcpol.2007.18873
7. Gilfillan RJ, Tomcavage J, Rosenthal MB, Davis DE, Graham J, Roy JA, et al. Value and the medical home: effects of transformed primary care. Am J Manag Care. (2010) 16:607–14.
8. Yuxin S, Tangshui S, Ling B QY. Experience and inspiration of contracting services of foreign family doctors. Chinese Foreign Entrep. (2019) 8:218–9.
9. Zwar N. Family medicine in the USA-an Australian perspective. Aust Fam Physician. (2010) 39:360–1.
10. Munge K, Mulupi S, Barasa E, Chuma J. A critical analysis of purchasing arrangements in Kenya: the case of micro health insurance. BMC Health Serv Res. (2019) 19:45. doi: 10.1186/s12913-018-3863-6
11. Wu D, Lam TP, Lam KF, Zhou XD, Sun KS. Health reforms in china: the public's choices for first-contact care in urban areas. Fam Pract. (2017) 34:194–200. doi: 10.1093/fampra/cmw133
12. Wu D, Lam TP. Underuse of primary care in China: the scale, causes, and solutions. J Am Board Fam Med. (2016) 29:240–7. doi: 10.3122/jabfm.2016.02.150159
13. Luo Z, Bai X, Min R, Tang C, Fang P. Factors influencing the work passion of Chinese community health service workers: an investigation in five provinces. BMC Fam Pract. (2014) 15:77. doi: 10.1186/1471-2296-15-77
14. Wang H, Shi L, Han X, Zhang J, Ma Y, Yang X, et al. Factors associated with contracted services of Chinese family doctors from the perspective of medical staff and consumers: a cross-sectional study. BMC Health Serv Res. (2019) 19:986. doi: 10.1186/s12913-019-4801-y
15. Yuan S, Wang F, Li X, Jia M, Tian M. Facilitators and barriers to implement the family doctor contracting services in China: findings from a qualitative study. BMJ Open. (2019) 9:e032444. doi: 10.1136/bmjopen-2019-032444
16. Lieber SR, Kim SY, Volk ML. Power and control: contracts and the patient-physician relationship. Int J Clin Pract. (2011) 65:1214–7. doi: 10.1111/j.1742-1241.2011.02762.x
17. Harris LE, Swindle RW, Mungai SM, Weinberger M, Tierney WM. Measuring patient satisfaction for quality improvement. Med Care. (1999) 37:1207–13. doi: 10.1097/00005650-199912000-00004
18. Hangzhou Statistical Yearbook. Available online at: http://tjj.hangzhou.gov.cn/art/2020/10/29/art_1229453592_3819709.html
19. Stoltzfus JC. Logistic regression: a brief primer. Acad Emerg Med. (2011) 18:1099–104. doi: 10.1111/j.1553-2712.2011.01185.x
20. Manzoor F, Wei L, Hussain A, Asif M, Shah SIA. Patient satisfaction with health care services; an application of physician's behavior as a moderator. Int J Environ Res Public Health. (2019) 16:3318. doi: 10.3390/ijerph16183318
21. Walker RC, Tong A, Howard K, Palmer SC. Patient expectations and experiences of remote monitoring for chronic diseases: systematic review and thematic synthesis of qualitative studies. Int J Med Inform. (2019) 124:78–85. doi: 10.1016/j.ijmedinf.2019.01.013
22. Wang Z, Li X, Chen M, Si L. Social health insurance, healthcare utilization, and costs in middle-aged and elderly community-dwelling adults in China. Int J Equity Health. (2018) 17:17. doi: 10.1186/s12939-018-0733-0
23. Choi WI, Shi H, Bian Y, Hu H. Development of commercial health insurance in China: a systematic literature review. Biomed Res Int. (2018) 2018:3163746. doi: 10.1155/2018/3163746
24. Notice of the General Office of the Hangzhou Municipal People's Government on Issuing the Implementation Plan (Trial) for the Integrated Contracted Services of Medical Care in Hangzhou. Available online at: http://wsjkw.hangzhou.gov.cn/art/2015/3/16/art_1671470_37097008.html
25. Wei X, Li H, Yang N, Wong SYS, Owolabi O, Xu J, et al. Comparing quality of public primary care between Hong Kong and Shanghai using validated patient assessment tools. PLoS ONE. (2015) 10:e0121269. doi: 10.1371/journal.pone.0121269
26. Xu J, Powell-Jackson T, Mills A. Effectiveness of primary care gatekeeping: difference-in-differences evaluation of a pilot scheme in China. BMJ Glob Heal. (2020) 5:e002792. doi: 10.1136/bmjgh-2020-002792
27. Chen W, Feng Y, Fang J, Wu J, Huang X, Wang X, et al. Effect of trust in primary care physicians on patient satisfaction: a cross-sectional study among patients with hypertension in rural China. BMC Fam Pract. (2020) 21:196. doi: 10.1186/s12875-020-01268-w
28. Wu D, Lam TP, Lam KF, Zhou XD, Sun KS. Public views towards community health and hospital-based outpatient services and their utilisation in Zhejiang, China: a mixed methods study. BMJ Open. (2017) 7:e017611. doi: 10.1136/bmjopen-2017-017611
29. Shang X, Huang Y, Li B, Yang Q, Zhao Y, Wang W, et al. Residents' awareness of family doctor contract services, status of contract with a family doctor, and contract service needs in Zhejiang Province, China: a cross-sectional study. Int J Environ Res Public Health. (2019) 16:3312. doi: 10.3390/ijerph16183312
30. Jiaoling H, Hong L, Weisheng Z, Jianmin Z, Chao W, Xiang C, et al. Influencing factor analysis of signing a contract with a family doctor among residents in Hongkou district. Chinese Gen Pract. (2019) 22:687–91. doi: 10.12114/j.issn.1007-9572.2018.00.340
31. Yuan L, Zhou C, Jiang P, Xu L, Zhang Q, Xu B. Community residents' demand for family physician service in Changning Districe, Shanghai. Chinese Gen Pract. (2014) 17:3860–4. doi: 10.3969/j.issn.1007-9572.2014.32.020
32. MH. Study on the status of family doctor signing service in different areas of guangdong province and it's countermeasure proposal. Guangzhou Guangzhou Med Univ. (2017).
33. Chen L, Horton R, Summerskill W. A call for research papers from China. Lancet. (2009) 373:1324. doi: 10.1016/S0140-6736(09)60754-6
34. Silina V, Kalda R. Challenges for clinical practice and research in family medicine in reducing the risk of chronic diseases. Notes on the EGPRN Spring Conference 2017 in Riga. Eur J Gen Pract. (2018) 24:112–7. doi: 10.1080/13814788.2018.1429594
35. Liu C, Wu Y, Chi X. Relationship preferences and experience of primary care patients in continuity of care: a case study in Beijing, China. BMC Health Serv Res. (2017) 17:585. doi: 10.1186/s12913-017-2536-1
36. Chen S, Chen Y, Feng Z, Chen X, Wang Z, Zhu J, et al. Barriers of effective health insurance coverage for rural-to-urban migrant workers in China: a systematic review and policy gap analysis. BMC Public Health. (2020) 20:408. doi: 10.1186/s12889-020-8448-8
37. Ma X, Wang H, Yang L, Shi L, Liu X. Realigning the incentive system for China's primary healthcare providers. BMJ. (2019) 365:l2406. doi: 10.1136/bmj.l2406
38. Farmer J, Iversen L, Campbell NC, Guest C, Chesson R, Deans G, et al. Rural/urban differences in accounts of patients' initial decisions to consult primary care. Health Place. (2006) 12:210–21. doi: 10.1016/j.healthplace.2004.11.007
39. Peckham S, Falconer J, Gillam S, Hann A, Kendall S, Nanchahal K, et al. The organisation and delivery of health improvement in general practice and primary care: a scoping study. Health Serv Deliv Res. (2015) 3:5. doi: 10.3310/hsdr03290
40. Li X, Krumholz HM, Yip W, Cheng KK, De Maeseneer J, Meng Q, et al. Quality of primary health care in China: challenges and recommendations. Lancet. (2020) 395:1802–12. doi: 10.1016/S0140-6736(20)30122-7
Keywords: primary care, consumer satisfaction, care contract, general practitioners, healthcare needs
Citation: Ren L, Ren J, Liu C, He M and Qiu X (2022) Policy Goals of Contract Arrangements in Primary Care in Jeopardy: A Cross-Sectional Consumer Satisfaction Survey of Community Residents in Hangzhou, China. Front. Public Health 10:800612. doi: 10.3389/fpubh.2022.800612
Received: 23 October 2021; Accepted: 12 April 2022;
Published: 02 May 2022.
Edited by:
Arch Mainous, University of Florida, United StatesReviewed by:
Saulo Vasconcelos Rocha, University State South-West of Bahia, BrazilCopyright © 2022 Ren, Ren, Liu, He and Qiu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianping Ren, anByZW4yMDE2QDE2My5jb20=; Chaojie Liu, Yy5saXVAbGF0cm9iZS5lZHUuYXU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.