 Mikaila Kaboré1*
Mikaila Kaboré1* Kongnimissom Apoline Sondo1,2
Kongnimissom Apoline Sondo1,2 Désiré Lucien Dahourou3
Désiré Lucien Dahourou3 Yacouba Cissoko4Issa Konaté4Abdoulaye Zaré1
Yacouba Cissoko4Issa Konaté4Abdoulaye Zaré1 Brice Bicaba5
Brice Bicaba5 Boukary Ouedraogo5Hermann Barro5Eric Arnaud Diendéré2Isabella Asamoah6Sandrine Nadège Damoue5Baperman Abdel Aziz Siri5Ismael Diallo2Peter Puplampu6Armel G. Poda7Yacouba Toloba4Sounkalo Dao4Martial Ouédraogo2Seni Kouanda3
Boukary Ouedraogo5Hermann Barro5Eric Arnaud Diendéré2Isabella Asamoah6Sandrine Nadège Damoue5Baperman Abdel Aziz Siri5Ismael Diallo2Peter Puplampu6Armel G. Poda7Yacouba Toloba4Sounkalo Dao4Martial Ouédraogo2Seni Kouanda3- 1Infectious Diseases Department, Yalgado Ouedraogo Teaching Hospital, Ouagadougou, Burkina Faso
- 2Training and Research Unit in Health Sciences, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso
- 3Department of Biomedical and Public Health, Research Institute of Health Sciences, Bobo Dioulasso, Burkina Faso
- 4Faculty of Medicine and Odontostomatology, University of Sciences, Techniques and Technologies of Bamako (USTTB), Bamako, Mali
- 5Ministry of Health, Ouagadougou, Burkina Faso
- 6Infectious Diseases Unit, Department of Medicine, Korle-Bu Teaching Hospital, Accra, Ghana
- 7Department of Infectious Diseases, Souro Sanon Teaching Hospital, Bobo-Dioulasso, Burkina Faso
Background: To limit the spread of COVID-19 due to imported cases, Burkina Faso has set up quarantine measures for arriving passengers. We aimed to determine the incidence and predictors of imported cases of COVID-19 in Burkina Faso.
Methods: A prospective cohort study was performed using data from passengers arriving at the airport from April 9 to August 31, 2020. The data was extracted from the District Health Information Software 2 (DHIS2) platform. Cox regression was used to identify predictors of imported cases of COVID-19.
Results: Among 6,332 travelers who arrived in the study period, 173 imported cases (2.7%) were recorded. The incidence rate was 1.9 cases per 1,000 traveler-days (95%CI: 1.6–2.2 per 1,000). Passengers arriving in April (Adjusted hazard ratio [aHR] = 3.56; 95%CI: 1.62–7.81) and May (aHR = 1.92; 95% CI: 1.18–3.12) were more at risk of being tested positive compared to those arriving in August, as well as, passengers presenting with one symptom (aHR = 3.71; 95% CI: 1.63–8.43) and at least two symptoms (aHR = 10.82; 95% CI: 5.24–22,30) compared to asymptomatic travelers.
Conclusions: The incidence of imported cases was relatively low in Burkina Faso between April and August 2020. The period of travel and the presence of symptoms at arrival predicted the risk of being tested positive to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This is essential in the context of the high circulation of virus variants worldwide and the low local capacity to perform genotyping tests to strengthen the surveillance and screening capacities at the points of entry into the country.
Introduction
In early December 2019, the first cases of infection with COVID-19 were recorded in China (1, 2). Gradually, other continents have been affected by tourism and trade-related movements of people (3–5). On March 11, 2020, WHO declared a pandemic in view of the spread of the virus around the world (6). As of October 30, 2020, there were 46,166,518 confirmed cases with 1,196,362 deaths worldwide with a case fatality of 2.6%. Africa remains one of the regions least affected by the coronavirus pandemic (7–9).
At the onset, the main driver of the pandemic's expansion was international tourists and commercial travels from China, which was the epicenter of the epidemic. Many cases of coronavirus infections have thus been associated with a travel history that suggests the notion of imported cases of COVID-19 (5, 10, 11).
Like other countries in the world, Burkina Faso has been facing this health crisis since March 9, 2020, when the first two imported cases were recorded in the country. As of March 19, 26 confirmed cases of COVID-19 were recorded (12). Since then, measures have been taken by the authorities to reduce the spread of the disease, including the closure of land, rail, and airport which took place on March 20, 2020 (13). This measure negatively impacted the country's economy, especially the livelihoods of populations. In the field of health, the COVID-19 pandemic has displayed a dysfunction of health systems with disruption of the epidemiological surveillance system (14).
The goal of this measure was to interrupt the transmission of the virus through cases imported by travelers from epidemic countries as did most countries in the world (13). From April 9, the government decided to repatriate Burkinabè as well as humanitarian aid workers and other Non-Governmental Organizations (NGOs) workers retained in countries, most of which were already in epidemics. To prevent the risk of imported cases of COVID-19, the authorities have put in place quarantine measures including 15 days of isolation upon arrival. It only concerned passengers entering by air.
Several previous studies conducted mostly in Asia reported epidemiological and clinical aspects of imported cases of COVID-19 (11, 15–18). However, little is known about the imported cases of COVID-19 in Africa. COVID-19 screening tests are carried out before and systematically on the day of departure of travelers, however, we find cases of COVID-19 upon their arrival in the countries of destination (19). Hence the interest of our study was to estimate the incidence and predictors of imported cases of COVID-19 among inbound travelers to Burkina Faso.
Methods
Study Site, Type, and Period
The study was conducted nationwide in Burkina Faso. There are two international airports located in the two largest cities namely Ouagadougou and Bobo Dioulasso. These cities have the highest concentration of the national urban population (80.5%) (20).
Figure 1 shows the 13 regions of the country. Of these, eight are expected to receive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive travelers. The Center region (157 cases), Haut-Bassins (5 cases), and Centre-Sud (5 cases) were the most affected.
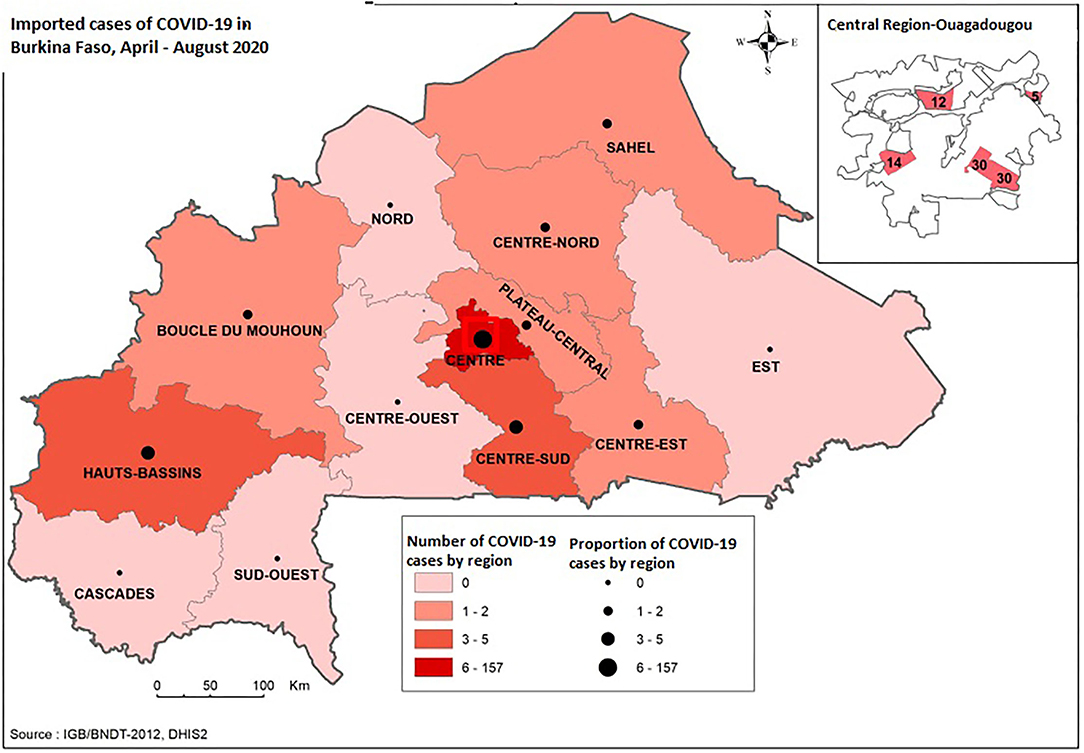
Figure 1. Mapping of regions of residence of imported COVID-19 cases, April-August 2020, Burkina Faso.
On arrival, passengers were systematically placed in quarantine in sites chosen for this purpose. These consisted mainly of hotels meeting the standards of amenities defined by the health authorities.
Quarantine or containment measures are restrictions of activities of suspicious persons who are not sick or the retaining of suspected baggage, containers, or goods. The objective of the quarantine is monitoring their symptoms and ensuring the early detection of cases so as to prevent the possible spread of infection (21). We conducted a prospective cohort study including arrival passengers from April 9 to August 31, 2020, with 15 days of the follow-up period.
Study Population
All arriving passengers by international flight at both airports who were admitted to quarantine sites for two weeks during the study period were eligible in this study.
Passengers who have correctly completed the notification forms and those who were compliant with the two weeks confinement were included in this study.
Data Source
As part of the fight against COVID-19, the Ministry of Health has set up a database to manage all data collected in relation to the disease. This database was designed using District Health Information Software (DHIS) version 2. The data collected in this database is follow-up information on patients, contacts, travelers, and laboratory data. We extracted data concerning incoming travelers by the airport.
Study Variables
The study variables were socio-demographic variables (age, gender, region, country of origin), clinical variables (symptoms declared by the traveler: fever or history of fever, asthenia, cough, dyspnea, rhinitis, chest pain, headache), and biological variables (dates and analysis report of SARS-CoV-2 RT-PCR form oral and/or nasopharyngeal specimen taken on day 1, day 8, and day 15).
Statistical Analyses
The study outcome was COVID-19 infection is defined as SARS-CoV-2 RT-PCR positive during follow-up. Study participant characteristics are presented as frequencies (percentage) for categorical variables, whereas continuous variables are presented using median and interquartile ranges (IQR). The participant's time at risk started at the arrival date and ended either at the first COVID-19 positive test or was censored at 15 days defining the end of the containment period for those with SARS-CoV-2 negative test at 1, 8, and 15 days. We estimated the cumulative incidence of COVID-19 infection with its confidence interval. Cox regression was used to estimate hazard ratios (HRs) of an RT-PCR-positive test. Variables associated with the univariate analysis with p < 0.25 were included in a multivariate analysis. Then, we conducted a stepwise descendant analysis. Variables were retained in the final model if significantly associated (p < 0.05) with the RT-PCR-positive test. All analyses were performed using SAS 9.4 (Cary, NC, USA).
Results
Basic Characteristics of Participants
From April 9 to August 31, 2020, 6,332 passengers arriving in Burkina Faso at the country's two international airports and compliant with the 15 days quarantine measures were included in this study. Table 1 provides the baseline characteristics of the study participants. Most of the participants were aged between 30 and 59 years. The majority was male (70%) and arrived in July and August 2020 (81.6%), from African countries (65.1%). Less than 1%, reported exposure history to symptomatic COVID-19 patients.
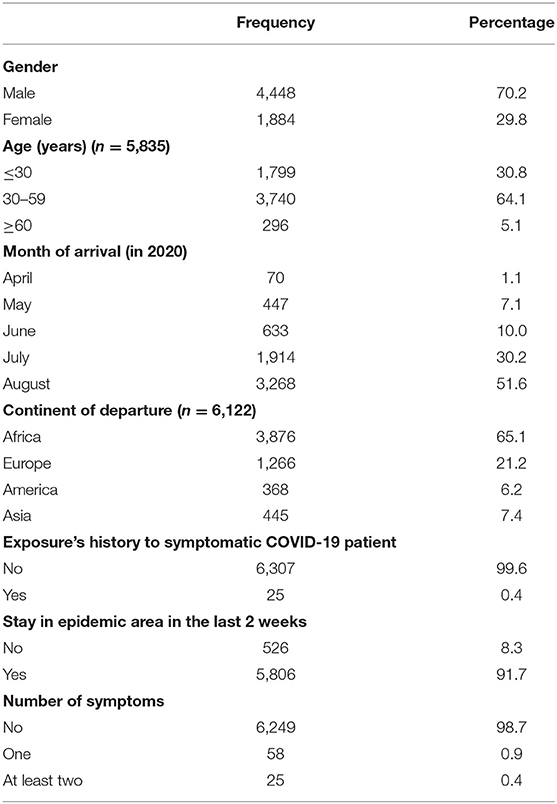
Table 1. Baseline characteristics of participants.
Overall, 98.7% of participants were asymptomatic at arrival. The remaining presented either one symptom (0.9%) or at least two symptoms (0.4%) during their containment.
Incidence of Imported Cases of COVID-19 in Burkina Faso
During follow-up, 173 passengers (2.7%) had at least one SARS-CoV-2 RT-PCR positive result. This represented 17.9% of 965 confirmed cases of COVID-19 during the study period. The total participant time at risk was 86,476.5 passengers-days. The incidence rate of SARS-CoV-2 infection was 1.9 cases per 1,000 passengers-day (95% CI: 1.6–2.2 per 1,000) (Figure 2). Among passengers who tested positive for SARS-CoV-2, 80% were tested positive on the first day of arrival, 11% on day 8, and 9% on day 15.
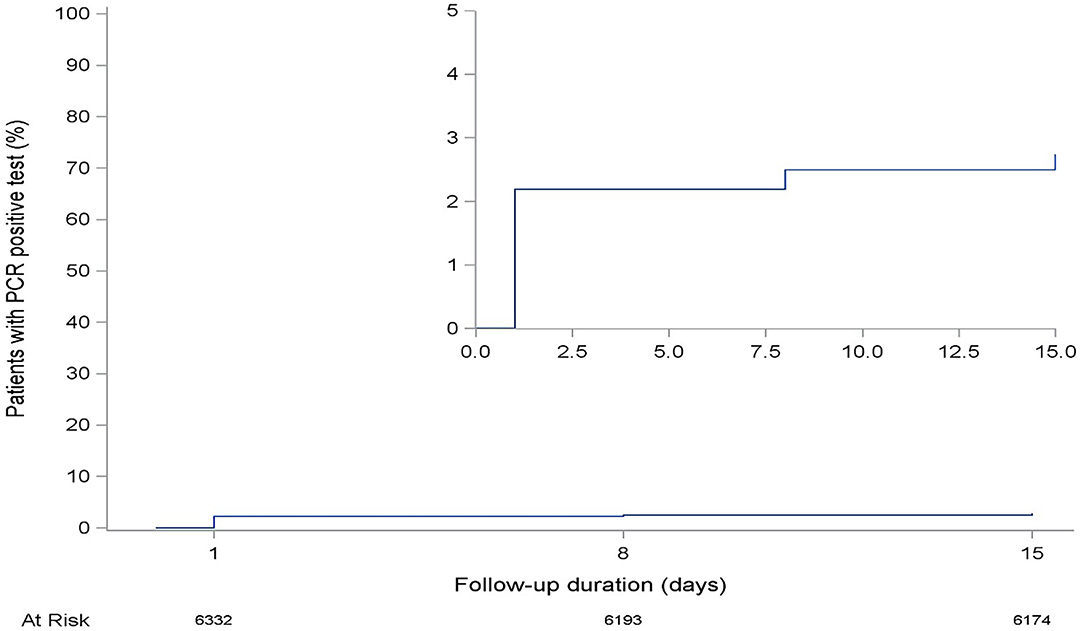
Figure 2. The cumulative incidence rate of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) test positivity among airport arrival passengers, April–August 2020, Burkina Faso.
Predictors of Imported Cases of COVID-19 in Burkina Faso
In the unadjusted analysis, gender, the period of arrival, the history of exposure to symptomatic patients two weeks before the travel, and the clinical condition of the passengers on arrival was associated with the SARS-CoV-2 RT-PCR test positivity in inbound passengers with p < 0.25 (Table 2).
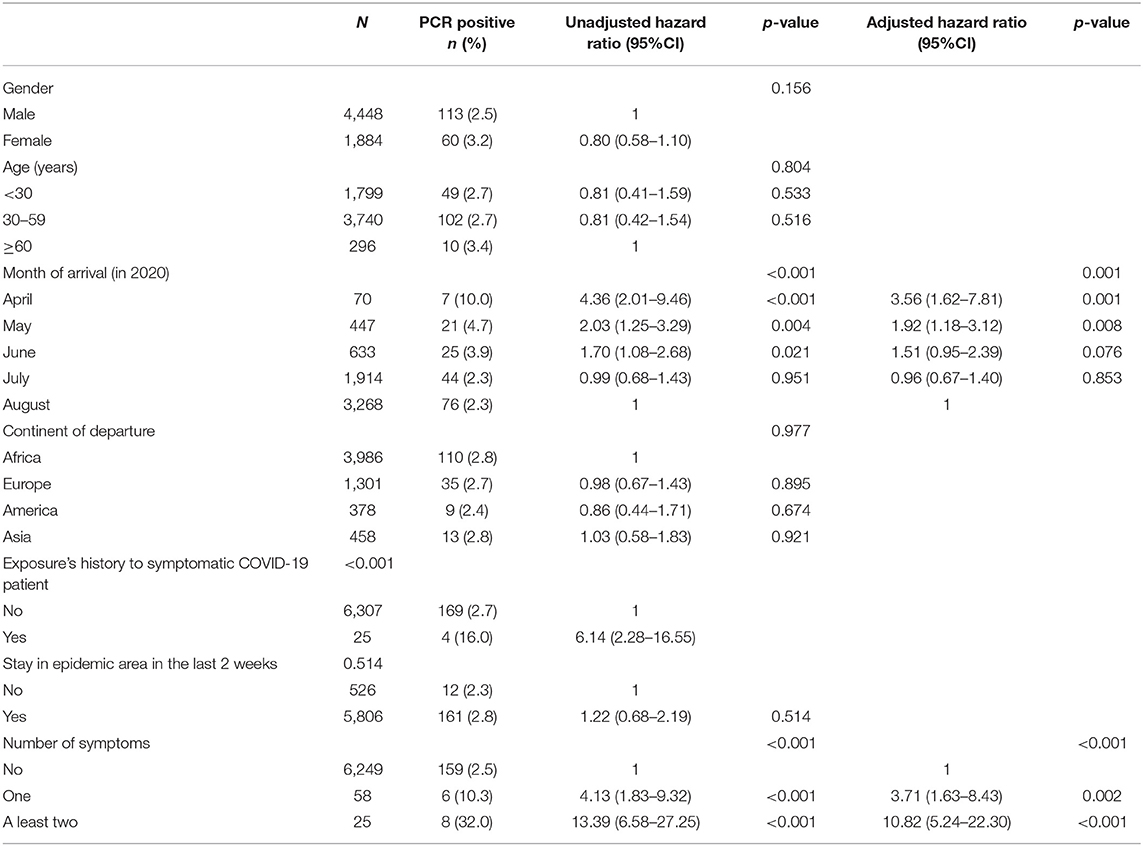
Table 2. Univariate and multivariate analysis of the risk of being PCR-positive.
In the multivariate analysis, the month of arrival (p < 0.001) and clinical conditions on arrival (p < 0.001) were significantly associated with SARS-CoV-2 infection. Thus, the risk of SARS-CoV-2 positivity was significantly greater among passengers who arrived in April (aHR = 3.56; 95% CI: 1.62–7.81) and May (aHR = 1.92; 95% CI: 1.18–3.12) compared to those who arrived in August.
Regarding the clinical conditions of the passengers, those who had presented one symptom and two symptoms or more during their quarantine were, respectively, 4 times (aHR = 3.71; 95% CI: 1.63–8.43) and 11 times (aHR = 10.82; 95% CI: 5.24–22.30) more likely to be positive to the SARS-CoV-2 RT-PCR compared to asymptomatic (Table 2).
Discussion
In this cohort study conducted from April 9 to August 31, 2020, the incidence of imported cases of COVID-19 was 1.9 cases per 1,000 passengers-day. Moreover, the strong predictors of imported cases were the period of travel and passengers' clinical condition on arrival and during the quarantine measure.
In this study, COVID-19 incidence was relatively low. This could be explained by the origin of our participants. Indeed, the majority of passengers (65.1%) arrived from African countries where the epidemic burden was less important than other continents at this period (8). Moreover, the lower incidence may be due to reduced international air travel (22). That was the case in our study where the air borders were closed until the end of July with a restriction of flights to Burkina Faso. In addition, we can assume that the implementation of systematic screening before the departure, plus screening on the day of travel in some airports could explain the low incidence of SARS-CoV-2 positive in travelers on arrival during our study period (19). However, despite this screening device on departure, we have notified positive cases on arrival, which leaves us perplexed and implies the need to systematically have a SARS-CoV-2 test on arrival for all passengers.
The proportion of imported cases was 17.9% of all the confirmed cases of COVID-19 from April 9 to August 31, 2020. In contrast to our study, a study analyzing the epidemiological and clinical aspects of imported cases of COVID-19 nationwide in Taiwan reported that 86.1% out of all 373 confirmed cases of COVID-19 from January 21 to April 6, 2020 were imported (15). This study took place <3 months after the onset of the pandemic, compared to our study which lasted 5 months. The probable lack of systematic screening for COVID-19 before departure could explain the high proportion of cases in their study. Moreover, the density of the air traffic for tourist or commercial reasons between Taiwan and other high epidemic burden countries like China at a beginning of the epidemic could explain this high frequency of imported cases in this study (23). Furthermore, our study began in April, therefore not taking into account the first imported cases recorded in the country before the border closure (24). In Spain, which was one of the European countries most affected by the COVID-19 epidemic, a mild proportion of imported cases were reported. It was estimated at around 0.08% based on the total number of confirmed cases of COVID-19 from May to December 2020. Considering this figure, the authors claim that the share of imported cases in the dynamics of disease's spread was relatively low so could not justify the strict and untargeted restrictions in countries with a high incidence of COVID-19 (25).
We identified two predictors of imported cases of COVID-19: the period of arrival and passengers' clinical condition on arrival. Indeed, those who arrived in April and May were, respectively, four and two times more likely to have a positive SARS-CoV-2 RT-PCR test, compared to those who arrived in August. Both these months were the period of epidemic peaks in many countries, including Burkina Faso (26) with more transmissions and a high number of confirmed cases. Despite the high flow of travelers from August due to the reopening of air borders, the risk of imported cases was low compared to other months. The measure of entrance restriction only cannot prevent the importation of COVID-19 cases in a country. Vigorous quarantine measures and screening of cases are essential to avoid the spread of the infection in the community.
Passengers who presented one symptom and those with two or more symptoms were, respectively, 4 times and 11 times more likely to test positive for COVID-19 compared to asymptomatic. In other words, the more symptomatic the passengers were on arrival, the greater the risk of COVID-19 test positivity. These results confirm the fact that the presence of symptoms known compatible with COVID-19 in any individual including passengers must require adequate measures to be taken to reduce the risk of transmission of the disease through systematic quarantine and surveillance, while doing the necessary to confirm the diagnosis. This highlights the issue of self-quarantine at home with the inability to monitor movements of the suspected cases, and probable community spread. Moreover, there is the problem of screening symptomatic passengers on departure and their flight ban to avoid future contamination. In the study carried out in Taiwan, only symptomatic travelers and passengers from epidemic countries were systematically screened with home quarantine. This strategy was related to several contaminations in the entourage of travelers (15). In our study, most of the passengers including the imported cases were asymptomatic (98.7%). If the COVID-19 test was applied only to symptomatic travelers, this measure would generate many cases of contamination in the community. Previous studies found that asymptomatic carriers are infectious and therefore can potentially transmit the disease and claim particular attention in their identification and monitoring (27, 28). The quarantine measures put in place may therefore have prevented the further spread of the epidemic in the community.
We noticed that the departure continent did not predict the COVID-19 test result among inbound travelers to Burkina Faso, although Asia and America were the continents that reported the highest prevalence of cases of COVID-19 at this period.
Our study has some limitations. First, we did not include passengers who have incorrectly completed the notification forms, those who were not compliant with the 2 weeks quarantine, and those who escaped from quarantine in this study. This selection bias might have underestimated the incidence of the COVID-19 imported cases. In fact, these passengers could be more at risk, which would explain their non-compliance with the quarantine measures. Except for fever, the other clinical signs were based on the passenger's statement. This could lead to an information bias if the passenger reports wrong information for fear of quarantine and stigmatization.
Notwithstanding these limitations, our study's strength resided firstly in the fact that it was performed at the national level and cover a period enough to appreciate the possible fluctuations due to the dynamics of the COVID-19 pandemic. Moreover, this is the first to report the incidence of imported cases in West Africa and to identify the factors associated with COVID-19 imported cases among international travelers during this pandemic period. These data are useful for the best preparedness the response to future challenges related to infectious disease outbreaks.
Conclusion
The COVID-19 pandemic poses a major threat to public health. In Burkina Faso, there has been a relatively low incidence rate of imported cases of COVID-19. The period of travel and the presence of symptoms at arrival predicted the risk of being tested positive for SARS-CoV-2 infection during the quarantine. It is therefore imperative to strengthen the surveillance and screening capacities at the entrance gates, regardless of the clinical symptom to break the chain of transmission related to imported cases. This is essential in a context of high circulation of virus variants worldwide and low local capacity to perform genotyping tests.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The protocol was approved by the Ethics Committee for Health Research in Burkina Faso (Deliberation No. 2020-9-211). The Ministry of Health has also given its approval for the use of data from the DHIS2 database. The confidentiality, as well as the anonymity of travelers, were respected during data processing.
Author Contributions
MK, KS, DD, SD, and SK developed the study concept. BO, HB, and BS managed the data with the software. BB and MO authorized the study performance. MK, KS, DD, and SK analyzed and interpreted the data. MK, KS, DD, and SD drafted the manuscript. YC, IK, AZ, IA, SD, ID, ED, PP, AP, YT, and SD contributed to the writing and revision of the manuscript. All authors approved the final version of the manuscript for submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the Ministry of Health through Centre des Opérations de Réponse aux Urgences Sanitaires (CORUS) and all the actors who contributed to this study. They are specifically: Simon Sanou, Drissa Lengane, Roselyne Sombie/Some, Wilfrid Landaogo S. Ouedraogo, and Claudine Lougué.
References
1. World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report: 28. (2020). Available at: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200217-sitrep-28-covid-19.pdf (accessed on November 1, 2020).
2. World Health Organization. Pneumonia of Unknown Cause—China. (2020). Available at: https://www.who.int/emergencies/emergency-events/item/2020-DON229 (accessed on November 1, 2020).
3. Han Y, Liu Y, Zhou L, Chen E, Liu P, Pan X, et al. Epidemiological assessment of imported coronavirus disease 2019 (COVID-19) cases in the most affected city outside of Hubei Province, Wenzhou, China. JAMA Netw Open. (2020) 3:e206785. doi: 10.1001/jamanetworkopen.2020.6785
4. European Centre for Disease Prevention Control. Outbreak of Acute Respiratory Syndrome Associated with a Novel Coronavirus, China: First Local Transmission in the EU/EEA—Third Update. Stockholm: ECDC. (2020). Available at: http://www.ecdc.europa.eu › documents (accessed on November 1, 2020).
5. Helmy YA Fawzy M Elaswad A Sobieh A Kenney SP and Shehata AA. The COVID-19 pandemic: a comprehensive review of taxonomy, genetics, epidemiology, diagnosis, treatment, and control. J Clin Med. (2020) 9:1225. doi: 10.3390/jcm9041225
6. World Health Organization. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19−11 March 2020. (2020). Available at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020 (accessed on November 1, 2020).
7. World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Data last updated: 2020/10/30, 4:28pm CET. Available at: https://covid19.who.int/ (accessed on October 31, 2020). doi: 10.46945/bpj.10.1.03.01
8. Bonnet E, Bodson O, Le Marcis F, Faye A, Sambieni NE, Fournet F, et al. The COVID-19 pandemic in francophone West Africa: from the first cases to responses in seven countries. BMC Public Health. (2021) 21. doi: 10.1186/s12889-021-11529-7
9. Mbow M, Lell B, Jochems SP, Cisse B, Mboup S, Dewals BG, et al. COVID-19 in Africa: dampening the storm? Science. (2020) 369:624–6. doi: 10.1126/science.abd3902
10. Hossain MP, Junus A, Zhu X, Jia P, Wen T-H, Pfeiffer D, et al. The effects of border control and quarantine measures on the spread of COVID-19. Epidemics. (2020) 32:100397. doi: 10.1016/j.epidem.2020.100397
11. Zhang L, Yang H, Wang K, Zhan Y, Bian L. Measuring imported case risk of COVID-19 from inbound international flights—A case study on China. J Air Transp Manag. (2020) 89:101918. doi: 10.1016/j.jairtraman.2020.101918
12. World Health Organization. Coronavirus disease (COVID-19) Weekly Epidemiological and Operational Update March 2020. (2020). Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on May 10, 2021).
13. Service d'Information du Gouvernement du Burkina Faso. Message à la nation de son Excellence Monsieur Roch Marc Christian Kaboré président du Faso, président du conseil des ministres sur l'épidémie du COVID 19. (2020). Available at: https://www.sig.gov.bf/actualites/details?tx_news (accessed on June 7, 2020).
14. USAID. IMMAP. COVID-19: Analyse de situation. Rapport annuel. Mars 2020-Juillet 2021. (2021). Burkina Faso. 74 p.
15. Liu J-Y, Chen T-J, Hwang S-J. Analysis of Imported Cases of COVID-19 in Taiwan: a Nationwide Study. Int J Environ Res Public Health. (2020) 17:3311. doi: 10.3390/ijerph17093311
16. Zhang J, Yang S, Xu Y, Qin X, Liu J, Guo J, et al. Epidemiological and clinical characteristics of imported cases of COVID-19: a multicenter study. BMC Infect Dis. (2021) 21:406. doi: 10.1186/s12879-021-06096-6
17. Lin C-Y, Wang W-H, Urbina AN, Tseng S-P, Lu P-L, Chen Y-H, et al. Importation of SARS-CoV-2 infection leads to major COVID-19 epidemic in Taiwan. Int J Infect Dis. (2020) 97:240–4. doi: 10.1016/j.ijid.2020.06.031
18. Menkir TF, Chin T, Hay JA, Surface ED, De Salazar PM, Buckee CO, et al. Estimating internationally imported cases during the early COVID-19 pandemic. Nat Commun. (2021) 12:311. doi: 10.1038/s41467-020-20219-8
19. Mouchtouri VA, Bogogiannidou Z, Dirksen-Fischer M, Tsiodras S, Hadjichristodoulou C. Detection of imported COVID-19 cases worldwide: early assessment of airport entry screening, 24 January until 17 February 2020. Trop Med Health. (2020) 48:79. doi: 10.1186/s41182-020-00260-5
20. INSD ICF International. Enquête Démographique et de Santé et à Indicateurs Multiples (EDSBF-MICSIV) 2010. (2012) Burkina Faso, Calverton, Maryland, USA.
21. World Health Organization. Considerations for Quarantine of Individuals in the Context of Containment for Coronavirus Disease (COVID-19): Interim Guidance. (2020). (accessed on June 18, 2021).
22. Skrip LA, Selvaraj P, Hagedorn B, Ouédraogo AL, Noori N, Orcutt A, et al. Seeding COVID-19 across Sub-Saharan Africa: an analysis of reported importation events across 49 Countries. Am J Trop Med Hyg. (2021) 104:1694–702. doi: 10.4269/ajtmh.20-1502
23. Haider N, Yavlinsky A, Simons D, Osman AY, Ntoumi F, Zumla A, et al. Passengers' destinations from China: low risk of Novel Coronavirus (2019-nCoV) transmission into Africa and South America. Epidemiol Infect. (2020) 148:e41. doi: 10.1017/S0950268820000424
24. Ross A. Burkina Faso Confirms First Cases of Coronavirus. US News. (2020). Available online at: htttps://www.usnews.com/news/world/articles/2020-03-09/burkina-faso-confirms-first-cases-of-coronavirus (accessed on June 4, 2020).
25. de Miguel Buckley R, Díaz-Menéndez M. Go to gate: COVID-19 imported cases in Madrid and the potential role of airport transmissions. Trans R Soc Trop Med Hyg. (2021) 115:731–2. doi: 10.1093/trstmh/traa198
26. Sun H, Dickens BL, Cook AR, Clapham HE. Importations of COVID-19 into African countries and risk of onward spread. BMC Infect Dis. (2020) 20:598. doi: 10.1186/s12879-020-05323-w
27. Zhang J, Wu S, Xu L. Asymptomatic carriers of COVID-19 as a concern for disease prevention and control: more testing, more follow-up. Biosci Trends. (2020) 14:206–8. doi: 10.5582/bst.2020.03069
Keywords: COVID-19, imported cases, incidence, predictors, Burkina Faso
Citation: Kaboré M, Sondo KA, Dahourou DL, Cissoko Y, Konaté I, Zaré A, Bicaba B, Ouedraogo B, Barro H, Diendéré EA, Asamoah I, Damoue SN, Siri BAA, Diallo I, Puplampu P, Poda AG, Toloba Y, Dao S, Ouédraogo M and Kouanda S (2022) Incidence and Predictors of Imported Cases of COVID-19 in Burkina Faso. Front. Public Health 10:743248. doi: 10.3389/fpubh.2022.743248
Received: 17 July 2021; Accepted: 17 January 2022;
Published: 17 February 2022.
Edited by:
Hai-Feng Pan, Anhui Medical University, ChinaReviewed by:
Neftali Eduardo Antonio-Villa, Universidad Nacional Autónoma de México, MexicoXiaobo Liu, National Institute for Communicable Disease Control and Prevention (China CDC), China
Copyright © 2022 Kaboré, Sondo, Dahourou, Cissoko, Konaté, Zaré, Bicaba, Ouedraogo, Barro, Diendéré, Asamoah, Damoue, Siri, Diallo, Puplampu, Poda, Toloba, Dao, Ouédraogo and Kouanda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mikaila Kaboré, bWlrYWlsYWthYkBnbWFpbC5jb20=