 Yumeng Gao1*
Yumeng Gao1* Liang Du
Liang Du- 1Department of Medical Insurance, Jinshan Hospital of Fudan University, Shanghai, China
- 2School of Public Health, Fudan University, Shanghai, China
Introduction: Prevalence of functional limitations (FLs) and disabled activities of daily living (ADL) cause heavy burdens to the health of the older people. Stratified by gender, this study aimed to explore the effects of FL and ADL on the mortality of the older people in China, and the mechanism was then discussed.
Methods: We used survey data of a prospective 10-year cohort (2008–2018), from the China Longitudinal Healthy Longevity Survey (CLHLS). The primary outcome was all-cause mortality, and Independent variables included FL, basic ADL (BADL), and instrumental ADL (IADL). Covariates involved socio-demographic characteristics, health-related behaviors, and health status of the participants in the CLHLS project.
Results: There were 967 (19.20%) male and 2,235 (32.36%) female older people performed functional limitations, and their survival time was 60.98 (SE = 0.66) and 55.19 (SE = 0.55) months, respectively. Old adults with FL had significantly poorer survival than the ones without (Log-rank test, P < 0.001). Weibull regression suggested that FL (P < 0.001), abnormal BADL (P < 0.001) and IADL (P < 0.001) were negatively associated with the survival of the older people. Further analysis showed that BADL and IADL performed significantly mediating roles in the relation of FL and survival time in old adults; additionally, for female older people, BADL also exhibited a significant moderating role in the effect of FL on survival.
Conclusions: Prevalence of FL was serious among the older people in China, especially for the women. Disabilities of BADL and IADL and FL were negatively associated with the survival time of the older people in China. Regarding the effect of FL on survival, BADL and IADL performed significantly mediating roles, and the moderating role of BADL existed only for the female. These suggested evidence to implement strategies to maintain health in the older people.
1. Introduction
The trend of population aging has become one of the severe challenges in most countries, including China which has the largest older people population globally and is increasing rapidly (1). In China, the population over 60 years old accounted for 17.9% of the total population (1.4 billion), and the population over 65 years old accounted for 10.9%. With the population of older people growth, lots of public health problems are becoming increasingly prominent, such as supporting and care them, diseases prevention and treatment. Physically functional limitations (FLs), which commonly bring a high burden on the health-related quality of life among the older people, can be recognized as a matter of great concern in China.
FL means the ability to move or the physical movement of any body part being limited for some reasons, which is commonly measured by extremity functional limitation in practice (2–4). The older people with FL are often linked to higher utilization of healthcare, lower levels of social cohesion, and poor mental health status (4, 5). Suffering from FL, the older people are more likely to depend on caregivers to satisfy their life needs, which require assistance or adaptive equipment, in general, to improve mobility. Besides, serious FL of the older people can lead to various physical illnesses. Associations between chronic diseases and FL in the older people have been found for arthritis, diabetes, hypertension, coronary heart disease, cardiovascular disease, depression, stroke, and visual impairment (6). Additionally, these non-communicable diseases could then harm the quality of life of the older people. Therefore, we hypothesize that:
H1: FL is directly associated with the death of the older people.
Generally, ADL is composed of basic activities of daily living (BADL) and instrumental activities of daily living (IADL). BADL refers to the physically self-care ability (e.g., dressing), while IADL means the higher-level skills that the older people need to live independently in their communities (e.g., shopping). Previous studies have proven that ADL impairments are associated with increased mortality risk in old adults (7, 8). However, it still lacks concrete evidence whether disabled ADL associates with the death of the older people in China. Disabilities of ADL, which is highly prevalent in China, can cause many adverse consequences, such as poor physical or mental health, and an increased risk of accident injuries (9, 10). Besides, ADL disabilities reflect the fact that the older people have lost some of their self-care abilities, and to some extent, they also isolate the social interaction, which may augment the risk of mortality in an older population. Therefore, we hypothesize that:
H2: disabled ADL is directly associated with the death of the older people.
Previous studies reported that disability of ADL was triggered by a reduction in muscle strength in the lower limbs, with consequent difficulties in bathing, walking, toileting, and transferring, followed later by disability regarding dressing and eating (11, 12). However, to date, few researches have focused on the relation between ADL and FL of the older people in China. Because of FL, the older people may lose the ability to take care of themselves, like dressing, eating, and bathing; additionally, the instrumental activities of the older people can also be impeded, such as shopping, washing clothes, and taking public transportation. Hence, we speculate that FL is associated with ADL of the older people. Social participation of the older people is thought to be a vital issue in their active aging. Mobility of the older people with FL could be restricted, which may reduce their engagement in self-care and social activities, and then cause extensive damage to cognitive function and health beliefs with age; and ability of IADL and BADL continually weaken for the negatively cumulative effects from FL, which may result in an increased risk of death in old adults (13–15). Given these, we further hypothesized that:
H3a: BADL mediates the relation between FL and death of the older people.
H3b: IADL mediates the relation between FL and death of the older people.
Performance of ADL is an essential indicator of the health status of older adults. Influenced by traditional Chinese concepts and cultural consciousness, combined with underdeveloped healthcare system, home-based care has become the preferred way for older adults, so most of the older people with ADL disability have no access to professional care (16). The older people with BADL disability are often unable to undertake self-care in daily life, and if they have inadequate external care and support, there will be great possibilities that the negative events leading to death due to limited physical functions (16–18). Likewise, the old adults suffering from IADL are also restricted from engaging in social interaction and require indispensable assistance to maintain health, which could result in senior citizens with FL at high-risk mortality (19, 20). Based on the reasoning above, we hypothesize that:
H4a: BADL moderates the relation between FL and death of the older people.
H4b: IADL moderates the relation between FL and death of the older people.
By literature review, it's noted that there are gender differences in both ADL disabilities (21, 22) and mortality (23) among older adults, and it is necessary to examine the hypotheses in male and female old adults, separately. Based on 10-years longitudinal data, stratified by gender, the purpose of this study was to examine the effects of FL and ADL on mortality in Chinese old adults. Furthermore, we explored the mediating and moderating effects of ADL on the relation between FL and mortality (Figure 1), which would provide a theoretical basis for promoting healthy aging in China in the future.
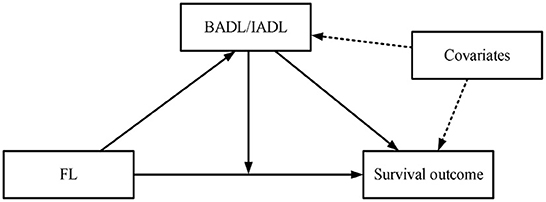
Figure 1. Potential study hypothesis based on literature review.
2. Methods
2.1. Study design and participants
The data used in this study came from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), which is conducting by the Center for Healthy Aging and Development Studies, Peking University. The CLHLS is a nationwide survey that selects randomly half of the cities and counties in 23 provinces of China since 1998. This area had a total population of 1,156 million in 2010, accounting for approximately 85% of the Chinese population. The CLHLS collected information on the health status and quality of life of the participants who were aged 65 years and older.
The CLHLS datasets from the sixth wave (2008/2009, at baseline) to the ninth wave (2017/2018) were used in this study. Some countries consider that the older people should be aged 60 and above, while others consider it to be aged 65 and above. In order to better generalize the study conclusions to a wider population, this study was conducted for people aged 65 years and older. There were 16,954 participants at baseline, and we excluded 391 participants aged <65 years and 4,455 observations due to loss to follow-up, which led to 12,108 eligible participants in this study.
2.2. Variables and measurements
2.2.1. Outcome definition
The primary outcome of this study was all-cause mortality. Mortality information was obtained from the follow-up survey done in 2011, 2014, and 2018. The date of death would be validated by death certificates when available–otherwise, the close family member's report was recorded. We then calculated the survival duration by months, from the investigation date to the participant's death.
2.2.2. Independent variables
Functional limitations were measured by five objective movements' examinations, including hand behind neck, hand behind the lower back, raising arms upright, standing up from sitting in a chair, and pick up a book from the floor. These items have been proven to measure functional limitations validly in previous studies (24, 25). We scored each term as 0 if the participant could complete it without help, otherwise scored 1. The participant was identified as absent function-limitation if one can complete all the items without any help. IADL status was measured by a valid scale made by Lawton and Brody (26), which was consisted of eight items: visiting neighbors, shopping, cooking, washing clothes, walking one kilometer, carrying a five-kilogram object, crouching and standing three times, and taking public transportation. The response for each question was “yes”, “a little difficult” or “unable to do so”. We categorized respondents as IADL disabled (coded as 1) if they had any difficulty in performing these items (otherwise coded as 0). The basic activities of daily living (BADL) were measured using the Katz Index by six items: bathing, dressing, toileting, indoor transferring, eating, and continence (27). Disability in BADL was defined if the participants could not independently complete any above item. Response categories for BADL were consistent with IADLs and coded similarly.
2.2.3. Covariates
This study covered three sets of potential confounders, including socio-demographic characteristics, health behaviors, and health status. The socio-demographic characteristics involved gender (male/female), age, education (schooling years), marriage status (married/unmarried/widowed), and household income (<10,000/10,000–30,000/30,001–60,000/>60,000 yuan per year). The health behaviors included smoking (yes/no), drinking (yes/no), and frequent physical exercise (yes/no). The health status was composed of body mass index (BMI), times of serious illness in the past 2 years, and the number of chronic diseases. BMI was calculated by [weight (in kilograms)/height (in meters) 2]. Several chronic diseases were measured by asking the question “Do you suffer from the following diseases?” The respondents could choose from 22 options, such as hypertension, diabetes, and stroke.
2.3. Statistical analysis
All analyses were stratified by gender, including subgroups of male, female, and total participants. Mean ± standard deviation (SD) was employed to describe the variables of normal distribution. Frequency and percentage (%) were applied to describe the categorical variables.
According to whether the older people had functional limitations or not, we calculated the means and its 95% confidence intervals (CIs) of survival time. Additionally, Kaplan-Meier survival analyses were used to depict the survival over time, and its 95% CI was estimated in the graph. Log-rank test was used to examine the equality of survival time in old adults with/without functional limitations. Then, adjusting three-sets covariates (socio-demographic characteristics, health behaviors, and health status), we employed Weibull regression to explore the risk factors of mortality in old adults, and regression coefficients and its standard error (SE) were reported. Furthermore, we tested the statistical assumption of the Weibull regression, and it was supported.
Finally, we explored the mediating and moderating effects of ADL (i.e., BADL & IADL) in the relation between functional limitations and mortality, stratifying by gender. Adjusting the covariates, we used the developed med4way command, in Stata software (Stata Corp LP, College Station, TX, USA), to calculate the mediating and moderating effects in this study. Med4way can be used when the outcome is continuous, dichotomous, count or survival time, and the mediator is continuous or binary. In this study, the outcome variables were survival data that did not satisfy the PH hypothesis after statistical testing (excluding Cox regression), and the probability of death increased rapidly over time (non-linear), so we employed the Weibull regression of accelerated failure-time form to explored the determinants of survival time of the older people. Additionally, due to binary BADL/IADL, Logistic regression was used for the mediator. Furthermore, med4way can decompose the overall effect of an exposure on an outcome into four components: (i) neither mediation nor interaction; (ii) just interaction (but not mediation); (iii) both mediation and interaction; and (iv) just mediation (but not interaction). Considering this study purpose, we only reported the mediation and interaction effects in the results. A detailed introduction of Med4way can be found elsewhere (28).
All the data analysis was done in the Stata 14.0 MP version (Stata Corp LP, College Station, TX, USA). All tests were two-sided, and P < 0.05 was considered statistical significance.
3. Results
3.1. Characteristics of the older people at baseline
We included 12,108 old adults at baseline. There were 7,009 (57.89%) female and 5,099 (42.11%) male older people. The average age of women (90.39 ± 11.18) was higher than that of men (85.07 ± 10.34). The total illiteracy rate was 65.63%, of which the female accounted for 74.96%. The divorced or widowed rate (71.84%) was high, and the rate of women (68.11%) was about twice as high as that of men (31.89%). About a half with an annual income of <10,000 yuan, while only 2,142 (17.69%) reported more than 30,000 yuan per year. Both smoking and alcohol consumption rates appeared higher among the male. Most of the older people (75.28%) lacked physical activities, and the female had a proportion of 62.21%. Mean BMI was 20.11 (SD = 3.56) in old adults, and most of the older people (82.72%) experienced no serious illness in the past 2 years, yet 2,092 (17.28%) did. Only 5,376 (44.40%) had no chronic diseases, but 2,917 (24.09%) had more than one chronic diseases; obviously, the female showed a higher rate of chronic diseases than the male ones (Table 1).
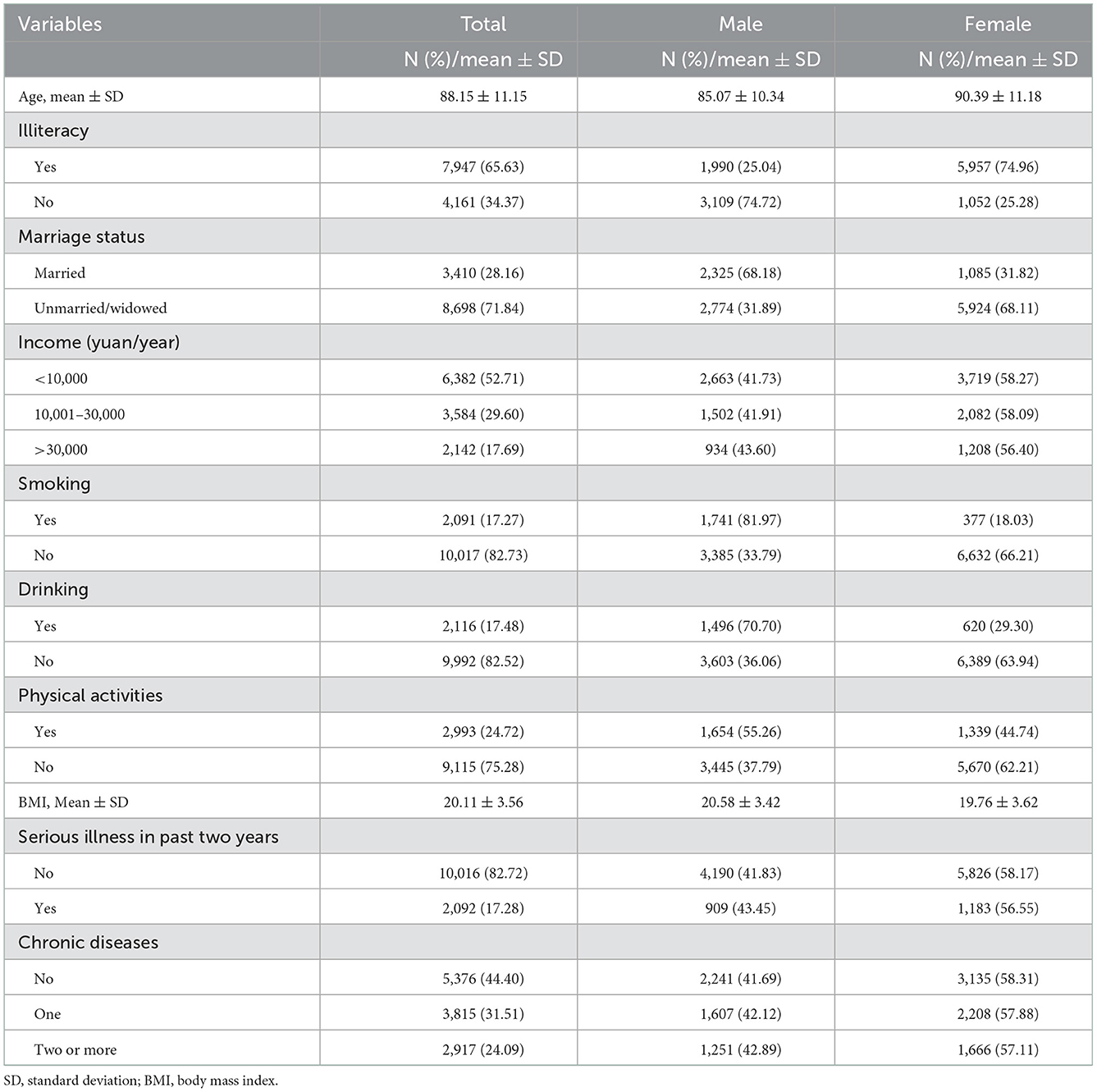
Table 1. Characteristics of the older people of a different gender at baseline.
3.2. Survival time of the older people in different gender
We calculated the survival time of the older people, and its difference was compared in the male and female, respectively. Survival time of the male and female older people were 60.98 (SE = 0.66) and 55.19 (SE = 0.55) months, respectively. In the male, there were 967 (19.20%) showed functional limitations, and their mean survival time was only 37.36 (SE = 1.17) months; while the older people without functional limitations showed a higher mean survival of 66.51 months (SE = 0.74). In the female, there were 2,235 (32.36%) showed functional limitations, and their mean survival time was only 36.35 (SE = 0.75) months; while the older people without functional limitations showed a higher mean survival of 64.20 months (SE = 0.69). Overall, there were 3,202 (26.81%) showed functional limitations, and their mean survival time was only 36.76 (SE = 0.63) months; while the older people without functional limitations showed a higher mean survival of 65.28 months (SE = 0.50) (Table 2).
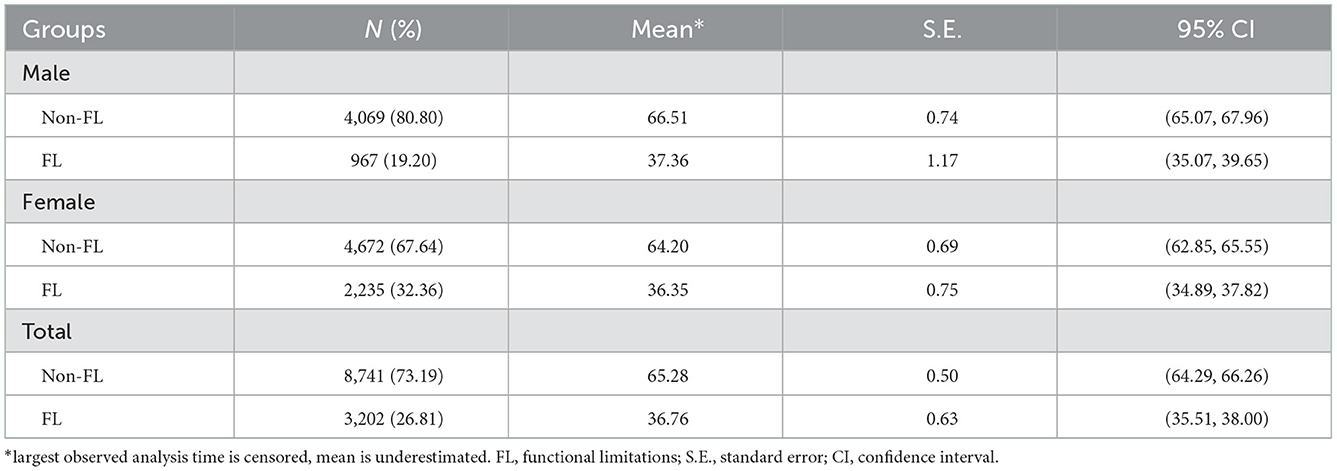
Table 2. Survival months of the older people in different gender.
3.3. Kaplan-Meier survival estimates of the older people
Kaplan-Meier survival analysis was used to estimate the difference of mortality in the older people with different functional status. Overall, it indicated that old adults with functional limitations had poorer survival than the ones without, and this difference was statistically significant (Log-rank test, Chi-square = 1,133.05, P < 0.001). Additionally, it showed that, over time, old adults with functional limitations had significantly poorer survival than the ones without, for either the male (Log-rank test, Chi-square = 389.64, P < 0.001) or female (Log-rank test, Chi-square = 690.41, P < 0.001) older people in China (Figure 2).
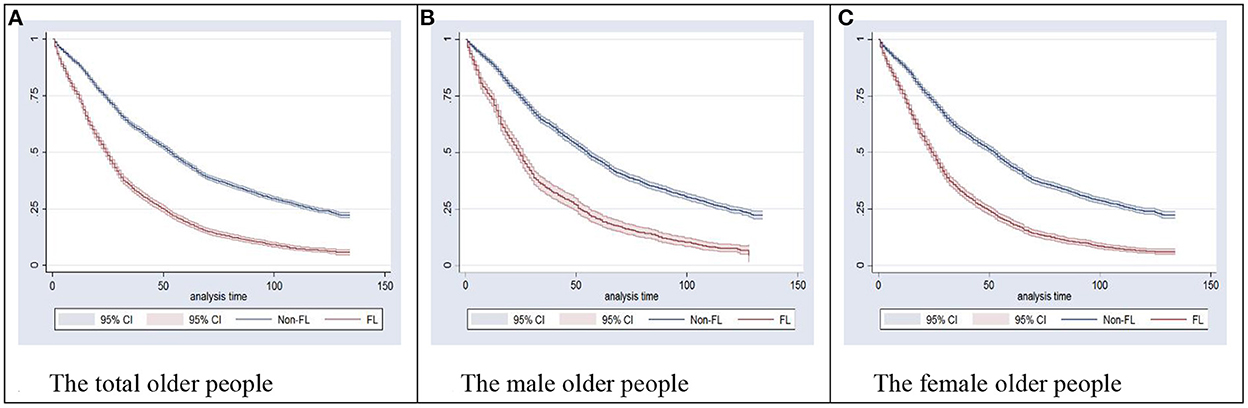
Figure 2. Kaplan-Meier survival estimates of the older people in different gender. (A) The total older people. (B) The male older people. (C) The female older people. Log-rank test was used to examine the equality of survivor functions among the total, male, and female older people, which indicated a significant difference between the FL and non-FL groups (P < 0.001). FL, functional limitations; CI, confidence interval.
3.4. Weibull regression for determinants of survival time
Weibull regression was used to explored the determinants of survival time in the older people. It suggested that functional limitations were negatively associated with the survival time of the older people (coefficient= −0.11, P < 0.001), and the male older people (coefficient = −0.16, P < 0.001) showed a higher risk of mortality than the female ones (coefficient = −0.11, P < 0.001). IADL disabilities also exhibited a significantly negative association with the survival time in old adults (coefficient = −0.25, P < 0.001). BADL disabilities negatively associated with the survival of the older people (coefficient = −0.27, P < 0.001), and the male (coefficient = −0.23, P < 0.001) showed a lower risk of mortality than the female (coefficient = −0.29, P < 0.001).
Besides, the risk of mortality in old adults (coefficient = −0.05, P < 0.001) increased with age. Comparing to the married older people, the unmarried/widowed showed a higher risk of mortality (coefficient = −0.11, P < 0.001), and the male (coefficient = −0.13, P < 0.001) showed a lower risk of mortality than the female ones (coefficient = −0.24, P < 0.001). No physical activities engagement exhibited a significant risk of mortality (coefficient = −0.10, P < 0.001). BMI exhibited positive effects on survival time (coefficient = 0.01, P < 0.01) (Table 3).
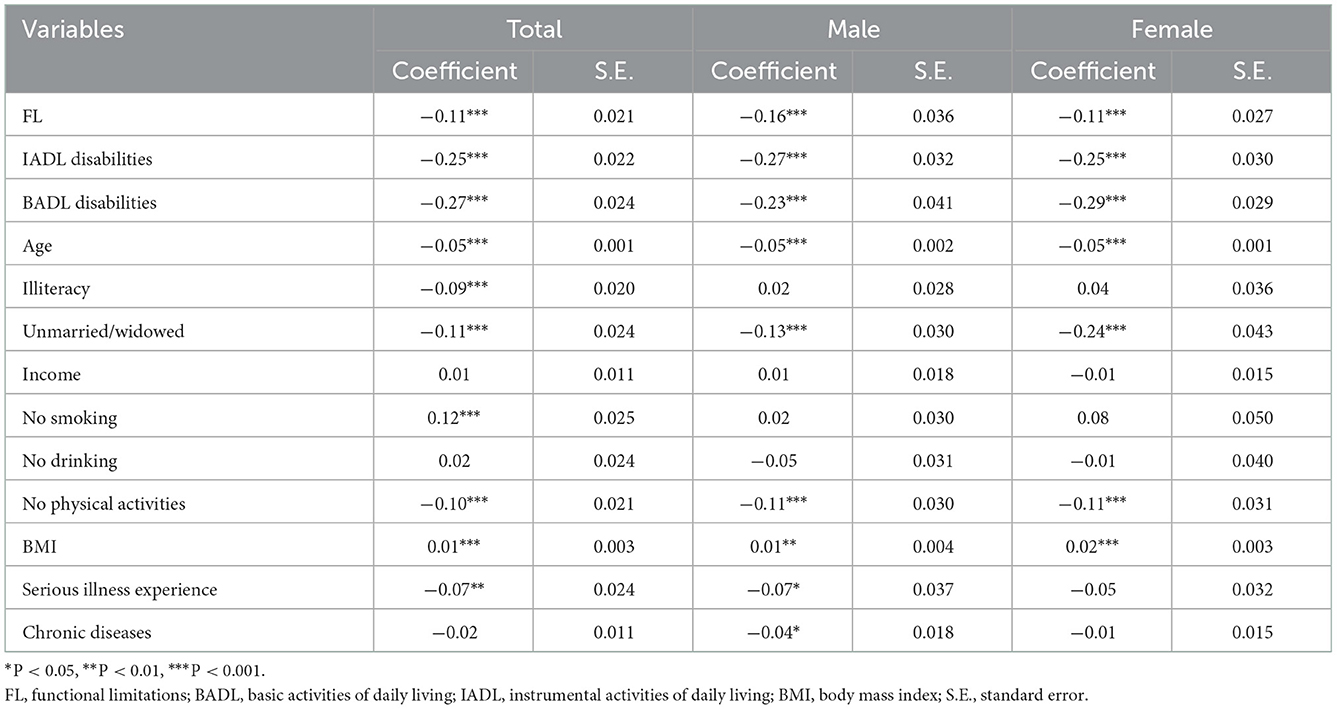
Table 3. Weibull regression for determinants of survival time of the older people.
3.5. Mediation and moderation role of ADL on survival
Finally, we explored the mediating and moderating role of IADL and BADL in the effect of functional limitations on survival time in the older people. For the male, the disabilities of BADL [coefficient = −0.06, 95% CI (−0.08, −0.04)] and IADL [coefficient = −0.08, 95% CI (−0.10, −0.06)] performed significantly mediating roles in the relation of functional limitations and survival time in old adults. For the female, the disabilities of BADL [coefficient = −0.11, 95% CI (−0.12, −0.09)] and IADL [coefficient= −0.08, 95% CI (−0.09, −0.06)] performed significantly mediating roles in the relation of functional limitations and survival in old adults; additionally, BADL [coefficient = −0.11, 95% CI (−0.18, −0.04)] exhibited a significantly moderating role in the effect of functional limitations on survival time. Overall, the disabilities of BADL [coefficient = −0.08, 95% CI (−0.10, −0.07)] and IADL [coefficient = −0.08, 95% CI (−0.10, −0.07)] performed significantly mediating roles in the relation of functional limitations and survival time in old adults; additionally, BADL [coefficient = −0.10, 95% CI (−0.14, −0.02)] exhibited a significantly moderating role in the effects of functional limitations on survival time (Table 4).
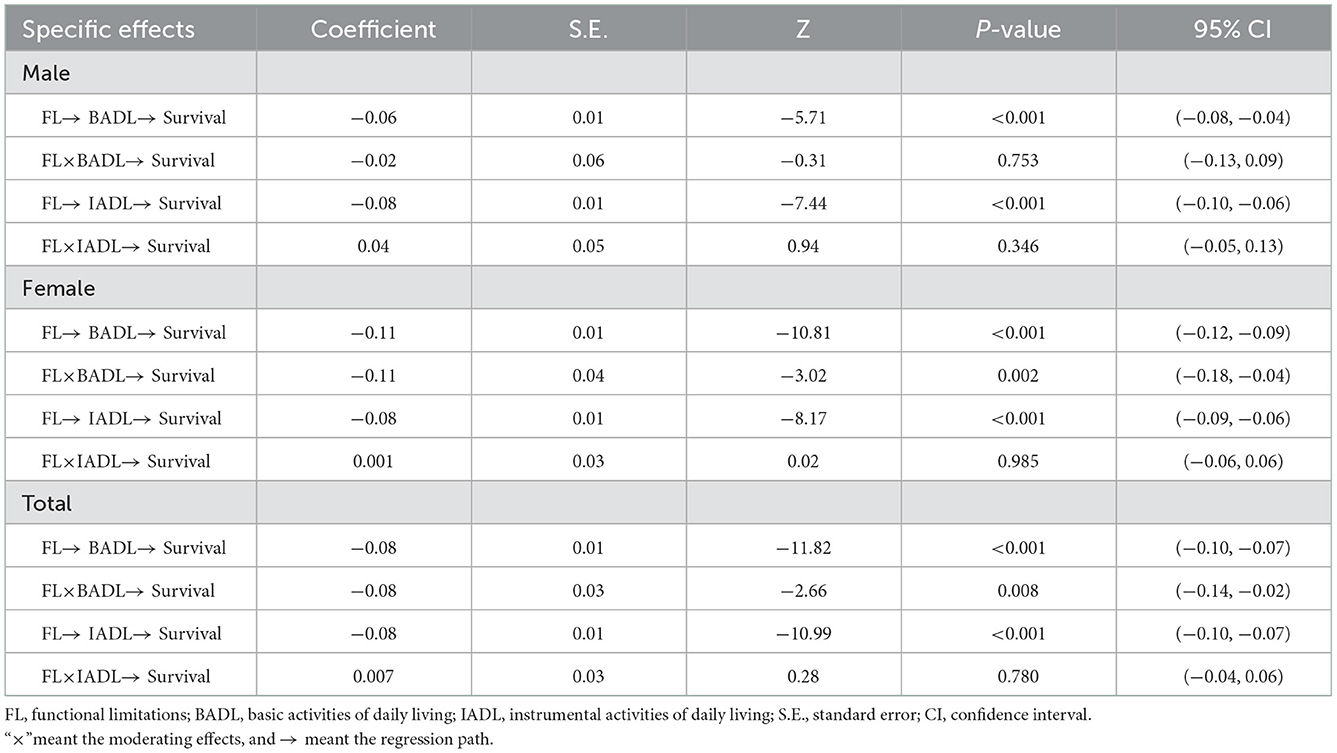
Table 4. Mediation and moderation role of ADL on survival of the older people.
4. Discussion
Exploring the prevalence and determinants of survival status among the older people is the basis of public health policy formulation and implementation, such as allocation of resources and health service planning, and are important for the healthy aging process. To our knowledge, no study to date has examined the effects of FL and ADL on the mortality of the older people in China. Using a nationwide 10-year cohort, by gender stratification, this study has explored the potential mechanism regarding the effects of FL and ADL on survival in the older people, which provided evidence to implement strategies to maintain their health.
This study found that the prevalence of FL was serious among the older people in China, and about a quarter (26.81%) suffered from FL at baseline. FL is a common kind of physical frailty when people get older, while it always influences the physiological wellbeing, mental health, and social interaction of the older people (29, 30). Higher prevalence of functional limitations could be associated with the absence of physical activities in the older people, and this study showed that about three quarters of them lacking physical activities in daily life. Previous studies have proven that physical activities could improve cardiorespiratory fitness, muscular strength, body composition, balance, flexibility, and muscular endurance in the older people (31). Hence in the future, more access to physical exercise should be provided to the older people to strengthen their functional health. Additionally, this study showed that the prevalence of FL was higher in the female older people than the male, which was in line with previous studies (32, 33). This finding, in practice, can be interpreted for many reasons: including under-education, unfavorable biological characteristics, higher propensity to admit illness, and different social roles and relationships, which could make women more vulnerable to poor health (34). Furthermore, the results indicated that the older people without FL had about extra 29 survival months longer than those with FL. Analyzing the ten-year survival rate, we found the older people with FL was <10% but non-FL older people was more than 20%. However, at present, the problems of FL in old adults have not yet received much attention from the public. Therefore, effective interventions should be put forward and implemented to the prevalence of FL in China, which ensures healthy late life of the aged population.
This study showed that FL was negatively associated with the survival time of the older people, and the survival of the female was more damaged than the male. The older people with FL often perform various problems of physician-rated health, and this could increase their risks of mortality (35). Additionally, FL could arise mental distress, such as anxiety, depression, and even suicidal thought, especially to the female, which multiply a negative impact on the survival of the older people (36). Also, ADL disabilities exhibited a significantly negative association with survival in old adults. IADLs are essential to living independently in a community, and IADL performance is thought to reflect underlying cognitive and physical function (37). So if an aged person is diagnosed with disabled IADL, then he/she could have a higher risk to die younger than the coeval. BADLs are the most important factors in characterizing the health status of frail old adults, and it is ordinarily evaluated to determine the levels of care that people should receive, which costs a lot in China (38). Low ADL level, causing greater negative impacts on women, has been proven to be associated with various chronic diseases, abnormal physiological indicators, and nutritional incidence in old adults, which can rise the possibility of mortality (21, 39). A population-based health survey in Norway found that physical inactivity could be the most important lifestyle risk factors for ADL/IADL disability (40). To compress the prevalence and harm of ADL disabilities of the older people in China advances in medications, healthy lifestyle, and socioeconomics should be achieved in the future (41).
This study found that the unmarried/widowed, comparing to the married older people, showed a higher risk of mortality, and the male showed a lower risk of mortality than the female ones. Family support networks, especially spousal support, and living arrangements are likely to be the most common determinants for the health of the older people in the current Chinese context (42). The married older people, especially the women, could have better health status than the unmarried ones because the spouses of the older people are the ones who spend the most lifetime with them, who have the most intimate relationship, and the loss of the spouse can spontaneously stimulate the mortality risk of the older people (43, 44). Besides, the results suggested that no physical activities engagement exhibited a significant risk of mortality in senior citizens. However, in daily life, a previous study indicated that over 50% of the older people do not meet recommended levels of regular physical activity (45), so we should take effective measures to improve the activities among old adults. Interestingly, our study also found that BMI exhibited a positive association with survival time. Higher BMI always implies a better living standard for the older people, so they are characterized by high survival duration.
Exploring the mediating and moderating role of ADL on the relation between FL and survival of the older people, we found that the disabilities of BADL negatively mediated the relation between FL and survival in old adults. This suggests that FL could increase the likelihood of incidence of BADL disability, and then to some extent, it increases the death of the older people. Therefore, improving the prevalence of FL in the older people cannot fundamentally prompt the survival increase, and further attention should be given to the impact of BADL on the survival of the older people in the future, to achieve better healthy aging in China (41). Additionally, we found that the disabilities of IADL negatively mediated the relation between FL and survival in old adults. The older people with FL were limited on physical activities, increasing the risk of disabled IADL, which greatly reduced the health status of the older people. IADL is an important indicator that affects health, but its impact on the health or death of the older people is often overlooked in China (9, 46). Hence, monitoring the IADL and FL condition of the older people to reduce the occurrence of adverse events is an important recommendation to improve their quality of life.
As the results showed, BADL disabilities negatively moderated the effect of FL on the survival of the older people. Impairment in the performance of BADL, especially in household settings, is considered far more complex than cellular or molecular mechanisms of aging due to the complex body and environmental systems involved (47). BADL disabilities often indicate a loss in muscle strength, which can jeopardize the health and even lead to mortality of the older people. Experiencing extreme difficulty in BADL and healthcare demand are not only related to decreased quality of life but also increased likelihood of long-term nursing home placement; and in this context, the older people with FL, generally accompanied by poor ability of balance mobility, could be suffering from higher risk of mortality (48). Stratified by gender, however, the results showed, for the male, BADL disabilities indicated no moderating effect on the relation between FL and survival. This may be since disability regarding ADL is more prevalent among the female, and BADL doesn't have that much impact on the lives of the male (21). Besides, the men older people perform lower frailty and better resilience than the women, which could interpret the no existence of moderating role of BADL in the male (21, 33, 49). Therefore, screening and improving the ADL, especially for the women, should arise wide public concern to develop the old-age policy in the future.
However, some limitations should be mentioned in this study. Firstly, FL and ADL (BADL/IADL), like many previous studies, were collected through self-report, which might lead to fuzzification of exposure. Secondly, more than a quarter of the cohort has been lost to follow-up, and most of the lost to follow-up were due to city construction and moving of living places. This may generate bias in our study results. Thirdly, since data from the CLHLS did not allow us to determine the reason for mortality, we thus did not further attribute FL and ADL disabilities to specific-cause mortality in the current study. Further studies focusing on the association of different subtypes and the duration of FL and ADL with mortality are needed. Finally, if we accounted for a set of common confounders, the results could be more robust. Some potential covariates, either unmeasured (e.g., medical treatment and diet) or unknown, might confound the association between FL, ADL, and mortality. The intensity and type of physical activities (strength training; walking; dancing; running; aquatic activities, etc.) could influence the ADL and survival status, while it was not collected in the CLHLS survey, which need explore the detailed associations among them in future study.
5. Conclusions
Prevalence of FL was serious among the older people in China, especially for the women, and the older people without FL had longer survival than that with FL. Disabilities of BADL and IADL and FL were negatively associated with the survival time of the older people in China. Additionally, the risk of mortality improved in old adults of higher age, women, unmarried/widowed marriage status, no physical activities engagement, and lower BMI. Disabilities of BADL and IADL performed significantly mediating roles in the relation of FL and survival. BADL disabilities negatively moderated the effect of FL on the survival of the older people, but this moderating effect was not significant for the male.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found here: http://opendata.pku.edu.cn/dataverse/CHADS<.
Ethics statement
The studies involving human participants were reviewed and approved by Duke University Health System Institutional Review Board. The patients/participants provided their written informed consent to participate in this study.
Author contributions
YG contributed to the management of the whole study, including the study conception, design, analysis, and interpretation of data, and drafted the article. LD, JC, and TH contributed to the revision of the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to acknowledge the Chinese Longitudinal Healthy Longevity Survey (CLHLS) team for providing data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. UN: United Nations Department Department of Economic and Social Affairs Population Division. World Population Ageing. New York, NY: United Nations Publication (2015).
2. Zhu A, Yan L, Wu C, Ji JS. Residential Greenness and frailty among older adults: a longitudinal cohort in China. J Am Med Dir Assoc. (2020) 21:759–65.e752. doi: 10.1016/j.jamda.2019.11.006
3. Wu C, Newman AB, Dong BR, Odden M. Index of healthy aging in chinese older adults: china health and retirement longitudinal study. J Am Geriatr Soc. (2018) 66:1303–10. doi: 10.1111/jgs.15390
4. Suzuki R, Blackwood J, Webster NJ, Shah S. Functional limitations and perceived neighborhood walkability among urban dwelling older adults. Front Public Health. (2021) 9:675799. doi: 10.3389/fpubh.2021.675799
5. Sathya T, Premkumar R. Association of functional limitations and disability with elder abuse in India: a cross-sectional study. BMC Geriatr. (2020) 20:220. doi: 10.1186/s12877-020-01619-3
6. Guccione AA, Felson DT, Anderson JJ, Anthony JM, Zhang Y, Wilson PW, et al. The effects of specific medical conditions on the functional limitations of elders in the Framingham study. Am J Public Health. (1994) 84:351–8. doi: 10.2105/ajph.84.3.351
7. Downer B, Pritchard K, Thomas KS, Ottenbacher K. Improvement in activities of daily living during a nursing home stay and one-year mortality among older adults with sepsis. J Am Geriatr Soc. (2021) 69:938–45. doi: 10.1111/jgs.16915
8. Tangen GG, Langballe EM, Strand B. Subjective memory impairment, instrumental activities of daily living and longitudinal effect on mortality among older adults in a population-based cohort study: the HUNT study. Scand J Public Health. (2020) 48:825–31. doi: 10.1177/1403494819885234
9. Chen S, Zheng J, Chen C, Xing Y, Cui Y, Ding Y, et al. Unmet needs of activities of daily living among a community-based sample of disabled elderly people in Eastern China: a cross-sectional study. BMC Geriatr. (2018) 18:160. doi: 10.1186/s12877-018-0856-6
10. Fu X, Su Y, Zeng C, Liu L, Guo Y, Wu Y. The mediation and interaction of depressive symptoms in activities of daily living and active aging in rural elderly: A cross-sectional survey. Front Public Health. (2022) 10:942311. doi: 10.3389/fpubh.2022.942311
11. Dunlop DD, Hughes SL, Manheim L. Disability in activities of daily living: patterns of change and a hierarchy of disability. Am J Public Health. (1997) 87:378–83. doi: 10.2105/ajph.87.3.378
12. Jagger C, Arthur AJ, Spiers NA, Clarke M. Patterns of onset of disability in activities of daily living with age. J Am Geriatr Soc. (2001) 49:404–9. doi: 10.1046/j.1532-5415.2001.49083.x
13. Paterson DH, Warburton D. Physical activity and functional limitations in older adults: a systematic review related to Canada's physical activity guidelines. Int J Behav Nutr Phys Act. (2010) 7:38. doi: 10.1186/1479-5868-7-38
14. Farias ST, Lau K, Harvey D, Denny KG, Barba C, Mefford A. Early functional limitations in cognitively normal older adults predict diagnostic conversion to mild cognitive impairment. J Am Geriatr Soc. (2017) 65:1152–8. doi: 10.1111/jgs.14835
15. Okun MA, August KJ, Rook KS, Newsom J. Does volunteering moderate the relation between functional limitations and mortality? Soc Sci Med. (2010) 71:1662–8. doi: 10.1016/j.socscimed.2010.07.034
16. Xu X, Yang L, Miao X, Hu X. An investigation and analysis of the activities of daily living of older adults living at home in Ningxia Hui Autonomous Region of China: a cross-sectional study. BMC Geriatr. (2020) 20:369. doi: 10.1186/s12877-020-01765-8
17. Dunlay SM, Manemann SM, Chamberlain AM, Cheville AL, Jiang R, Weston SA, et al. Activities of daily living and outcomes in heart failure. Circ Heart Fail. (2015) 8:261–7. doi: 10.1161/circheartfailure.114.001542
18. Luo D, Yu S, Wang J, Zhu Y, Yang L, Bai R, et al. Social participation of community-dwelling older adults in western China: a latent profile analysis. Front Public Health. (2022) 10:874204. doi: 10.3389/fpubh.2022.874204
19. Ono LM, Confortin SC, Figueiró TH, Rech CR, d'Orsi E. Influence of instrumental activities of daily living on the cognitive impairment: EpiFloripa study. Aging Ment Health. (2020) 24:382–6. doi: 10.1080/13607863.2018.1534079
20. Pudaric S, Sundquist J, Johansson S. Country of birth, instrumental activities of daily living, self-rated health and mortality: a Swedish population-based survey of people aged 55-74. Soc Sci Med. (2003) 56:2493–503. doi: 10.1016/s0277-9536(02)00284-8
21. Alexandre Tda S, Corona LP, Nunes DP, Santos JL, Duarte YA, Lebrão M. Gender differences in incidence and determinants of disability in activities of daily living among elderly individuals: SABE study. Arch Gerontol Geriatr. (2012) 55:431–7. doi: 10.1016/j.archger.2012.04.001
22. Zhao Y, Duan Y, Feng H, Nan J, Li X, Zhang H, et al. Trajectories of physical functioning and its predictors in older adults: A 12-year longitudinal study in China. Front Public Health. (2022) 10:923767. doi: 10.3389/fpubh.2022.923767
23. Global regional and and national age-sex-specific mortality for 282 causes of death in 195 countries and territories 1980-2017: 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/s0140-6736(18)32203-7
24. Gu D, Dupre ME, Sautter J, Zhu H, Liu Y, Yi Z. Frailty and mortality among Chinese at advanced ages. J Gerontol B Psychol Sci Soc Sci. (2009) 64:279–89. doi: 10.1093/geronb/gbn009
25. Yang F, Gu D. Predictability of frailty index and its components on mortality in older adults in China. BMC Geriatr. (2016) 16:145. doi: 10.1186/s12877-016-0317-z
26. Lawton MP, Brody E. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86
27. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe M. Studies of illness in the aged the index of adl: a standardized measure of biological and psychosocial function. JAMA. (1963) 185:914–9. doi: 10.1001/jama.1963.03060120024016
28. Discacciati A, Bellavia A, Lee JJ, Mazumdar M, Valeri L. Med4way: a Stata command to investigate mediating and interactive mechanisms using the four-way effect decomposition. Int J Epidemiol. (2018). doi: 10.1093/ije/dyy236
29. Latorre-Román PA, Laredo-Aguilera JA, García-Pinillos F, Soto-Hermoso VM, Carmona-Torres JM. Physical activity, weight and functional limitations in elderly Spanish people: the National Health Survey (2009-2014). Eur J Public Health. (2018) 28:778–83. doi: 10.1093/eurpub/ckx219
30. von dem Knesebeck O, Vonneilich N, Lüdecke D. Income and functional limitations among the aged in Europe: a trend analysis in 16 countries. J Epidemiol Community Health. (2017) 71:584–91. doi: 10.1136/jech-2016-208369
31. Bai X, Soh KG, Omar Dev RD, Talib O, Xiao W, Cai H. Effect of brisk walking on health-related physical fitness balance and life satisfaction among the elderly: a systematic review. Front Public Health. (2021) 9:829367. doi: 10.3389/fpubh.2021.829367
32. Merrill SS, Seeman TE, Kasl SV, Berkman L. Gender differences in the comparison of self-reported disability and performance measures. J Gerontol A Biol Sci Med Sci. (1997) 52:M19–26. doi: 10.1093/gerona/52a.1.m19
33. Dunlop DD, Manheim LM, Sohn MW, Liu X, Chang R. Incidence of functional limitation in older adults: the impact of gender, race, and chronic conditions. Arch Phys Med Rehabil. (2002) 83:964–71. doi: 10.1053/apmr.2002.32817
34. Serrano-Alarcón M, Perelman J. Ageing under unequal circumstances: a cross-sectional analysis of the gender and socioeconomic patterning of functional limitations among the Southern European elderly. Int J Equity Health. (2017) 16:175. doi: 10.1186/s12939-017-0673-0
35. Giltay EJ, Vollaard AM, Kromhout D. Self-rated health and physician-rated health as independent predictors of mortality in elderly men. Age Ageing. (2012) 41:165–71. doi: 10.1093/ageing/afr161
36. Burns RA, French D, Luszcz M, Kendig HL, Anstey K. Heterogeneity in the health and functional capacity of adults aged 85+ as risk for mortality. J Am Geriatr Soc. (2019) 67:1036–42. doi: 10.1111/jgs.15780
37. Feger DM, Willis SL, Thomas KR, Marsiske M, Rebok GW, Felix C, et al. Incident instrumental activities of daily living difficulty in older adults: which comes first? Findings from the advanced cognitive training for independent and vital elderly study. Front Neurol. (2020) 11:550577. doi: 10.3389/fneur.2020.550577
38. Hu Z, Zheng B, Kaminga AC, Zhou F, Xu H. Association between functional limitations and incident cardiovascular diseases and all-cause mortality among the middle-aged and older adults in china: a population-based prospective cohort study. Front Public Health. (2022) 10:751985. doi: 10.3389/fpubh.2022.751985
39. Nakazawa A, Nakamura K, Kitamura K, Yoshizawa Y. Association between activities of daily living and mortality among institutionalized elderly adults in Japan. J Epidemiol. (2012) 22:501–7. doi: 10.2188/jea.je20110153
40. Storeng SH, Sund ER, Krokstad S. Factors associated with basic and instrumental activities of daily living in elderly participants of a population-based survey: the Nord-Trøndelag health study, Norway. BMJ Open. (2018) 8:e018942. doi: 10.1136/bmjopen-2017-018942
41. Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel J. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet. (2017) 389:1619–29. doi: 10.1016/s0140-6736(17)30548-2
42. Chen J, Zeng Y, Fang Y. Effects of social participation patterns and living arrangement on mental health of Chinese older adults: A latent class analysis. Front Public Health. (2022) 10:915541. doi: 10.3389/fpubh.2022.915541
43. Chung W, Kim R. Does marriage really matter to health? Intra- and inter-country evidence from China, Japan, Taiwan, and the Republic of Korea. PLoS ONE. (2014) 9:e104868. doi: 10.1371/journal.pone.0104868
44. Blanner C, Mejldal A, Prina AM, Munk-Jørgensen P, Ersbøll AK, Andersen K. Widowhood and mortality: a Danish nationwide register-based cohort study. Epidemiol Psychiatr Sci. (2020) 29:e149. doi: 10.1017/s2045796020000591
45. Paganini-Hill A, Kawas CH, Corrada M. Activities and mortality in the elderly: the Leisure World cohort study. J Gerontol A Biol Sci Med Sci. (2011) 66:559–67. doi: 10.1093/gerona/glq237
46. Hou C, Ma Y, Yang X, Tao L, Zheng D, Liu X, et al. Disability transitions and health expectancies among elderly people aged 65 years and over in china: a nationwide longitudinal study. Aging Dis. (2019) 10:1246–57. doi: 10.14336/ad.2019.0121
47. Pennathur A, Magham R, Contreras LR, Dowling W. Daily living activities in older adults: part I - a review of physical activity and dietary intake assessment methods. Int. J. Ind. Ergon. (2003) 32:389–404. doi: 10.1016/s0169-8141(03)00098-2
48. Zhang Z, Dong J., Zhao C, Li Q. Trends of healthy life expectancy of the elderly in china in 1994-2015: revisiting from the perspective of morbidity transition. Front Public Health. (2021) 9:774205. doi: 10.3389/fpubh.2021.774205
Keywords: functional limitations, BADL, IADL, mortality, elderly, China
Citation: Gao Y, Du L, Cai J and Hu T (2023) Effects of functional limitations and activities of daily living on the mortality of the older people: A cohort study in China. Front. Public Health 10:1098794. doi: 10.3389/fpubh.2022.1098794
Received: 15 November 2022; Accepted: 22 December 2022;
Published: 20 January 2023.
Edited by:
Pablo Jorge Marcos-Pardo, University of Almeria, SpainReviewed by:
Rodrigo Gomes De Souza Vale, Rio de Janeiro State University, BrazilAndrea Guimarães, Universidade Federal de São João del-Rei, Brazil
Copyright © 2023 Gao, Du, Cai and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yumeng Gao,  eW1fZ2FvMDkyNSYjeDAwMDQwOzE2My5jb20=
eW1fZ2FvMDkyNSYjeDAwMDQwOzE2My5jb20=