 Yixuan Li
Yixuan Li Xueling Xiao
Xueling Xiao Yaqin Zhou
Yaqin Zhou Xinyi Su
Xinyi Su Honghong Wang
Honghong Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 09 January 2023
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1066781
This article is part of the Research TopicMental Health and Suicidal Behaviours among Sexual MinoritiesView all 5 articles
Background: Men who have sex with men (MSM) living with HIV suffer from psychosocial pressures and marginalization as a result of being HIV-positive and belonging to a sexual minority group, and self-injury or suicidal ideation are prevalent among this group. Studies have found that both perceived self-stigma and altered executive function is related to self-injury or suicidal ideation. However, the combined contribution of self-stigma and executive function to self-injury or suicidal ideation remains unclear, especially in MSM living with HIV. Therefore, this study is conducted to explore the mechanism of self-injury or suicidal ideation by hypothesizing that executive function plays a mediating role in the relationship between self-stigma and self-injury or suicidal ideation.
Methods: We conducted a cross-sectional survey among 448 MSM living with HIV who were recruited in the HIV clinic of a tertiary general hospital in Changsha, China, from November 2021 to February 2022. A questionnaires survey was adopted to collect sociodemographic and disease-related information and data related to executive function (including working memory, inhibition, and task monitoring), self-stigma, and self-injury or suicidal ideation. Structural equation modeling and bootstrap testing were used to investigate the potential mediating role of executive function in the relationship between self-stigma and suicidal ideation.
Results: The participants were aged 18–76 years. Those who had ever had self-injury or suicidal ideation accounted for 32.8% of the total. A higher level of self-stigma and poorer executive function were associated with more frequent self-injury or suicidal ideation (p < 0.01). The mediation model analysis showed a good fit (x2/df = 1.07, p = 0.381). The direct effect of self-stigma on self-injury or suicidal ideation (β = 0.346, p < 0.001) and the indirect effect of self-stigma via executive function (β = 0.132, p < 0.001) were significant, with the indirect effect accounting for 27.6% of the total effect.
Conclusions: This study demonstrates that executive function mediates the relationship between self-stigma and self-injury or suicidal ideation among MSM living with HIV. It suggests that future studies targeting enhancing executive function and decreasing self-stigma may reduce self-injury or suicidal ideation among MSM living with HIV.
The number of men who have sex with men (MSM) living with HIV has steadily increased. Globally, the proportion of new HIV infections among MSM rose by 25% between 2010 and 2021 (1). Further, among the 1.5 million individuals newly infected with HIV in 2021, an estimated 21% were MSM (2). MSM living with HIV are a vulnerable and marginalized population. They suffer from psychosocial pressures as a result of being HIV-positive and belonging to a sexual minority group because of their homosexual identity (3). MSM living with HIV exhibit increased risks of self-injury or suicidal ideation owing to various issues including mental and physical health problems and risk-taking behaviors (4–6). Self-injury or suicidal ideation has a high possibility of leading to injury or death as ideation leads to actual behaviors (7), and the ideation of self-injury and suicide usually overlap and exist on a continuum which could be combined to predict actual suicide (8, 9). Concerningly, the incidence of self-injury or suicidal ideation among MSM living with HIV is 10.7–47.0% (10–12), which is 2.22 times higher than that among HIV-negative counterparts (13). Thus, we measured the self-injury or suicidal ideation as one combined outcome, and tried to understand its mechanism of self-injury or suicidal ideation among this specific population to enhance suicide prevention efforts.
Self-stigma, namely, the devaluation on oneself because of the perception of negative characteristics from the broader society (14), is considered an essential risk factor for self-injury or suicidal ideation in MSM living with HIV. In both developed and developing settings, MSM, as a sexual minority group, suffer unfairness and rejection from their peers and face a high risk of losing their jobs or experiencing barriers to accessing health care, all of which can increase their self-stigma (15, 16). For MSM living with HIV report even higher levels of self-stigma, reflecting their worse situation (17, 18). MSM living with HIV suffer from higher self-stigma because of the prejudice of the public toward them, such as through beliefs that such individuals engaged in immoral sexual behaviors (e.g., having condom-less anal sex after substance use or having multiple sexual partners) (16). High levels of self-stigma can have various negative consequences, including experiences of prejudice and social isolation in daily life and a fear of seeking healthcare (19). These findings are particularly troublesome given that being isolated or lacking healthcare prevent these individuals from getting professional HIV treatment and necessary mental health support they need (20). Ultimately, this combination of factors marginalizes such individuals and drives them into a state of hopelessness (21), which can lead to self-injury, suicidal ideation, or even suicide (22). A previous study showed that MSM living with HIV and perceiving self-stigma were 2.4 times more likely to have suicidal ideation than those without self-stigma (23).
Executive function also has a potential impact on self-injury or suicidal ideation among MSM living with HIV. Executive function is a high-level cognitive process that facilitates individuals to behave reasonably, purposefully, and thoughtfully (24). Theoretically, the core aspects of executive function, including working memory, inhibition, and task monitor, are associated with individuals' behaviors and intentions (25). Deficits in executive function can result in misunderstandings and inaccurate responses to internal and external environmental challenges; consequently, individuals may be easily overwhelmed and may engage in self-injury or suicidal ideation (26). Previous studies found executive function impairments among the HIV-negative population with suicidal ideation or suicidal behavior (27–29). Although limited evidence is available for HIV-positive individuals, one previous study suggested that suicidal ideation in this population might be a reflection of executive function deficits (30). Moreover, executive function impairment has been widely reported among HIV-positive individuals, as the virus can invade the frontal lobe of the brain, which is the area that controls executive function (31–33). Therefore, the connection between executive function and self-injury or suicidal ideation needs to be examined among MSM living with HIV who are vulnerable to having impaired executive function.
In addition, self-stigma is associated with executive function. It has been reported that self-stigma can have a direct effect on cognitive performance as it can reduce reasoning ability (34), thus influencing the executive function. Sexual minorities often report both impaired executive function and a high level of self-stigma (35–38). This association was also demonstrated among people living with HIV. Two studies revealed that HIV-related stigma is a significant predictor of poor performance on cognitive tests and may have long-lasting effects on brain function, especially executive function (39, 40). Moreover, a previous study investigating 70 MSM living with HIV reported that individuals with lower HIV-related self-stigma performed better in working memory, a core aspect of executive function (41). In this regard, self-stigma, especially that related to HIV, may be associated with deficits in executive function.
However, how executive function affects the relationship between self-stigma and self-injury or suicidal ideation is unclear as executive function impairment is associated with both. Furthermore, this correlation needs to be explored in MSM living with HIV as this vulnerable population faces all three difficulties: impaired executive function, severe self-stigma, and a high level of self-injury or suicidal ideation. Thus, this study is conducted to investigate the mechanism of self-injury or suicidal ideation among MSM living with HIV by hypothesizing that executive function is negatively associated with suicidal ideation and mediates the relationship between self-stigma and self-injury or suicidal ideation. The study could provide evidence for the further understanding and development of interventions for the prevention of self-injury and suicidal ideation among MSM living with HIV.
The present cross-sectional study was conducted from November 2021 to February 2022 in Changsha, China. We recruited participants in an HIV clinic of a tertiary general hospital in Changsha, where the annual outpatient volume is approximately 35,000 visits. The eligibility criteria were individuals (1) aged 18 years or older; (2) born as males; (3) self-reporting as being homosexual, bisexual, or having sex with men; and (4) diagnosed with HIV (as confirmed by diagnosis report). Individuals who self-reported having a history of brain injury or brain surgery, or who were unable to finish the survey for any intellectual or physical reason, were excluded.
Participants were recruited when they came to the HIV clinic to access health services. Four trained research assistants approached and screened 724 males for eligibility to participate. Of these, 58 were excluded because they did not have a confirmed HIV diagnosis (n = 55) or were unable to complete the questionnaire (n = 3). Around 30% (218/724) of eligible MSM living with HIV rejected to participate in this study because they were not interested or did not have time. Finally, 449 participants completed the survey.
Participation was on a voluntary basis. The HIV-infected status was confirmed through each participants' diagnosis report. After obtaining informed consent from the participants, the research assistants provided a brief explanation of how to complete the survey. Participants were then invited to answer the questionnaire in a quiet office with good privacy. Every completed questionnaire was deposited in a locked storage box by the research assistants. One incomplete questionnaire was excluded, resulting in a total of 448 valid questionnaires being included in this study.
The questionnaire consisted of four parts to collect sociodemographic and disease-related information, and data related to self-injury or suicidal ideation, executive function, and self-stigma.
Sociodemographic characteristics included age, education level, occupational status, marital status, and monthly income. Disease-related information included HIV duration (time elapsed since the HIV diagnosis), latest CD4 count (cells/μl), and HIV viral load, all of which were obtained from medical records. An HIV viral load lower than 20 copies per ml was categorized as target not detected (TND). Those without CD4 count and HIV viral load data were defined as unknown.
Self-injury or suicidal ideation was assessed using a single item: “Over the last 2 weeks, how often have you been bothered by thoughts that you would be better off dead or hurting yourself in some way?” This method has been used in several studies (42–44) and has proven validity in assessing individuals' self-injury or suicidal ideation. The response options ranged from 0 to 3 (0 = not at all, 1= several days, 2 = more than half the days, 3 = nearly every day). In this study, self-injury or suicidal ideation was categorized as a dichotomous variable by combining those who chose 1, 2, or 3 as “yes” and those who chose 0 as “no.”
Executive function was assessed using the Chinese version of the Behavior Rating Inventory of Executive Function—Adult Version, a widely used 3-point Likert scale with perfect psychometric characteristics (45). This scale includes eight dimensions, each of which measures one aspect of executive function (46). Specifically, we measured three core dimensions of executive function—inhibition (e.g. “I have difficulty in waiting in line”), working memory (e.g. “I am prone to forgetting instructions”), and task monitoring (e.g. “I do not check for mistakes in my work”)—which contained 8, 8, and 6 items respectively. Every item was scored from 1 to 3 (1= never, 2 = sometimes, 3 = always). The possible range were 8–24, 8–24, and 6–18 for the domain of inhibition, working memory, and task monitoring, respectively, and a higher score in a particular dimension reflected poorer executive function in this domain.
Self-stigma among MSM living with HIV was measured by a brief stigma scale containing 10 items for HIV-positive individuals. This scale is widely used to assess the HIV-related stigma of people living with HIV and is known to show good reliability and validity (47). This scale includes four domains of self-stigma: personalized stigma, disclosure concerns, negative self-image, and public attitudes. For example, one of the items had asked “I feel that I am not as good a person as others”, and the answer rated on a 4-point Likert scale ranged from “strongly disagree” to “strongly agree.” The total score ranged from 10 to 40, and a higher score reflected a higher level of self-stigma.
All data were double input in EpiData Version 3.1 to ensure accuracy and integrity. The descriptive and correlation analyses were conducted in SPSS Version 22.0. Percentages were used to summarize categorical variables. For continuous variables, a normality test was performed first, and the means (standard deviations, SDs) and medians (interquartile, IQR) were adopted accordingly. Pearson's correlation test was used to identify the association between continuous variables, and a point-biserial correlation test was used to verify the association between continuous variables and the binary variable.
The mediation model was explored using Mplus Version 7.0. The Mplus code was based on the original PROCESS diagrams by Andrew Hayes (48). We modified model number 4d, which showed an example of how to handle a dichotomous outcome. We used bootstrap testing with 1,000 resamples to calculate the 95% confidence intervals (CIs). It indicated a significant direct and indirect effect if the 95% CI excluded zero. We tested the unadjusted mediation model and then the adjusted model with the confounding variables being controlled. Variables that showed a significant effect on the mediating or outcome variable after monofactor analysis were defined as confounding variables (49). In this mediation model, we found no confounders of self-injury; however, age, education level, and occupational status were identified to be confounding variables of executive function. Thus, these three variables were controlled in the adjusted model. Statistical test volumes including x2/df, root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker–Lewis index (TLI) were used to evaluate the goodness-of-fit of the model. As suggested by Dexin Shi (50), RMSEA should be lower than 0.08, CFI and TLI should be no < 0.90, and x2/df should not be higher than 2.00.
This study was approved by the Institutional Review Board of the Xiangya School of Nursing, Central South University. Participants who reported having self-injury or suicidal ideation were directed to a psychological clinic in the city for further treatment and guidance. We provided a compensation of Renminbi 50 Yuan (equaling to USD $6.95) to each participant. No identifying information was collected in this study, and only research group members had access to the data.
A total of 448 valid questionnaires were included in this study, and the sample characteristics are shown in Table 1. The participants were aged 18–76 years, with a median age of 30 years. Only around a quarter (26.1%) were married or partnered. The HIV durations were 1–210 months, with a median duration of 47.5 months. A majority of the participants (n = 401, 89.5%) had a CD4 count above 200 cells/μl, and around three-quarters (n = 332, 74.1%) were in TND status.
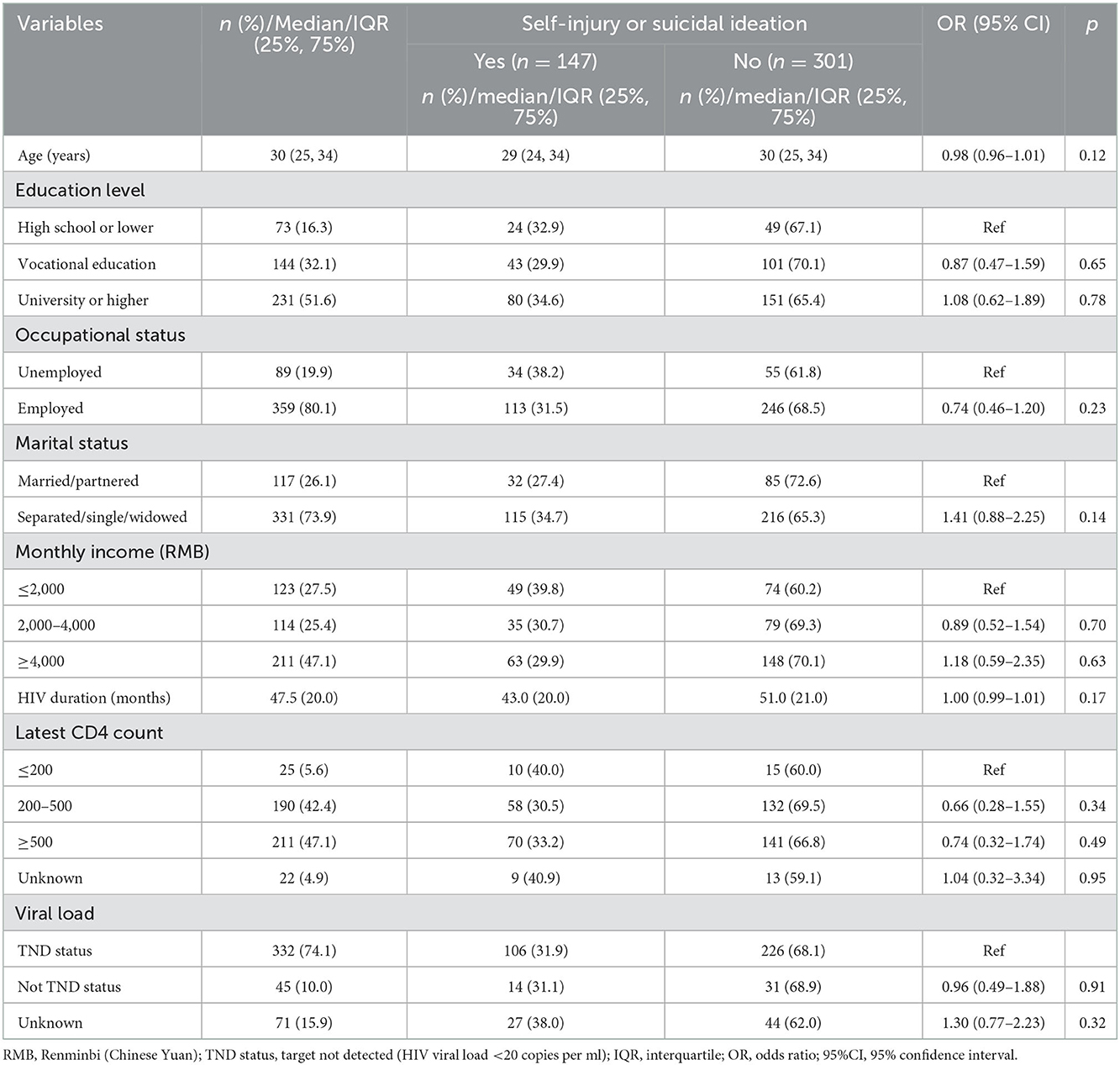
Table 1. Differences in self-injury or suicidal ideation according to general characteristics (n = 448).
Overall, 32.8% (147/448) of the participants reported self-injury or suicidal ideation. Specifically, around one-fifth (21.7%, 97/448) of the participants reported that they had thought of suicide or hurting themselves in some way for several days over the past 2 weeks; 8.3% (n = 37) had this ideation more than half of the days; and 13 participants reported that they had thought of self-injury or suicide nearly every day. However, there was no statistically significant difference in self-injury or suicidal ideation based on general characteristics (see Table 1).
As shown in Table 2, the mean score for self-stigma was 28.46 (SD 5.97), exceeding 70% of the possible range. The scores for the three core executive functions, namely, inhibition, working memory, and task monitoring, were all at an intermediate level, with medians of 12, 11, and 9, respectively.
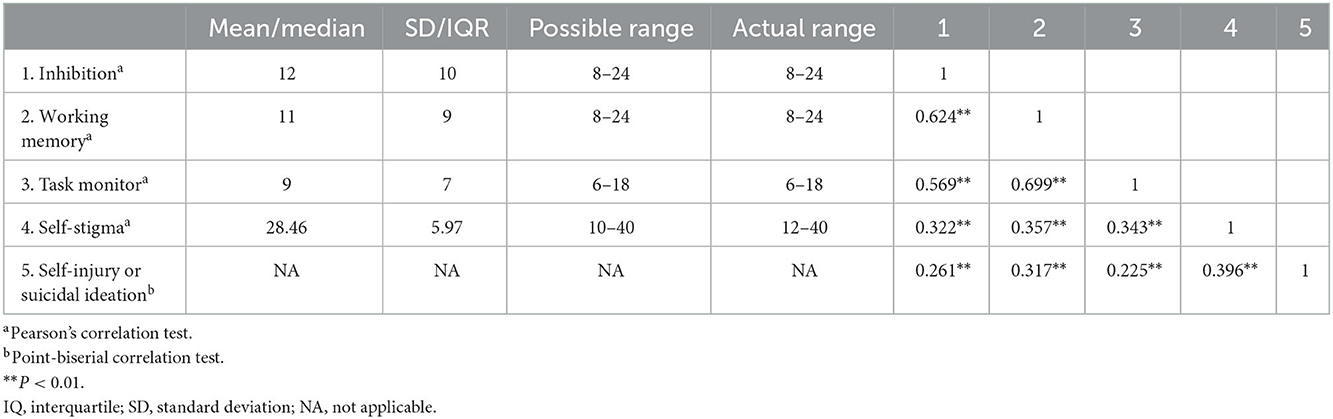
Table 2. Correlations for the relationships between executive function (inhibition, working memory, task monitor), self-stigma, and self-injury or suicidal ideation.
Self-injury or suicidal ideation was significantly associated with inhibition (r = 0.261, p < 0.01), working memory (r = 0.317, p < 0.01), and task monitoring (r = 0.225, p < 0.01; Table 2). Furthermore, suicidal ideation had a positive correlation with self-stigma (r = 0.396, p < 0.01), indicating that higher self-stigma was associated with more frequent self-injury or suicidal ideation. Self-stigma was also related to three core executive functions, with the correlation coefficient ranging from 0.322 to 0.357 (p < 0.01).
The results of the mediation analysis are shown in Table 3 and Figure 1. In the unadjusted model, the direct effect of self-stigma on self-injury or suicidal ideation was statistically significant (β = 0.349, p < 0.001), as was the indirect effect (β = 0.131, p < 0.001). The indirect effect accounted for 27.3% of the total effect.
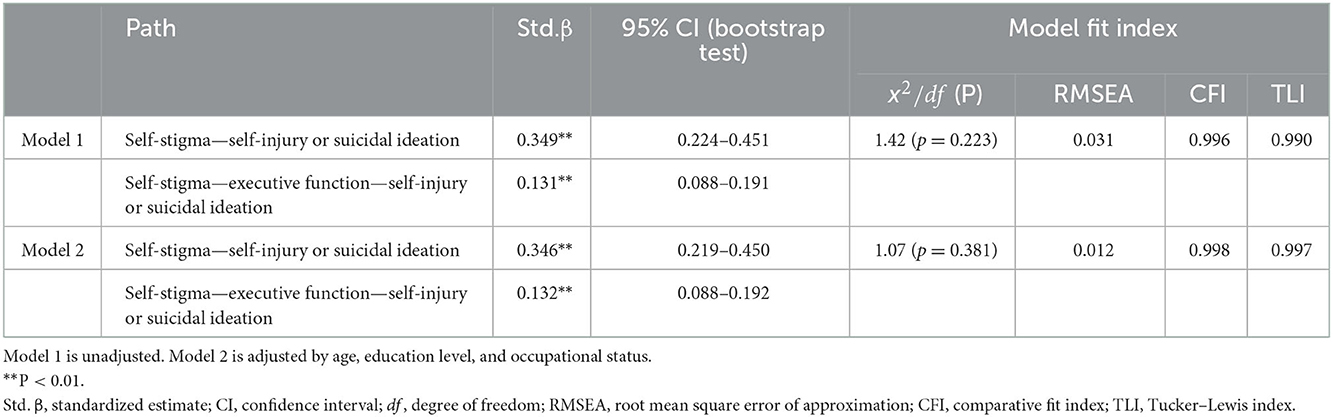
Table 3. Parameters of the mediated model of self-stigma and self-injury or suicidal ideation mediated by executive function.
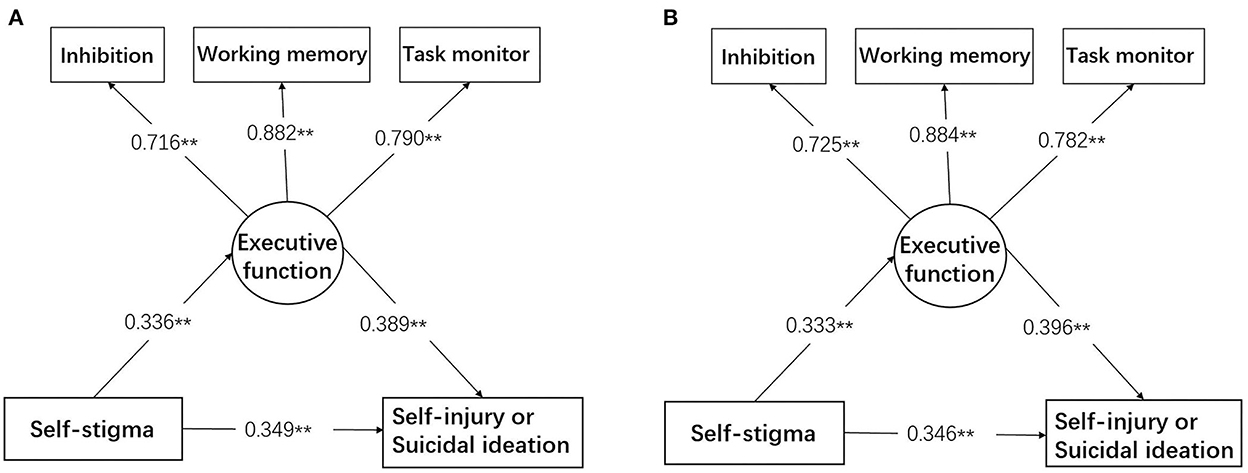
Figure 1. Mediation model in which the relationship between self-stigma and self-injury or suicidal ideation was mediated by the three core executive functions, namely, inhibition, working memory, and task monitor. (A) Shows the unadjusted model. (B) Shows the model adjusted by age, education level, and occupational status. **p < 0.001.
The adjusted model with age, education level, and occupational status being controlled (Figure 1B) showed a higher proportion of indirect effect (27.6%) compared to the case of the unadjusted model. The direct effect of self-stigma on self-injury or suicidal ideation decreased to 0.346 (p < 0.001), and the indirect effect increased to 0.132 (p < 0.001).
The three significant variables of inhibition, working memory, and task monitor well represented the executive function, with factor loadings of 0.716–0.882 (p < 0.001). The mediation model also demonstrated good fit information, and the fit index was better when adjusted for confounding variables (x2/df = 1.07, p = 0.381, RMSEA = 0.012, CFI = 0.998, TLI = 0.997).
This study explored the relationships between self-injury or suicidal ideation, self-stigma, and executive function among MSM living with HIV. Our sample showed high levels of both self-injury or suicidal ideation and self-stigma, indicating that the participants were suffering from a heavy psychosocial burden. Overall, in line with our hypothesis, poorer executive function was associated with a higher level of self-injury or suicidal ideation, and the relationship between self-injury or suicidal ideation and self-stigma among MSM living with HIV was partly mediated by their executive function.
Around 30% of MSM living with HIV reported self-injury or suicidal ideation in this sample, which was consistent with the results of previous studies in China (23, 51). The proportion was much higher than that in countries with more inclusive sexual attitudes, such as the US (3.2%) and Spain (15.3%) (52, 53). The high prevalence of self-injury or suicidal ideation may be attributed to the traditional sexual values that are deeply rooted in Chinese society, namely, that homosexuality is unacceptable to the majority of Chinese people (54). In China, individuals living with HIV are considered to be reckless individuals, and they suffer from stigma and discrimination from the public and even their family members or friends, which can increase the likelihood of suicide (55). Importantly, the incidence of self-injury or suicidal ideation among MSM living with HIV is higher than that among general MSM (18.3%) or heterosexual HIV-positive individuals (22.5%) (56, 57). This may be explained by the fact that MSM living with HIV are under the dual pressure of being HIV-positive and belonging to a sexual minority group, which could drive them to hurt themselves. As stated in the Minority Stress Theory (58), MSM living with HIV perceived a culturally sanctioned and categorically ascribed inferior status, resultant prejudice, and discrimination. The cumulative experiences were gradually internalized to the internal stress which worsened their survival situation and may lead to the appearance of self-injury or suicidal ideation. Thus, there is a more urgent need to increase support for MSM living with HIV compared to that for general HIV-positive individuals or other sexual minorities.
As we hypothesized, executive function was negatively associated with self-injury or suicidal ideation among MSM living with HIV. This finding was aligned with previous studies that focused on mood disorder samples, which showed that impaired executive function could be a risk factor of suicidality, because those with suicidal ideation showed reduced structural connectivity among the frontal-subcortical circuits, including in the regions associated with executive function (59, 60). In addition, executive function deficit was considered a candidate endophenotype for genetics research on suicidal behavior (61). Individuals with executive function deficits find it difficult to be reflective, are likely to act impulsively (62), are unable to reason based on factual information and evaluation (63), and lack rational thinking (64–66). It is therefore understandable that for some individuals with impaired executive function, committing suicide seems to be the only option when they face stressful life events, because they struggle to reflect, reason, and think rationally about their situation and are likely to make an impulsive decision.
Our results show that executive function partially mediated the relationship between self-stigma and self-injury or suicidal ideation among MSM living with HIV. Moreover, the fact that executive function accounted for 27.6% of this association indicates that executive function plays an important role in it. Perceptions of stigma, especially HIV-related self-stigma, drive individuals to avoid social activities and isolate themselves (67). Social isolation may have a negative effect on brain structures, which is reflected in low executive function performance (68). A possible explanation for the negative effect is that those with a high level of self-stigma suffer from chronic stress caused by people around them or even themselves (17). When they are stressed, they are more concerned about being judged negatively than about thinking rationally to reach their goals (69). Gradually, they lose their goal-oriented behavioral ability, eventually leading to retrogressive executive function. In turn, MSM living with HIV who have executive function deficits are thought to have difficulty in thinking about long-term outcomes and usually focus on the current dilemma (70, 71), which might culminate in despair and lead to self-injury or suicidal ideation as the only solution they recognize. In light of this, it is necessary to think about the impact of executive function when analyzing self-injury or suicidal ideation and self-stigma among MSM living with HIV.
To the best of our knowledge, this was the first study conducted among MSM living with HIV to explore the mediating role of executive function in the relationship between self-injury or suicidal ideation and self-stigma. This research provides a theoretical basis for and empirical evidence of the mechanism of self-injury or suicidal ideation among this population, thus enabling a better understanding. Moreover, it provides a possible route for future intervention development to decrease suicidal behavior among MSM living with HIV. This study implies that strategies for improving executive function and simultaneously eliminating self-stigma may achieve an optimal outcome in reducing self-injury or suicidal ideation or behavior among MSM living with HIV. Existing studies have demonstrated the effectiveness of self-stigma avoidance methods such as increasing the awareness of mental health condition and strengthening self-regulation skills (72, 73). Further, executive function training, such as helping them identify their own motivating goals or activate intentional self-regulation in stressful situations, showed effectiveness in changing behaviors such as sedentary activity, unhealthy eating and inability to sit still (74, 75). These abovementioned strategies could be adopted among MSM living with HIV to reduce self-injury or suicidal ideation.
Inevitably, there were some limitations in this study. First, the cross-sectional design limited the study's ability to confirm the causal associations between variables. A longitudinal study should be conducted to obtain a deeper understanding of these relationships. Second, this study only explored three core executive functions instead of all the domains. Therefore, the generalization of the results related to executive function and self-injury or suicidal ideation should be treated with caution. Third, our sample only included MSM living with HIV in Hunan. A sample from other regions with various economic and cultural backgrounds may have generated different results, because the public attitudes toward MSM and HIV are deeply associated with the local culture and social norms.
The MSM living with HIV suffer from a high level of self-injury or suicidal ideation, and executive function is negatively associated with this. Importantly, the correlation between self-stigma and self-injury or suicidal ideation is partially mediated by executive function among this specific population. Therefore, interventions that target promoting executive function and reducing self-stigma may work optimally to reduce self-injury and suicidal ideation in this population.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Institutional Review Board of the Nursing School of Xiangya, Central South University. The patients/participants provided their written informed consent to participate in this study.
XX designed this study. YL wrote the manuscript and performed the statistical analyses. YZ and XS contributed to data interpretation. XX and HW edited and revised the manuscript for important intellectual content and gave scientific advice. All authors contributed to this article and approve the final submission.
This study was supported by the National Natural Science Foundation of China (Grant Number 82204169).
The authors are grateful to all participants for their participation and to the staff of the HIV Clinic of a Tertiary General Hospital in Changsha for their assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1066781/full#supplementary-material
1. UNAIDS. UNAIDS Global AIDS Update:In Danger. E. coli. (2022). Available online at: https://www.unaids.org/en/resources/documents/2022/in-danger-global-aids-update (accessed November 18, 2022).
2. World Health Organization. E. coli. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. (2021). Available online at: who.int (accessed September 15, 2022).
3. Winter S, Diamond M, Green J, Karasic D, Reed T, Whittle S, et al. Transgender people: health at the margins of society. Lancet. (2016) 388:390–400. doi: 10.1016/S0140-6736(16)00683-8
4. Cook MC, Morisky DE, Williams JK, Ford CL, Gee GC. Sexual risk behaviors and substance use among men sexually victimized by women. Am J Public Health. (2016) 106:1263–9. doi: 10.2105/AJPH.2016.303136
5. Parsons JT, Grov C, Golub SA. Sexual compulsivity, co-occurring psychosocial health problems, and HIV risk among gay and bisexual men: further evidence of a syndemic. Am J Public Health. (2012) 102:156–62. doi: 10.2105/AJPH.2011.300284
6. Scott RL, Lasiuk G, Norris C. The relationship between sexual orientation and depression in a national population sample. J Clin Nurs. (2016) 25:3522–32. doi: 10.1111/jocn.13286
7. Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annual Rev Clin Psychol. (2016) 12:307–30. doi: 10.1146/annurev-clinpsy-021815-093204
8. Asarnow JR, Porta G, Spirito A, Emslie G, Clarke G, Wagner KD, et al. Suicide attempts and nonsuicidal self-injury in the treatment of resistant depression in adolescents: findings from the TORDIA study. J Am Acad Child Adolesc Psychiatry. (2011) 50:772–81. doi: 10.1016/j.jaac.2011.04.003
9. Wester KL, Ivers N, Villalba JA, Trepal HC, Henson R. The relationship between nonsuicidal self-injury and suicidal ideation. J Counsel Dev. (2016) 94:3–12. doi: 10.1002/jcad.12057
10. Deuba K, Ekstrom AM, Shrestha R, Ionita G, Bhatta L, Karki DK. Psychosocial health problems associated with increased HIV risk behavior among men who have sex with men in Nepal: a cross-sectional survey. PLoS ONE. (2013) 8:e58099. doi: 10.1371/journal.pone.0058099
11. Wang YY, Dong M, Zhang QE, Xu DD, Zhao J, Ng CH, et al. Suicidality and clinical correlates in Chinese men who have sex with men (MSM) with HIV infection. Psychol Health Med. (2019) 24:137–43. doi: 10.1080/13548506.2018.1515495
12. Peltekis A, Koulentianou M. Clinical presentation and requests for support of people with HIV/AIDS seeking counselling and psychotherapy in Greece. Psychiatriki. (2019) 30:120–8. doi: 10.22365/jpsych.2019.302.120
13. Stahlman S, Grosso A, Ketende S, Pitche V, Kouanda S, Ceesay N, et al. Suicidal ideation among MSM in three West African countries: Associations with stigma and social capital. Int J Soc Psychiatry. (2016) 62:522–31. doi: 10.1177/0020764016663969
14. Alonzo AA, Reynolds NR. Stigma, HIV and AIDS: an exploration and elaboration of a stigma trajectory. Soc Sci Med. (1995) 41:303–15. doi: 10.1016/0277-9536(94)00384-6
15. Cáceres CF, Konda KA, Klausner JD. Syphilis in men who have sex with men: advancing research and human rights. Lancet Glob Health. (2021) 9:e1039–40. doi: 10.1016/S2214-109X(21)00269-2
16. Clements-Nolle K, Marx R, Guzman R, Katz M, HIV. prevalence, risk behaviors, health care use, and mental health status of transgender persons: Implications for public health intervention. Am J Public Health. (2001) 91:915–21. doi: 10.2105/AJPH.91.6.915
17. Nelson LE, Wilton L, Agyarko-Poku T, Zhang NH, Aluoch M, Thach CT, et al. The association of HIV stigma and HIV/STD knowledge with sexual risk behaviors among adolescent and adult men who have sex with men in Ghana, West Africa. Res Nurs Health. (2015) 38:194–206. doi: 10.1002/nur.21650
18. Fitzgerald-Husek A, Van Wert MJ, Ewing WF, Grosso AL, Holland CE, Katterl R, et al. Measuring stigma affecting sex workers (SW) and men who have sex with men (MSM): a systematic review. PLoS ONE. (2017) 12:e0188393. doi: 10.1371/journal.pone.0188393
19. Jeffries WL, Townsend ES, Gelaude DJ, Torrone EA, Gasiorowicz M, Bertolli J, et al. stigma experienced by young men who have sex with men (MSM) living with HIV infection. AIDS Educ Prevent. (2015) 27:58–71. doi: 10.1521/aeap.2015.27.1.58
20. Brewer R, Hood KB, Moore M, Spieldenner A, Daunis C, Mukherjee S, et al. An exploratory study of resilience, HIV-related stigma, and HIV care outcomes among men who have sex with men (MSM) living with HIV in Louisiana. AIDS Behav. (2020) 24:2119–29. doi: 10.1007/s10461-020-02778-5
21. Farias OO, Guedes DDS, Freitas PCA, Galvão MTG, Cunha GHD, Lima ICV. Analysis of the needs for help of men who have sex with men and live with HIV. Rev Esc Enferm USP. (2020) 54:e03650. doi: 10.1590/s1980-220x2019010303650
22. Abelson J, Lambevski S, Crawford J, Bartos M, Kippax S. Factors associated with 'feeling suicidal': the role of sexual identity. J Homosex. (2006) 51:59–80. doi: 10.1300/J082v51n01_04
23. Wu YL, Yang HY, Wang J, Yao H, Zhao X, Chen J, et al. Prevalence of suicidal ideation and associated factors among HIV-positive MSM in Anhui, China. Int J STD AIDS. (2015) 26:496–503. doi: 10.1177/0956462414544722
24. Diamond A. Executive functions. In: Fiske ST, editor. Annu Rev Psychol. (2013) 64:135–68. doi: 10.1146/annurev-psych-113011-143750
25. Gawronski B, Payne BK. Handbook of Implicit Cognition: Measurement, Theory, and Applications. New York, NY: Guilford Publications (2010).
26. Vance DE, Ross JA, Moneyham L, Farr KF, Fordham P. A model of cognitive decline and suicidal ideation in adults aging with HIV. J Neurosci Nurs. (2010) J42:150–6. doi: 10.1097/JNN.0b013e3181d4a35a
27. Fernández-Sevillano J, Alberich S, Zorrilla I, González-Ortega I, López MP, Pérez V, et al. Cognition in recent suicide attempts: altered executive function. Front Psychiatry. (2021) 12:701140. doi: 10.3389/fpsyt.2021.701140
28. McGirr A, Dombrovski AY, Butters MA, Clark L, Szanto K. Deterministic learning and attempted suicide among older depressed individuals: cognitive assessment using the wisconsin card sorting task. J Psychiatr Res. (2012) 46:226–32. doi: 10.1016/j.jpsychires.2011.10.001
29. Richard-Devantoy S, Berlim MT, Jollant F. A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychol Med. (2014) 44:1663–73. doi: 10.1017/S0033291713002304
30. Vance DE, Moneyham L, Farr KF. Suicidal ideation in adults aging with HIV NEUROLOGICAL AND COGNITIVE CONSIDERATIONS. J Psychosoc Nurs Ment Health Serv. (2008) 46:33–8. doi: 10.3928/02793695-20081101-11
31. Anderson AM, Perez-Santiago J, Zheng ZD, Huang E, Franklin D, Iudicello J, et al. Better executive function is independently associated with full HIV suppression during combination therapy. AIDS. (2019) 33:2309–16. doi: 10.1097/QAD.0000000000002348
32. Irollo E, Luchetta J, Ho C, Nash B, Meucci O. Mechanisms of neuronal dysfunction in HIV-associated neurocognitive disorders. Cell Mol Life Sci. (2021) 78:4283–303. doi: 10.1007/s00018-021-03785-y
33. Kanmogne GD, Fonsah JY, Tang B, Doh RF, Kengne AM, Umlauf A, et al. Effects of HIV on executive function and verbal fluency in Cameroon. Sci Rep. (2018) 8:17794. doi: 10.1038/s41598-018-36193-7
34. Chan SKW, Kao SYS, Leung SL, Hui CLM, Lee EHM, Chang WC, et al. Relationship between neurocognitive function and clinical symptoms with self-stigma in patients with schizophrenia-spectrum disorders. J Ment Health. (2019) 28:583–8. doi: 10.1080/09638237.2017.1340599
35. Parker CM, Hirsch JS, Philbin MM, Parker RG. The urgent need for research and interventions to address family-based stigma and discrimination against lesbian, gay, bisexual, transgender, and queer youth. J Adol Health. (2018) 63:383–93. doi: 10.1016/j.jadohealth.2018.05.018
36. Huebner DM, McGarrity LA, Smith TW, Perry NS, Suchy Y. Changes in executive function following a stressful interpersonal task are associated with condomless anal intercourse among men who have sex with men. Ann Behav Med. (2018) 52:406–11. doi: 10.1093/abm/kax020
37. Snyder HR. Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: a meta-analysis and review. Psychol Bull. (2013) 139:81–132. doi: 10.1037/a0028727
38. Pescosolido BA, Medina TR, Martin JK, Long JS. The “Backbone” of stigma: identifying the global core of public prejudice associated with mental illness. Am J Public Health. (2013) 103:853–60. doi: 10.2105/AJPH.2012.301147
39. Zhao JF Ji LL, Du SS, Gu H, Zhao Q, Chi PL, et al. Working memory impairment in children orphaned by parental HIV/AIDS: an event-related potentials study. Psychol Health Med. (2021) 26:1–14. doi: 10.1080/13548506.2021.1896761
40. Gu H, Shan X, He H, Zhao J, Li X, EEG. Evidence of altered functional connectivity and microstate in children orphaned by HIV/AIDS. Front Psychiatry. (2022) 13:898716. doi: 10.3389/fpsyt.2022.898716
41. Ruiz-Robledillo N, Clement-Carbonell V, Ferrer-Cascales R, Portilla-Tamarit I, Alcocer-Bruno C, Gabaldon-Bravo E. Cognitive functioning and its relationship with self-stigma in men with HIV who have sex with men: the mediating role of health-related quality of life. Psychol Res Behav Manag. (2021) 14:2103–14. doi: 10.2147/PRBM.S332494
42. Batterham PJ, Calear AL, Christensen H, Carragher N, Sunderland M. Independent effects of mental disorders on suicidal behavior in the community. Suicide Life Threat Behav. (2018) 48:512–21. doi: 10.1111/sltb.12379
43. Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, et al. Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics. (2015) 135:E496–509. doi: 10.1542/peds.2014-1864
44. Salman M, Shehzadi N, Mustafa ZU, Mallhi TH, Khan YH, Khan TM, et al. Self-harm and suicidal ideation in Pakistani youth amid COVID-19 pandemic: findings of a large, cross-sectional study. Psychol Health Med. (2022) 4:1–9. doi: 10.1080/13548506.2022.2119483
45. Du QQY, Yufeng W. Reliability and validity of the adult version of the self-assessment questionnaire of the Executive Functioning Behavior Rating Scale Clinical Psychiatry, China. (2010) 24:647–79. doi: 10.3969/j.issn.1000-6729
46. Rabin LA, Roth RM, Isquith PK, Wishart HA, Nutter-Upham KE, Pare N, et al. Self- and informant reports of executive function on the BRIEF-A in MCI and older adults with cognitive complaints Arch Clin Neuropsychol. (2006) 21:721–32. doi: 10.1016/j.acn.2006.08.004
47. Wright K, Naar-King S, Lam P, Templin T, Frey M. Stigma scale revised: Reliability and validity of a brief measure of stigma for HIV plus youth. J Adol Health. (2007) 40:96–8. doi: 10.1016/j.jadohealth.2006.08.001
48. Stride CB, Gardner S, Catley N, Thomas F. Mplus Code for Mediation, Moderation, Moderated Mediation Models'. (2015). Available online at: http://www.offbeat.group.shef.ac.uk/FIO/mplusmedmod.htm. (accessed July,5 2022).
49. Davood Tofighi KK. Assessing omitted confounder bias in multilevel mediation models. Multivariate Behav Res. (2016) 51:86–105. doi: 10.1080/00273171.2015.1105736
50. Shi DX, Lee T, Maydeu-Olivares A. Understanding the model size effect on SEM fit indices. Educ Psychol Meas. (2019) 79:310–34. doi: 10.1177/0013164418783530
51. Mo PK, Lau JT, Wu X. Relationship between illness representations and mental health among HIV-positive men who have sex with men. AIDS Care. (2018) 30:1246–51. doi: 10.1080/09540121.2018.1445825
52. Dolengevich-Segal H, Gonzalez-Baeza A, Valencia J, Valencia-Ortega E, Cabello A, Tellez-Molina MJ, et al. Drug-related and psychopathological symptoms in HIV-positive men who have sex with men who inject drugs during sex (slamsex): data from the U-SEX GESIDA 9416 Study. PLoS ONE. (2019) 14:e0220272. doi: 10.1371/journal.pone.0220272
53. Durham MD, Armon C, Mahnken JD, Novak RM, Palella FJ Jr, et al. Rates of suicidal ideation among HIV-infected patients in care in the HIV Outpatient Study 2000-2017, USA. Prev Med. (2020) 134:106011. doi: 10.1016/j.ypmed.2020.106011
54. Miles-Johnson T, Wang YR. “Hidden identities': perceptions of sexual identity in Beijing. Br J Soc. (2018) 69:323–51. doi: 10.1111/1468-4446.12279
55. Xu WJ, Zheng LJ, Xu Y, Zheng Y. Internalized homophobia, mental health, sexual behaviors, and outness of gay/bisexual men from Southwest China. Int J Equity Health. (2017) 16:36–45. doi: 10.1186/s12939-017-0530-1
56. Mu HJ Li YX, Liu L, Na J, Yu LY Bi XJ, et al. Prevalence and risk factors for lifetime suicide ideation, plan and attempt in Chinese men who have sex with men. BMC Psychiatry. (2016) 16:117–26. doi: 10.1186/s12888-016-0830-9
57. Gebremariam EH, Reta MM, Nasir Z, Amdie FZ. Prevalence and associated factors of suicidal ideation and attempt among people living with HIV/AIDS at Zewditu Memorial Hospital, Addis Ababa, Ethiopia: A Cross-Sectional Study. Psychiatry J. (2017) 2017:2301524. doi: 10.1155/2017/2301524
58. Meyer IH. Minority stress and mental health in gay men. J Health Soc Behav. (1995) 36:38–56. doi: 10.2307/2137286
59. Marzuk PM, Hartwell N, Leon AC, Portera L. Executive functioning in depressed patients with suicidal ideation. Acta Psychiatr Scand. (2005) 112:294–301. doi: 10.1111/j.1600-0447.2005.00585.x
60. Myung W, Han CE, Fava M, Mischoulon D, Papakostas GI, Heo JY, et al. Reduced frontal-subcortical white matter connectivity in association with suicidal ideation in major depressive disorder. Transl Psychiatry. (2016) 7:e835. doi: 10.1038/tp.2016.110
61. Mann JJ, Arango VA, Avenevoli S, Brent DA, Champagne FA, Clayton P, et al. Candidate endophenotypes for genetic studies of suicidal behavior. Biol Psychiatry. (2009) 65:556–63. doi: 10.1016/j.biopsych.2008.11.021
62. Miyake A, Friedman NP, Emerson MJ, Witzki AH, Howerter A, Wager TD. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn Psychol. (2000) 41:49–100. doi: 10.1006/cogp.1999.0734
63. Nassar R, Kaczkurkin AN, Xia CH, Sotiras A, Pehlivanova M, Moore TM, et al. Gestational age is dimensionally associated with structural brain network abnormalities across development. Cereb Cortex. (2019) 29:2102–14. doi: 10.1093/cercor/bhy091
64. Marazziti D, Catena Dell'osso M, Conversano C, Consoli G, Vivarelli L, Mungai F, et al. Executive function abnormalities in pathological gamblers. Clin Pract Epidemiol Ment Health. (2008) 4:7. doi: 10.1186/1745-0179-4-7
65. Reid RC, Karim R, McCrory E, Carpenter BN. Self-reported differences on measures of executive function and hypersexual behavior in a patient and community sample of men. Int J Neurosci. (2010) 120:120–7. doi: 10.3109/00207450903165577
66. O'Connor RC, Nock MK. The psychology of suicidal behaviour. Lancet Psychiatry. (2014) 1:73–85. doi: 10.1016/S2215-0366(14)70222-6
67. Winter S. Lost in transition: health of transgender people in Asia Pacific. Lancet. (2012) 379:1924. doi: 10.1016/S0140-6736(12)60840-X
68. Cacioppo JT, Hawkey LC. Perceived social isolation and cognition. Trends Cogn Sci. (2009) 13:447–54. doi: 10.1016/j.tics.2009.06.005
69. Terpstra AR, Worthington C, Ibáñez-Carrasco F, O'Brien KK, Yamamoto A, Chan Carusone S, et al. I'm just forgetting and i don't know why: exploring how people living with HIV-associated neurocognitive disorder view, manage, and obtain support for their cognitive difficulties. Qual Health Res. (2018) 28:859–72. doi: 10.1177/1049732318761364
70. Hallard RI, Wells A, Aadahl V, Emsley R, Pratt D. Metacognition, rumination and suicidal ideation: an experience sampling test of the self-regulatory executive function model. Psychiatry Res. (2021) 303:114083. doi: 10.1016/j.psychres.2021.114083
71. Bredemeier K, Miller IW. Executive function and suicidality: a systematic qualitative review. Clin Psychol Rev. (2015) 40:170–83. doi: 10.1016/j.cpr.2015.06.005
72. Yatirajula SK, Kallakuri S, Paslawar S, Mukherjee A, Bhattacharya A, Chatterjee S, et al. An intervention to reduce stigma and improve management of depression, risk of suicide/self-harm and other significant emotional or medically unexplained complaints among adolescents living in urban slums: protocol for the ARTEMIS project. Trials. (2022) 23:612. doi: 10.1186/s13063-022-06539-8
73. Baldofski S, Kohls E, Bauer S, Becker K, Bilic S, Eschenbeck H, et al. Efficacy and cost-effectiveness of two online interventions for children and adolescents at risk for depression (Emotion trial): study protocol for a randomized controlled trial within the ProHEAD consortium. Trials. (2019) 20:53. doi: 10.1186/s13063-018-3156-8
74. Allom V, Mullan B, Smith E, Hay P, Raman J. Breaking bad habits by improving executive function in individuals with obesity. BMC Public Health. (2018) 18:505. doi: 10.1186/s12889-018-5392-y
Keywords: men who have sex with men, HIV, self-injury or suicidal ideation, self-stigma, executive function
Citation: Li Y, Xiao X, Zhou Y, Su X and Wang H (2023) The mediating role of executive function in the relationship between self-stigma and self-injury or suicidal ideation among men who have sex with men living with HIV. Front. Public Health 10:1066781. doi: 10.3389/fpubh.2022.1066781
Received: 11 October 2022; Accepted: 19 December 2022;
Published: 09 January 2023.
Edited by:
Jinghua Li, Sun Yat-sen University, ChinaReviewed by:
Yong Cai, Shanghai Jiao Tong University, ChinaCopyright © 2023 Li, Xiao, Zhou, Su and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xueling Xiao,  eHVlbGluZ3hpYW85M0Bob3RtYWlsLmNvbQ==
eHVlbGluZ3hpYW85M0Bob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.