
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 12 January 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1064408
This article is part of the Research Topic Contemporary Strategies: Advancing Healthcare for HIV, STIs, and Beyond View all 14 articles
 Esha Abraham1,2
Esha Abraham1,2 Eric P. F. Chow1,2,3
Eric P. F. Chow1,2,3 Christopher K. Fairley1,2David Lee2
Christopher K. Fairley1,2David Lee2 Fabian Y. S. Kong3
Fabian Y. S. Kong3 Limin Mao4Jane L. Goller3Nicholas Medland5
Limin Mao4Jane L. Goller3Nicholas Medland5 Benjamin R. Bavinton5
Benjamin R. Bavinton5 Budiadi Sudarto1Stefan Joksic6Jessica Wong6
Budiadi Sudarto1Stefan Joksic6Jessica Wong6 Tiffany R. Phillips1,2†
Tiffany R. Phillips1,2† Jason J. Ong1,2,7*†
Jason J. Ong1,2,7*†Objectives: Gay, bisexual and other men who have sex with men (GBMSM) and trans and gender diverse (TGD) people are disproportionately affected by poorer sexual health outcomes compared to heterosexual populations. We aimed to explore the preferences of GBMSM and TGD for using eHealth for sexual health (eSexualHealth).
Methods: We distributed an anonymous online survey from April to August 2021among the lesbian, gay, bisexual, transgender, intersex, queer and other people of diverse sexuality or gender (LGBTIQA+) community in Australia. The survey collected data on sociodemographic characteristics and sexual behaviors, their preferences for app/website functions and preferred HIV and sexually transmitted infection (STI) testing reminders. We used descriptive statistics to summarize the characteristics of the study population. Free-text responses were thematically analyzed.
Results: Of 466 participants included, most identified as cisgender males (92.7%). The median age was 48 [interquartile range (IQR): 37–56]. For accessing sexual health-related information, 160 (34.6%) would use either a website or an app, 165 (32.7%) would prefer a website, 119 (25.8%) would prefer an app, and 33 (7.1%) would not use either platform. There was no significant difference between GBMSM and TGD people. Participants were most interested in information about STI clinics, HIV/STI hotspots, and sexual health education. Participants stressed the need for privacy and anonymity when using eHealth. Regarding reminders to test for HIV/STIs, receiving regular SMS was most popular (112/293, 38.2%), followed by regular emails (55/293 18.8%) and a reminder function on their phone (48/293, 16.4%).
Conclusion: Our study suggests a promising future for eHealth among GBMSM and TGD people. Sexual health is still a stigmatized area, and eHealth may circumvent barriers this population faces.
While HIV notification rates have decreased in Australia in recent years, gay and bisexual men who have sex with men (GBMSM) continue to be disproportionally affected compared to their heterosexual counterparts (1). Furthermore, STI incidence rates are higher among GBMSM living with HIV than among HIV-negative GBMSM (2). A 2018 survey of trans and gender diverse (TGD) people found that more than half believed they received poor sexual health education during their school years. Additionally, 51.2% reported receiving insensitive sexual health care. Most participants (65%) also reported inconsistent condom use with casual sexual partners. Combined with their poor experiences in sexual health care, it increases their risk for HIV/STIs (3). As a result, greater effort needs to be put into educating and facilitating HIV/STI testing among GBMSM and TGD people.
GBMSM and TGD people can face several barriers when accessing healthcare, such as: experiencing stigma due to their sexuality, a lack of knowledge and culturally appropriate training amongst healthcare providers; and personal concerns around disclosing their sexual identity (4–6). Specialized sexual healthcare is scarce in Australia, and patients can face long waiting times or high costs if they need to access these services through a general practitioner or private clinic (7). Digital health interventions, also known as eHealth, can improve healthcare access among LGBTIQA+ people (8). These can be delivered through mobile devices, laptops, websites (e.g., acon.org.au and transhub.org.au, or smartphone apps, and can provide private, personalized content that is easily accessible (9). However, to be successful, input from the target audience is essential in creating an intervention that addresses their needs and, in turn, results in increased uptake (10, 11). Previous studies have determined that there is a promising future for an eHealth app among GBMSM (12). However, few studies have investigated the preferences and types of features for different platforms.
This study sought to understand the features of a website or smartphone app that GBMSM and TGD people prefer to access information related to sexual health. We also aimed to measure whether GBMSM and TGD people currently use eHealth for reminding themselves to test for HIV/STIs.
This was an anonymous online survey distributed among the LGBTIQA+ community in Australia. We included all respondents aged 16 years and above who identified as LGBTQIA+. Completion of the survey was taken as implied consent. The online survey link was disseminated through the authors' professional networks, social media, and clients at Melbourne Sexual Health Centre (MSHC), a public sexual health clinic in Australia. This included a short messaging service (SMS) or email from MSHC (if they had previously consented to receive them), a dating app (Grindr), and LGBTIQA+ community groups. These community groups included Equinox, Your Community Health, Switchboard, Minus18, QLife, and Rainbow Health Victoria. The survey was run from 10 April 2021 to 3 August 2021. Given that most respondents identified as GBMSM or TGD, the decision was made to limit the analysis to only include these respondents.
The survey instrument was developed by the researcher team which included clinicians, sexual health researchers and community members. A pilot test was conducted among ten individuals who were part of the target population to check the comprehensibility and feasibility of the survey (data was not included in the final analysis). This resulted in minor edits to how questions were phrased. The survey was accessed through an online link (hosted by Qualtrics). The survey collected data on sociodemographic characteristics and sexual practices. Respondents were provided with a list of app/website functions and asked to rate how useful each function would be using a five-point Likert scale. Participants were also asked about current and preferred HIV/STI testing reminders and were able to rank their top three answers. Participants were not required to answer all questions and could rank less than three options if desired. Free text response to the questions: “If you could design an app, website, or health service for LGBTIQA+ people that would make it easier to get tested for HIV/STIs? What would it do? Feel free to be creative–all answers and ideas are welcome!” this allowed participants to expand on any features they intervention.
We cleaned the data and used descriptive statistics to summarize the characteristics of the study population, using Stata (version 17, StataCorp, College Station, TX). Differences between GBMSM and TGD were assessed using Chi-squared test. Statistical significance was defined as a p-value of <0.05. The free-text responses were thematically analyzed using NVivo (Release 1.6, QSR International Pty Ltd., Melbourne, Australia).
Ethics approval was granted by the Alfred Ethics Committee (670/20), including allowing respondents from age 16 onwards to participate. There was no financial reimbursement for survey completion.
The survey was accessed 727 times during the study period, and 704 people consented to participate of whom 513 (72.9%) completed the survey. There were 47 (9.2%) participants who did not identify as GBMSM or TGD and were excluded, leaving a total of 466 participants for the analysis. Most were recruited through an SMS or email from MSHC (306/466, 65.7%), followed by Grindr (93/466, 20.0%), then community groups (41/466, 8.8%).
Table 1 summarizes the sociodemographic characteristics of the study population. Of the 466 participants, the majority identified as cisgender males (92.7%). The median age was 48 [interquartile range (IQR): 37–56] and three-quarters were born in Australia. There were 98 (21.2%) of participants living with HIV and had an undetectable viral load. Among those not living with HIV, 139 (37.8%) reported PrEP use.
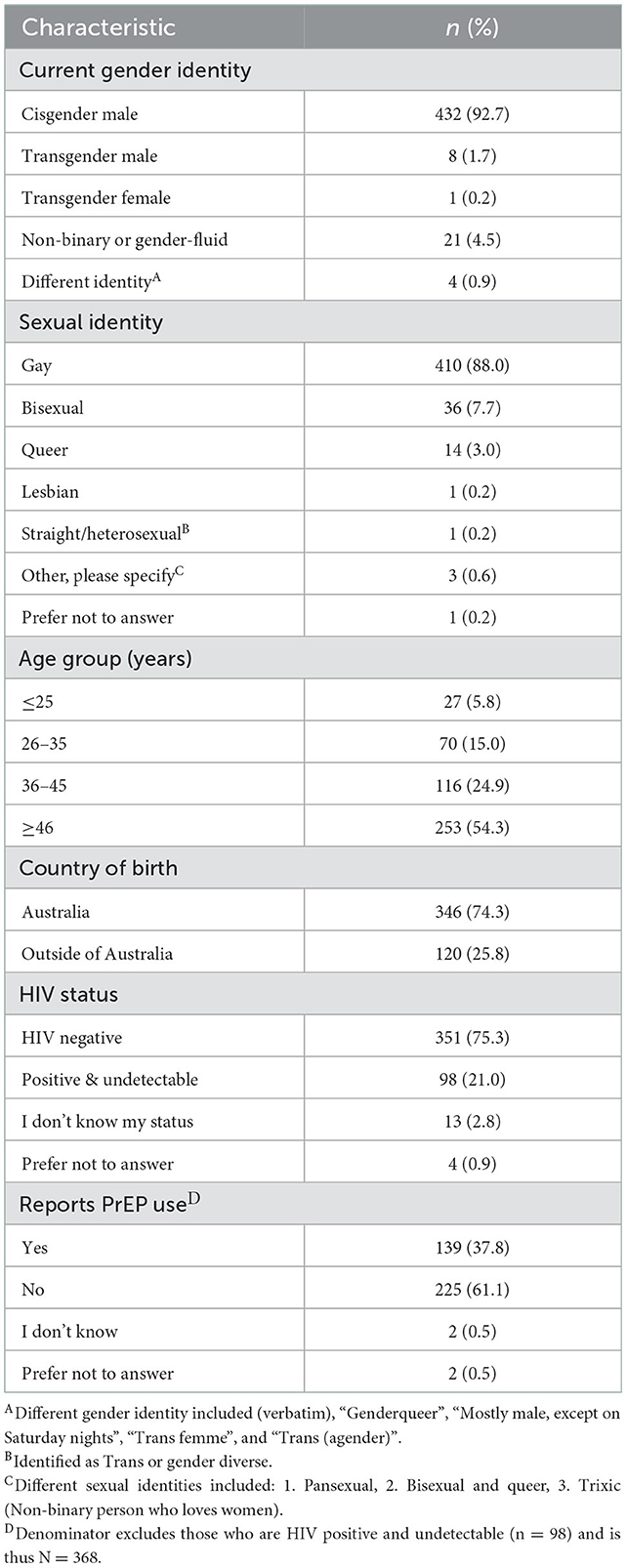
Table 1. Sociodemographic characteristics of the study population (N = 466).
Overall, there was no clear preference for an app or website-based sexual health platform. Of the 462 participants that answered the question, 160 (34.6%) would use either a website or an app, 165 (32.7%) would prefer a website, 119 (25.8%) would prefer an app, and 33 (7.1%) would not use either platform. There was no significant difference between GBMSM and TGD people (Supplementary Table S1). Figures 1, 2 provide the preferences for functions on an app and web-based platform, respectively. Supplementary Figures S1–S4 separates out preferences of GBMSM and TGD, and found that GBMSM were more likely to priorities information about pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP) (Supplementary Figures S1–S4).
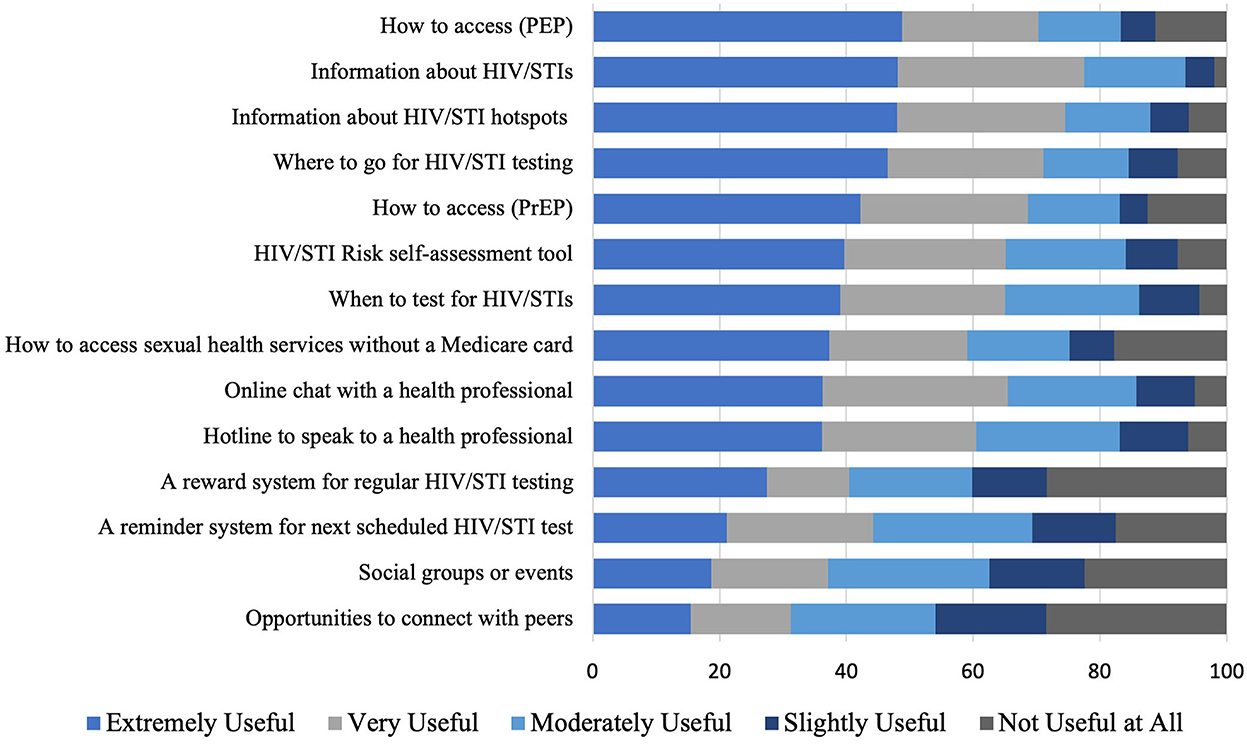
Figure 1. Preferences for functions on an app-based platform among GBMSM and TGD.
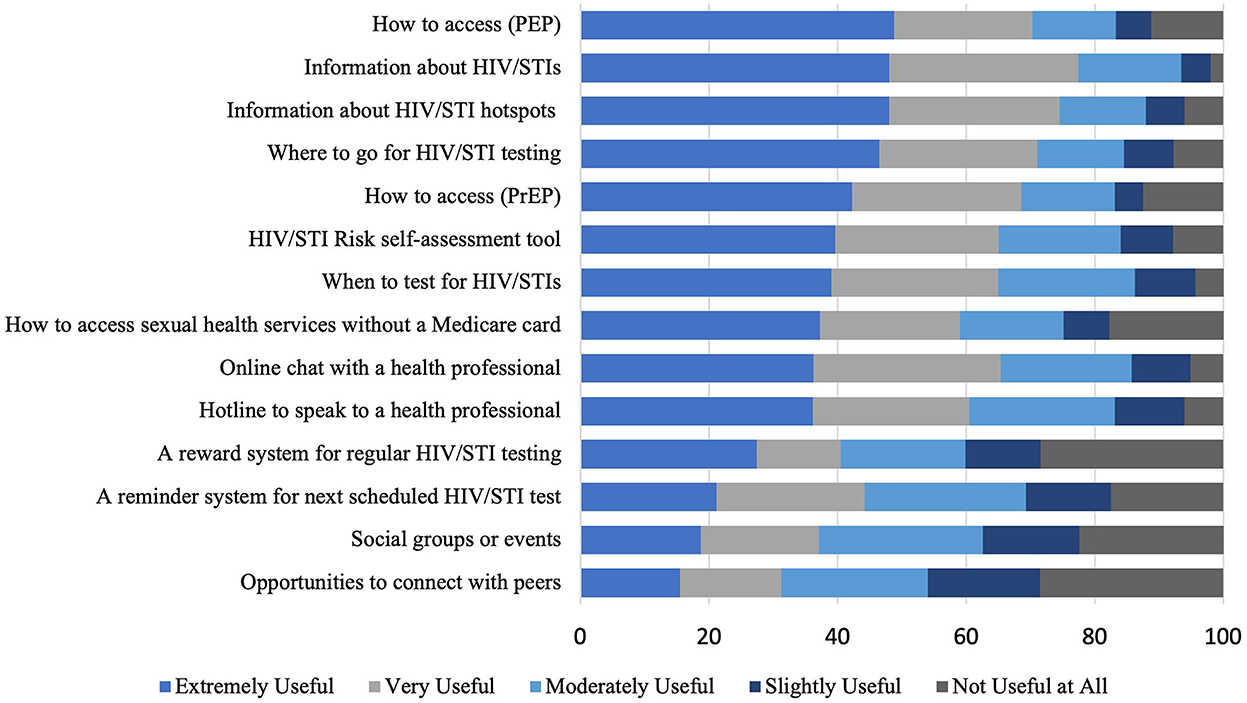
Figure 2. Preferences for functions on a web-based platform among GBMSM and TGD.
In the free-text response, there was a strong emphasis on the need for information, particularly about STI clinics, HIV/STI hotspots (geographical areas with high levels of STI diagnoses), and sexual health education. Concerning STI clinics, most respondents wanted information on their location, opening hours, contact details, and the cost of the services. Other themes that emerged included the need for anonymity, accessibility, and a simple user interface. A few participants also highlighted that they would want a discreet app. Most participants were interested in features such as a sexual activity tracker (i.e., an online diary that recorded sexual encounters), a daily PrEP reminder system, and an HIV/STI testing reminder system. Some participants suggested introducing an online booking system for clinics, which would allow them to book an appointment in advance.
Over a third of respondents would prefer regular SMS reminders (112/293, 38.2%), followed by regular email reminders (55/293, 18.8%) and a reminder function on their phone (48/293, 16.4%) (Figure 3). Testing reminder preferences were similar between GBMSM and TGD people (Supplementary Figures S5–S6).
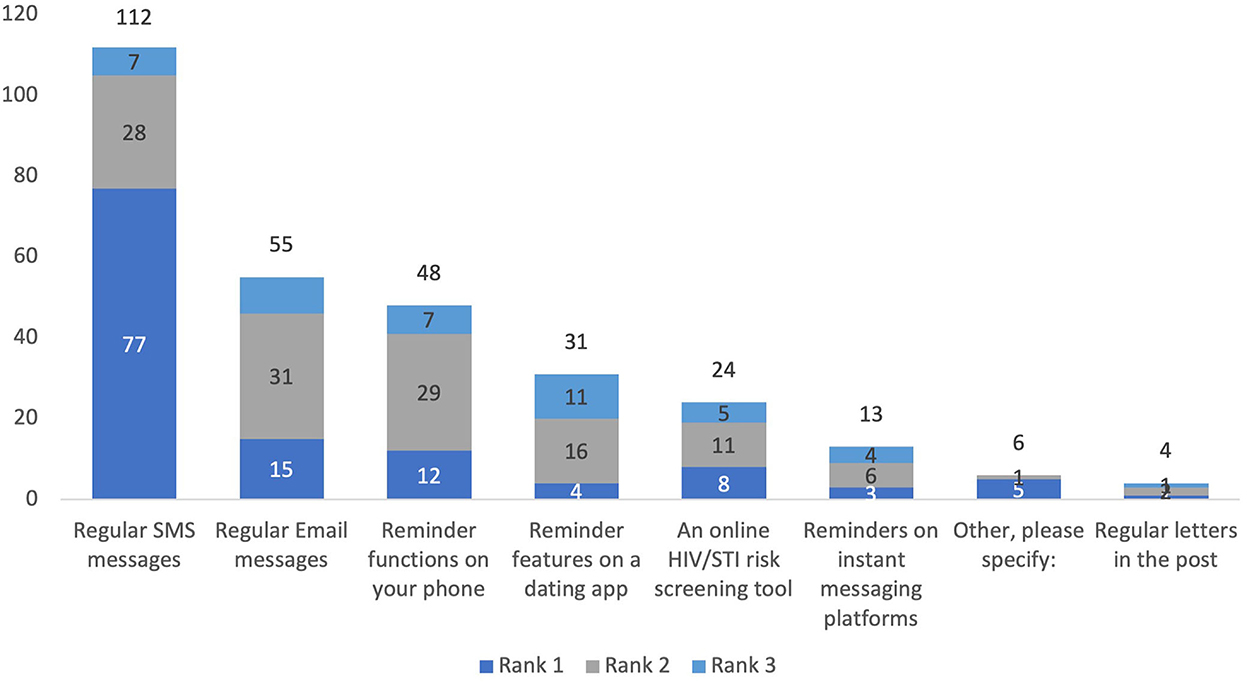
Figure 3. Preferred HIV/STI testing reminder system on an eHealth platform, stratified by rank.
This study provided insights into how GBMSM and TGD people viewed the use of eHealth for sexual health. Specifically, we identified what features may be desirable for a new eHealth intervention, providing useful information for future implementation research to optimize the use of eHealth among GBMSM and TGD. Participants highlighted their desire for privacy and sexual health information. Furthermore, we found that GBMSM were more likely to priorities wanting information about PrEP and PEP in comparison to TGD people.
The use of eHealth is a relatively new concept, and international data suggests that this has been accepted elsewhere. A study among 495 GBMSM from the USA found that 91% would be interested in an app with sexual health features tailored to GBMSM (12). A 2015 study using qualitative interviews of 35 MSM in China found that they supported the use of mobile phones and websites for sexual health (13). Most participants agreed that this provided a level of convenience, and provided information about testing services. Similarly, Nguyen et al. conducted five focus group discussions among MSM in Vietnam. The majority of participants were agreeable to eHealth. They also requested similar content to our participants, such as information about HIV/STIs and testing, and safe sex practice (14). The dissemination of sexual health information through social media and dating apps was acceptable to GBMSM in England, however, some participants felt that receiving this information on dating apps could negatively impact user experience (15). These participants felt that it may dampen the mood when searching for sexual partners, and create negative connotations with new partners.
Ensuring privacy when accessing the services was a prominent theme. It is unclear whether these concerns were due to the stigma surrounding sexual health or whether they resulted from a previous negative experience. Muessig et al. also reported concerns about privacy and confidentiality when accessing eHealth for sexual health (13). Another study found that the use of eHealth would depend on the privacy policy for most participants in the study (16). As a result, they may feel that they need to attend a specialist clinic to meet their healthcare needs. However, this can be difficult to access, and these barriers can discourage GBMSM and TGD people from seeking traditional sexual health services such as face-to-face consultations with health care professionals (17). eHealth could address these barriers by offering privacy and easy access to sexual health services, however more empirical data is required to assess its feasibility. These eHealth interventions can be delivered through computers, websites, and personal devices and can deliver content tailored to an individual's needs. In turn, these address barriers to health care access like cost and accessibility (18). This was a major concern for respondents, and our findings suggest that future eHealth interventions should priorities anonymity to ensure uptake and continued use of the services.
SMS for HIV/STI testing reminders was the most popular choice among respondents in our survey. Several studies have already evaluated the use of an SMS reminder system on HIV/STI testing. A minority of participants from our study indicated that they would prefer an email reminder, however, this has not been evaluated previously. A 2013 study conducted by Zou et al. at MSHC found that GBMSM who received quarterly STI testing reminders by text or email were more likely to return for a test (median 3 vs. 1 test in 12 months) than controls (19). However, this study did not stratify results by the modality used. A 2011 study looking at STI testing rates among Australian GBMSM found that those who received 3 to 6-monthly SMS reminders were 4.4 times more likely to retest for HIV/STIs than those who did not receive a text (20). Similarly, a 2019 USA study reported that men who received a quarterly SMS testing reminder had a shorter interval between HIV tests than men who did not receive a text (21). SMS reminders are a feasible intervention that is relatively affordable and can help increase STI testing rates and has a lower burden on the health system than phone calls or other in-person interventions. Second, mobile technology is almost universally used and can effectively reach a wider population. A 2020 meta-analysis found that there were high levels of feasibility for mHealth tailored to GBMSM. However, most studies reviewed were pilot trials, and it is unclear whether these mHealth interventions would be successful on a larger scale (22).
Our study has several limitations. First, this is a cross-sectional study, and thus we cannot make causal inferences. Secondly, our study only recruited through one gay dating app (Grindr) but no other mainstream apps, such as Tinder, Bumble, and Hinge. This may have skewed the results, and as a result, we only included GBMSM and TGD people in the analysis; thus, our findings are not generalizable to other members of the LGBTIQA+ population. Relatedly, the median age of our study population was 48 years old and therefore, our reported preferences may differ among younger GBMSM and TGD. To make any future intervention successful, it will require further collaboration between developers and a more representative sample of the population. Third, our sample was mostly derived from men who had recently attended a sexual health service. These individuals would therefore be biased toward individuals who are comfortable attending services and so our estimates are likely to underestimate preferences for eHealth services. Future studies should seek the views of individuals who are at risk but not attending services although we appreciate undertaking such a study is difficult. Fourth, whilst Qualtrics records IP addresses to identify duplicates, it is possible, though unlikely, that the same person could submit multiple surveys from different devices. Finally, HIV/STI-related stigma, potentially influencing perceived engagement with digital platforms and data security, was not measured.
Overall, our study suggests a promising future for eHealth among GBMSM and TGD people. Sexual health is still a stigmatized area, and eHealth may circumvent barriers this population faces. Further research that provides in-depth data on the themes raised in this study is required to ensure the acceptability and feasibility of any future interventions. Specifically, confidentiality and options to remain anonymous should be considered in future developments of eHealth for sexual health.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Alfred Ethics Committee. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JO conceived the idea. EC, DL, FK, LM, JG, BB, BS, SJ, and JW assisted with recruitment. EA and TP analyzed the data. EA wrote the first draft of the paper. Community members as part of the target population were involved in the design, conduct, reporting, and dissemination plans of our research. All authors contributed to writing the manuscript and approved the final version for submission.
EC and JO were each supported by an Australian National Health and Medical Research Council Emerging Leadership Investigator Grants (GNT1172873 and GNT1193955, respectively). CF was supported by an Australian NHMRC Leadership Investigator Grant (GNT1172900).
We thank the survey participants for contributing to the research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1064408/full#supplementary-material
1. Kirby Institute. Nation HIV Notification Q1 2016 - Q4 2020. Sydney: University of New South Wales (2020).
2. Kirby Institute. National Update on HIV, Viral Hepatitis and Sexually Transmissible Infections in Australia: 2009–2018. Kensington, NSW: The Kirby Institute, UNSW Sydney (2020).
3. Callander D, Wiggins J, Rosenberg S, Cornelisse V, Duck-Chong E, Holt M, et al. The 2018 Australian Trans and Gender Diverse Sexual Health Survey: Report of Findings. Kensington, NSW: Syd NSW Kirby Inst UNSW Syd (2019).
4. Brown A, Rice SM, Rickwood DJ, Parker AG. Systematic review of barriers and facilitators to accessing and engaging with mental health care among at-risk young people. Asia-Pacific Psychiatry. (2016) 8:3–22. doi: 10.1111/appy.12199
5. Sanchez NF, Sanchez JP, Danoff A. Health care utilization, barriers to care, and hormone usage among male-to-female transgender persons in New York City. Am J Public Health. (2009) 99:713–9. doi: 10.2105/AJPH.2007.132035
6. Bien-Gund CH, Zhao P, Cao B, Tang W, Ong JJ, Baral SD, et al. Providing competent, comprehensive and inclusive sexual health services for men who have sex with men in low- and middle-income countries: a scoping review. Sex Health. (2019) 16:320–31. doi: 10.1071/SH18191
7. Conway DP, Holt M, Couldwell DL, Smith DE, Davies SC, McNulty A, et al. Barriers to HIV testing and characteristics associated with never testing among gay and bisexual men attending sexual health clinics in Sydney. J Int AIDS Soc. (2015) 18:20221. doi: 10.7448/IAS.18.1.20221
8. Minichiello V, Rahman S, Dune T, Scott J, Dowsett G. E-health: potential benefits and challenges in providing and accessing sexual health services. BMC Public Health. (2013) 13:1–7. doi: 10.1186/1471-2458-13-790
9. Sun CJ, Anderson KM, Mayer L, Kuhn T, Klein CH. Findings from Formative Research to Develop a Strength-Based HIV Prevention and Sexual Health Promotion mHealth Intervention for Transgender Women. Transgend Health. (2019) 4:350–8. doi: 10.1089/trgh.2019.0032
10. McCurdie T, Taneva S, Casselman M, Yeung M, McDaniel C, Ho W, et al. mHealth consumer apps: the case for user-centered design. Biomed Instrum Technol. (2012) 46:49. doi: 10.2345/0899-8205-46.s2.49
11. Yardley L, Spring BJ, Riper H, Morrison LG, Crane DH, Curtis K, et al. Understanding and promoting effective engagement with digital behavior change interventions. Am J Prev Med. (2016) 51:833–42. doi: 10.1016/j.amepre.2016.06.015
12. Ventuneac A, John SA, Whitfield TH, Mustanski B, Parsons JT. Preferences for sexual health smartphone app features among gay and bisexual men. AIDS Behav. (2018) 22:3384–94. doi: 10.1007/s10461-018-2171-9
13. Muessig KE, Bien CH, Wei C, Lo EJ, Yang M, Tucker JD, et al. A mixed-methods study on the acceptability of using eHealth for HIV prevention and sexual health care among men who have sex with men in China. J Med Internet Res. (2015) 17:e100. doi: 10.2196/jmir.3370
14. Nguyen LH, Nguyen HLT, Larsson M, Tran BXL, Stein M, Rocha LEC, et al. An exploratory assessment of the preference for eHealth interventions to prevent HIV and sexually transmitted infections among men who have sex with men in Hanoi, Vietnam. BMC Public Health. (2020) 20:1387. doi: 10.1186/s12889-020-09449-z
15. Kesten JM, Dias K, Burns F, Crook P, Howarth A, Mercer CH, et al. Acceptability and potential impact of delivering sexual health promotion information through social media and dating apps to MSM in England: a qualitative study. BMC Public Health. (2019) 19:1236. doi: 10.1186/s12889-019-7558-7
16. Goldman J, Hudson Z. Perspective: virtually exposed: privacy and e-health. Health Aff. (2000) 19:140–8. doi: 10.1377/hlthaff.19.6.140
17. Scheim AI, Travers R. Barriers and facilitators to HIV and sexually transmitted infections testing for gay, bisexual, and other transgender men who have sex with men. AIDS Care. (2017) 29:990–5. doi: 10.1080/09540121.2016.1271937
18. Shrestha R, Lim SH, Altice FL, Copenhaver M, Wickersham JA, Saifi R, et al. Use of smartphone to seek sexual health information online among Malaysian men who have sex with men (MSM): implications for mHealth intervention to increase HIV testing and reduce HIV risks. J Community Health. (2020) 45:10–9. doi: 10.1007/s10900-019-00713-x
19. Zou H, Fairley CK, Guy R, Bilardi J, Bradshaw CS, Garland SM, et al. Automated, computer generated reminders and increased detection of gonorrhoea, chlamydia and syphilis in men who have sex with men. PLoS ONE. (2013) 8:e61972-e. doi: 10.1371/journal.pone.0061972
20. Bourne C, Knight V, Guy R, Wand H, Lu H, McNulty A. Short message service reminder intervention doubles sexually transmitted infection/HIV re-testing rates among men who have sex with men. Sex Transm Infect. (2011) 87:229–31. doi: 10.1136/sti.2010.048397
21. Ronen K, Golden MR, Dombrowski JC, Kerani RP, Bell TR, Katz DA. Uptake and impact of short message service reminders via STI partner services on HIV/STI testing frequency among men who have sex with men. Sex Transm Dis. (2019).
Keywords: lesbian, gay, bisexual and transgender (LGBT) issues, sexual health, sexually transmitted infections, eHealth (mobile health), mHealth (mobile health)
Citation: Abraham E, Chow EPF, Fairley CK, Lee D, Kong FYS, Mao L, Goller JL, Medland N, Bavinton BR, Sudarto B, Joksic S, Wong J, Phillips TR and Ong JJ (2023) eSexualHealth: Preferences to use technology to promote sexual health among men who have sex with men and trans and gender diverse people. Front. Public Health 10:1064408. doi: 10.3389/fpubh.2022.1064408
Received: 08 October 2022; Accepted: 19 December 2022;
Published: 12 January 2023.
Edited by:
Vinodh Aroon Edward, Aurum Institute, South AfricaReviewed by:
Marie-Pierre Gagnon, Laval University, CanadaCopyright © 2023 Abraham, Chow, Fairley, Lee, Kong, Mao, Goller, Medland, Bavinton, Sudarto, Joksic, Wong, Phillips and Ong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jason J. Ong,  amFzb24ub25nQG1vbmFzaC5lZHU=
amFzb24ub25nQG1vbmFzaC5lZHU=
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.