
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 09 January 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1062199
 Xiaohang Chen1†
Xiaohang Chen1† Pan Zhang2†Ruhan Zhang3Shuting Li4Rui Cao5Fen Hu5,6Ying-Hui Jin7
Pan Zhang2†Ruhan Zhang3Shuting Li4Rui Cao5Fen Hu5,6Ying-Hui Jin7 Likai Lin8
Likai Lin8 Lin Cai9Bilong Feng5,6*Chunhua Zhang5*
Lin Cai9Bilong Feng5,6*Chunhua Zhang5* Xinghuan Wang7,10,11*
Xinghuan Wang7,10,11*Purpose: This study aimed to develop and test the validity and reliability of the Knowledge, Attitudes, Practise, and Experience regarding Infection Prevention and Control-associated Questionnaire for environmental service workers.
Design: This study was a development and validation study of a questionnaire using multiple methods, including literature review, questionnaire survey, and Delphi technique.
Methods: Phase I of the study entailed the development of items through an extensive literature review and two round Delphi process with 15 experts specialised in infection prevention and control, environmental service worker management, or scale construction to examine the content validity of the questionnaire. Phase II involved administering the questionnaire to a convenience sample of 1,176 environmental service workers from the public hospital from 13 provinces in China to evaluate its construct validity and reliability.
Findings: In the two rounds of Delphi consultation, the recovery rate were 93.75 and 100%. Moreover, the expert authority coefficient was 0.93, and the coordination coefficients of expert opinions in the first round were as follows: correlation of 0.204 and importance of 0.249 for the first-level index; correlation of 0.128 and importance of 0.142 for the secondary index. In round two, the coordination coefficients of expert opinions were as follows: correlation of 0.221 and importance of 0.221 for the first-level indicators; correlation of 0.096 and importance of 0.101 for the secondary index. The results for the index were P < 0.05 for the two rounds. The pilot survey shows the instrument was excellent content validity (S-CVI/Ave = 0.989). The overall internal consistency was excellent (Cronbach's α = 0.967). The questionnaire ultimately comprised four first-level indices (knowledge, attitudes, practise, and experience) and 49 second-level indices.
Conclusion: The Questionnaire demonstrated good reliability and validity and is effective in measuring levels of infection prevention and control-related knowledge, attitudes, practise, and experience among environmental service workers. It will provide a tool for future national investigations of the current infection prevention and control situation among environmental service workers. Future research should explore determinants of environmental service workers' knowledge, attitudes, practise, and experience and associations between infection prevention and control knowledge, attitudes, practises, and experience.
Health care-acquired infections (HAIs)1 are a serious global public health issue, affecting millions of patients worldwide every year (1). The burden of HAIs needs to be highlighted not only because of the large number of patients affected every year but also for their significant impact in terms of excess costs, prolonged hospital stay-attributable mortality, and other complications (2). An estimated 15% of patients globally develop one or more infections during a hospital stay, with the greatest risk in low-income countries (3). In Europe alone, HAIs cause 16 million extra days of hospital stay and 37,000 attributable deaths and contribute to an additional 110,000, almost 9 million deaths are recorded every year (4). Pathogens linked with HAIs can not only cause disease but also survive in the hospital environment for weeks. More evidence suggests that the hospital environment should be cleaned and disinfected to prevent pathogen cross-transmission and remove infectious agents from fomites in the health care environment (5–7).
With the ongoing COVID-19 pandemic (8), strengthening infection prevention and control (IPC)2 was endorsed to reduce HAIs and prevent and control outbreaks by the World Health Organisation (WHO) (9).3 Over the last few years, the important role of hospital environment cleaning and disinfection in IPC has become more apparent (10). Numerous studies have shown that environmental service workers (ESWs)4 are a weak link in IPC in hospitals (11–13). Meanwhile, ESWs play a central role in effective environmental cleaning and disinfection, the critical frontline of defence against HAIs (14). In the context of the COVID-19 pandemic, we urgently need to understand the current situation of ESWs regarding their knowledge, attitudes, practise, and experience of IPC.
However, through a literature review, we found that the ESW assessment scale mostly addresses knowledge, attitudes, and practises of routine cleaning and disinfection of ESWs. The results showed that ESWs lacked knowledge of environmental disinfection (15, 16). There was no standardised instrument to evaluate IPC among ESWs. Therefore, it was important to develop a scientific method to develop a valid and reliable instrument for measuring ESWs' IPC practises considering knowledge, attitudes, practises, and experience. Considering that COVID-19 poses a challenge to IPC, we added COVID-19 to the questionnaire, for example, how to deal with the medical waste generated by COVID-19 patients and how to arrange the room disinfection of COVID-19 patients. This study aimed to develop a Knowledge, Attitudes, Practise, and Experience regarding Infection Prevention and Control-associated Questionnaire (KAPE-IPC-Q)5 for Chinese ESWs using the application of the Delphi technique and a pilot survey. The study findings will provide a tool for future national investigations of the current IPC situation among ESWs.
Email invitations were sent to experts from all over China to participate on 15th August 2021 to discuss the final questionnaire.
Multidisciplinary teams were formed consisting of 12 members, including one methodological expert on tool building, one IPC manager, one research methodologist, two clinical medicine experts, three clinical nursing experts, and four IPC nurses.
A literature review, official documents, focus interviews, and team discussions selected the item pool for the questionnaire. (a) A literature review was conducted using the PubMed and ProQuest databases to define HAI, determine the risk factors and prevention measures, and establish a questionnaire item pool. (b) We searched websites, including the Chinese Centre for Disease Control (CDC) (6), Joint Commission International, WHO guidelines about IPC among health workers, and government documents (9, 17–20). (c) Focus interviews were conducted between the team members and 16 ESWs and their eight leaders. (d) Discussions among all team members after the literature review and the focus interviews were conducted; the team members classified the literature, policies, and interview information and removed the duplicate content to establish an item pool.
To ensure broad and varied expertise in the field of IPC and ESW management, CiteSpace V5.7.R2 was used to select potential experts (Figure 1). The potential experts were chosen by discussing and consulting the research field of interest over the past 3 years, and the experts building the panel are composed of the following characteristics: (1) own experience and expertise in IPC, ESWs management in a scientific or clinical context, scale development, or research personnel, (2) at least 10 years of relevant experience, (3) possession of a senior professional post, and (4) broad geographic spread (Table 1).
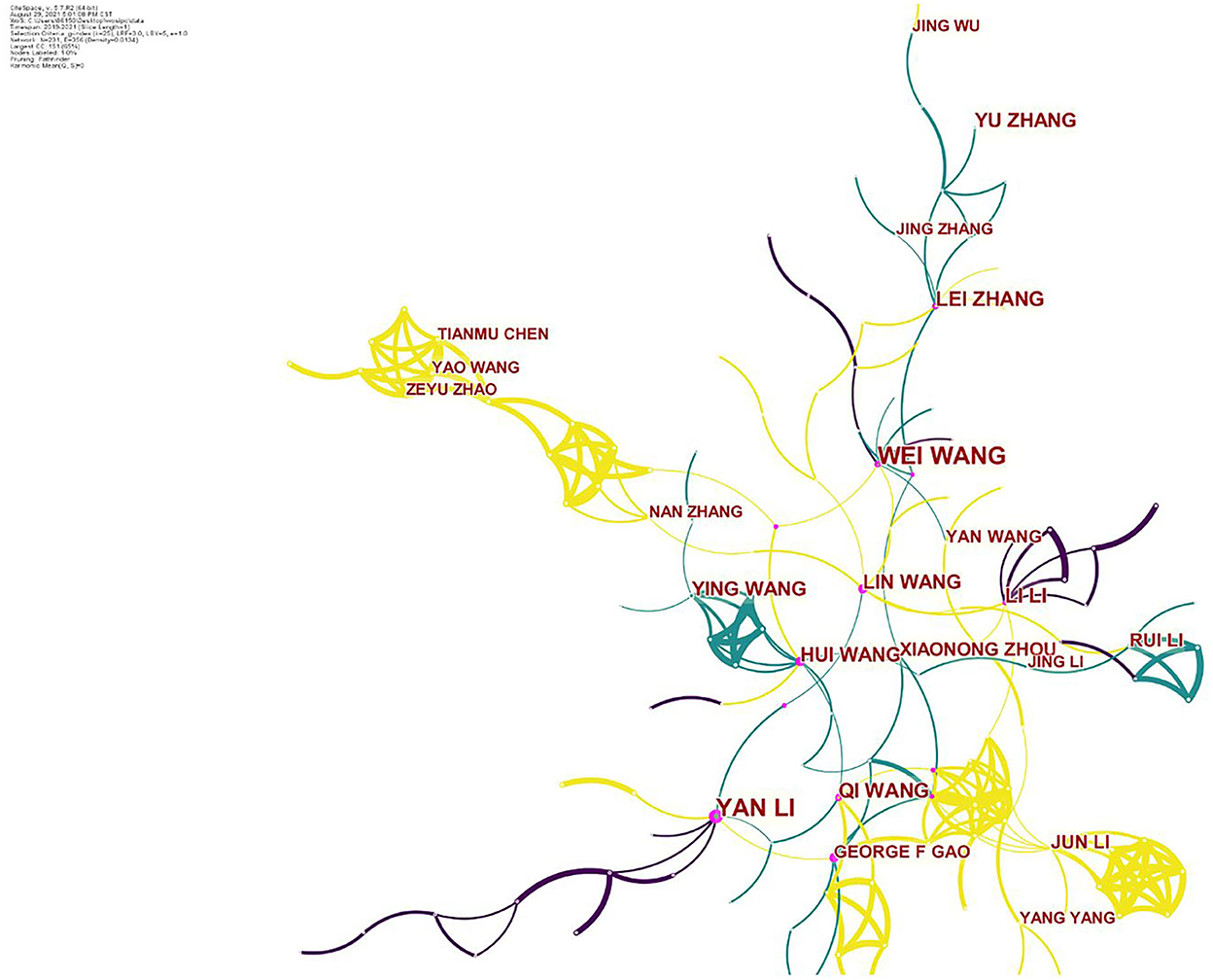
Figure 1. Expert selection.
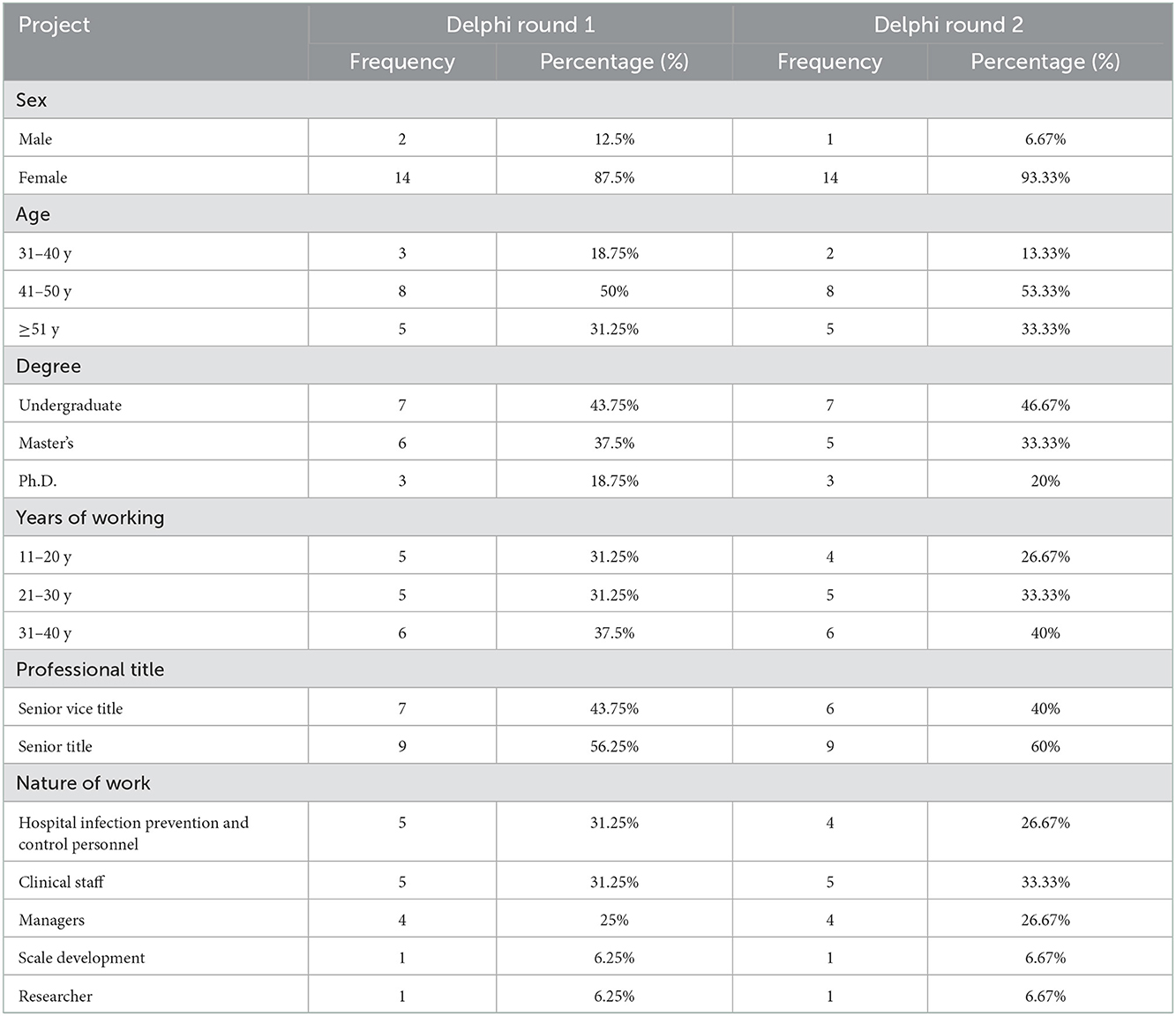
Table 1. Expert information.
Email invitations were sent to 16 experts from all over China to participate (from 10 major cities, including Beijing, Shanghai, Guangdong, Hubei, Jiangsu, Jiangxi, Sichuan, Hebei, Liaoning, and Shanxi). Upon acceptance, experts were included in the Delphi process to generate consensus but did not know the identity of the other participants. Participation was voluntary, and consent was implied if the participant responded to the survey. The Delphi questionnaire comprised two sections. The first section included the complete KAPE-IPC-Q with detailed descriptions of each subscale and item. Experts were asked to rate each item on a five-point Likert scale (1 = not important/not correlated, 5 = very important/correlated) with additional blanks to allow them to fill in revision comments. At the end of the questionnaire, experts could also provide opinions or suggestions for content that had not been included in the questionnaire. The second section asked for experts' personal information (i.e., age, professional title, occupation, and education level).
The pilot survey was performed with a convenience sample of ESWs at the public hospital from 13 provinces in China. The inclusion criteria were ESWs employed by hospitals. They were asked to provide their comments about problems in completing the questionnaire, including whether it was clear and understandable and whether the content was relevant to their practise, and we recorded the time spent filling out the questionnaire.
The questionnaire comprised two sections. The first section assessed sociodemographic variables (i.e., age, education level, marital status, and income), the second section comprised KAPE-IPC-Q items. Each item was rated on a three—or five-point Likert scale, and there were eight reverse scoring questions in this questionnaire, with higher total scores representing greater knowledge, attitudes, practise, and experience regarding IPC. Given that the KAPE-IPC-Q is self-reported, ESWs who could read and write completed the questionnaire by themselves; however, ESWs who struggled with reading and writing received the interviewer-administered survey, and their responses were recorded by the interviewer verbatim (Figure 2).
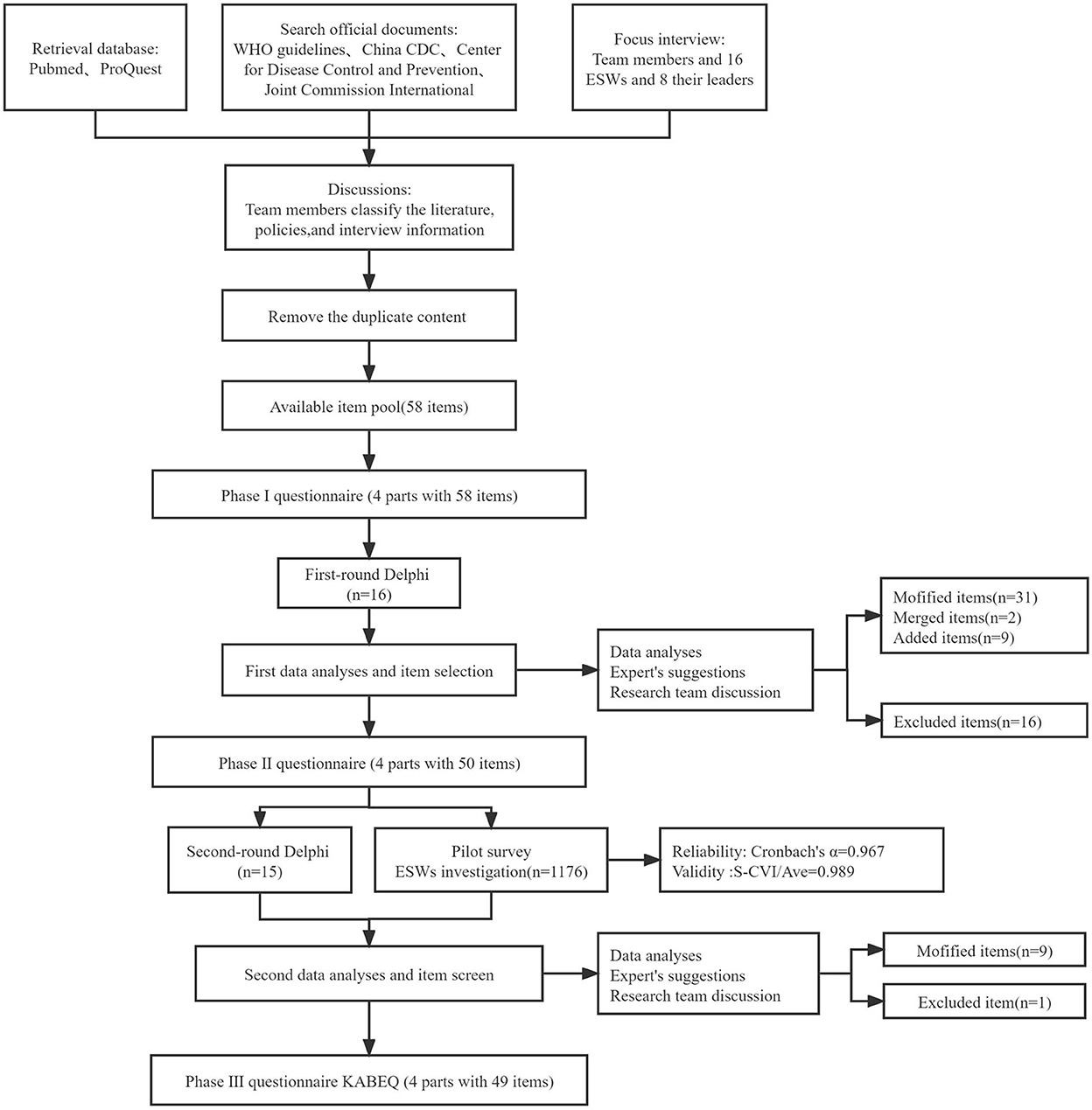
Figure 2. Flow chart of the development questionnaire.
In each Delphi round, experts were asked to rate each statement according to its importance and correlation to the questionnaire using a five-point Likert scale. Moreover, they were invited to comment on each item. Questionnaire item data are presented as the mean, standard deviation (SD), coefficient of variation (CV), and Kendall W. The larger the mean, the more important the index, and vice versa; the larger the CV, the greater the difference in the experts' understanding of the content of the questionnaire, and the lower the consistency of their opinions. Kendall's W-test was used to confirm the relevance of the experts' responses for all items (21). The higher the Kendall W-value, the higher the level of agreement among the members of the expert panel. The authority coefficient (Cr) is used to evaluate the degree of authority of experts, which is related to the technical ability of evaluation indicators and is determined by the familiarity and the mean value of the judgement basis (22).
According to the results of the Delphi process, the item importance average score ≥ 3.5 points or the coefficient of variation ≤ 0.25 was used as the screening criteria (23), and the items were screened after the experts' revision opinions and reviewed after repeated discussions among the research team members.
Using these data, we performed further item selection and revision through analyses of the internal consistency (Cronbach's α), and a Cronbach's α of ≥0.70 was considered to indicate acceptable reliability (24). Content validity reflects the consistency between the content measured by the questionnaire and the content to be measured. The S-CVI/Ave value is used to express content validity. At present, the most commonly used evaluation index of content validity is the S-CVI/Ave. When the S-CVI/Ave > 0.90, the content validity of the questionnaire is good (25).
A database was constructed using EpiData version 3.5.2 and all data were double-entered by two data managers to avoid any possible data entry errors. Statistical analyses were performed using SPSS software (version 23.0; SPSS Inc.). A p-value < 0.05 (two-tailed) was considered significant.
The initial item pool comprised 58 items describing knowledge, attitudes, practise, and experience regarding IPC. The items were divided into hospital environmental surface cleaning and disinfection management, isolation systems and hand hygiene, occupational protection, medical treatment, and COVID-19-related terminal disinfection.
Sixteen eligible experts were recruited in the first round of the Delphi method and 15 experts provided effective responses. Sixteen items were excluded, 31 items were modified, two items were merged, and nine items were added because their CVs were >0.25 or based on expert opinions (Table 2). The remaining 33 items all had CVs ≤ 0.25 [correlation value Kendall's W = 0.204/0.128; importance value Kendall's W = 0.249/0.142, p < 0.001 (Table 3)].

Table 2. Results of Delphi round 1 (N = 16).
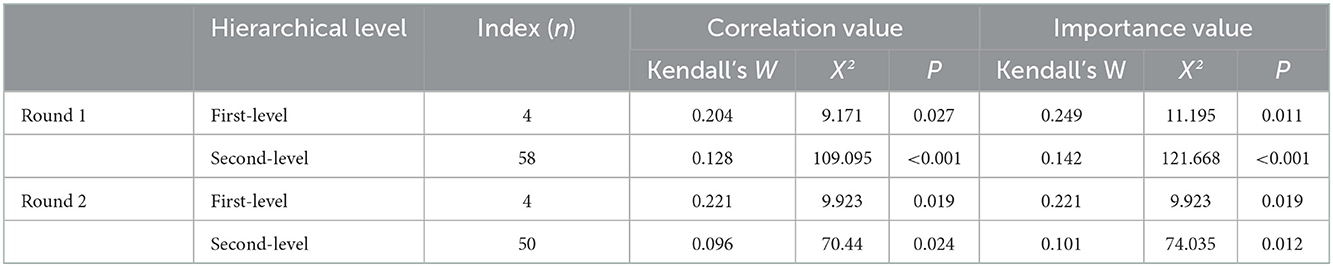
Table 3. Coordinate coefficients of expert advice for two rounds of consultations.
In the second-round Delphi method, all 15 experts who responded to the first round returned suitable responses. All items had CVs ≤ 0.25, and one item was excluded, with nine modified items, based on expert opinions (Table 4). Some items in the questionnaire were not colloquial enough [correlation value Kendall's W = 0.221/0.096; importance value Kendall's W = 0.221/0.101, p < 0.05 (Table 3)].
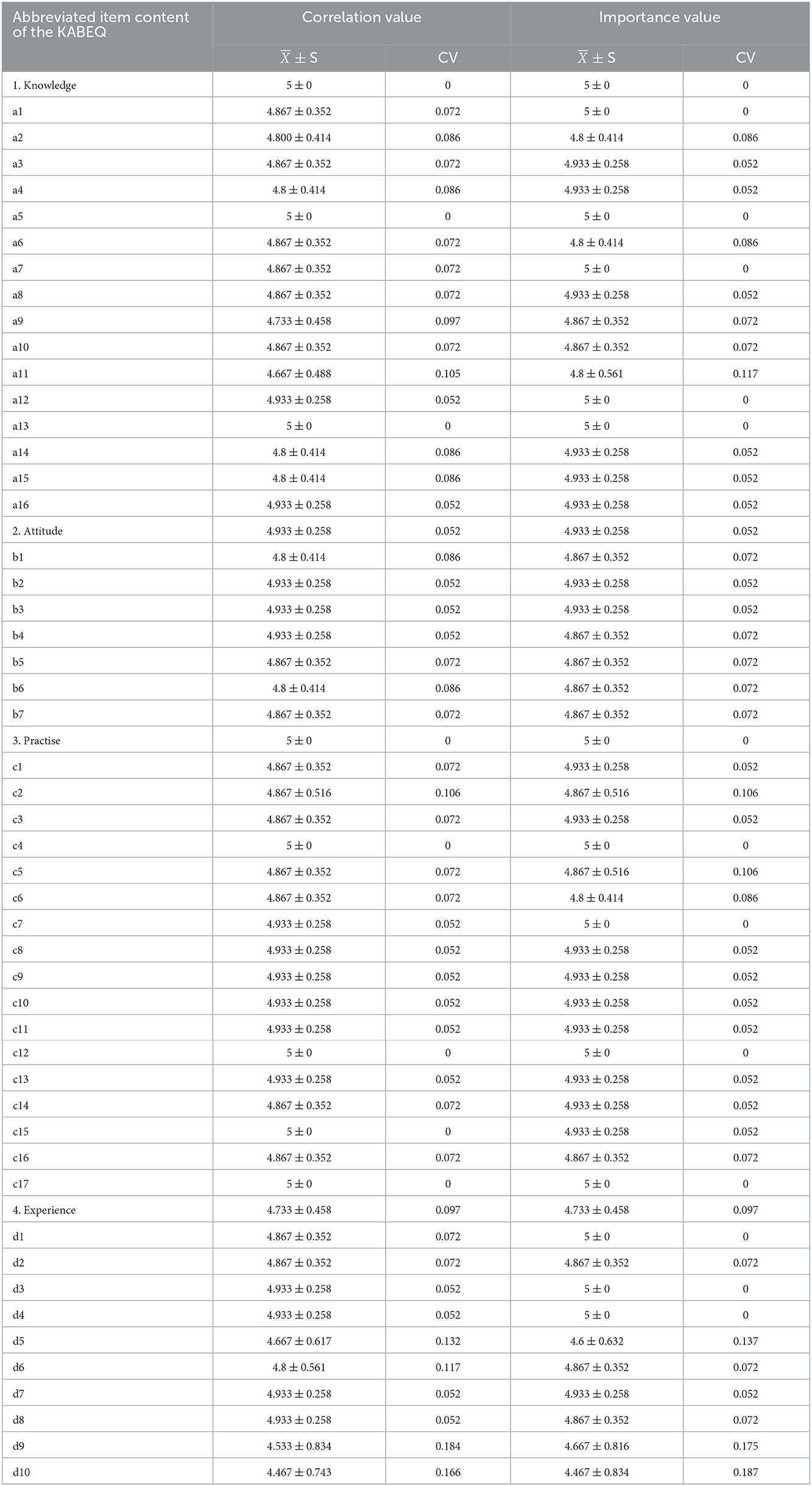
Table 4. Results of Delphi round 2 (N = 15).
After two rounds of the Delphi and in-depth discussion among the team members, 18 items were excluded, 31 items were modified, two items were merged, and 10 items were added based on the exclusion criteria and expert opinions. The KAPE-IPC-Q ultimately comprised four first-level indices (knowledge, attitudes, practise, and experience) and 49 second-level indices (Table 5).
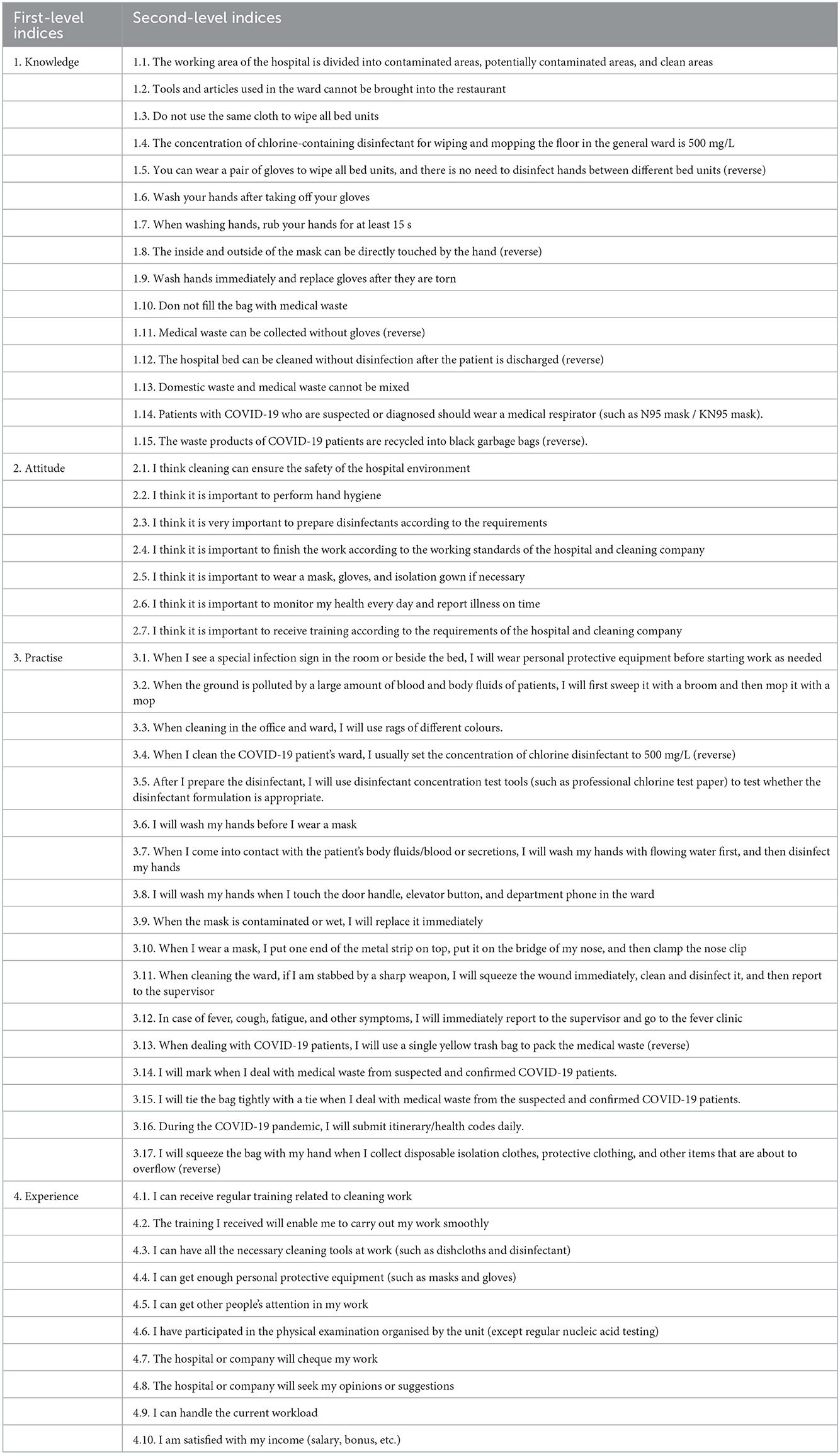
Table 5. Final tool.
We used the collected questionnaires for the pilot survey, 1,176 ESWs participated. The Cronbach's α coefficient was 0.967, and the S-CVI/Ave was 0.989. Therefore, the definitive version of the KAPE-IPC-Q after the two rounds of testing had four sections with 49 items.
IPC management is not only the focus of hospital management but also an important public health problem (26). ESWs in medical institutions are vital for the development of IPC, and health authorities must develop effective strategies to improve IPC compliance of ESWs. To formulate effective measures, it is essential to obtain the current situation on knowledge, attitudes, practise, and experience among ESWs regarding IPC. Since there was no available international measurement tool at the time of our survey, we designed a questionnaire entitled knowledge, attitudes, practise, and experience among ESWs regarding IPC in Chinese hospitals and examined its reliability and validity. We believe that our study has filled an important gap in the assessment of knowledge, attitudes, practise, and experience regarding IPC for ESWs in developing countries (e.g., China).
First, we based on information from the China Centres for Disease Control and Prevention (CDC), Joint Commission International, and WHO. Most of these websites have a strong global influence, especially in terms of hospital IPC. And according to the literature review and theoretical framework related to hospital environmental surface cleaning and disinfection management, the isolation system and hand hygiene, occupational protection, medical treatment, and COVID-19-related terminal disinfection. And then we conducted several research group meetings and two rounds of the Delphi process, combining the theoretical framework of IPC for ESWs. Accordingly, this study developed a questionnaire on knowledge, attitudes, practise, and experience regarding IPC among ESWs, it is scientific, comprehensive, and practical.
In the Delphi method, the number of experts in the panel was functionally related to the accuracy of the study results, which suggests that at least 10–18 expert members per panel are required to achieve a range of opinions (27). The quality of the consulting experts directly determines the success or failure of the Delphi method (28). In this study, 15 experts had influence and outstanding performance in IPC, scale development, evidence-based medicine, and hospital management, all with rich work experience and high-level job titles and academic qualifications, thus ensuring that the indicator system was rich in practical experience and a theoretical basis; the experts came from 10 different provinces (regions). Therefore, using the Delphi method, the quality of experts was high, and the quality index system was more reliable. Furthermore, this questionnaire had good reliability and validity through a pilot survey. Accordingly, the questionnaire is reliable.
The questionnaire items were set up as colloquially as possible because the respondents were culturally diverse and had a wide distribution of ages. Because of extensive outsourcing of hospital cleaning services, high turnover and inadequate training occur around the world (29). The inevitable result: A study of more than 1,000 patient rooms across 23 hospitals revealed that <50% of surfaces are properly cleaned (30). Around the world, ESWs' current situation is similar to that in China (31). Although our framework was developed in the Chinese context, we believe that it can be used in other countries for assessing knowledge, attitudes, practise, and experience regarding IPC for ESWs. Accordingly, the questionnaire is practical.
Knowledge and information are the foundation and the establishment of positive, correct beliefs and attitudes. Beliefs and attitudes are the motivating force for healthy behaviour change. Moreover, these two factors enhance and help evaluate IPC knowledge in ESWs as well as help ESWs recognise possible interventions to improve behavioural and attitudinal changes. Positive attitudes and behavioural changes are driven by the level of knowledge and perceptions towards preventive practices (32).
Previous studies have showed that surface contamination with pathogens results from inadequate cleaning by ESWs (11–13). Other studies have shown that the important measure to reduce the risk of hospital infection was correct and effective cleaning and disinfection (33). With this in mind, the knowledge and behavioural dimensions of this questionnaire include a large amount of hospital environmental surface cleaning and disinfection management, content, such as “Ordinary wiping and floor mopping disinfectant formulation: 5,000 ml (5 L) water + five tablets of chlorine-containing effervescent tablets”; the experts suggested changing to a specific concentration of chlorine-containing disinfectant, which was later changed to “the concentration of chlorine disinfectant in the common ward wipes and wet mops on the ground is 500 mg/L.” and “I can use chlorine disinfectants (e.g., 84 disinfectant) test tools to detect whether the disinfectant formulation is appropriate.” The experts recommended changing the chlorine disinfectant test tool to professional chlorine test paper when cleaners formulate the disinfectant; they used the disinfectant concentration test tool (such as professional chlorine test paper) to test whether the disinfectant formulation was appropriate. Cleaning and disinfection of the surface of the hospital environment are very important for cleaners.
Respondents reported that hand hygiene knowledge and practise among ESWs were unsatisfactory, but hand hygiene for ESWs may contribute to reducing the risk of cross-transmission (34). This questionnaire contained 8 items to investigate hand hygiene in ESWs. Hand hygiene is a complex behaviour that is easily influenced by knowledge, attitudes, values, and beliefs (35). Therefore, a survey of the knowledge and behaviour of hand hygiene among cleaners can facilitate the development of hand hygiene training in later stages.
When cleaning staff clean debris and sharps, they are likely to be stabbed by infusion needles, injection needles, scissor knives, or other medical devices (36). Most of the cleaners in China have not been trained in formal medical knowledge, and their awareness of their protection in daily operations is relatively weak. The treatment after being stabbed by needles is not standardised enough, and even a small number of cleaners have not undergone any treatment. The reason cleaners may not report a needlestick injury to the hospital infection office is that the reporting procedure is cumbersome and deemed unnecessary. There are still considerable safety hazards in the treatment of needle puncture injuries of cleaning staff, and the management mechanism of acupuncture wounds in hospitals also needs to be improved. Based on the above situation, this questionnaire set up the item “when cleaning the ward and pricked by a sharp weapon, I will immediately squeeze, clean, and disinfect and then report to my superior”; on the one hand, the handling of cleaning staff's needle puncture wound would be investigated, and on the other hand, the cleaner would be informed on how to correctly handle the needle puncture injury process.
One of the main risk factors that threaten a patient's health is HAIs (37). There are nearly 20 million HAI patients in the United States each year, of which nearly 90,000 die, and the direct economic loss is ~$28 billion to $45 billion (38). China surveyed 1,766 hospitals in 2014 and found that the HAI prevalence rate was 2.67%, which severely affected the patients' prognoses and increased the financial burden on patients, but 20–30% of HAIs were preventable (39). Central to effective disinfection is the ESW (40). When a hospitalised patient suffers an infection, the next patient to occupy their room has a 6-fold greater risk of acquiring the same pathogen (41). Terminal disinfection is an effective method of removing bacteria from the ward or bed (42). The questionnaire designed by the study set up the item “the bed unit after the patient is discharged from the hospital cannot be cleaned and disinfected” to understand the mastery of the terminal disinfection knowledge of the cleaning staff in preparation for future targeted hospital IPC training.
At present, the novel coronavirus is spreading rapidly around the world, the pressure to prevent the transmission of the virus continues to increase worldwide, and the task of epidemic prevention and control is still arduous (43). ESWs play an important role in the prevention of HAIs (16). The questionnaire designed for this study included the item “The use of a medical protective mask (e.g., N95 mask/KN95 mask) when exposed to suspected or confirmed COVID-19” and how to deal with medical waste generated by COVID-19 patients. The item “When I have symptoms such as fever, cough, and fatigue, I will immediately report it to my superior manager and go to the fever clinic,” which helps the cleaners to do a good job in epidemic prevention and control during the novel coronavirus epidemic.
A strength of this study was that the questionnaire was designed to fit a daily work scenario, which was easier for ESWs to understand. To minimise the misunderstanding of the medical terms included in the survey, the questionnaire avoided using medical jargon where possible and completed piloting by ESWs. It is recommended that a response rate of 70% be achieved for each round of the Delphi method to reduce bias and reach a meaningful consensus (44). Accordingly, the present study had response rates of over 70% between the rounds. It was considered that two rounds were sufficient to reach a consensus, and the consequence of undertaking further rounds included participant fatigue and higher drop-out rates (45).
This study has some limitations. First, as this study was conducted only in China, further validation studies are necessary for generalisation to other countries. Furthermore, the Delphi technique has been criticised for a lack of standardisation, and the reliability of the Delphi technique has not been confirmed (44–47).
In summary, this study was based on the Delphi method to develop a questionnaire on knowledge, attitudes, practise, and experience regarding IPC among ESWs that has good reliability and validity and has certain scientific and practical value.
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Zhongnan Hospital of Wuhan University Medical Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
XW, BF, and CZ are responsible for formulating overarching research goals and aims. PZ, RZ, and RC are accountable for the application of statistics. CZ and XC are responsible for verifying the overall replication of results and other research outputs. XC and PZ are responsible for explicitly writing the initial draught. Y-HJ, FH, SL, and LL are responsible for critical review, commentary, or revision—including pre- or post-publication stages. XW, BF, CZ, and LC are responsible for supervision, oversight, and leadership responsibility for the research activity planning and execution, including mentorship external to the core team. All authors contributed to the article and approved the submitted version.
The authors would like to thank all organisations and facilities that participated in the test and provided valuable feedback. Among these, they wish to recognise the following: Medical Administration and Administration Bureau of the National Health Commission, Evidence-Based Medicine Centre, Zhongnan Hospital, Wuhan University, 16 experts in the prevention and control of nosocomial infections, from the tertiary hospitals or universities (Zhongnan Hospital of Wuhan University, West China Hospital of Sichuan University, Affiliated Hospital of Xuzhou Medical University, The First People's Hospital Affiliated to Dalian Medical University, Longhua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, The First Affiliated Hospital of Jinzhou Medical University, Shanghai First People's Hospital, The First Affiliated Hospital of Jinan University, The Second Hospital of Hebei Medical University, The Second Affiliated Hospital of Nanchang University, and Shanxi Medical University).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Health care-acquired infections (HAIs).
2. ^Infection prevention and control (IPC).
3. ^World Health Organization (WHO).
4. ^Environmental service workers (ESWs).
5. ^Knowledge, Attitudes, Practise, and Experience regarding Infection Prevention and Control-associated Questionnaire (KAPE-IPC-Q).
1. Tartari E, Tomczyk S, Pires D, Zayed B, Coutinho Rehse AP, Kariyo P, et al. Implementation of the infection prevention and control core components at the national level: A global situational analysis. J Hosp Infect. (2021) 108:94–103. doi: 10.1016/j.jhin.2020.11.025
2. World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Wordwide. Geneva: WHO (2011). Available online at: https://apps.who.int/iris/handle/10665/80135 (accessed August 31, 2021).
3. World Health Organization. WHO Calls for Better Hand Hygiene and Other Infection Control Practices. (2021). Available online at: https://www.who.int/news/item/05-05-2021-who-calls-for-better-hand-hygiene-and-other-infection-control-practices (accessed August 31, 2021).
4. Cassini A, Plachouras D, Eckmanns T, Abu Sin M, Blank HP, Ducomble T, et al. Burden of six healthcare-associated infections on European Population Health: Estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. (2016) 13:e1002150. doi: 10.1371/journal.pmed.1002150
5. Chen YC, Huang HM, Lin PY, Shi ZY. Comparing visual inspection and performance observation for evaluation of hospital cleanliness. Am J Infect Control. (2021) 25:S0196-655300487-9. doi: 10.1016/j.ajic.2021.07.011
6. Mermel LA, Jefferson JA, Smit MA, Auld DB. Prevention of hospital-acquired respiratory viral infections: Assessment of a multimodal intervention program. Infect Control Hosp Epidemiol. (2019) 40:362–4. doi: 10.1017/ice.2018.337
7. Xu H, Jin H, Zhao L, Wei X, Hu L, Shen L, et al. A randomized, double-blind comparison of the effectiveness of environmental cleaning between infection control professionals and environmental service workers. Am J Infect Control. (2015) 43:292–4. doi: 10.1016/j.ajic.2014.11.009
8. Sharma A, Borah SB, Moses AC. Responses to COVID-19: The role of governance, healthcare infrastructure, and learning from past pandemics. J Bus Res. (2021) 122:597–607. doi: 10.1016/j.jbusres.2020.09.011
9. World Health Organization. Infection Prevention and Control Guidance for Long-Term Care Facilities in the Context of COVID-19. Interim Guidance. (2020). World Health Organization. Available online at: https://apps.who.int/iris/handle/10665/331508 (accessed August 31, 2021).
10. Kenters N, Gottlieb T, Hopman J, Mehtar S, Schweizer ML, Tartari E. An international survey of cleaning and disinfection practices in the healthcare environment. J Hosp Infect. (2018) 100:236–41. doi: 10.1016/j.jhin.2018.05.008
11. Hota B, Blom DW, Lyle EA, Weinstein RA, Hayden MK. Interventional evaluation of environmental contamination by vancomycin-resistant enterococci: Failure of personnel, product, or procedure? J Hosp Infect. (2009) 71:123–31. doi: 10.1016/j.jhin.2008.10.030
12. Dancer SJ. The role of environmental cleaning in the control of hospital-acquired infection. J Hosp Infect. (2009) 73:378–85. doi: 10.1016/j.jhin.2009.03.030
13. Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: Norovirus, Clostridium difficile, and Acinetobacter species. Am J Infect Control. (2010) 38:S25–33. doi: 10.1016/j.ajic.2010.04.196
14. Tyan K, Cohen PA. Investing in our first line of defense: Environmental services workers. Ann Intern Med. (2020) 173:306–7. doi: 10.7326/M20-2237
15. Bernstein DA, Salsgiver E, Simon MS, Greendyke W, Eiras DP, Ito M, et al. Understanding barriers to optimal cleaning and disinfection in hospitals: A knowledge, attitudes, and practices survey of environmental services workers. Infect Control Hosp Epidemiol. (2016) 37:1492–5. doi: 10.1017/ice.2016.206
16. Jennings A, Sitzlar B, Jury L. A survey of environmental service workers' knowledge and opinions regarding environmental cleaning. Am J Infect Control. (2013) 41:177–9. doi: 10.1016/j.ajic.2012.03.012
17. World Health Organization. Advocacy, Communication and Social Mobilization to Fight TB: A 10-Year Framework for Action/ASCM Subgroup at Country Level. Geneva: WHO (2006). Available online at: https://apps.who.int/iris/handle/10665/43474 (accessed August 31, 2021).
18. Health Committee of the People's Republic of China. Technical Guide to the Prevention and Control of New Coronavirus Infections in Medical Institutions. 2nd ed. Available online at: http://www.nhc.gov.cn/yzygj/s7659/202104/f82ac450858243e598747f99c719d917.shtml (accessed August 31, 2021).
19. World Health Organization. Infection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or Confirmed. Interim Guidance. (2021). Available online at: https://apps.who.int/iris/handle/10665/342620 (accessed August 31, 2021).
20. World Health Organization. Mask use in the Context of COVID-19. Interim Guidance. (2020). Available online at: https://apps.who.int/iris/handle/10665/337199 (accessed August 31, 2021).
21. Fu TC, Su DH, Chang SH. Serial association analyses of recurrent gap time data via Kendall's tau. Biostatistics. (2016) 17:188–202. doi: 10.1093/biostatistics/kxv034
22. Gao JL, Liu XM, Che WF, Xin X. Construction of nursing-sensitive quality indicators for haemodialysis using Delphi method. J Clin Nurs. (2018) 27:3920–30. doi: 10.1111/jocn.14607
23. Holey EA, Feeley JL, Dixon J, Whittaker VJ. An exploration of the use of simple statistics to measure consensus and stability in Delphi studies. BMC Med Res Methodol. (2007) 7:52. doi: 10.1186/1471-2288-7-52
24. Nunnally J, Bernstein I. Psychometric Theory. New York, NY: McGraw-Hill (1994). Available online at: http://www.researchgate.net/publication/309254394_Henri_J.M._Claessen_Constructing_the_early_state_The_rise_of_a_research_programme (accessed August 31, 2021).
25. Lynn MR. Determination and quantification of content validity. Nurs Res. (1986) 35:382–5. doi: 10.1097/00006199-198611000-00017
26. Glasper A. Keeping patients safe from hospital-acquired infection. Br J Nurs. (2019) 28:890–1. doi: 10.12968/bjon.2019.28.13.890
27. Williamson C, Kelly P, Tomasone JR, Bauman A, Mutrie N, Niven A, et al. A modified Delphi study to enhance and gain international consensus on the Physical Activity Messaging Framework (PAMF) and Checklist (PAMC). Int J Behav Nutr Phys Act. (2021) 18:108. doi: 10.1186/s12966-021-01182-z
28. Brown BB. Delphi Process: A Methodology Used for the Elicitation of Opinions of Experts. Santa Monica, CA: RAND Corporation (1968). p. 3,925. Available online at: https://www.rand.org/pubs/papers/P3925.html (accessed March 30, 2022).
29. Toffolutti V, Reeves A, McKee M, Stuckler D. Outsourcing cleaning services increases MRSA incidence: Evidence from 126 English acute trusts. Soc Sci Med. (2017) 174:64–9. doi: 10.1016/j.socscimed.2016.12.015
30. Carling PC, Parry MF, Von Beheren SM. Identifying opportunities to enhance environmental cleaning in 23 acute care hospitals. Infect Control Hosp Epidemiol. (2008) 29:1–7. doi: 10.1086/524329
31. Ni K, Chen B, Jin H, Kong Q, Ni X, Xu H. Knowledge, attitudes, and practices regarding environmental cleaning among environmental service workers in Chinese hospitals. Am J Infect Control. (2017) 45:1043–5. doi: 10.1016/j.ajic.2017.02.029
32. Larson EL, Bryan JL, Adler LM, Blane C. A multifaceted approach to changing handwashing behavior. Am J Infect Control. (1997) 25:3–10. doi: 10.1016/S0196-6553(97)90046-8
33. Santos-Junior AG, Ferreira AM, Frota OP, Rigotti MA, Barcelos LDS, Lopes de Sousa AF, et al. Effectiveness of surface cleaning and disinfection in a Brazilian healthcare facility. Open Nurs J. (2018) 12:36–44. doi: 10.2174/1874434601812010036
34. Zhou K, He X, Huo L, An J, Li M, Wang W, et al. Development of the body image self-rating questionnaire for breast cancer (BISQ-BC) for Chinese mainland patients. BMC Cancer. (2018) 18:19. doi: 10.1186/s12885-017-3865-5
35. Kohli E, Ptak J, Smith R, Taylor E, Talbot EA, Kirkland KB. Variability in the Hawthorne effect with regard to hand hygiene performance in high- and low-performing inpatient care units. Infect Control Hosp Epidemiol. (2009) 30:222–5. doi: 10.1086/595692
36. Wang HJ, Huang SQ, Shen PP. Application of nursing interventions in acupuncture injuries of cleaning staff in hospital operating rooms. Zhejiang Clin Med J. (2018) 20:2.
37. Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, et al. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. (2014) 370:1198–208. doi: 10.1056/NEJMoa1306801
38. Stone PW. Economic burden of healthcare-associated infections: An American perspective. Expert Rev Pharmacoecon Outcomes Res. (2009) 9:417–22. doi: 10.1586/erp.09.53
39. Zhang Y, Zhong ZF, Chen SX, Zhou DR, Li ZK, Meng Y, et al. Prevalence of healthcare-associated infections and antimicrobial use in China: Results from the 2018 point prevalence survey in 189 hospitals in Guangdong Province. Int J Infect Dis. (2019) 89:179–84. doi: 10.1016/j.ijid.2019.09.021
40. Hewage SCN, Cao LTT, Jones RM, Fraser AM. Factors associated with environmental service worker cleaning practices in health care settings: A systematic review of the literature. Am J Infect Control. (2021) 49:919–27. doi: 10.1016/j.ajic.2021.01.001
41. Cohen B, Liu J, Cohen AR, Larson E. Association between healthcare-associated infection and exposure to hospital roommates and previous bed occupants with the same organism. Infect Control Hosp Epidemiol. (2018) 39:541–6. doi: 10.1017/ice.2018.22
42. Manian FA, Griesnauer S, Senkel D. Impact of terminal cleaning and disinfection on isolation of Acinetobacter baumannii complex from inanimate surfaces of hospital rooms by quantitative and qualitative methods. Am J Infect Control. (2013) 41:384–5. doi: 10.1016/j.ajic.2012.04.321
43. Burki TK. Omicron variant and booster COVID-19 vaccines. Lancet Respir Med. (2022) 10:e17. doi: 10.1016/S2213-2600(21)00559-2
44. Sumsion T. The Delphi technique: An adaptive research tool. Br J Occup Ther. (1998) 61:153–6. doi: 10.1177/030802269806100403
45. Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. (2000) 32:1008–15. doi: 10.1046/j.1365-2648.2000.t01-1-01567.x
46. Vernon W. The Delphi technique: A review. Int J Ther Rehabil. (2009) 16:69–76. doi: 10.12968/ijtr.2009.16.2.38892
Keywords: infection prevention and control, environmental service worker, knowledge, attitude, practise, experience, Delphi method
Citation: Chen X, Zhang P, Zhang R, Li S, Cao R, Hu F, Jin Y-H, Lin L, Cai L, Feng B, Zhang C and Wang X (2023) Development and validation of the regarding infection prevention and control among environmental service workers on knowledge, attitudes, practise, and experience questionnaire. Front. Public Health 10:1062199. doi: 10.3389/fpubh.2022.1062199
Received: 05 October 2022; Accepted: 20 December 2022;
Published: 09 January 2023.
Edited by:
Zongxin Ling, Zhejiang University, ChinaReviewed by:
Nina Musurlieva, Plovdiv Medical University, BulgariaCopyright © 2023 Chen, Zhang, Zhang, Li, Cao, Hu, Jin, Lin, Cai, Feng, Zhang and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinghuan Wang,  d2FuZ3hpbmdodWFuQHdodS5lZHUuY24=; Bilong Feng, ZmJsMTAxOUAxMjYuY29t; Chunhua Zhang, MTY0ODI3NjA3OUBxcS5jb20=
d2FuZ3hpbmdodWFuQHdodS5lZHUuY24=; Bilong Feng, ZmJsMTAxOUAxMjYuY29t; Chunhua Zhang, MTY0ODI3NjA3OUBxcS5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.