 Lydia C. Parr
Lydia C. Parr Thelma J. Mielenz
Thelma J. Mielenz
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 10 January 2023
Sec. Aging and Public Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1059164
This article is part of the Research TopicShifting the Narrative on Unpaid Care for Older Adults: Perspectives on Positive Caregiving Experiences and OutcomesView all 7 articles
Background: The literature demonstrates an association between aspects of caregiving and support with caregiver burden and differences by race. Our objective was to examine correlates of caregiver wellbeing, and if the effect is moderated by race.
Methods: The National Study of Caregiving (NSOC) is a survey of unpaid and familial caregivers affiliated with participants in the National Health and Aging Trends Study, a nationally representative survey of Medicare beneficiaries. A total of 899 participants were examined cross-sectionally with logistic and multinomial logistic regression models to obtain adjusted odds ratios (aOR) and 95% confidence intervals (CI) for NSOC Round 3 (2017), stratified by race, to determine the association between aspects of caregiving and support variables with the two outcomes, three-level caregiving gains, and response to the statement “life has meaning and purpose.”
Results: Among black caregivers with no family or friends to help, there were lower gains compared to very high gains (aOR: 2.82, 95% CI: 1.18, 6.77). Black and white caregivers who endorsed lower ratings regarding being appreciated by the care recipient had lower gains for “life has meaning and purpose” (aOR: 2.46, 95% CI: 1.00, 6.02; aOR: 1.65, 95% CI: 1.06, 2.56). Black caregivers with lower ratings regarding being appreciated had lower gains compared to very high gains (aOR: 5.04, 95% CI: 1.48, 17.17). White caregivers endorsing lower ratings to the same question had lower gains compared to very high gains (aOR: 3.27, 95% CI: 1.77, 6.04), and those with more help had lower gains (aOR: 0.81, 95% CI: 0.70, 0.93).
Conclusion: The relationship between various correlates and positive aspects of caregiving is moderated by black and white races. Further study on the impact of aspects of caregiving and support networks for caregivers may shed light on factors contributing to racial differences and areas for intervention.
With the increasing aging population of the United States, the population of unpaid and familial caregivers has also increased (1–3). Caregiver wellbeing, including the perception of purpose in life, is associated with better mental and physical health as well as decreased mortality (4). Prior studies found that caregiver wellbeing and burden are moderated by race/ethnicity for measures such as care burden, psychological wellbeing, and self-rated health, as well as varying use of support such as respite services based on race (5, 6). Additional research found evidence that black caregivers have higher levels of caregiving intensity such as assistance with activities of daily living (ADLs) as well as time spent on caregiving, and quality of life was most drastically impacted by caregiving intensity for female caregivers (7). The literature suggests negative emotional burden associated with high-intensity care and positive emotions related to caregiving vary by race and age, levels of social burden vary relating to caregiving intensity and caregiver's age, and high-intensity caregiving was associated with varying measures of quality of life for those of different racial groups, genders, ages, and incomes (3, 8–10). Other studies found associations between outlook, purpose in life, and positive caregiving outcomes for caregivers of older adults (4, 11, 12), indicating that both relationship and perception of the caregiving role may influence caregiver wellbeing. Demographic and personal-level factors, as well as domains aspects of caregiving, support environment, and duration of caregiving, all seem to contribute to caregiver wellbeing (5–8).
This study identifies key correlates of wellbeing and potential moderation regarding domains of caregiving and wellbeing. Most literature on unpaid caregiving for older adults focuses on the burden of care, and positive experiences and impacts on caregivers warrant attention as well (1, 13–16). This type of research may allow for public health policy and messaging regarding caregiving, which considers personal-level, socioeconomic, and political factors relating to caregiving outcomes rather than centering policy and messaging around negative aspects of caregiving. Such policy and messaging would be strengthened by an understanding of the effect social determinants related to race/ethnicity have on caregiver wellbeing. Examining what contributes to positive wellbeing outcomes may help better support caregivers, offer a balanced perception of caregiving, and make strides to improve wellbeing outcomes as demographic shifts continue to necessitate informal caregiving.
This study aims (1) to determine the correlates of caregiver wellbeing through analysis of the impact of the domains duration of care, aspects of caregiving, and support environment on caregiver wellbeing and (2) to study the wellbeing of caregivers based on both personal-level factors such as race and gender as well as domains of caregiving duration of care, aspects of caregiving, and support environment.
Data were obtained from the National Study of Caregiving (NSOC) for the calendar year 2017 for this cross-sectional analysis. The NSOC is a nationally representative survey of family and other unpaid caregivers for older persons in the USA, and it has been conducted three times in conjunction with the National Health and Aging Trends Study (NHATS), which samples Medicare enrollees aged 65 and older (17).
For round 3, which represented caregivers initially interviewed in 2015 and re-interviewed in 2017, there were 2,361 caregivers interviewed. This study utilized 899 participants from the interview conducted in 2017 who did not have missing values for variables in the analyses. Caregivers are eligible if identified by an NHATS participant; assist with at least one of a list of mobility, self-care, household, and other activities; and are related to the NHATS participant (regardless of whether or not they are paid) or are unrelated and unpaid (17).
The primary outcomes are purpose in life and caregiving gains, which are derived from five variables in the NSOC.
The measure of caregiving gains is derived by summing four variables with four-level Likert responses that ask caregivers if their caregiving situation made them more confident about their abilities, taught them to deal with difficult situations, brought them closer to the care recipient, or had given them the satisfaction that the care recipient is well cared for (4).
The measure of purpose in life is derived from an NSOC question that asks caregivers to respond to the statement “My life has meaning and purpose” on a Likert scale from one to four (4, 12, 16).
The potential exposures included in this analysis are as follows: duration of care measured in weeks of assistance and hours per week of care; aspects of caregiving such as relationship quality, perception of caregiving, living arrangement with the care receiver, relationship with the care receiver, and type of care provided such as assistance with ADLs and instrumental ADLs; support environments such as the caregivers' social network size and social participation as well as any social support with caregiving such as participation in support groups, training, or financial help.
Covariates for the model include the gender of the caregiver, coded dichotomously as male or female. The caregiver's age in years is continuous. Education level is categorized as less than high school, high school, and associate or beyond. In addition, one covariate will represent a number of chronic conditions (multiple morbidities) of the caregiver; this will be derived from dichotomous questions regarding if the caregiver has ever had a heart attack, heart disease, high blood pressure, arthritis, osteoporosis, diabetes, lung disease, cancer, difficulty seeing, difficulty hearing, chronic pain, breathing problems, limited strength in limbs, or fatigue. The number of comorbidities will be divided into the following categories: none, one, two, or three, and four or more (17, 18).
Associations between measures of caregiving gains and purpose in life with each potential exposure will be examined using the chi-square test. Linearity was assessed with age and ordinal variables as well as collinearity to identify any variables that were correlated. Due to collinearity with the hours help daily variable, how often help with chores, shopping, getting around the home, and help with personal care were omitted from the aspects of caregiving models. Whether the caregiver had attended a support group was omitted from the support model due to collinearity. Due to small cell sizes, certain categories were collapsed. For caregiving gains, the three lower strata were collapsed into one, including moderate, low, and very low gains. For “Life has meaning and purpose,” the responses “Agree somewhat” and “Disagree” were collapsed into one category. Other relative and non-relative relationships to the care recipient were collapsed into one category, with immediate family or spouse being the other category. Responses “A little” and “Not at all” to questions regarding the caregiving enjoying being with the care recipient, feeling that the care recipient appreciates them, and the frequency the caregiver speaks to the care recipient's medical provider were collapsed into one category for the analysis due to small cell sizes.
Nominal logistic regression and logistic regression analyses accounting for sampling weights will be performed to obtain adjusted odds ratios with 95% confidence intervals. We will also perform a Hosmer–Lemeshow test for goodness of fit of the logistic regression models to determine whether the model is adequate or whether there are correlates with a significant lack of fit. Variables included in this investigation will reflect hypotheses regarding the correlates of caregiver wellbeing, and analyses will be stratified by both race and gender, which were both seen to affect the modifiers of caregiving outcomes in prior studies (6–8). All analyses will be performed in StataBE v17.
Table 1 shows unweighted counts and column proportions of caregiving and demographic variables by black and white races. For the “Life has meaning and purpose” variable, 91.08% of black caregivers endorsed “Agree Strongly,” while for white caregivers, a lesser proportion, 80.79%, endorsed “Agree Strongly.” For the “Caregiving gains” variable, 58.36% of black caregivers scored very high, while 30.32% of white caregivers scored very high. Black caregivers were slightly younger on average compared to white caregivers (56.29 vs. 61.55 years), and a greater proportion was female than white caregivers (77.7% vs. 57.9%). A smaller proportion of black caregivers were immediate family or spouse to the care recipient compared to white caregivers (85.25% vs. 91.9%), a greater proportion enjoyed being with the care recipient (91.08% vs. 77.94%), and a greater proportion reported speaking to the care recipient's medical provider “A Lot” (66.17% vs. 42.22%).
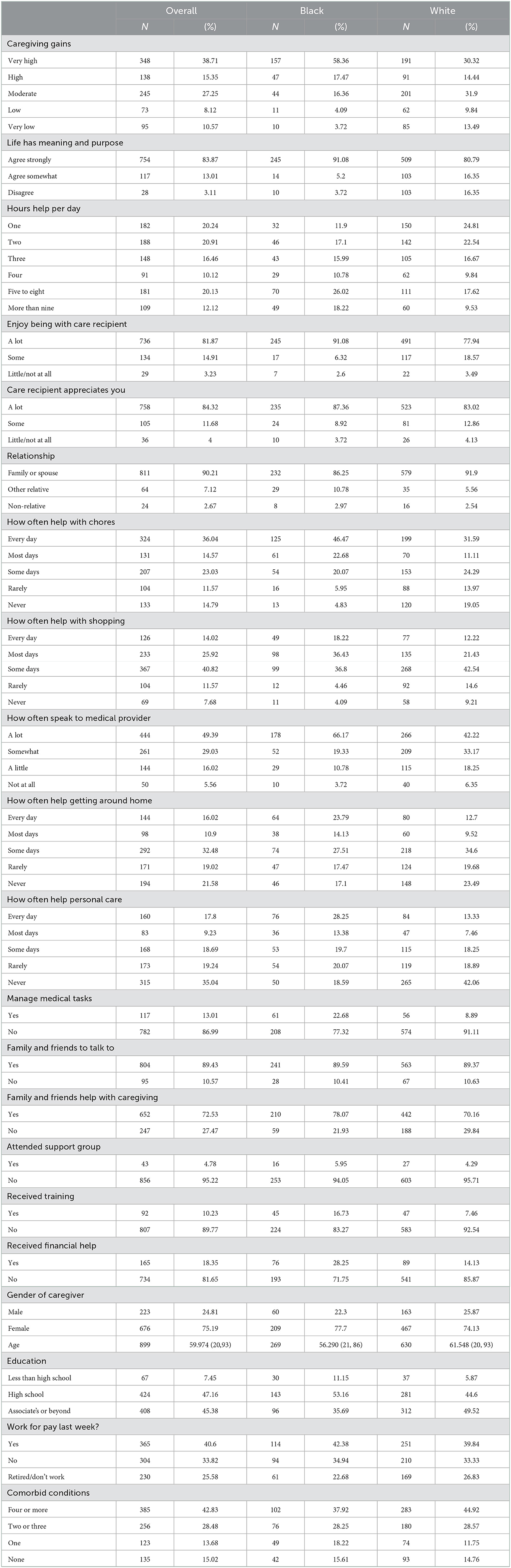
Table 1. Unweighted demographic characteristics.
Multivariate regression results of the support models, which included correlates with family or friends to talk to, family or friends help caregiving, received financial help, and received caregiver training, found significant correlates among black caregivers. The “Life has meaning and purpose” and support model did not converge after accounting for sampling weights, and the caregiver training was completely determined for the unweighted model. Among black caregivers who had no friends or family to talk to, the unweighted analysis indicated there was 3.43 times the odds of endorsing “Somewhat Agree” or “Disagree” rather than “Strongly Agree” to the statement “Life has meaning and purpose” compared to those who did have family or friends to talk to, adjusting for education, number of comorbidities, caregiver age, and caregiver gender [adjusted odds ratio (aOR): 3.43, 95% confidence interval (CI): 1.08, 10.91]. The covariate received caregiver training predicted black caregivers' responses to “Life has meaning and purpose” perfectly. For the “Life has meaning and purpose” and support covariates model, family or friends to help caregiving, having received financial help, and having received caregiver training were not significant for black caregivers in the unweighted model, and no correlates were significant for white caregivers in the weighted model (Table 2).
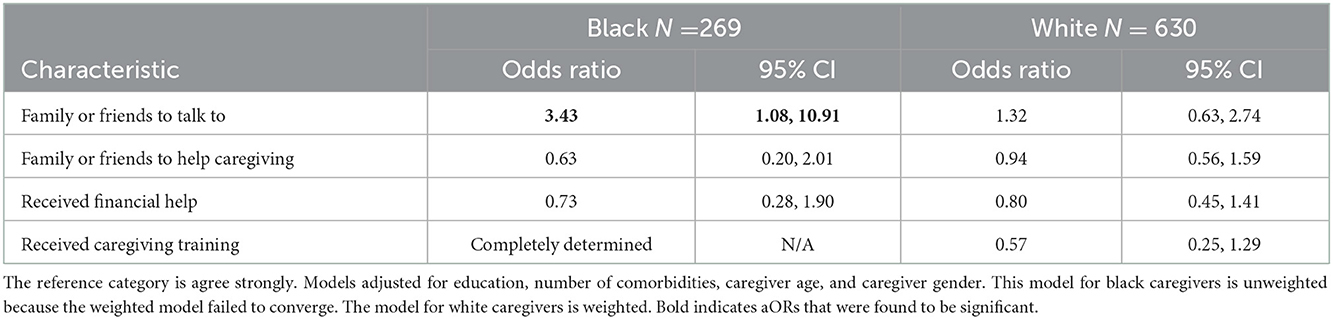
Table 2. Life has meaning and purpose and support.
In the weighted analyses, among black caregivers with no family or friends to help with caregiving, there was 2.82 times the odds of having moderate to very low gains rather than very high gains compared to those with family or friends to help caregiving, adjusting for education, number of comorbidities, caregiver age, and caregiver gender (aOR: 2.82, 95% CI: 1.17, 6.77). Among black caregivers who had not received caregiving training, there was 4.52 times the odds of having high rather than very high gains compared to those with family or friends to help with caregiving, adjusting for education, number of comorbidities, caregiver age, and caregiver gender (aOR: 4.52, 95% CI: 1.43, 14.25). For the caregiving gains and support model, having family or friends to talk to and having received financial help were not significant correlates of caregiving gains for black caregivers, and no correlates were significant for white caregivers (Table 3).
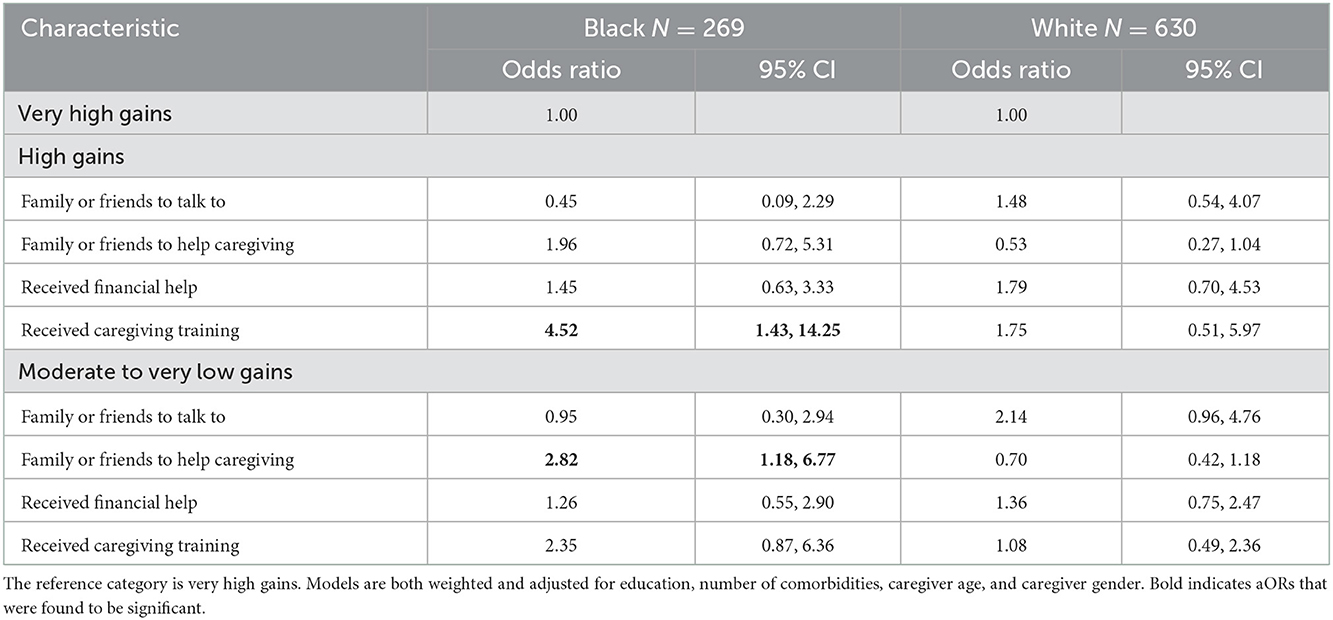
Table 3. Caregiver gains and support.
The aspect of caregiving models includes variables relating to whether the caregiver has helped with medical tasks, talks to medical providers, their relationship with the care recipient (immediate relative or spouse vs. other), if they believe the care recipient appreciates them, and the hours they help the care recipient daily. For the model aspects of caregiving and “Life has meaning and purpose,” among black caregivers, those who endorsed responses “Some,” “Little,” or “Not at all” to the statement that the care recipient appreciates them had 2.45 times the odds of endorsing “Agree somewhat” or “Disagree” rather than “Agree strongly” to the statement “Life has meaning and purpose” compared to those who said the care recipient appreciates them “A lot,” adjusting for education, number of comorbidities, caregiver age, and caregiver gender (aOR: 2.45, 95% CI: 1.00, 6.02).
Among white caregivers, those who endorsed responses “Some,” “Little,” or “Not at all” to the statement that the care recipient appreciates them had 1.65 times the odds of endorsing “Agree somewhat” or “Disagree” rather than “Agree strongly” to the statement “Life has meaning and purpose” compared to those who said the care recipient appreciated them “A lot,” adjusting for the same demographic covariates (aOR: 1.65, 95% CI: 1.06, 2.56). Across the aspects of caregiving and “Life has meaning and purpose” models, the caregiver helping with medical tasks, talking to medical providers, relationship with the care recipient, and hours spent helping daily were not significant correlates of response to the statement “Life has meaning and purpose.” Both models were weighted (Table 4).
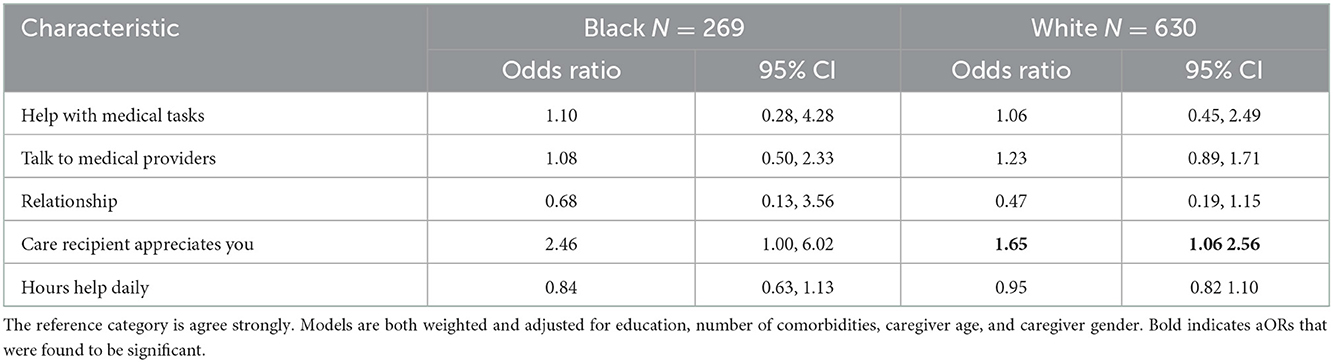
Table 4. Life has meaning and purpose and aspects of caregiving.
For the models relating to aspects of caregiving and caregiving gains, among black caregivers who only “Somewhat,” “A little,” or “Not at all” spoke to medical providers, there was 2.15 times the odds of very low to moderate gains rather than very high gains compared to those who talked to medical providers “A lot” (aOR: 2.15, 95% CI: 1.32, 3.50). Among white caregivers who only “Somewhat,” “A little,” or “Not at all” spoke to medical providers, there was 1.65 times the odds of very low to moderate gains rather than very high gains compared to those who talked to medical providers “A lot” (aOR: 1.65, 95% CI: 1.19, 2.29).
Among black caregivers who endorsed “Some,” “Little,” or “Not at all” to the statement that the care recipient appreciates them, there was 5.04 times the odds of very low to moderate gains rather than very high gains compared to those who endorsed the care recipient appreciates them “A lot” (aOR: 5.04, 95% CI: 1.48, 17.17). Among white caregivers who endorsed “Some,” “Little,” or “Not at all” to the statement that the care recipient appreciates them, there was 3.27 times the odds of very low to moderate gains compared to very high gains compared to those who endorsed the care recipient appreciates them “A lot” (aOR: 3.27, 95% CI: 1.77, 6.04).
Among black caregivers helping the care recipient at a one-category increase of hours (one, two, three, four, five to eight, and greater than nine) per day, there was 0.72 times the odds of very low to moderate gains rather than very high gains compared to those who helped the care recipient for a lower time category (aOR: 0.72, 95% CI: 0.57, 0.93). Among white caregivers helping the care recipient at a one-category increase of hours per day, there was 0.81 times the odds of very low to moderate gains rather than very high gains compared to those who helped the care recipient for a lower time category (aOR: 0.81, 95% CI: 0.70, 0.93). Helping with medical tasks and relationship with care recipients were not significant correlates of caregiving gains for black or white caregivers. Both models were weighted (Table 5).
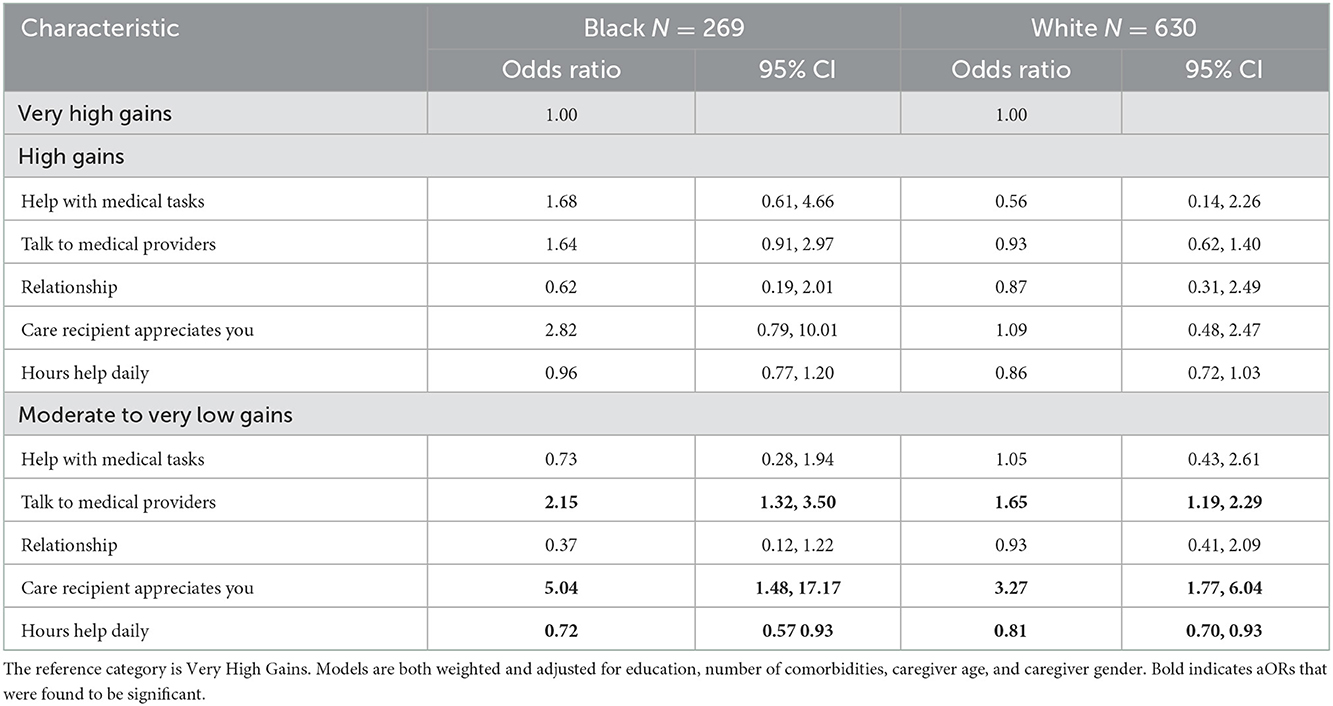
Table 5. Caregiver gains and aspects of caregiving.
Many of the observed associations aligned with our expectations. In the caregiving gains and aspects of caregiving models, for both races, those who endorsed lower frequencies of helping with medical tasks were more likely to have moderate, low, and very low compared to very high caregiving gains. This relationship warrants further study.
The models showed differences by black and white races, which was expected. Previous research using NSOC data found differences in caregiver outcomes by race (5). For the support models, “Life has meaning and purpose” and caregiving gains were only significant among black caregivers. Having family and friends to talk to related to endorsing “Agree strongly” to the statement “Life has meaning and purpose,” and for black caregivers without family or friends to help with caregiving, there were elevated odds of moderate, low, and very low compared to very high caregiving gains. The ORs for “Care recipient appreciates you” were significant for both races but differed in the “Life has meaning and purpose” and aspects of the caregiving model. In the caregiving gains and aspects of the caregiving model, the magnitude of the ORs differed by race for talking to medical providers and care recipient appreciates you. The high compared to very high caregiving gains category was only significant for black caregivers, and relationship with care recipient and hours help daily were only significant among white caregivers.
Higher caregiving intensity was represented by the hours help daily variable, which was found to be significantly associated with lower categories of caregiving gains for white caregivers. The relationship between caregiving intensity and caregiver burden has been previously established (7, 8). Social support variables and the caregiver's outlook on caregiving were found to be associated with positive wellbeing outcomes in previous studies as well (4, 8). This study provides further evidence that social support and a positive perception of the relationship with the care recipient relate to caregiver wellbeing.
This study has a few limitations. The constructs of caregiver wellbeing have not been widely studied, and other positive outcomes may be more appropriate. Causal relationships cannot be determined from this cross-sectional analysis. For both predictor and outcome variables, categories had to be collapsed due to small strata, but the resulting categories were still meaningful. There was a high proportion of missing data, which may cause bias and a lack of precision, and there may be a lack of generalizability because only black and white races were included in the analysis, while the non-Hispanic Other and Hispanic categories were excluded due to small cell sizes.
This is a preliminary analysis, and a future study will utilize multiple time points of the NSOC for longitudinal analysis to see whether the relationship persists across three time points when the third wave of longitudinal data is available. Studies on the impact of aspects of caregiving and support networks for caregivers may shed light on factors contributing to racial differences. In addition, further study may identify any areas for intervention and causal explanation for some of the associations identified in this study.
Publicly available datasets were analyzed in this study. This data can be found here: National Study of Caregiving. Produced and distributed by www.nhats.org with funding from the National Institute on Aging [Grant numbers R01AG054004 (NSOC III) and R01AG062477 (NSOC IV)].
The studies involving human participants were reviewed and approved by Columbia University Research Compliance and Administration System IRB. The patients/participants provided their written informed consent to participate in this study.
TM and LP were involved in conceptualizing data analysis, manuscript preparation, interpretation of data, and critical revisions of the manuscript. LP performed data analysis. TM contributed to and supervised data analysis. All authors contributed to the article and approved the submitted version.
This research was supported in part by Grant 1 R49 CE002096-01 from the Centers for Disease Control and Prevention, the National Center for Injury Prevention and Control to the Center for Injury Epidemiology and Prevention at Columbia University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
1. Cohen SA, Cook S, Kelley L, Sando T, Bell AE. Psychosocial factors of caregiver burden in child caregivers: results from the new national study of caregiving. Health and Quality of Life Outcomes. (2015) 13:120–5. doi: 10.1186/s12955-015-0317-2
2. Haley WE, West CA, Wadley VG, Ford GR, White FA, Barrett JJ, Roth DL. Psychological, social, and health impact of caregiving: a comparison of black and white dementia family caregivers and noncaregivers. Psychol Aging. (1995) 10:540–52. doi: 10.1037/0882-7974.10.4.540
3. Willert B, Minnotte KL. Informal caregiving and strains: exploring the impacts of gender, race, and income. Appl Res Qual Life. (2021) 16:943–64. doi: 10.1007/s11482-019-09786-1
4. Polenick CA, Sherman CW, Birditt KS, Zarit SH, Kales HC. Purpose in life among family care partners managing dementia: links to caregiving gains. Gerontologist. (2019) 59:e424–32. doi: 10.1093/geront/gny063
5. Moon HE, Haley WE, Rote SM, Sears JS. Caregiver well-being and burden: variations by race/ethnicity and care recipient nativity status. Innov Aging. (2020) 4:igaa045. doi: 10.1093/geroni/igaa045
6. Parker LJ, Fabius CD. Racial differences in respite use among black and white caregivers for people living with dementia. J Aging Health. (2020) 32:1667–75. doi: 10.1177/0898264320951379
7. Cohen SA, Cook SK, Sando TA, Brown MJ, Longo DR. Socioeconomic and demographic disparities in caregiving intensity and quality of life in informal caregivers: a first look at the national study of caregiving. J Gerontol Nurs. (2017) 43:17–24. doi: 10.3928/00989134-20170224-01
8. Cook SK, Snellings L, Cohen S. A socioeconomic and demographic factors modify observed relationship between caregiving intensity and three dimensions of quality of life in informal adult children caregivers. Health Qual Life Outcomes. (2018) 16:169. doi: 10.1186/s12955-018-0996-6
9. Skarupski KA, McCann JJ, Bienias JL, Evans DA. Race differences in emotional adaptation of family caregivers. Aging Mental Health. (2009) 13:715–24. doi: 10.1080/13607860902845582
10. Sorensen S, Pinquart M. Racial and ethnic differences in the relationship of caregiving stressors, resources, and sociodemographic variables to caregiver depression and perceived physical health. Aging Mental Health. (2005) 9:482–95. doi: 10.1080/13607860500142796
11. Lawton MP, Moss M, Kleban MH, Glicksman A, Rovine M. A two-factor model of caregiving appraisal and psychological well-being. J Gerontol. (1991) 46:P181–P189. doi: 10.1093/geronj/46.4.p181
12. McKnight PE, Kashdan TB. Purpose in life as a system that creates and sustains health and well-being: an integrative, testable theory. Rev General Psychol. (2009) 13:242–51. doi: 10.1037/a0017152
13. Cohen CA, Colantonio A, Vernich L. Positive aspects of caregiving: rounding out the caregiver experience. Int J Geriatr Psychiatry. (2002) 17:184–8. doi: 10.1002/gps.561
14. Mackenzie A, Greenwood N. Positive experiences of caregiving in stroke: a systematic review. Disabil Rehabil. (2012) 34:1413–22. doi: 10.3109/09638288.2011.650307
15. Mollica MA, Smith AW, Kent EE. Caregiving tasks and unmet supportive care needs of family caregivers: a US population-based study. Patient Educ Counsel. (2020) 103:626–34. doi: 10.1016/j.pec.2019.10.015
16. Sánchez-Izquierdo M, Prieto-Ursúa M, Caperos JM. Positive aspects of family caregiving of dependent elderly. Educ Gerontol. (2015) 41:745–56. doi: 10.1080/03601277.2015.1033227
17. Freedman VA, Skehan ME, Hu M, Wolff J, Kasper JD. National Study of Caregiving I-III User Guide. Baltimore: Johns Hopkins Bloomberg School of Public Health (2019). Available online at: www.nhats.org (accessed December 28, 2022).
Keywords: positive aspects of caregiving, NSOC, NHATS, Medicare, race
Citation: Parr LC and Mielenz TJ (2023) Correlates of caregiver well-being: The National Study of Caregivers. Front. Public Health 10:1059164. doi: 10.3389/fpubh.2022.1059164
Received: 01 October 2022; Accepted: 12 December 2022;
Published: 10 January 2023.
Edited by:
Narelle Warren, Monash University, AustraliaReviewed by:
Mohamad-Rodi Isa, Universiti Teknologi MARA, MalaysiaCopyright © 2023 Parr and Mielenz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thelma J. Mielenz,  dGptMjE0MUBjdW1jLmNvbHVtYmlhLmVkdQ==
dGptMjE0MUBjdW1jLmNvbHVtYmlhLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.