
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 05 January 2023
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1058807
 Nicole H. T. M. Dukers-Muijrers1,2*
Nicole H. T. M. Dukers-Muijrers1,2* Ymke Evers1,3†
Ymke Evers1,3† Veja Widdershoven1,3†
Veja Widdershoven1,3† Udi Davidovich4,5
Udi Davidovich4,5 Philippe C. G. Adam6,7
Philippe C. G. Adam6,7 Eline L. M. Op de Coul8Paul Zantkuijl9Amy Matser4,10,11
Eline L. M. Op de Coul8Paul Zantkuijl9Amy Matser4,10,11 Maria Prins4,10,11Henry J. C. de Vries4,8,10,12
Maria Prins4,10,11Henry J. C. de Vries4,8,10,12 Casper den Heijer1,3
Casper den Heijer1,3 Christian J. P. A. Hoebe1,3,13Anne-Marie Niekamp1,3
Christian J. P. A. Hoebe1,3,13Anne-Marie Niekamp1,3 Francine Schneider2Juliana Reyes-Urueña14Roberto Croci14Angelo D'Ambrosio14Marc van der Valk10,15
Francine Schneider2Juliana Reyes-Urueña14Roberto Croci14Angelo D'Ambrosio14Marc van der Valk10,15 Dirk Posthouwer13,16
Dirk Posthouwer13,16 Robin Ackens17
Robin Ackens17 Henriette ter Waarbeek1
Henriette ter Waarbeek1 Teymur Noori14
Teymur Noori14 Elske Hoornenborg4,10,11
Elske Hoornenborg4,10,11Introduction: In the 2022 multicountry mpox (formerly named monkeypox) outbreak, several countries offered primary preventive vaccination (PPV) to people at higher risk for infection. We study vaccine acceptance and its determinants, to target and tailor public health (communication-) strategies in the context of limited vaccine supply in the Netherlands.
Methods: Online survey in a convenience sample of gay, bisexual and other men who have sex with men, including transgender persons (22/07-05/09/2022, the Netherlands). We assessed determinants for being (un)willing to accept vaccination. We used multivariable multinominal regression and logistic regression analyses, calculating adjusted odds ratios (aOR) and 95 percent confidence-intervals. An open question asked for campaigning and procedural recommendations.
Results: Of respondents, 81.5% (n = 1,512/1,856) were willing to accept vaccination; this was 85.2% (799/938) in vaccination-eligible people and 77.7% (713/918) in those non-eligible. Determinants for non-acceptance included: urbanization (rural: aOR:2.2;1.2–3.7; low-urban: aOR:2.4;1.4–3.9; vs. high-urban), not knowing mpox-vaccinated persons (aOR:2.4;1.6–3.4), and lack of connection to gay/queer-community (aOR:2.0;1.5–2.7). Beliefs associated with acceptance were: perception of higher risk/severity of mpox, higher protection motivation, positive outcome expectations post vaccination, and perceived positive social norms regarding vaccination. Respondents recommended better accessible communication, delivered regularly and stigma-free, with facts on mpox, vaccination and procedures, and other preventive options. Also, they recommended, “vaccine provision also at non-clinic settings, discrete/anonymous options, self-registration” to be vaccinated and other inclusive vaccine-offers (e.g., also accessible to people not in existing patient-registries).
Conclusion: In the public health response to the mpox outbreak, key is a broad and equitable access to information, and to low-threshold vaccination options for those at highest risk. Communication should be uniform and transparent and tailored to beliefs, and include other preventive options. Mpox vaccine willingness was high. Public health efforts may be strengthened in less urbanized areas and reach out to those who lack relevant (community) social network influences.
Mpox (formerly named monkeypox) outbreaks have been reported in non-endemic countries since May 2022 (1–3). Since the start until 6 December 2022, 82,088 confirmed cases of mpox, and 64 deaths, were reported worldwide, and 20,934 mpox cases from 29 EU/EEA countries, including 1,251 in the Netherlands (3, 4). Compared to the peak of reported cases (2,164 cases during week 29; 18–24 July 2022), there has been a decrease in the number of newly reported cases (by 98.8% during week 44) (3). Mpox cases during the outbreak were associated with transmission by sexual and intimate contact, and gay, bisexual and other men who have sex with men and transgender persons (GBMSM/TGP) who had multiple sexual partners had been disproportionally affected (1, 2). On July 23, 2022, the WHO Director-General declared the escalating global mpox outbreak a Public Health Emergency of International Concern (5). To address these outbreaks with the required urgency, countries applied preventive measures as active case finding, contact tracing, self-isolation, and quarantine. As mpox is caused by a virus similar to smallpox, smallpox vaccines are expected to prevent or reduce the severity of the mpox infection and onward transmission (6–8). Smallpox vaccine development has a long history, and during the outbreak, various countries had offered these vaccines as post-exposure vaccination (PEPV) to contacts of a mpox case and as primary preventive pre-exposure vaccination (PPV) (9). Scarce vaccine supplies challenge an equitable global and national public health response (10). Countries that do have available vaccines, including the Netherlands, have limited vaccine supply and did restrict access to PPV based on high risk of mpox exposure (11). To achieve a high vaccination coverage in people who have a high risk for exposure is important to control the spread of mpox. People's willingness to accept PPV is a vital step. An online survey in the European region conducted during the peak of the outbreak, in 32,902 users of gay dating apps, demonstrated high willingness to accept PPV in Northern [84.8–90.4%] and Western Europe [83.1–87.7%] and somewhat lower in South-Eastern [60.9–70.2%] and Eastern Europe [59.9–71.1%] (12).
For the design of successful public health strategies, it is key to know the relevant determinants for vaccine acceptance (13–15). Some of these determinants can inform the targeting of public health efforts to subgroups that have lower PPV acceptance. Other theory-based determinants can reflect the underlying beliefs for PPV acceptance and thereby can inform the tailoring of communication-messages.
We conducted an online survey in mpox unvaccinated GBMSM/TGP, around the start of the mpox PPV-program in the Netherlands (16). The survey evaluates willingness to accept PPV and its determinants, and it also asked persons for their recommendations in campaigning and PPV-program procedures. These insights will contribute to preparing for and the shaping of an equitable and inclusive public health response to an infectious diseases outbreak.
PEPV was already available at an earlier stage and the PPV program started at 25 July 2022 (11). The most affected large cities started, and in August, PPV activities were gradually rolled out throughout the country. A total number of vaccine doses were available to invite 32,000 people by personal email or letter, based on patient-registries of public health Center for Sexual Health (CSH), HIV outpatient clinics, or general practitioners (GP). PPV eligible were GBMSM/TGP participating in (or on a waiting list for) the national pre-exposure prophylaxis program for HIV (HIV-PrEP), were living with HIV and deemed at mpox risk by the HIV-nurse, or had according to a CSH registry in the past 6 months a sexually transmitted infection (STI) diagnosis (syphilis, gonorrhea, or chlamydia), were notified for STI/HIV, or had more than three sex partners (11).
A prospective online survey of which baseline data are reported (cross-sectional design). Respondents were recruited by convenience sampling via social media channels and “offline” at CSH, HIV outpatient clinics, and sex-on-premises venues. Details on recruitment channels are available in Supplementary material 1. Recruitment was from 22 July to 5 September 2022, around the early roll-out of PPV in the Netherlands. During the survey-period, vaccination was by subcutaneous route of administration.
People who were 16 years or older were eligible for participation. Participation started after providing informed consent to the study. Consent was also asked to respondents whether they agreed to be approached for later follow-up. The Medical Ethical Committee of Maastricht University waived ethical approval because the data were coded and were analyzed anonymously (METC 2022-3324). People who (ever) had sex with a man were included in analyses when they also reported (i) male sex or intersex and male, non-binary, genderfluid, or agender gender identity (GBMSM), or (ii) male sex and female gender identity, or female sex and male gender identity (TGP). See Figure 1 for the flowchart of included persons in the study population.
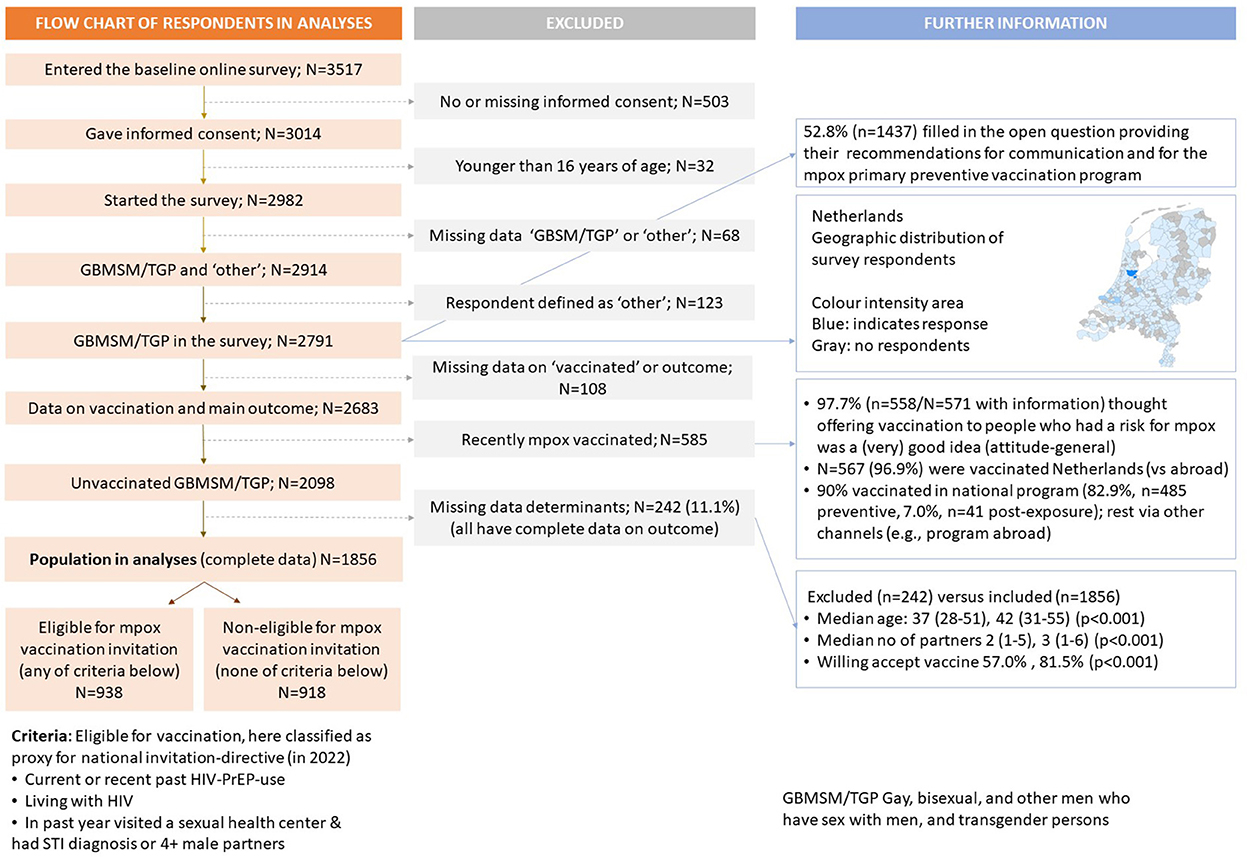
Figure 1. Flow chart of the number of respondents in the Dutch online mpox-survey.
The questionnaire was available in Dutch and English, and its development was informed by a community consultation. Details on variables and their order (e.g., the questionnaire assessed willingness at the start) are available in Supplementary material 2.
Intention is operationalized as willingness to accept PPV when offered, by the statement “If you could receive a vaccine against mpox, would you get vaccinated against mpox?” with response options 1–5 (Likert scale), “No, certainly not,” “No, probably not,” “Neutral,” “Yes, probably,” “Yes, certainly.” As a secondary outcome, willingness to accept PEPV was assessed (same Likert scale) by the statement “Suppose you had sex with someone with mpox, would you get vaccinated?”.
Sociodemographic, medical, social environment factors, and behaviors were considered as important determinants to inform the targeting of strategies to determinant-subgroups with higher PPV non-acceptance.
Socio-cognitive determinants such as attitudes, cognitions, and perceptions (here called: beliefs) may influence willingness to accept vaccination (17–21). Beliefs are reputed modifiable by tailored communication-messages. Beliefs were presented in Supplementary material 2, and include (i) perceived risk, severity, and concern about mpox, (ii) motivation/perceived importance to protect against mpox, (iii) perceived response efficacy of vaccination, and (iv) perceived norms/social influence. Beliefs were selected based on their relevance at the time of survey-design before PPV-program start. All were theory-based derived from the Protection Motivation Theory, Health belief model, and Theory of Planned Behavior (18–20).
To collect non-guided insights in mpox communication and procedural preferences from GBMSM/TPG participants, an open question was included stating “What do you think is important in communication about vaccination against Mpox? You can, for example, indicate what and how, in your opinion, organizations can best communicate about this to people, or where you would like to get the vaccine.”
Respondents were categorized as likely PPV “eligible” or “non-eligible,” which is a best proxy for the actual Dutch directive for PPV-eligibility (11). Categorization was based on self-reported information only (not clinic registry information) and based on similar criteria as in the directive (exact criteria were not known at the time of survey-design) (11). Respondents were categorized as “eligible” when they reported (i) HIV-PrEP use in the past 3 months or longer ago, (ii) living with HIV (regardless of antiretroviral therapy use or sexual behavior), or (iii) visited a CSH in the past year and reported a diagnosis of chlamydia, gonorrhea, or syphilis in the past year or reported more than three male sex partners in the past 3 months. All other respondents not reporting any of these criteria were categorized as PPV non-eligible.
Analyses were performed for the entire group, and for eligible and non-eligible respondents. Firstly, descriptive statistics were provided on study population characteristics. Secondly, we provided descriptive statistics on the outcomes of this study, by its five categories and a priori regrouping into three categories, i.e., willing to accept PPV (certainly willing and likely willing), neutral, and unwilling (likely and certainly not willing). Thirdly, we evaluated non-modifiable determinants that could serve as targets of prevention strategies. Evaluated were categorical sociodemographic, medical, social environment, and behavior factors (Supplementary material 2). Using univariable multinominal logistic regression analyses, the odds for being unwilling or neutral were expressed for each of the variable-categories compared to the reference category, calculating odds ratios (ORs) and 95 percent confidence intervals (CI). For multivariable analyses, we used a bidirectional stepwise procedure to identify the most important determinants. The bidirectional stepwise procedure started by a forward approach followed by backward elimination (variables with p<0.05 could stay in the model) and repeating these steps (including initial variables) until no new variables were added. This procedure was performed for the entire study population, those eligible and those non-eligible for PPV. In sensitivity analyses, we added calendar week and channel of recruitment to the multivariable models and these recruitment factors appeared not associated (Supplementary material 3). Fourthly, we aimed to identify key beliefs (Supplementary material 2) to inform tailoring of communication-strategies. In those eligible and in those non-eligible for PPV, we used univariable logistic regression analyses, expressing the odds of being willing to accept vaccination, for each point increase on the beliefs-scores. As aim was to assess all relevant modifiable targets to inform tailoring of communications, a separate multivariable model was constructed for each belief, adjusting for identified important non-modifiable determinants. Across analyses, we considered a P < 0.05 as statistically significant. All analyses were performed using SPSS package vs24 (IBM Corp., Armonk, New York, USA).
Answers were assessed (ND, YE) and categorized into main themes that arose from the answers (inductive coding). Saturation in the answers had been reached. Comments were described per theme and illustrated with examples of citations, and where possible linked to theoretical evaluated beliefs and other determinants (deductive coding).
Of the 2,683 GBMSM/TGP respondents, 2,098 were unvaccinated for mpox of whom 1,856 (88.5%) completed the survey and 242 not completed the survey. This latter group was younger, had fewer recent sex partners, and were more often unwilling/neutral to PPV acceptance, compared to those who completed the survey (Supplementary material 4).
Of 1,856 unvaccinated respondents included in analyses, 84% were born in the Netherlands, 23% lived in moderate urban to rural areas, 25% had a low/medium educational level, and median age was 42 (Table 1).

Table 1. Characteristics of the study population who are unvaccinated for mpox; GBMSM/TGP participating in Dutch online mpox-survey (22 July-5 Sept 2022).
Of 938 PPV eligible respondents, 52% used HIV-PrEP and 24% were living with HIV (96% used ART) (Table 1). 28% knew someone who had mpox, 45% knew someone who was vaccinated against mpox, 38% lacked connectedness to the gay/queer-community, and over the past 3 months 40% reported group sex, 66% reported unprotected anal intercourse (UAI) during casual sex, and 70% reported more than three sex partners.
Of 918 PPV non-eligible respondents (HIV negative/untested; none used HIV-PrEP), 82% not attended a CSH in the past year, 48% lacked connectedness to the gay/queer-community, and over the past 3 months 15% reported group sex, 23% reported UAI during casual sex, 25% reported more than three sex partners (none engaged in SHC care), and 12% used drugs during sex.
Of respondents, 81.5% were willing to accept vaccination; this was 85% in those PPV eligible and 78% in those non-eligible (Table 2). Of respondents, 12% were unwilling to accept vaccination; this was 10% in those eligible and 13.5% in those non-eligible. The remaining respondents (7; 5, 9%) were neutral. Of respondents, 90% were willing to accept PEPV; this was 90% in those PPV eligible and 90% in those non-eligible (Table 2).
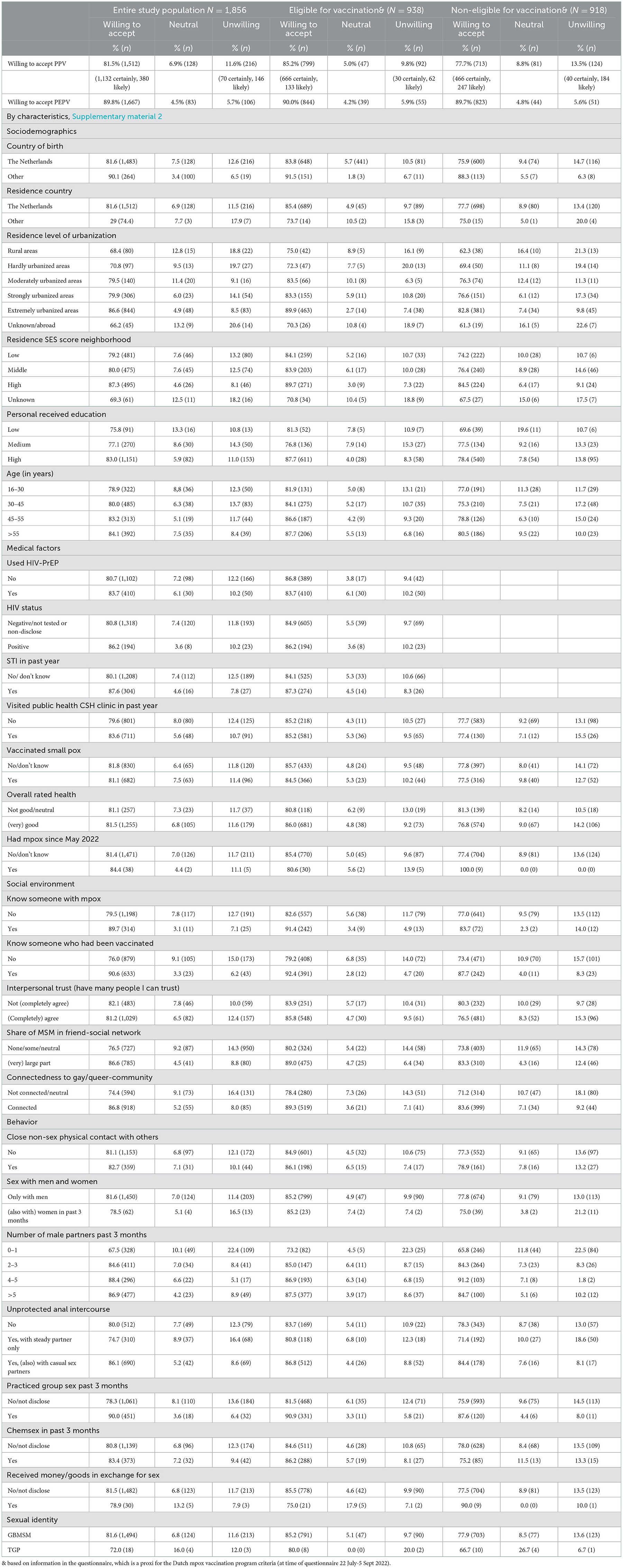
Table 2. Proportion of respondents who reported (certainly or likely) willing to accept vaccination when offered, those who were neutral, and those who were reporting (likely or certainly) not willing to accept vaccination after being invited, by population subgroups, GBMSM/TGP participating in Dutch online mpox-survey (22 July-5 Sept 2022).
Proportions of respondents being willing to accept PPV, neutral, or unwilling were presented for each of the determinant-subgroups in Table 2.
The odds of being unwilling/neutral (vs. being willing) were higher for those born in the Netherlands, who live in lower urbanized areas, or in lower socioeconomic status neighborhoods, who have lower educational level (for “neutral” only), or younger age (for “unwilling” only), who are HIV negative/untested (for “neutral” only), had past STI diagnosis, did not know a person with mpox or vaccinated for mpox, not had many MSM-friends in their friend-networks, lacked connectedness to the gay/queer community, had at most one recent sex partner, always used condoms/or practiced UAI only with a steady partner, or not recently had group sex (Supplementary material 5).
These associated determinants were observed in the entire population; these were also observed in PPV-eligible respondents (except for neighborhood socioeconomic status, age, HIV and STI status, and UAI) and in non-eligible respondents [except for educational level, age, and STI (HIV not evaluated)] (Supplementary material 5).
The odds of being unwilling/neutral to accept PPV were higher for those born in the Netherlands, who live in lower urbanized areas, not knew mpox-vaccinated people, lacked connectedness to the gay/queer community, or who had at most one recent sex partner (Figure 2). These determinants increased odds for both “unwilling” and “neutral” in the entire population and these same determinants were found associated in PPV-eligible and in non-eligible respondents (Figure 2). For those eligible, being born in the Netherlands increased odds only for “neutral” and having at most one partner increased odds only for “unwilling.” For those non-eligible, being born in the Netherlands, live in less urbanized areas [just borderline significant], or lack of connection to the gay/queer community only increased odds for “unwilling.”
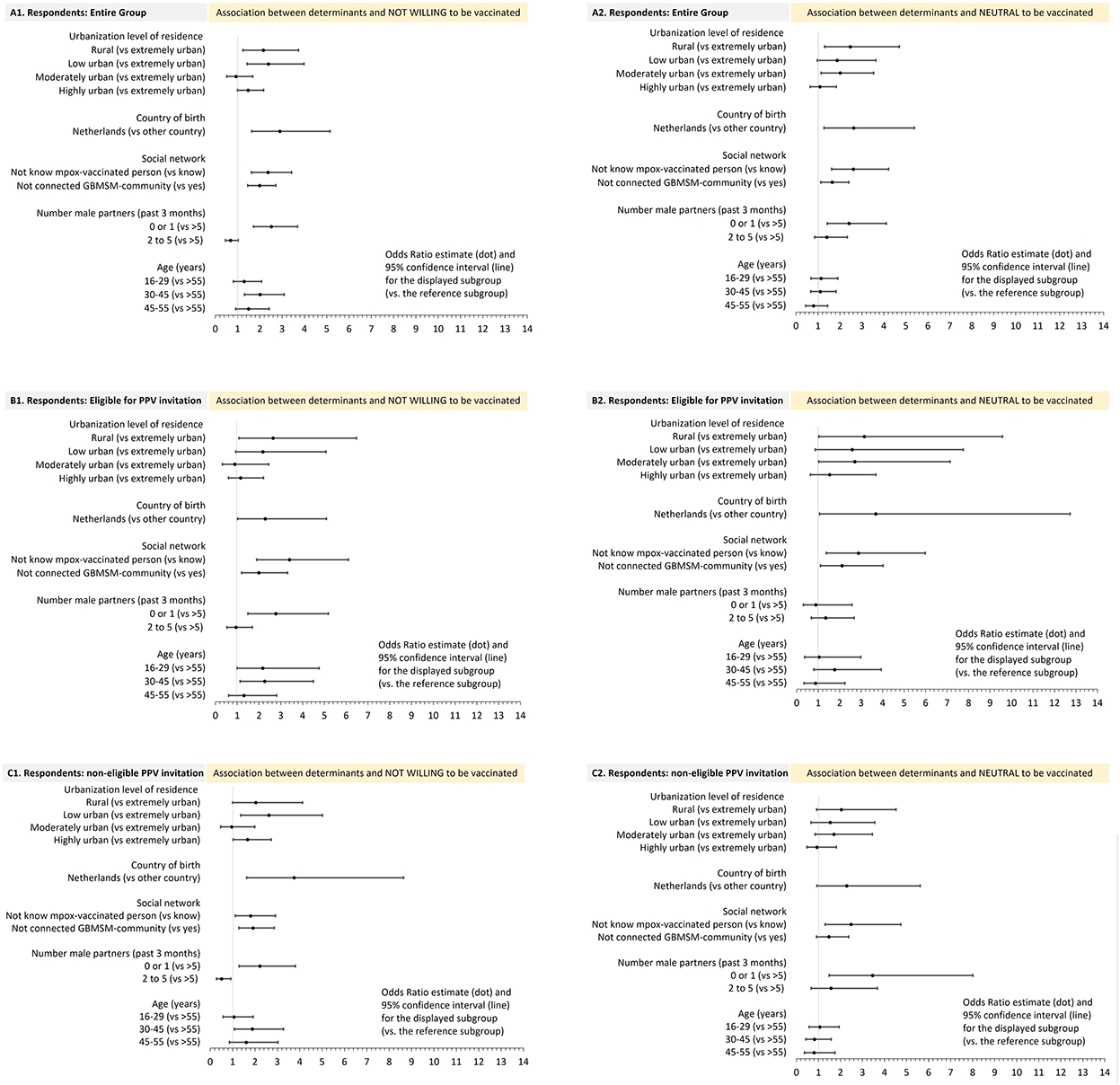
Figure 2. Sociodemographic, social environment, and behavioral determinants and their association with being not willing, or neutral, to accept mpox vaccination when offered, (compared to being willing), in multivariable multinominal regression analyses, mpox unvaccinated GBMSM/TGP participating in the Dutch online mpox-survey (22 July-5 Sept 2022). (A1, A2) entire group; (B1, B2) PPV eligible; (C1, C2) PPV non-eligible.
Figure 2 presents the distribution of the response scores (1–5), for each belief. The proportion and number of respondents with a score of 4 or 5 were as follows:
(i) Perceived risk, severity and concern about mpox: 32.9% (n = 309) of eligible respondents and 13.0% (n = 119) of non-eligible respondents considered themselves at risk for mpox, 69.7 and 67.2% thought that symptoms could be severe, and 58.5 and 41.8% were concerned about acquiring mpox.
(ii) Motivation/importance to protect against mpox: 87.3% of PPV eligible respondents and 79.8% of those non-eligible considered it important to protect themselves from mpox, 82.8 and 71.8% considered it important to be mpox vaccinated, 93.3 and 91.1% stated that vaccinating people with high risk was a good idea.
(iii) Perceived response efficacy of mpox vaccination: 87.6% of eligible and 86.9% of non-eligible respondents expected to be protected by the vaccine, 45.1 and 45.0% (score 1 or 2) did not expect severe side effects of vaccination, 81.1 and 80.6% had trust in information about mpox vaccine as provided by Dutch institutions.
(iv) Perceived social norms: 73.0% of eligible and 67.6% of non-eligible respondents thought the gay/queer community was concerned about mpox, 72.9 and 58.3% thought that many/most in their social network considered mpox vaccination important, 70.9 and 59.0% thought many/most in their social network would get mpox vaccinated, and 30.9 and 15.5% stated that they often discussed vaccination with others.
In both PPV eligible and non-eligible respondents, all evaluated beliefs were associated with being willing to accept PPV in both univariable (Supplementary material 6) and multivariable (Figure 3) logistic regression analyses. Multivariable models adjusted for country of birth, urbanization level, knowing mpox-vaccinated persons, connectedness to the gay/queer community, and number of sex partners.
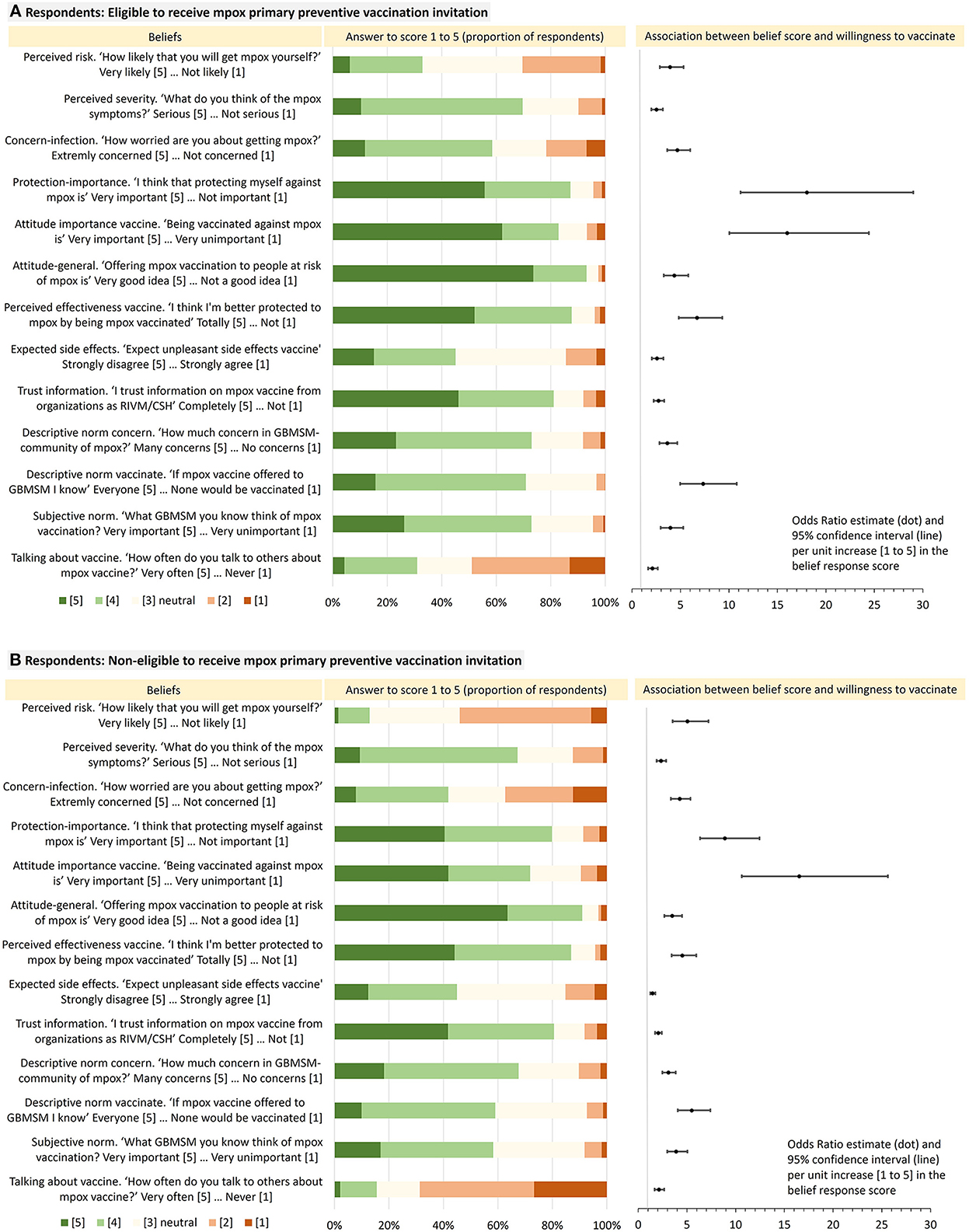
Figure 3. Distribution of responses to belief-statements in respondents who are eligible to receive PPV-invitation and those non-eligible (left), and the odds for each of these beliefs (right) for their association with being willing (certainly or likely) to accept mpox vaccination when offered (compared to not willing/being neutral), in multivariable logistic regression analyses, mpox unvaccinated GBMSM/TGP participating in Dutch online mpox-survey (22 July-5 Sept 2022).
A total of 1,437 (52.8%) respondents filled in the open question to give their recommendations and two main themes arose from the answers, which were communication about mpox and the PPV program and were related to (lifting) barriers regarding the access to information and to PPV.
Respondents recommended to provide information about mpox to increase public awareness/knowledge and to improve appraisal of personal risk and severity. Respondents mentioned the importance of communicating both pros and cons of mpox vaccination, degree of protection conferred, and the development of the vaccine (“What is the vaccine made from, and history of developing it, is it safe and reliable”) and also how vaccination relates to other mpox prevention strategies (“What can we do to protect ourselves besides vaccination? Why is vaccination the best option?”). Participants suggested to also explain other mpox preventive options but not advocating abstinence. Explain the goal of the PPV-program (note: public health goal of PPV is to limit mpox spread). Such communications could stimulate a positive attitude toward mpox vaccination and increase response efficacy of mpox vaccination, as well as protection by other preventive strategies.
Respondents stated the importance of non-stigmatizing language, such as linking infection risks to behaviors (such as multiple sexual partners), not to sexual orientation (“it is not a gay disease”). It was found important to be more transparent and factual in communication (“Honest, open information, don't beat around the bush”; “Give facts, statistics”).
For optimal access to information for all people at high risk, respondents recommended to use mainstream media to underpin the importance of mpox and use public media to reach more “hidden” target groups (“Announce it publicly just like you give vaccination against COVID-19”), while others suggested community-specific channels (“Communication through gay social media”). Respondents labeled discrepant information content across channels as disruptive, and they recommended more uniformity in communication-messages across the different communication channels, also have a central website, and with more frequent provision.
Respondents asked for more transparent information on who was eligible and when invited. Often respondents mentioned that the operational information around PPV was unclear and differed between healthcare providers (“It was unclear where and when I would receive my invitation for the vaccination”). They also asked to communicate who is non-eligible and what is the prospect of receiving PPV later for the non-eligible person.
Participants stated that the clarity and uniformity in both the information and in the PPV procedures across healthcare settings and geographical regions could be improved [“people who are in the PrEP program of the GGD (CSH) get priority over people who get PrEP through their GP”].
Respondents commented to improve PPV access and self-efficacy, with low-threshold options to get vaccinated. They recommended “self-registration” (“It's a pity that you can't sign up for vaccination”) in addition to personal invitations. Respondents suggested to offer vaccination at various clinic-and non-clinic settings, also outside the region of residence, including anonymous and discrete PPV options, in neighborhoods where people live (reduce travel distance), and where people get together (“Gay hangout places. But also, a mobile driving van on weekend party places. GP should be better informed and able to vaccinate and make it easier for access”), to offer vaccination at Hiv clinic, or to offer vaccination as done “with COVID-19,” “at test streets” or as is routinely done during a the CSG visit (“as with Hepatitis B”).
Respondents expressed concern that people with high risk for exposure are currently not invited for vaccination. For more inclusive vaccination-access, respondents frequently recommended to make PPV available for a broader group of people who had high risk. They mentioned to include people who not disclosed risk behavior to a healthcare professional or those who not engaged in preventive healthcare, and to offer PPV based on people's willingness, rather than on categorization of people into subgroups (“That anyone who wants a vaccine, can get the vaccine, not just HIV+ and PrEP users”). Respondents recommended to speed-up vaccination.
Other quotes regarding mpox communication and mpox PPV program are shown in Table 3.
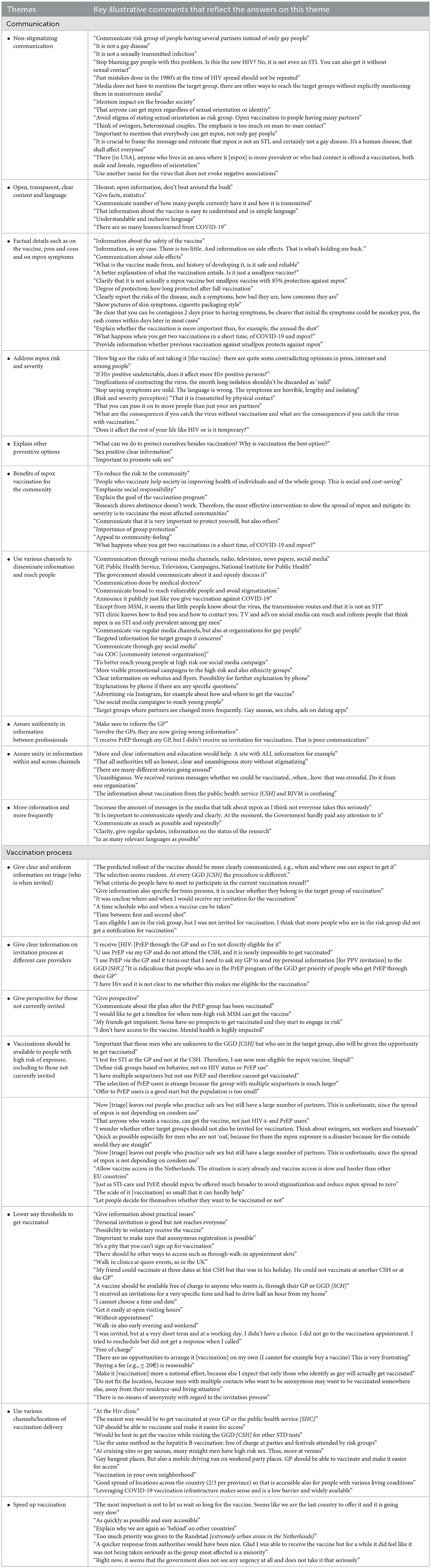
Table 3. Recommendations for health-professionals and institutions to communicate on mpox vaccination and the mpox vaccination program, according to GBMSM/TGP participating in Dutch online mpox-survey (22 July-5 Sept 2022).
This survey was conducted during the 2022 multicountry mpox outbreak at the start of the national mpox PPV program in the Netherlands. This research in a convenience sample of GBMSM/TGP, assessed willingness and associated determinants for PPV (non-)acceptance, and collated respondents' recommendations on campaigning and PPV-procedures, to inform inclusive and equitable strategies in the public health response to the mpox outbreak.
Willingness to accept vaccination in this sample was high with 81.5% (86% in PPV eligible respondents). Another Dutch survey recruiting early July 2022 had observed 70% PPV willingness (21), which was confirmed in the current study showing 73% in the early recruitment at the end of July (Supplementary material 3). A large-scale European survey recruiting in the first half of August, observed 85–90% (northern countries) and 83–88% (western countries) (12), in line with our current Dutch study showing 86% PPV willingness in the first half of August. It should be noted that willingness fluctuated without showing an independent time trend. Fluctuations in vaccine acceptance over time are known to occur in an unfolding epidemic, with changing vaccine availability, media coverage, and number of vaccinated people and of cases over time, as was demonstrated for COVID-19 (23).
In the evolving public health response, strategies can be further optimized to ensure broad access to information for all people, and low threshold access to vaccination for people with high risk for mpox.
The beliefs found important in mpox PPV acceptance were in line with those important in COVID-19 vaccination acceptance and in previous surveys on mpox PPV acceptance (15, 22–24). These beliefs included perceived risk/severity, motivation to protect against infection, perceived response efficacy of PPV, and perceived social norms. Of PPV-eligible respondents a third felt at risk (another third not felt at risk), over half were concerned, and majority (70%) thought that mpox symptoms could be severe. Majority of respondents (over 80%) were motivated to prevent mpox and also were positive about PPV but varied in their expectancy of side effects. Public health communication messages should include factual information on mpox (exposure risk, transmission routes, symptoms) and on the vaccine (side-effects, degree of protection for oneself and the community, history of development). This should help a person who has high risk for exposure to feel at risk and appraise mpox as potentially serious and PPV as beneficial in balance with risks of vaccinating (possible side effects) and of not vaccinating (health-and social impact of having mpox for self and others). Communications can address current uncertainties, such as around vaccine-effectiveness, and be clear that such uncertainty is well-weighted in the PPV-program choices.
People need to have access to relevant facts to be able to make an informed autonomous choice (23). Communication-messages should include information on PPV-program affairs (“who, where, and when” to increase self-efficacy to get PPV).
Communication may further address perceived social norms. Most respondents (71–73%) thought that the gay/queer community was concerned about mpox and that those people they knew deemed PPV as important and would accept PPV. It is notable that part of PPV-eligible respondents never (13%) or only sometimes (36%) discussed vaccination with others. Discussions with social network members can be helpful to encourage preventive behavior, but people might expect or experience difficulties in talking to network members about mpox prevention. Previous research on STI testing learned that people may anticipate negative reactions (public stigma) and shame (self-stigma) when discussing STI and testing, and they avoid stigma by choosing to disclose only to single/few trusted peers (selective disclosure) (25). Difficulties to discuss mpox vaccination might also arise in relation to unequal and unclear vaccine-access. It is important that information is transparent and clear about triage. Further, public health mpox communication strategies might be designed to encourage a person to talk about mpox prevention with a close trusted person and be designed to leverage possible difficulties to enable discussion of the topic in the wider community.
Messages can be delivered with the personal PPV invitation/reminder, which is the moment when the actual choice for PPV is made. Other channels include social media or websites which offer further benefits such as ease of maximizing dose and frequency of information exposure, and attractive (visual) tailoring to address problematic beliefs, to support decision making, norm setting, and maintenance of helpful beliefs over time (23). Most (81%) respondents in the current survey trusted information from the institutions. They recommended multiple channels to disseminate information, including mainstream media, general health websites, at clinics, at venues (where people get together), and using specific community-based channels. Respondents thereby urged to pay attention to uniformity in the information across the different channels. Information-diffusion could also be promoted by the community itself in peer-to-peer activities, although this may be less suited to reach disconnected people. Any channel chosen to reach people eligible for PPV will also reach persons currently non-eligible for PPV and thus communication should also include messages to address prevention needs of people non-eligible for PPV (explained below).
Low-threshold options to get vaccinated will increase the accessibility and thereby the use of PPV. To lift possible (regional-specific) barriers for PPV-invited people, respondents suggested to bring vaccination facilities close to a person's home, provide vaccination at venues where people get together, offer discrete (anonymous) vaccination, provide vaccination at the sexual health check-up, and offer the option to actively self-register for getting a vaccination, in addition to a personal invitation for PPV.
Subgroups less likely to want vaccination were defined by where they were born and live (born in the Netherlands, live in less urbanized areas), their social networks (no mpox-vaccinated social network members, lack of connection to a gay/queer community), and by their sexual behavior (at most one recent partner). Those who live in less urbanized areas and those who lack connection to a gay/queer community might benefit from strengthened public health efforts tailored to their context. Disparities by urbanization level in mpox PPV uptake and in other mpox mitigation strategies were demonstrated in two US studies (26, 27), and were also observed in HIV testing uptake (28). Local stakeholder networks, community based organizations and local communities can be engaged to maximize access to information (for all) and access to PPV (for those at highest risk). Respondents who lacked connectedness to the gay/queer community were less likely to want PPV, in line with research findings on HIV testing and COVID-19 testing uptake (28, 29). Disconnected people are also known to less engage in preventive healthcare. Social connectedness is a strong factor in health and driver of prevention, as people may be supported by their peers and peers can be behavioral role-models (30–32). Additional public health outreach efforts are needed to inform people who have a high risk of exposure and lack connection to a gay/queer community or to care; they may, according survey-respondents, include bisexual men, sexworkers, migrant people, very young GBMSM/TGP, and those who not disclose as GBMSM/TGP including male swingers.
People who did not receive a mpox PPV invitation had unmet needs regarding the prevention of mpox. Most PPV-non-eligible respondents in our survey did not engage in CSG/hospital care (GP was not asked for) and some reported recent group sex (15%), UAI in casual sex (23%), more than three sex partners (25%), or chemsex (12%). In the Netherlands, the PPV program aims to target people at highest risk for mpox and specifically people with multiple sexpartners. In practice, access to PPV is organized by sending personal invitation based on information as available in existing patient registries (11). While this allows to reach people in a relatively quick and feasible way, such strategy excludes those people at risk who not engaged in healthcare or had missing registry information.
Survey-respondents asked for a more inclusive PPV-access. In a US study among persons who not received mpox vaccination, more than a quarter had tried to get vaccinated (27). In current study, vaccine-non-eligible respondents showed concern about acquiring mpox (42%), wanted to protect themselves against mpox (80%), and would accept PPV when offered (78%). It is important to explore public health activities that allow low-threshold access to PPV, also for people who have high risk but who were not in existing invitation-selections.
The US and other countries had realized expansion of the number of people that can receive PPV, by application of intradermal injection, after FDA and EMA has approved its use (33, 34). However, intradermal injection will not be implemented in the Netherlands, as was stated in a recent policy brief (35). In addition to low threshold vaccine offers, well-designed communication-strategies have a crucial role in ensuring an equitable and inclusive access to information and access to preventive care options. In the challenging context of limited vaccine supply, transparent and uniform communication about triaging is especially important (36). As recommended by respondents, for all people who have a risk for exposure to mpox, regardless PPV-eligibility, information should be actively provided and easily accessible, with specific, non-stigmatizing and sex-positive guidance to enable people to act on the various mpox mitigation and care options (e.g., seek care for symptoms, and reduce close/intimate contact exposure risks) to prevent mpox acquisition, morbidity, and spread.
Important subgroups, such as very young people, people with lower educational level, bisexual men, sexworkers, and TGP were underrepresented in this study, just as they are underrepresented in care. The sample is a convenience sample and not representative for all GBMSM/TGP in the Netherlands. Therefore, the main limitation is external validity, limiting generalizability of the overall proportion of willingness to vaccinate to the wider target population of GBMSM/TGP. We cannot rule out selection bias toward including respondents with a more positive attitude to PPV than the “general” GBMSM/TGP population. Strategies were taken to minimize selection bias and not to influence participation-interest or answers on beliefs, such as keeping communications in the survey text to strict a minimum. Further, selection bias might have been introduced by differential drop-out of younger people who had fewer sexual partners (Supplementary material 4). That drop-outs were more often non-accepting of PPV was in line with the more frequent PPV non-acceptance observed in respondents with few sexual partners in the survey (Table 2). Furthermore, it should be noted that overall retention in this online survey was high with 89%.
An important general limitation hampering the guidance on public health mpox preventive actions, is the lack of reliable (national, regional or subpopulation level) data on the number of people invited and vaccinated among invitees.
The study sample was substantial, and respondents had representation across a variety of subgroups and geographic areas. Another strength includes the timing of the survey and the assessment of a wide range of determinants at the early start of vaccination roll-out, which provided timely data to improve preventive strategies during the mpox vaccination program. A further asset is the theoretical underpinning of the research using a combination of theoretical behavioral change models to define determinants for PPV behavior. Triangulation was applied of quantitative data on determinants and qualitative data on campaigning and procedural aspects of the PPV-program. Finally, a major strength of this study was the highly diverse and complementary composition of the research team, including scientists from fields of epidemiology, behavioral science, intervention design, implementation research, communication experts from public health centers and community-based organizations, and healthcare professionals who serve the target population. In the context of a new epidemic and its public health response, this team-collaboration made it possible to quickly collect and process data, followed by immediate communication to policy makers and those involved in mpox prevention and PPV-program activities.
In the 2022 multicountry mpox epidemic, primary preventive pre-exposure vaccination of people at high risk was a key public health measure. Peoples' willingness to be vaccinated was high and they recommended low threshold options to get vaccinated, alongside clear, uniform and factual information. See for a visual summary of the findings, Figure 4. Public health efforts may be strengthened for those at risk but less likely to want vaccination, by regional approaches in less urbanized areas or outreach strategies for people who lack connection with the gay/queer community. Communication strategies will benefit from belief-tailored messages that are also transparent and uniform and provide non-stigmatizing guidance for mitigation and healthcare options. In the context of an outbreak, public health strategies should be particularly careful to maintain equitable and inclusive access to broad preventive information and care options.
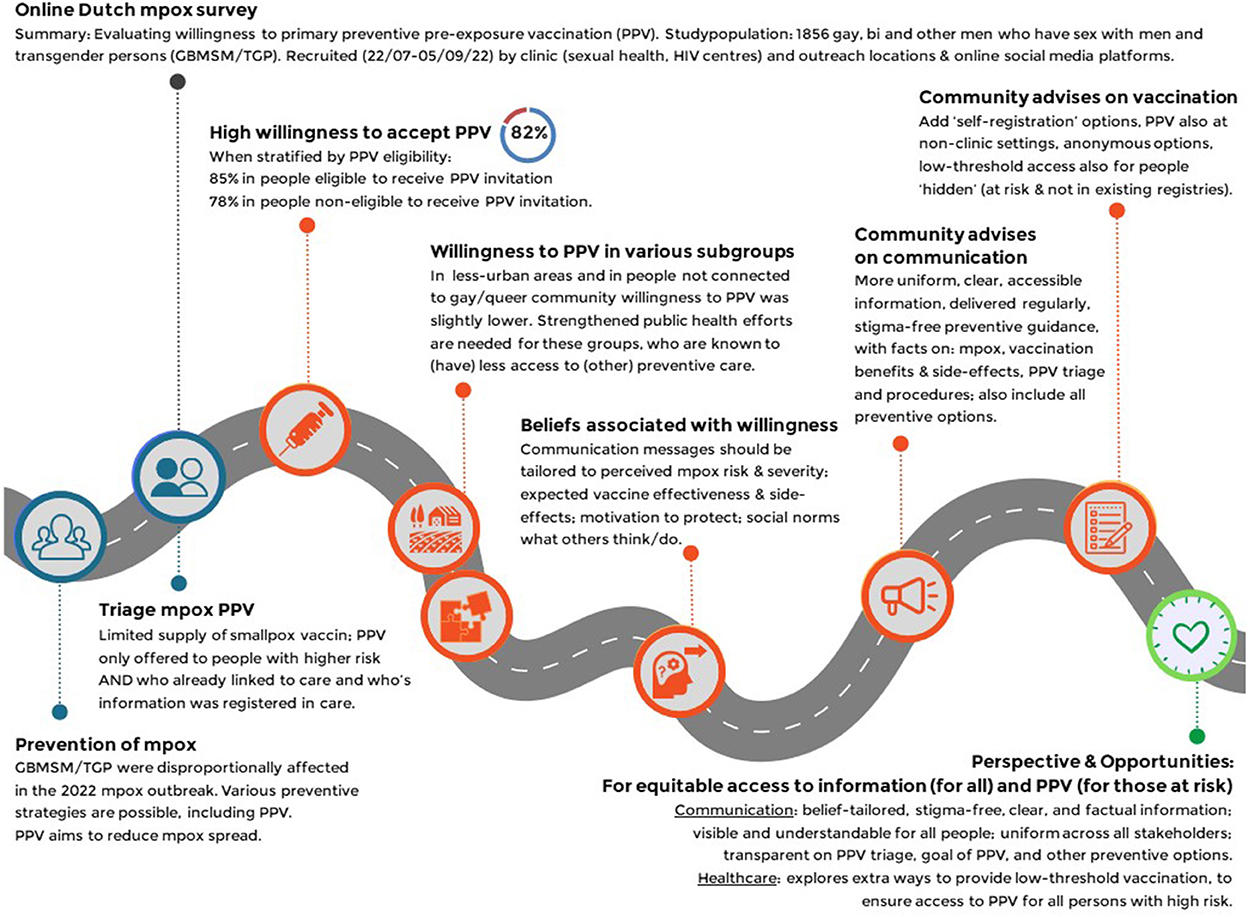
Figure 4. Visual summary of the study findings and conclusion. Dutch online mpox-survey (22 July-5 Sept 2022).
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Medical Ethical Committee of Maastricht University waived ethical approval because the data were coded and were analyzed anonymously (METC 2022-3324). People who were 16 years or older were eligible for participation. Participation started after providing informed consent to the study. Respondents were also asked whether they consented to be approached for later follow-up. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
ND-M drafted the report and performed the statistical analyses. YE, FS, and AD'A contributed to statistical analysis. ND-M, YE, FS, CHe, A-MN, AM, UD, EH, and FS contributed to design of the survey. ND-M and YE coded the qualitative data [on respondents recommendations]. All authors reviewed the results, provided guidance, drafted, reviewed, and provided critical feedback on the report.
We are grateful to the following people and organizations for involvement in the recruitment of study participants: DC klinieken Lairesse Amsterdam (Hans-Erik Nobel), MUMC+ Department of infectious diseases, CSH Amsterdam (Adriaan Tempert and Justin Luidens), CSH South Limburg (Angelique Lahaut, Rocxanne Theuerzeit, Marita Werner, Ronald van Hooren), CSH Northern Limburg, CSH Utrecht (Mark van den Elshout), CSH Rotterdam-Rijnmond (Masja van der Pas and Charlotte Lantinga), CSH Gelderland-Zuid (B. Pool), CSH Ijsselland (Janine van den Brink), COC Limburg (Manuel Spier), Noordwest Ziekenhuisgroep (Frieda von Truien), and sex on premises-venues Limburg. Further, we are in depth to facilitating online social media recruitment to STI AIDS Netherlands (Sjoerd Visser and Laurian Kuiper), and John de Wit from University Utrecht for fruitful discussions, Kevin Konings for providing assistance with the data analyses, and Rianne Wit, Sabine Steins, and Lisanne Steijvers for visualization. We are indebted to our community-panel members for collaboration in designing this study. Finally, we thank all participants for contributing with their invaluable comments and responses. This work is available as Preprint: Dukers-Muijrers et al. (16).
PZ was employed by Soa Aids Nederland.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1058807/full#supplementary-material
1. Thornhill JP, Barkati S, Walmsley S, Rockstroh J, Antinori A, Harrison LB, et al. Monkeypox virus infection in humans across 16 countries - April-June 2022. N Engl J Med. (2022) 387:679–91. doi: 10.1056/NEJMoa2207323
2. Vaughan AM, Cenciarelli O, Colombe S, Alves de Sousa L, Fischer N, Gossner CM, et al. A large multi-country outbreak of monkeypox across 41 countries in the WHO European Region, 7 March to 23 August 2022. Euro Surveill. (2022) 27:2200620. doi: 10.2807/1560-7917.ES.2022.27.36.2200620
3. European Centre for Disease Prevention Control. Epidemiological Data on the 2022 Monkeypox Outbreak. Available online at: ‘https://www.ecdc.europa.eu/en/monkeypox-outbreak' (accessed December 7, 2022).
4. Mathieu E, Spooner F, Dattani S, Ritchie H, Roser M. “Monkeypox”. Published online at OurWorldInData.org (2022). Available online at: https://ourworldindata.org/monkeypox (accessed December 7, 2022).
5. World Health Organization. News. Available online at: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed September 26, 2022).
6. Hammarlund E, Lewis MW, Carter SV, Amanna I, Hansen SG, Strelow LI, et al. Multiple diagnostic techniques identify previously vaccinated individuals with protective immunity against monkeypox. Nat Med. (2005) 11:1005–11. doi: 10.1038/nm1273
7. Poland GA, Kennedy RB, Tosh PK. Prevention of monkeypox with vaccines: a rapid review. Lancet Infect Dis. (2022) 22:e349–58. doi: 10.1016/S1473-3099(22)00574-6
8. Petersen E, Zumla A, Hui DS, Blumberg L, Valdoleiros SR, Amao L, et al. Vaccination for monkeypox prevention in persons with high-risk sexual behaviours to control on-going outbreak of monkeypox virus clade 3. Int J Infect Dis. (2022) 122:569–71. doi: 10.1016/j.ijid.2022.06.047
9. World Health Organization. Vaccines and Immunization for Monkeypox: Interim Guidance, 24 August 2022. Available online at: https://www.who.int/publications/i/item/WHO-MPX-Immunization-2022.2-eng (accessed September 26, 2022).
10. Nuzzo JB, Borio LL, Gostin LO. The WHO declaration of monkeypox as a global public health emergency. JAMA. (2022) 328:615–7. doi: 10.1001/jama.2022.12513
11. National Institute for public health the environment Netherlands. Public Information Vaccination Monkeypox. Available online at: https://www.rivm.nl/monkeypox-apenpokken/vaccinatie (accessed September 9, 2022).
12. Reyes-Urueña J, D'Ambrosio A, Croci R, Bluemel B, Cenciarelli O, Pharris A, et al. High monkeypox vaccine acceptance among male users of smartphone-based online gay-dating apps in Europe, 30 July to 12 August 2022. Euro Surveill. (2022) 27:2200757. doi: 10.2807/1560-7917.ES.2022.27.42.2200757
13. Fernandez ME, Ruiter R, Markham CM, Kok G. Intervention mapping: theory- and evidence-based health promotion program planning: perspective and examples. Front Public Health. (2019) 7:209. doi: 10.3389/fpubh.2019.00209
14. Kok G. A practical guide to effective behavior change: How to apply theory- and evidence-based behavior change methods in an intervention. Eur Health Psychol. (2014) 16:156–70.
15. Ten Hoor GA, Varol T, Mesters I, Schneider F, Kok G, Ruiter R. Just-in-time, but still planned: lessons learned from speeding up the development and implementation of an intervention to promote COVID-19 vaccination in university students. Health Promot Pract. (2022). doi: 10.31234/osf.io/r8yzs
16. Dukers-Muijrers NH, Evers Y, Widdershoven V, Davidovich U, Adam PCG, Op de Coul ELM, et al. Monkeypox vaccination willingness, determinants, and communication needs in gay, bisexual, and other men who have sex with men, in the context of limited vaccine availability in the Netherlands (Dutch MPX-survey). MedRxiv. (2022). doi: 10.1101/2022.10.11.22280965
17. Rogers RW. A protection motivation theory of fear appeals and attitude change. J Psychol. (1975) 91:93–114. doi: 10.1080/00223980.1975.9915803
18. Rogers RW. Cognitive and physiological processes in fear appeals and attitude change: a revised theory of protection motivation. In:Cacioppo J, Petty R, , editors. Social Psychophysiology New York, NY: Guilford Press (1983).
19. Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley (1975).
20. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-T
21. Luger TM. Health beliefs/health belief model. In:Gellman MD, Turner JR, , editors. Encyclopedia of Behavioral Medicine. New York, NY: Springer (2013).
22. Wang H, d'Abreu de Paulo K, Gültzow T, Zimmermann H, Jonas KJ. Monkeypox self-diagnosis abilities, determinants of vaccination and self-isolation intention after diagnosis among MSM, the Netherlands, July 2022. Euro Surveill. (2022) 27:2200603. doi: 10.2807/1560-7917.ES.2022.27.33.2200603
23. Sanders JG, Spruijt P, van Dijk M, Elberse J, Lambooij MS, Kroese FM, et al. Understanding a national increase in COVID-19 vaccination intention, the Netherlands, November 2020-March 2021. Euro Surveill. (2021) 26:2100792. doi: 10.2807/1560-7917.ES.2021.26.36.2100792
24. Varol T, Schneider F, Mesters I, Ruiter R, Kok G, Ten Hoor GA. Facilitating informed decision making: determinants of university students' COVID-19 vaccine uptake. Vaccines. (2022) 10:704. doi: 10.3390/vaccines10050704
25. Theunissen KA, Bos AE, Hoebe CJ, Kok G, Vluggen S, Crutzen R, et al. Chlamydia trachomatis testing among young people: what is the role of stigma? BMC Public Health. (2015) 15:651. doi: 10.1186/s12889-015-2020-y
26. Hubach RD, Owens C. Findings on the monkeypox exposure mitigation strategies employed by men who have sex with men and transgender women in the United States. Arch Sex Behav. (2022) 51:3653–8. doi: 10.1007/s10508-022-02423-3
27. Delaney KP, Sanchez T, Hannah M, Edwards OW, Carpino T, Agnew-Brune C, et al. Strategies adopted by gay, bisexual, and other men who have sex with men to prevent monkeypox virus transmission - United States, August 2022. MMWR Morb Mortal Wkly Rep. (2022) 71:1126–30. doi: 10.15585/mmwr.mm7135e1
28. Leenen J, Wijers J, Den Daas C, de Wit J, Hoebe C, Dukers-Muijrers N, et al. Testing behaviour and associated factors in men who have sex with men by level of urbanisation: a cross-sectional study in the Netherlands. BMJ Open. (2022) 12:e049175. doi: 10.1136/bmjopen-2021-049175
29. Hammoud MA, Wells N, Holt M, Bavinton B, Jin F, Maher L, et al. COVID-19 Testing in a weekly cohort study of gay and bisexual men: the impact of health-seeking behaviors and social connection. AIDS Behav. (2022). doi: 10.1007/s10461-022-03831-1
30. Hawkinson DE, Operario D, Hess S, van den Berg JJ. Bridging the age gap: intergenerational communication of HIV risk and prevention among younger and older men who have sex with men. AIDS Care. (2022). doi: 10.1080/09540121.2022.2085865
31. Lyu H, Zhou Y, Dai W, Zhen S, Huang S, Zhou L, et al. Solidarity and HIV testing willingness during the COVID-19 epidemic: a study among men who have sex with men in China. Front Public Health. (2021) 9:752965. doi: 10.3389/fpubh.2021.752965
32. Valente TW. Social networks and health behavior. In:Rimer B, Glanz K, Vishwanath V, , editors. Health Behavior: Theory, Research and Practice. 6th Ed. New York, NY: Wiley (2015). p. 205–22.
33. Larkin HD. FDA authorizes intradermal vaccine, streamlines rules to increase monkeypox treatment access. JAMA. (2022) 328:819. doi: 10.1001/jama.2022.14692
34. European Medicine Agency. EMA's Emergency Task Force Advises on Intradermal use of Imvanex / Jynneos Against Monkeypox. Available online at: https://www.ema.europa.eu/en/news/emas-emergency-task-force-advises-intradermal-use-imvanex-jynneos-against-monkeypox (accessed September 26, 2022).
35. Dutch Government Policy Brief. Available online at: https://www.rijksoverheid.nl/binaries/rijksoverheid/documenten/kamerstukken/2022/09/29/kamerbrief-over-stand-van-zaken-apenpokken/kamerbrief-over-stand-van-zaken-apenpokken.pdf (accessed September 29, 2022).
Keywords: vaccination, communication, GBMSM, mpox, public health, prevention, low urban, social network
Citation: Dukers-Muijrers NHTM, Evers Y, Widdershoven V, Davidovich U, Adam PCG, Op de Coul ELM, Zantkuijl P, Matser A, Prins M, de Vries HJC, Heijer Cd, Hoebe CJPA, Niekamp A-M, Schneider F, Reyes-Urueña J, Croci R, D'Ambrosio A, Valk Mvd, Posthouwer D, Ackens R, Waarbeek Ht, Noori T and Hoornenborg E (2023) Mpox vaccination willingness, determinants, and communication needs in gay, bisexual, and other men who have sex with men, in the context of limited vaccine availability in the Netherlands (Dutch Mpox-survey). Front. Public Health 10:1058807. doi: 10.3389/fpubh.2022.1058807
Received: 30 September 2022; Accepted: 13 December 2022;
Published: 05 January 2023.
Edited by:
Saadullah Khattak, Henan University, ChinaReviewed by:
Wajid Hussain, Huazhong University of Science and Technology, ChinaCopyright © 2023 Dukers-Muijrers, Evers, Widdershoven, Davidovich, Adam, Op de Coul, Zantkuijl, Matser, Prins, de Vries, Heijer, Hoebe, Niekamp, Schneider, Reyes-Urueña, Croci, D'Ambrosio, Valk, Posthouwer, Ackens, Waarbeek, Noori and Hoornenborg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicole H. T. M. Dukers-Muijrers,  bmljb2xlLmR1a2Vyc0BnZ2R6bC5ubA==
bmljb2xlLmR1a2Vyc0BnZ2R6bC5ubA==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.