
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 05 January 2023
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1056484
This article is part of the Research TopicCardiovascular Health in Children and Adolescents: Present and futureView all 36 articles
 Mario Leone1,2*
Mario Leone1,2* Patrick Levesque1
Patrick Levesque1 Sabrina Bourget-Gaudreault1
Sabrina Bourget-Gaudreault1 Jean Lemoyne3Emilia Kalinova4
Jean Lemoyne3Emilia Kalinova4 Alain Steve Comtois4Hung Tien Bui2
Alain Steve Comtois4Hung Tien Bui2 Luc Léger5Pierre Frémont6
Luc Léger5Pierre Frémont6 Maxime Allisse7
Maxime Allisse7Background: In the context of concerns regarding the cardiorespiratory fitness (CRF) of youth populations, the aims of this study were: (1) to update reference values for the VO2max for school-aged Canadians and (2) to document secular trends in CRF after a 35-year interval.
Methods: Between September 2014 and April 2017, the CRF of 3725 students (53.2% boys; 6.0 to 17.9 yrs) was determined using the 20-m shuttle run test. The sample was collected in 36 different schools from six cities of Québec (Canada).
Results: Median values of VO2max decreased with age in both sexes (p ≤ 0.05). By the age of 10, more than 20% of boys showed VO2max values below the recommended value (42 ml·kg−1·min−1). At the age of 17, that proportion reached 56.8%. A similar proportion of 12 yrs girls (20%) were under the recommended minimal value (37 ml·kg−1·min−1) and that value reached 69.9% at the age of 17. Compared to 1982, the VO2max at age 17 has declined by 18% for boys and 12% for girls. The situation is worse in terms of functional capacity (number of stages completed) with an overall decrease of more than 30%.
Conclusion: This study demonstrates that, compared to data obtained using the same methodology 35 years ago, the CRF and functional capacity of children and adolescents has declined to levels that should raise concerns from a public health perspective. Thus, the development of strategies to promote a physically active lifestyle in youth is more relevant than ever.
According to Health Canada (2016) (1) the prevalence of obesity in youth (5–17 years) has more than tripled over the last 30 years. One of the most common explanations is related to the marked decline in physical activity levels during childhood and adolescence (2, 3). In fact, some recent studies have also shown the huge impact of a physically active lifestyle on the prevention and management of multiple chronic health problems such as cardiometabolic risk factors, several cancers, mental health problems and more (4–6). Data from the Public Health Agency of Canada report (2016) (7) indicate that the vast majority of young Canadians fail to meet recommended levels of physical activity due to increased sedentary behaviors. In fact, nearly 91% of children and youth aged 5–17 do not reach the Canadian Physical Activity Guidelines (8) recommendation of 60 min of moderate to vigorous physical activity daily.
CRF is such a key determinant of health (4, 9) that it has been proposed as a vital sign that should be monitored in clinical practice (10). In childhood and adolescence specifically, poor CRF is a major precursor to the development of short-term and later-life cardiometabolic risk factors and chronic diseases (10–13). According to the WHO and based on several studies, VO2max which represents the maximal capacity of the organism to consume oxygen during maximum physical exertion, has long been considered the leading indicator of CRF (14–17). Although some authors have questioned the usefulness and relevance of field tests for the evaluation of the CRF (18, 19) there is a strong consensus in favor of the use of this type of test, particularly for population surveillance (20–22). In fact, over the last 4 decades, the most commonly used test to assess aerobic fitness in school is the 20-m shuttle run test (23). The popularity of this field test relies on the fact that it is easy to manage, requires little equipment and time, is inexpensive and can be administered to several individuals simultaneously. In 2019, Statistics Canada released a set of normative percentile reference values including CRF (24). For practical reasons, the aerobic test chosen was the Modified Canadian Aerobic Fitness Test (mCAFT), a submaximal step test used to estimate an individual's CRF. Due to the very different nature of the procedures, the two tests cannot be interchanged for population surveillance purposes since the estimated VO2max values will be different.
Thus, the first objective of this study was to provide an update of the reference values for VO2max for the Canadian youth population (aged 6–17). The second objective was document the suspected secular trends in youth CRF by comparing the data collected in 1982 by Léger et al. (23) with the results of the present study.
This study is a descriptive comparative research with a cross-sectional design based on a large sample of children and adolescents from Québec (Canada).
Between September 2014 and April 2017, a total of 3,725 students (boys = 1,983; girls = 1,742) were recruited for this study. The age varied between 6.0 and 17.9 years, which covers elementary and high school education in Canada. The participants were recruited in 36 different schools (elementary school = 24 and high school = 12) from six cities in the province of Québec (Montréal, Québec city, Saguenay, Trois-Rivières, Laval and Sherbrooke). The data was collected in the gymnasium of each school during physical education classes. Parents and students were informed of our presence and could indicate their refusal to participate in the project (a consent form was signed by the school authorities). The Institutional Ethical Committee Board (University of Québec in Chicoutimi) approved the project (no: 602-225-01).
A three-stage sampling approach was used for the selection of a representative number of school boards, schools and classrooms. Each school received an invitation letter in order to take part in the project. Following the sending of approximately 1,200 invitations to school principals, over 300 schools expressed their interest to participate in this project. Particular attention was also paid to the equitable representation of the various socioeconomic status in our sample through a socioeconomic school rating from the Québec government (Ministère de l'Éducation et de l'Enseignement Supérieur, 2017).
All schools and classrooms were randomly selected by lot. Apart from very rare exceptions, all students of the same class were assessed, thus eliminating a selection bias. If a chosen school would withdraw, a new draw was then carried out. All participants were free from illnesses, disabilities, or injuries that could have been aggravated by physical activity. The sample size required for conducting this study was determined from a Cohen's d power analysis in order to detect small effects (d < 0.1) with a 1-β = 0.95 for α = 0.05 using G Power software version 3.1.9.4. Thus, 1,564 youths per sex were required for a total of 3,128 participants.
Anthropometric variables were collected using procedures proposed by Lohman et al. (25). Body mass (BM) was noted to the nearest 0.1 kg using a Detecto scale (Missouri, USA). Body height (BH) was assessed using a Lafayette stadiometer (Louisiana, USA) at the nearest 0.1 cm. Body mass index (BMI) was also calculated. BMI (typical vs. overweight and obese youths) was classified according to age and sex as suggested by Cole et al. (26).
CRF was determined in accordance with the 20-m shuttle run test described and validated by Léger et al. (23). Briefly, the test took place in a standard size gymnasium of at least 25 m. The entire classroom (generally around twenty students) took up position on the starting line. Whenever a participant could no longer follow the required running speed, he or she was stopped and the number of the last completed stage was recorded. At the end of the test, the following information was then extracted or estimated for each student: the number of the final stage, the associated running speed (km·h−1) and the estimated VO2max value (ml·kg−1·min−1).
All descriptive values are reported as mean ± standard deviation (SD). Confidence intervals (CI) were set at the 95% level. Cohen's effect sizes were calculated for various intergroup comparisons. The Shapiro-Wilk test for normality was compiled for each variable. When normality was violated, a Box-Cox transformation (27) was conducted using the following equation:
Where, BC, Box-Cox transformation; VAR, variable; L, lambda
The Box-Cox power exponential method, which smoothed the curves by cubic splines, has been used to create the curves.
Outliers were identified using the method proposed by Hoaglin et al. (28, 29). The equation reads as follows:
Where Q75 = 3rd quartile; Q25 = 4th quartile; g = 2.2
Percentiles values were computed using the LMS method, (30) which read as follows:
Where, P = percentile; M = median; L = Lambda; S = coefficient of variation; S = Z-score for the desire percentile.
In order to be able to assess changes that have occurred between 1982 and 2017, the data from the present study were compared with the study carried out by Léger et al. (23) using an unpaired T-Test. Statistical analysis was produced by the IBM-SPSS software version 24.
Anthropometric (BM, BH and BMI) and cardiorespiratory (number of stages completed and VO2max) characteristics as a function of age and sex are shown in Table 1. From the age of 10, girls are heavier and taller than boys until about the age of 13 years, which is consistent with puberty in girls. The cardiorespiratory profile presents a different picture where boys already have higher values for all age groups. This difference is particularly marked for the functional component of the test, which is reflected by the number of stages completed in the 20-m shuttle run test.
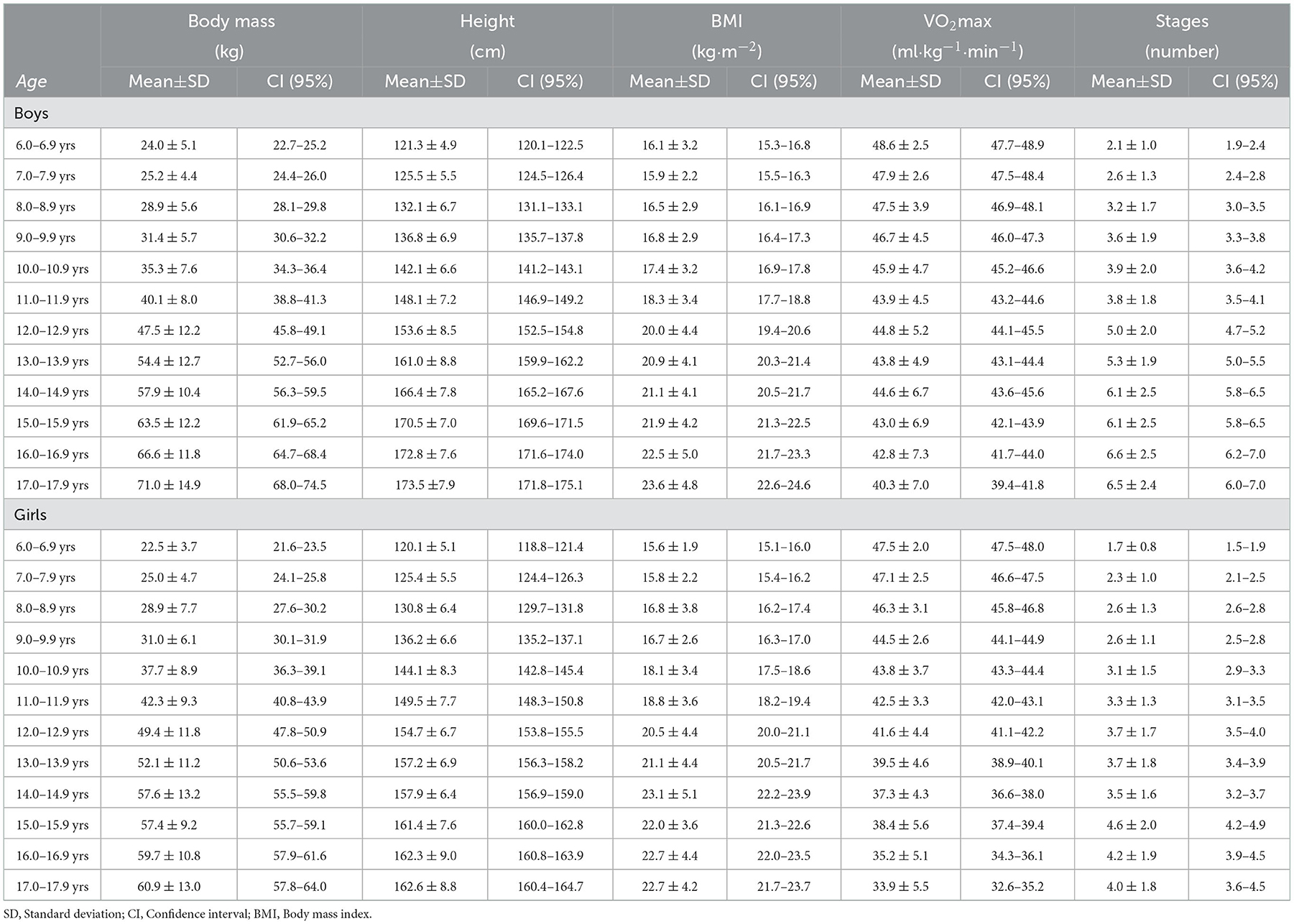
Table 1. Anthropometric and cardiorespiratory profiles of boys and girls aged 6–17 years old.
Percentile curves of VO2max and functional capacity, for boys and girls aged 6 to 17, are presented in Figures 1A, B. Between age 6 and 17, the median values for VO2max declines by about 14% for boys and 27% for girls. Also, this trend appears to be strongly affected by the percentile (VO2max) reached in early childhood. For example, for the 25th percentile value, a decline of 21% for boys and 33% for girls is observed between the age of 6 and 17. In Figures 1C, D, the percentile curves of the number of stages during the 20-m shuttle run test provide useful information regarding the functional aspect of the cardiorespiratory capacity. Thus, individuals in the upper percentiles tend to considerably improve the number of stages completed throughout the physical growth period compared to individuals in the lower percentiles.
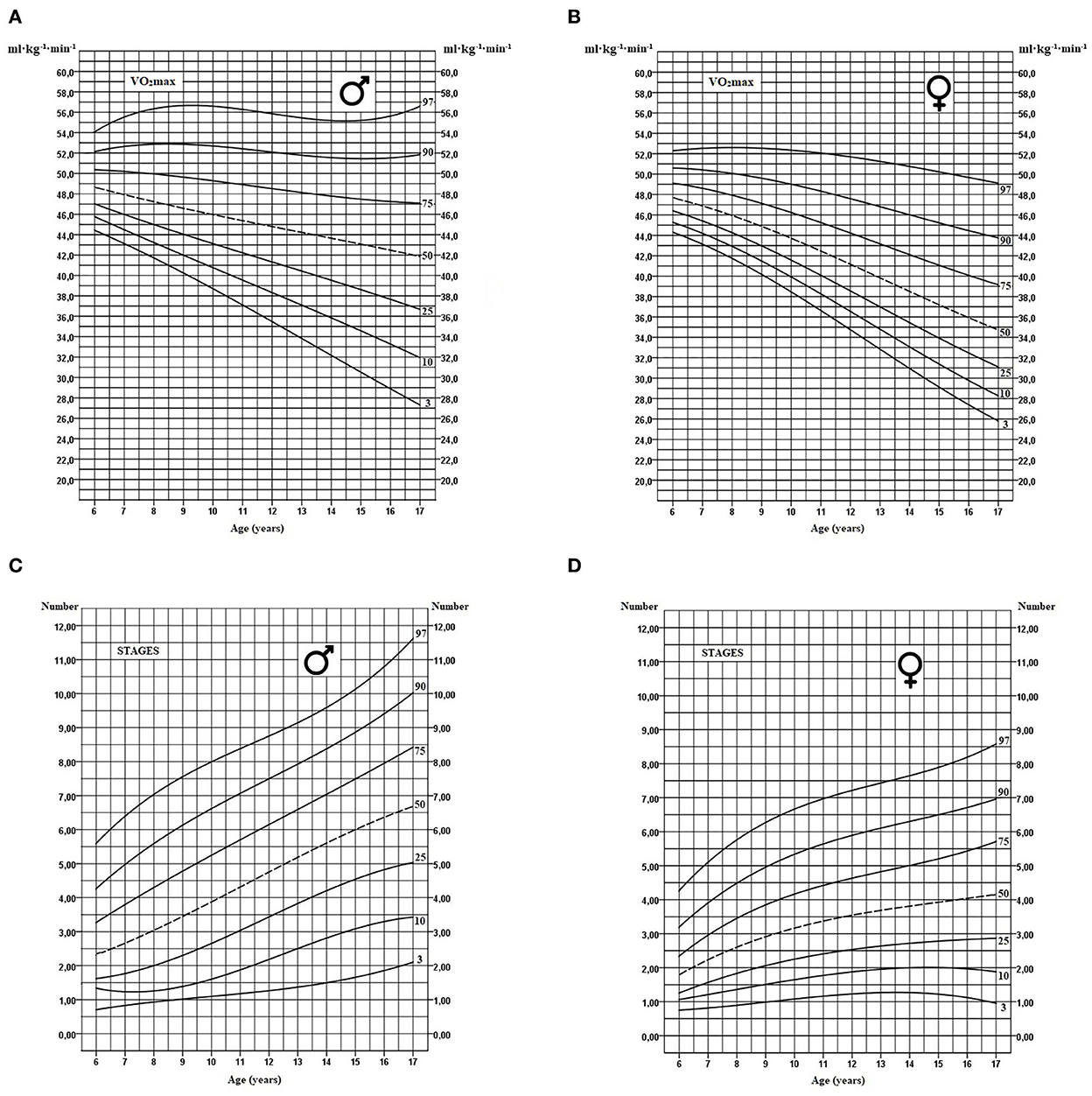
Figure 1. Age-specific smoothed percentile curves for VO2max and the number of stages completed estimated using the 20-m shuttle run test for boys (A, C) and girls respectively (B, D).
Tables 2, 3 provide the standardized values for VO2max and functional capacity (stages) respectively. All parameters included in the LMS method are reported for each year of chronological age (6–17 years) for both sexes. Additionally, values for the 3rd, 10th, 25th, 50th, 75th, 90th, and 97th percentiles are also shown.
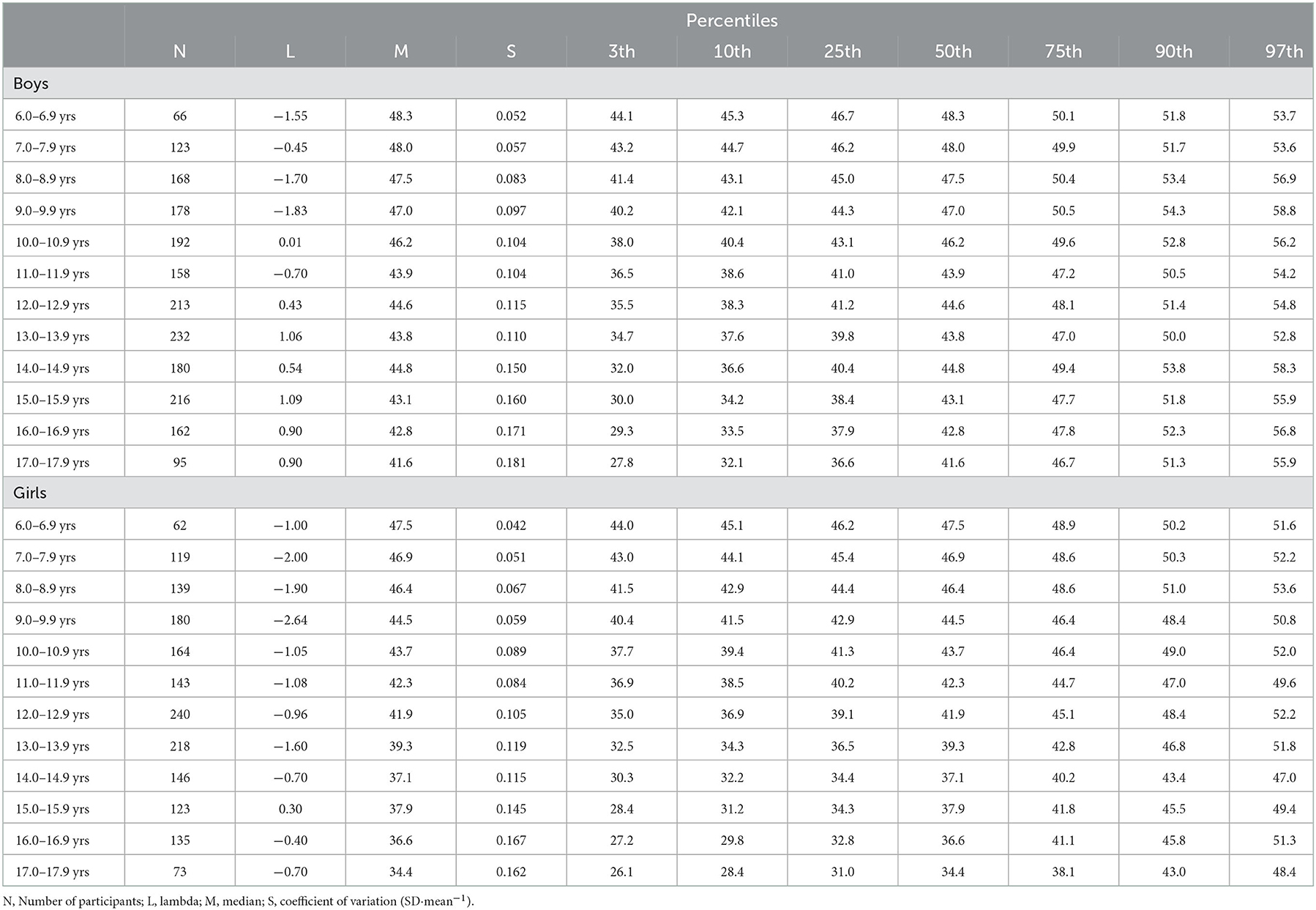
Table 2. Percentile references values for VO2max according to age and gender in Québec children and adolescents (N = 3725).
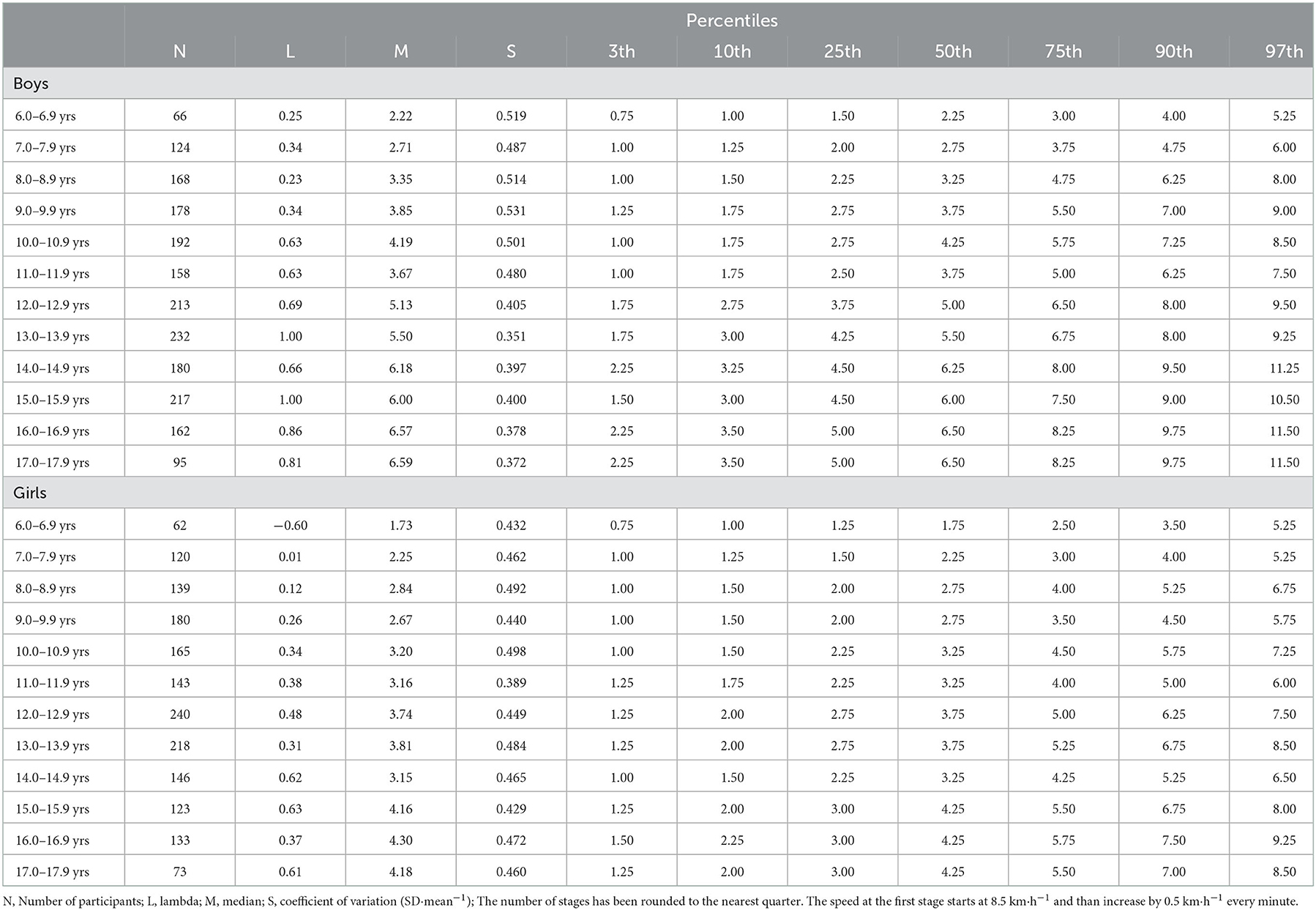
Table 3. Percentile reference values for the number of stages completed during the 20-m shuttle run test according to age and gender in Québec children and adolescents (N = 3725).
The impact of BMI on VO2max was also examined (Figures 2A, B). As shown in Table 4, boys in the overweight/obese zone have VO2max values markedly lower than individuals with typical BMI across all age groups and this difference increases between the age of 14 and 17. In girls, a similar but less important difference is observed between overweight/obese individuals and those with typical BMI follows a slightly shifted curve which increases with age in favor of the former. For the functional aspect of the 20-m shuttle run test, a very large discrepancy is also observed when comparing individuals from the two BMI categories (Figures 2C, D).
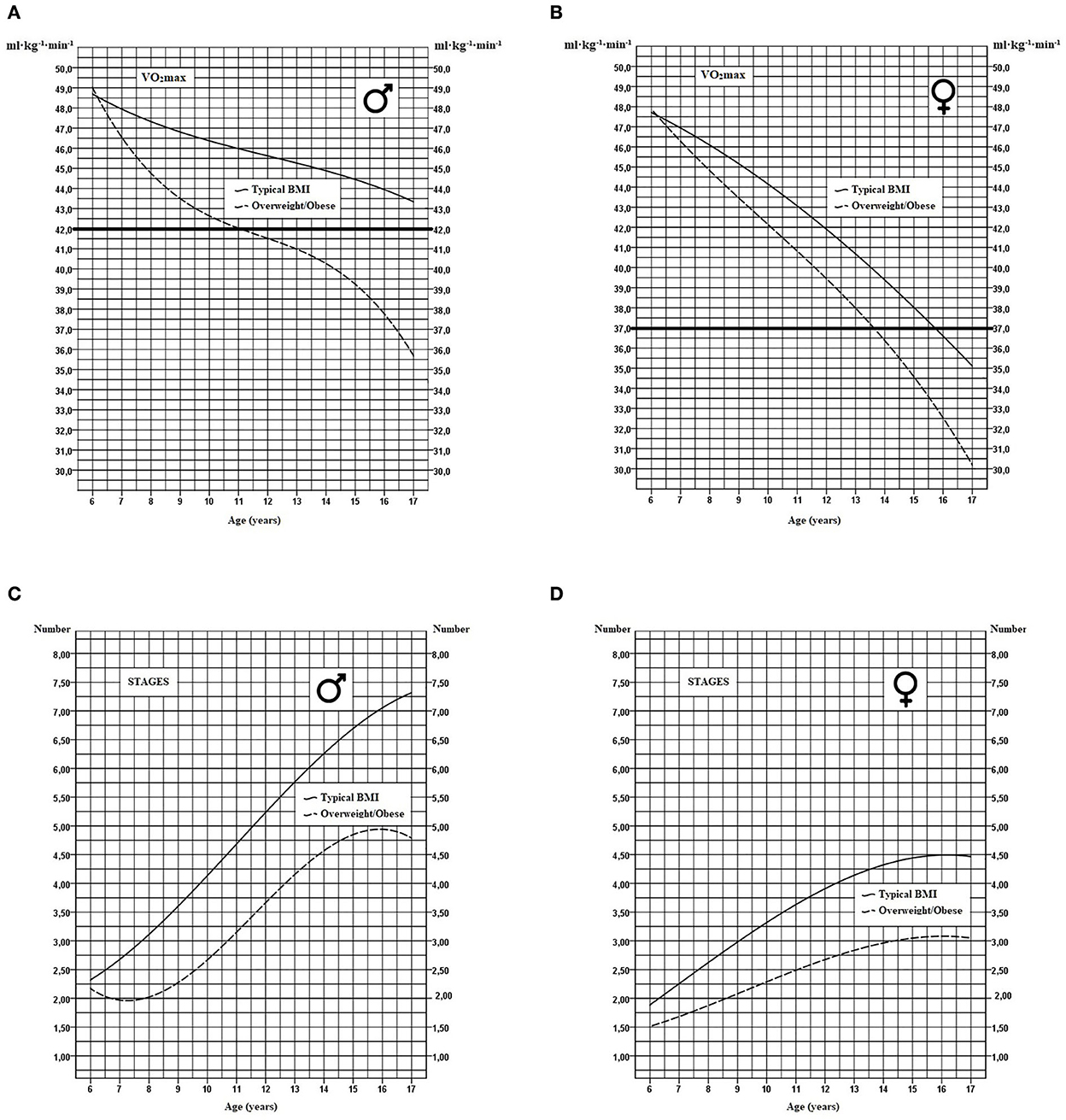
Figure 2. Modeling of VO2max curves and the number of stages completed in youth with typical BMI or with overweight/obese profile in boys (A, C) and girls (B, D). The thick horizontal line represents the critical cutoff health zone.
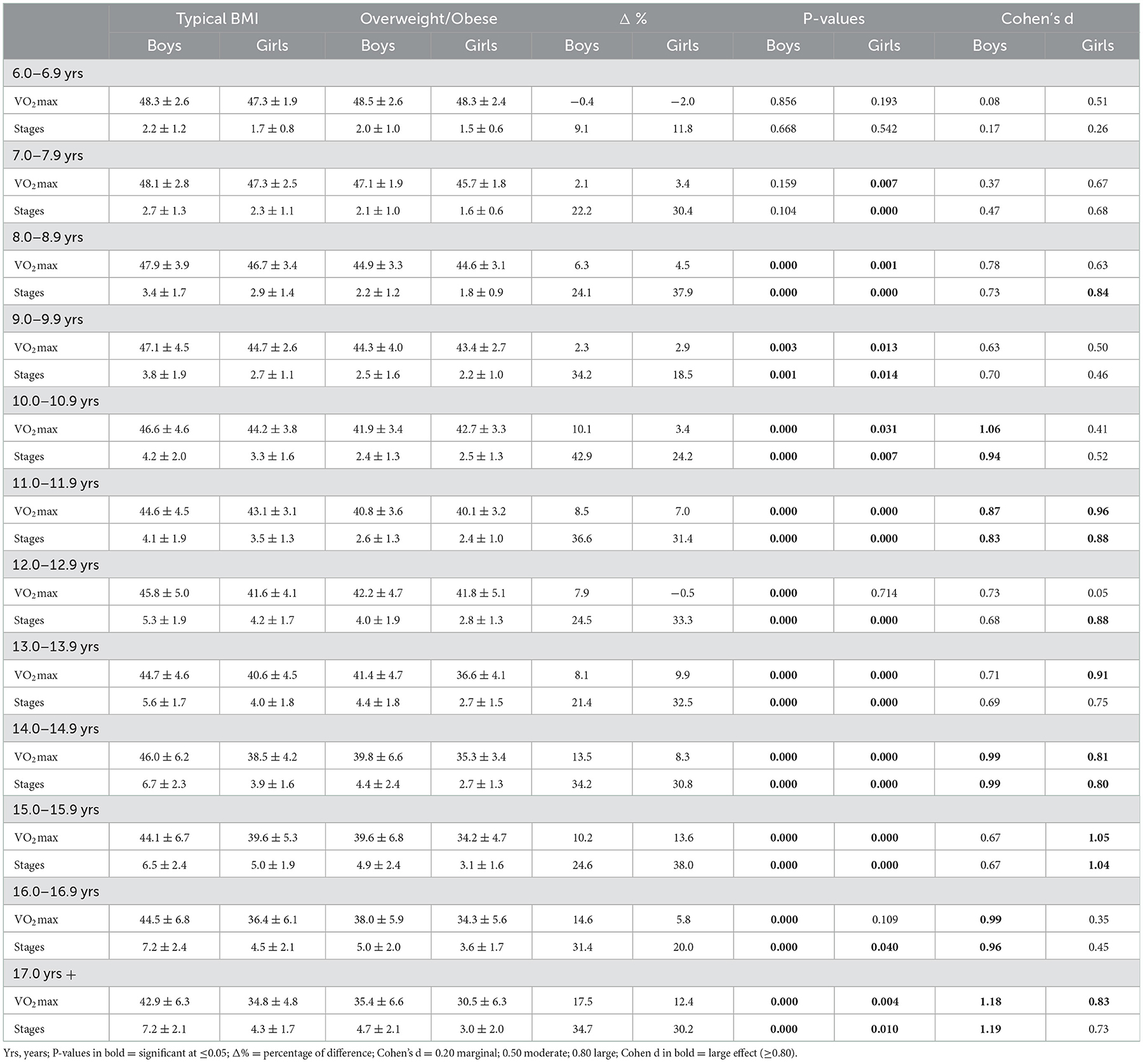
Table 4. Comparison of VO2max and the number of stages completed in children and adolescents with typical or overweight/obese BMI profile.
Secular trend for VO2max (Figures 3A, B) and the number of stages completed in the 20-m shuttle run test (Figures 3C, D) over a 35-year interval are illustrated by comparing data from the present study with data collected in 1982 using the same methodology (23). Over 35 years, median VO2max decreased by 7.6% for boys and 8.3% for girls at the age of 6 and this difference increases to nearly 18% in boys and 12.2% in girls by the age of 17 (Table 5). Compared to 1982, a significant decrease is also observed for all age groups for the number of stages completed for boys and girls.

Figure 3. Modeling of the secular trend curves for median VO2max and for the number of stages completed between 1982 and 2017 for 6 to 17 yrs boys (A, C) and girls (B, D). The thick horizontal line represents the critical cutoff health zone.
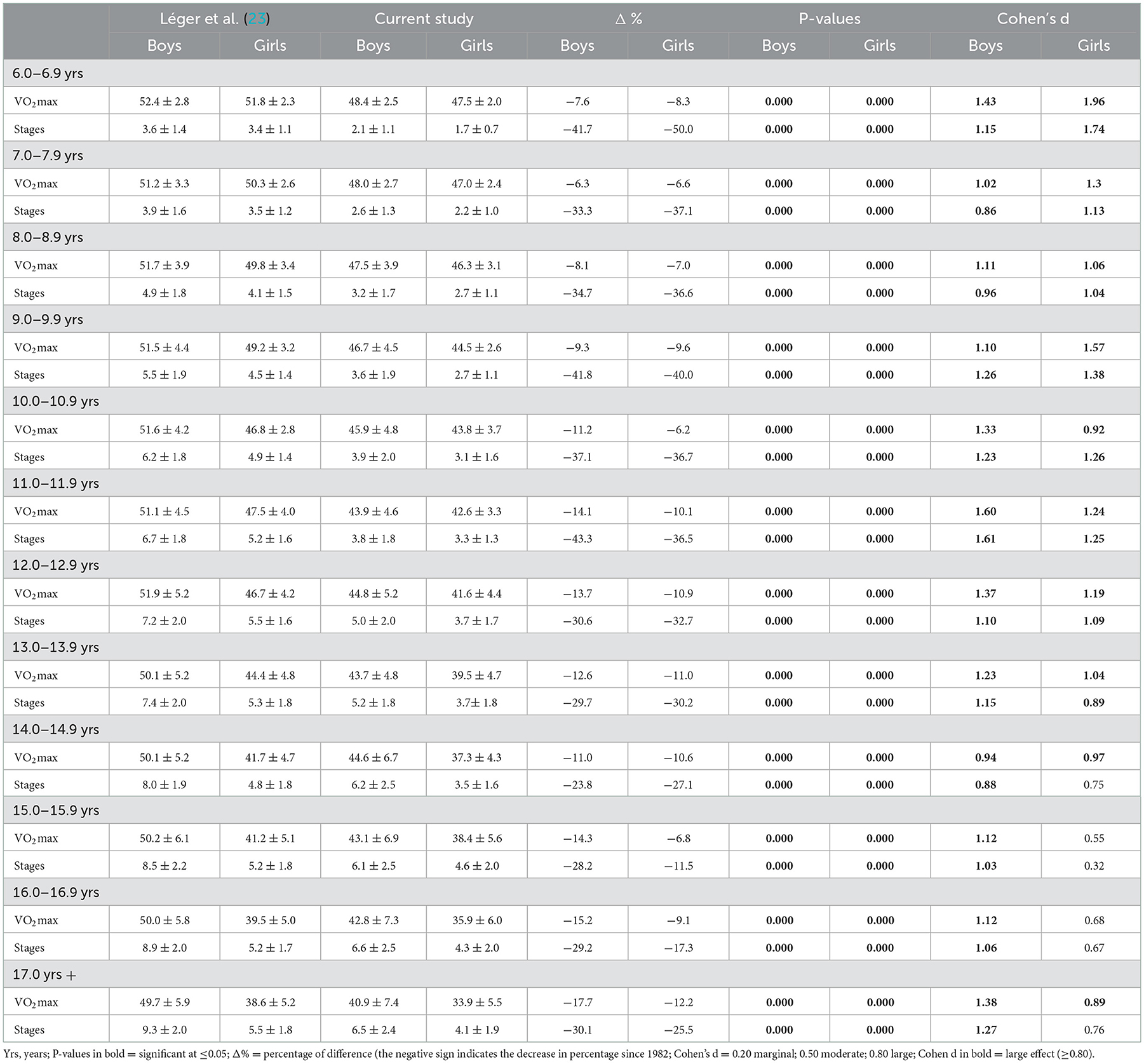
Table 5. Comparison of VO2max and the number of stages completed in children and adolescents between 1982 and 2017.
Given that the difference in body mass between 1982 and 2017 could influence the VO2max observed between the two periods, BM normalization was carried out. The discrepancies observed between the 2 periods are not attenuated by BM standardization as shown in Table 6. Similarly, BM normalization did not affect the secular trends observed between 1982 and 2017 regarding the number of stages completed.
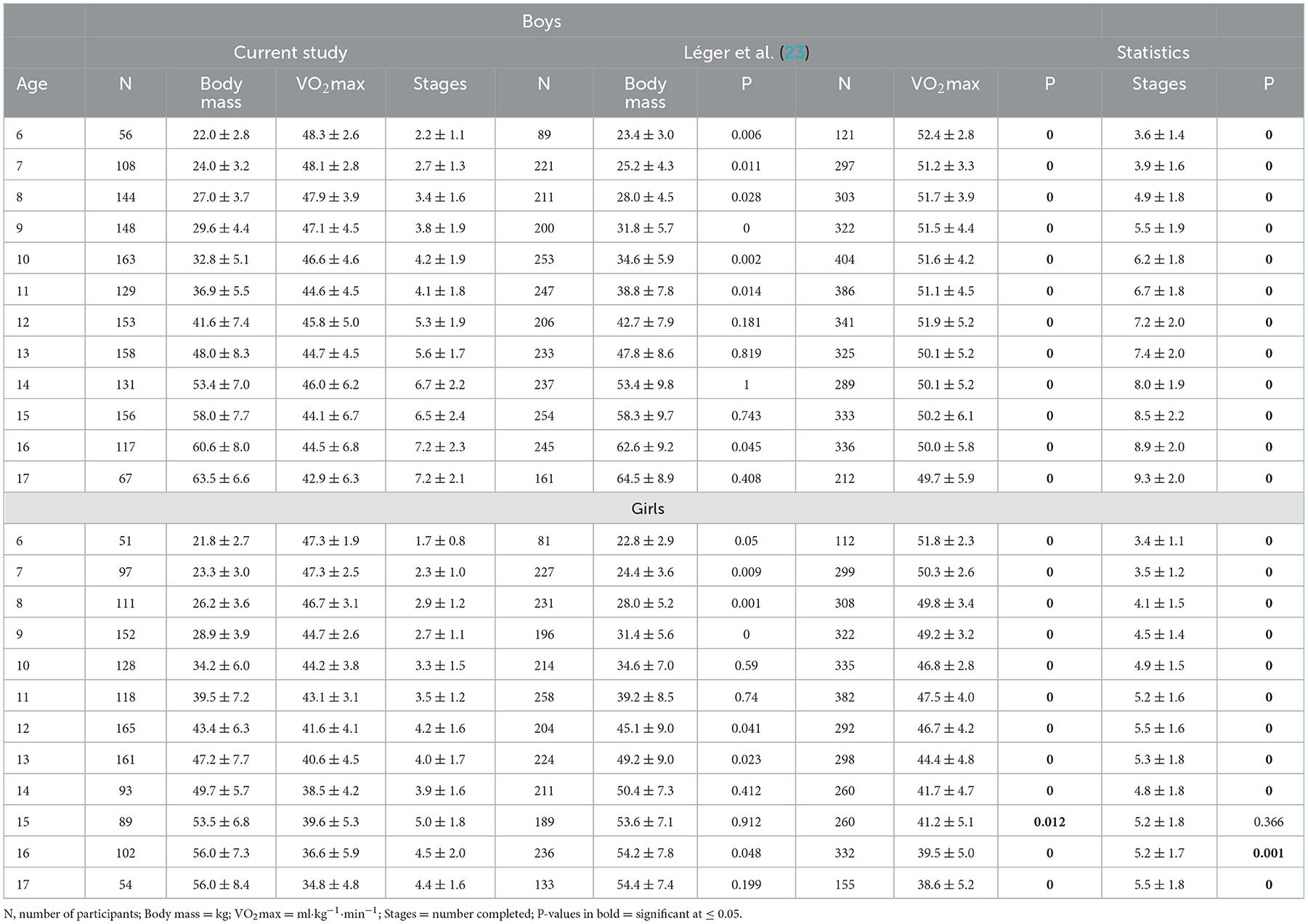
Table 6. Comparison of VO2max and the number of stages completed between Current study and Léger et al. (23) with adjustment for BM.
This study provides recent reference values for the maximal aerobic 20-m shuttle run test in children and adolescents of the province of Québec (Canada). It also provides unique opportunity to directly compare recent CRF data with reference values initially documented for this test in the same geographic area and age group in 1982 (31).
According to different studies and regardless of age, it is estimated that a minimum VO2max value of approximately 42 ml·kg−1·min−1 in boys and 37 ml·kg−1·min−1 in girls is required to minimize the risk of developing severe health problems (32, 33). Considering these CRF thresholds, the reference values documented in this study raise a powerful red flag by showing that, by the age of 17 in boys and 15 in girls, the median VO2max value is below the minimal CRF level associated with favorable health outcomes later in life. These results are consistent with the reference values reported by Tomkinson et al. (6) in a metanalysis of 177 studies, most of which were published between 2000 and 2015.
Functional capacity is also affected, demonstrating that today's youth have a reduced ability to sustain moderate/intense effort. In fact, this decrease begins 1 year earlier than the decline in VO2max. This finding is certainly as worrying as the decrease in VO2max.
The results also indicate that the higher the CRF reached at a young age, the greater the chances that it will be maintained during the growth period. Assuming that this tendency persists later in life through adulthood, these results further support the notion that childhood CRF can contribute to prevent the development of cardiometabolic risk factors and diseases later in life (14).
Although obesity is recognized as a major cause of morbidity, (1, 32) a recent metanalysis indicated that it is not an independent factor of premature mortality (14). In the present study, data stratification for BMI (typical vs. overweight/obese) shows that, in the later group, a higher proportion evolves toward a VO2max value below the minimal CRF level associated with favorable health outcomes. In boys with the overweight/obese profile, it is noted that the critical median cutoff value of VO2max is crossed as soon as the age of 11, which never happens for the typical BMI group.
The number of stages completed as a function of age is also heavily impaired in the overweight/obese BMI group. These results further support the notion that lower CRF and functional capacity are factors that likely contribute to unfavorable cardiometabolic outcomes in youth with BMI that correspond to the definition of overweight and obesity. However, other factors also need to be taken into account since in girls with a normal BMI median VO2max will eventually fall below the recommended cutoff by the age of 16. Reduced physical activity combined with increased passive activities has been suggested as a likely factor that explains this situation (32, 34, 35).
The great heterogeneity of CRF assessment procedures makes comparisons between studies complicated. In 1982, Léger and colleagues developed the 20-m shuttle run test and developed reference values for the CRF of youth living in Quebec (23). International reference values for the 20-m shuttle run test were recently developed by combining data from studies published up to 2015 (6). However, these more recent reference values do not allow comparison for specific population over time. The present study has the advantage of using the same test, administered under the same conditions, in the same cities and in the same school boards as 35 years earlier by Léger et al. (23).
This methodology resulted in a unique opportunity to objectively appreciate the evolution of CRF in youth between 1982 and 2017. The results confirmed an important decrease of CRF (estimated VO2max) and functional capacity (number of stages completed) in the study population. This difference tends to accentuate with age, with a VO2max decrease reaching nearly −18% for males and −12% for females at the age of 17. The functional impact of this situation is even more important in terms of the number of stages completed with an overall decrease of more than −30%. Furthermore, in 1982, all age groups of both sexes displayed VO2max values above the minimal recommended threshold associated with positive health outcomes. In the present study population, this is no longer the case from the age of 16 for boys and 15 for girls.
While some authors deny the fact that CRF has decreased over the last decades (18, 19) our results clearly show an alarming decline, both in relative (ml·kg−1·min−1) and functional values (number of stages). It has been suggested that the decrease in VO2max when expressed in relative values is predictable given the increase in body mass in youth over the past decades. However, data from the present study indicates that, after normalization for BM, significant differences remain for VO2max and for the number of stages completed in all age groups for both sexes. It may be noted that even when the body mass of Léger's cohort age groups was heavier, the relative and functional values remain markedly higher in their favor. Under these circumstances, it is reasonable to assume that body mass alone is insufficient to explain these differences.
It is assumed that, in addition to the body mass gain observed in recent decades in children and adolescents, increased time spent on sedentary activities is the factor that probably best explains the decrease in CRF (14, 21). Back in the 1980s when the 20-m shuttle run test was developed, computers and video games were in their infancy. With the development of the Internet and social networks youth became less physical active with an increase of time spent on sedentary activities (36, 37). As of 2016, combined data from 146 countries indicates that over 80% of adolescents do not meet the recommended levels of physical activity (38). Even more recently, the substantial reduction in physical activity due to containment measures related to COVID-19 is expected to further accelerate this decline (39).
In this paper, we use two distinct concepts that deserve to be explained. Based on the Centers for Disease Control and Prevention (DCC) in 2002, (40) reference values reflect the current situation without regard to its impact on health (what is). This information should not be interpreted as an objective to be achieved. This seems quite obvious as the VO2max values as well as the number of stages completed (i.e., functional capacity) have considerably decreased over the last decades. Thus, the role of the reference values is to make possible to measure the actual changes, and perhaps those that may occur in the future. They also allow comparison of current values with those from other studies.
On the other hand, the standard values represent what is minimally desirable in order to protect against certain potential health problems (what should be). In the case of VO2max, the minimum threshold should be around 42 ml in boys and 37 ml in girls. In order to stay above these thresholds, the reference values indicate that youths should follow at least around the 65th percentile curve throughout the growth period.
The large sample size (n > 3700) allows a valid representation of youths living in Québec (Canada). The test used to estimate the VO2max is internationally accepted as valid and reliable. The procedure used was repeated under the same conditions: same cities, same test and same school boards as the original 1982 study, which allows to assess the secular trends with a reduced number of biases. However, some limitations should also be noted. The cross-sectional nature of the data restricts inferences. VO2max values were estimated instead of measured directly, which affected the accuracy. Finally, although some towns were in suburban areas, cities in rural zones were not represented.
While providing updated reference values for the 20-m shuttle run test, this study provides direct comparative evidence of an alarming decrease of CRF and functional capacity in a population of children and adolescents since the 1980s. This further highlights the threat of an epidemic of cardiometabolic pathologies in the near future. Thus, development of population surveillance tools and public health strategies to promote a physically active lifestyle is more important than ever.
The raw data supporting the conclusions of this article will be made available from the corresponding author, without undue reservation.
The studies involving human participants were reviewed and approved by the Université du Québec à Chicoutimi (CER). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
ML was involved in the design and concept of the study, data collection, data analysis, drafted the initial, and final version of the manuscript. MA and EK co-ordinated, supervised data collection, involved in the study design, drafted the initial manuscript, reviewed, and revised the manuscript. AC, HB, and JL were involved in the study design, initial analyses, data collection, drafted the initial manuscript, reviewed, and revised the manuscript. LL and PF were involved in the data analysis, reviewed, and drafted the manuscript for important intellectual content. PL co-ordinated, supervised data collection, involved in initial data analysis, drafted the initial manuscript, reviewed, and revised the manuscript. SB-G was involved in the data collection, the initial data analysis, drafted the initial manuscript, reviewed, and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
This study was financially supported by the Center for Interdisciplinary Research on Quality and Healthy Lifestyles – UQAC: Grant no. UBR 324029.
The authors wish to acknowledge the principals, physical education teachers, school boards, and students who agreed to participate in this study. Special thanks to the interns who also helped with the data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Health Canada (Government of Canada). Childhood Obesity. 2016. Available online at: https://www.canada.ca/en/public-health/services/childhood-obesity/childhoodobesity.html (accessed September 15, 2020).
2. Moraes Ferrari GL, Bracco MM, Matsudo VK, Fisberg M. Cardiorespiratory fitness and nutritional status of school children: 30-year evolution. J Pediatr. (2013) 89:366–73. doi: 10.1016/j.jped.2012.12.006
3. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. (2012) 380:247–57. doi: 10.1016/S0140-6736(12)60646-1
4. Ozemek C, Laddu DR, Lavie CJ, Claeys H, Kaminski LA, Ross R, et al. An update on the role of cardiorespiratory fitness, Structured Exercise and lifestyle physical activity in preventing cardiovascular disease and health risk. Prog Cardiovasc Dis. (2018) 61:484–90. doi: 10.1016/j.pcad.2018.11.005
5. Sun C, Magnussen CG, Ponsonby AL, Schmidt MD, Carlin JB, Huynh Q, et al. The contribution of childhood cardiorespiratory fitness and adiposity to in?ammation in young adults. Obesity. (2014) 22:2598–605. doi: 10.1002/oby.20871
6. Tomkinson GR, Lang JJ, Tremblay MS, Dale M, LeBlanc AG, Belanger K, et al. International normative 20 m shuttle run values from 1,142,026 children and youth representing 50 countries. Br J Sports Med. (2017) 51:1545–54. doi: 10.1136/bjsports-2016-095987
7. Public Agency of Canada. How Healthy are Canadians? A Trend Analysis of the Health of Canadians From a Healthy Living and Chronic Disease Perspective. (2016). Available online at: http://www.publications.gc.ca/site/eng/9.825964/publication.html (accessed September 15, 2020).
8. Canadian Society of Exercise Physiology. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. (2020). Available online at: https://csepguidelines.ca/wpcontent/themes/csep2017/pdf/Canadian24HourMovementGuidelines2016_2.pdf (accessed September 15, 2020).
9. Sui X, Sarzynski MA, Lee DC, Kokkinos PF. Impact of changes in cardiorespiratory fitness on hypertension, dyslipidemia and survival: an overview of the epidemiological evidence. Prog Cardiovasc Dis. (2017) 60:56–66. doi: 10.1016/j.pcad.2017.02.006
10. Högström G, Nordström A, Nordström P. High aerobic fitness in late adolescence is associated with a reduced risk of myocardial infraction later in life: a nationwide cohort study in men. Eur Heart J. (2014) 35:3133–40. doi: 10.1093/eurheartj/eht527
11. Lang JJ, Phillips EW, Hoffmann MD, Prince SA. Establishing modified Canadian Aerobic Fitness Test (mCAFT) cut-points to detect clustered cardiometabolic risk among Canadian children and youth aged 9 to 17 years. Appl Physiol Nutr Metab. (2020) 45:311–7. doi: 10.1139/apnm-2019-0303
12. Ross R, Blair SN, Arena R, Church TS, Després JP. Franklin Ba, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American heart association. Circulation. (2016) 134:e653–99. doi: 10.1161/CIR.0000000000000461
13. García-Hermoso A, Ramírez-Vélez R, García-Alonso Y, Alonso-Martínez AM, Izquierdo M, Ramirez-Vélez R. Association of cardiorespiratory fitness levels during youth with health risk later in life: a systematic review and meta-analysis. JAMA. (2020) 174:952–60. doi: 10.1001/jamapediatrics.2020.2400
14. Raghuveer G, Hartz J, Lubans DR, Takken T, Wiltz JL, Mietus-Snyder M, et al. Cardiorespiratory fitness in youth: An important marker of health: a scientific statement from the American heart association. Circulation. (2020) 142:e101–18. doi: 10.1161/CIR.0000000000000866
15. Ortega FB, Ruiz JR, Castillo MJ, Sjöström M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. (2008) 32:1–11. doi: 10.1038/sj.ijo.0803774
16. Shephard RJ, Allen C, Benade AJ, Davies CT, Di Prampero PE, Hedman R et al. The maximum oxygen intake. An international reference standard of cardiorespiratory fitness. Bull World Health Organ. (1968) 38:757–64.
17. Taylor HL, Buskirk E, Henschel A. Maximal oxygen intake as an objective measure of cardio-respiratory performance. J Appl Physiol. (1955) 8:73–80. doi: 10.1152/jappl.1955.8.1.73
18. Armstrong N, Welsman J. Twenty-metre shuttle run: (mis)representation, (mis)interpretation and (mis)use. Br J Sports Med. (2019) 53:1199. doi: 10.1136/bjsports-2018-100082
19. Armstrong N, Welsman J. Youth cardiorespiratory fitness: evidence, myths and misconceptions. Bull World Health Organ. (2019) 97:777–82. doi: 10.2471/BLT.18.227546
20. Tomkinson GR, Lang JJ, Blanchard J, Léger L, Tremblay MS. The 20-m shuttle run : assessment and interpretation of data in relation to youth aerobic fitness and health. Pediatr Exerc Sci. (2019) 31:152–63. doi: 10.1123/pes.2018-0179
21. Tomkinson GR, Lang JJ, Tremblay MS. Temporal trends in the cardiorespiratory fitness of children and adolescents representing 19 high-income and upper middle-income countries between 1981 and 2014. Br J Sports Med. (2019) 53:478–86. doi: 10.1136/bjsports-2017-097982
22. Olds T, Tomkinson G, Léger L, Cazorla G. Worldwide variation in the performance of children and adolescents: an analysis of 109 studies of the 20-m shuttle run test in 37 countries. J Sports Sci. (2006) 24:1025–38. doi: 10.1080/02640410500432193
23. Léger L, Lambert J, Goulet A. Aerobic capacity of 6 to 17-year-old Quebecois 20-meter shuttle run test with 1 minute stages. Can J Appl Sport Sci. (1984) 9:64–9.
24. Hoffmann MD, Colley RC, Doyon CY, Wong SL, Tomkinson GR, Lang JJ. Normative-referenced percentile values for physical fitness among Canadians. Health Rep. (2019) 30:14–22. doi: 10.25318/82-003-x201901000002-eng
25. Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Champaign, IL: Human Kinetics Books (1988).
26. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. (2000) 320:1240–3. doi: 10.1136/bmj.320.7244.1240
27. Box GEP, Cox DR. An analysis of transformations. J R Stat Soc Series B Stat Methodol. (1964) 26:211–52. doi: 10.1111/j.2517-6161.1964.tb00553.x
28. Hoaglin DC, Iglewicz B, Tukey JW. Performance of some resistant rules for outlier labeling. J Am Stat Assoc. (1986) 81:991–9. doi: 10.1080/01621459.1986.10478363
29. Hoaglin DC, Iglewicz B. Fine tuning some resistant rules for outlier labeling. J Am Stat Assoc. (1987) 82:1147–9. doi: 10.1080/01621459.1987.10478551
30. Cole TJ, Green PJ. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med. (1992) 11:1305–19. doi: 10.1002/sim.4780111005
31. Tarp J, Fagerland MW, Dalene KE, Johannessen JS, Hansen BH, Jefferis BJ, et al. Device-measured physical activity, adiposity and mortality: a harmonised meta-analysis of eight prospective cohort studies. Br J Sports Med. (2021) 56:1–9. doi: 10.1136/bjsports-2021-104827
32. Ruiz JR, Cavero-Redondo I, Ortega FB, Welk GJ, Andersen LB, Martinez-Vizcaino V. Cardiorespiratory fitness cut points to avoid cardiovascular disease risk in children and adolescents; what level of fitness should raise a red flag? A systematic review and meta-analysis. Br J Sports Med. (2016) 50:1451–8. doi: 10.1136/bjsports-2015-095903
33. Ruiz JR, Huybrechts I, Cuenca-García M. Cardiorespiratory fitness and ideal cardiovascular health in European adolescents. Heart. (2015) 101:766–73. doi: 10.1136/heartjnl-2014-306750
34. Dobbins M, Husson H, DeCorby K, LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6-18 (Review). Cochrane Database Syst Rev. (2013) 4:CD007651. doi: 10.1002/14651858.CD007651.pub2
35. Arango CM, Parra DC, Gómez LF, Lema L, Lobelo F, Ekelund U. Screen time, cardiorespiratory fitness and adiposity among school-age children from Monteria, Colombia. J Sci Med Sport. (2014) 17:491–5. doi: 10.1016/j.jsams.2013.09.010
36. Sigmundová D, El Ansari W, Sigmund E, Frömel K. Secular trends: a ten-year comparison of the amount and type of physical activity and inactivity of random samples of adolescents in the Czech Republic. BMC Public Health. (2011) 11:731. doi: 10.1186/1471-2458-11-731
37. Ryu S, Kim H, Kang M, Pedisic Z, Loprinzi PD. Secular Trends in Sedentary Behavior Among High School Students in the United States, 2003 to 2015. Am J Health Promot. (2019) 33:1174–81. doi: 10.1177/0890117119854043
38. Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. (2020) 4:23–35. doi: 10.1016/S2352-4642(19)30323-2
39. López-Bueno R, Calatayud J, Andersen LL, Casana J, Ezzatvar Y, Casajus JA, et al. Cardiorespiratory fitness in adolescents before and after the COVID-19 confinement: a prospective cohort study. Eur J Pediatr. (2021) 180:2287–93. doi: 10.1007/s00431-021-04029-8
40. Kuczmarski RJ. 2000 CDC Growth Charts for the United States: methods development (No. 246). Department of Health Human Services, Centers for Disease Control Prevention, National Center for Health Statistics. (2002). Available online at: https://www.cdc.gov/nchs/data/series/sr_11/sr11_246.pdf (accessed November 9, 2022).
Keywords: normative reference values, VO2max, functional capacity, secular trends, youth, cardiorespiratory fitness
Citation: Leone M, Levesque P, Bourget-Gaudreault S, Lemoyne J, Kalinova E, Comtois AS, Bui HT, Léger L, Frémont P and Allisse M (2023) Secular trends of cardiorespiratory fitness in children and adolescents over a 35-year period: Chronicle of a predicted foretold. Front. Public Health 10:1056484. doi: 10.3389/fpubh.2022.1056484
Received: 28 September 2022; Accepted: 05 December 2022;
Published: 05 January 2023.
Edited by:
Zhen-Yu Zhang, KU Leuven, BelgiumReviewed by:
Malgorzata Wojcik, Jagiellonian University Medical College, PolandCopyright © 2023 Leone, Levesque, Bourget-Gaudreault, Lemoyne, Kalinova, Comtois, Bui, Léger, Frémont and Allisse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mario Leone,  bWFyaW8ubGVvbmVAdXFhYy5jYQ==
bWFyaW8ubGVvbmVAdXFhYy5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.