
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 11 January 2023
Sec. Children and Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1049851
 Yuheng Feng1,2,3
Yuheng Feng1,2,3 Xiaohong Li1,2,3*Xueqi Ma1,2,3Zhixu Zhu1Kaiyue Chen1,2,3Jun Gao4Jingwei Xia5Ruo Jiang1,2,3Jun Lu1,2,3
Xiaohong Li1,2,3*Xueqi Ma1,2,3Zhixu Zhu1Kaiyue Chen1,2,3Jun Gao4Jingwei Xia5Ruo Jiang1,2,3Jun Lu1,2,3Introduction: Unintentional injury among children represents a major public health problem. Online-social-network-based parental-health-education is a potential way to reduce child unintentional injuries. The study aimed to explore the mechanisms by which online-social-network-based health education may reduce the unintentional injuries among children aged 0–3 years.
Methods: We conducted a participant-blinded, randomized controlled, online-social-network-based health-education intervention study from March 2019 to February 2020 in Shanghai. We established four WeChat groups (two intervention groups and two control groups). For the intervention groups, a doctor's assistant regularly delivered information regarding unintentional injuries among children, and community childcare doctors answered parents' questions concerning their children's health, including unintentional injuries. Meanwhile, the control groups did not receive any information from the assistant. The study selected one intervention group and one control group and compared the ego network and whole network indicators to determine the differences between the intervention and control groups.
Results: In the intervention and control groups, 64.5% and 31.9% of the members, respectively, engaged in communication, and 1,736 and 273 records, respectively, were obtained. Regarding ego network, the doctor showed the largest network in the intervention group, and the size of the intervention group's network was twice that of the control group; the number of ties in the intervention group was nine times that of the control group. Fourteen and four parents in the intervention and control group played an active role, respectively. Regarding centrality, all WeChat groups were loose and multiple centers existed. Regarding subgroup cohesion, the intervention group had 28 cliques with 27 members, and the control group had 4 cliques with 4 members. For structural hole, 23.7% and 7.5% members in the intervention and control group actively participated in interactions, respectively, having strong control and influence over other parents; 69.2% and 59.1% members in the intervention and control group, respectively, had values of < 1.000, showing that they had strong ability to cross-jump structural holes.
Discussion: Online-social-networks-based health education interventions could enhance communication among parents, and between parents and community childcare doctors, and also shorten the social distance between them. Thus, online-social-network-based parental-health-education-intervention can be a feasible and generalizable means of preventing unintentional injuries among children.
Unintentional injury is an important public-health problem, not only because it is the major cause of death among children, but also because it can result in disability and heavy economic burden (1–6). West et al. (7) reported that children aged 0–4 years show high mortality from unintentional injuries, with the highest mortality being among children under 1 year old. From the perspective of time-data analysis, although a gradual declining trend of mortality in unintentional injuries among children under 5 years of age was reported, however, effective measures remain necessary to further reduce unintentional injuries (8–10).
Young children, such as children under five years of age, are vulnerable to unintentional injury, and their safety is dependent on their caregivers' (e.g., parents, grandparents, and babysitters) supervision (11–14). Thus, children's caregivers play an important role in protecting children from unintentional injuries. The main reasons for these children's vulnerability to unintentional injury include parents' lack of safety knowledge, parents' attitudes and behaviors, and the children's own attributes, such as impulsive and highly active (6, 12–16). Thus, it is essential to improve caregivers' knowledge, attitudes, and behaviors in this regard. Notably, studies have shown that health-education interventions for parents are an effective means of reducing unintentional injuries among children (17, 18).
The number of online social media users increase rapidly, such as Facebook and Twitter (19). In America, up to 46% people stated that they use social media as a sourcetool to look news in 2016, which is almost twice for 2013 (20). In China, mobile instant messaging users were up to 668 million in 2017 which covered 92.3% Chinese internet users. WeChat users, a popular mobile social app in China, covered 79.6% Chinese internet users (21, 22). As of 2019, the users' number of WeChat had reached about 1.17 billion, which was an increasing figure (23). So, interventions that are conducted through online social media can be considered promising. Additionally, this way also can be considered cost-effective (24). Notably, app-based interventions are widely used in health education (25–28).
Some apps, such as aforementioned software, are free to use and have large numbers of users. These popular apps, as convenient group-communication platforms, feature functions that are familiar to many people; for example, the facility to establish groups among people who have similar interests and goals. This suggests that such apps are suitable hosts for generalizable health-education interventions. Such apps can not only represent tools for delivering information, but also platforms for interaction. The effectiveness of online-social-network-based interventions has been confirmed in several areas of public health, such as mental health (29), smoking-prevention (30), and weight loss (31). Thus, online-social-network-based health-education interventions for parents represent a potential means of reducing the incidence of unintentional injuries among children. However, few studies have examined in detail the effect mechanism of online-social-network-based interventions (31); in addition, little is known about the mechanism underlying interactions among parents and health providers on online social media.
A small number of studies have explored app-based interventions for unintentional injuries among children (1). In a cluster randomized trial conducted in China, a new specialized app was developed to deliver to parents information concerning unintentional-injury-prevention and provide an interaction platform for parents and health-care providers; this study found that an app-based intervention can improve parents' knowledge and behaviors (32). However, its withdraw rate was higher than expected and developing a new app is expensive, which limits its generalizability. Therefore, there are several questions to be answered: (1) Can popular free apps be used as health education tools to prevent unintentional injuries among children aged 0–3 years? (2) What is the effect mechanism of such apps?
To investigate these questions, we previously conducted a randomized trial using WeChat, a free app that is very popular in China (33). Due to home is the main live environment for children aged 0–3 whose safety much more depends on their parents and seldom focused on them (1, 13, 14), the trial targeted parents of children aged 0–3 years, and confirmed the positive effect of a parental-health-education intervention based on online social media on reducing the occurrence of unintentional injuries via enhancing parents' associated knowledge, skills, and behaviors. In this study, we analyze the mechanism of interaction to understand the how such an online social network intervention can have this effect.
Social-network analysis (SNA) is a major social-science methodology that is used to analyze characteristics of social relationships; for example, sharing of values, capital, and knowledge among social units such as individuals, groups, and societies (34–36). In the health-care field, SNA has been widely used to characterize aspects such as relationships (37, 38), chronic disease management (39) and infectious disease (40); however, there has been little SNA-based investigation in relation to health education (41). A scoping review stated that SNA can not only be used to explore the function of complex interventions across different phases (42), but that SNA can graphically illustrate hidden relations between group members in social networks (43–45). Specifically, the main strength of SNA is its ability to allow researchers to examine mechanisms of interaction in online social networks (41).
In the present study, an online parental-health-education intervention was conducted through the use of WeChat groups that included a community childcare doctor, the doctor's assistant, and the target parents. SNA was used to analyze the mechanisms of health education via online social networks.
A characteristic element of the relationship among WeChat group members is information asymmetry, because community childcare doctors, as health-care providers, possess more knowledge about childcare, and parents, as healthcare demanders, lack such knowledge despite having the responsibility to care for their children. Hence, for the present study we created the following hypotheses:
Research hypothesis H01: In WeChat groups, the community childcare doctor is situated at the core. In addition, parents who have better knowledge about child health and are ready to help others voluntarily answer other parents' questions.
Research hypothesis H02: The WeChat-group-based parental-health-education intervention facilitated by the doctor and the assistant encourages more parents to participate in the interactions between group members.
Research hypothesis H03: The WeChat-group-based parental-health-education intervention can connect parents and promote their acquiring of childcare knowledge via mutual communication with other parents.
The study was conducted in the central area of Jiading District, Shanghai, China, from March 2019 to December 2020, and featured three phases (Figure 1).
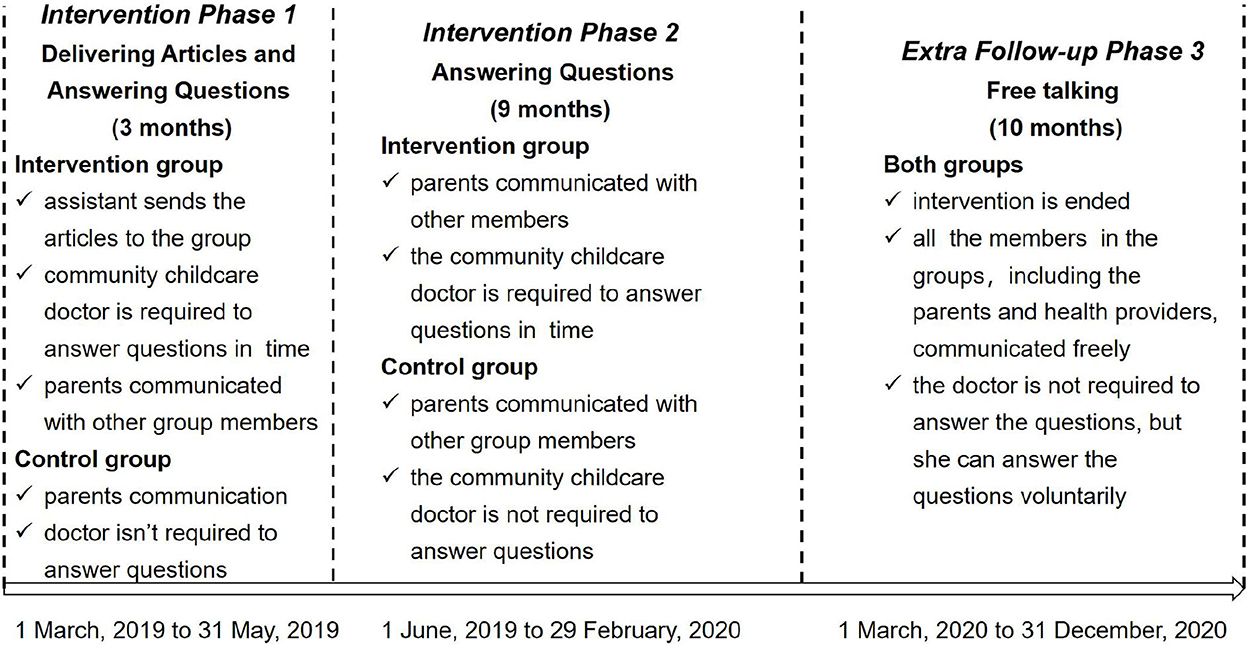
Figure 1. The phases of study design.
Phase 1 comprised a 12-week (~3 months) health-education intervention designed to improve parents' knowledge, skills, and behaviors regarding unintentional injuries among children. The Phase 1 process was conducted by the assistant to the community childcare doctor, who posted 2–3 articles per week on the official WeChat account and also sent the articles to the intervention groups (also via WeChat), reminding parents to read them. The parents could also ask questions and communicate with each other during this period. The doctor was required to answer parents' questions within 48 h.
Phase 2 comprised the 9 months following Phase 1, during which parents could continue to communicate with each other and ask the community childcare doctor questions about childcare. The difference between the intervention and control group during this phase was that the community childcare doctor was not required to answer the control-group questions within 48 h.
Phase 3 comprised an additional follow-up, which lasted 10 months; this represented the post-intervention period, and provided an indication of the group members' voluntary behaviors regarding seeking and providing information concerning unintentional injuries among children. Parents could freely communicate with the other members, and the community childcare doctor was not required to answer any questions unless she wished to do so.
This study was approved (IRB No. 2018-01-0663) by the Medical Research Ethics Committee, School of Public Health, Fudan University and registered at Chinese Clinical Trial Registry on 17 January, 2019. All participants provided informed consent prior to participation.
We calculated sample size using a formula for comparing two incidences at a 1:1 ratio (representing the intervention group and control group, respectively); unintentional injury rate was used as the indicator. The formula was:
In a previous non-controlled intervention study conducted in China, on-site research focusing on children aged 1–6 years found unintentional injury rates of 23% and 4% before and after the intervention, respectively (47). We used the following values for the sample-size calculation: α = 0.05, β = 0.20, P1 = 0.10, P2 = 0.23, which indicated that each group should comprise at least 125 parents. Assuming a dropout rate of 10–50% (based on typical rates for online interventions) (48, 49), this meant that 138–188 parents were required for each group. All sample-size calculations were completed using PASS 2021.
According to the Children Health Management System, the central area of Jiading District contains 38 resident committees, and ~3,500 children aged 0–3 years who are registered with the child-care-management system of the local community health service centers and who receive regular physical examinations. There are two towns in the area, and each town has one health community center (Jiading Town Health Community Center and Juyuan Town Health Community Center, respectively). From January 1 to February 28, 2019, parents who brought their children to the community health service centers to receive physical examinations were asked to participate in this study, and those that agreed were allocated to one of four WeChat groups. Stratified sampling by child age was used for recruitment. In each town, the parents who agreed to participate were randomly allocated to an intervention group or a control group using a random number table. Thus, the following four WeChat groups were consequently created: Jiading invention group and Jiading control group, and Juyuan invention group and Juyuan control group, respectively. The present study analyzed data for the Jiading intervention group and the Jiading control group. The socio-demographic characteristics comparison and the time-series plot of chatting records were shown in Supplementary Tables S1–S7 and Supplementary Figures S1–S3.
The inclusion criteria for parents were as follows: (1) having a child aged 0–3 years; (2) being the main child caregiver (also eligible if other parent was the main child caregiver) who cares child in daily life and spends much time on caring; (3) being a frequent user of WeChat who uses it in daily life and spends much time on it; (4) having the ability of reading and writing; (5) willing to voluntarily provide informed consent; (6) not planning to move residence from March 2019 to December 2020.
The exclusion criteria for parents were as follows: (1) providing missing data for children about importance indicators and cannot be filled; (2) not cooperating with community childcare doctors in regard to completing their child's treatment; (3) the presence of a disability among the child or parents; (4) participating (the parents and/or their children) in another study.
No patients or members of the public were involved in the design, conduct, reporting, or dissemination of this research.
Before the establishment of the WeChat groups, the research team created 30 educational articles concerning five potential unintentional injuries and parents' beliefs and skills (of varying severity and susceptibility) among children (33). Among of them, three articles about falls, five articles about burns, five articles about drowning, three articles about poisoning, five articles about asphyxia, and nine articles about parents' beliefs and skills (see Supplementary Table S11). The injuries were chosen through expert consultation based on the Haddon matrix and parents' existing skills and knowledge. An official WeChat account named Child Safety and Health was established, and all articles were delivered through this platform. To prevent intergroup pollution, the official WeChat account was set as a private platform and was accessible only to the parents from the intervention groups. The control group members could not search for the group or follow it. The four WeChat groups were established on March 1, 2019, and all members were added individually by the assistant to the community childcare doctor.
Both intervention groups comprised the participating parents, a community childcare doctor, and the doctor's assistant. All parents were asked to follow the official WeChat account and, over the first 3 months, the assistant regularly uploaded articles and sent relevant messages and URLs to the groups. Additionally, all parents could ask the community childcare doctor questions about childcare, and they could also exchange perspectives with other parents and attempt to answer other parents' questions.
Both control groups had the same member composition as the intervention groups, but the parents were not asked to follow the official WeChat account and the community childcare doctor and assistant did not send them relevant messages and URLs. However, due to ethics requirements, the community childcare doctor did answer any emergency questions from the parents.
Finally, all communication records were exported to Excel 2019 through Python, and all group members were given unique numbers; the assistant was numbered “8888,” and the community childcare doctor was numbered “9999.” All records were screened and paired based on criteria of interaction that were used to determine each group member's engagement with the research contents (Supplementary Table S12).
All communication records were exported as a text file, and input in an Excel file to form interactive pairs based on Supplementary Table S12. They were imported into a text file to generate an interactive matrix in the Ucinet 6 data language. As all interactions in each group were shaped by all group members in each group, the social networks for this study represented one-mode directed networks, which meant that the nodes for each row and column were the same (50). All of the indicators listed below were calculated using Ucinet 6.
All sociodemographic statistics were analyzed using Stata 17.0. Continuous variables were described using means (95% confidence intervals) and tested using a two independent samples t-test (for continuous variables which are normal distribution, such as parents' age). Discrete variables were described using n (%) and tested using a two independent samples chi-square test (for categories variables without ranks) and Wilcoxon test (for categories variables with ranks).
SNA, which was completed by Ucinet 6, includes both ego network analysis and whole network analysis (50, 51). Hypothesis H01 could be tested through ego network analysis; Hypothesis H02 could be tested using the density, distance, centrality, and cohesion subgroups; and, finally, hypothesis H03 could be tested using structural hole. The interpretations of them were listed in Supplementary material.
Coreness reflects the degree of activity of each group member, and can be used to divide group members into five ranks: core, active, little activity, silent, and alienated (for details, see Supplementary Table S13) (52). Coreness was calculated using the following path: “Network → Core/Periphery → Continuous.” For this calculation, the inputted data should follow an adjacency matrix that contains only 0 and 1.
Basic measures for ego comprise 14 indicators. Among these, the size of the ego network, the number of directed ties, the network's density, its two-step reach, and the reach efficiency are important. For Parent A, the size of the ego network represents the number of other parents directly linked with Parent A, including Parent A himself; the number of directed ties represents all ties (Supplementary Table S12) in Parent A's ego network; density represents number of actual ties divided by ties in theory; two-step reach represents the percentage of actors in the network who are within two steps; and reach efficiency represents two-step reach divided by the network size, which provides standardized data. The above indicators can be calculated using the following path: “Network → Ego networks → Basic ego measures.” The input data should be in the form of an adjacency matrix.
If two parents have mutual communications, they have a reciprocal relationship (53); if all members have reciprocal relationships, the social network is named a “complete network” (50). Density is an indicator that reflects whether group members have a close association with other members (54). It can be calculated by dividing the number of relationships in fact by the number of relationships in theory. For a directed network, we can suppose that each members' number is “n” and the number of relationships in fact is “m”; thus, the number of relationships in theory is “n(n-1)” and the formula for the density is . Density can be calculated using the following path: “Network → Cohesion → Density → Overall Density.” The input data should be in the form of an origin matrix. Greater values here mean more interconnections.
Distance indicates the length of the shortest path between any two nodes in the social network. Three indicators are included: average distance, distance-based cohesion (compactness), and distance-weighted fragmentation (50). The present study focused on distance-based cohesion (compactness), which represents the average of all multiplicative inverses determined based on each distance in the distance matrix, and demonstrates the degree of closeness between all social-network members. Larger values indicate more closeness and more cohesion. Density can be calculated using the following path: “Network → Cohesion → Geodesic distance.” The input data should be in the form of an adjacency matrix.
Centrality was used to demonstrate, for each WeChat group member, whether they held a central position in the group and the level of power they had. Centrality is based on three kinds of indicators: point centrality, betweenness centrality, and closeness centrality. In the Ucinet 6, the input data should be in the form of an adjacency matrix.
2.6.2.3.1. Point centralityPoint centrality means the number of other parents who directly link with Parent A; a bigger value indicates a more central position (55). Additionally, for directed social networks the point centrality of each parent can be divided into in-degree centrality, which represents the number of connections received, and out-degree centrality, which represents the number of connections delivered. Point centrality can be calculated using the following path: “Network → Centrality → Degree”; data should not be treated as symmetric.
2.6.2.3.2. Betweenness centralityBetweenness centrality demonstrates the degree that Parent A can control the communication between other parents, or between other parents and the community childcare doctor. In a social network, this indicator represents the geodesic distance between Parent A and other pairs of parents. Bigger values indicate higher degrees of control of communication between other parents or between other parents and the community childcare doctor (55). Betweenness centrality can be calculated using the following path: “Network → Centrality → Freeman betweenness → Node betweenness.”
2.6.2.3.3. Closeness centralityCloseness centrality represents the degree to which Parent A is not controlled by other members. This indicator is calculated by determining the sum of the geodesic distances between Parent A and the other parents and between Parent A and the community childcare doctor. Higher values indicate further distance from the core of the social network (55). Closeness centrality can be calculated using the following path: “Network → Centrality → Closeness.”
Cohesion subgroups reflect the substructure of each WeChat group. To consider the social network's characteristics, for the present study we based on reciprocal relationships (56). This perspective included two aspects: components and cliques.
2.6.2.4.1. ComponentsIf any two group members can be connected by a certain pathway across a set of points, this pathway is called a “component.” There are two kinds of components: strong, which relates to a directed graph, and weak, which relates to an undirected graph (57). Components can be measured using the following path: “Network → Regions → Components → Simple graphs,” with both weak and strong component types being considered. The input data should be in the form of an adjacency matrix.
2.6.2.4.2. CliquesCliques indicate that the relationships between all members in a subgroup are reciprocal, and that no new member can be added to the subgroup (56). A clique represents the most basic cohesion subgroup, and can be measured using the following path: “Network → Subgroups → Cliques. The input data should be in the form of a symmetric adjacency matrix. To reveal possibly hidden cliques, decrease the number of cliques, and/or determine the main members, outsiders, and leaders in a clique, a co-membership matrix is used, which outputs data in the form of a “clique-by-clique actor co-membership matrix.”
Structural holes were first suggested by Burt, and were used in this study to identify non-redundant relationships between two parents (58). Supplementary Figure 4 provides details regarding the redundant and non-redundant relationships in the network. Supplementary Figure S4a shows a structural hole in which ego has an association not only with Parent A, but also with Parent B, while Parent A and Parent B have no relationship; this represents a hole because ego must deliver information to parent A and parent B, respectively. In Supplementary Figure S4b, a structural hole is not present because Parent A has an association with Parent B, and ego only needs to deliver information to Parent A, who can then provide the information to Parent B; thus, the relationship between ego and Parent B is redundant.
There are four important indicators for structural holes: (1) the effective size of the network: this indicator represents the number of non-redundant factors in Parent A's network; (2) efficiency: for Parent A, this indicator represents the ratio of effective size to actual size; (3) constraint: this demonstrates the impact of the presence of structural holes in an ego network; and (4) hierarchy: this demonstrates the extent to which constraint focuses on each parent and the community childcare doctor. Among these, the effective size of the network and constraint are very important. Structural holes can be calculated using the following path: “Network → Ego Networks → Structural holes,” with “whole network model—normal method” selected as the method. The input data should be in the form of a symmetric adjacency matrix.
Seventy-four parents were enrolled in the Jiading intervention group, and 64 parents were enrolled in the Jiading control group. There were no statistical differences between the intervention group and the control group in terms of sociodemographic characteristics (Supplementary Table S2). Additionally, there were not statistical difference for participants who withdrawn and completed this study in Jiading and Juyuan (Supplementary Tables S8–S10).
Including the community childcare doctor and the assistant, 66 and 76 members were included in the control and intervention groups, respectively. In the control group, 11 members (31.9%) communicated during the intervention and follow-up and 273 communication records were obtained. In the intervention group, 49 members (64.5%) communicated and 1,736 communication records were obtained. A time-series plot (Figure 2) showed that the intervention group was more active than the control group, which indicates that a health-education program based on a WeChat group may enhance parents' activity in regard to (1) obtaining knowledge about children aged 0–3 years, (2) exchanging their thoughts with other parents and community childcare doctors, and (3) taking the initiative in regard to asking community childcare doctors questions.
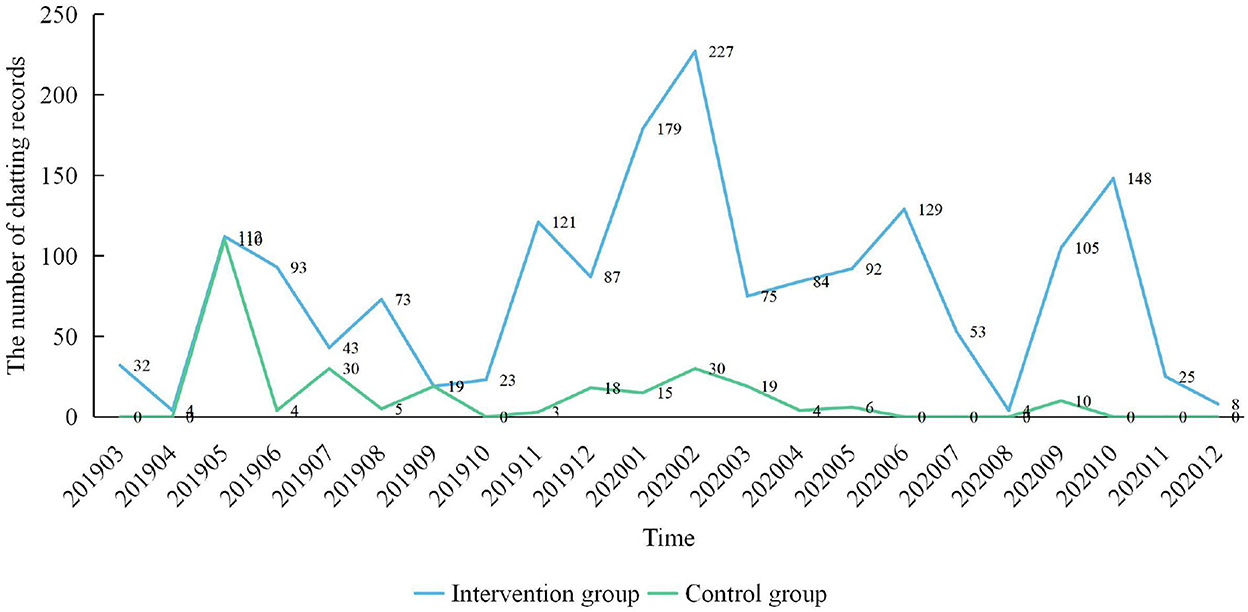
Figure 2. The time-series plot of intervention group and control group chatting records.
In the control group, 17 members (25.8%) were identified as core members, three members (4.5%) were active, and 46 members (69.7%) were alienated. In the intervention group, 15 members (22.7%) were core members, 33 (50.0%) were active, one member (1.5%) was showed little activity, and 27 members (40.9%) were alienated.
The community childcare doctor showed that the ego network (the size value was 17 and 44 in the control and intervention groups, respectively), had the largest number of ties (the ties value was 14 and 128 in the control and intervention groups, respectively), but the smallest density (the density value was 5.15% and 6.77% in the control and intervention groups, respectively), which demonstrated that the community childcare doctor was positioned in a core situation, mainly received (rather than sent) parents' messages, and was responsible for answering parents' questions. In addition, the two-step reach of the community childcare doctor was 29.23% and 65.33% in the control and intervention group, respectively, which was relatively high in all ego networks, and which demonstrates that the community childcare doctor had an ability to deliver information regarding the safety of children aged 0–3.
For the other parents, in the control group four parents (parent 1104, parent 1128, parent 1145 and parent 1200) had sizes of 6, 5, 4, and 3, respectively; the values for their ties were 8, 7, 4, and 2, respectively, their density values were 26.67%, 35.00%, 33.33%, and 33.33%, respectively; and their two-step reach values were 32.31%, 29.23%, 32.31%, and 26.15%, respectively. This demonstrated that they played an active role, not only asking questions of the community childcare doctor, but also answering other parents' questions or providing suggestions. Additionally, they, as core WeChat group members, participated in most interactions.
In the intervention group, 14 parents (parent 1119, parent 1074, parent 1196, parent 1004, parent 1146, parent 1222, parent 1058, parent 1241, parent 1056, parent 1080, parent 1109, parent 1189, parent 1218 and parent 1174) showed sizes of 19, 17, 15, 13, 12, 11, 11, 10, 10, 9, 8, 8, 7, and 7, respectively; the values for their ties were 95, 95, 82, 56, 45, 41, 61, 46, 49, 48, 35, 12, 28, and 19, respectively; their density values were 27.78%, 34.93%, 39.05%, 35.90%, 34.09%, 37.27%, 55.45%, 51.11%, 54.44%, 66.67%, 62.50%, 21.43%, 66.67%, and 45.24%, respectively, and their two-step reach values were 64.00%, 64.00%, 65.33%, 64.00%, 64.00%, 64.00%, 62.67%, 64.00%, 61.33%, 61.33%, 61.33%, 61.33%, 62.67%, and 37.33%, respectively. This suggests that these parents played an important role in helping the community childcare doctor answer some of the other parents' questions.
Compared to the control group, the intervention group was more active and featured more parents who may have played a role in answering questions, which shaped its post-intervention ego network (Supplementary Tables S13, S14).
Figure 3 shows social network graphs for the control and intervention groups. Besides the community childcare doctor, who was numbered “9999,” all parents who were mentioned above as being at the core of their social networks and who served as leaders were responsible for sharing the community childcare doctor's workload in terms of answering questions from parents in the group. Although both the control and intervention group featured parents who served as core members, the control group network was less close than the intervention group network. All of the following results are based on the social network graphs.
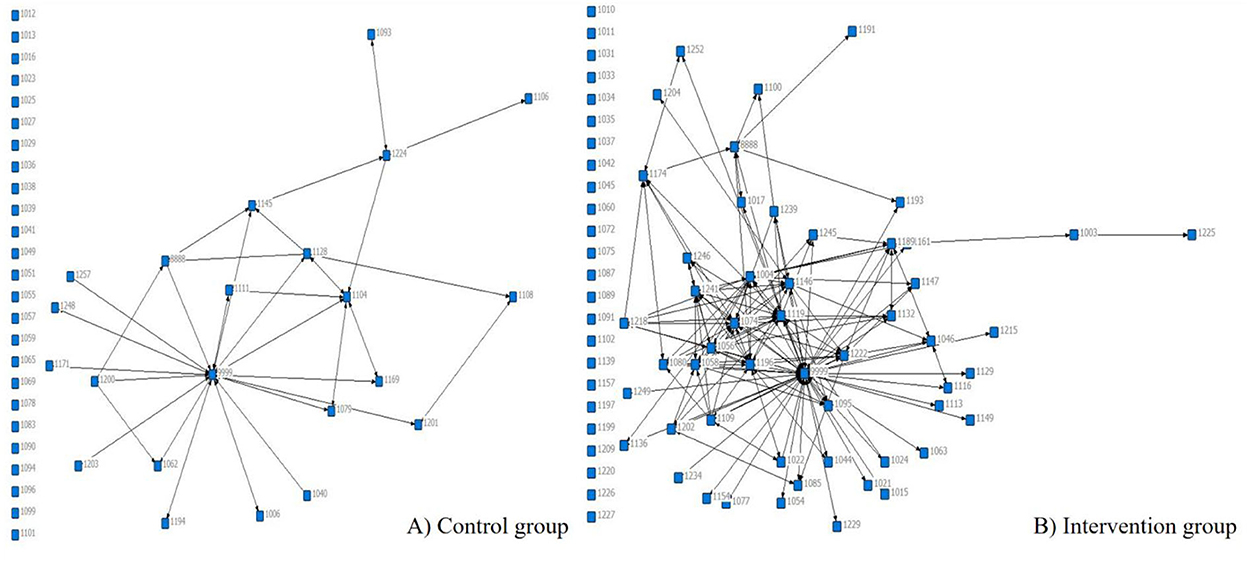
Figure 3. The social network of intervention group and control group.
For the control group, the density was 0.0590 and the distance-based cohesion (compactness) was 4.4%. For the intervention group, the density was 0.2912 and the distance-based cohesion (compactness) was 21.6%. Compared to the control group, the intervention group had ~ five-times the density and compactness, which demonstrated that the communication in the intervention group was closer and that more interactions occurred between parents. This indicated that the online-social-network-based parental health education intervention has a positive impact on enhancing parents' knowledge, beliefs, and skills about child unintentional injuries (see Supplementary material).
In the control group, the community childcare doctor had the largest in-degree centrality, 16, and out-degree centrality, 13, which was ~ three times that of the other parents. In addition, all group members had approximately the same in-degree and out-degree centrality values, which demonstrated that the parents mainly communicated only with the doctor (Supplementary Table S16).
In the intervention group, the overall situation was similar to the control group. However, parent 1196, parent 1004, parent 1218, and parent 1109 showed greater out-degree centrality than in-degree centrality, which demonstrated that they were willing to help other parents in regard to answering their questions. Meanwhile, parent 1056, parent 1058, and parent 1080, showed greater in-degree centrality than out-degree centrality, which demonstrated that they frequently received help from other parents (Supplementary Table S17).
In the control group, the community childcare doctor had the largest betweenness centrality, 256.5; meanwhile, parent 1145 and parent 1224 had the largest betweenness centrality when compared with other parents (64.7 and 53.5, respectively), which demonstrated that they had acquired considerable information about children aged 0–3, and could play an important role in regard to facilitating communication among group members (Supplementary Table S16).
In the intervention group, parent 1003 showed the largest betweenness centrality (1,706.5), while parent 1004, parent 1010, parent 1011, parent 1015, and parent 1017 also showed larger betweenness centralities than the other parents (157.0, 133.9, 122.6, 115.0, and 112.5, respectively). The community childcare doctor's betweenness centrality was 0, which demonstrated that, after receiving the intervention, some parents could resolve certain problems through mutual communication (Supplementary Table S17).
In the control and intervention groups, all group members' in-closeness centrality and out-closeness centrality were the same and small, at almost 2 and 3, respectively, which demonstrated that the social network was loose and had multiple centers (Supplementary Tables S16, S17).
Regarding weak components among the group members who participated in the social communication network, the control and intervention groups featured a component that included 22 nodes and 52 nodes, respectively, and the proportion was 33.3% and 68.4%, respectively (Tables 1, 2).
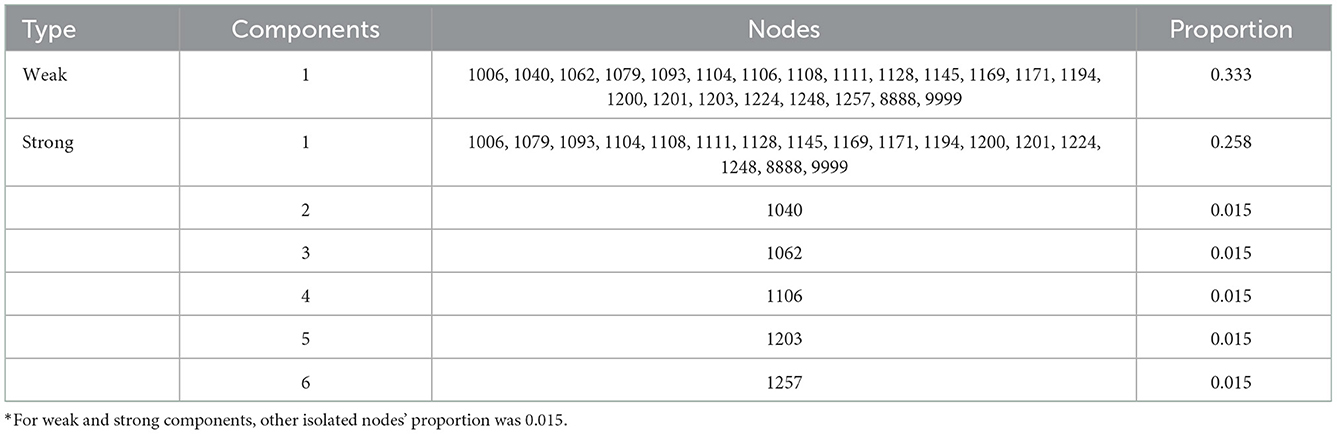
Table 1. The component of control group social network nodes except isolation nodes.
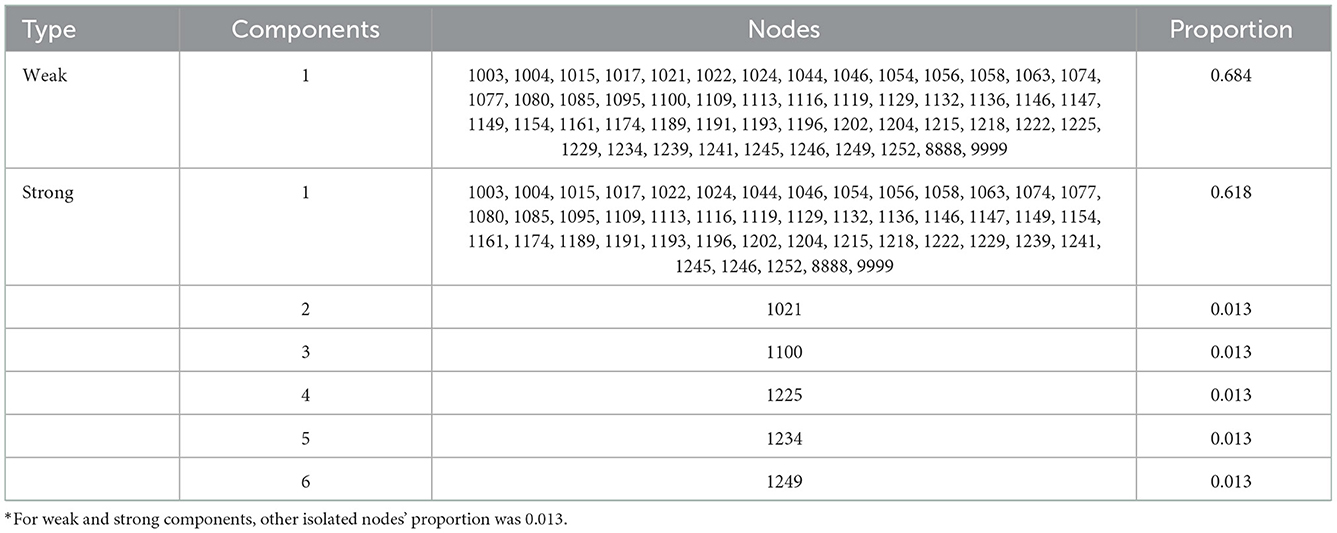
Table 2. The component of intervention group social network nodes except isolation nodes.
There were six strong components in the control group; among these, one component included 17 nodes and the proportion was 25.8%; the other components were parent 1040, parent 1062, parent 1106, parent 1203, and parent 1257, respectively, and the proportion was 1.5%. For the intervention group, there were six strong components; among these, one component included 47 nodes and the proportion was 61.8%; the other components were parent 1021, parent 1100, parent 1225, parent 1234, and parent 1249, respectively, and the overall proportion was 1.3%. This demonstrated that they showed inactive communication with others (Tables 1, 2).
For the control group, four cliques were found: “1079, 1104, and 9999,” “1104, 1111, and 9999,” “1104, 1128, and 9999,” and “1104, 1169, 9999,” respectively. The other parents were not included in any cliques. Based on a “clique-by-clique actor co-membership matrix,” the cliques could combine to form a large clique comprising “1079, 1104, 9999, 1111, 1128, and 1169”; the core of this clique was “1104 and 9999” (Table 3).
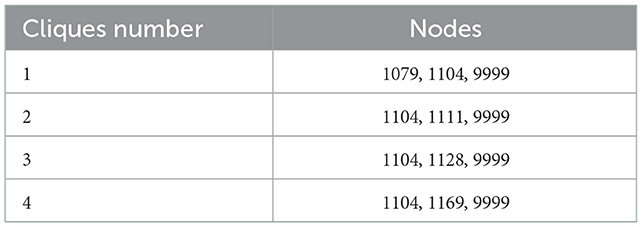
Table 3. The cliques of control group.
For the intervention group, 28 cliques were found, comprising a total of 27 group members' the other parents were not included in any cliques. Based on the “clique-by-clique actor co-membership matrix,” the cliques could be combined to form a large clique comprising “9999, 1074, 1119, 1196, 1004, 1189, 1241, 1056, 1109, 1222, 1080, 1132, 1146, 1174, 1202, 1245, 8888, 1022, 1044, 1058, 1085, 1095, 1147, 1161, 1218, 1239, and 1246.” Here, the main members were “9999, 1074, 1119, and 1004” (Table 4).

Table 4. The cliques of intervention group.
Although, according to the “clique-by-clique actor co-membership matrix,” both the control and intervention group formed large cliques, when compared to the control group the intervention group featured more parents who served as core members and who participated in many cliques. For the control group, the community childcare doctor controlled virtually all communications and answered virtually all of the parents' questions. For the intervention group, more parents participated in communications in the post-intervention period.
From the perspective of their education, high education level (college or above) occurred in some cliques usually, which demonstrated that high education level parents may serve as child-unintentional-injuries-related information transporter in different subgroups. For community childcare doctor, they should arouse high education level parents activity and passion of studying child-unintentional-injuries-related information and teaching other parents according to their understand and exercise.
Tables 5, 6 show, for the control and intervention groups, effective size and constraint, respectively.
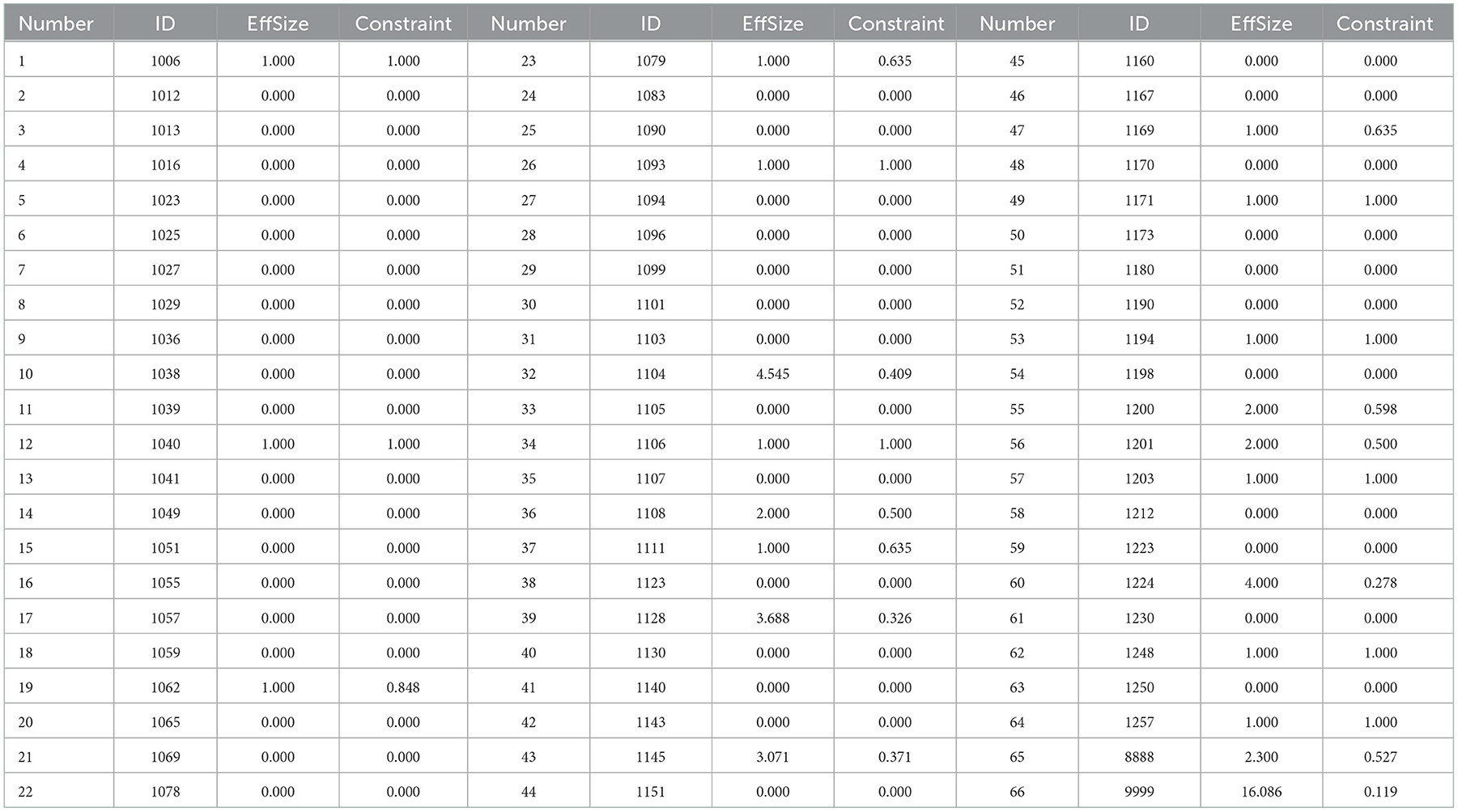
Table 5. The structural hoes of control group.
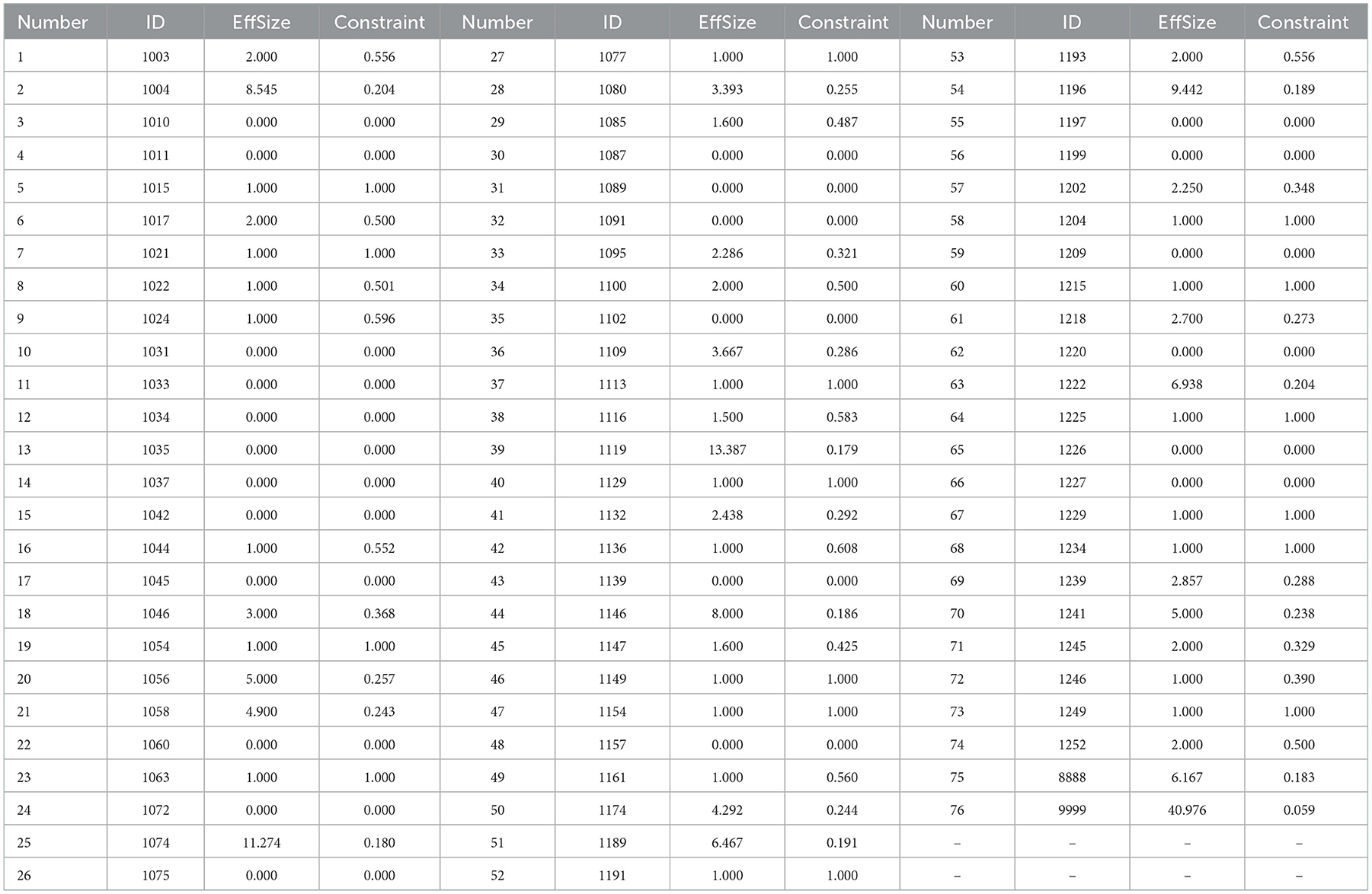
Table 6. The structural holes of intervention group.
For the control group, 7.5% showed an effective size exceeding 2.000, which indicated that they actively participated in interaction and had strong control over and influence on other parents. The community childcare doctor had the largest effective size, at 16.086, and parent 1104, parent 1224, parent 1128, and parent 1145 showed the largest effective sizes among the parents, at 4.545, 4.000, 3.688, and 3.071, respectively. Seventeen (25.8%) parents had effective sizes between 2.000 and 1.000, which demonstrated that they seldom participated in group interaction. Forty-four (66.7%) parents had an effective size of 0.000, meaning they merely viewed the communications without participating.
For the intervention group, 23.7% of the members had effective sizes larger than 2.000, which indicated that they actively participated in the interactions and had strong control over and influence on other parents. The community childcare doctor had the largest effective size, at 40.976, and among the parents, parent 1119, parent 1074, parent 1196, parent 1004, parent 1146, and parent 1222 had the largest effective sizes, at 13.387, 11.274, 9.442, 8.545, 8.000, 6.938, and 6.467, respectively. Meanwhile, some parents had effective sizes of 3.000–5.000. Thirty-four (44.7%) parents had effective sizes between 2.000 and 1.000, demonstrating that they seldom participated in the group interaction. Twenty-four (31.6%) parents had an effective size of 0.000, meaning they only viewed the communications and did not participate in them.
Comparing the control group to the intervention group showed that, besides the community childcare doctor, more parents from the intervention group improved their knowledge about children aged 0–3 years, and the intervention-group parents' participation activity increased after receiving the health education.
For group members who had an effective size of ≥1.000, nine (40.9%) from the control group and 16 (30.8%) from the intervention group showed constraint values of 1.000, which demonstrated that they were strictly constrained by the associated group members, showed the largest constraint or dependence, and that their ability to cross-jump structural holes was very weak. For the other group members, the constraint values were < 1.000, which demonstrated that they were strictly constrained by the associated group members, had smaller constraint or dependence, and very strong ability to cross-jump structural holes.
Compared to the control group, the intervention group showed a closer association.
Considering aforementioned indicators comprehensively, in-degree centrality was associated with out-degree centrality in intervention group and control group (rs = 0.939, P < 0.001; rs = 0.890, P < 0.001), in-closeness centrality was associated with out-closeness centrality in intervention group and control group (rs = 0.745, P < 0.001; rs = 0.716, P < 0.001). It demonstrated that in social network, if parents received much more information from other parents, they will also deliver much more information to other parents so that the communications between parents get strengthened. For aforementioned parents (4 parents in control group and 14 parents in intervention group) who play active role in social network to help community childcare doctor to deliver child-unintentional-injuries-related information and teach other parents, 86.1% parents' education level was college or above, 11.1% parents' education level was senior high school, 2.8% parents' education level was middle school. Percent 25 parents were other and unemployed, they have much more time to care their child.
Above all, high education level parents may serve as community childcare doctors' assistant to provide service or response to other parents. In community parental health education intervention, community health workers can inspire parents' motivation to study child-unintentional-injuries-related information and participate in community health management by implementing health education on high education level parents in the community social network. Additionally, from the perspective of childcare, community health workers should focus on parents who have much more time to accompany with their child and can calculate a certain experience about childcare.
The present study aimed to explore the mechanisms underlying the effect of online-social-media-based parental health-education interventions for improving children's health status and parents' associated knowledge and skills. To perform this exploration, SNA was applied. Comparing the outcomes for the intervention group with those for the control group provided the following main results:
Regarding hypothesis H01, some parents (four parents in the control group and 14 parents in the intervention group) who acquired better knowledge about childcare voluntarily sought to answer other parents' questions, which was effective for relieving the community childcare doctor's workload. Most of these parents were mothers who were married, usually worked in Shanghai, and had undergraduate or higher education level; this suggests that they were better able to locate and acquire knowledge about childcare and to care for children. Comparing the number of core parents in the two groups showed that the intervention group had approximately four times the number of those in the control group, which suggested that the intervention and the communication with the community childcare doctor effectively enhanced the knowledge of the parents in the intervention group. Hence, if parents acquire more knowledge, their roles may transfer from information recipient to a combination of information recipient and sender, and they may then more actively participate in interactions.
Regarding hypothesis H02, the intervention conducted by the doctor and assistant encouraged more parents to participate in interactions between group members. The interactions of the intervention group members were closer than those of the control group members, and the intervention group's centrality also improved significantly when compared to the control group. Comment frequencies and comment days also improved significantly. First, because the doctor and assistant were professionals, if parents had questions they could receive answers quickly from the doctor. Second, the design of the intervention tool focused mainly on potential unintentional injuries and aspects that can be easily missed by parents, meaning the intervention could arouse parents' enthusiasm to participate in interactions. Third, in the WeChat groups parents' questions are visible to all group members, meaning if a parent felt that a question concerned a topic related to their own child, they could participate in the interaction. Additionally, most of the parents were ~30 years old, had a high education level, and were likely to have had discussions with their parents regarding childcare, meaning they were likely to be relatively accustomed to intense discussions on childcare topics. The parents were able to reach a consensus on some aspects by showing their agreement with the community childcare doctor, and this may have encouraged the parents to engage in further study beyond the intervention articles. This indicates that the WeChat-group-based intervention could strengthen and tighten communication between parents and community childcare doctors and between parents and other parents.
Regarding hypothesis H03, a bridge was created between parents, which enhanced their acquiring of childcare knowledge. As only one community childcare doctor was included in the WeChat group, it was difficult to rely solely on communication with the childcare doctor to receive a timely answer to certain questions. After receiving health education, the parents from the intervention group showed a larger effective size and stronger ability to cross-jump structural holes. Through observing the results for centrality, especially betweenness centrality, it was deemed that, although the social networks had multiple centers, the intervention group contained more parents who served as bridges for conveying information. Additionally, according with the aforementioned hypothesis, if other parents asked similar questions these parents were willing to provide answers voluntarily. Through this, the parents shared the doctor's responsibility. Hence, the WeChat-group-based parental health education served to build a bridge to promote interaction between parents rather than merely between parents and the doctor.
From the perspective of the intervention platform and tools, the present study used WeChat as the intervention platform. WeChat is not only free, but is also used widely in China to communicate with others one-to-one or in groups. In addition, this application can help people search for specific information. WeChat has similar functions to Facebook and Twitter, which are widely used in Western countries such as America; this is notable because these social-network systems have been found to potentially be effective for providing health education and for sharing information with others (31). A previous cluster randomized controlled trial explored an app-based unintentional-injuries-prevention intervention that featured a similar design to the intervention tool used in the present study (e.g., the Haddon matrix) (32). The study found that the health education platform and tools were effective for reducing the incidence of unintentional injuries among children.
From the perspective of SNA, some studies of community-based interventions have found that the intervention information can be diffused through social interactions, such as active and voluntary communication with other group members; this is similar to the observations of the present study (59, 60). Further, a previous investigation of a community-based parenting intervention that featured children's primary caregivers as subjects stated that community mobilization is an effective tool for helping children's primary caregivers study how to prevent and reduce health and social risk factors (60). In the present study, health education was conducted through WeChat groups and the intervention articles delivered by the doctor's assistant, with some general introductions to the main content of the articles being included. This process helped to motivate parents to study and acquire related knowledge, which also improved their skills.
The health education conducted in this study was in an mHealth format, and the strengths of this health-education program and study were as follows:
First, this health-education program could shorten social distance. Social distance, one of the components of psychological distance (61), means the degree to which individuals or groups are excluded by others (62). It can influence not only the degree of trust between people, but also their information receptiveness and mutual emotions (63). The present study concluded that a WeChat-group-based intervention can not only eliminate barriers of time and space, but also afford direct communication with others and with community childcare doctors. In addition, this intervention was conducted during the Coronavirus Disease 2019 Pandemic, a time when many people were isolated at home and may have had difficulties attending health-care facilities; mHealth and telemedicine health education represent possible means of mitigating this issue.
Second, health education could save community childcare doctors time. Through expert interviews, the community childcare doctor stated that the health education allowed more parents to acquire childcare knowledge and improve their knowledge and skills relating to preventing children from acquiring injuries. Concurrently, the intervention also encouraged parents to answer other parents' questions, leaving the community childcare doctor to merely judge whether the parents' answers were correct and sufficiently detailed.
Third, the WeChat-group-based parental-health-education intervention imitated real-world communication, lending it a certain sense of realness.
Fourth, this is the first study to explore the mechanism of an online-social-network-based parental-health education intervention designed to reduce the incidence of unintentional injuries among children, and it was found that such an intervention can enhance parents' knowledge, attitudes, and behaviors in this regard.
In contrast, the study also had some limitations:
First, the study featured social desirability bias. This study was conducted in Shanghai, China, where parents generally have a higher level of education (64); this means that, when compared to people from other areas of China (e.g., northern cities), it may have been easier for these parents to learn the content and answer questions in the WeChat groups.
Second, because the health-education platform was online social media, to access the health-education platform a certain level of regional economic development was necessary.
Third, to assess the mechanisms of health education and their effectiveness, two groups were established, a WeChat group containing parents only and a WeChat group that featured parents and a community childcare doctor. However, the parents-only WeChat group still provided a low level of health education. The reason we did not create a blank control is that it is difficult to confirm parents' issues and questions when examining off-line health education.
The interaction of the intervention group was closer than that of the control group, which may indicate that the effectiveness of the health education originates from communication between parents and/or from communication between parents and the community childcare doctor. In short, although SNA is seldom used to analyze the mechanism of unintentional-injury prevention, the present study obtains the same conclusions as similar previous studies (31): that online social community-based health education via social media is an effective way to generally improve health status. The difference between this previous study and the study was study design. The study validated the effectiveness of online social media-based intervention which established two online social communities by randomized controlled trial, which provided a strong evidence to indicate that the implementation of health education through online social communities can be generalized.
The interaction of the intervention group was closer than that of the control group, which could indicate that the effectiveness of the health education originates from communication between parents and/or between parents and the community childcare doctor. In short, although SNA has seldom been used to analyze the mechanism of unintentional-injury prevention, compared with similar studies the present study obtains the same conclusions: that online-social-community-based health education via social media is an effective way to improve general health status. This also indicates that implementing health education through online social communities can be generalized. Parents who received the intervention formed a habit of consulting the community childcare doctor if they had questions regarding childcare. This phenomenon indicates that establishing an online social community that gathers parents in a group and inviting community childcare doctors to participate in the group to provide timely help can foster community interaction that can enhance parents' childcare-related activity. Further, the childcare doctor can also observe inter-parent communication and play a core role in terms of providing education, improving degree of participation, and arousing enthusiasm for group interaction.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Medical Research Ethics Committee, School of Public Health, Fudan University. The patients/participants provided their written informed consent to participate in this study.
YF contributed to data acquisition, analysis, interpretation, drafting, and revision of the manuscript. XL contributed to data acquisition, interpretation, conception, design, and revision of the manuscript. XM contributed to data acquisition, design, and revision of the manuscript. JG and JX contributed to providing some suggestions on study design, questionnaire, and intervention. RJ contributed to study design and suggested the intervention. ZZ and KC contributed to the analysis of words frequencies. JL contributed to the design and revision of the manuscript. All authors contributed to the article and approved the submitted version.
The project was supported by the National Natural Science Foundation of China (Nos. 71974037 and 71573049) and the National Social Science Foundation of China (No. 17ZDA078). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We are grateful to the staff at the Community Health Centers. We would also like to thank all the residents for their participation. We would like to thank Editage (www.editage.cn) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1049851/full#supplementary-material
1. Tupetz A, Friedman K, Zhao D, Liao H, Von Isenburg M, Keating EM, et al. Prevention of childhood unintentional injuries in low- and middle-income countries: a systematic review. PLoS ONE. (2020) 15:e0243464. doi: 10.1371/journal.pone.0243464
2. Yamamoto N, Honda C, Nagata S. Current trends and age-based differences of unintentional injury in Japanese children. Biosci Trends. (2016) 10:152–7. doi: 10.5582/bst.2016.01032
3. Shi X, Shi J, Wheeler KK, Stallones L, Ameratunga S, Shakespeare T, et al. Unintentional injuries in children with disabilities: a systematic review and meta-analysis. Inj Epidemiol. (2015) 2:21. doi: 10.1186/s40621-015-0053-4
4. Pant PR, Towner E, Pilkington P, Ellis M. Epidemiology of unintentional child injuries in the South-East Asia Region: a systematic review. Int J Inj Contr Saf Promot. (2015) 22:24–32. doi: 10.1080/17457300.2013.842594
5. Jiangxi Center for Disease Control. Jiangxi Injury Survey: Child Injury Report. Jiangxi: Jiangxi Center for Disease Control, The Alliance for Safe Children, UNICEF-China, Jiangxi Provincial Health Bureau, Chinese Field Epidemiology Training Program (2006).
7. West BA, Rudd RA, Sauber-Schatz EK, Ballesteros MF. Unintentional injury deaths in children and youth, 2010-2019. J Safety Res. (2021) 78:322–30. doi: 10.1016/j.jsr.2021.07.001
8. Çaylan N, Yalçin SS, Tezel B, Aydin S, Özen Ö, Sengelen M, et al. Evaluation of injury-related under-five mortality in Turkey between 2014-2017. Turk J Pediatr. (2021) 63:37–47. doi: 10.24953/turkjped.2021.01.005
9. Yao M, Wu G, Zhao Z, Luo M, Zhang J. Unintentional injury mortality among children under age five in urban and rural areas in the Sichuan province of west China, 2009–2017. Sci Rep. (2019) 9:2963. doi: 10.1038/s41598-019-38936-6
10. World Health Organization. World Health Statistics 2022: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: WHO (2022).
11. Wang L, Cheng X, Yin P, Cheng P, Liu Y, Schwebel DC, et al. Unintentional drowning mortality in China, 2006–2013. Inj Prev. (2019) 25:47–51. doi: 10.1136/injuryprev-2017-042713
12. Sengoelge M, Hasselberg M, Ormandy D, Laflamme L. Housing, income inequality and child injury mortality in Europe: a cross-sectional study. Child Care Health Dev. (2014) 40:283–91. doi: 10.1111/cch.12027
13. Pearce A, Li L, Abbas J, Ferguson B, Graham H, Law C. Does the home environment influence inequalities in unintentional injury in early childhood? Findings from the UK Millennium Cohort Study. J Epidemiol Community Health. (2012) 66:181–8. doi: 10.1136/jech.2011.139626
14. Jones VC, Shields W, Ayyagari R, Frattaroli S, McDonald EM, Gielen AC. Association between unintentional child injury in the home and parental implementation of modifications for safety. JAMA Pediatr. (2018) 172:1189–1190. doi: 10.1001/jamapediatrics.2018.2781
15. Nocera M, Gjelsvik A, Wing R, Amanullah S. The association of parental coping and childhood injury. Matern Child Health J. (2016) 20:2357–66. doi: 10.1007/s10995-016-2059-0
16. Santagati G, Vezzosi L, Angelillo IF. Unintentional injuries in children up to six years of age and related parental knowledge, attitudes, and behaviors in Italy. J Pediatr. (2016) 177:267–272.e2. doi: 10.1016/j.jpeds.2016.06.083
17. Kendrick D, Mulvaney CA, Ye L, Stevens T, Mytton JA, Stewart-Brown S. Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane Database Syst Rev. (2013) 2013:CD006020. doi: 10.1002/14651858.CD006020.pub3
18. Nansel TR, Weaver NL, Jacobsen HA, Glasheen C, Kreuter MW. Preventing unintentional pediatric injuries: a tailored intervention for parents and providers. Health Educ Res. (2008) 23:656–69. doi: 10.1093/her/cym041
19. Brandtzaeg PB, Følstad A, Chaparro Domínguez MÁ. How journalists and social media users perceive online fact-checking and verification services. J Practice. (2018) 12:1109–29. doi: 10.1080/17512786.2017.1363657
20. Reuters. Reuters Institute Digital News Report 2016. (2016). Available online at: http://www.digitalnewsreport.org/ (accessed August 31, 2022).
21. CNNIC. The 40th Statistical Report on Internet Development in China. (2017). Available online at: http://cnnic.com.cn/IDR/ReportDownloads/201807/P020180711387563090220.pdf (accessed August 2022).
22. CNNIC. The 39th Statistical Report on Internet Development in China. (2017). Available online at: http://cnnic.com.cn/IDR/ReportDownloads/201706/P020170608523740585924.pdf (accessed August 2022).
23. Tencent Technology,. Tencent Announces 2019 Fourth Quarter Results. (2020). Available online at: https://www.tencent.com/uploads/2020/03/18/7fceaf3d1b264debc61342fc1a27dd18.pdf (accessed August 31, 2022).
24. De La Torre-Díez I, López-Coronado M, Vaca C, Aguado JS, de Castro C. Cost-utility and cost-effectiveness studies of telemedicine, electronic, and mobile health systems in the literature: a systematic review. Telemed J E Health. (2015) 21:81–5. doi: 10.1089/tmj.2014.0053
25. Villinger K, Wahl DR, Boeing H, Schupp HT, Renner B. The effectiveness of app-based mobile interventions on nutrition behaviours and nutrition-related health outcomes: a systematic review and meta-analysis. Obes Rev. (2019) 20:1465–84. doi: 10.1111/obr.12903
26. Lee M, Lee H, Kim Y, Kim J, Cho M, Jang J, et al. Mobile app-based health promotion programs: a systematic review of the literature. Int J Environ Res Public Health. (2018) 15:2838. doi: 10.3390/ijerph15122838
27. Ferré-Grau C, Raigal-Aran L, Lorca-Cabrera J, Lluch-Canut T, Ferré-Bergadà M, Lleixá-Fortuño M, et al. A mobile app-based intervention program for nonprofessional caregivers to promote positive mental health: randomized controlled trial. JMIR Mhealth Uhealth. (2021) 9:e21708. doi: 10.2196/21708
28. van Beelen ME, Beirens TM, den Hertog P, van Beeck EF, Raat H. Effectiveness of web-based tailored advice on parents' child safety behaviors: randomized controlled trial. J Med Internet Res. (2014) 16:e17. doi: 10.2196/jmir.2521
29. Renfrew ME, Morton DP, Morton JK, Hinze JS, Beamish PJ, Przybylko G, et al. A web- and mobile app-based mental health promotion intervention comparing email, short message service, and videoconferencing support for a healthy cohort: randomized comparative study. J Med Internet Res. (2020) 22:e15592. doi: 10.2196/15592
30. Chen J, Ho E, Jiang Y, Whittaker R, Yang T, Bullen C. Mobile social network-based smoking cessation intervention for chinese male smokers: pilot randomized controlled trial. JMIR Mhealth Uhealth. (2020) 8:e17522. doi: 10.2196/17522
31. Xu R, Cavallo D. Social network analysis of the effects of a social media-based weight loss intervention targeting adults of low socioeconomic status: single-arm intervention trial. J Med Internet Res. (2021) 23:e24690. doi: 10.2196/24690
32. Ning P, Cheng P, Schwebel DC, Yang Y, Yu R, Deng J, et al. An app-based intervention for caregivers to prevent unintentional injury among preschoolers: cluster randomized controlled trial. JMIR Mhealth Uhealth. (2019) 7:e13519. doi: 10.2196/13519
33. Feng Y, Ma X, Zhang Q, Jiang R, Lu J, Chen K, et al. Effectiveness of WeChat-group-based parental health education in preventing unintentional injuries among children aged 0-3: randomized controlled trial in Shanghai. BMC Public Health. (2022) 22:2086. doi: 10.1186/s12889-022-14462-5
34. Scott J. Social network analysis. Contemp Sociol. (1988) 22:109–27. doi: 10.1177/0038038588022001007
36. Crossley N, Bellotti E, Edwards G, Everette M, Koskinen J, Tranmer M. Social Network Analysis for Ego-Nets. Los Angeles, CA: SAGE (2015). doi: 10.4135/9781473911871
37. Yiu K, Dimaras H, Valdman O, Franklin B, Prochaska J, Loh L. Characterizing a community health partnership in Dominican Republic: network mapping and analysis of stakeholder perceptions. Can Med Educ J. (2018) 9:e60–71. doi: 10.36834/cmej.36924
38. Assegaai T, Schneider H. The supervisory relationships of community health workers in primary health care: social network analysis of ward-based outreach teams in Ngaka Modiri Molema District, South Africa. BMJ Glob Health. (2019) 4:e001839. doi: 10.1136/bmjgh-2019-001839
39. Holtrop JS, Ruland S, Diaz S, Morrato EH, Jones E. Using social network analysis to examine the effect of care management structure on chronic disease management communication within primary care. J Gen Intern Med. (2018) 33:612–20. doi: 10.1007/s11606-017-4247-z
40. Lopreite M, Puliga M, Riccaboni M, De Rosis S. A social network analysis of the organizations focusing on tuberculosis, malaria and pneumonia. Soc Sci Med. (2021) 278:113940. doi: 10.1016/j.socscimed.2021.113940
41. Isba R, Woolf K, Hanneman R. Social network analysis in medical education. Med Educ. (2017) 51:81–8. doi: 10.1111/medu.13152
42. Smit LC, Dikken J, Schuurmans MJ, de Wit NJ, Bleijenberg N. Value of social network analysis for developing and evaluating complex healthcare interventions: a scoping review. BMJ Open. (2020) 10:e039681. doi: 10.1136/bmjopen-2020-039681
43. Lockhart N. Social network analysis as an analytic tool for task group research: a case study of an interdisciplinary community of practice. J Spec Group Work. (2017) 42:152–75. doi: 10.1080/01933922.2017.1301610
44. Cross R, Parker A. The Hidden Power of Social Networks. Boston, MA: Harvard Business School Press (2004).
46. Lwanga SK Lemeshow S World Health Organization. Sample Size Determination in Health Studies: A Practical Manual. Geneva: World Health Organization (1991)
47. Chen H. Effect of health education on prevention of child injuries at home. Occup Health. (2013) 29:1718–21. doi: 10.13329/j.cnki.zyyjk.2013.14.018
48. Choi Y, Ahn HY. Developing and evaluating a mobile-based parental education program for preventing unintentional injuries in early childhood: a randomized controlled trial. Asian Nurs Res. (2021) 15:329–36. doi: 10.1016/j.anr.2021.12.001
49. Cox CM, Kenardy JA, Hendrikz JK. A randomized controlled trial of a web-based early intervention for children and their parents following unintentional injury. J Pediatr Psychol. (2009) 35:581–92. doi: 10.1093/jpepsy/jsp095
50. Liu J. Whole Network Approach: A Practical Guide to UCINET (3rd). Shanghai, China: People's Press (2019).
51. Hanneman RA, Mark R. Introduction to Social Network Methods. Riverside, CA: University of California, Riverside (2005).
52. Wang F, Zhai Y. Social structure and evolvement of WeChat groups: a case study based on text mining. J China Soc Sci Tech Inform. (2016) 35:617–29. doi: 10.3772/j.issn.1000-0135.2016.006.006
53. Jason LA, Stevens E, Kassanits J, Reilly A, Bobak T, Guerrero M, et al. Recovery homes: a social network analysis of Oxford Houses for Native Americans. J Ethn Subst Abuse. (2020) 19:174–89. doi: 10.1080/15332640.2018.1489748
54. van Woudenberg TJ, Simoski B, Araújo EFd, Bevelander KE, Burk WJ, Smit CR, et al. Identifying influence agents that promote physical activity through the simulation of social network interventions: agent-based modeling study. J Med Internet Res. (2019) 21:e12914. doi: 10.2196/12914
55. Freeman LC. Centrality in social networks conceptual clarification. Soc Netw. (1978) 1:215–39. doi: 10.1016/0378-8733(78)90021-7
56. Wasserman S, Faust K. Social Network Analysis. Cambridge, UK: Cambridge University Press (1994). doi: 10.1017/CBO9780511815478
58. Burt RS. Structural Holes: The Social Structure of Competition. Cambridge, MA: Harvard University Press (1992).
59. McGlashan J, Nichols M, Korn A, Millar L, Marks J, Sanigorski A, et al. Social network analysis of stakeholder networks from two community-based obesity prevention interventions. PLoS ONE. (2018) 13:e0196211. doi: 10.1371/journal.pone.0196211
60. Kleyn LM, Hewstone M, Ward CL, Wölfer R. Using longitudinal social network analysis to evaluate a community-wide parenting intervention. Prev Sci. (2021) 22:130–43. doi: 10.1007/s11121-020-01184-6
61. Kim K, Meng Z, Li X. Effects of temporal and social distance on consumer evaluations. J Consum Res. (2008) 35:706–13. doi: 10.1086/592131
62. Bogardus ES. Measurement of personal-group relations. Sociometry. (1947) 10:306–11. doi: 10.2307/2785570
63. Brown G K, Langer A. A general class of social distance measures. Polit Anal. (2017) 24:211–25. doi: 10.1093/pan/mpw002
64. National Statistical Bureau. China Statistical Yearbook. (2020). Available online at: http://www.stats.gov.cn/tjsj/ndsj/2021/indexch.htm (accessed August 31, 2022).
Keywords: unintentional injury, social network analysis, WeChat, online social networks, randomized controlled trial
Citation: Feng Y, Li X, Ma X, Zhu Z, Chen K, Gao J, Xia J, Jiang R and Lu J (2023) Using online social networks to provide a parental health-education intervention for preventing unintentional injuries among children aged 0–3 years: A randomized controlled trial and social network analysis in Shanghai, China. Front. Public Health 10:1049851. doi: 10.3389/fpubh.2022.1049851
Received: 21 September 2022; Accepted: 19 December 2022;
Published: 11 January 2023.
Edited by:
Xiuquan Shi, Zunyi Medical University, ChinaReviewed by:
Peishan Ning, Central South University, ChinaCopyright © 2023 Feng, Li, Ma, Zhu, Chen, Gao, Xia, Jiang and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaohong Li,  bGl4aEBmdWRhbi5lZHUuY24=
bGl4aEBmdWRhbi5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.