
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 06 December 2022
Sec. Public Mental Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1043216
This article is part of the Research TopicPsychosocial, Behavioral, and Clinical Implications for Public Mental Health During the COVID-19 PandemicView all 16 articles
 Juan Jesús García-Iglesias1
Juan Jesús García-Iglesias1 Juan Gómez-Salgado1,2*
Juan Gómez-Salgado1,2* Francisco Javier Fernández-Carrasco3,4Luciano Rodríguez-Díaz5*Juana María Vázquez-Lara5Blanca Prieto-Callejero6
Francisco Javier Fernández-Carrasco3,4Luciano Rodríguez-Díaz5*Juana María Vázquez-Lara5Blanca Prieto-Callejero6 Regina Allande-Cussó7
Regina Allande-Cussó7Background: COVID-19 has caused a series of economic, social, personal, and occupational consequences that may affect the mental health of healthcare workers (HCWs), with the consequent risk of developing suicidal ideation and behaviors.
Objectives: The aim of this study was to identify the main risk factors that may predispose HCWs to suicidal ideation and suicide attempts during the COVID-19 pandemic.
Methods: A systematic review of studies published between January 2020 and August 2022 was conducted following the PRISMA guidelines in the following electronic databases: Pubmed, Scopus, Web of Science, CINAHL, and PsycINFO. Methodological quality was assessed using the critical appraisal tools for non-randomized studies of the Joanna Briggs Institute (JBI). The followed protocol is listed in the International Prospective Register of Systematic Reviews (PROSPERO) with code CRD42022340732.
Results: A total of 34 studies were included in this review. There are a number of underlying factors such as higher rates of depression, anxiety, pre-pandemic lifetime mental disorders or previous lifetime suicide attempt, living alone, having problems with alcohol and/or other drugs, etc. that favor the emergence of suicidal tendencies and ideation in times of COVID-19. Similarly, the pandemic may have precipitated a series of factors such as economic concerns, assessing one's working conditions as poor, having family members or friends infected, changes in services or functions, and feeling discriminated against or stigmatized by society. Other factors such as age, sex, or type of healthcare worker show differences between studies.
Conclusion: Organizations should ensure the adoption of strategies and programmes for early detection of suicides as well as increased attention to the mental health of professions with a high workload.
Systematic review registration: PROSPERO, identifier CRD42022340732.
The WHO (1) estimates that there are more than 700,000 suicide deaths per year. This phenomenon is considered a complex public health problem due to its multivariate casuistry, where psychological, sociocultural, biological, economic, and personal factors may converge.
According to the Columbia Classification Algorithm of Suicide Assessment (C-CASA) (2), there are eight categories related to suicidal behavior. Among these eight categories, we find completed suicide (self-injurious behavior that triggers the death of an individual); suicide attempt (potentially self-injurious behavior in which the individual had the intention to commit suicide); preparatory acts toward imminent suicidal behavior (where the individual takes steps to self-harm but the self or third parties prevent the act of self-harm itself); suicidal ideation (passive thoughts about wanting to be dead or active thoughts about killing oneself but not accompanied by preparatory behavior); and self-injurious behavior (self-injurious behavior where the associated intention to die is unknown and cannot be inferred).
In an attempt to explain what drives a person to commit suicide, to plan and think about it, a number of theories have been established. According to the Interpersonal Theory of Suicide (3), a person will not attempt suicide unless they have both the desire to die by suicide and the ability to do so, so there must be thwarted belongingness and perceived burdensomeness. According to the Integrated Motivational-Volitional Model of Suicidal Behavior, individuals go through three phases in which feelings of defeat and entrapment are key elements, and in which the biopsychosocial context in which suicidal behavior arises, the factors involved in suicidal ideation, and those factors linked to the transition between suicidal ideation and suicidal action are precipitating factors (4). In addition, there are other theories (5) such as the Eco-developmental Model of Suicide Attempts (6), in which individual, relational, community, and social factors converge; the Cultural Theory and Model of Suicide, where there is a cultural component of suicide that goes beyond the individual and can affect relationships, the community, and society; or the Three-Step Theory (7), in which factors such as grief and hopelessness, lack of connection or attachment to other people, the absence of a meaningful job or life project coexist with the capacity for suicide itself, among others.
All these theories refer to risk or predisposing factors for suicidal behavior. The risk factor construct is understood in terms of probability and refers to a variable or factor that predisposes an individual to develop a certain disease or pathology (8). For the general population (3, 9), there are a number of risk factors that predispose to suicidal behavior such as childhood abuse, mental disorders and previous suicide attempts, situations of social isolation, despair, lack of resources, family conflict, incarceration or unemployment, problems with authorities, alcohol and other drug abuse, family history of suicide, diagnosis of physical illness, serotonergic dysfunction, seasonal variation, and personal traits such as impulsivity, predisposition to struggle, and low self-esteem or feelings of shame or guilt. Likewise, females have a higher risk of attempted suicide than males, although males have higher rates of completed suicide (10, 11), a phenomenon known as the gender paradox (12). With all these factors, we have now added a variable such as the pandemic caused by COVID-19 [Coronavirus disease 2019, an infectious disease caused by the Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2)]. The COVID-19 pandemic has led to confinement, limited mobility, changes in people's social lives, and economic problems that have negatively affected both the mental health and wellbeing of individuals (13). Compared to previous epidemics (14), suicide rates may have increased during and after health crises, as corroborated by a systematic review on suicidal ideation and behaviors during the COVID-19 pandemic (15). It is true that in recent years it has become apparent that some occupations are more prone to suicide risk, such as healthcare workers (HCWs), who are 3–5 times more likely to be at risk of suicide (16) and who, as expected, have been closely affected by the different epidemic waves of the COVID-19 pandemic (17). This suggests that suicide rates may be increased by pre-existing or emerging mental health conditions. In fact, it is estimated that the suicide rate among male clinicians is almost 1.5 times higher than that of female clinicians and 2.3 times higher than in the general population (11, 18). Among female nurses, there are also higher suicide rates than in the general population (19). Healthcare professionals appear to have occupation-specific risks for suicide as a result of their highly stressful work environment or the impact of the situations they experience, such as being involved in a physician error, among others (11). The consequences of suicidal ideation can lead to suicide attempts and completed suicide with the resulting personal loss. More specifically, in clinical practice, such thoughts can affect adequate professional performance due to a lack of empathy, kindness, compassion, and active listening skills, in detriment to the quality of care provided (17).
Especially at the beginning of the pandemic, HCWs may have felt worried about infecting their loved ones, may have been afraid of the disease, felt stigmatized and isolated by society, suffered traumatic experiences and ethical dilemmas, and may have been subjected to high levels of stress, anxiety, and depression (20, 21). In addition, in the work environment, many HCWs have lacked personal protective equipment, have had increased patient load, have had to make difficult decisions, have witnessed a high number of deaths of patients under their care, have been forced to double shifts, and have been relocated from their services (22). All this factors have had the potential to undermine the mental health of HCWs, with the consequent risk of developing suicidal ideation and behavior (23). While it is true that the pandemic has fluctuated, a study in Bangladesh (15) found that, from April 2020 to July 2020, the prevalence of suicidal ideation had increased from 5 to 19%, similar figures to those reported by Mortier et al. (24), which range from 4.4 to 13%. In another study, suicidal thoughts had a prevalence of 11% among HCWs, compared to 6% in the general population (25). It should not be disregarded that suicidal ideation is a predictor of future suicide attempts and suicide deaths (26), hence the importance of addressing it at early stages. In this regard, Sahimi et al. (27) and Rodney et al. (21) found that 17% of physicians reported suicidal ideation, of whom 1% had attempted suicide. Furthermore, HCWs are more likely than non-HCWs to succeed in suicide attempts as they have greater access to more lethal drugs and have knowledge about the sufficient dosage to end their lives (28). In the systematic review by Dutheil et al. (20) carried out in 2019, ~1.0% of physicians attempted suicide and 17% of physicians had suicidal ideation. These figures decreased as the pandemic progressed, especially in European countries. The monitoring of cases throughout the pandemic could require a specific approach to this issue, and also more longitudinal studies should be carried out to assess events in this field. As can be seen, there is wide variability and contradictions between different research results affecting suicide. For this reason, the aim of this review was to identify the main risk factors that may predispose a healthcare professional to suicidal ideation and suicide attempts during the COVID-19 pandemic.
A systematic review was conducted following the PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses) (29). The protocol followed is listed in the International Prospective Register of Systematic Reviews (PROSPERO) with code CRD42022340732. Ethical aspects.
The databases used were Pubmed, Scopus, Web of Science, Cumulative Index to Nursing and Allied Health Literature Complete (CINAHL), and PsycINFO. The search strategy used to collect the studies in the aforementioned databases was based on the key words obtained from the PECOT strategy, which yielded the research question: What factors may influence a healthcare professional to present suicide attempts and suicidal ideation during the COVID-19 pandemic? (Table 1).
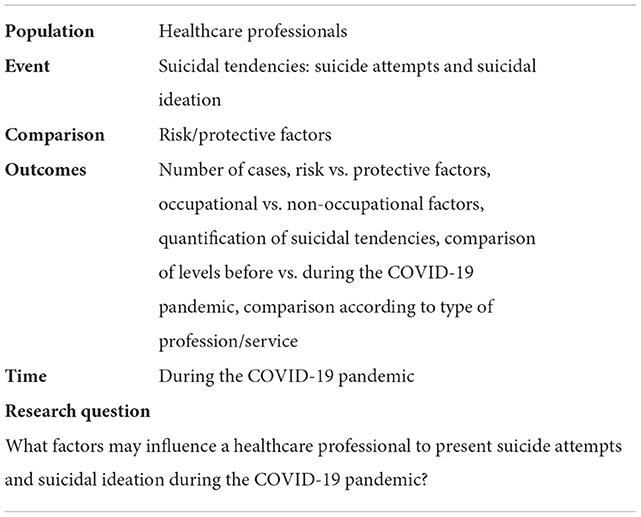
Table 1. PECOT format: keywords.
Following these keywords, the Medical Subject Headings (MeSH) thesaurus was consulted, yielding the descriptors health personnel, COVID-19, and suicide. In order to expand the search for published studies in line with the subject of the study, the use of free terms together with the MeSH descriptors was put in practice through the use of the Boolean operators AND and OR (Table 2).
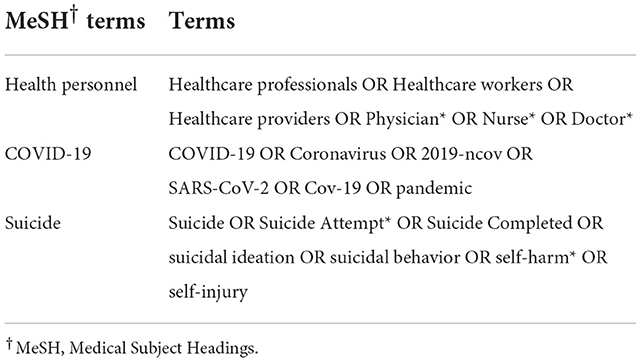
Table 2. Search terms.
Table 3 shows the search strategy used, carried out on 08 August 2022 for each of the above-mentioned databases during the search process.
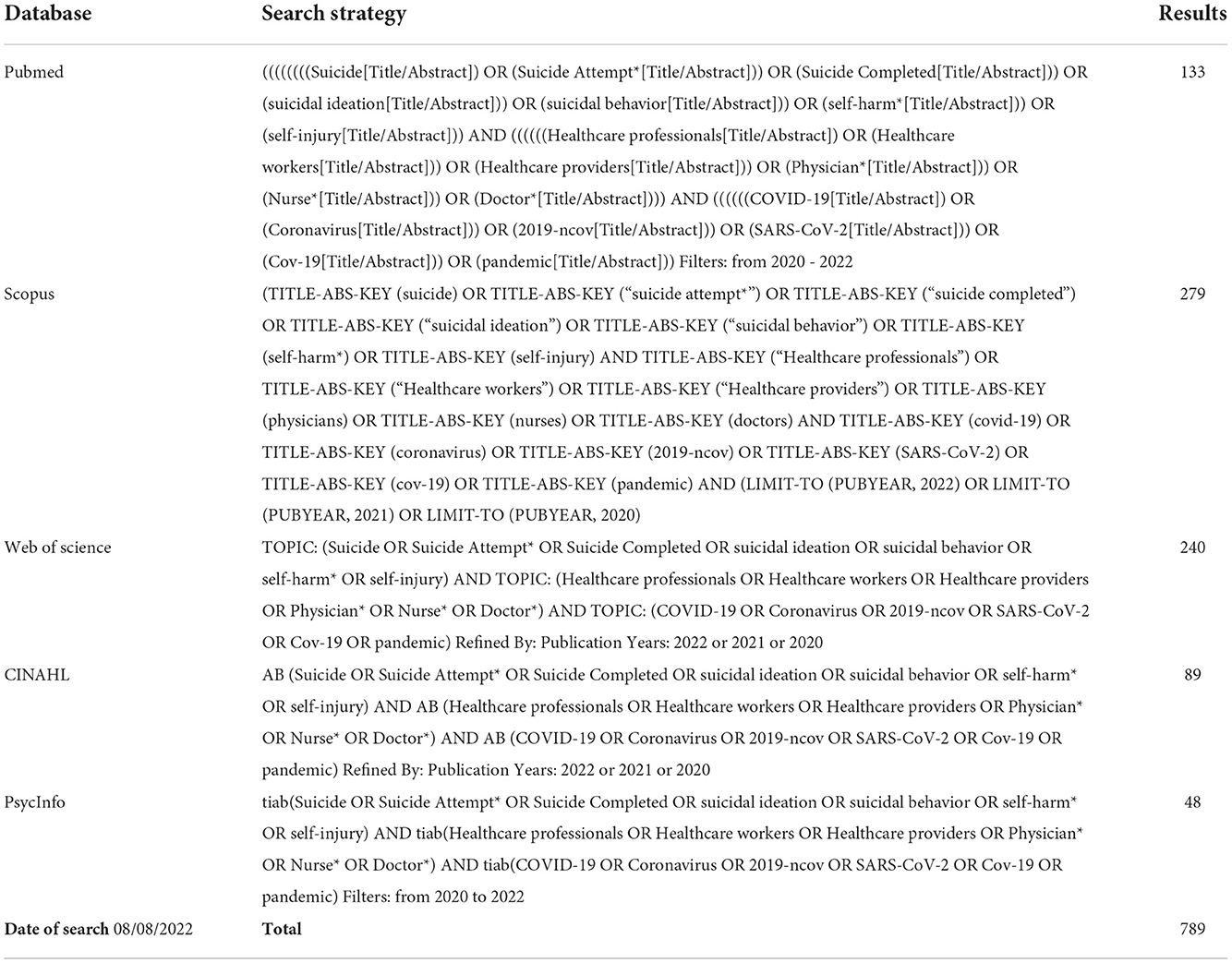
Table 3. Search strategy for each database.
The following inclusion criteria were used for the selection of articles: (1) design criterion: cross-sectional, longitudinal, and interventional studies; (2) language criterion: articles published in English, Spanish, French, and Portuguese; (3) data collection period: articles where data were collected during the COVID-19 pandemic and; (4) outcome measure criterion: articles measuring any of the following values/indicators: number of cases or proportion of suicidal tendencies, risk factors vs. protective factors, occupational vs. non-occupational factors, comparison of levels before vs. during the COVID-19 pandemic, comparison according to type of profession/service/level of exposure to COVID-19. On the other hand, the exclusion criteria were (1) language reasons (language other than English, Spanish, French, and Portuguese); (2) low scientific-technical quality after applying the quality assessment tool; (3) by type of article (published conference proceedings, conference abstracts, and theses or studies including animals); (4) population: students who do not perform healthcare practices; and (5) studies in which the collection date, study population, or measurement instrument could not be determined.
For data collection and extraction, two researchers independently searched the databases according to agreed keywords. They eliminated duplicate studies and selected articles that could be included according to the previously established criteria after reading the title and abstract. Then, these two authors reviewed the full text of the studies that could potentially be included in the review and the decision to include or exclude them in the review was made at this stage by consensus, with a third author having the discretion to include or not a study in case of discrepancy between the two authors. For the selection report, the two authors collected information from the studies regarding authorship, year of publication, country and date of data collection, overall objective, study design, population, measurement instrument, and main results; in addition, the results of the Joanna Briggs Institute (JBI) critical appraisal tool were added.
Two reviewers independently determined the methodological quality of the selected studies using the critical appraisal tools for non-randomized studies of the JBI of the University of Adelaide (30). These tools allow assessing the methodological quality of a study and determining the extent to which a study had minimized the possibility of bias in its design, development, and/or analysis. The versions for cross-sectional quantitative studies (eight items) and for case control studies (10 items) were used, setting the cut-off point at 6/8 for the former and 8/10 for the latter to accept their inclusion in this review (Supplementary material).
The primary search in the databases yielded 789 citations. After eliminating duplicates (n = 288), titles and abstracts of 501 articles were screened. Of these, 414 citations were discarded upon reviewing title and abstract. After having read the full text of the 87 remaining citations, 53 were discarded, either because they contained repeated data (n = 2), the population was not HCWs (n = 8), the data were collected before the pandemic by COVID-19 or the date of collection was not stated (n = 8), the tool was not detailed (n = 3), because of the type of study (n = 12), because the study was not related to the objective (n = 17), and for low quality (n = 3). The flow diagram is presented in Figure 1.
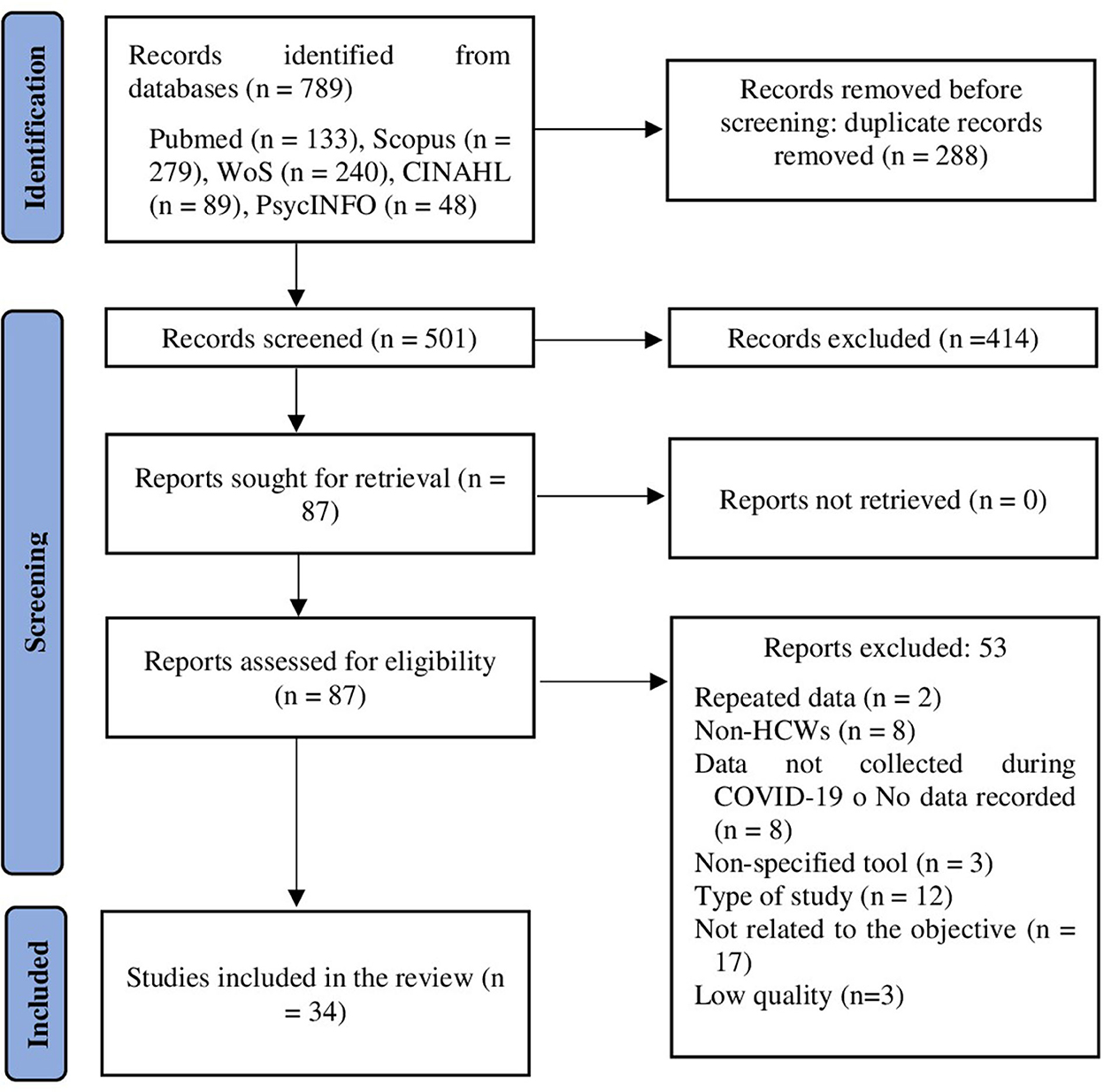
Figure 1. Identification of studies via databases (PRISMA flow diagram).
Table 4 presents the study characteristics of the 34 selected articles. Of the total number of studies, five were conducted in China, five in Spain, four in the United States, four in the United Kingdom, two in Australia, and one in other countries (Bangladesh, Belgium, Brazil, Chile, Colombia, Egypt, Germany, India, Iran, Malaysia, Pakistan, Republic of Ireland, Russia, and Turkey). Regarding the data collection period, in 32 of the 34 studies it was carried out during the year 2020, preferably in the first and second quarter of the year, coinciding with the first wave of the pandemic. Regarding the sample, 5 of the 34 studies only included nurses and 3 of the 34, only physicians; the rest included two or more healthcare professions. Finally, regarding the measurement instrument, 12 of the 34 studies used item 9 of the PHQ-9, 8 of the 34 used the C-SSRS, 5 used a dichotomous question on whether they had suicidal thoughts, and the rest used other instruments (SSEV, question 17 of the SRQ-20, BSSI, CES-D-SI, SIS, CIS-R, Self-Injurious Thoughts and Behavior Interview, and SSI).

Table 4. Characteristics of the studies included in the systematic review.
The included studies were assessed with the JBI critical appraisal tool, where high mean scores were obtained in all the finally included studies.
Suicidal thoughts were reported by 21.7 to 2.4% of HCWs. 0.5 to 12.6% reported at least one lifetime suicide attempt, 0.5 to 3.5% reported a recent suicide attempt, and 3.0 to 0.5% had self-harmed (33, 48, 54).
Major factors associated with increased suicidality include higher rates of depression (27, 32, 33, 36, 37, 39, 40, 55); anxiety (19, 27, 32, 36–39, 52, 55); post-traumatic stress disorder (32, 42); pre-pandemic lifetime mental disorders (24) or previous lifetime suicide attempt; insomnia severity; nightmare frequency; poorer subjective health (32, 33, 36, 47, 60); and burnout (32). In addition, other personal factors predisposing to suicidal thoughts include being female (58); having friends or family members infected with COVID-19 (24, 32, 56); living alone; having poor physical health (32); being single (27, 39), divorced, legally separated, or widowed (24); higher alcohol consumption (32, 34); psychotropic drug use (34, 42); and change in vitamin D levels (45). Younger age is considered a risk factor for some participants (32, 35), a protective factor for others (39), and shows no clear age pattern for the rest (35). Regarding work-related factors during the pandemic, suicidal ideation was associated with financial concerns (24, 32, 34), assessing one's working conditions as poor (34) or perceived lack of preparedness of the health care facility (24); having had job functions changed (51); having been isolated or quarantined for COVID-19 (24, 56); having been moved to a specific workplace related to COVID-19; being an auxiliary nurse (24) or a nurse (44, 46); reporting high workload (34) or stress (56); feeling perceived discrimination (43, 50) and not feeling support from family (47) or superiors (52); and reporting an increased post-pandemic burden (34). As for HCWs coping with COVID-19, no differences in suicidal ideation were found between nurses with and without direct contact with persons with COVID-19 (33, 49, 57), although another study presents discrepancies indicating that frontline HCWs reported a clearly higher presence of thoughts of death (35, 37, 38).
Finally, factors such as having dependent children (32), having a per capita income of more than three minimum monthly wages (34) or higher than 2200 euros (24), resilience and self-perceived social support (35), not having an infected family member, and lower work stress had protective effects on suicidal ideation (47). In addition, HCWs with more than 10 years of service had a significantly lower rate of current suicidal ideation (27).
This study sought to review the factors that may protect or predispose HCWs to suicide attempts and suicidal ideation during the COVID-19 pandemic. The results suggest that there are a number of personal, social, and occupational factors that may predispose HCWs to develop and tend to suicidal ideation, as well as others that may reduce the number of suicidal thoughts and tendencies, such as support systems and certain personal factors.
In previous studies, suicidal behaviors were found to have increased during the pandemic in the general population and in samples of HCWs (61). This already corroborates findings from pre-pandemic studies where suicide rates among HCWs were already higher than those reported in the general population, with differences between men and women, especially among female physicians. There is a wide variability in the prevalence of suicidal ideation and suicide attempts in the different samples consulted within a COVID-19 (38) pandemic setting. This phenomenon could be explained by the variability of the samples, by the impact of disease control measures in each country, as well as by the difference in the levels of stress, anxiety, fear, and depression experienced by HCWs during the pandemic (62). Indeed, in the meta-analytic study by Dragioti et al. (63) of one hundred and seventy-three studies conducted between February and July 2020, the COVID-19 pandemic was found to have a greater impact on mental health in people living in low-income countries, in those who had adopted more restrictive measures, and in more vulnerable populations. Rudenstine et al. (64) consider that the risk factors influencing the general population are those that affect material and economic variables, the social level, and those related to accessing vital resources. In the case of HCWs, these factors may have a different relevance during the pandemic and others may become more relevant, so synergistic relationships may be established between them (55).
In this line, there are a number of factors associated with higher suicidality such as higher rates of depression (27, 32, 33, 36, 37, 39, 40, 55); anxiety (19, 27, 32, 36–39, 52, 55); post-traumatic stress disorder (32, 42); pre-pandemic lifetime mental disorders (24) or previous lifetime suicide attempt; insomnia severity; nightmare frequency; a poorer self-perceived health (32, 33, 36, 47, 60); and burnout (32). In most cases, all these risk factors have increased in impact during the COVID-19 pandemic and, as Mamun and Ullah (65) estimate, approximately 90% of suicides are due to psychological distress in the face of continued exposure to highly stressful situations.
Although most suicidal ideation is due to problems related to psychological distress, the explanation may be varied and multicausal (60, 66). HCWs have been repeatedly exposed to death and pain during the COVID-19 pandemic (67), and as postulated by Smith and Cukrowicz (68), constant exposure to pain and death may favor suicidal behavior and ideation. This may suggest that work environments where there is a higher risk of infection may favor a worsening of the mental health of particularly exposed HCWs (69). In this case, there is certain controversy as to the higher or lower prevalence of suicide rates among frontline HCWs compared to other types of workers. Some studies (33, 49, 57) have found no statistically significant differences in terms of suicidal ideation rates between HCWs working on the front line and those without direct contact. Others, on the other hand, have indeed found differences in this regard (24, 35, 37, 38). In the latter case, this could be justified by a change in the work environment, the functions to be carried out, and a greater perception of risk in relation to the disease. Studies such as the one by Salman et al. (37) estimated that HCWs working on the front line are up to 2.25 times more likely to have suicidal ideation. Changing functions or work location has also been considered by Mediavilla et al. (51) as another risk factor, since it can worsen the mental health of HCWs. In fact, even before the pandemic, there were services in which suicide rates were higher than in others, such as the case of HCWs working in the operating room (70). Other authors found that Internal medicine and other non-surgical specialties had the highest rates of suicidal ideation (39). Other factors such as having been hospitalized due to COVID-19 infection, having had family members infected with COVID-19, and self-perceived probability of contracting COVID-19 may be predisposing factors to the uncertainty caused by the disease (71). In this regard, in a case study of press reports, being infected with COVID-19 was the most common reported reason for suicide, followed by work-related stress, fear of COVID-19 infection, fear of transmitting the virus to others, anxiety about witnessing overwhelming death, and mental distress (14).
On the other hand, a series of factors do not show a clear trend between studies. This is the case of age, sex, or the type of HCW studied. As indicated by Mamun et al. (58), Alvarado et al. (40), Jahan et al. (14), and Mosolova et al. (53), being female may be a risk factor that increases the rates of suicidal ideation compared to males, but other studies such as the one by Bismark et al. (32) and another one by Dobson et al. (44) differ from these conclusions and postulate that males offer higher ideation rates than females. To overcome this dichotomy, homogeneous samples should be compared to avoid possible biases. Being younger is considered a risk factor for some studies (32), a protective factor for others (39), and shows no clear age pattern for the rest (35). In relation to the type of role of the HCW, the prevalence of suicidality may vary. In the study by Mortier et al. (52) in Spain, an auxiliary nurse was 2 times more likely to develop suicidal thoughts and behaviors. In the case of the study by Greenberg et al. (46), 1 in 5 nurses reported suicidal thoughts compared to 1 in 10 physicians. Likewise, in the study by Mosolova et al. (53), the group with the highest risk was that of physicians, compared to the rest of HCWs. In contrast, in the study by Xu et al. (56), physicians, nurses, technicians, and administrators showed a similar prevalence. In this vein, the study by Dobson et al. (44) carried out in Australia (April–May, 2020) on a sample of 320 HCWs, suicidal ideation was more present among nurses. The differences between groups may respond to the fact that nurses may have a more intense nurse-patient relationship than other professionals because of the long hours they spend with patients.
Just as some factors have proven to be predisposing to suicidal tendencies and behaviors, there are others that can be considered protective. In many cases, these factors are related to the support system that the HCW has at the individual, family, and work level. Factors such as having dependent children (32), per capita income > 3 minimum monthly wages (34) or higher than 2200 euros (24), resilience and self-perceived social support (35), no family member infected, and lower job-related stress had protective effects on suicidal ideation (47). In addition, HCWs with more than 10 years of service duration had a significantly lower rate of current suicidal ideation (27).
All in all, the findings of this review show that the context surrounding the COVID-19 pandemic at the social, occupational, family, personal, and public health levels may have had an impact on suicidal ideation and suicide attempts in the general population and, in particular, in healthcare workers as a result of the factors they are exposed to in their professional performance and the social and healthcare context that surrounds them. It is true, though, as previously mentioned, that suicidal ideation and suicide attempts will not only depend on the extrinsic factors that affect the healthcare worker in a pandemic context, but internal factors related to previous health problems, adequate support networks, financial solvency, among others, are also particularly relevant.
This systematic review is not without limitations. Firstly, most of the included studies were cross-sectional and used hetero-administered instruments via online surveys. In this sense, population characteristics, methodological differences, heterogeneous samples, etc. meant that the resulting findings were very heterogeneous. Thirdly, the timing of data collection and measures of confinement/isolation was different in each study, hence the data were considered inadequate for meta-analysis. Finally, the health system, the allocation of resources for mental health promotion, as well as the adoption of preventive measures adopted by different countries may differ, and these deviations may influence the comparability of indicators.
There are a number of underlying factors such as higher rates of depression, anxiety, pre-pandemic lifetime mental disorders or previous lifetime suicide attempt, living alone, having problems with alcohol and/or other drugs, etc. that favor the emergence of suicidal tendencies and ideation in times of COVID-19. Similarly, there are a series of factors that the pandemic may have precipitated, such as economic concerns, assessing one's working conditions as poor, having infected family members or friends, changes in services or functions, feeling discriminated against or stigmatized by society. Other factors such as age, sex, or type of HCW differ between studies.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
FF-C, RA-C, JG-S, and JV-L: conceptualization and writing–review and editing. BP-C, JV-L, and JG-I: data curation. BP-C, FF-C, RA-C, JV-L, and JG-I: formal analysis. BP-C and FF-C: investigation. RA-C, JG-S, JV-L, and JG-I: methodology. RA-C, JG-S, and JG-I: project administration. BP-C, FF-C, RA-C, JG-S, JV-L, and JG-I: resources. BP-C and RA-C: software. RA-C, JG-S, and JV-L: supervision. FF-C, RA-C, JG-S, and JG-I: validation. BP-C, JG-S, JV-L, and JG-I: visualization. BP-C, FF-C, and JG-I: writing–original draft. All authors contributed to the article and approved the submitted version.
Funding for open access charge: Universidad de Huelva/CBUA.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1043216/full#supplementary-material
1. World Health Organization. Suicide. Geneva: World Health Organization. (2021). Available online at: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed October 24, 2022).
2. Posner K, Oquendo MA, Gould M, Stanley B, Davies M. Columbia classification algorithm of suicide assessment (C-CASA): classification of suicidal events in the FDA's pediatric suicidal risk analysis of antidepressants. Am J Psychiatry. (2007) 164:1035–43. doi: 10.1176/ajp.2007.164.7.1035
3. Van Orden KA, Witte TK, Cukrowicz KC, Braithwaite SR, Selby EA, Joiner TE. The interpersonal theory of suicide. Psychol Rev Psychol Rev. (2010) 117:575–600. doi: 10.1037/a0018697
4. Ordóñez-Carrasco JL, Cuadrado-Guirado I, Rojas-Tejada AJ. Experiential avoidance in the context of the integrated motivational–volitional model of suicidal behavior: A moderation study. Cris J Cris Interv Suicide Prev. (2021) 9:284–91. doi: 10.1027/0227-5910/a000721
5. Zayas LH, Lester RJ, Cabassa LJ, Fortuna LR. Why do so many latina teens attempt suicide? A conceptual model for research. Am J Orthopsychiatry. (2005) 75:275–87. doi: 10.1037/0002-9432.75.2.275
6. Centers for Disease Control Prevention. The Social-Ecological Model: A Framework for Prevention. Washington, DC: Centers for Disease Control and Prevention; (2017). Available online at: https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (accessed October 24, 2022).
7. David Klonsky E, May AM. The three-step theory (3ST): A new theory of suicide rooted in the “ideation-to-action” framework. Int J Cogn Ther. (2015) 8:114–29. doi: 10.1521/ijct.2015.8.2.114
8. Wagner BM. Family risk factors for child and adolescent suicidal behavior. Psychol Bull Psychol Bull. (1997) 121:246–98. doi: 10.1037/0033-2909.121.2.246
9. Centers for Disease Control and Prevention. Suicide Prevention-Risk and Protective Factors. Washington, DC: Centers for Disease Control and Prevention (2021).
10. Barroso-Martínez AA, Barroso-Martínez AA. Comprender el suicidio desde una perspectiva de género: una revisión crítica bibliográfica [Understanding suicide from a gender perspective: a critical literature review]. Rev la Asoc Española Neuropsiquiatría Asociación Española de Neuropsiquiatría. (2019) 39:51–66. doi: 10.4321/s0211-57352019000100004
11. Patel M, Swift S, Digesu A. Mental health among clinicians: what do we know and what can we do? Int Urogynecol J. (2021) 32:1055–9. doi: 10.1007/s00192-021-04805-y
12. Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. (1998) 28:1–23. doi: 10.1111/j.1943-278X.1998.tb00622.x
13. García-Iglesias JJ, Gómez-Salgado J, Martín-Pereira J, Fagundo-Rivera J, Ayuso-Murillo D, Martínez-Riera JR, et al. Impacto del SARS-CoV-2 (COVID-19) en la salud mental de los profesionales sanitarios: una revisión sistemática. [Impact of SARS-CoV-2 (COVID-19) on the mental health of healthcare professionals: a systematic review]. Rev Esp Salud Publica. (2020) 94:23.
14. Jahan I, Ullah I, Griffiths MD, Mamun MA. COVID-19 suicide and its causative factors among the healthcare professionals: Case study evidence from press reports. Perspect Psychiatr Care. (2021) 57:1707–11. doi: 10.1111/ppc.12739
15. Mamun MA. Suicide and suicidal behaviors in the context of COVID-19 pandemic in Bangladesh: a systematic review. Psychol Res Behav Manag. (2021) 14:695–704. doi: 10.2147/PRBM.S315760
16. Kalmoe MC, Chapman MB, Gold JA, Giedinghagen AM. Physician suicide: a call to action. Mo Med. (2019) 116:211–6.
17. Blacker CJ, Lewis CP, Swintak CC, Bostwick JM, Rackley SJ. Medical student suicide rates: a systematic review of the historical and international literature. Acad Med. (2019) 94:274–80. doi: 10.1097/ACM.0000000000002430
18. Young KP, Kolcz DL, O'Sullivan DM, Ferrand J, Fried J, Robinson K. Health care workers' mental health and quality of life during COVID-19: Results from a mid-pandemic, national survey. Psychiatr Serv. (2021) 72:122–8. doi: 10.1176/appi.ps.202000424
19. Ariapooran S, Ahadi B, Khezeli M. Depression, anxiety, and suicidal ideation in nurses with and without symptoms of secondary traumatic stress during the COVID-19 outbreak. Arch Psychiatr Nurs. (2022) 37:76–81. doi: 10.1016/j.apnu.2021.05.005
20. Dutheil F, Aubert C, Pereira B, Dambrun M, Moustafa F, Mermillod M, et al. Suicide among physicians and health-care workers: A systematic review and meta-analysis. PLoS ONE. (2019) 14:193. doi: 10.2139/ssrn.3397193
21. Rodney T, Heidari O, Miller HN, Thornton CP, Jenkins E, Kang HK. Posttraumatic stress disorder in nurses in the United States: prevalence and effect on role. J Nurs Manag. (2022) 30:226–33. doi: 10.1111/jonm.13478
22. Liu CY, Yang YZ, Zhang XM, Xu X, Dou QL, Zhang WW, et al. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: a cross-sectional survey. Epidemiol Infect. (2020) 148:e98. doi: 10.1017/S0950268820001107
23. Awan S, Diwan MN, Aamir A, Allahuddin Z, Irfan M, Carano A, et al. Suicide in healthcare workers: determinants, challenges, and the impact of COVID-19. Front Psychiatry. (2022) 12: 792925. doi: 10.3389/fpsyt.2021.792925
24. Mortier P, Vilagut G, Alayo I, Ferrer M, Amigo FF, Aragonès E, et al. Four-month incidence of suicidal thoughts and behaviors among healthcare workers after the first wave of the Spain COVID-19 pandemic. J Psychiatr Res. (2022) 149:10–7. doi: 10.1017/S2045796021000093
25. Phiri P, Ramakrishnan R, Rathod S, Elliot K, Thayanandan T, Sandle N, et al. An evaluation of the mental health impact of SARS-CoV-2 on patients, general public and healthcare professionals: a systematic review and meta-analysis. EClin Med. (2021) 34:100806. doi: 10.1016/j.eclinm.2021.100806
26. Hubers AAM, Moaddine S, Peersmann SHM, Stijnen T, Duijn E Van, Mast RC Van Der, et al. Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations : a meta-analysis. Epidemiol Psychiatr Sci. (2019) 2:186–98. doi: 10.1017/S2045796016001049
27. Sahimi HMS, Mohd Daud TI, Chan LF, Shah SA, Rahman FHA, Nik Jaafar NR. Depression and suicidal ideation in a sample of malaysian healthcare workers: a preliminary study during the COVID-19 pandemic. Front Psychiatry. (2021) 12: 658174. doi: 10.3389/fpsyt.2021.658174
28. Kingston AM. Break the silence: physician suicide in the time of COVID-19. Mo Med. (2020) 117:426–9.
29. Moher D, Liberati A, Tetzlaff J ADPG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
30. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Manual for Evidence Synthesis. Adelaide: JBI (2020).
31. Brady C, Fenton C, Loughran O, Hayes B, Hennessy M, Higgins A, et al. Nursing home staff mental health during the COVID-19 pandemic in the Republic of Ireland. Int J Geriatr Psychiatry. (2022) 37:5648. doi: 10.1002/gps.5648
32. Bismark M, Scurrah K, Pascoe A, Willis K, Jain R, Smallwood N. Thoughts of suicide or self-harm among Australian healthcare workers during the COVID-19 pandemic. Aust N Z J Psychiatry. (2022) 7:48674221075540. doi: 10.1192/bjo.2022.509
33. Höller I, Forkmann T, Hoeller I, Forkmann T, Höller I, Forkmann T. Ambivalent heroism? – Psychological burden and suicidal ideation among nurses during the COVID-19 pandemic. Nurs Open. (2022) 9:785–800. doi: 10.1002/nop2.1130
34. Oliveira MM de, Treichel CADS, Bakolis I, Alves PF, Coimbra VCC, Cavada GP, et al. Mental health of nursing professionals during the COVID-19 pandemic: a cross-sectional study. Rev Saude Publica. (2022) 56:8. doi: 10.11606/s1518-8787.2022056004122
35. Ortiz-Calvo E, Martínez-Alés G, Mediavilla R, González-Gómez E, Fernández-Jiménez E, Bravo-Ortiz MF, et al. The role of social support and resilience in the mental health impact of the COVID-19 pandemic among healthcare workers in Spain. J Psychiatr Res. (2022) 148:181–7. doi: 10.1016/j.jpsychires.2021.12.030
36. Que J-Y, Shi L, Yan W, Chen S-J, Wu P, Sun S-W, et al. Nightmares mediate the association between traumatic event exposure and suicidal ideation in frontline medical workers exposed to COVID-19. J Affect Disord. (2022) 304:12–9. doi: 10.1016/j.jad.2022.02.033
37. Salman M, Mallhi TH, Khan YH, Mustafa ZU, Shehzadi N, Khan TM, et al. Suicidal ideation amid COVID-19 pandemic: a cross-sectional study among healthcare workers during the first wave of COVID-19 in Pakistan. Disaster Med Public Health Prep. (2022) 12:1–2. doi: 10.1017/dmp.2022.124
38. Abdelghani M, Hassan MS, Elgohary HM, Fouad E. Exploring the factors associated with coronaphobia among physicians during the COVID-19 outbreak in Egypt. Egypt J Neurol Psychiatry Neurosurg. (2021) 57:105. doi: 10.1186/s41983-021-00357-6
39. Al-Humadi S, Bronson B, Muhlrad S, Paulus M, Hong H, Cáceda R. Depression, suicidal thoughts, and burnout among physicians during the COVID-19 pandemic: a survey-based cross-sectional study. Acad Psychiatry. (2021) 45:557–65. doi: 10.1007/s40596-021-01490-3
40. Alvarado R, Ramírez J, Lanio Í, Cortés M, Aguirre A, Bedregal P, et al. Impact of COVID-19 pandemic on the mental health of healthcare workers. Rev Med Chil. (2021) 149:1205–14. doi: 10.4067/s0034-98872021000801205
41. Amsalem D, Lazarov A, Markowitz JC, Naiman A, Smith TE, Dixon LB, et al. Psychiatric symptoms and moral injury among US healthcare workers in the COVID-19 era. BMC Psychiatry. (2021) 21:1–8. doi: 10.1186/s12888-021-03565-9
42. Bruffaerts R, Voorspoels W, Jansen L, Kessler RC, Mortier P, Vilagut G, et al. Suicidality among healthcare professionals during the first COVID19 wave. J Affect Disord. (2021) 283:66–70. doi: 10.1016/j.jad.2021.01.013
43. Campo-Arias A, Jiménez-Villamizar MP, Caballero-Domínguez CC. Healthcare workers' distress and perceived discrimination related to COVID-19 in Colombia. Nurs Heal Sci. (2021) 23:763–7. doi: 10.1111/nhs.12854
44. Dobson H, Malpas CB, Burrell AJC, Gurvich C, Chen L, Kulkarni J, et al. Burnout and psychological distress amongst Australian healthcare workers during the COVID-19 pandemic. Austr Psychiatry. (2021) 29:26–30. doi: 10.1177/1039856220965045
45. Duru H. The Continuing effect of COVID-19 pandemic on physical well-being and mental health of ICU healthcare workers in turkey: a single-centre cross-sectional later-phase study. J Intensive Care Med. (2021) 37:1206–14. doi: 10.1177/08850666211070740
46. Greenberg N, Weston D, Hall C, Caulfield T, Williamson V, Fong K. Mental health of staff working in intensive care during COVID-19. Occup Med. (2021) 71:62–7. doi: 10.1093/occmed/kqaa220
47. Hong S, Ai M, Xu X, Wang W, Chen J, Zhang Q, et al. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-19 outbreak in China: a cross-sectional study. Nurs Outlook. (2021) 69:6–12. doi: 10.1016/j.outlook.2020.07.007
48. Lamb D, Gnanapragasam S, Greenberg N, Bhundia R, Carr E, Hotopf M, et al. Psychosocial impact of the COVID-19 pandemic on 4378 UK healthcare workers and ancillary staff: Initial baseline data from a cohort study collected during the first wave of the pandemic. Occup Environ Med. (2021) 78:801–8. doi: 10.1136/oemed-2020-107276
49. Majumder P, Jeve Y, Sales CP. Voices from the frontline: The psychological impact and coping mechanisms used by healthcare staff during COVID-19. Br J Heal Care Manag. (2021) 27:1–11. doi: 10.12968/bjhc.2020.0168
50. Mediavilla R, Fernández-Jiménez E, Andreo J, Morán-Sánchez I, Muñoz-Sanjosé A, Moreno-Küstner B, et al. Association between perceived discrimination and mental health outcomes among health workers during the initial COVID-19 outbreak. Rev Psiquiatr Salud Ment. (2021) 18:S1888. doi: 10.1016/j.rpsm.2021.06.001
51. Mediavilla R, Fernández-Jiménez E, Martinez-Ales G, Moreno-Kustner B, Martinez-Morata I, Jaramillo F, et al. Role of access to personal protective equipment, treatment prioritization decisions, and changes in job functions on health workers' mental health outcomes during the initial outbreak of the COVID-19 pandemic. J Affect Disord. (2021) 295:405–9. doi: 10.1016/j.jad.2021.08.059
52. Mortier P, Vilagut G, Ferrer M, Serra C, de Dios Molina J, López-Fresneña N, et al. Thirty-day suicidal thoughts and behaviors among hospital workers during the first wave of the Spain COVID-19 outbreak. Depress Anxiety. (2021) 38:528–44. doi: 10.1002/da.23129
53. Mosolova E, Sosin D, Mosolov S. Stress, anxiety, depression and burnout in frontline healthcare workers during two peaks of COVID-19 pandemic in Russia. Psychiatry Res. (2021) 306:114226. doi: 10.1016/j.psychres.2021.114226
54. Murata S, Rezeppa T, Thoma B, Marengo L, Krancevich K, Chiyka E, et al. The psychiatric sequelae of the COVID-19 pandemic in adolescents, adults, and health care workers. Dep Anxiety. (2021) 38:233–46. doi: 10.1002/da.23120
55. Parthasarathy R, Jaisoorya TS, Thennarasu K, Murthy P. Mental health issues among health care workers during the COVID-19 pandemic – A study from India. Asian J Psychiatr. (2021) 58:102626. doi: 10.1016/j.ajp.2021.102626
56. Xu X, Wang W, Chen J, Ai M, Shi L, Wang L, et al. Suicidal and self-harm ideation among Chinese hospital staff during the COVID-19 pandemic: prevalence and correlates. Psychiatry Res. (2021) 296:113654. doi: 10.1016/j.psychres.2020.113654
57. Cai Q, Feng H, Huang J, Wang M, Wang Q, Lu X, et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: a case-control study. J Affect Disord. (2020) 275:210–5. doi: 10.1016/j.jad.2020.06.031
58. Mamun MA, Akter T, Zohra F, Sakib N, Bhuiyan AKMI, Banik PC, et al. Prevalence and risk factors of COVID-19 suicidal behavior in Bangladeshi population: are healthcare professionals at greater risk? Heliyon. (2020) 6:e05259. doi: 10.1016/j.heliyon.2020.e05259
59. Rathod S, Pallikadavath S, Young AH, Graves L, Rahman MM, Brooks A, et al. Psychological impact of COVID-19 pandemic: Protocol and results of first three weeks from an international cross-section survey - focus on health professionals. J Affect Disord Reports. (2020) 1:100005. doi: 10.1016/j.jadr.2020.10000
60. Xiaoming X, Ming A, Su H, Wo W, Jianmei C, Qi Z, et al. The psychological status of 8817 hospital workers during COVID-19 Epidemic: a cross-sectional study in Chongqing. J Affect Disord. (2020) 276:555–61. doi: 10.1016/j.jad.2020.07.092
61. Dubé JP, Smith MM, Sherry SB, Hewitt PL, Stewart SH. Suicide behaviors during the COVID-19 pandemic: a meta-analysis of 54 studies. Psychiatry Res. (2021) 301:113998. doi: 10.1016/j.psychres.2021.113998
62. Efstathiou V, Stefanou M-I, Siafakas N, Makris M, Tsivgoulis G, Zoumpourlis V, et al. Suicidality and COVID-19: suicidal ideation, suicidal behaviors and completed suicides amidst the COVID-19 pandemic (Review). Exp Ther Med. (2021) 23:1–8. doi: 10.3892/etm.2021.11030
63. Dragioti E, Li H, Tsitsas G, Lee KH, Choi J, Kim J, et al. A large-scale meta-analytic atlas of mental health problems prevalence during the COVID-19 early pandemic. J Med Virol. (2022) 94:1935–49. doi: 10.1002/jmv.27549
64. Rudenstine S, Schulder T, Bhatt KJ, McNeal K, Ettman CK, Galea S. Suicidal ideation during COVID-19: The contribution of unique and cumulative stressors. Psychiatry Res. (2022) 310:114475. doi: 10.1016/j.psychres.2022.114475
65. Mamun MA, Ullah I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty? – The forthcoming economic challenges for a developing country. Brain Behav Immun. (2020) 87:163–6. doi: 10.1016/j.bbi.2020.05.028
66. Batterham PJ, van Spijker BAJ, Mackinnon AJ, Calear AL, Wong Q, Christensen H. Consistency of trajectories of suicidal ideation and depression symptoms: evidence from a randomized controlled trial. Depress Anxiety. (2019) 36:321–9. doi: 10.1002/da.22863
67. Reger MA, Piccirillo ML, Buchman-Schmitt JM. COVID-19, mental health, and suicide risk among health care workers: looking beyond the crisis. J Clin Psychiatry. (2020) 81:20com13381. doi: 10.4088/JCP.20com13381
68. Smith PN, Cukrowicz KC. Capable of Suicide: A functional model of the acquired capability component of the interpersonal-psychological theory of suicide. Suicide Life-Threatening Behav. (2010) 40:266–75. doi: 10.1521/suli.2010.40.3.266
69. Lin CY, Alimoradi Z, Ehsani N, Ohayon MM, Chen SH, Griffiths MD, et al. Suicidal ideation during the COVID-19 pandemic among a large-scale iranian sample: the roles of generalized trust, insomnia, and fear of COVID-19. Healthcare. (2022) 10:1–11. doi: 10.3390/healthcare10010093
70. Shanafelt TD, Dyrbye LN, West CP, Sinsky C, Tutty M, Carlasare LE, et al. Suicidal ideation and attitudes regarding help seeking in us physicians relative to the US working population. Mayo Clin Proc. (2021) 96:2067–80. doi: 10.1016/j.mayocp.2021.01.033
Keywords: COVID-19, health personnel, suicide, mental health, risk factors, public health
Citation: García-Iglesias JJ, Gómez-Salgado J, Fernández-Carrasco FJ, Rodríguez-Díaz L, Vázquez-Lara JM, Prieto-Callejero B and Allande-Cussó R (2022) Suicidal ideation and suicide attempts in healthcare professionals during the COVID-19 pandemic: A systematic review. Front. Public Health 10:1043216. doi: 10.3389/fpubh.2022.1043216
Received: 13 September 2022; Accepted: 18 November 2022;
Published: 06 December 2022.
Edited by:
Wai-kit Ming, City University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Guanhua Fan, Shantou University, ChinaCopyright © 2022 García-Iglesias, Gómez-Salgado, Fernández-Carrasco, Rodríguez-Díaz, Vázquez-Lara, Prieto-Callejero and Allande-Cussó. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Gómez-Salgado, c2FsZ2Fkb0B1aHUuZXM=; Luciano Rodríguez-Díaz, bHVjaWFub3JkQHVnci5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.