 BinBin Su
BinBin Su Yu Wu
Yu Wu Zhao Yihao
Zhao Yihao Chen Chen
Chen Chen- School of Population Medicine and Public Health, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
Objectives: China has implemented an equalization of public health Services policy for migrants in 40 pilot cities since 2013. The main objective of this study is to explore the effect of this migrant-based reform policy on the health status of the migrant population in China.
Methods: Using the China Migrants Dynamic Survey (CMDS), we included 152,000 migrants aged 15 years or over in 2018. Standardized questionnaires were used to collect socio-economic information and self-reported health status. The Associations between the equalization of public health services and health status were estimated using Multiple regression estimation models and Propensity Score Matching (PSM) methods.
Results: Public health equalization reform in China has a significant and positive effect on the health status of the migrant population (β = 0.033, p < 0.001). Compared to males, higher income, under 60 years of age, inter-provincial mobility, and migrants those already living in urban areas, the equalization of public health Services had shown more significant positive effects on the groups who were inter-provincial migration (β = 0.055, p < 0.001), females (β = 0.055, p < 0.001), having low-income (β = 0.077, p < 0.001), aged over 60 years old (β = 0.191, p < 0.001), and living in rural areas (β = 0.038, p < 0.001). And multiple robustness tests prove that the above results are reliable.
Conclusions and implications: Our findings confirmed the positive health effect of the equalization of public health services reform on china's migrant population, especially among vulnerable groups such as those in low income groups, in rural areas and females. And we recommend that it is necessary to further promote the practices and experiences of the pilot cities. First, strengthen health education for the mobile population and improve their health literacy. Second, further increase the financial investment to improve the coverage of public health services and the equity in resource allocation among regions. Last, strengthen the information-based management of the migrant population and prevent and control infectious diseases.
1. Introduction
Internal migration refers to the movement of persons within a particular geopolitical unit, which is a common phenomenon in many countries and regions worldwide, such as the United States, Europe, and China (1–5). The migrant population has made indelible contributions to China's rapid economic development, and migration is sometimes an important survival strategy for millions of people living in rural areas (6).
China has the largest migrant population in the world. According to the Seventh National Population Census, in 2020, there were 376 million migrants in China, among which 33.2% of migrants had moved from one province to another, and these figures have increased by 69.73 and 85.70% respectively, compared to the sixth National Population Census of 2010 (4). With the advancement of urbanization, the scale of the migrant population in China has changed from a continuous rising mode to a slow declining mode since 2015. The migrant population reportedly declined by 1.71 and 0.82 million respectively in 2016 and 2017 compared with 2015. Despite this, the number of migrants is still considerable due to China's huge population base.
In China, internal migrants are those whose current address does not coincide with their household registration, also known as Hukou (7). Most public policies and social benefits in China are configured and formulated on the basis of Hukou in China, rather than on the basis of the population actually living in a certain area (8). As a result, many social benefits, including health care coverage, are restricted to the urban domestic population, while the migrant population has no access or limited access (9).
While a large number of migrant movements have provided human resources to meet the growing market demand as a result of China's growing economy (10), the population health has not developed synchronously (11), and the public health services of these migrant communities lag behind that of permanent residents (12). Accompanied by the registered the residence status, the migrant population usually faces unequal treatment with the inflow of urban residents in terms of access to urban public services and social welfare, especially equal public health services (13). Therefore, they usually face more health risks than the urban residents. Although the legal right to health care for migrants varies from country to country, health practitioners report that they face similar problems when caring for the migrant population, including access problems, limited communication, and associated legal issues (14).
To improve this situation, in 2013, the Chinese government Piloted a policy for migrant populations called “Equalization Program of Basic Public Health and Family Planning Services for Migrants” (EPHSM) (15). Under this project, 40 prefectural cities were designated as pilot cities. And in these areas, a range of free policies and services to address the health needs of local internal migrants have developed. For example, establish health records, carry out health education programs and implement infectious diseases prevention measures for the migrant population. However, the health effect of this package of reform actions on the migrant population remains unclear, and there is a lack of relevant empirical studies in China. The aim of this study is to analyze the effect of EPHSM on the health of migrant populations by constructing a quasi-natural experiment on the reform of equalization of public health services for China's migrants.
This study has the following innovative contributions to the existing research gap. First, this study constructed a quasi-natural experiment to identify the effect of EPHSM on Chinese migrants' health status using the latest micro-data from China. Second, this study provides new evidence in China that public health policies can protect and improve the health status of the internal migrants. Third, the findings of this study will enable a better understanding of the public health services policy launched by the Chinese government and will ultimately be a valuable guide to interventions to improve the health among the migrant communities as well.
2. Materials and methods
2.1. Study design and data sources
China Migrants Dynamic Monitoring Survey (CMDS) is a national periodical survey carried out by the China Population Development Research Center. This nationally representative survey was first established in 2010, and then has been performed every year to investigate the migrant population in terms of the socio-economic status, health outcomes and determinations of medical services use. In this study, we used the data from the CMDS in 2018. The 2018 CMDS implemented a stratified a sampling strategy with three-stage probability proportionate sampling (PPS). 10,300 communities from 348 cities in China were included in this survey. And at the community level, 20 independent individuals were randomly selected from each community to form the final survey sample. Aged over 15 years migrants who moved across counties and lived locally for more than 1 month were interviewed. The CMDS is considered to be a good representative sample, as well as having a small sampling error (16). In total, 1,52,000 migrants were interviewed. After removing the samples with missing and extreme values of core variables, the final sample size included in this study was 1,51,639.
2.2. Variable measurement
2.2.1. Dependent variables: The health status of the migrant population
Based on the 2018 CMDS questionnaire, this study used self-reported health to measure the overall health status of Chinese migrants. The self-rated health was indicated by choices to the question, “How do you think your health is? The options are very good, good, fair or poor?” We assigned a value of “1,” “2,” “3,” and “4” when respondents chose “very poor (unable to take care of myself),” “poor (unhealthy but able to take care of myself),” “average (basically healthy),” and “good (good healthy),” respectively. Self-reported health is considered to be a common indicator that effectively represents an individual's overall health status. Numerous studies have suggested that Self-reported health could predict the death risk and effectively represent the health level of adults (17–19).
2.2.2. Independent variables: Equalization of public health services
The variable of equalization of public health services was constructed using the pilot of EPHSM carried out by the National Health Commission. The specific definition is: if the city is in the pilot list, the value is 1; If the city is not in the pilot list, the value is 0 (20).
2.2.3. Controlled variables
The following variables were controlled in this analysis to minimize the possible estimation bias caused by missing variables. First, individual characteristic indicators of the migrants, including gender, age, marital status, registration local, ethnic status, political identity, family size, and flow range; Second, socio-economic status indicators, including the level of education, monthly household income, medical insurance and the types of work. Finally, to control for the effects of different urban characteristics (e.g., size, population and economic development), we also controlled city fixed effects. The specific information and descriptive analysis of the variables are shown in following (Table 1).
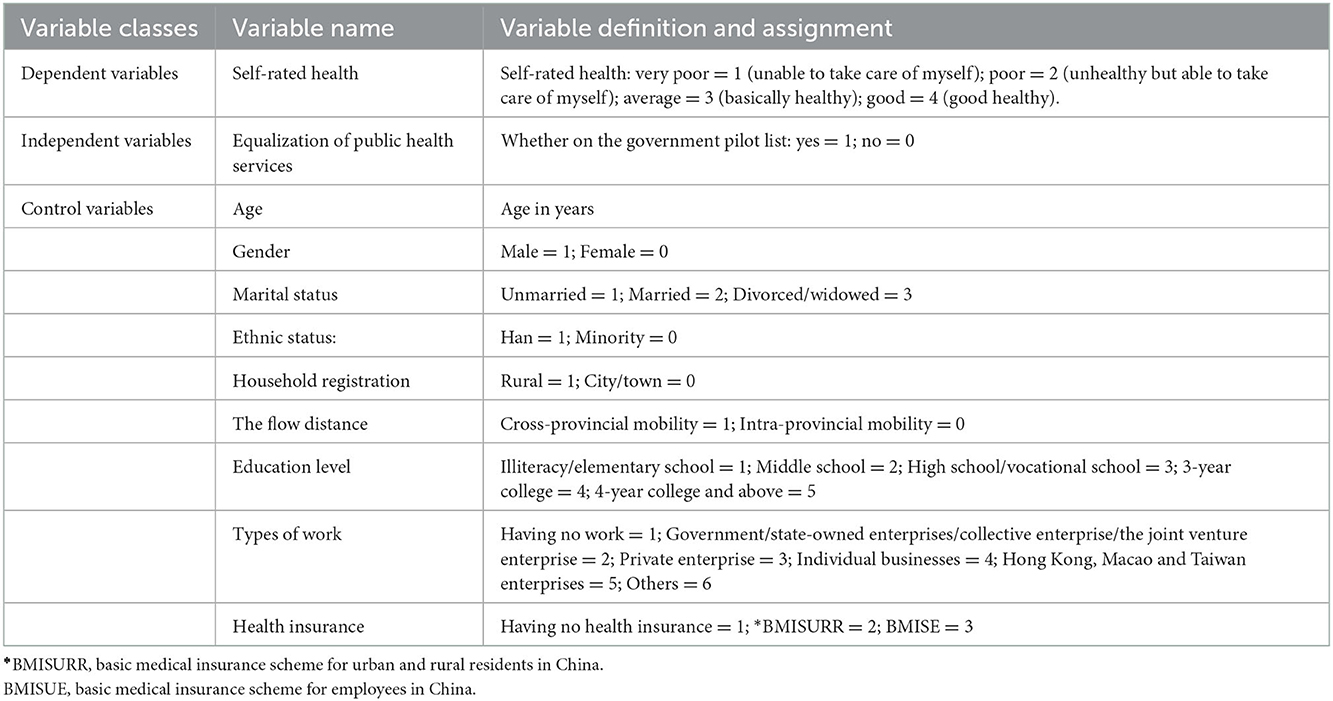
Table 1. Variable selection, definition, and assignment.
2.3. Statistical methods
Stata version17.0 was used to calculate the health effect of equalization of public health services on the Chinese migrants. We adopted the OLS model, ordered probit model and ordered logit model to explore the connection between the equalization of public health services and china's migrants' health. The basic model is:
Healthi represents an individual's self-rated health status, Equalizationi indicates the policy of equalization of public health services. β1 indicates the coefficient for the effect of the reform on self-rated health, and βk is the correlation coefficient of the control variables. εi is the random disturbance term. Moreover, we used the Propensity Score Matching (PSM) technology to reduce the potential endogenous problems. The PSM model is able to reduce some of the confounding effects and a number of potential endogeneity problems in the model (21). In this study, we used kernel matching, K-nearest neighbor matching and caliper matching methods to joint test the health effect.
3. Results
3.1. Descriptive results
The results of descriptive analysis is presented in Table 2. After removing the samples with missing and extreme values of core variables, we included 1,51,639 migrants in the final analysis. Of these, 53,704 migrants (35.36%) live in the pilot cities for equalization of public health Services, 78,092 (1.41%) were male, 1,38,838 (91.41%) were Han, 1,22,702 (80.78%) were married, 7,967 (5.25%) had political status, and 1,04,422 (68.75%) were from the rural areas. The average age of the migrant population in China was 37.05 ± 11.20 years. The mean value of health of the migrant population was 3.85 ± 0.42 scores, indicating that the health of this study population is at a relatively high level.
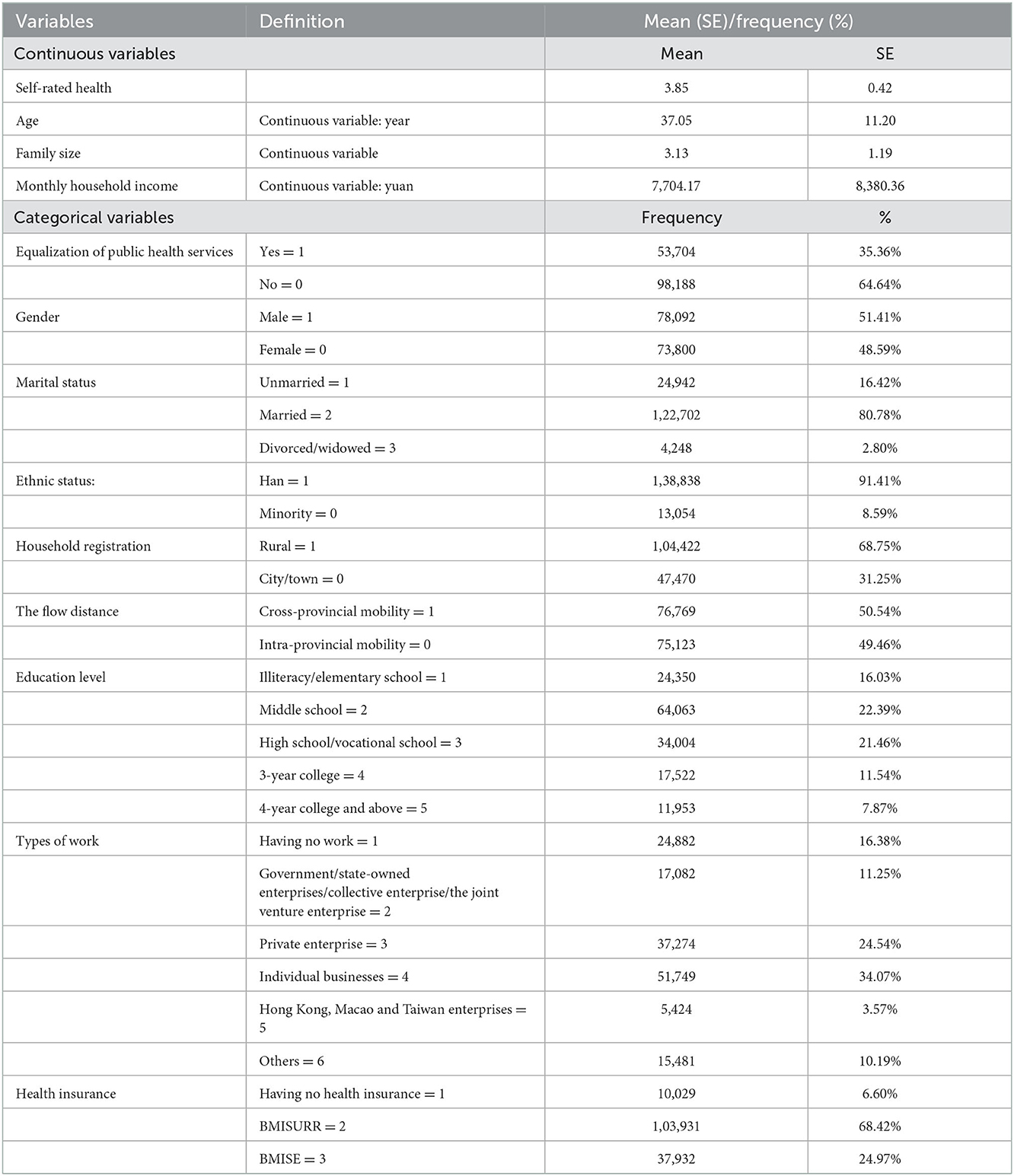
Table 2. The results of descriptive statistics.
For the flow range, 76,769 (50.54%) migrant population were inter-provincial migrants, and 75,123 (49.46%) migrated within the province. In terms of socio-economic conditions, the average monthly household income of migrants was 7,704.17 ± 8,380.36 yuan. 89,023 (58.61%) migrants work in private or individual enterprises. And most of the migrants in China have health insurance (93.40%). It is worth noting that a considerable part of the migrant population is unemployed (24,882, 16.38%).
3.2. The effect of equalization of public health services on health
We used Maximum Likelihood Method (MLE) and the OLS method to estimate the effect of equalization of public health services on health among the migrant population. Columns (1)–(2) of Table 2 reported the association between the equalization of public health services and health using the ordered probit model. Column (1) showed that equalization of public health services was positively associated with health when we did not include any control variables (β = 0.113, p < 0.001). Column (2) indicated that the regression coefficient decreased to 0.033 after controlling for other confounding variables (p < 0.001).
To examine the robustness of the results, columns (3)–(6) of Table 2 reported the relationship between the equalization of public health services and health by using the ordered logit model and OLS method. The results also suggested that equalization of public health services was positively associated with the migrant population's health (p < 0.001), which was consistent with the data results in columns (1)–(2).
Moreover, among controlled variables, increasing age and family size were negatively associated with health (p < 0.001). In contrast, male, individuals married with a spouse, higher education level and longer flow distance were positively associated with health for the migrant population (p < 0.001). In terms of socio-economic indicators, higher household income and participation in BMISURR had a significant effect on the migrant population's health (p < 0.001). Relative to the migrant population who had no job, those with formal or informal work positively affected migrants' health (p < 0.001).
3.3. Heterogeneous analysis
Columns (1)–(2) of Table 3 divided the range of mobility of the migrants into two types: “cross-provincial mobility” and “Intra-provincial mobility,” and reported the effect of equalization of public health services on the health of the migrants under different flow distances. The results suggested that the reform of equalization of public health services significantly improved of the intra-provincial migrants' health (β = 0.055, p < 0.001), but it did not affect the cross-provincial migrant population.
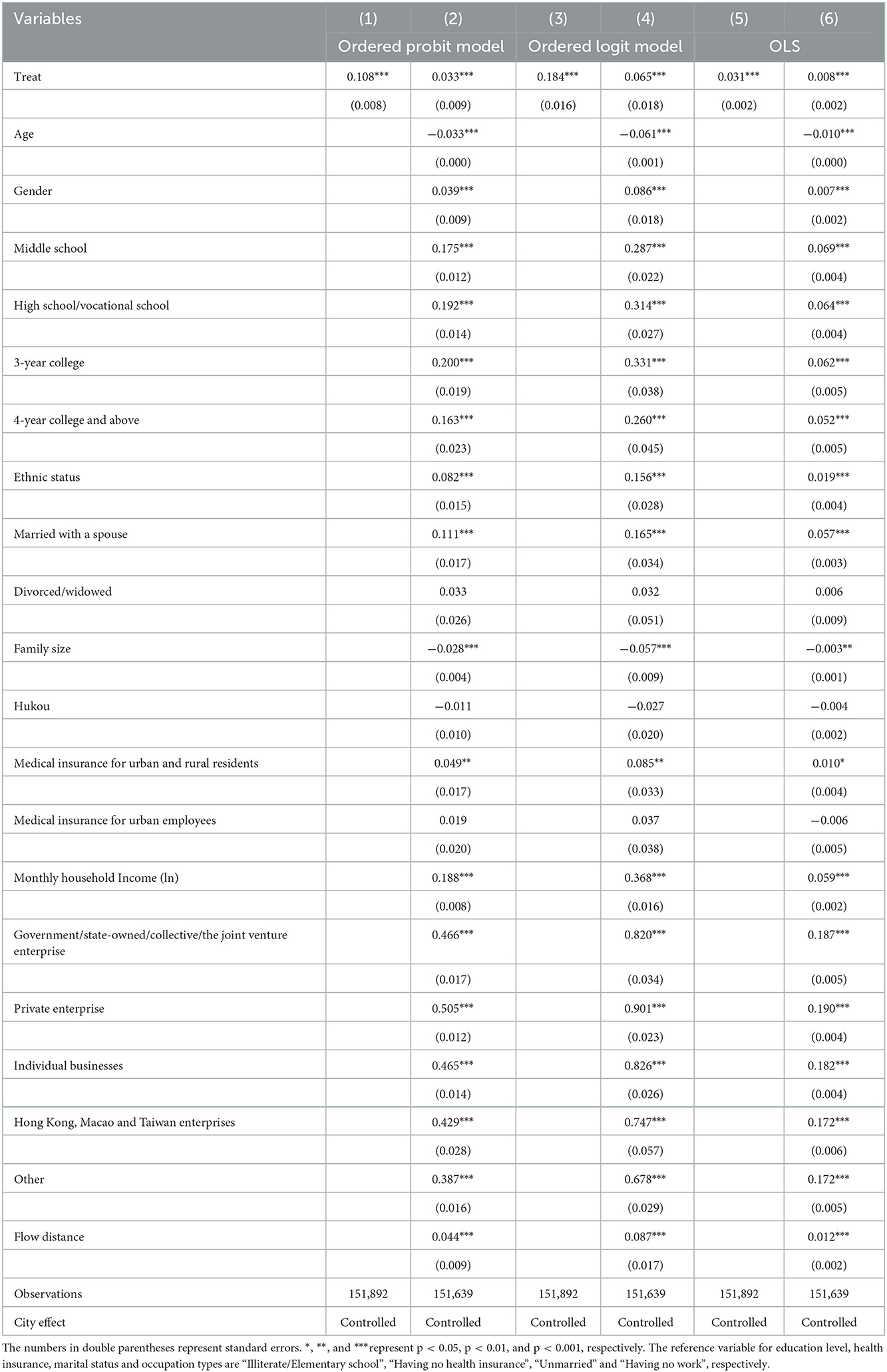
Table 3. The results for the effect of equalization of public health services on the health of the migrant population in China.
Columns (3)–(4) of Table 3 reported the age differences regarding the effect of the public health services equalization reform on health of China's migrants. The regression results have shown that the reform had a more significant impact on the older migrant population (β = 0.191, p < 0.001) than on the non-elderly (< 60 years) migrant population.
Columns (5)–(6) of Table 3 reported the regional differences in the effect of the equalization reform of public health services on the health of the migrant population. The results suggested that the reform of equalization of public health services significantly improved the health level of the rural migrant population (β = 0.038, p < 0.001), but it had no impact on the urban migrant population.
Columns (7)–(8) of Table 3 reported the gender differences regarding the health effect of the equalization reform of public health services on China's migrants. The results indicated that the equalization reform effectively improved the health level of the female migrant population (β = 0.055, p < 0.001), but it had no impact on the male migrant population.
Columns (9)–(13) of Table 4 reported the income differences regarding the health effect of the equalization reform of public health services on China's migrants. The results indicated that the equalization reform effectively improved the health level of the low-income migrant population (β = 0.077, p < 0.001), but it had no effect on other income-level migrant populations.
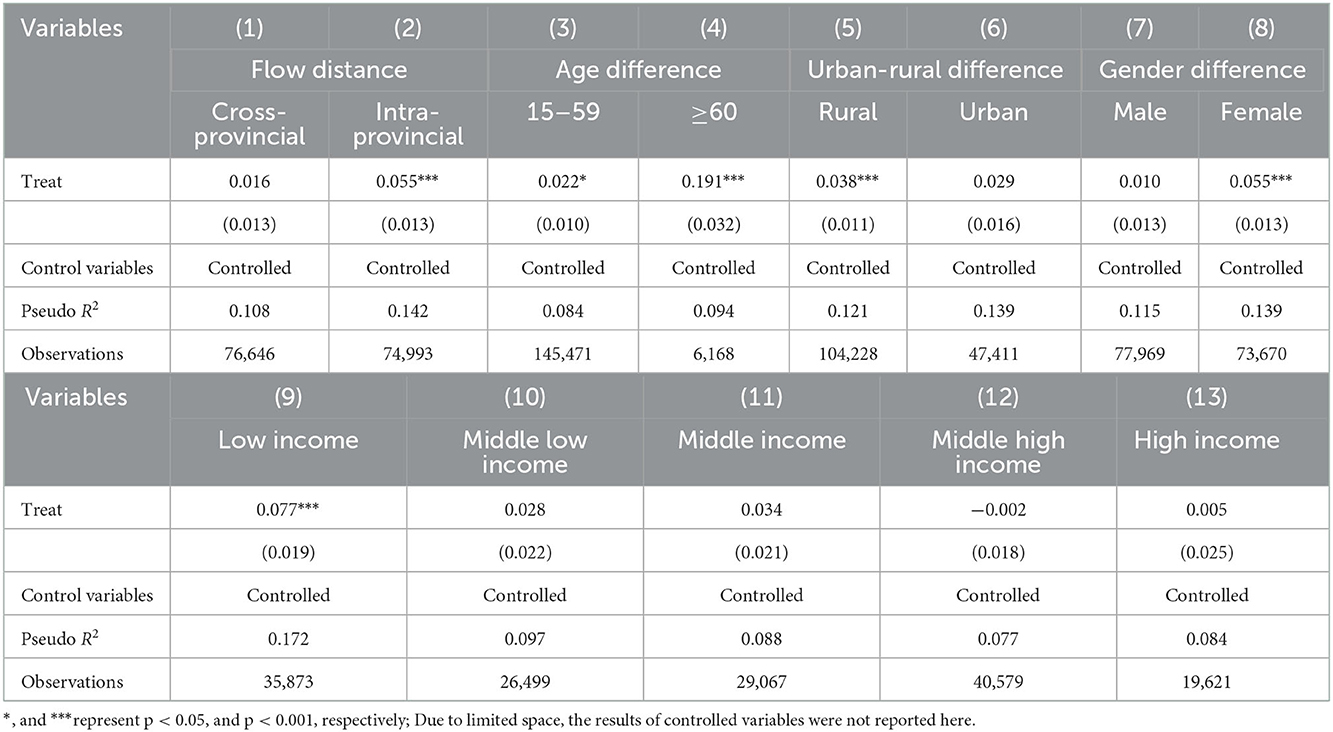
Table 4. The regression results of the heterogeneous analysis.
4. Robustness test
4.1. Robustness test with different PSM methods
We examine the robustness of PSM by employing different matching techniques to effectively reduce the potential endogenous problem between EPHSM policy and migrants' health. We used different PSM matching techniques to verify the robustness of the results. Table 4 showed that the coefficients of K-nearest neighbor matching, caliper matching, and kernel matching respectively. And the figures were 0.0063, 0.0067, and 0.0073, these results were consistent with Table 5, indicating that the EPHSM policy significantly promoted the health status of the migrant population after overcoming the potential endogenous problems.

Table 5. PSM results for the effect of equalization of public health services on the health of the migrant population.
4.2. Robustness test with replacement of dependent variables
To resolve measurement errors in variables, We carried out several robustness tests by substituting the dependent variables with year-round disease prevalence, the corresponding question in the questionnaire is “Have you been personally ill (injured) or unwell in the past year?” and year-round hospitalization, whose corresponding question is “Have you personally been hospitalized in the last year?” Table 6 shows the results of robustness tests for replacing the dependent variable, and the results are consistent with the coefficients in Table 5. This suggests that our conclusions are relatively robust.
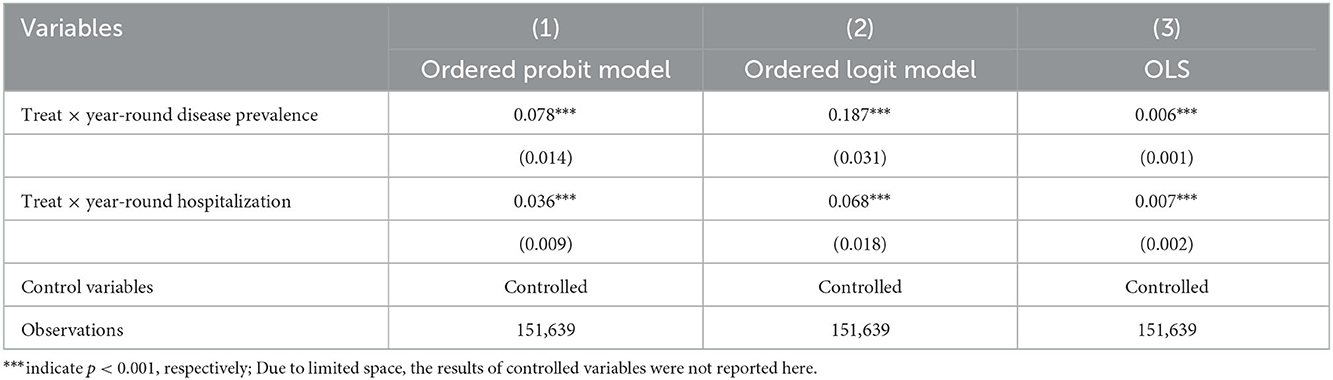
Table 6. Robustness test: replacement of dependent variables.
5. Discussion
Based on large samples, 1,51,639 individuals were selected to identify the health effect of the EPHSM on the Chinese migrant population. In this study, we concentrated not only on the effect of the equalization of public health services on migrants' health status, but also on the health effects of different segments of migrant populations. As a developing country with the largest floating population in the world, this empirical evidence from China will have important practical significance.
The results of this study demonstrated that the reform of equalization of public health services has a significant positive effect on the self-report health in the Chinese migrant population, and the results obtained by different PSM methods were consistent with it. Migrant population cannot be granted equal access to public health services as urban residents, thus affecting the health level of the migrant population (22), As increasing health accessibility for mobile populations is the core purpose of EPHSM policy, one possible mechanism is that the equalization of public health services has increased access to health services (23), but further validation is needed.
We also found that the health status of migrant populations was at a relatively high level, which may be attributable to the “healthy immigration” and the “salmon bias” hypotheses (24). And according to The Social Integration Assessment Report of China's Urban Migrant Population 2018, the level of equalization of public health services in pilot cities has improved significantly compared with non-pilot cities (20). This is also partly a testament to the effectiveness of this policy.
From the perspective of other influencing factors, the results shown that the health status of the migrant population who were male, highly educated and had a stable job was better. Moreover, China's Han migrant population has better health status than ethnic minorities. These findings were consistent with other studies in China (25–27). At the same time, the insurance type of urban and rural residents played a significant role in promoting the health status of the migrant population, but the urban workers' insurance had no considerable health promotion effects (15), one possible reason was that urban workers' insurance accounts for a relatively smaller proportion of the floating population (28).
Further heterogeneity analysis found that compared to the groups who were the provincial migrations, males, having higher-than-average income and living in urban areas, equal access to public health services had shown more pronounced health effects to the groups who were inter-provincial migrants, females, having low-income and living in rural areas. It suggested that the practice of equalization of public health services in China had a more substantial health effect on the relatively vulnerable groups and paid more attention to fairness among different groups (29), which made significant contribution to help narrow the gap between urban and rural health outcomes to a certain extent (30). Migrant people who were 60 years old and above had more significant health benefits than those aged 15–69 years. This may be due to the health depreciation effect of age, making the average health level of the elder group lower than that of the young group, thus showing different health effects of the public health services equalization policy (31). Besides, we should pay more attention to the health of the elderly migrant population, since the proportion of elderly migrants has increased steadily due to greater mobility that allows families to migrate together (32). At the same time, compared with the inter-provincial migrant population, the health effect of the migrant population in the province was more significant. One possible reason was that immigrants in the province often had more medical security and family support (33–35).
This study also has the following limitations: First, for the reason of data accessibility, this study was unable to obtain self-reported health data for the mobile population prior to 2013. Therefore, it was not possible to further rigorously examine the causal relationship. Second, for the evaluation of health status, we have only analyzed a single self-assessed health indicator, lacking comprehensive judgment of multidimensional health indicators. Third, this study fails to provide an in-depth analysis of the mechanisms associated with the equalization of public health services affecting the health of migrant populations. In the future, more researches refer to causal design and multidimensional health measurement as well as mechanisms research need to be further explored.
6. Conclusions and implications
Overall, the equalization of public health services reform in China has significantly improved the overall health status of the internal migrant population, especially the vulnerable groups. In the future, the government should fully absorb the experience of the pilot project of equalization of public health services for the migrants and further promote the equalization of basic public services in other fields. Most importantly, the government need to narrow the gap between the migrant population and the urban registered residence population in terms of the public services and social welfare.
We make the following policy implications based on the findings above, First, the Chinese government should strengthen health education and improve the health literacy of the migrant population. It is necessary to carry out targeted health education for the migrant population groups with different characteristics from the aspects of a healthy lifestyle and health skills. Moreover, in addition to health education, we should start with universal education and use school education and social education to comprehensively improve the health literacy of the migrant population. Second, the government departments should further increase the financial investment to improve the coverage of public health services and the equity in resource allocation among regions. Third, the government should strengthen the information-based management of the migrant population and the prevention and control of infectious diseases. As a susceptible population to infectious diseases (36), especially since the outbreak of COVID-19, the massive flow of people has posed a great challenge to China's epidemic prevention and control system. We need to further strengthen the monitoring of infectious diseases among the migrant population, deal with the epidemic situation of infectious diseases promptly, and effectively implement policies such as free treatment of COVID-19, AIDS, tuberculosis, and other infectious diseases among the migrant population. The challenges posed by internal migrants in China require immediate as well as long-term efforts from the whole society and the relevant authorities and stakeholders to cope with (37).
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://www.chinaldrk.org.cn/wjw/.
Author contributions
XZ and BS contributed to the conception or design of the work. BS, YW, CC, and ZY contributed to the work's acquisition, analysis, or interpretation of data. BS drafted the manuscript. XZ critically revised the manuscript. All gave final approval and agreed to be accountable for all aspects of work, ensuring integrity, and accuracy.
Funding
This paper was supported by the Major Project of the National Social Science Fund of China (Grant No. 21ZDA107).
Acknowledgments
All authors are grateful to the Migrant Population Service Center, National Health Commission P.R. China, who provided the data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang Q. Health of the elderly migration population in China: benefit from individual and local socioeconomic status? Int J Environ Res Public Health. (2017) 14(4):37 Wang Q. Health of the elderly migration population in China: benefit from individual and local socioeconomic status? Int J Environ Res Public Health. (2017) 14:370. doi: 10.3390/ijerph14040370
2. Greenwood MJ. Chapter 12 internal migration in developed countries. In: Handbook of Population and Family Economics. Vol 1. Amsterdam: Elsevier (1997). p. 647–720.
3. Lucas REB. Chapter 13 internal migration in developing countries. In: Handbook of Population and Family Economics. Vol 1. Amsteradm: Elsevier (1997). p. 721–798.
4. Molloy R, Smith CL, Wozniak A. Internal migration in the United States. J Econ Perspect. (2011) 25:173–96. doi: 10.1257/jep.25.3.173
5. Lagakos D. Urban–rural gaps in the developing world: does internal migration offer opportunities? J Econ Perspect. (2020) 34:174–92. doi: 10.1257/jep.34.3.174
6. ILO. Pandemic Realities for Asia-Pacific's 48 Million International Migrants. Geneva: ILO (2021). Available online at: https://www.ilo.org/asia/media-centre/news/WCMS_793027/lang–en/index.htm (accessed August 19, 2021).
7. Wu X, Treiman DJ. The household registration system and social stratification in China: 1955–1996. Demography. (2004) 41:363–84. doi: 10.1353/dem.2004.0010
8. Hu X, Cook S, Salazar MA. Internal migration and health in China. Lancet. (2008) 372:1717–9. doi: 10.1016/S0140-6736(08)61360-4
9. Nielsen I, Nyland C, Smyth R, Zhang M, Zhu CJ. Which rural migrants receive social insurance in Chinese cities? Evidence from Jiangsu survey data. Global Soc Policy. (2005) 5:353–81. doi: 10.1177/1468018105057416
10. Fang C, Dewen W. Migration as marketization: what can we learn from China's 2000 census data? China Rev. (2003) 3:73–93. Available online at: http://www.jstor.org/stable/23461905
11. Liu S, Griffiths SM. From economic development to public health improvement: China faces equity challenges. Public Health. (2011) 125:669–74. doi: 10.1016/j.puhe.2011.08.004
12. Guo M, Guo L. The situation and problems research on immediate settlement on ecdemic medical care at different locations for floating population. Chin Health Econ. (2014) 33:26–8. doi: 10.7664/CHE20140107
13. Zhu Y, Österle A. Rural–urban disparities in unmet long-term care needs in China: the role of the Hukou status. Soc Sci Med. (2017) 191:30–7. doi: 10.1016/j.socscimed.2017.08.025
14. Dauvrin M, Lorant V, Sandhu S, Devillé W, Dia H, Dias S, et al. The Esg. Health care for irregular migrants: pragmatism across Europe. A qualitative study. BMC Res Notes. (2012) 5:99. doi: 10.1186/1756-0500-5-99
15. China HCo,. The Notice of the General Office of the National Health Family Planning Commission on Printing Distributing the Pilot Program of Equalization of Basic Public Services for Floating Population's Health Family Planning. China Health Family Planning Commission (2013). Available online at: http://www.nhc.gov.cn/ldrks/s3577/201312/39f344bd0a4f419ca66ef8b933eaa561.shtml (accessed October 31, 2022).
16. Rongbin L, Cheng Y. The empirical study of migrant identity under the perspective of social change——based the migrant dynamic monitoring survey data in China. Popul Dev. (2013) 19:26–35. Available online at: http://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDHIS2&filename=SCRK201306004&uniplatform=NZKPT&v=XLNwCd6pawdK9W-roZse776q4Ze9UFJka1DmGkAjQWuwpcfZ4Eq0MagpQXst_TUi
17. Dowd JB, Zajacova A. Does self-rated health mean the same thing across socioeconomic groups? Evidence from biomarker data. Ann Epidemiol. (2010) 20:743–9. doi: 10.1016/j.annepidem.2010.06.007
18. Salomon JA, Tandon A, Murray CJL. Comparability of self-rated health: cross sectional multi-country survey using anchoring vignettes. BMJ. (2004) 328:258. doi: 10.1136/bmj.37963.691632.44
19. Jylhä M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med. (2009) 69:307–16. doi: 10.1016/j.socscimed.2009.05.013
20. Xiao Zihua XY, Jinwei L. The Social Integration Assessment Report of Urban Migrant Population in China. Beijing: Press SSA (2019).
21. Li M. Using the propensity score method to estimate causal effects: a review and practical guide. Org Res Methods. (2013) 16:188–226. doi: 10.1177/1094428112447816
22. Wu L. Current situation of the development of public health services for the migrant population and suggestions for optimisation. People's Forum. (2013) 32:159–61. doi: 10.16619/j.cnki.rmlt.2013.32.008
23. Yang X, Yang S. A study on health literacy of migrant population and its improvement mechanism: based on dynamic monitoring data in Jiangsu Province. Northwest Popul. (2019) 40:38–47. doi: 10.15884/j.cnki.issn.1007-0672.2019.06.004
24. Qi Y, Niu J, Mason W, Treman D. China's internal migration and health selection effect. Popul Res. (2012) 36:102–12.
25. Chen T, Li J, Yang Y. Social determinants of mental health changes of rural-urban migrants in Chengdu: based on Oaxaca blinder decomposition. J Sichuan Univ. (2022) 53:656–62. doi: 10.12182/20220760303
26. Guo W, Lu J, Liu L. Healthy China in an age of mobility: socioeconomic status, health literacy, and health outcomes. Popul J. (2022) 44:1–18. doi: 10.16405/j.cnki.1004-129X.2022.02.001
27. Wang C, Liao JL. A study on influencing factors and urban-rural differences of residents' financing choices. J South China Normal Univ. (2017) 14:274. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2018&filename=HNSB201706002&uniplatform=NZKPT&v=4kebGuasV4xgrL4CKfbaLTXSUi7Tw85QGiqLTAGFtgWoCOu6gHb92uyofJfW5Fsp
28. Yao Q, Chen A. Influencing paths of medical insurance enrollment location on the health conditions of elderly migrants in China: based on data from 2015 China migrants dynamic survey. Chin J Health Policy Res. (2022) 15:57–63. doi: 10.3969/j.issn.1674-2982.2022.01.008
29. Cai W. Feasibility research on the national essential health service package in China [Master]. Weifang Medical University (2009).
30. Yang L, Sun L, Wen L, Zhang H, Li C, Hanson K, et al. Financing strategies to improve essential public health equalization and its effects in China. Int J Equity Health. (2016) 15:194. doi: 10.1186/s12939-016-0482-x
31. Zhang F, Shi X, Zhou Y. The impact of health insurance on healthcare utilization by migrant workers in China. Int J Environ Res Public Health. (2020) 17:1852. doi: 10.3390/ijerph17061852
32. Yu W. Health disparities between urban and rural areas and its influencing factors among elderly floating population in China. J Northeast Agric Univ Soc Sci. (2022) 20:56–65. Available online at: https://knscnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2022&filename=DBNY202201007&uniplatform=NZKPT&v=K7kqRMB2sVg-TzhxbsuzXPJS5ZMFBwK8TvTJFZMubqv5bi3R8-5n-ORMIYvDtwWU.
33. Song Y, Zhang G. Utilization of public health services and its influencing factors among migrant people with hypertension or diabetes in China. Chin J Public Health. (2021) 37:198–202. doi: 10.11847/zgggws1123492
34. Liu W, Li J, Ren L, Xu J, Li C, Li S. New measures for medical insurance convenience: instant settlement of medical treatment in different places in the province. Sichuan Labor Sec. (2015) 02:56. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2015&filename=LDBZ201502056&uniplatform=NZKPT&v=xwRp6wUNWja0rERnoWfraiuSOZ91N8toP24GH50GUSkoD1NHiWVfComXFRfSDyUi
35. Zhu L. Working time and occupational health of rural migrant workers. Chin J Soc Sci. (2009) 01:133–207. Available online at: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFD2009&filename=ZSHK200901012&uniplatform=NZKPT&v=dFLLqocIUtJ_QOqiAdaWjIA2A5Vn5e2ySdXjZyX1Iibs0szAi59v58092ud28pji
36. Castelli F, Sulis G. Migration and infectious diseases. Clin Microbiol Infect. (2017) 23:283–9. doi: 10.1016/j.cmi.2017.03.012
37. Parliament E. Joint Motion for a Resolution on Migration and Refugees in Europe. Strasbourg: Parliament E (2015). Available online at: http://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP//TEXT+MOTION+P8-RC-2015-0832+0+DOC+XML+V0//EN&language=en (accessed August 20, 2015).
Keywords: migrant population, equalization of public health services, health impact, China, Migrants Dynamic Survey
Citation: Su B, Wu Y, Yihao Z, Chen C, Panliang Z and Zheng X (2023) The effect of equalization of public health services on the health China's migrant population: Evidence from 2018 China Migrants Dynamic Survey. Front. Public Health 10:1043072. doi: 10.3389/fpubh.2022.1043072
Received: 13 September 2022; Accepted: 16 December 2022;
Published: 10 January 2023.
Edited by:
Stefania Salmaso, Independent Researcher, Rome, ItalyReviewed by:
Tuerhongjiang Tuxun, First Affiliated Hospital of Xinjiang Medical University, ChinaFan Yang, Sichuan University, China
Mostafa Saidur Rahim Khan, Hiroshima University, Japan
Copyright © 2023 Su, Wu, Yihao, Chen, Panliang and Zheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoying Zheng,  emhlbmd4aWFveWluZ0BzcGgucHVtYy5lZHUuY24=
emhlbmd4aWFveWluZ0BzcGgucHVtYy5lZHUuY24=