 Ruping Liu1†Xiaotong Dong1†Xiaoning Ji1Shihan Chen1Qingqing Yuan1Yi Tao1
Ruping Liu1†Xiaotong Dong1†Xiaoning Ji1Shihan Chen1Qingqing Yuan1Yi Tao1 Yaping Zhu1
Yaping Zhu1 Sufang Wu1*
Sufang Wu1* Jingfen Zhu2*
Jingfen Zhu2* Yongbin Yang1*
Yongbin Yang1*- 1Department of Obstetrics and Gynecology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China
- 2School of Public Health, Shanghai Jiao Tong University, Shanghai, China
Background: Although global contraceptive coverage has increased significantly, high rates of unintended pregnancy remain the current global status quo. A comparative analysis of the differences and correlations of knowledge, attitude and practice (KAP) of sexual and reproductive health (SRH) of both partners will help guide public health work according to gender characteristics and needs, and reduce the occurrence of unintended pregnancy.
Methods: A questionnaire survey of people with unintended pregnancies including women and their male partners (n = 1,275 pairs) who sought help from the Shanghai General Hospital Affiliated to Shanghai Jiao Tong University School of Medicine from October 2017 to October 2021. Data were collected on sexual and reproductive health knowledge, attitudes, and practices in both partners who had unintended pregnancies. Chi-square test and Logistic regression were used to analyze the relationship between the occurrence of unintended pregnancy and KAP and its influencing factors. Paired odds ratio and McNemar's test were used to estimate the difference and concordance of KAP between partners.
Results: This study included 1,275 partners with a mean age of 30.0 years. The partner's overall level of KAP is good. Compared with women, men had better knowledge (χ2 = 3.93, p = 0.047) and more active contraceptive practices (χ2 = 19.44, p < 0.001). In the analysis of partner concordance, male contraceptive intention was found to be better than female [matched pairs odds ratio (ORMP) = 2.56, p < 0.001], and the concordance of positive contraceptive practice between partners increased with male education [adjusted odds ratio (aOR) = 1.556, 95% confidence interval (CI) = 1.185–2.044, p = 0.001]. In partner-paired regression analysis, compared with good contraceptive knowledge in both men and women in the partner, the risk of negative contraceptive practice was 1.7 times (aOR = 1.721, 95% CI = 1.234–2.400, p = 0.001) higher with good contraceptive knowledge in women but negative in men, while women with poor contraceptive knowledge but men with good knowledge are 1.3 times (aOR = 1.349, 95% CI = 1.000–1.819, p = 0.05) more likely to have negative contraceptive practices. In addition, compared with partners with positive contraceptive attitudes, women with positive attitudes but negative men and women with negative attitudes but positive men had 1.7 and 1.4 times the risk of negative contraceptive practices, respectively.
Conclusion: The study found that unintended pregnancy occurs mainly in young people, and the younger age of first sexual intercourse, the low education background and the lack of discussion of contraception between partners are risk factors for not taking contraceptive measures. Men's better knowledge and contraceptive practices compared with female partners, and poor male contraceptive knowledge and attitudes may lead to a higher risk of negative contraceptive practices, the results suggest that male KAP plays an important role in promoting contraceptive use and reducing unintended pregnancy.
Introduction
Unintended pregnancy, including unwanted and mistimed pregnancies, is one of the major public health challenges and a major reproductive health problem (1). It has now affected the health, economic and social life of women and their families, and can lead to adverse social consequences, such as school dropout, violence and suicide, placing enormous physical, psychological and economic burdens on individuals, families and societies. In recent years, despite the almost universal use of condoms and other contraceptive methods, the incidence of unintended pregnancies has been increasing year by year (2). Worldwide, ~120 million unintended pregnancies occur each year, accounting for 40% of all pregnancies (3–6).
Studies have shown that most of these unintended pregnancy groups choose induced abortion to terminate the pregnancy, which has become a global phenomenon (7). The ever-increasing number of induced abortions not only has adverse consequences for women's physical and mental health (8), but in severe cases can lead to an increased risk of infertility, maternal mortality and neonatal mortality (9–13). According to statistics, worldwide, about 5 million women are hospitalized due to complications of unsafe abortion every year, and 47,000 women die from unsafe abortion (14), especially in less developed countries. In addition, the latest reports say that the US Supreme Court has overturned the 1973 Roe v Wade decision, ending women's 50 years old constitutional right to abortion and imposed comprehensive restrictions on abortion (15, 16), which may increase the incidence of unsafe abortion in the future. In fact, a multinational study found that countries with liberal abortion laws were more likely to offer safe abortion than countries that restricted abortion (14), and a hypothetical nationwide abortion ban would have catastrophic effects on maternal health (17). At the same time, in the United States, people have been relying on safe and legal abortion to cope with unintended pregnancies (18). However, the aftermath of this abortion ban suggests that women living in states that prohibit abortion may face unsafe abortions or may travel to another state or country to evade laws restricting abortion. It is clear that restricting abortion does not reduce its incidence, but rather reduces its safety (19), putting people's health, safety and property at great risk. Therefore, scientific contraception and reducing the occurrence of unintended pregnancy are particularly important.
The most common causes of unintended pregnancy are contraceptive failure and never use of contraceptive methods (20). Among them, the lack of contraceptive knowledge and the unreasonable choice of contraceptive methods are closely related to the increased risk of unintended pregnancy (21). Although people have a preliminary understanding of the existing contraceptive methods, the in-depth understanding of these methods is limited, or the misunderstanding of contraceptive knowledge will lead to an increase in the proportion of ineffective contraception (22), which will lead to the occurrence of unintended pregnancy. In addition, never use of contraceptive methods is also one of the main reasons for unintended pregnancy, and it can be seen from the Demographic and Health Survey (DHS) that the proportion of never use of contraceptive methods is high in developing countries (23), which is mainly related to the partner's negative contraceptive attitude, and of course to the partner's limited awareness of contraceptive methods, less sex education, and limited choice of effective contraceptives (24, 25). In conclusion, the importance of partners' knowledge, attitude and practice (KAP) of sexual and reproductive health (SRH) in reducing unintended pregnancies is well-documented. Proper knowledge and a positive attitude can increase partners' awareness of contraceptive practices and maximize the rational use of contraceptive methods, thereby preventing unnecessary risks.
Previous articles highlighted some of the current research aspects. First, in China and many other developing countries, research on the causes of unintended pregnancy and reproductive health services and education has focused primarily on women, exploring and documenting women's KAP of SRH is associated with the occurrence of unintended pregnancy (21, 26–29). In recent years, there has been renewed focus on the role of men in preventing unintended pregnancies (30, 31), and male attitudes and practices have been found to play a key role in contraceptive practice (30–33). And the World Health Organization and the United Nations and other organizations (34) mentioned in the global policy initiative on reducing unintended pregnancy that in clinical practice, health promotion and sexual health education, men's participation in decisions related to the prevention and management of unintended pregnancy should be considered. The aim is to encourage men to participate in discussions about contraception and pregnancy decisions.
In fact, decisions about sex, contraceptive use, and termination of pregnancy are rarely made by a woman or a man alone (35, 36), and partners' attitudes and practices also influence each other. Therefore, women and men are equally responsible for causing unintended pregnancy. However, there are few research data combined with both partners to analyze the causes of unintended pregnancy and explore the relationship between KAP of SRH and unintended pregnancy. It is known that in many countries, especially in China, women rely mainly on contraception and reproductive health decision-making and education are often also targeted at women (21). Although the use of contraceptive methods has increased significantly, the incidence of unintended pregnancy has increased year by year (37). Based on such a status quo, it shows that the focus of the past is only on women and not the key to solving the problem, and the previous research results that only used men or women as research objects were relatively one-sided. Therefore, this study conducted an in-depth comparison and analysis of the status of unintended pregnancy by both partners, aiming to jointly analyze the relationship between KAP of SRH and unintended pregnancy from the perspectives of men and women, and put forward gender-specific recommendations to reduce the number of unintended pregnancies, and improve women's reproductive health.
In China, with the release of second and third births, many people feel that “family planning” is outdated. However, according to the World Health Organization (WHO), family planning means “having the ability” to have the desired number of children at the interval and timing of births desired by individuals and partners through the use of contraceptive methods. All in all, the focus of family planning research both now and in the past is to ensure women's access to safe and effective comprehensive contraceptive measures, to protect women's reproductive health and fertility, and to strengthen high-quality fertility. The current status quo suggests that a key direction for the future is estimating the impact of the Coronavirus disease 2019 (COVID-19) pandemic on family planning indicators. Reports and early modeling efforts from administrative agencies and health systems suggest that large-scale disruptions to family planning services occurred in 2020 (38–41), affecting many people's need for abortion and contraception, and the long-term persistence of such changes is likely to result in change long-term fertility desires (42). There are reports that 60% of people's fear of COVID-19 is mainly hindered by the need for abortion, and 42% report that women are much less likely to seek an abortion during the pandemic, seriously affecting people's life plans (43). In addition, a qualitative study of young women under the age of 30 in six countries reported that among women who do not have access to abortion services due to COVID-19, some women choose to use medical abortions at home (44), and others seek unsafe abortions in local informal abortion facilities, increasing the incidence of complications such as infertility, reproductive system infections, and severe gynecological diseases, which can lead to maternal death. As a result, the overall level of contraceptive use reported in population-based surveys has increased to some extent as the pandemic has progressed, along with an increase in the demand for contraceptive and abortion information and a greater desire for access to knowledge (45, 46).
In addition, according to the World Health Organization and related research reports, during the new crown pneumonia pandemic, the provision of sexual and reproductive health guidance services in relevant medical departments was significantly reduced and interrupted (of different length and scale) (41, 47–50), but the proportion of the population in demand for reproductive health services increased from 23% in April 2020 to 40% in September 2020 (48). Therefore, exploring the relationship between the partner's KAP and unintended pregnancy, popularizing sexual and reproductive health knowledge and enhancing contraceptive determination have guiding significance for reducing the incidence of unintended pregnancy in the future.
Materials and methods
Study design and sample
This study was a retrospective questionnaire-based study of women and their male partners who sought help in the Department of Obstetrics and Gynecology, Shanghai General Hospital Affiliated to Shanghai Jiao Tong University School of Medicine for an unintended pregnancy. First, the investigator explained the purpose of the research study to the respondents and obtained informed consent. The Nurses explained precautions to women and their male partners and ensured the confidentiality of their participation in this study. The survey was conducted using an online self-administered questionnaire, including closed-ended and open-ended questions, and took 5–8 min. All questionnaires were conducted from October 2017 to 2021. The studies involving human participants were reviewed and approved by ethics committee of Shanghai Jiao Tong University School of Medicine (SJUPN-201718).
A total of 3,104 females and 1,952 male partners aged 15–49 were collected in this study. The male and female partners were matched according to their names and basic information. Excluding males and females who failed to match successfully, there were 1,402 couples, of which 106 couples lost some information. As well as considering the universality of the research results, the age standard of the research subjects was controlled at 18–45 years old, a total of 21 couples were excluded, and the complete answers of 1,275 couples were finally included in the analysis. In the end, 1,275 couples' complete answers were included in the analysis, as shown in Figure 1. We define a partner as “two opposite-sex partners or couples.”
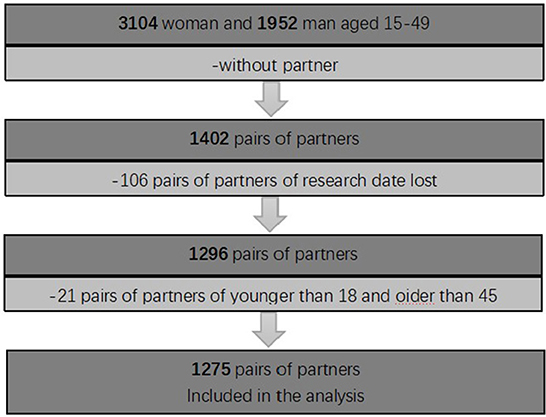
Figure 1. Description of the research sample.
Research surveys included participants' sociodemographic characteristics and sexual and reproductive health. A self-made questionnaire was designed after reviewing previous similar surveys. Subsequently, the readability and comprehension of the questionnaire were verified. The validity of the questionnaire was checked by five experts in obstetrics and gynecology, and the questionnaire was discussed and adjusted with experts in public health and statistics, and content verification was completed in the final data analysis. By calculating the Cronbach's alpha value, which is 0.721, this means that there is acceptable reliability and consistency between test items.
Categories
The final version of the questionnaire that collected the data consisted of four parts. The first part consists of six basic questionnaires, including age, gender, registration, education, profession, and income. The second part is about four items related to reproductive health, including the number of abortions, whether to discuss contraceptive matters, the age of first sexual intercourse, and the number of sexual partners. The third part includes seven questions related to contraception and abortion knowledge and aims to assess women's and men's sexual and reproductive health knowledge. The fourth part further evaluated the partner's contraceptive attitude and practice intention by answering three contraceptive attitude-related questions and three contraceptive practice questions.
Measures
To assess participants' knowledge of sexual and reproductive health, participants were asked a series of questions about reproductive health knowledge, attitudes and practices. Among them, there are five questions about contraceptive knowledge, including “fertile periods of the menstrual cycle,” “rhythm contraception is an effective method of contraception,” “occasional unprotected sex won't lead to pregnancy,” “best time for emergency contraception,” “emergency contraceptives can be used frequently instead of oral contraceptives,” there are two questions about abortion knowledge, including “the harm of painless abortion is less than that with pain” and “abortion is harmful to the body.” There are three questions about contraceptive attitude, including “actively take contraceptive measures in the future,” “pregnancy can be avoided by taking proper contraceptive measures,” “contraception is troublesome, but worth it.” There are three questions on contraceptive practice, including “use contraception during sex,” “I can stick to contraception when my partner refuses it,” “I can stick to contraception.”
All questions use optional variables, and according to whether the answers were correct or not, the overall correct rate of each question, the correct rate of women and men respectively, and the overall response of each pair of partners were counted. For example, a question is “rhythm contraception is an effective method of contraception” and if the answer is “false,” then the question is recorded as the correct answer and is coded as “1.” If the answer is “correct,” “unclear,” or “haven't heard of the safe period,” the answer is recorded as wrong and coded as “0.” The cumulative total scores for KAP of SRH were calculated separately for men, women, and partners. Finally, with the median as the boundary, respondents with a total score at or above the median were defined as “good,” and those with scores below the median were defined as “poor.”
In addition, in order to assess the prevalence of partner concordance in KAP of SRH, according to whether the answers to questions related to reproductive health knowledge, contraceptive attitudes, and contraceptive practices were correct or not, we cross-tabulated the number (and percentage) of concordant and discordant answers among partners in four categories: both men and women in a couple answered correctly (W+M+); both men and women answered incorrectly (W-M-); women answered correctly, but men were wrong (W+M-); women answered incorrectly, but men were right (W-M+). Partner concordance on KAP was defined as practice in which both partners answered correctly or incorrectly on a question. Frequency and matched-pair odds ratio analyses were used to estimate patterns of partner concordance for KAP of SRH. The McNemar's test was used to determine the differences in KAP of SRH between male and female partners. “Paired” data were used in the estimation of the odds ratios and McNemar's test.
Furthermore, in order to calculate the concordance values for partner KAP of SRH, we coded the pattern “W+M+” as 1 and 0 otherwise. Univariate and multivariate logistic regression analyses were then used to calculate the matched pairs odds ratio (ORMP), and to test the statistical significance of the association between partner concordance in reproductive health knowledge, contraceptive attitudes and partner consistency in contraceptive practice. In addition, stratified analysis using multivariate logistic regression, according to the ages, registration and education of the couples, were used to confirm that the associations between partner concordance in reproductive health knowledge, contraceptive attitudes and partner concordance in contraceptive practice were consistent among different strata.
Finally, we recorded the total score of the answers to all questions about contraception and abortion knowledge, contraceptive attitude, and contraceptive practice, respectively, greater than the median as good, less than the median as poor, divided into four categories: that is, both women and men in couples were good (W+M+); both men and women were worse (W-M-); women were good, but men were worse (W+M-); women were worse, but men were good (W-M+). Univariate and multivariate logistic regression analyses were then used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) and to test the statistical significance of the association between partners in KAP of SRH.
Analyses
After the data were exported as SPSS files from the Internet, the data were checked and sorted, and statistical analysis was carried out using IBM SPSS25.0 statistical software. Categorical variables were described using relative indicators such as rate and percentage. Statistical inference was performed using χ2 analyses, describing the demographic characteristics of 1,275 partners, using a multivariate logistic regression model to examine the association between participants' basic characteristics and KAP variables, reporting unadjusted and adjusted odds ratios (ORs and aORs) and 95% confidence intervals. Frequency and ORMP analyses were used to assess partner concordance in KAP of SRH problems. Finally, after adjusting the variables of age, registration and education level of the partner, multivariate logistic regression was used for analysis. All statistical analysis tests were two-sided hypothesis tests, and the p-value < 0.05 was considered to be statistically significant.
Results
Socio-demographic characteristics
Table 1 shows the sociodemographic characteristics of the participants. A total of 1,275 pairs of partners (2,550 participants) were included and analyzed in this study. Among them, the average age of women is 28 years old, and the average age of men is 31 years old. Unintended pregnancy was most common among women (34.3%) between the ages of 18 and 25. The overall age of unintended pregnancy in men was higher than that in women, especially the number of unintended pregnancies in men over 35 years old (27.2%) was higher than that in women (16.4%). In addition, the study found that more than 41% of the participants were registered in rural areas, and most of the partners had a college education background or above, and they all had their own jobs and good incomes. Among them, it can be seen from the survey results that men's work income is significantly higher than that of women, with a significant difference (p < 0.001).
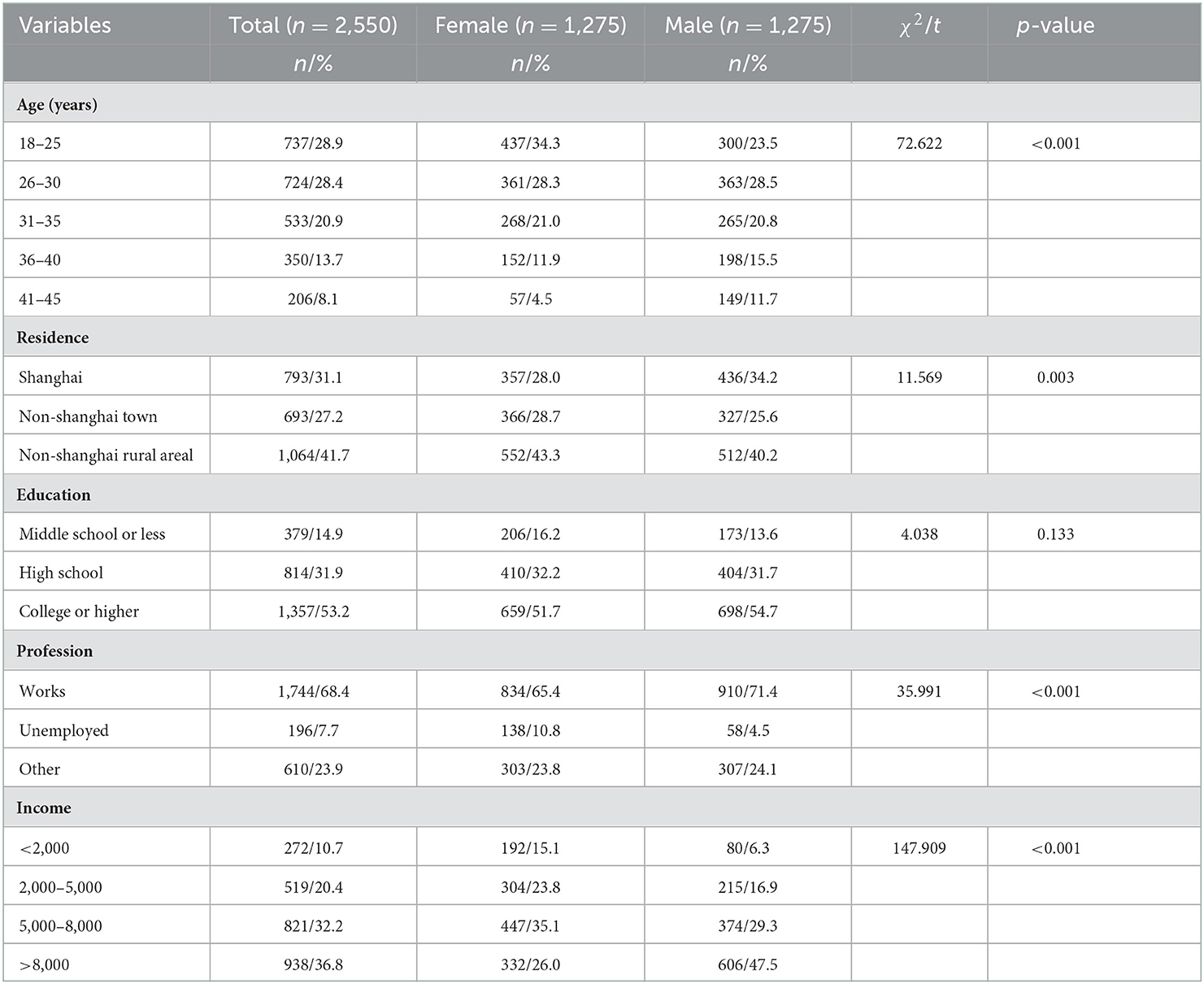
Table 1. Sociodemographic characteristics of the participants (n = 1,275 pairs).
Partner's response to KAP of SRH
Table 2 investigates issues related to contraception and abortion knowledge, contraceptive attitudes, and contraceptive practices. Overall, it can be seen that the overall practice of KAP by partners with unintended pregnancies is good. Among them, in terms of reproductive health knowledge, most partners believe that occasional unprotected sex won't lead to pregnancy (57.3% for women and 70.4% for men), and that Rhythm contraception is an effective method of contraception (67.4% for women and 54.5% for men), this wrong perception may be related to the weak knowledge of contraception and the psychology of luck. In addition, the correct rate of contraceptive knowledge about “fertile periods of the menstrual cycle” and “emergency contraceptive oral time” is significantly lower, indicating that people have a certain understanding of existing contraceptive methods, but their in-depth understanding of these methods is limited. As for the knowledge of abortion, although more than half of the partners believe that an abortion is harmful to the body (65.9% of women and 67.6% of men), a considerable number of people (80.6% of women and 78.3% of men) believed that painless abortion was less harmful to the body than painful abortions. This misperception of abortion methods may lead to partners not paying enough attention to the use of contraceptive methods, which may increase the probability of unintended pregnancies. Overall, compared with women's knowledge level, men had better understandings of sexual and reproductive health knowledge (χ2 = 3.93, p = 0.047).
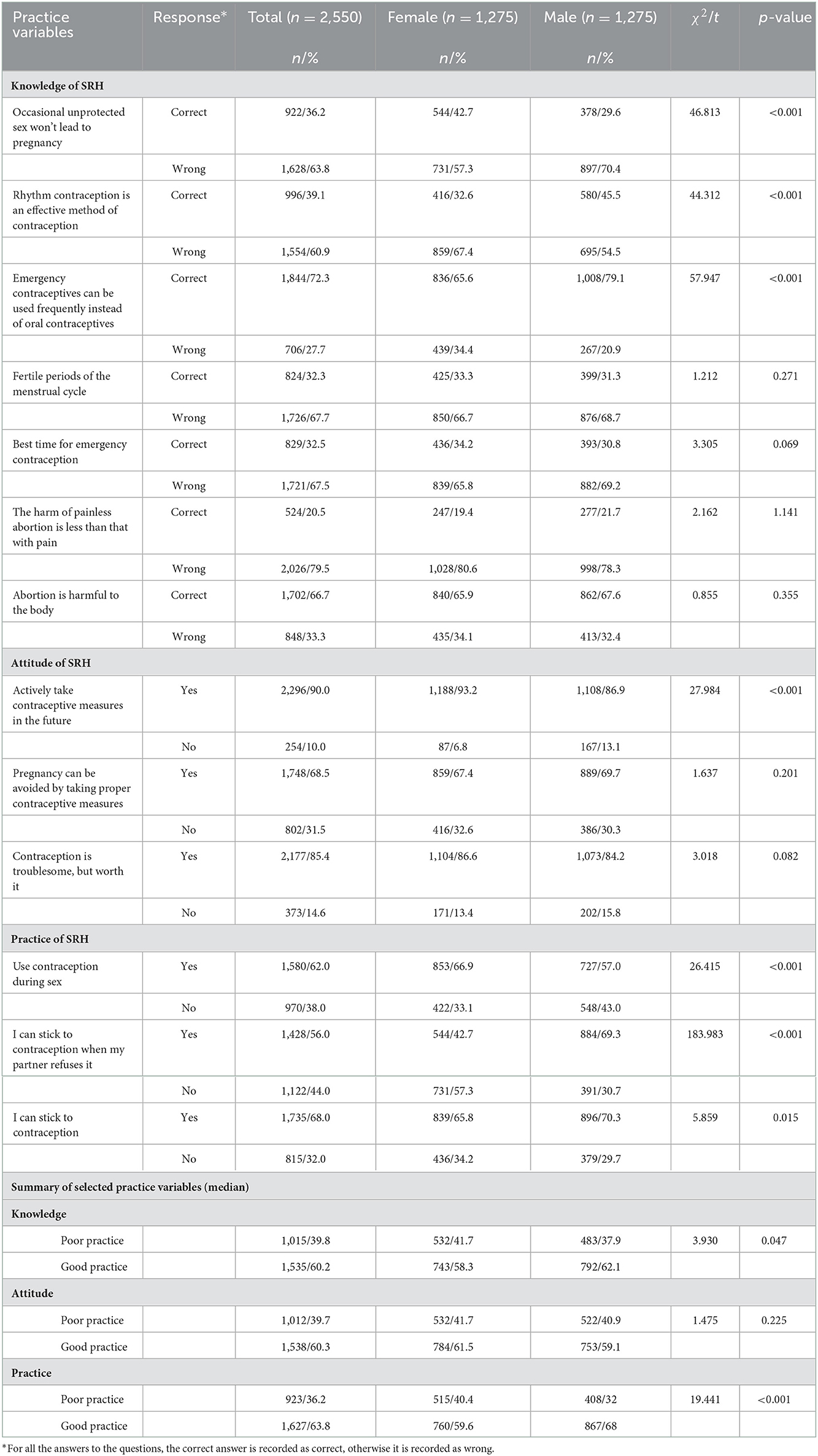
Table 2. Partner responses to questions about KAP of SRH (n = 1,275 pairs).
In terms of contraceptive attitudes, both males and females had positive contraceptive attitudes. Compared with males, females were more determined to contraceptives (χ2 = 27.984, p < 0.001). Compared with female contraceptive behavior intentions, males are more active, and this difference is statistically significant (χ2 = 19.44, p < 0.001).
Associations between sociodemographic and reproductive health characteristics and KAP of SRH among partners
This study used logistic regression analysis to determine the association between sociodemographic and reproductive health characteristics and KAP of SRH, as shown in Table 3. From the results of the study, it can be seen that the educational level of the partner and whether or not to discuss contraceptive matters are closely related to KAP of SRH. Among them, compared with the participants with higher education level, the risk of reporting poor contraceptive knowledge is higher among those with high school or less, which was twice as high as those with college education and above (female, aOR = 2.389, p < 0.001 and male, aOR = 2.461, p < 0.001). Compared with men and women who did not discuss contraception and had only one sexual partner, men and women who discussed contraceptive matters frequently and had multiple sexual partners had good knowledge of contraception. In addition, the study found that women's knowledge level was also related to the number of abortions. Compared with women who had experienced more than one abortion, women who had never had an abortion were 1.3 times more likely to report poor contraceptive knowledge (aOR = 1.301, p < 0.030). Finally, an analysis of male participants found that older age (aOR = 0.723, p = 0.013) and younger age at first sexual intercourse (aOR = 1.283, p = 0.048) were also risk factors for poorer contraceptive knowledge.
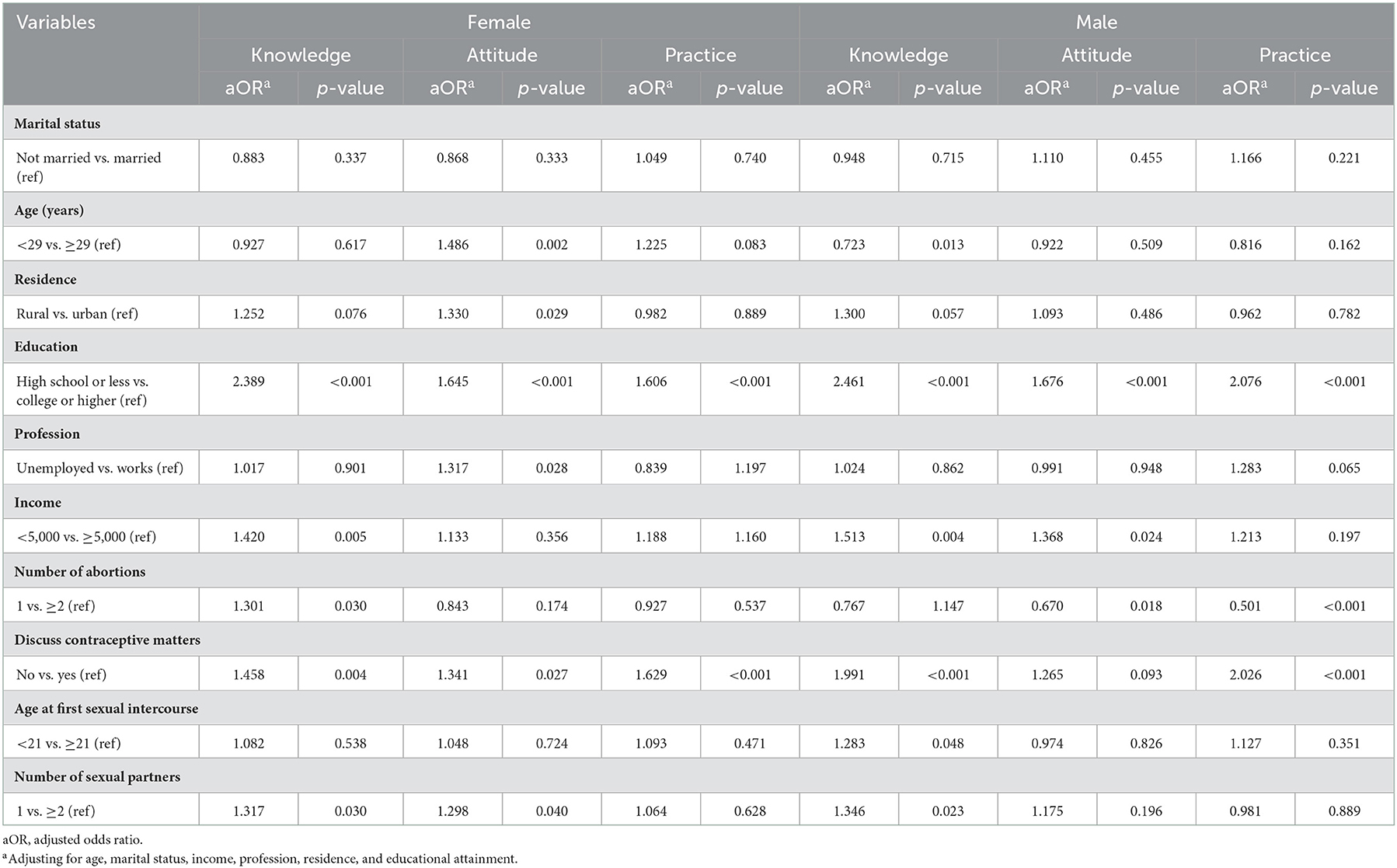
Table 3. Logistic regression for the associations between sociodemographic characteristics, reproductive health characteristics and KAP among Partners.
In the analysis of contraceptive attitudes, the study found that young women with rural registration and less education were at higher risk of reporting poor contraceptive attitudes, while women who often discussed contraceptive matters with their partners and had multiple sexual partners had more positive contraceptive attitudes. In addition, the study also found that contraceptive attitudes and practices were more negative among men who caused women to have more than one abortion.
Partner concordance for KAP of SRH
Table 4 describes the patterns of sexual and reproductive health knowledge, contraceptive attitudes, and practices among partners, comparing differences between male and female partners. Among them, the correct rate for the question of “whether emergency contraceptives can be used frequently instead of oral contraceptives” is highly consistent (55.1%). Male partners were more likely than female partners to believe that emergency contraceptives should not be used frequently instead of oral contraceptives (ORMP = 2.277, p < 0.001). At the same time, there are also many partners (45.5%) who agree that an abortion has a great impact on the body, and the error rates of the questions about “female fertile period” and “best time for emergency contraception” are relatively high (47.5 and 48.6%). In addition, some partners (39.5%) mistakenly believe that rhythm contraception is an effective contraceptive method, and more than half (64.4%) of the partners agree that painless abortion is less harmful to women. Finally, through a comprehensive analysis of the answers to sexual and reproductive health knowledge, it again shows that the male partner's knowledge of contraception is better than that of the female partner (ORMP = 2.26, p = 0.031).
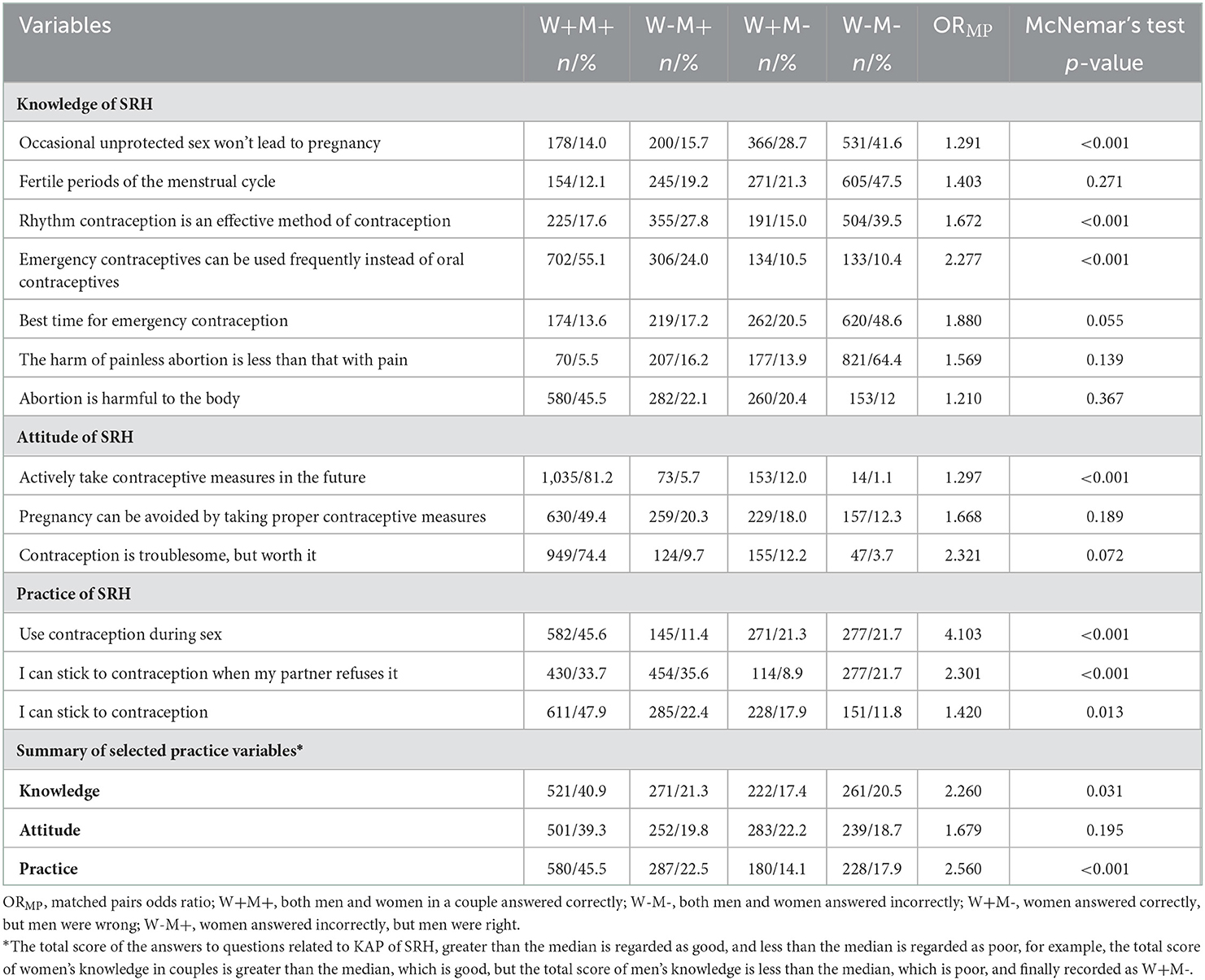
Table 4. Partner concordance for KAP of SRH, and comparisons among different patterns (n = 1,275 pairs).
Regarding contraceptive attitudes, there was a high concordance (81.2%) between partners on “actively take contraceptive measures in the future,” and female partners had more positive contraceptive attitudes than male partners, with a statistically significant difference (ORMP = 1.297, p < 0.001). Nearly half (45.5%) of the partners agreed on the use of contraceptive methods in future sex and were able to stick to contraception together. Among them, male partners had better contraceptive intention than female partners (ORMP = 2.56, p < 0.001). On the whole, both partners have positive attitudes toward contraception, and the concordance is good, but the error rate concordance of some relatively professional common sense related to contraception is much higher than the accuracy rate concordance, which shows that partners' in-depth knowledge of sexual and reproductive health knowledge is weak, leading to an increased risk of contraceptive failure.
After adjusting for male and female age, registration, and education level, it can be seen from Table 5 that the concordance of active contraceptive practice between partners may increase with the education level of male partners (aOR = 1.556, 95% CI = 1.185–2.044, p = 0.001). It shows that the higher the male education level in the partner, the greater the partner's determination to use contraception together. Among them, from the analysis results of contraceptive attitudes, it can be seen that compared with partners with negative contraceptive attitudes, the probability of positive contraceptive practices increases by 2.9 times for couples who are more determined to contraception in the future (aOR = 2.953, 95% CI = 2.103–4.148, p < 0.001).
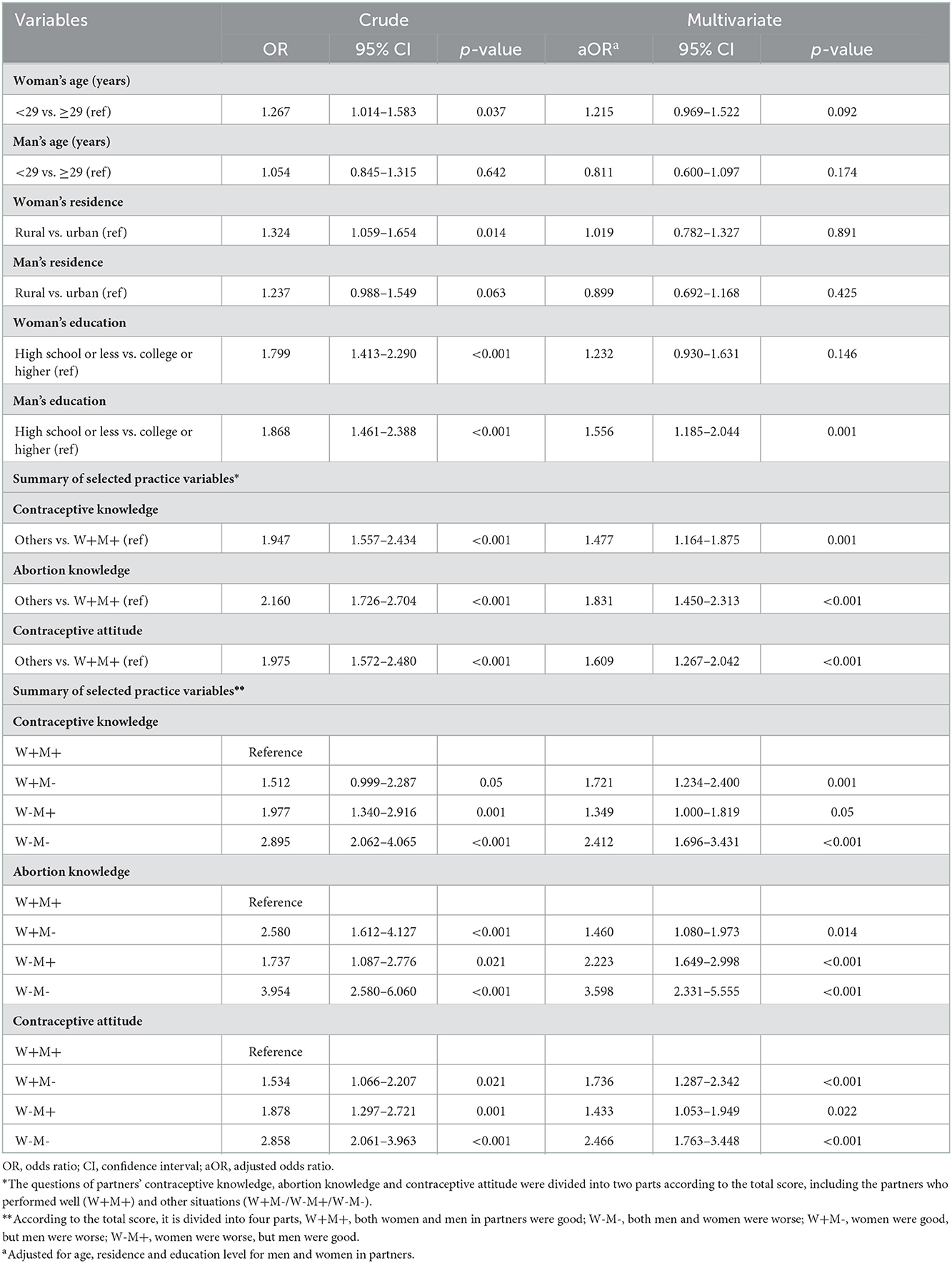
Table 5. Logistic regression of associations between knowledge, attitudes of SRH, and contraceptive practice among partners.
In addition, in the analysis of contraceptive and abortion knowledge and contraceptive attitude and contraceptive practice, it can be seen from Table 5 that the good concordance of contraceptive knowledge among partners increases the probability of positive contraceptive practice partner concordance by 1.477 times (aOR = 1.477, 95% CI = 1.164–1.875, p = 0.001). The concordance of correct abortion knowledge and positive contraceptive attitude among partners increased the odds of positive contraceptive practice concordance by 1.831 and 1.609 times (aOR = 1.831, 95% CI = 1.450–2.313, p < 0.001; aOR = 1.609, 95% CI =1.267–2.042, p < 0.001). It shows that good contraceptive and abortion knowledge and positive contraceptive attitude of both partners will promote the use of contraceptive methods, while poor contraceptive and abortion knowledge and negative contraceptive attitude are the risk factors for not taking contraceptive methods in sexual life between partners.
Analyzing the relationship with contraceptive practice in partner models with different knowledge and attitudes about sexual and reproductive health, it can be seen that compared with partners with good contraception and abortion knowledge and positive contraceptive attitudes, poor contraceptive knowledge (aOR = 2.412, 95% CI = 1.696–3.431, p < 0.001), poor abortion knowledge (aOR = 3.598, 95% CI = 2.331–5.555, p < 0.001), and negative contraceptive attitudes (aOR = 2.466, 95% CI = 1.763–3.448, p < 0.001) in both partners were risk factors for reporting partners' negative contraceptive practice.
In a more detailed comparative analysis of partners, it can be seen that in terms of contraceptive knowledge, compared with good contraceptive knowledge in both men and women in the partner (W+M+), the risk of negative contraceptive practice was 1.7 times (aOR = 1.721, 95% CI = 1.234–2.400, p = 0.001) higher in the partner with good contraceptive knowledge in women but negative in men (W+M-), while women with poor contraceptive knowledge but men with good knowledge (W-M+) are 1.3 times (aOR = 1.349, 95% CI =1.000–1.819, p = 0.05) more likely to have negative contraceptive practices. It also further indicated that, compared with female partners, poor contraceptive knowledge of male partners may lead to a higher risk of negative contraceptive practice, and thus a greater risk of unintended pregnancy. That is, men with good contraceptive knowledge can promote the use of contraceptive methods. In addition, compared with couples with positive contraceptive attitudes (W+M+), the risk of negative contraceptive practice for women with positive attitudes but negative for men (W+M-) and for women with negative attitudes but positive for men (W-M+) were 1.7 and 1.4 times. That is to say, partners with only men with good knowledge and attitudes had a 0.3–0.4 times lower risk of negative contraceptive practice compared with only women who performed well. Therefore, men's positive contraceptive attitudes have a greater impact on the use of contraceptive methods. The difference is that in terms of abortion knowledge, compared with men who have good abortion knowledge, women's good abortion knowledge has a greater positive impact on contraceptive practice.
Discussion
This study analyzed the relationship between KAP of SRH and the occurrence of unintended pregnancy from the unique perspectives of both partners. Through investigation and analysis, we found that the vast majority of partners believed that good contraceptive knowledge (aOR = 1.477), good abortion knowledge (aOR = 1.831) and positive contraceptive attitude (aOR = 1.609) were the positive promoting factors of partners' contraceptive practice. Among them, compared with women's knowledge level (58.3%), men have better knowledge level (62.1%). This is inconsistent with previous research on American women (26), which showed that men have lower levels of knowledge about contraception than women. Compared with female contraceptive behavior intention, male performance was more positive. One possible explanation is that the vast majority of studies in China have found that men perceive actual or potential unintended pregnancy as a life event that will bring them moral and material dilemmas (34). Or with the development of society, men's sense of responsibility increases, and women's reproductive health may be considered, so they have strong contraceptive intentions, and the understanding of contraceptive knowledge will be more serious and active than women. In terms of contraceptive attitudes, both men and women are more positive in their determination to use contraception in the future, but compared with men, women are more determined to use contraception in the future. This may be because the occurrence of unintended pregnancy is closely related to women's reproductive health, so women's attitude toward contraception is more positive.
Most previous similar studies have investigated the association of KAP with male or female sociodemographic and reproductive health backgrounds on a country-by-country basis (22, 34, 51–54). In this study, we conducted a more detailed analysis of whether men and women in each partner had good knowledge and attitudes, and explored the impact and association of knowledge and attitudes on contraceptive practice between men and women in partners. The results of the study found that among partners, compared with women, men with poor contraceptive knowledge and negative contraceptive attitudes had a higher risk of negative contraceptive practice, and thus a greater risk of unintended pregnancy. That is to say, men with good contraceptive knowledge and positive contraceptive attitude can promote the use of contraceptive methods, indicating that men play an important role in promoting contraceptive practice and reducing the occurrence of unintended pregnancy, and this is similar to the findings (22, 34, 51, 54). Therefore, it is particularly important to reduce the occurrence of unintended pregnancies by changing the previous gender norms of “contraception depends on women.” However, according to the latest research report, male contraceptive initiative is generally not high in the world (55), so future research directions should highlight the theoretical focus of intervention behaviors to promote male contraceptive use, and call for reducing the occurrence of unintended pregnancy by helping men move from anticipation or consideration to action when adopting contraceptive practice.
In addition, the study also found that partners' education and income levels were strongly associated with KAP among participants' demographic characteristics. People with higher education and income have better knowledge of contraception and abortion, and have more positive contraceptive attitudes and practices. A survey shows that 74 million (86%) of the 86 million unintended pregnancies worldwide occur in economically underdeveloped countries (56). Compared with high-income countries, low-income countries have less personalized counseling on the choice of contraceptive measures, and more limited sources of effective and easily accessible reproductive health knowledge and modern contraceptive methods (3). For example, people with economic difficulties often choose the method of rhythm contraception, so they are more likely to have unintended pregnancy.
It is not difficult to understand that the level of education can determine a person's differences in cognition of the same things, which not only affects whether to use contraceptives, but also affects the choice of contraceptive methods and the decision-making of unintended pregnancy. Low education level limits the ability of individuals to receive contraceptive knowledge and abortion hazards, while the higher the education level, the higher the relative income level, and the more likely they are to independently acquire contraceptive-related knowledge through multiple channels. This is similar to the results of previous studies (57, 58), reporting that educational background is one of the most important factors for low contraception and abortion knowledge.
At the same time, after adjusting the variables of age, registration and education level, it was found that the concordance of active contraceptive practice between partners may increase with the education level of men (aOR = 1.556), that is to say, the higher the education level of the male partner, the greater the partner's determination to use contraception together. This can be explained by the fact that people from low educational backgrounds are more likely to see pregnancy as a positive life event, an opportunity to transform into a mature and responsible parent, and thus have relatively negative contraceptive attitudes and practices. For those with higher education, they believe that unintended pregnancy is an obstacle to becoming a mature and responsible person, which will affect their career planning (34), so contraceptive attitudes and practices are more positive. In response to this finding, we need to popularize sexual and reproductive health knowledge among targeted populations. For example, compared with people with high education level, it is particularly important to implement education on sexual and reproductive health knowledge for people with low education background and low income, and stablish relevant policy systems to enable young people to contact and understand relevant knowledge early.
According to the results of the investigation on the causes of unintended pregnancy (result not shown), 53.5% of the population did not use contraceptive methods, 30.8% of the population became pregnant due to contraceptive failure, and 15.7% had unknown reasons, indicating that the main cause of unintended pregnancy was not using contraceptive measures. This is similar to the results of previous studies. Globally, about 21% of married or cohabiting partner use contraceptive methods (57), indicating that the vast majority of partners do not use contraceptive methods during sex. In developing countries, ~50–60% of the population does not use contraception (23). In sub-Saharan Africa, South, Central, and Southeast Asia, up to 87% of unintended pregnancies occur in women who do not use contraception (59), which may be related to people's lower educational background, limited awareness of contraceptive methods, less sex education, and limited choice of effective contraceptives (20, 24).
The survey results show that although the overall knowledge level of the investigators in this study is relatively good, the correct rate of individual basic common-sense questions is low, such as the fertile periods of the menstrual cycle and the best time for oral contraceptives. At the same time, the concordance analysis found that the error rate concordance of some relatively detailed knowledge of contraception is much higher than the accuracy rate concordance and more than half (64.4%) of the partners in the KAP of SRH concordance analysis on the knowledge of abortion agreed that the painless abortion is less harmful to the body than the painless one. This misconception about contraceptive methods can affect the use of a partner's method of contraception. In recent years, although painless abortion has been accepted by increasing number of women because of its advantages such as less pain during an operation and faster recovery after an operation, it might even take abortion as a routine remedy for contraceptive failure. However, studies have shown that the rate of repeated abortion after painless abortion was higher than that after traditional artificial abortion (11), which increased the risk of anesthesia accidents (60) and also the incidence of complications such as uterine cavity adhesion, genital tract infection, and secondary infertility (8). The short-term and long-term complications affected women's physical and mental health.
In addition, due to people's inherent ideas or just listening to the descriptions of their friends around them, they will also have some wrong perceptions, which will increase the incidence of unintended pregnancy. For example, older women over 40 years of age believe that their reproductive function has deteriorated and they cannot conceive, thus reducing the use of contraceptives, which is likely to lead to unintended pregnancy. Many mothers during lactation believe that they will not be pregnant without menstruation, and they do not need to take contraceptive measures. But in fact, during lactation, even if they do not have menstruation, they may ovulate, and ovulation means there is a risk of unintended pregnancy. It also shows that people lack in-depth understanding of relevant knowledge and lack relatively professional guidance on accurate information and knowledge related to contraception, which has been mentioned in multiple studies (58, 61). Therefore, professionals should be encouraged to attach importance to popularizing knowledge, such as increasing online or offline popularization, promoting convenient and free contraceptive services provided by health care providers, and increasing the popularization of contraceptive methods among pharmacy workers to those in need of contraception.
The use of contraceptive methods has increased substantially worldwide since 1970 (55), but the incidence of unintended pregnancies has increased year by year. This also shows that most partners who have unintended pregnancy are willing to contraception, but do not use contraceptives or take incorrect contraceptive methods due to lack of contraceptive knowledge, and thus have a higher risk of unintended pregnancy. At the same time, the study found that unintended pregnancy was most common in the youngest age group (18–25 years old; 34.3% of women and 23.5% of men), and more than half of the respondents had their first sexual intercourse under the age of 21. In recent years, both the age of gestation and the age of first sexual intercourse tend to be younger (62–64), showing a downward trend (65–69), which is similar to the results of several studies (58, 70–73). Moreover, the study also found that men with smaller AFSI had a lower understanding of reproductive health knowledge (p < 0.05), and a younger AFSI is associated with a higher risk of unplanned pregnancy, which is consistent with other studies conducted in China (73). This makes sense given that younger women have lower knowledge of contraceptive methods and have higher frequency of intercourse and fertility. This result may be related to school education patterns and parental educational philosophies regarding sexual and reproductive health in China. Sexual issues are highly individual and secretive, family sex education should be the enlightenment education at the stage of sex education. However, influenced by traditional moral values, parents often avoid talking about sexual behavior with their children, let alone educate them about sex. On the other hand, the school curriculum in China rarely involves sex education or takes it seriously. Therefore, the educational concept of Chinese parents should be improved, and early sexual health education should be carried out for students in school to encourage them to take a more serious attitude.
Limitations
Our analysis has some limitations. First, in China, because sex-related issues are still a very sensitive topic, and participants must recall the past, there may be reporting bias in responses to KAP-related questions, especially among unmarried adolescents. Second, in qualitative studies, there is no uniform definition of contraception or partner communication, and findings are limited in terms of generalizability and risk of bias. The population of this study is limited to paired partners, excluding most of the people who have not been successfully paired, as well as too young and too old partners, and the reported results are relatively limited. Finally, the respondents in this study were matched couples, including unmarried and married couples, and no differential analysis was conducted. There are differences in needs and perceptions of issues between these two groups.
Conclusion
Although the global contraceptive coverage rate has increased significantly in recent years, and the contraceptive penetration rate in China is as high as 80%, the high incidence of unintended pregnancy is still the current global status quo. This study illustrates the lack of sexual and reproductive health education for partners in China through partner profiles. The key role of men in promoting contraceptive use is proposed, while providing evidence for the importance of male KAP in reducing unintended pregnancies between partners, filling the gap in the literature on joint research of both men and women with unintended pregnancy in developing countries and even around the world. Studies have shown that compared with women, men have more reproductive health knowledge, more positive contraceptive practice, and men's knowledge and attitudes are more positive factors in promoting contraception between partners. It shows that in the reproductive health education, the comprehensive education of partners should be given priority, and gender characteristics and needs should also be taken into consideration, not only taking into account the relative weakness of women's knowledge, but also paying attention to the role and role of male KAP in avoiding unintended pregnancy. It promotes male initiative and implements it into the contraceptive action between partners, so that men can be guaranteed in terms of contraceptive responsibility and attitude. In addition, it is also critical to identify targeted strategies when popularizing sexual and reproductive health knowledge. This study found that the younger age of the partner, low educational background, and lack of in-depth knowledge of relevant knowledge are risk factors for unintended pregnancy. Therefore, targeted education should be carried out for low-educated and young people. While emphasizing early sex education in schools and families, the government and health departments should also expand popular methods and promote the concept of “scientific contraception to reduce unintended pregnancy.”
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by Shanghai Jiao Tong University School of Medicine. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JZ, YY, RL, and XD contributed to conception and design of the study. YY organized the database. RL and XD performed the statistical analysis. RL wrote the first draft of the manuscript. XD wrote sections of the manuscript. XJ, SC, QY, and YT participated in data collection. JZ, YY, YZ, and SW have oversight and leadership responsibility for the planning and execution of research activities. YY and XJ provided financial support. All authors contributed to manuscript revision, read, and approved the submitted version.
Acknowledgments
The authors thank the experts from Shanghai General Hospital Affiliated to Shanghai Jiao Tong University School of Medicine in Obstetrics and Gynecology and Shanghai Jiao Tong University in Public Health and Statistics for their discussion and adjustment of the questionnaire design. Thank all the medical staff in the Gynecology and Obstetrics Clinic of Shanghai General Hospital Affiliated to Shanghai Jiao Tong University School of Medicine who participated in the questionnaire collection, including the nurses' patient guidance to the participants in filling in the questionnaire and the answers of the outpatient doctors to the questions about sexual and reproductive health. Five reviewers provided helpful and constructive comments that improved the manuscript substantially. We also would like to express our sincere gratitude to the support of the Shanghai Municipal Public Health Bureau (Grant No. 201540355) and the Shanghai Jiao Tong University (Grant No. YG2019QNA63).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zeleke LB, Alemu AA, Kassahun EA, Aynalem BY, Hassen HY, Kassa GM. Individual and community level factors associated with unintended pregnancy among pregnant women in Ethiopia. Sci Rep. (2021) 11:1–9. doi: 10.1038/s41598-021-92157-4
2. Hellstrom A, Gemzell Danielsson K, Kopp Kallner H. Trends in use and attitudes towards contraception in Sweden: results of a nationwide survey. Eur J Contracept Reprod Health Care. (2019) 24:154–60. doi: 10.1080/13625187.2019.1581163
3. Bottcher B, Abu-El-Noor MA, Abu-El-Noor NI. Causes and consequences of unintended pregnancies in the Gaza Strip: a qualitative study. Br Med J Sex Reprod Health. (2019) 2018:200275. doi: 10.1136/bmjsrh-2018-200275
4. Mohammed F, Musa A, Amano A. Prevalence and determinants of unintended pregnancy among pregnant woman attending ANC at Gelemso General Hospital, Oromiya Region, East Ethiopia: a facility based cross-sectional study. BMC Womens Health. (2016) 16:56. doi: 10.1186/s12905-016-0335-1
5. Bearak J, Popinchalk A, Alkema L, Sedgh G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model. Lancet Glob Health. (2018) 6:e380–9. doi: 10.1016/S2214-109X(18)30029-9
6. Singh S, Sedgh G, Hussain R. Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plann. (2010) 41:241–50. doi: 10.1111/j.1728-4465.2010.00250.x
7. Fathalla MF. Safe abortion: the public health rationale. Best Pract Res Clin Obstet Gynaecol. (2020) 63:2–12. doi: 10.1016/j.bpobgyn.2019.03.010
8. Shakya S, Shrestha S, Shrestha RK, Giri U, Shrestha S. Knowledge, attitude and practice of emergency contraceptive pills among community pharmacy practitioners working in Kathmandu Valley: a cross-sectional study. BMC Health Serv Res. (2020) 20:699. doi: 10.1186/s12913-020-05543-5
9. Kantorová V. Unintended pregnancy and abortion: what does it tell us about reproductive health and autonomy? Lancet Glob Health. (2020) 8:e1106–7. doi: 10.1016/S2214-109X(20)30342-9
10. Gipson JD, Koenig MA, Hindin MJ. The effects of unintended pregnancy on infant, child, and parental health: a review of the literature. Stud Fam Plann. (2008) 39:18–38. doi: 10.1111/j.1728-4465.2008.00148.x
11. Maravilla JC, Betts KS, Couto ECC, Alati R. Factors influencing repeated teenage pregnancy: a review and meta-analysis. Am J Obstet Gynecol. (2017) 217:52–45.e31. doi: 10.1016/j.ajog.2017.04.021
12. Monea E, Thomas A. Unintended pregnancy and taxpayer spending. Perspect Sex Reprod Health. (2011) 43:88–93. doi: 10.1363/4308811
13. Espinoza C, Samandari G, Andersen K. Abortion knowledge, attitudes and experiences among adolescent girls: a review of the literature. Sex Reprod Health Matters. (2020) 28:1744225. doi: 10.1080/26410397.2020.1744225
14. Ganatra B, Gerdts C, Rossier C, Johnson BR, Tuncalp O, Assifi A, et al. Global, regional, and subregional classification of abortions by safety, 2010-14: estimates from a Bayesian hierarchical model. Lancet. (2017) 390:2372–81. doi: 10.1016/S0140-6736(17)31794-4
15. Cohen IG, Murray M, Gostin LO. The end of roe v wade and new legal frontiers on the constitutional right to abortion. JAMA. (2022) 328:325–6. doi: 10.1001/jama.2022.12397
16. Tanne JH. US Supreme Court ends constitutional right to abortion. Br Med J Publish Group. (2022) 377:o1575. doi: 10.1136/bmj.o1575
17. Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. (2021) 58:2019–28. doi: 10.1215/00703370-9585908
18. Lazzarini Z. The end of Roe v. Wade—states' power over health and well-being. N Engl J Med. (2022) 387:390–3. doi: 10.1056/NEJMp2206055
19. Guillaume A, Rossier C, Reeve P. Abortion around the world. An overview of legislation, measures, trends, and consequences. Population. (2018) 73:217–306. doi: 10.3917/popu.1802.0225
20. Habib MA, Raynes-Greenow C, Nausheen S, Soofi SB, Sajid M, Bhutta ZA, et al. Prevalence and determinants of unintended pregnancies amongst women attending antenatal clinics in Pakistan. BMC Pregn Childb. (2017) 17:1–10. doi: 10.1186/s12884-017-1339-z
21. Ding R, Guo C, Song X, Zheng X. Male knowledge, attitude and practice and partner pregnancy among Chinese unmarried youth. PLoS ONE. (2019) 14:e0214452. doi: 10.1371/journal.pone.0214452
22. Kagesten A, Bajos N, Bohet A, Moreau C. Male experiences of unintended pregnancy: characteristics and prevalence. Hum Reprod. (2015) 30:186–96. doi: 10.1093/humrep/deu259
23. Jain AK, Obare F, RamaRao S, Askew I. Reducing unmet need by supporting women with met need. Int Perspect Sex Reprod Health. (2013) 39:133–41. doi: 10.1363/3913313
24. Nguyen BT, Violette C, Li HZ, Jensen JT. Expectations for sex without birth control among young men: risk factors from the USA National Survey of Reproductive and Contraceptive Knowledge. World J Men's Health. (2019) 2019:190098. doi: 10.5534/wjmh.190098
25. Dixit P, Ram F, Dwivedi LK. Determinants of unwanted pregnancies in India using matched case-control designs. BMC Pregnancy Childbirth. (2012) 12:1–12. doi: 10.1186/1471-2393-12-84
26. Quak XES, Sultana R, Aau WK, Goh CC, Tan NC. A 3-year retrospective study of unintended pregnancy in a developed multi-ethnic Asian community: A call for better healthcare system for family planning. Front Public Health. (2022) 10:996696. doi: 10.3389/fpubh.2022.996696
27. Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. (2016) 374:843–52. doi: 10.1056/NEJMsa1506575
28. Razzaq S, Jessani S, Rizvi N, Saleem S. Unintended pregnancy and the associated factors among pregnant females: Sukh Survey-Karachi, Pakistan. J Pak Med Assoc. (2021) 71(11Suppl.7):S50.
29. Yenealem F, Niberet G. Prevalence and associated factors of unintended pregnancy among pregnant woman in Gondar town, North west Ethiopia, 2014. BMC Res Notes. (2019) 12:1–5. doi: 10.1186/s13104-019-4203-6
30. Bell DL, Garbers S, Catallozzi M, Hum RS, Nechitilo M, McKeague IW, et al. Computer-assisted motivational interviewing intervention to facilitate teen pregnancy prevention and fitness behavior changes: a randomized trial for young men. J Adolesc Health. (2018) 62:S72–80. doi: 10.1016/j.jadohealth.2017.06.015
31. Wheeler NJ, Pilgrim N, Jennings JM, Sanders R, Page KR, Loosier PS, et al. Missed opportunities to address pregnancy prevention with young men in primary care. Clin Pediatr. (2018) 57:1558–66. doi: 10.1177/0009922818793351
32. Saewyc EM. What about the boys? The importance of including boys and young men in sexual and reproductive health research. J Adolesc Health. (2012) 51:1–2. doi: 10.1016/j.jadohealth.2012.05.002
33. Mishra A, Nanda P, Speizer IS, Calhoun LM, Zimmerman A, Bhardwaj R. Men's attitudes on gender equality and their contraceptive use in Uttar Pradesh India. Reprod Health. (2014) 11:41. doi: 10.1186/1742-4755-11-41
34. Kane J, Lohan M, Kelly C. Adolescent men's attitudes and decision making in relation to pregnancy and pregnancy outcomes: an integrative review of the literature from 2010 to 2017. J Adolesc. (2019) 72:23–31. doi: 10.1016/j.adolescence.2018.12.008
35. Hayford SR, Guzzo KB. Racial and ethnic variation in unmarried young adults' motivation to avoid pregnancy. Perspect Sex Reprod Health. (2013) 45:41–51. doi: 10.1363/4504113
36. Sassler S, Miller A, Favinger SM. Planned parenthood? Fertility intentions and experiences among cohabiting couples. J Fam Iss. (2009) 30:206–32. doi: 10.1177/0192513X08324114
37. Singh S. Hospital admissions resulting from unsafe abortion: estimates from 13 developing countries. Lancet. (2006) 368:1887–92. doi: 10.1016/S0140-6736(06)69778-X
38. Dasgupta A, Kantorová V, Ueffing P. The impact of the COVID-19 crisis on meeting needs for family planning: a global scenario by contraceptive methods used. Gates Open Res. (2020) 4:2. doi: 10.12688/gatesopenres.13148.2
39. Riley T, Sully E, Ahmed Z, Biddlecom A. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low-and middle-income countries. Int Perspect Sex Reprod Health. (2020) 46:73–6. doi: 10.1363/46e9020
40. Li G, Tang D, Song B, Wang C, Qunshan S, Xu C, et al. Impact of the COVID-19 pandemic on partner relationships and sexual and reproductive health: cross-sectional, online survey study. J Med Internet Res. (2020) 22:e20961. doi: 10.2196/20961
41. Organization WH. Pulse Survey on Continuity of Essential Health Services During the COVID-19 Pandemic: Interim Report, 27 August 2020. Geneva: World Health Organization (2020).
42. Sobotka T, Skirbekk V, Philipov D. Economic recession and fertility in the developed world. Popul Dev Rev. (2011) 37:267–306. doi: 10.1111/j.1728-4457.2011.00411.x
43. Endler M, Al-Haidari T, Benedetto C, Chowdhury S, Christilaw J, El Kak F, et al. How the coronavirus disease 2019 pandemic is impacting sexual and reproductive health and rights and response: results from a global survey of providers, researchers, and policy-makers. Acta Obstet Gynecol Scand. (2021) 100:571–8. doi: 10.1111/aogs.14043
44. Meherali S, Adewale B, Ali S, Kennedy M, Salami BO, Richter S, et al. Impact of the COVID-19 pandemic on adolescents' sexual and reproductive health in low- and middle-income countries. Int J Environ Res Public Health. (2021) 18:13221. doi: 10.3390/ijerph182413221
45. Polis CB, Biddlecom A, Singh S, Ushie BA, Rosman L, Saad A. Impacts of COVID-19 on contraceptive and abortion services in low-and middle-income countries: a scoping review. Sexual Reprod Health Matters. (2022) 30:2098557. doi: 10.1080/26410397.2022.2098557
46. Michael TO, Agbana RD, Ojo TF, Kukoyi OB, Ekpenyong AS, Ukwandu D. COVID-19 pandemic and unmet need for family planning in Nigeria. Pan Afr Med J. (2021) 40:186. doi: 10.11604/pamj.2021.40.186.27656
47. Organization WH. Impact of Covid-19 on SRMNCAH Services, Regional Strategies, Solutions and Innovations: A Comprehensive Report. Geneva (2020).
48. Sánchez SM, Rivera-Montero D, Murad-Rivera R, Calderón-Jaramillo M, Roldán D, Castaño LM, et al. Changes COVID-19 post-quarantine behaviors, hygiene and expectations in Colombia: population survey from 1st to 13th September, 2020. medRxiv. (2020) 2020:20239442. doi: 10.1101/2020.11.26.20239442
49. Bukuluki P, Kisaakye P, Mulekya F, Mushomi J, Mayora C, Palattiyil G, et al. Disruption in accessing sexual and reproductive health services among border populations during COVID-19 lockdown in Uganda. J Glob Health. (2022) 12:04065. doi: 10.7189/jogh.12.04065
50. Vora KS, Saiyed S, Natesan S. Impact of COVID-19 on family planning services in India. Sexual Reprod Health Matters. (2020) 28:1785378. doi: 10.1080/26410397.2020.1785378
51. Le Guen M, Ventola C, Bohet A, Moreau C, Bajos N. Men's contraceptive practices in France: evidence of male involvement in family planning. Contraception. (2015) 92:46–54. doi: 10.1016/j.contraception.2015.03.011
52. Schrager SM, Olson J, Beharry M, Belzer M, Goldsich K, Desai M, et al. Young men and the morning after: a missed opportunity for emergency contraception provision? J Fam Plann Reprod Health Care. (2015) 41:33–7. doi: 10.1136/jfprhc-2013-100617
53. Rehnstrom Loi U, Lindgren M, Faxelid E, Oguttu M, Klingberg-Allvin M. Decision-making preceding induced abortion: a qualitative study of women's experiences in Kisumu, Kenya. Reprod Health. (2018) 15:166. doi: 10.1186/s12978-018-0612-6
54. Thummalachetty N, Mathur S, Mullinax M, DeCosta K, Nakyanjo N, Lutalo T, et al. Contraceptive knowledge, perceptions, and concerns among men in Uganda. BMC Public Health. (2017) 17:1–9. doi: 10.1186/s12889-017-4815-5
55. Haakenstad A, Angelino O, Irvine CMS, Bhutta ZA, Bienhoff K, Bintz C, et al. Measuring contraceptive method mix, prevalence, and demand satisfied by age and marital status in 204 countries and territories, 1970-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2022) 400:295–327. doi: 10.1016/S0140-6736(22)00936-9
56. Haffejee F, O'Connor L, Govender N, Reddy P, Sibiya MN, Ghuman S, et al. Factors associated with unintended pregnancy among women attending a public health facility in KwaZulu-Natal, South Africa. South Afri Fam Practice. (2017) 60:79–83. doi: 10.1080/20786190.2017.1396790
57. Liang M, Simelane S, Fillo GF, Chalasani S, Weny K, Canelos PS, et al. The state of adolescent sexual and reproductive health. J Adolesc Health. (2019) 65:S3–S15. doi: 10.1016/j.jadohealth.2019.09.015
58. Sarder A, Islam SMS, Talukder A, Ahammed B. Prevalence of unintended pregnancy and its associated factors: evidence from six south Asian countries. PLoS ONE. (2021) 16:e0245923. doi: 10.1371/journal.pone.0245923
59. Lopez LM, Grey TW, Tolley EE, Chen M. Brief educational strategies for improving contraception use in young people. Cochr Database Systemat Rev. (2016) 3:CD012025. doi: 10.1002/14651858.CD012025.pub2
60. Xie K, Zhang W, Fang W, Lian Y, Lin S, Fang J. The analgesic efficacy of oxycodone hydrochloride versus fentanyl during outpatient artificial abortion operation: a randomized trial. Medicine. (2017) 96:e7376. doi: 10.1097/MD.0000000000007376
61. Irani L, Speizer IS, Fotso J-C. Couple characteristics and contraceptive use among women and their partners in urban Kenya. Int Perspect Sex Reprod Health. (2014) 40:11. doi: 10.1363/4001114
62. Cavazos-Rehg PA, Krauss MJ, Spitznagel EL, Schootman M, Bucholz KK, Peipert JF, et al. Age of sexual debut among US adolescents. Contraception. (2009) 80:158–62. doi: 10.1016/j.contraception.2009.02.014
63. McGrath N, Nyirenda M, Hosegood V, Newell M-L. Age at first sex in rural South Africa. Sex Transm Infect. (2009) 85:i49–55. doi: 10.1136/sti.2008.033324
64. Wellings K, Collumbien M, Slaymaker E, Singh S, Hodges Z, Patel D, et al. Sexual behaviour in context: a global perspective. Lancet. (2006) 368:1706–28. doi: 10.1016/S0140-6736(06)69479-8
65. Zaba B, Pisani E, Slaymaker E, Boerma JT. Age at first sex: understanding recent trends in African demographic surveys. Sex Transm Infect. (2004) 80:ii28–35. doi: 10.1136/sti.2004.012674
66. Slaymaker E, Bwanika JB, Kasamba I, Lutalo T, Maher D, Todd J. Trends in age at first sex in Uganda: evidence from Demographic and Health Survey data and longitudinal cohorts in Masaka and Rakai. Sex Transm Infect. (2009) 85:i12–9. doi: 10.1136/sti.2008.034009
67. Finer LB. Trends in premarital sex in the United States, 1954–2003. Public Health Rep. (2007) 122:73–8. doi: 10.1177/003335490712200110
68. Yu J. Teenage sexual attitudes and behaviour in China: a literature review. Health Soc Care Community. (2012) 20:561–82. doi: 10.1111/j.1365-2524.2011.01054.x
69. Burke L, Nic Gabhainn S, Kelly C. Socio-demographic, health and lifestyle factors influencing age of sexual initiation among adolescents. Int J Environ Res Public Health. (2018) 15:1851. doi: 10.3390/ijerph15091851
70. Christin-Maitre S. History of oral contraceptive drugs and their use worldwide. Best practice and research. Clin Endocrinol Metabol. (2013) 27:3–12. doi: 10.1016/j.beem.2012.11.004
71. Sanga K, Mola G, Wattimena J, Justesen A, Black IK. Unintended pregnancy amongst women attending antenatal clinics at the Port Moresby General Hospital. Austr N Zeal J Obstetr Gynaecol. (2014) 54:360–5. doi: 10.1111/ajo.12219
72. Exavery A, Kanté AM, Njozi M, Tani K, Doctor HV, Hingora A, et al. Predictors of mistimed, and unwanted pregnancies among women of childbearing age in Rufiji, Kilombero, and Ulanga districts of Tanzania. Reprod Health. (2014) 11:1–9. doi: 10.1186/1742-4755-11-63
Keywords: unintended pregnancy, partner, contraception, knowledge, attitude, practice
Citation: Liu R, Dong X, Ji X, Chen S, Yuan Q, Tao Y, Zhu Y, Wu S, Zhu J and Yang Y (2023) Associations between sexual and reproductive health knowledge, attitude and practice of partners and the occurrence of unintended pregnancy. Front. Public Health 10:1042879. doi: 10.3389/fpubh.2022.1042879
Received: 13 September 2022; Accepted: 07 December 2022;
Published: 04 January 2023.
Edited by:
Harshad Thakur, Tata Institute of Social Sciences, IndiaReviewed by:
Haiyan Zhu, First Affiliated Hospital of Wenzhou Medical University, ChinaShanaz Ghuman, Durban University of Technology, South Africa
Copyright © 2023 Liu, Dong, Ji, Chen, Yuan, Tao, Zhu, Wu, Zhu and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yongbin Yang,  eXlidnN5d3pAMTYzLmNvbQ==; Jingfen Zhu, emh1amluZ2Zlbmp0QHNoc211LmVkdS5jbg==; Sufang Wu, d3NmX3NmcGhAc2p0dS5lZHUuY24=
eXlidnN5d3pAMTYzLmNvbQ==; Jingfen Zhu, emh1amluZ2Zlbmp0QHNoc211LmVkdS5jbg==; Sufang Wu, d3NmX3NmcGhAc2p0dS5lZHUuY24=
†These authors have contributed equally to this work and share first authorship