 Tore Bonsaksen1,2Anne Mari Steigen1*Tonje Holte Stea3Annette Løvheim Kleppang3,4Lars Lien1,5Marja Leonhardt5,6
Tore Bonsaksen1,2Anne Mari Steigen1*Tonje Holte Stea3Annette Løvheim Kleppang3,4Lars Lien1,5Marja Leonhardt5,6- 1Department of Health and Nursing Sciences, Inland Norway University of Applied Sciences, Elverum, Norway
- 2Department of Health, VID Specialized University, Stavanger, Norway
- 3Department of Health and Nursing Science, University of Agder, Kristiansand, Norway
- 4Department of Public Health and Sports Sciences, Inland Norway University of Applied Sciences, Elverum, Norway
- 5Norwegian National Advisory Unit on Concurrent Substance Abuse and Mental Health Disorders, Innlandet Hospital Trust, Brumunddal, Norway
- 6Faculty of Health Studies, VID Specialized University, Oslo, Norway
Social media are an integral part of adolescents' daily lives, and reviews have suggested an overall small association between more social media use and mental health problems. However, researchers have commonly investigated social media use in a time use perspective, rendering nuances in adolescents' social media experience less well explored. Thus, studies of relationships between social media use and mental health problems need also examine the nature of the events taking place on social media. This study aimed to examine depressive symptoms in adolescents in relationship to time spent on social media, negative social media-related experiences, and general self-efficacy. Data collected in a national survey, Ungdata 2021 (n = 139,841), was used. Multivariate linear regression analyses showed that time spent on social media was associated with depressive symptoms (β = 0.09, p < 0.001). However, negative social media-related experiences were more strongly associated with depressive symptoms (β ranging 0.09–0.22, all p < 0.001), and their inclusion weakened the initial association between time on social media and depressive symptoms. General self-efficacy was directly associated with lower symptom levels (β = −0.29, p < 0.001) but did not change the associations between social media use and depressive symptoms. The findings imply that not only time spent on social media, but in particular negative social media-related experiences, are related to depressive symptoms in Norwegian adolescents. General self-efficacy is an important resource for adolescents' mental health.
Introduction
Social media broadly refers to applications that allow users to engage in virtual interactions, with wider or narrower audiences (1). Social media have become a prominent aspect of 21st century culture, and they are widely adopted across the world (2, 3). Young people use social media more often than older people (4, 5), and certain types of image-based social media, such as Instagram and Snapchat, are more often preferred among people in the younger age groups (5). Most social media are financed through advertising that is algorithmically controlled, which means that each user gets content that is tailored to their special target group, and what the user has shown interest in in the past (6).
In Norway, 99% of young people between 13 and 18 years use social media, with YouTube, Snapchat, Instagram, Facebook, and TikTok being the most popular (7). Social media is an important arena for socialization among young people, and engaging with social media gives rise to positive as well as negative experiences (8). Compared to boys, girls appear to have more positive (e.g., communication, positive attention) and negative experiences (e.g., pressure, social comparison) on social media (8), and more negative experiences have also been found among adolescents with lower sociodemographic status (9). While longitudinal studies are still relatively few, studies of adolescents in Norway have found that more time spent on social media has predicted subsequent increases in alcohol use (10, 11) as well as increases in depressive symptoms and conduct problems (11). International studies have reported higher social media use to be associated with more conflict within the family (12) and lower satisfaction with family life (13). Together, the studies indicate a need for further research on the possible long-term consequences of social media use among adolescents, as well as on consequences for the families involved.
There is a need to expand the scope of inquiry beyond the mere time spent on social media to also include the nature of the interactions taking place on social media and the consequences they may have. While some have emphasized social media's positive potential for connection and inclusion (14–16), others have argued that social media are substitutes for real-life relationships and rather serve to increase stress, such as “fear of missing out” (17, 18). For adolescents, social media use may instigate a pressure toward having a large number of followers and receiving affirmation (“likes”) as indicators of social acceptance, and lack of affirmation has been found to result in negative emotions and higher levels of depressive symptoms (19). In a large cross-national study of adolescents aged 11–15 years from 42 countries throughout Europe (weighted n = 180,919), about 12% have experienced cyber-bullying on social media, and more time spent on social media has been related to a greater risk of being bullied (20). Social media may in the case of late night use cause sleep problems (21, 22), which is a risk factor for attention problems in school (23) and for developing depression (24). However, such specific consequences of social media use may go unnoticed in studies where time use is the sole measure of social media use. Thus, when specific negative social media-related events are not considered, the commonly detected associations between time spent on social media and poorer mental health may concern very different circumstances and obscure more relevant relationships (25, 26).
Researchers have found diverging results with regard to the relationships between social media use and aspects of mental health. Whereas several studies have shown associations between higher levels of social media use and poorer mental health (18, 22, 27–29), recent reviews have indicated mixed results and an overall weak negative association across studies (1, 30). The great variety of methods for measuring both social media use and mental health outcomes may partly account for the mixed results (31). Associations between social media use and mental health have also been found to vary by gender, with more social media use related to poorer mental health in females (32). Thus, to move research forward, future studies should carefully specify the population of interest and which aspect of social media use is of interest.
Among young people, psychological resource factors such as general self-efficacy have been associated with favorable mental health outcomes in several studies over the last decades (33–35). In addition, self-efficacy has been found to moderate associations between various aspects of social media use and mental health, indicating that associations between more social media use and poorer mental health may be stronger for people with low self-efficacy (36, 37). Thus, while self-efficacy in adolescents may be vulnerable to the influence from social media, self-efficacy may also be viewed as a psychological resource that can buffer against a potentially negative influence from social media on mental health. The aim of the study was to examine depressive symptoms in adolescents in relationship to social media use, negative social media-related experiences, and general self-efficacy.
Methods
Design and procedure
A comprehensive cross-sectional study, the Ungdata survey, is offered annually to municipalities throughout Norway. Usually, the survey is conducted every third year in each municipality (38). In 2021 the survey was completed by 139,841 Norwegian adolescents, aged 13–19 years, representing 209 out of 356 Norwegian municipalities. Ungdata has become an essential source of information on young peoples' health and wellbeing, both at the national and municipal levels (see www.ungdata.no). The survey is conducted by the Norwegian Social Research (NOVA) at Oslo Metropolitan University in a collaboration with the Regional Drug and Alcohol Competence Centers (KoRus). The surveys are financed partially by the Norwegian Directorate of Health and gauge different aspects of adolescents' lives, i.e., health issues, local environment, school issues, social media use, diet, alcohol consumption, relationships with friends and parents, leisure time activities and symptoms of depression.
Parents and students were informed via mail in advance, and parents of under-age adolescents (13–17 years of age) were assured that they could withdraw their children from participation at any time. If no prohibiting response was received from parents of under-age adolescents, the adolescents decided independently whether or not to participate in the survey. They decided in school whether they wanted to participate after being informed that participation was voluntary and that they could skip questions that they did not want to answer. The study was conducted as a web-based questionnaire administered at school during school hours with a teacher or an administrator present to answer questions. The students used approximately 30–45 min to complete the questionnaire.
Some parts of the questionnaire are used nationally in all participating municipalities, whereas other parts are selected or de-selected by each municipality. Therefore, the number of responses vary greatly between mandatory and elective parts of the questionnaire. In this study, most employed variables were derived from the mandatory questions used nationally, while some variables (general self-efficacy, reports on conflicts or arguments in the family due to social media use, and reports on not getting enough sleep due to social media use) were derived from elective parts of the survey. In addition, it was possible to complete only parts of the survey and leave the remaining questions unanswered. Thus, the number of responses on a specific question varied according to (i) whether the question was included in the survey presented to the individual participants (i.e., a decision made by the municipality), and (ii) whether the individual participant chose to respond to it.
Measures
Depressive symptoms
Depressive symptoms were measured using a six-item scale derived from the Depressive Mood Inventory (39), which was again based on the Hopkins Symptom Checklist (40). The adolescents were asked if during the past week they have been affected by any of the following: “Felt that everything is a struggle” (item 1), “had sleep problems” (item 2), “felt unhappy, sad or depressed” (item 3), “felt hopelessness about the future” (item 4), “felt stiff or tense” (item 5), “worried too much about things” (item 6). The six questions have four response categories: “Not been affected at all” (1), “not been affected much” (2), “been affected quite a lot” (3) and “been affected a great deal” (4). Sum scores were computed, ranging from 6 to 24; high scores indicated higher symptoms of depression. The depression scale has been psychometric evaluated among Norwegian adolescents. The scale showed good reliability (Person Separation Index: 0.802), and as a whole, the scale works reasonably well at a general level (41).
Sociodemographic factors
Gender (male/female), grade and centrality were used as covariates. Grade was used as an indicator for age, as age is not assessed within the survey. Centrality, as defined by Statistics Norway (42), was applied as a proxy for the grade of how centrally located a municipality in Norway is. Parents' level of education was measured by asking: “Did your parents go to university or to a university college?” Adolescents who were not in touch with one or both parents were asked to miss the question out. The response options were “No, none of them” (0) “Yes, one of them” (1), and “Yes, both of them” (2).
Social media use
Daily time spent on social media was measured by asking: “Think about what you do in a normal day, how much time do you spend on the following things: social media (Facebook, Instagram etc.).” Response options were no time, <30 min, 30 min−1 h, 1–2 h, 2–3 h and >3 h.
Negative social media-related experiences
Online bullying was assessed with the question “Have you been threatened or excluded on the internet?” with response options “yes, several times a week”; “yes, approximately once a week”; “yes, approximately once every 14 days”; “yes, approximately once a month”; “almost never” and “never.” Participants were asked whether the use of social media had resulted in “conflicts or arguments in the family” or “not getting enough sleep,” with response options “yes” and “no.” Further, the adolescents were asked to indicate on a five-point scale (not at all–very much) whether they had experienced “pressure to have many followers and likes on social media.” Responses on the scaled variables (“online bullying” and “pressure to have many followers and likes”) were recoded into dichotomous variables prior to analysis, with “never experienced online bullying” and “no pressure to have many likes and followers” coded as “no” and all other responses coded as “yes.”
Psychological resources
The General Self-Efficacy Scale (GSE) (43) is a questionnaire for assessing general self-efficacy among the general population aged 12 years and older. It has been translated into several languages (44), including Norwegian (45). The scale measures optimistic self-beliefs in coping with the demands of life. The short version of the GSE used in this study consists of 5 statements that respondents rate on a scale from 1 “completely disagree” to 4 “completely agree.” Example statements are: “I always manage to solve difficult problems if I try hard enough” (item 1) and “If someone opposes me, I can find the means and ways to get what I want” (item 2). The score is calculated by summing the individual's scores on all items. The score range is 5–20, with higher scores indicating higher self-efficacy. High correlations with self-appraisal, self-acceptance, and optimism indicate theoretical accuracy of the self-efficacy concept (46), and psychometric analyses of the GSE has consistently produced one latent dimension and high measures of internal consistency between items (47–49). In the current study, Cronbach's α was 0.87.
Statistical analysis
Individuals who did not respond to specific items were removed casewise. The internal consistency of items in utilized scales were calculated by Cronbach's α. Descriptive analyses were performed for all employed measures. The dependent variable (depressive symptoms score) had a distribution which deviated from the normal distribution (Kolmogorov-Smirnov test p < 0.001), and it was skewed toward lower scores (skewness = 0.46, SE = 0.01) with the median value (Md = 12.0) being lower than the mean value (M = 12.9). However, skewed distributions frequently occur in large public health datasets without normally compromising the validity of parametric statistical testing (50). Therefore, we proceeded with parametric tests.
Depending on the number of groups to be compared, group differences in depressive symptoms were examined with independent t-tests or one-way ANOVA. In multiple comparisons, the Bonferroni correction was applied. Single (Model 0) and multiple linear regression analyses (Models 1–3) were used to assess associations between independent variables and depressive symptoms. In the multiple linear regression analyses, independent variables were entered in this sequence: Model (1) included daily time spent on social media and negative social media-related experiences (i.e., victim of online bullying; experienced conflicts or arguments in the family; experienced too little sleep due to social media use; and experienced pressure to have followers and likes on social media). Model (2) included the Model (1) variables while also including general self-efficacy. In Model 3, we included the Model (2) variables while adjusting for sociodemographic variables (age, gender, centrality, parents' education). Interaction analyses were performed to examine whether associations between negative social media-related experiences and depressive symptoms varied by gender and levels of general self-efficacy. In the event of statistically significant interactions, post-hoc analyses would repeat Model 3 separately for boys and girls and for participants with higher/lower general self-efficacy, respectively. Due to the large sample size, results with a corresponding p < 0.01 were considered statistically significant. The strength of associations (effect sizes) was interpreted in line with Cohen: β about 0.10 is small, about 0.30 is medium, and about 0.50 is large (51). Multicollinearity was checked with standard guidelines, stating that VIF should be below 5 and tolerance above 0.2 (52).
Ethics
The study was conducted in accordance with the Declaration of Helsinki. Before participating in the study, all students were asked to provide informed consent. The parents received oral and written information about the study and were given the opportunity to withdraw their children from participation. The information letter was approved by The Norwegian Center for Research Data (NSD). All data were collected anonymously and then analyzed by independent researchers who did not participate in the collection of the data. The study was approved by the Institutional Ethics Review Board at Inland Norway University of Applied Sciences (protocol code 21/01894).
Results
Sample characteristics
The characteristics of the sample are shown in Table 1. Participants in the survey were 139,841 pupils from lower secondary (13–15 years of age) and upper secondary schools (16–19 years of age). The response rate in lower secondary schools was 83% and in upper secondary schools 67%, yielding an average response rate of 75% (38). The age distribution in the sample was similar between most categories, yet with declining participation rates in the higher age groups. The proportions of boys and girls were similar. The largest groups of participants lived in places classified to be in the middle range on the centrality index. Among 47% of the sample, both parents had higher education.
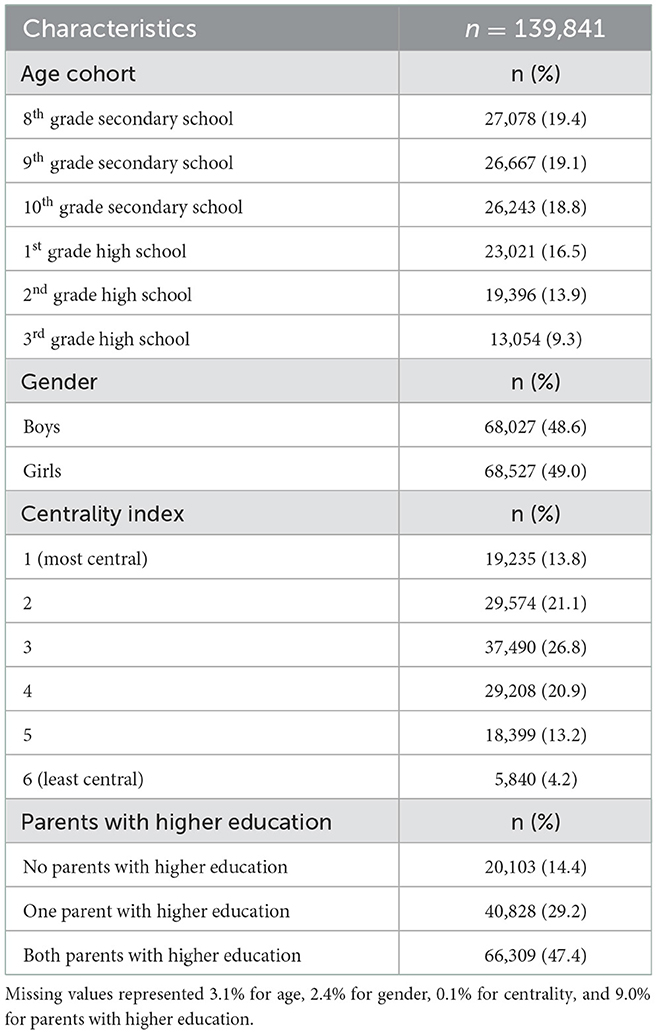
Table 1. Sample characteristics.
Depressive symptoms, general self-efficacy, social media use and negative social media-related experiences
Information about depressive symptom levels, general self-efficacy, social media use, and negative social media-related experiences is shown in Table 2. The mean level of depressive symptoms was 12.9 (SD = 4.9), while the mean level of general self-efficacy was 14.7 (SD = 3.1). Thirty-three percent of the sample reported to use social media daily for more than 3 h. Twenty-two percent had experienced being bullied on the internet, while 30% had experienced pressure toward having followers and receiving likes on social media. There were fewer participants with valid responses to the questions about having experienced social media-related conflicts or arguments in the family, or not getting enough sleep due to social media use. Among those with valid responses on these questions, 13% reported to have experienced social media-related conflicts or arguments in the family, while 49.5% reported to have experienced not getting enough sleep due to social media use.
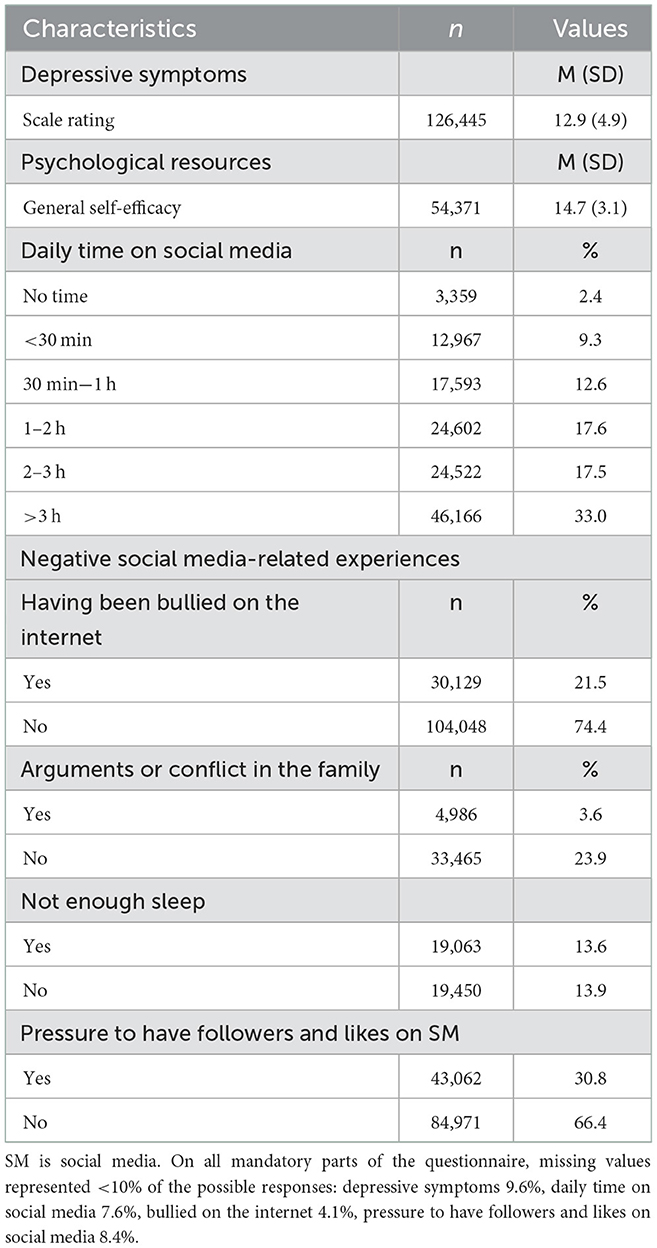
Table 2. Depressive symptoms, psychological resources, social media use, and negative social media-related experiences in the sample.
Depressive symptom levels in sample subgroups
The levels of depressive symptoms in sample subgroups are shown in Table 3. Depressive symptom levels were higher in the higher age groups, and girls had higher levels than boys. Depressive symptoms were also higher among adolescents living in urban districts, compared to rural, and higher among those whose parents did not have higher education. Those with higher levels (i.e., above median levels) of general self-efficacy had lower levels of depressive symptoms, compared to their counterparts. Those who spent more time on social media reported higher levels of depressive symptoms, compared to those who used social media less. For all types of negative social media-related experiences, the levels of depressive symptoms were significantly higher among those who had experienced the event, compared to their counterparts.
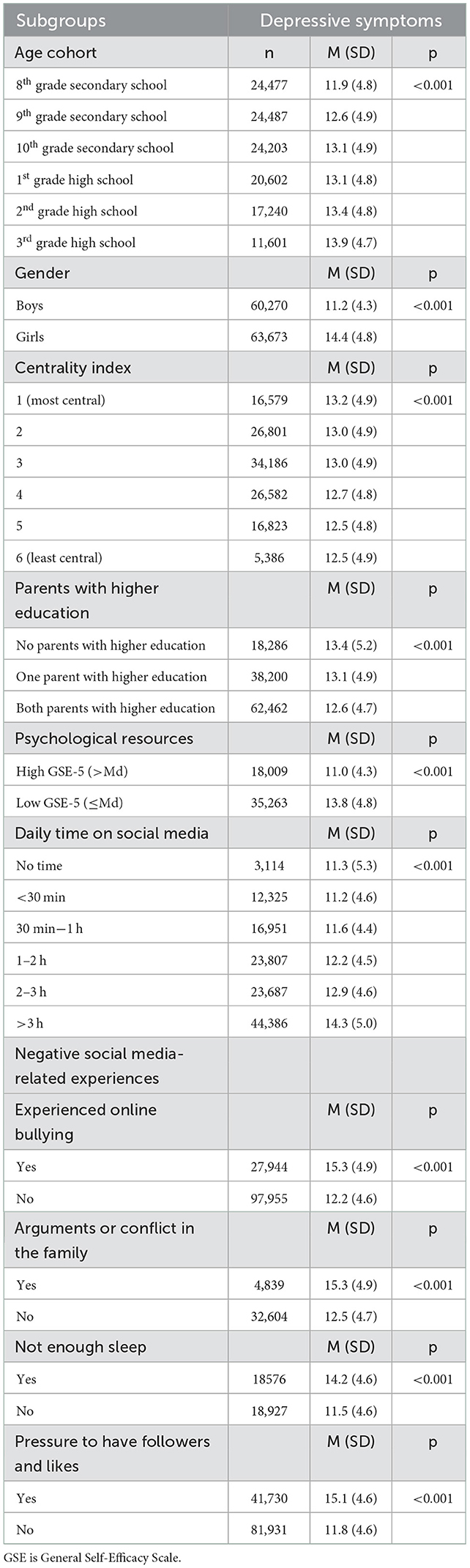
Table 3. Depressive symptoms in sample subgroups.
In the pairwise comparisons for variables with three or more categories (data not shown), differences in depressive symptom levels between age groups were statistically significant with one exception (10th grade vs. 1st grade high school). Depressive symptom levels were also significantly different between levels of centrality, with two exceptions (between levels 2 and 3, and between levels 5 and 6). The highest levels of depressive symptoms were found among adolescents where none of the parents had higher education, whereas the lowest levels were found among adolescents where both parents had higher education. Higher levels of social media use were, for the most part, significantly related to higher levels of depressive symptoms, but depressive symptom levels were not significantly different between adolescents who did not use social media and those using social media for < 1 h daily.
Social media use, negative social media-related experiences, and general self-efficacy associated with depressive symptoms
In preparation of the regression analyses, time spent on social media was re-categorized in order to obtain similar group sizes and a linear relationship with depressive symptoms (see Table 3). The two categories indicating the least daily time spent on social media were collapsed into one category (no social media use, up to 30 min daily). Otherwise, categories remained as before. No multicollinearity problems were detected (all VIFs ≤ 1.25, tolerance ≥ 0.80).
The results of the analysis of factors associated with depressive symptom levels are shown in Table 4. Crude associations with depressive symptoms were found for all included variables. More time spent daily on social media was associated with higher depressive symptom levels (β = 0.23, p < 0.001), as was experience with any of the negative social media-related events (β ranging between 0.20 and 0.32, all p < 0.001). Higher levels of general self-efficacy were associated with lower levels of depressive symptoms (β = −0.38, p < 0.001).
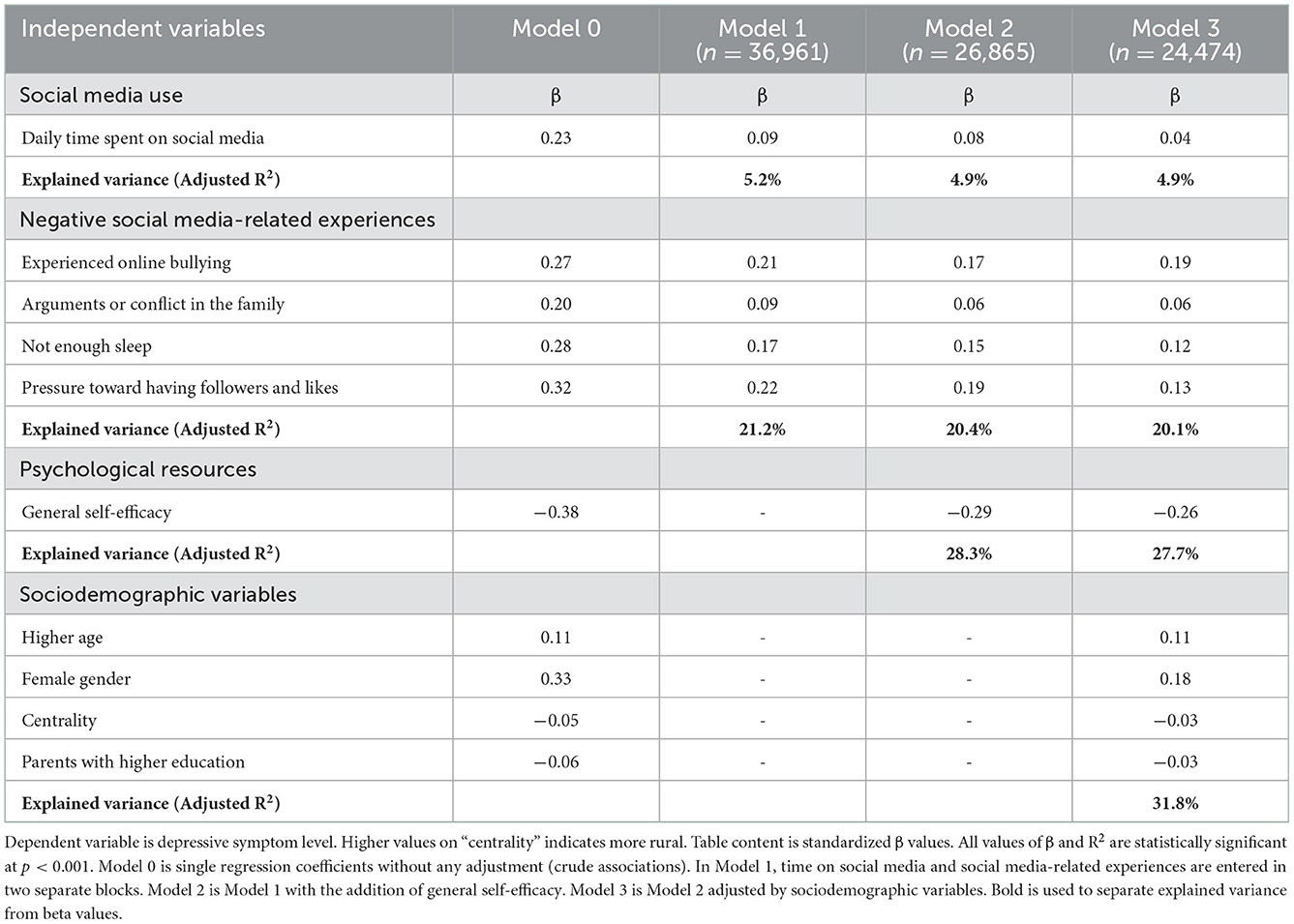
Table 4. Linear regression analysis showing associations between daily time spent on social media, negative social media-related experiences, general self-efficacy, and depressive symptoms.
As shown for the multivariate Model 1, more time spent on social media was associated with higher depressive symptom levels, but the association was weaker compared with the crude association (β = 0.09, p < 0.001). Having experienced any of the negative social media-related events was associated with higher depressive symptom levels, with associations being of varying strength (β ranging between 0.09 and 0.22, all p < 0.001). Variation in the negative social media-related events accounted for a larger proportion of the outcome variance (16.0%), compared to the variation in time spent on social media (5.2%).
When included in Model 2, higher self-efficacy was related to lower levels of depressive symptoms (β = −0.29, p < 0.001), explaining and additional 7.9% of the variance in depressive symptoms. The inclusion of general self-efficacy did not substantially change the associations between social media use, negative social media-related experiences, and depressive symptoms.
After adjusting by sociodemographic variables in Model 3, time spent daily on social media and having experienced any of the negative social media-related events were still associated with higher depressive symptom levels, and higher general self-efficacy was still related to lower depressive symptom levels. Higher age, female gender, living in more central areas, and having parents who did not have higher education were associated with higher depressive symptom levels.
Interaction analyses
Interaction analyses were performed to examine whether associations between negative social media experiences and depressive symptoms were moderated by gender and levels of general self-efficacy, respectively. Interactions were added in two subsequent iterations of the Model 3 regression analysis. In the first iteration, interaction terms gender × negative social media-related experiences (i.e., four separate interaction terms) were added to the Model 3 predictors, and in the second we added the interaction terms general self-efficacy × negative social media-related experiences. Gender significantly interacted with “arguments or conflict in the family” (p < 0.001), whereas the remaining three interaction terms yielded non-significant results. General self-efficacy interacted with “arguments or conflict in the family” and “pressure toward having followers and likes” (both p < 0.001), whereas the two remaining interaction terms were non-significant. Based on these results, we repeated the Model 3 regression analysis separately for boys and girls, and for participants with higher and lower general self-efficacy scores (spilt by the median score).
The results for boys and girls are displayed in Table 5. The pattern of associations was mostly identical for the two genders. However, having experienced conflicts or arguments related to social media use was associated with a higher level of depressive symptoms among girls, but not among boys. Also, for girls the model accounted for a somewhat larger proportion of the variance in depressive symptoms, and the association between higher general self-efficacy and lower levels of depressive symptoms was stronger than for boys.
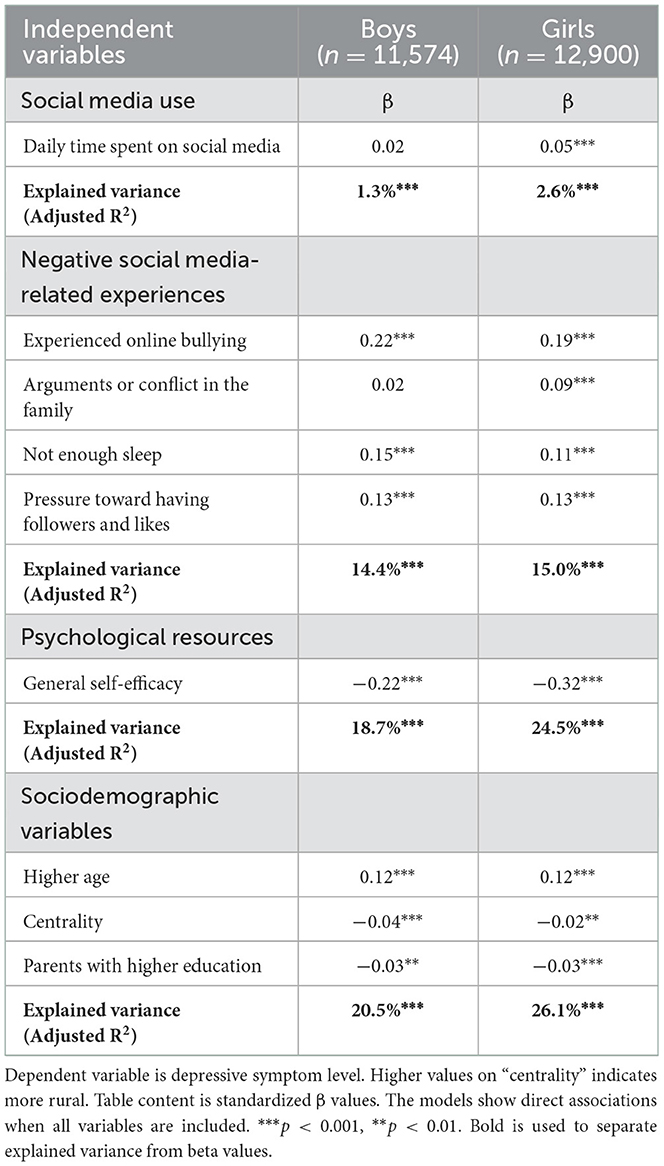
Table 5. Linear regression analysis showing associations between daily time spent on social media, negative social media-related experiences, general self-efficacy, and depressive symptoms by gender.
The results for higher and lower levels of general self-efficacy are displayed in Table 6. The pattern of associations was practically identical for the two groups, and the models accounted for similar proportions of the outcome variance. The association between female gender and depressive symptoms was slightly stronger for adolescents with lower levels of general self-efficacy, compared to those with higher levels.
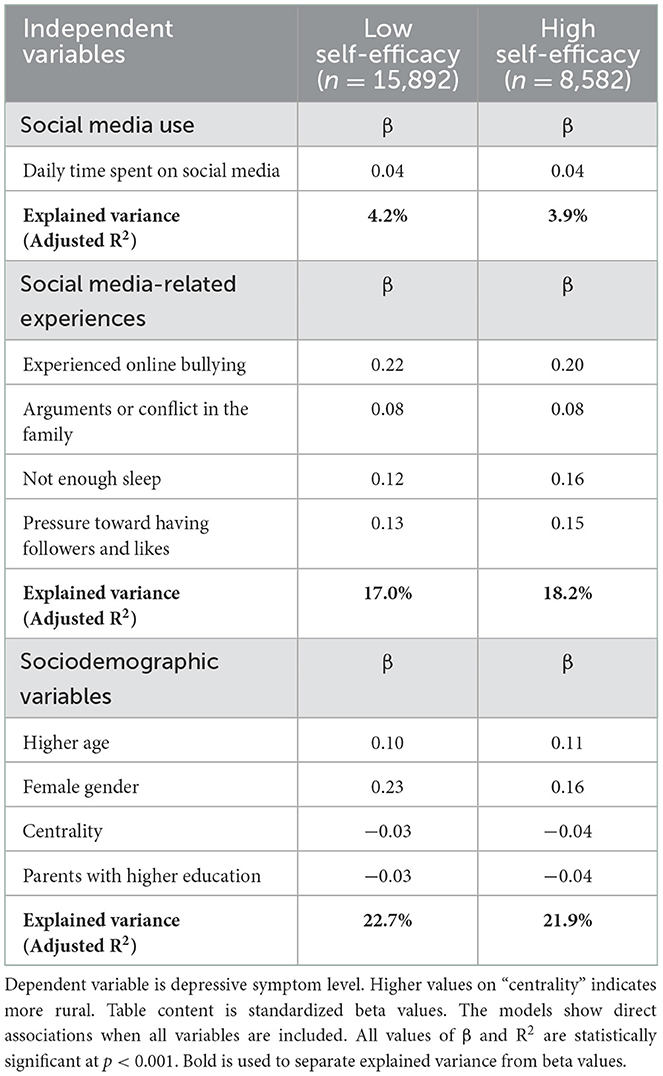
Table 6. Linear regression analysis showing associations between daily time on social media, social media-related experiences, and depressive symptoms by general self-efficacy levels.
Differences between the initial and the final sample
Given the loss of participants in the multivariate analysis, we compared the sample included in the Model 3 regression analysis with the initial sample. In comparison to the initial sample, the restricted sample included in the Model 3 analysis had a lower level of depressive symptoms (M = 12.8 vs. M = 12.9, Cohen's d = 0.02, p < 0.001) but a higher level of social media use (M = 4.6 vs. M = 4.5, Cohen's d = 0.09, p < 0.001). The restricted sample also had a higher proportion of participants in senior high school (54.3 vs. 37.8%), a higher proportion of girls (53 vs. 50%), a higher proportion had both parents without higher education (17.0 vs. 15.5%), and a higher proportion living in the less central areas of the country (44.3 vs. 36.9%, all p < 0.001).
Discussion
Main summary of results
This study found that negative social media-related experiences were associated with higher levels of depressive symptoms among Norwegian adolescents. When including negative social media-related experiences as independent variables together with daily time spent on social media, the association between time spent on social media and depressive symptoms was weakened, suggesting that negative social media-related events were responsible for some (but not all) of the association between time spent using social media and higher levels of depressive symptoms. Higher general self-efficacy levels were associated with lower levels of depressive symptoms.
Factors associated with depressive symptoms
In this study, more time spent on social media use was associated with higher levels of depressive symptoms. This corresponds with results from previous reviews that have suggested social media use to be associated with higher levels of depressive symptoms in adolescence (53). However, using a wider lens, a recent review and meta-analysis reported that associations between more social media use and poorer mental health varied considerably, with effect sizes ranging between 0.02 (ns) and 0.17 (54). In view of the variable results between studies and the small effect sizes often obtained, other factors may influence the relationship between social media use and depressive symptoms in adolescents (55).
In this study, we found that the inclusion of negative social media-related experiences in the regression model weakened the initial association between social media use and depressive symptoms, hence possibly accounting for some of the covariation between social media use and depressive symptoms. Among the included negative experiences, having experienced online bullying was shown to be most strongly associated with depressive symptoms. A relationship between having experienced online bullying and higher levels of depressive symptoms is consistent with findings from previous studies (56). These results support the idea that the content of social media use–what people experience during, and as a consequence of, social media use–is important to consider in relation to mental health outcomes, and that time spent on social media is merely one aspect of the social media exposure. While the results indicate that negative experiences related to social media use are relevant to consider, they also support the notion that there remains an independent relationship between time spent on social media and depressive symptoms in adolescents. This remaining relationship may be bi-directional or reversed, as recently suggested (57).
Almost half of the participants who responded to the questions related to sleep and social media use, reported not getting enough sleep due to social media use. This is in accordance with a recent Norwegian research report, stating that 50% of adolescents go to bed later than they should due to social media use (8). Previous studies have also suggested that social media use may cause sleep problems (21, 22), and our study substantiated higher depressive symptom levels among adolescents who have experienced sleep problems due to social media use. In addition, the results from our study showed that other problematic social media related experiences, such as “conflicts or arguments in the family” and “pressure to have many followers and likes,” were associated with higher depressive symptom levels. We should note that family conflicts related to social media hinges not only on the adolescent's social media use, but also on parents' attitudes and behaviors toward their adolescent's use of social media. Studies have shown that over the past decades parents have become increasingly aware of, and involved with, their children's social media use (58, 59), which in turn may lead to more family conflict centered around the issue (12). In combination, the findings suggest that substantial proportions of adolescents experience problematic consequences of their social media use, and that having such experiences are related to higher depressive symptoms. However, the nature of the relationship is uncertain, and bi-directional relationships are viable (57).
Moreover, the frequency of experiencing negative social media-related events may differ between groups. For example, adolescents from less affluent backgrounds have been found to report negative experiences from social media use more often than those from more affluent backgrounds (9), and possibly, associations between social media-related experiences and depressive symptoms may differ between groups with higher or lower vulnerability. Supporting this view, a recent study concluded that getting fewer likes on social media was a greater risk factor for negative affect and thoughts and feeling rejected among adolescents who were already victims of school bullying, compared to those who were not (19).
While this study has focused on depressive symptoms as the potential outcome of social media use and -encounters, social media may also have a beneficial effect on adolescent wellbeing. Social media may ease the access to supports and allow for a diversity of interactions and friendships (53), and for some, the virtual interaction may be easier than face-to-face social interaction (14–16). In a Norwegian qualitative study adolescents revealed that social media contributes to amplify social relations, as it is much easier to communicate and keep in touch via social media than in real life (60). However, negative experiences on social media have been found to be more potent than positive experiences, as negative experiences have been significantly associated with higher levels of depressive symptoms, while positive experiences have been associated with minor and not statistically significant decreases in depressive symptoms (61). Individuals with depressive symptoms may also be more inclined to engage in social media for various reasons (57) and they may experience more negative interactions while doing so (61).
In this study, higher general self-efficacy levels were significantly associated with lower levels of depressive symptoms. Similarly, a previous study also showed that self-efficacy was related to depressive symptom levels, both concurrently and prospectively, but the nature of the associations varied by self-efficacy domain (62): a strong sense of efficacy for regulating negative affect was related to lower depressive symptoms, while stronger empathic self-efficacy was related to higher depressive symptom levels. In addition, a more recent study examining a cross-lagged model of associations found that depressive symptom levels predicted academic and emotional self-efficacy 6 months later, whereas self-efficacy did not predict subsequent depressive symptoms (63). Thus, the issue of causality in the relationship between self-efficacy and depressive symptoms is debated, and cyclical relationships are also viable. Previous studies have found that self-efficacy moderated associations between social media use and mental health (36, 37). Similarly, our study showed that general self-efficacy significantly moderated two of the associations between negative social media-related experiences and depressive symptoms. However, associations were only marginally different between adolescents with higher and lower levels of self-efficacy. In addition, including general self-efficacy in the regression model (Model 3) did not substantially change the associations between social media use, negative social media-related experiences, and depressive symptoms. Thus, despite significant interaction effects, the comparison of effect sizes in our study supports the view that associations between social media use and negative social media-related experiences and depressive symptoms do not differ substantially between adolescents with different levels of self-efficacy.
Comparisons with other studies are, to some extent, hampered by different questions and conceptualizations used across studies. For example, 22 % of the adolescents in this study reported to have experienced online bullying. This proportion is higher compared to the results of Craig et al. (20), where 12% reported having experienced cyberbullying on social media. However, these results are not fully comparable, given that more adolescents would logically report having experienced online bullying (as we asked in this study), compared to those having experienced cyberbullying on social media (as asked by Craig and co-workers). Online bullying, the concept used in our study, would logically encompass bullying within a wider internet-based context, including e.g., online gaming, and is not necessarily restricted to the social media context. For these reasons, our results should be interpreted with caution.
Study strengths and limitations
A considerable strength of the present study is the high participation rate, the large sample size, and the use of recently collected data (2021) which provide updated descriptions of adolescents' perceptions of life in Norway. The very large sample, and the resulting high statistical power, give rise to challenges in the interpretation of associations, where statistically significant results must be scrutinized with an emphasis on effect size. In this study, for example, we found several statistically significant interaction effects, yet close to negligible group differences when comparing categories of the moderator variables.
Another limitation is that the sample used for the Model 3 regression analysis was different from the initial sample with regards to the participants' level of depressive symptoms, time spent on social media use, age, gender, centrality, and their parents' educational level. Thus, our results concerned with factors associated with depressive symptoms are not fully representative of the general population of adolescents, in particular with regards to the age distribution.
A limitation of this study is the cross-sectional design, which precludes inferences about causal relationships. Depressive symptoms may not only be a result of social media use and exposure; such symptoms may also increase social media use and potentially the risk of experiencing adverse events, such as online bullying. In addition, the study relies on self-report measures, some of which with unknown psychometric properties, which may have led to unidentified misclassifications or measurement errors. While the questions used to assess negative social media-related experiences have been used in the Ungdata surveys for several years (64), we have no information about the validity of the questions. Furthermore, the associations found between social media use and depressive symptoms might be influenced by other factors that were not controlled for in the study.
Conclusion and implications for future research
This study showed that negative social media-related events were associated with higher levels of depressive symptoms among adolescents in Norway, and negative social media-related events appeared to account for some of the association between time spent using social media and higher levels of depressive symptoms. Higher general self-efficacy levels were associated with lower levels of depressive symptoms. More knowledge is needed about what types of events might constitute both positive and negative events related to social media use, and what outcomes they might produce. In particular, further research on cyberbullying and its contexts, is needed. Such research may include a larger diversity of online platforms where people interact with each other, including both social network platforms and online gaming platforms. Future research may also focus on identifying potential moderating variables, to enable a more comprehensive understanding of how social media use and -exposure may be differently associated with mental health outcomes in various groups of adolescents.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The data and materials from the Ungdata Surveys are stored in a national database administered by NOVA. The data are available for research purposes upon application. Further information about the study and the questionnaires can be found on the web page https://www.nsd.no/nsddata/serier/ungdata_eng.html. Requests to access these datasets should be directed to dW5nZGF0YUBvc2xvbWV0Lm5v.
Ethics statement
The studies involving human participants were reviewed and approved by Institutional Ethics Review Board, Inland Norway University of Applied Sciences. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
TB analyzed the data and drafted the manuscript. AS, TS, AK, LL, and ML provided input to the analysis and presentation and edited the manuscript. All authors agreed to be responsible for the final submitted version of the manuscript.
Acknowledgments
We thank the study participants for their participation. We thank Norwegian Social Research (NOVA) at Oslo Metropolitan University and the Regional Drug and Alcohol Competence Centers (KoRus) for data administration.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Meier A, Reinecke L. Computer-mediated communication, social media, and mental health: a conceptual and empirical meta-review. Comm Res. (2021) 48:1182–209. doi: 10.1177/0093650220958224
2. Boulianne S. Social media use and participation: a meta-analysis of current research. Inform Comm Soc. (2015) 18:524–38. doi: 10.1080/1369118X.2015.1008542
3. Hunt YM, Beckjord EB, Moser RP, Hesse BW. Social media use in the United States: implications for health communication. JMIR. (2009) 11:e48. doi: 10.2196/jmir.1249
4. Feng G, Zhang Y, Lin Z. A meta-analysis of the effects of sociodemographic factors on social media adoption. Int J Comm. (2019) 13. Available online at: https://ijoc.org/index.php/ijoc/article/view/10088
5. Auxier B, Anderson M. Social Media Use in 2021. Pew Research Center. (2021). Available online at: https://www.pewresearch.org/internet/2021/04/07/social-media-use-in-2021/ (accessed October 1, 2022).
6. Carr CT, Hayes RA. Social media: defining, developing, and divining. Atlant J Comm. (2015) 23:46–65. doi: 10.1080/15456870.2015.972282
7. The Norwegian Media Authority. Children and Media 2020. [In Norwegian: Barn og medier 2020]. Oslo: Medietilsynet. (2020). Available online at: https://www.medietilsynet.no/globalassets/publikasjoner/barn-og-medier-undersokelser/2020/201015-barn-og-medier-2020-hovedrapport-med-engelsk-summary.pdf (accessed October 1, 2022).
8. Hjetland GJ, Finserås TR, Skogen JC. Worldwide in a keystroke - Adolescents' use and experiences with social media and online gaming [Norwegian: Hele verden er et tastetrykk unna. Ungdommers Bruk og Opplevelser Med Sosiale Medier og Online Gaming] Oslo: Norwegian Institute of Public Health. (2022). Available online at: https://www.fhi.no/publ/2022/hele-verden-er-et-tastetrykk-unna—ungdommers-bruk-og-opplevelser-med-sosi/
9. Skogen JC, Bøe T, Finserås TR, Sivertsen B, Hella RT, Hjetland GJ. Lower subjective socioeconomic status is associated with increased risk of reporting negative experiences on social media. Findings from the “LifeOnSoMe”-study. Front Public Health. (2022) 10. doi: 10.3389/fpubh.2022.873463
10. Brunborg GS, Skogen JC, Burdzovic Andreas J. Time spent on social media and alcohol use among adolescents: a longitudinal study. Addict Behav. (2022) 130:107294. doi: 10.1016/j.addbeh.2022.107294
11. Brunborg GS, Burdzovic Andreas J. Increase in time spent on social media is associated with modest increase in depression, conduct problems, and episodic heavy drinking. J Adolesc. (2019) 74:201–9. doi: 10.1016/j.adolescence.2019.06.013
12. Vannucci A, McCauley Ohannessian C. Social media use subgroups differentially predict psychosocial well-being during early adolescence. J Youth Adolesc. (2019) 48:1469–93. doi: 10.1007/s10964-019-01060-9
13. Savci M, Akat M, Ercengiz M, Griffiths MD, Aysan F. Problematic social media use and social connectedness in adolescence: the mediating and moderating role of family life satisfaction. Int J Mental Health Addict. (2022) 20:2086–102. doi: 10.1007/s11469-020-00410-0
14. Morahan-Martin J, Schumacher P. Loneliness and social uses of the Internet. Comput Hum Behav. (2003) 19:659–71. doi: 10.1016/S0747-5632(03)00040-2
15. Nowland R, Necka EA, Cacioppo JT. Loneliness and social internet use: pathways to reconnection in a digital world? Perspect Psychol Sci. (2018) 13:70–87. doi: 10.1177/1745691617713052
16. Thomas L, Orme E, Kerrigan F. Student loneliness: the role of social media through life transitions. Comput Educ. (2020) 146:103754. doi: 10.1016/j.compedu.2019.103754
17. Fumagalli E, Dolmatzian MB, Shrum LJ. Centennials, FOMO, and loneliness: an investigation of the impact of social networking and messaging/VoIP apps usage during the initial stage of the coronavirus pandemic. Front Psychol. (2021) 12. doi: 10.3389/fpsyg.2021.620739
18. Hunt MG, Marx R, Lipson C, Young J. No more FOMO: limiting social media decreases loneliness and depression. J Soc Clin Psychol. (2018) 37:751–68. doi: 10.1521/jscp.2018.37.10.751
19. Lee HY, Jamieson JP, Reis HT, Beevers CG, Josephs RA, Mullarkey MC, et al. Getting fewer “likes” than others on social media elicits emotional distress among victimized adolescents. Child Develop. (2020) 91:2141–59. doi: 10.1111/cdev.13422
20. Craig W, Boniel-Nissim M, King N, Walsh SD, Boer M, Donnelly PD, et al. Social media use and cyber-bullying: a cross-national analysis of young people in 42 countries. J Adolesc Health. (2020) 66(6, Supplement):S100–S8. doi: 10.1016/j.jadohealth.2020.03.006
21. Woods HC, Scott H. #Sleepyteens: Social media use in adolescence is associated with poor sleep quality, anxiety, depression and low self-esteem. J Adoles. (2016) 51:41–9. doi: 10.1016/j.adolescence.2016.05.008
22. Kelly Y, Zilanawala A, Booker C, Sacker A. Social media use and adolescent mental health: findings from the UK Millennium Cohort Study. E Clin Med. (2018) 6:59–68. doi: 10.1016/j.eclinm.2018.12.005
23. Chen M, Xu Q, Cui M. Sleep problems, attention, and classroom learning behaviors of Chinese elementary school children: the moderating role of gender. School Psychol Int. (2021) 42:341–57. doi: 10.1177/0143034321993502
24. Sivertsen B, Harvey AG, Lundervold AJ, Hysing M. Sleep problems and depression in adolescence: results from a large population-based study of Norwegian adolescents aged 16–18 years. Eur Child Adoles Psych. (2014) 23:681–9. doi: 10.1007/s00787-013-0502-y
25. Trifiro BM, Gerson J. Social media usage patterns: research note regarding the lack of universal validated measures for active and passive use. Soc Media Soc. (2019) 5. doi: 10.1177/2056305119848743
26. Bekalu MA, McCloud RF, Viswanath K. Association of social media use with social well-being, positive mental health, and self-rated health: disentangling routine use from emotional connection to use. Health Educ Behav. (2019) 46:69S−80S. doi: 10.1177/1090198119863768
27. Geirdal AØ, Ruffolo M, Leung J, Thygesen H, Price D, Bonsaksen T, et al. Mental health, quality of life, wellbeing, loneliness and use of social media in a time of social distancing during the COVID-19 outbreak. A cross country comparative study. J Mental Health. (2021) 30:148–55. doi: 10.1080/09638237.2021.1875413
28. Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE. (2020) 15:e0231924. doi: 10.1371/journal.pone.0231924
29. Kleppang AL, Steigen AM, Ma L, Søberg Finbråten H, Hagquist C. Electronic media use and symptoms of depression among adolescents in Norway. PLoS ONE. (2021) 16:e0254197. doi: 10.1371/journal.pone.0254197
30. Keles B, McCrae N, Grealish A. A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int J Adoles Youth. (2020) 25:79–93. doi: 10.1080/02673843.2019.1590851
31. Petropoulos Petalas D, Konijn EA, Johnson BK, Veldhuis J, Bij de Vaate NAJD, Burgers C, et al. Plurality in the measurement of social media use and mental health: an exploratory study among adolescents and young adults. Soc Media Society. (2021) 7. doi: 10.1177/20563051211035353
32. Blomfield Neira CJ, Barber BL. Social networking site use: linked to adolescents' social self-concept, self-esteem, and depressed mood. Austral J Psychol. (2014) 66:56–64. doi: 10.1111/ajpy.12034
33. Najafi M, Foladjang M. The relationship between self- efficacy and mental health among high school students. Clin Psychol Pers. (2007) 5:69–83. Available online at: http://cpap.shahed.ac.ir/article_2599.html?lang=en
34. Abdel-Khalek AM, Lester D. The association between religiosity, generalized self-efficacy, mental health, and happiness in Arab college students. Pers Indiv Diff. (2017) 109:12–6. doi: 10.1016/j.paid.2016.12.010
35. Parto M, Besharat MA. The direct and indirect effects of self- efficacy and problem solving on mental health in adolescents: assessing the role of coping strategies as mediating mechanism. Procedia Soc Behav Sci. (2011) 30:639–43. doi: 10.1016/j.sbspro.2011.10.124
36. Calandri E, Graziano F, Rollé L. Social media, depressive symptoms and wellbeing in early adolescence. The moderating role of emotional self-efficacy and gender. Front Psychol. (2021) 12:1871. doi: 10.3389/fpsyg.2021.660740
37. Li Y. Upward social comparison and depression in social network settings. Internet Res. (2019) 29:46–59. doi: 10.1108/IntR-09-2017-0358
38. Bakken A. Ungdata 2021. Nasjonale Resultater [Ungdata 2021: National results]. Oslo: NOVA, OsloMet. NOVA Report 8/21. (2021).
39. Kandel DB, Davies M. Epidemiology of depressive mood in adolescents: an empirical study. Arch Gen Psych. (1982) 39:1205–12. doi: 10.1001/archpsyc.1982.04290100065011
40. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symptom Checklist (HSCL): a self-report symptom inventory. Behav Sci. (1974) 19:1–15. doi: 10.1002/bs.3830190102
41. Kleppang AL, Steigen AM, Finbråten HS. Using Rasch measurement theory to assess the psychometric properties of a depressive symptoms scale in Norwegian adolescents. Health Qual Life Outcomes. (2020) 18:127. doi: 10.1186/s12955-020-01373-5
42. Statistics Norway. Classification of Centrality. Oslo: Statistics Norway. (2020). Available online at: https://www.ssb.no/en/klass/klassifikasjoner/128 (accessed October 1, 2022).
43. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In:Weinman J, Wright S, Johnston M, editors. Measures in Health Psychology: A User's Portfolio. Winsor, United Kingdom: Nfer-Nelson. (1995). p. 35–7.
44. Luszczynska A, Scholz U, Schwarzer R. The general self-efficacy scale: Multicultural validation studies. J Psychol Interdisc Appl. (2005) 139:439–57. doi: 10.3200/JRLP.139.5.439-457
45. Røysamb E. Adolescent risk making: behaviour patterns and the role of emotions and cognitions. (PhD thesis). Oslo, Norway: University of Oslo. (1997).
46. Posadzki P, Stockl S, Musonda P, Tsouroufli M. A mixed-method approach to sense of coherence, health behaviors, self-efficacy and optimism: towards the operationalization of positive health attitudes. Scand J Psychol. (2010) 51:246–52. doi: 10.1111/j.1467-9450.2009.00764.x
47. Leganger A, Kraft P, Røysamb E. Perceived self-efficacy in health behaviour research: Conceptualisation, measurement and correlates. Psychol Health. (2000) 15:51–69. doi: 10.1080/08870440008400288
48. Bonsaksen T, Lerdal A, Heir T, Ekeberg Ø, Skogstad L, Grimholt TK, et al. General self-efficacy in the Norwegian population: differences and similarities between sociodemographic groups. Scand J Public Health. (2019) 47:695–704. doi: 10.1177/1403494818756701
49. Steigen AM, Finbraaten H, Kleppang A. Using Rasch analysis to assess the psychometric properties of a five-item version of the General Self-Efficacy Scale in adolescents. Int J Environ Res Public Health. (2022) 19:3082. doi: 10.3390/ijerph19053082
50. Lumley T, Diehr P, Emerson S, Chen L. The importance of the normality assumption in large public health data sets. Annu Rev Public Health. (2002) 23:151–69. doi: 10.1146/annurev.publhealth.23.100901.140546
52. Hocking RR. Methods and Applications of Linear Models: Regression and the Analysis of Variance. Hoboken, NJ: Wiley. (2013).
53. Vidal C, Lhaksampa T, Miller L, Platt R. Social media use and depression in adolescents: a scoping review. Int Rev Psych. (2020) 32:235–53. doi: 10.1080/09540261.2020.1720623
54. Valkenburg PM, Meier A, Beyens I. Social media use and its impact on adolescent mental health: an umbrella review of the evidence. Curr Opin Psychol. (2022) 44:58–68. doi: 10.1016/j.copsyc.2021.08.017
55. Ivie EJ, Pettitt A, Moses LJ, Allen NB. A meta-analysis of the association between adolescent social media use and depressive symptoms. J Affect Disord. (2020) 275:165–74. doi: 10.1016/j.jad.2020.06.014
56. Fisher BW, Gardella JH, Teurbe-Tolon AR. Peer cybervictimization among adolescents and the associated internalizing and externalizing problems: a meta-analysis. J Youth Adoles. (2016) 45:1727–43. doi: 10.1007/s10964-016-0541-z
57. Hartanto A, Quek FYX, Tng GYQ, Yong JC. Does social media use increase depressive symptoms? A reverse causation perspective. Front Psych. (2021) 12. doi: 10.3389/fpsyt.2021.641934
58. Herring SC, Kapidzic S. Teens, gender, and self-presentation in social media. In:Wright J, editor. International Encyclopedia of Social and Behavioral Sciences. 2 ed. Amsterdam: Elsevier. (2015). p. 146–52.
59. Wang R, Bianchi SM, Raley SB. Teenagers' internet use and family rules: a research note. J Marriage Fam. (2005) 67:1249–58. doi: 10.1111/j.1741-3737.2005.00214.x
60. Hjetland GJ, Schønning V, Hella RT, Veseth M, Skogen JC. How do Norwegian adolescents experience the role of social media in relation to mental health and well-being: a qualitative study. BMC Psychol. (2021) 9:78. doi: 10.1186/s40359-021-00582-x
61. Primack BA, Bisbey MA, Shensa A, Bowman ND, Karim SA, Knight JM, et al. The association between valence of social media experiences and depressive symptoms. Depress Anx. (2018) 35:784–94. doi: 10.1002/da.22779
62. Bandura A, Caprara GV, Barbaranelli C, Gerbino M, Pastorelli C. Role of affective self-regulatory efficacy in diverse spheres of psychosocial functioning. Child Dev. (2003) 74:769–82. doi: 10.1111/1467-8624.00567
Keywords: adolescents, depressive symptoms, general self-efficacy, nationwide study, social media
Citation: Bonsaksen T, Steigen AM, Stea TH, Kleppang AL, Lien L and Leonhardt M (2023) Negative social media-related experiences and lower general self-efficacy are associated with depressive symptoms in adolescents. Front. Public Health 10:1037375. doi: 10.3389/fpubh.2022.1037375
Received: 05 September 2022; Accepted: 14 December 2022;
Published: 06 January 2023.
Edited by:
Chao Guo, Peking University, ChinaReviewed by:
Mohammad Rahim Kamaluddin, The National University of Malaysia, MalaysiaSeren Yenikent, Symanto Research, Germany
Xiangyu Tao, Fordham University, United States
Copyright © 2023 Bonsaksen, Steigen, Stea, Kleppang, Lien and Leonhardt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anne Mari Steigen,  YW5uZS5zdGVpZ2VuQGlubi5ubw==
YW5uZS5zdGVpZ2VuQGlubi5ubw==