 Liangwen Ning
Liangwen Ning Huanhuan Jia2
Huanhuan Jia2 Xihe Yu
Xihe Yu- 1School of Public Administration, Jilin University, Changchun, China
- 2School of Public Health, Jilin University, Changchun, China
Background: The prolonged COVID-19 pandemic has seriously impacted the mental health of healthcare workers. This study aimed to explore the mental health status of healthcare workers, compare the differences in mental health between physicians and nurses, and verify the impact of risk perception on mental health in the long-term COVID-19 pandemic in Jilin Province, China.
Methods: A stratified random sample was used to conduct an on-site questionnaire survey in December 2020 to measure the mental health status, risk perceptions, and demographic characteristics of healthcare workers in Jilin Province, China. A total of 3,383 participants completed the questionnaire survey, of which 3,373 were valid questionnaires.
Results: A total of 23.6% (n = 795) of participants had symptoms of depression, 27.4% (n = 923) had symptoms of anxiety, and 16.3% (n = 551) had symptoms of stress. Physicians reported significantly higher rates of depression and anxiety than nurses (p = 0.023, p = 0.013, respectively). There was no significant difference in the proportion of participants with stress between physicians and nurses (p = 0.474). Multivariate logistic regression results showed that healthcare workers who had a high level of risk perception were more likely to have symptoms of depression (AOR = 4.12, p < 0.001), anxiety (AOR = 3.68, p < 0.001), and stress (AOR = 4.45, p < 0.001) after controlling for other variables.
Conclusion: At least one in six healthcare workers experienced mental health problems, and physicians were more likely than nurses to suffer from depression during the prolonged COVID-19 epidemic. Risk perception was highly predictive of depression, anxiety, and stress symptoms in medical staff. Public health interventions are needed to mitigate the long-term psychological impact of the COVID-19 pandemic.
Introduction
The outbreak of the COVID-19 pandemic in early 2020 continues to threaten societies all over the world and has had a major impact on health systems (1). The World Health Organization (WHO) declared the COVID-19 pandemic a Public Health Emergency of international concern in January 2020 (2), and researchers generally agreed that the outbreak of COVID-19 is likely to be the worst pandemic since the 1918 influenza pandemic (3). COVID-19 continues to spread internationally, with the totals for infections and deaths rising. How governments and communities around the world have responded to the COVID-19 pandemic has varied widely (4). Studies have shown that the pandemic is still an ongoing major public health challenge (5).
The mental health status of health professionals has attracted much attention during the COVID-19 pandemic. Previous studies have demonstrated that COVID-19 has introduced a global macrostressor that has a major negative influence on the mental health of populations worldwide (6), and many studies have shown that the impact of COVID-19 on the mental health of medical staff has been more severe than that of the general public (7). Scientific evidence has revealed that healthcare workers, especially those on the front-line of the epidemic, have endured enormous psychological pressure during the COVID-19 pandemic because of increased workload, the risk of exposure to COVID-19, fatigue, burnout, stigma, etc. (8). In addition, the risk effect has been amplified due to extensive media coverage that may increase the perception of risk among medical staff. The perceived and actual need for healthcare workers to go to the front lines of the epidemic to support prevention efforts, resulting in a break in the routine work style, may further increase their mental health burdens (9). A study conducted in the UK and the US found that front-line healthcare workers had increased risk of contracting COVID-19 compared to the general populations (10). Previous studies have observed fatigue, decreased cognitive function and job performance, stress, crying, suicidal intention and other problems (11, 12). Lai et al.'s survey of healthcare workers during the outbreak in Wuhan showed that the proportions of respondents reporting symptoms of depression, anxiety, insomnia, and suffering were 50.4, 44.6, 34.0, and 71.5%, respectively (13). Female nurses on the front-lines working in Wuhan, China, reported more severe measures of all mental health symptoms than other healthcare workers. The negative impact on healthcare workers does not only affect the prevention and control of COVID-19 but may also lead to other serious consequences, such as lower morale of healthcare workers, lower job satisfaction, higher absenteeism, and lower quality of medical services or treatment (14, 15). The psychological problems of healthcare workers in the context of a pandemic have become a focus of attention for scholars and health departments, and the protection against psychological problems in healthcare workers during a pandemic has become an important issue.
Few studies have looked at the long-term effects of infectious diseases on the mental health of health care workers, but the results have been inconsistent. Wu et al. found that usual ward nurses were more prone to burnout during the epidemic than frontline nurses, suggesting the need to pay attention to medical staff who deal with COVID-19 daily during this crisis (16). Similarly, Lee et al. found a significant increase in mental health problems among healthcare workers a year after the SARS outbreak (17). The longitudinal study by Cai et al. of Chinese medical personnel showed that depression, anxiety, and posttraumatic stress disorder symptoms were significantly higher during the outbreak than during the stabilization of the outbreak (18). However, Zhou's longitudinal study of healthcare workers on emergency medical assistance teams supporting Hubei Province found that healthcare workers were in a worse mental state after returning to their hometown (19). The results from another year-long longitudinal study of health workers in emergency departments in Singapore by Th'ng et al. showed significant improvement in anxiety symptoms and a significant increase in depressive symptoms 1 year after the outbreak (20).
Several studies have focused on differences in psychological problems between physicians and nurses during the COVID-19 pandemic, and most of these findings suggest that nurses are prone to more severe mental health problems during the current outbreak (21–23). A study of Belgian health professionals found that 63.2% of nurses reported symptoms of anxiety compared to 23.5% of doctors (24). However, a few studies reflect inconsistent findings. A cross-sectional survey conducted by Wang and colleagues in four hospitals in Guangdong Province, China, showed that physicians were more likely to suffer from moderate or severe depression than nurses (25). A longitudinal study in Singapore showed an increased prevalence of depression among a population of physicians in emergency departments in 2021 compared with a year earlier, and also showed higher total depression scores in this population than nursing staff (20). A comprehensive understanding of the vulnerability of healthcare workers' mental health in the context of the COVID-19 pandemic is critical for the development of relevant preventative and social policies during a pandemic. It is necessary to continue to compare the differences in mental health issues between physician and nurse populations during the prolonged COVID-19 pandemic.
According to cognitive assessment theory, risk perception can be considered a form of threat assessment and thus a determinant of mental health responses (26). According to the psychometric paradigm of Slovic, risk perception has two dimensions, “fear” and “unknown”(27), which are exacerbated in healthcare workers by the prevalence of COVID-19. A large body of previous research from psychology, clinical medicine, and economics suggests that risk perceptions often drive emotional and psychological distress (28). Several studies have assessed risk perceptions associated with COVID-19 and mental health. Ding et al. found that risk perceptions of COVID-19 were associated with levels of depression (29). Teufel et al. observed similar levels of risk perception and levels of COVID-19-related fear, depression, and generalized anxiety (30). However, while some studies have suggested an association between risk perception and mental health, others have questioned whether this association can be attributed to differences in sample selection, methodology, and social context between studies (31). In addition, previous studies mainly focused on the general public, and paid little attention to the association between risk perception and mental health among medical staff. Therefore, there is a need to further explore the relationship between risk perceptions and mental health among medical staff during the prolonged COVID-19 epidemic.
The Joint WHO-China 2019 report on the Coronavirus Disease Mission from February 16 to 24, 2020, suggests that China has begun to return to normal (32). According to statistics from the National Health Commission of China (33), Jilin Province had new cases in February, May, and July following the first confirmed cases announced on January 22, 2020. The number of confirmed cases in July reached 138, the highest in the whole year. Subsequently, the epidemic crisis in Jilin Province ended and there were no further outbreaks by the end of the year. Despite the absence of new cases in Jilin Province during this period, there are still clusters or scattered outbreaks of cases in other Chinese provinces and cities as well as globally. Jilin Province continues to face potential threats and pressures, and healthcare workers remain in a highly stressful state of risk preparedness. Therefore, we conducted a study during the regular prevention and control of the COVID-19 epidemic in Jilin Province to achieve three research objectives: (1) investigating the prevalence of the mental health among healthcare workers, (2) comparing the differences in mental health between physicians and nurses in China, and (3) exploring the impact of risk perception on mental health.
Materials and methods
Design and sample
Most data collection efforts on healthcare workers' mental health used online surveys to obtain samples, because of the COVID-19 pandemic. Despite the strengths of flexibility, speed, timeliness, convenience, etc., online surveys still have unavoidable weaknesses, such as sample selection bias, and low implementation and response rates, which may have some effect on sample representativeness (34). This study conducted an on-site cross-sectional survey of medical staff in public hospitals in Jilin Province from December 1 to December 30, 2020. First, a stratified sampling method was used to divide all public hospitals in Jilin Province into municipal public hospitals and county public hospitals. Since urban public hospitals are more clustered, 25% of public hospitals were randomly selected according to their region, type, and level. Since counties are more dispersed and public hospitals at the county level are more heterogeneous, one public general hospital and one public TCM hospital were randomly selected in each county. Ultimately, 29 municipal public hospitals and 80 county-level public hospitals were included in the study sample. Then, 20 doctors and 10 nurses were selected from each hospital for the on-site survey using a quota sampling method. The criteria for inclusion in this study were: in-service physicians and nurses between 18 and 60, were able to complete the questionnaire on their own and agreed to participate in the study. The exclusion criteria for participants were: physicians and nurses who were on leave during the period of investigation; did not want to participate in the study and were supporting other regions due to the COVID-19 pandemic.
Sample size
We used PASS 15 to estimate the study sample. we calculated a sample size value of 2449, assuming that the 50% of healthcare workers have mental health problems and setting the confidence level at 95% and the margin of error at 2%. Considering the non-response rate and missing values, the final sample size was inflated by 20% to be 3061.
Data collection
Our study was approved by the Medical Ethics Committee of Jilin University and IRB code is No. 2019-12-03. The purpose and protocol of the study were clearly explained by the investigator at the beginning of the survey. Participants had to agree to the study statement before starting the questionnaire. In total, 3,383 people participated the questionnaire. The collected questionnaires were verified and 10 questionnaires with logical errors were excluded, resulting in a valid sample size of 3373 (99.7% of the returned questionnaires) for inclusion in the study.
Measurement
Demographic variables
The demographic variables in this study included hospital location, gender, age, marital status, education level, department, professional title, working years, average monthly income, and whether or not they were exposed to COVID-19 positive patients. Previous studies suggest an association between demographic variables and mental health in the COVID-19 epidemic.
Risk perception
Risk perception was measured with a scale based on a previous study during the SARS outbreak in 2003 to measure healthcare workers' threat perception of COVID-19-related risks (35). The scale consists of 10 items such as “I believed that my job poses a great risk to me” which were rated on a 5-point Likert scale (1 = completely disagree and 5 = completely agree). The language of Risk Perception Scale is Chinese and the results of reliability and validity analysis show that the risk perception scale had good reliability (Cronbach's = 0.870) and validity (RMSEA = 0.985, GFI = 0.986, TLI = 0.957). The average score of all items above 3 was deemed high in risk perception.
Mental health
We measured depression, anxiety and stress to assess the mental health of medical staff during the COVID-19 epidemic. Depression is a condition characterized by a sad mood, low self-esteem, apathy, and when severe, suicidal impulses; while anxiety often manifests itself as excessive worry, hypervigilance; symptoms of stress are usually associated with excitement or tension as a result of a lack of coping strategies (36).
The Chinese version of the Depression Anxiety and Stress Scale (DASS-21 scale) was used in this study to assess the prevalence of depression, anxiety, and stress among healthcare workers in China. The DASS-21 scale was originally developed by Lovibond (36), and Gong developed a Chinese version of the scale based on it (37). The scale has been used in several studies in China during the COVID-19 epidemic (38, 39). In this study, the Cronbach's α of the total DASS-21 scale was 0.971, indicating that the scale has good reliability. The results of the confirmatory factor analysis indicated that the scales had good validity (CFI = 0.984, TLI = 0.976, RMSEA = 0.049).
The scale contains 3 subscales, and each subscale comprises seven items covering depression, anxiety, and stress. Items on the depression scale assess symptoms of dysphoric mood, and example items include “I could not seem to experience any positive feeling at all.” Items on the anxiety scale measure symptoms pertaining to physiological hyperarousal, such as “I was aware of dryness of my mouth.” Items on the stress scale evaluate negative affectivity, such as, “I found it hard to wind down.” A 4-point Likert scale was used for all responses (0 = never a problem, 1 = sometimes a problem, 2 = often a problem, and 3 = almost always a problem).
We multiplied each score by two for comparison with the original 42 items of the DASS scale (40). The total score of each dimension was categorized as “normal,” “mild,” “moderate,” “severe,” and “extremely severe,” according to the DASS manual. On the depression scale, 0–9 indicates normal depression, 10–13 indicates mild depression, 14–20 indicates moderate depression, 21–27 indicates severe depression and 28–42 indicates extremely severe depression. On the anxiety scale, 0–7 indicates normal, 8–9 indicates considered mild anxiety, 10–14 indicates moderate anxiety, 15–19 indicates severe anxiety and 20–42 indicates extremely severe anxiety. On the stress scale, 0–14 indicates normal, 15–18 indicates mild stress, 19–25 indicates moderate stress, 26–33 indicates severe stress and 34–42 indicates extremely severe stress. Participants who fell into the “mild” or higher category were identified as experiencing symptoms of depression, anxiety, or stress.
Statistical analysis
Our study described the characteristics of the study participants by frequency analysis. The mean and standard deviation (SD) of the scores for each risk perception entry were calculated, and the physician and nurse groups were compared using independent t-test. A chi-square test was used to test for differences in the prevalence of depression, anxiety, and stress symptoms between the physician and nurse groups.
Participants were divided into two groups: those who suffered from symptoms of depression, anxiety, or stress, and those who did not. A chi-square test was used to compare significant differences between different demographic characteristics and depression, anxiety, and stress. Three logistic regression models were developed to identify predictors of depression, anxiety, and stress symptoms. Variables related to sociodemographic characteristics, work-related variables, and risk perception variables were entered into the regression models. To test the robustness of the results of the logistic regression model, we developed a linear regression model that treated depression, anxiety, and stress symptom scores as a continuous variable (Supplementary material).
IBM SPSS Statistics 25 programs were used for statistical analysis.
Results
Demographic characteristics of respondents
As shown in Table 1, 63.7% of the sample were doctors, and 36.3% were nurses in total. Most of the respondents were female (69.8%), 31–45 years old (52.9%), married (79.8%), had a bachelor's degree (61.2%), had a junior or not-professional rank (44.4%), had <10 years of work experience (45.3%) and had a monthly income of 5,000 yuan or less (63.3%).
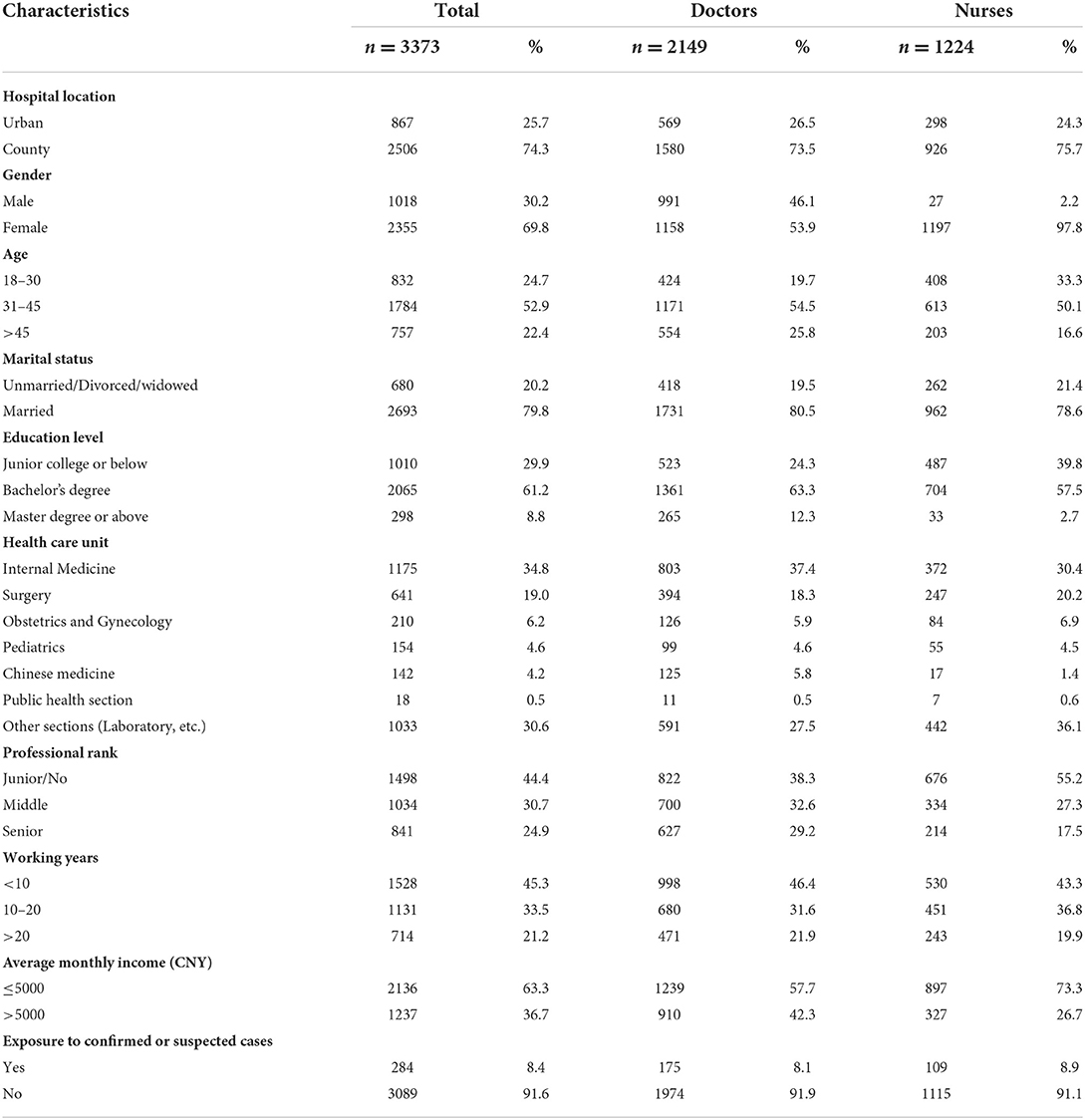
Table 1. Sociodemographic characteristics of study participants.
Prevalence of depression, anxiety, and stress symptoms in the sample
Table 2 demonstrates the percentages of healthcare workers who experienced various levels of symptoms of depression, anxiety, and stress. In total, 23.6% (n = 795) of the respondents had symptoms of depression, 27.4% (n = 923) of participants had symptoms of anxiety, 16.3% (n = 551) of participants had symptom of stress.
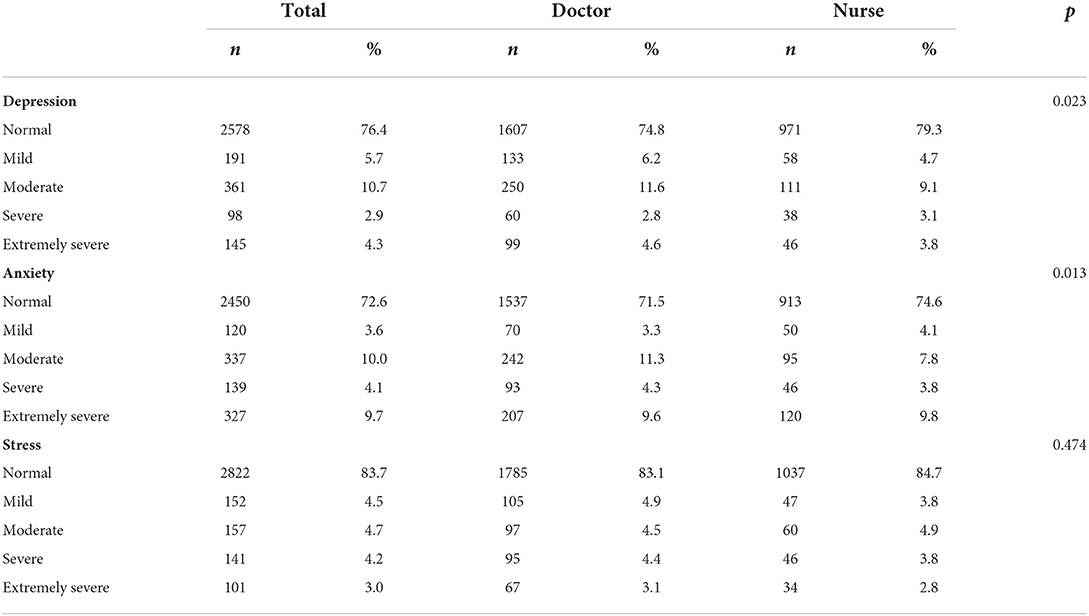
Table 2. Prevalence of depression, anxiety and stress symptoms in the sample.
In addition, Table 2 also shows statistically significant differences in the proportions of different levels of depression and anxiety symptoms between the doctors and nurse groups, with significantly more physicians reporting depression and anxiety than nurses (p = 0.023, p = 0.013, respectively). There was no significant difference in the proportion of participants with stress between doctors and nurses (p = 0.474).
Risk perception of respondents
Table 3 shows the risk perception scores of the healthcare workers. On the risk perception sections of the survey, a total of 596 (17.7%) respondents gave a rating higher than 3 out of a possible score of 5. A total of 379 (17.6%) doctors had a high level of risk perception about COVID-19, and 217 (17.7%) nurses had a high level of risk perception. No significant differences were found for perceived risk between doctors and nurses (p = 0.946).
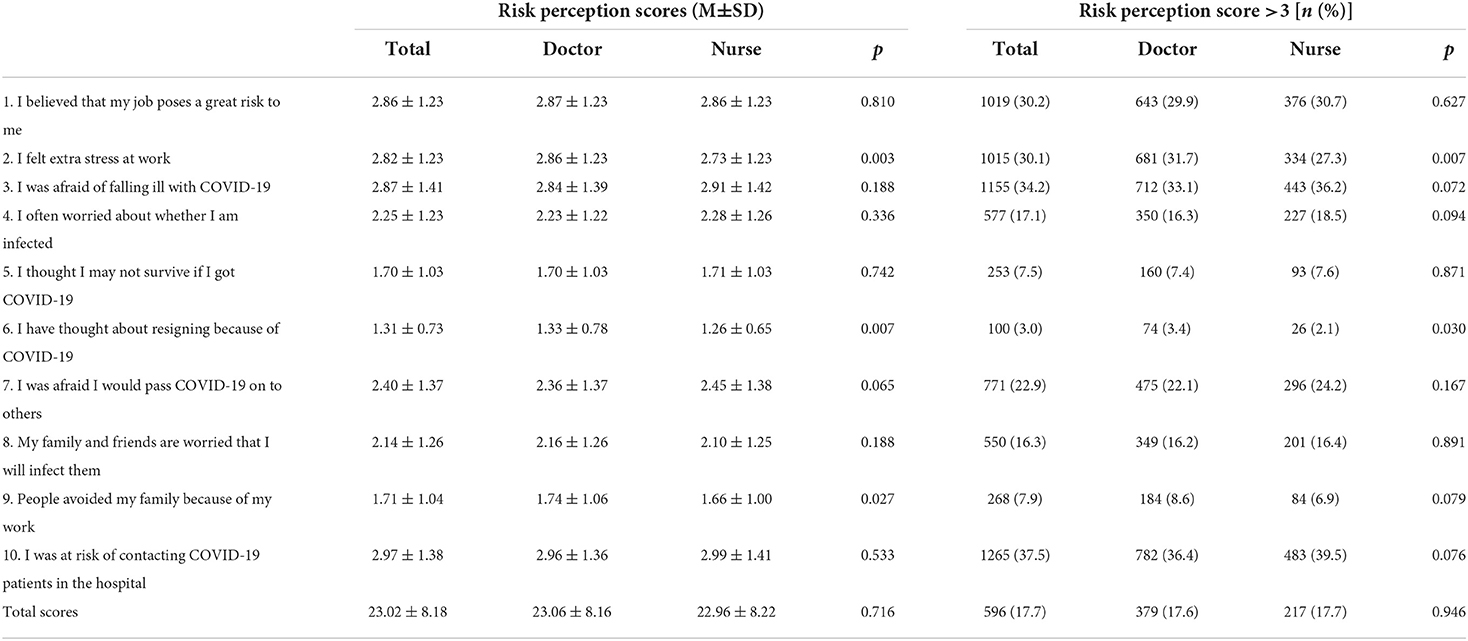
Table 3. Risk perception of respondents.
Univariate analysis of symptoms of depression, anxiety, and stress
As shown in Table 4, univariate analysis demonstrated that hospital location, education level, professional rank, career category, risk perception, and exposure to COVID-19 cases were significantly associated with symptoms of depression (p < 0.05); hospital location, health care unit, risk perception, and exposure to COVID-19 cases were significantly associated with symptoms of anxiety (p < 0.05); and gender, risk perception, and exposure to COVID-19 cases were significantly associated with symptoms of stress (p < 0.05).
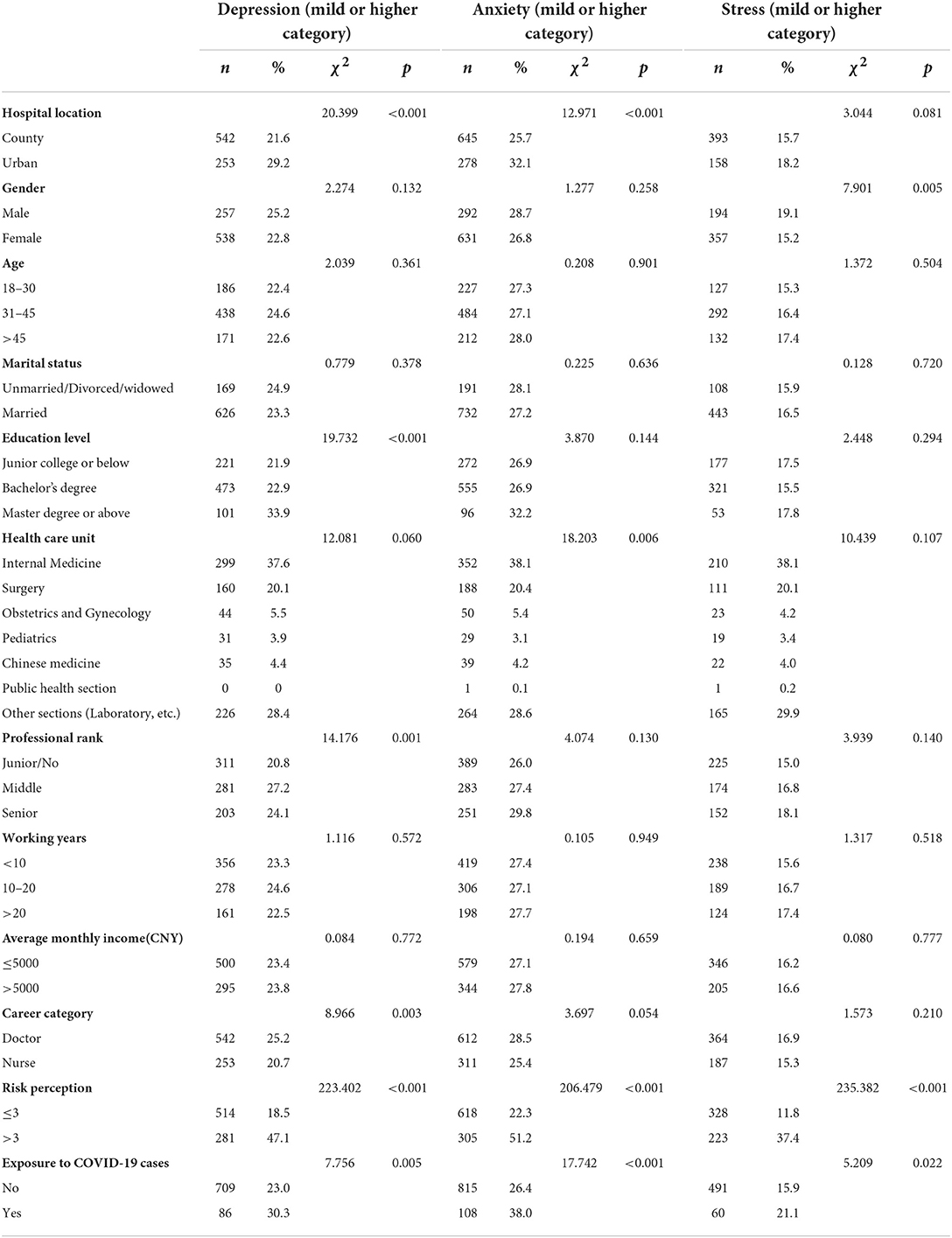
Table 4. Univariate analysis of symptom of depression, anxiety, and stress.
Factors associated with symptoms of depression, anxiety, and stress
The results of correlation analysis and VIF showed that there was no multicollinearity between the independent variables (Supplementary material).
Multivariate logistic regression results as shown in Table 5 revealed that healthcare workers in urban public hospitals (AOR = 1.41, P = 0.001), those with a master's degree or higher (AOR = 1.56, P = 0.012), those with a mid-level rank (AOR = 1.43, P = 0.003), and those with high-risk perceptions (AOR = 4.12, P < 0.001) were more likely to suffer from depression. Nurses (AOR = 0.80, P = 0.037) were less likely to develop depression than physicians; healthcare workers in urban public hospitals (AOR = 1.35, P = 0.002), those with high-risk perception (AOR = 3.68, P < 0.001), and those in contact with COVID-19 patients (AOR = 1.53, P = 0.002) were more likely to have anxiety disorders; healthcare workers in urban public hospitals (AOR = 1.26, P = 0.048), those with high-risk perceptions (AOR = 4.45, P < 0.001) were more likely to suffer from stress, while women (AOR = 0.75, P = 0.021) were less likely to suffer from stress than men.
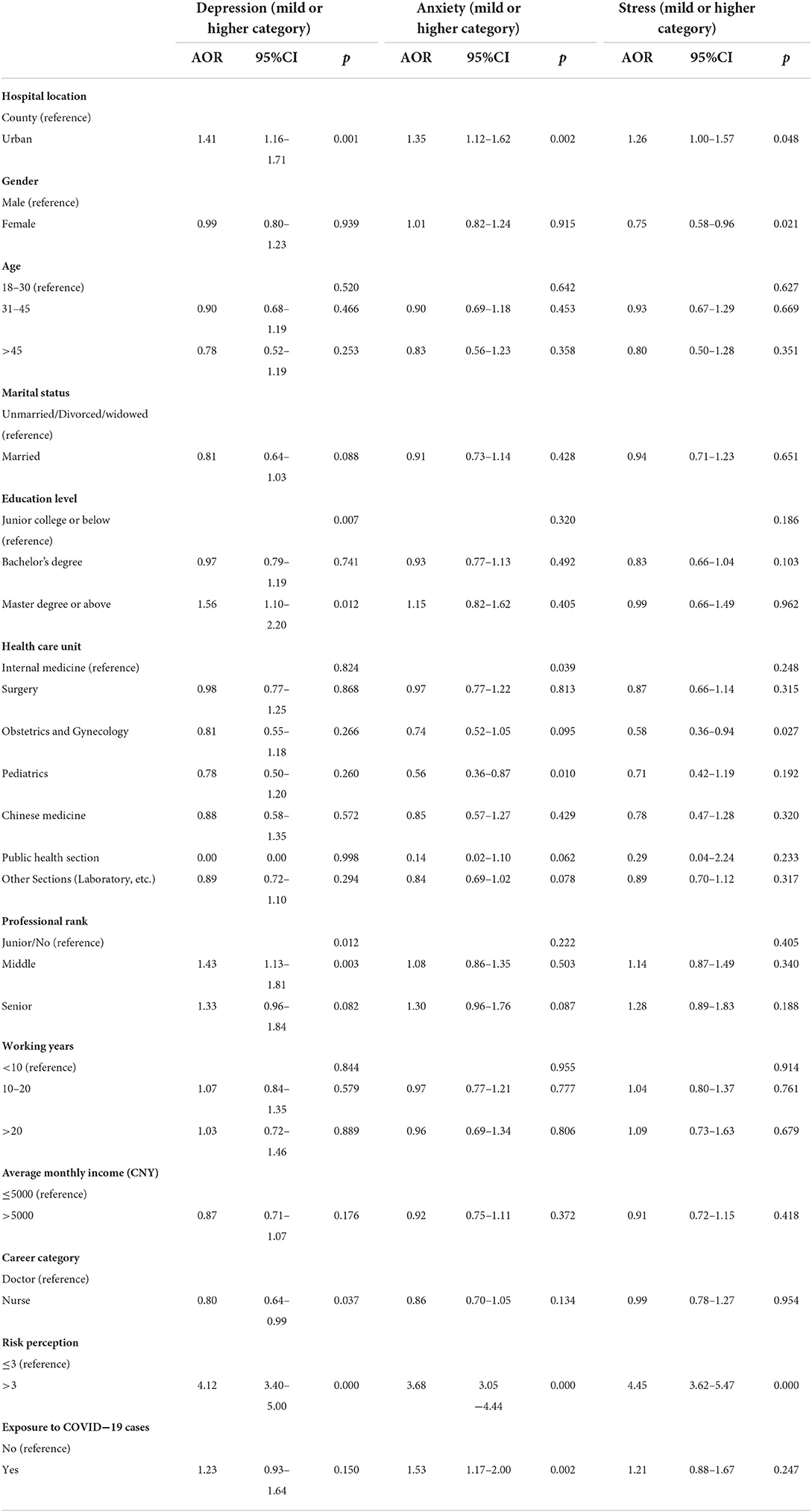
Table 5. Factors associated with symptom of depression, anxiety, and stress.
Discussion
The purpose of this study was to assess the mental health problem among physicians and nurses in Jilin Province, China, during a period of regular COVID-19 epidemic prevention and control. The COVID-19 epidemic in China was sporadically distributed across several regions, while Jilin Province had no confirmed COVID-19 cases or deaths for seven consecutive months, indicating a relatively stable epidemic situation in the region during the investigation. There is substantial evidence in the previous literature that healthcare workers may have a considerable burden of psychological distress during an outbreak, which has a significant impact on their mental health, outbreak prevention and control efforts, and healthcare decisions (10, 41).
Our study showed that the estimated prevalence rates of depression, anxiety, and stress symptoms were 23.6, 27.4, and 16.3%, respectively, in the population as a whole. A study conducted by Teris Cheung in 2015 on nurses in Hong Kong, China, showed that 35.8% of participants had a prevalence of depression, 37.3% had symptoms of anxiety and 41.1% had symptoms of stress. In their study, the results of depression, anxiety and stress were all higher than those in our study (42). In addition, the level of emotional distress among healthcare workers was lower in our study compared to an early 2020 study (13, 43). The first month of the COVID-19 study conducted by Benedetta Demartini in Italy showed that 41.5% of the population experienced pathological depression, 38.2% experienced anxiety, and 48% experienced stress (43). The results study conducted in Wuhan, China in early 2020 were 50.4% for depression, 44.6% for anxiety, and 71.5% for stress (13). However, the results of the present study differ from those of previous studies following infectious disease epidemics. Lee et al.'s study showed that SARS survivors exhibited worrying levels of psychological stress 1 year after the SARS outbreak, manifesting alarmingly high levels of depression, anxiety, and posttraumatic symptoms, as well as high rates of potential cases of psychiatric disorders (17). Lee suggests that the results may be related to concerns about the complications of SARS and its treatment, economic issues or stigma. We suggest that the results of this study may be related to the stage of development of the COVID-19 epidemic. The gradual control of the epidemic with appropriate government intervention and the reduction of patients could improve the psychological state by reducing the stress of security threats to medical personnel (44). In addition, adequate protective equipment and experience in prevention and control may also contribute to the psychological relief of health care workers.
We found that the prevalence of depression and anxiety was significantly higher in the physician population than in the nurse population in Jilin Province in the context of a seven-month period with no new cases of Covid-19 during normative prevention and control (depression, 25.2% for physicians vs. 20.7% for nurses; anxiety, 28.5% for physicians vs. 25.4% for nurses, p < 0.05), which differs from the results of many other previous related studies (21–23). Some studies suggest that the nature of nurses' work, which requires them to be in close contact with patients and to work longer hours, can lead to more severe mental health problems (13, 22, 23). However, some studies show similarities to our results. In other studies, increased mental health symptoms amongst physicians were attributed to burnout caused by the dual stress of the physician population needing to assess and diagnose patients and the stress of COVID-19 infection. Burnout is a state of physical and mental exhaustion that occurs as a result of being in an emotionally demanding work environment for a long period (45). Maslach et al. described burnout as a three-dimensional syndrome consisting of emotional exhaustion, personal depersonalization, and reduced personal accomplishment (46). Numerous previous studies have confirmed the correlation between burnout and depressive symptoms in medical professionals (47). The results of a survey conducted during the Spanish outbreak showed that physicians experienced higher levels of burnout than nurses, possibly related to the added stress on physicians in a crisis needing to make quick, correct decisions amongst unknown factors (48). This is supported by our study's finding that medical professionals with master's degrees or higher and mid-level titles were more likely to experience depressive symptoms. This is likely because related studies have shown that education and job title have an impact on burnout among healthcare workers (49, 50).
The multivariate logistic regression results of this study showed that risk perception was a significant factor that influenced depression, anxiety, and stress in healthcare workers and that healthcare workers with high-risk perception were 3–4 times more likely to suffer from depression, anxiety, and stress than those with low-risk perception. Previous studies have also found a strong correlation between perceived risk and emotional distress in the context of COVID-19, which is consistent with other studies during the pandemic. According to Slovic's psychometric paradigm, there are two main dimensions of risk perception: “fear” and “unknown” (27). The occurrence of a public health emergency is likely to stimulate these two psychological dimensions in people; the perception of risk drives emotional reactions and psychological distress. According to social stress theory, the threat of COVID-19 may trigger significant stress in groups, leading to high levels of risk perception, which may lead to mental health problems (51). In addition, studies have shown that individuals' subjective perceptions of risk may not be consistent with the objective situation. Therefore, it is necessary to focus on the subjective risk perceptions of medical personnel regarding COVID-19 infection during the stabilization of the epidemic, and guide them to maintain a correct and positive subjective perception of the risk of COVID-19 infection, thereby alleviating emotional distress and improving mental health problems of medical personnel.
One interesting observation from our study is that although exposure to COVID-19 patients was associated with depression, anxiety, and stress in the univariate analysis, medical staff exposed to newly diagnosed patients were more likely to suffer from anxiety after controlling for other variable interference, while depression and stress did not demonstrate significant differences, which may be related to the long period without new cases in Jilin Province during the survey period, while the national epidemic continued to emerge. We also found that health professionals with a master's degree or higher were more likely to suffer from depression, which is inconsistent with other results (52) and may be related to the fact that those with higher education among health professionals tend to take on heavier workloads and decision-making tasks. In addition, consistent with other studies, we found that medical staff in urban public hospitals were more likely to suffer from depression and anxiety symptoms, which may be related to the higher workload of urban medical staff compared to county medical staff and the higher number of anti-epidemic tasks supporting other provinces with epidemics. In contrast to previous studies, our study found that men were more likely to suffer from stress symptoms than women, which may be related to the fact that the Chinese physician population is predominantly male.
This study has some limitations. First, because this study used a cross-sectional design, no inferences can be made about the causal relationships of the variables. Second, some healthcare workers supported other cities during the survey, which may have led to some bias in the sampling. Third, due to the large variation in the number of healthcare workers between hospitals, we used the quota sampling method. However, it is non-probability sampling and has limitations in terms of sample representativeness. Fourth, according to Jilin Statistical Yearbook (2021), a total of 212,140 health technical personnel and 3,066,700 hospital admissions in Jilin Province in 2020. The ratio is 0.069. Previous studies have mentioned shortage of health human resources as a cause of increased stress and mental health problems during the COVID-19 pandemic and an exploration of the shortage of human resources for health is lacking in our study. Future studies may need to consider further research on the mental health of healthcare workers in prolonged epidemics through longitudinal studies, probability sampling methods and consideration of human resources for health issues.
Conclusion
Compared with those reported during the early outbreak of COVID-19 in the early 2020s, mental health problems among healthcare workers were lower in a stable prevention-and-control situation and corroborated converged recent national and international studies. Physicians were more likely to suffer from depression than nurses. Risk perception was highly predictive of depression, anxiety, and stress symptoms among medical personnel.
Data availability statement
The datasets presented in this article are not readily available because the datasets are currently used for another project, but are available from the corresponding author on reasonable request. Requests to access the datasets should be directed to XY, eGh5dUBqbHUuZWR1LmNu.
Author contributions
Conceptualization: XY and LN. Methodology: HJ and LN. Formal analysis and investigation: SG, PS, and PC. Writing—original draft preparation: LN. Writing—review and editing: JY and HJ. Funding acquisition and supervision: XY. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1030808/full#supplementary-material
References
1. Been JV, Ochoa LB, Bertens LCM, Schoenmakers S, Steegers EAP, Reiss EKM. Impact of COVID-19 mitigation measures on the incidence of preterm birth: a national quasi-experimental study. Lancet Public Health. (2020) 5:E604–11. doi: 10.1016/S2468-2667(20)30223-1
2. WHO. WHO Director-General's opening remarks at the media briefing on COVID-19–11 March 2020. (2020). Available online at: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 (accessed March 11, 2020).
3. Oliveira JF, Jorge DCP, Veiga RV, Rodrigues MS, Torquato MF, da Silva NB., et al. Mathematical modeling of COVID-19 in 148 million individuals in Bahia, Brazil. Nat Commun. (2021) 12:333. doi: 10.1038/s41467-020-19798-3
4. Aknin LB, Andretti B, Goldszmidt R, Helliwell JF, Petherick A, De Neve JE, et al. Policy stringency and mental health during the COVID-19 pandemic: a longitudinal analysis of data from 15 countries. Lancet Public Health. (2022) 7:e417–26. doi: 10.1016/S2468-2667(22)00060-3
5. Yu L, Wang J, Li X, Mao L, Sui Y, Chen W, et al. Simultaneous detection of SARS-CoV-2 and pandemic (H1N1) 2009 virus with real-time isothermal platform. Heliyon. (2021) 7:e07584. doi: 10.1016/j.heliyon.2021.e07584
6. Dlugosz P, Kryvachuk L. Neurotic generation of Covid-19 in Eastern Europe. Front Psychiatry. (2021) 12:654590. doi: 10.3389/fpsyt.2021.654590
7. Zhang WR, Wang K, Yin L, Zhao WF, Xue Q, Peng M, et al. Mental health and psychosocial problems of medical health workers during the COVID-19 Epidemic in China. Psychother Psychosom. (2020) 89:242–50. doi: 10.1159/000507639
8. Tsamakis K, Tsiptsios D, Ouranidis A, Mueller C, Schizas D, Terniotis C, et al. COVID-19 and its consequences on mental health (Review). Exp Ther Med. (2021) 21:1. doi: 10.3892/etm.2021.9675
9. De Kock JH, Latham HA, Leslie SJ, Grindle M, Munoz SA, Ellis L, et al. Rapid review of the impact of COVID-19 on the mental health of healthcare workers: implications for supporting psychological well-being. BMC Public Health. (2021) 21:104. doi: 10.1186/s12889-020-10070-3
10. Nguyen LH, Drew DA, Graham MS, Joshi AD, Guo CG, Ma WJ, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. (2020) 5:E475–83. doi: 10.1016/S2468-2667(20)30164-X
11. Shen X, Zou X, Zhong X, Yan J, Li L. Psychological stress of ICU nurses in the time of COVID-19. Crit Care. (2020) 24:200. doi: 10.1186/s13054-020-02926-2
12. Sun P, Wang M, Song T, Wu Y, Luo J, Chen L, et al. The Psychological impact of COVID-19 pandemic on health care workers: a systematic review and meta-analysis. Front Psychol. (2021) 12:626547. doi: 10.3389/fpsyg.2021.626547
13. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. (2020) 3:e203976. doi: 10.1001/jamanetworkopen.2020.3976
14. Brooks SK, Dunn R, Amlot R, Rubin GJ, Greenberg N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J Occup Environ Med. (2018) 60:248–57. doi: 10.1097/JOM.0000000000001235
15. Brooks SK, Gerada C, Chalder T. Review of literature on the mental health of doctors: are specialist services needed? J Ment Health. (2011) 20:146–56. doi: 10.3109/09638237.2010.541300
16. Wu Y, Wang J, Luo C, Hu S, Lin X, Anderson AE, et al. Comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J Pain Symptom Manage. (2020) 60:e60–5. doi: 10.1016/j.jpainsymman.2020.04.008
17. Lee AM, Wong JG, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. (2007) 52:233–40. doi: 10.1177/070674370705200405
18. Cai ZX, Cui Q, Liu ZC Li JJ, Gong X, Liu JF, et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J Psychiatr Res. (2020) 131:132–7. doi: 10.1016/j.jpsychires.2020.09.007
19. Zhou YF, Ding HL, Zhang YF, Zhang BY, Guo YR, Cheung T, et al. Prevalence of poor psychiatric status and sleep quality among frontline healthcare workers during and after the COVID-19 outbreak: a longitudinal study. Transl Psychiat. (2021) 11:1–6. doi: 10.1038/s41398-020-01190-w
20. Th'ng F, Rao KA, Ge LX, Mao D, Neo HN, De Molina JA, et al. A one-year longitudinal study: changes in depression and anxiety in frontline emergency department healthcare workers in the COVID-19 pandemic. Int J Env Res Pub He. (2021) 18:11228. doi: 10.3390/ijerph182111228
21. Shaukat N, Ali DM, Razzak J. Physical and mental health impacts of COVID-19 on healthcare workers: a scoping review. Int J Emerg Med. (2020) 13:1–8. doi: 10.1186/s12245-020-00299-5
22. Pappa S, Sakkas N, Sakka E. A year in review: sleep dysfunction and psychological distress in healthcare workers during the COVID-19 pandemic. Sleep Med. (2022) 91:237–45. doi: 10.1016/j.sleep.2021.07.009
23. Fteropoulli T, Kalavana TV, Yiallourou A, Karaiskakis M, Koliou Mazeri M, Vryonides S, et al. Beyond the physical risk: Psychosocial impact and coping in healthcare professionals during the COVID-19 pandemic. J Clin Nurs. (2021) 00:1–15. doi: 10.1111/jocn.15938
24. Tiete J, Guatteri M, Lachaux A, Matossian A, Hougardy JM, Loas G, et al. Mental health outcomes in healthcare workers in COVID-19 and non-COVID-19 care units: a cross-sectional survey in Belgium. Front Psychol. (2021) 11:612241. doi: 10.3389/fpsyg.2020.612241
25. Wang HJ, Huang DZ, Huang HG, Zhang JH, Guo L, Liu YT, et al. The psychological impact of COVID-19 pandemic on medical staff in Guangdong, China: a cross-sectional study. Psychol Med. (2022) 52:884–92. doi: 10.1017/S0033291720002561
26. Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongis A, Gruen RJ. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J Pers Soc Psychol. (1986) 50:992. doi: 10.1037/0022-3514.50.5.992
28. Loewenstein GF, Weber EU, Hsee CK, Welch N. Risk as feelings. Psychol Bull. (2001) 127:267–86. doi: 10.1037/0033-2909.127.2.267
29. Ding Y, Xu J, Huang S, Li P, Lu C, Xie S. Risk perception and depression in public health crises: evidence from the COVID-19 crisis in China. Int J Env Res Pub He. (2020) 17:5728. doi: 10.3390/ijerph17165728
30. Teufel M, Schweda A, Dörrie N, Musche V, Hetkamp M, Weismüller B, et al. Not all world leaders use Twitter in response to the COVID-19 pandemic: impact of the way of Angela Merkel on psychological distress, behaviour and risk perception. J Public Health. (2020) 42:644–6. doi: 10.1093/pubmed/fdaa060
31. Imai H, Okumiya K, Fukutomi E, Wada T, Ishimoto Y, Kimura Y, et al. Association between risk perception, subjective knowledge, and depression in community-dwelling elderly people in Japan. Psychiatry Res. (2015) 227:27–31. doi: 10.1016/j.psychres.2015.03.002
32. He M, Xian Y, Lv X, He J, Ren Y. Changes in body weight, physical activity, and lifestyle during the semi-lockdown period after the outbreak of COVID-19 in China: an online survey. Disaster Med Public Health Prep. (2020) 14:1–6. doi: 10.1017/dmp.2020.237
33. China NHCO. The latest updates on COVID-19 outbreaks. Available online at: http://www.nhc.gov.cn/xcs/yqtb/list_gzbd.shtml (accessed September, 2020).
34. Evans JR, Mathur A. The value of online surveys: a look back and a look ahead. Internet Res. (2018) 28:854–87. doi: 10.1108/IntR-03-2018-0089
35. Wu P, Fang YY, Guan ZQ, Fan B, Kong JH, Yao ZL, et al. The psychological impact of the SARS epidemic on hospital employees in china: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiat. (2009) 54:302–11. doi: 10.1177/070674370905400504
36. Lovibond PF, Lovibond SH. The structure of negative emotional states—comparison of the depression anxiety stress scales (dass) with the beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
37. Gong X, Xie XY, Xu R, Luo YJ. (2010). Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chinese J Clin Psychol. 443–6. doi: 10.16128/j.cnki.1005-3611.2010.04.020
38. Wang CY, Pan RY, Wan XY, Tan YL, Xu LK, McIntyre RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behavior Immun. (2020) 87:40–8. doi: 10.1016/j.bbi.2020.04.028
39. Du JF, Mayer G, Hummel S, Oetjen N, Gronewold N, Zafar A, et al. Mental health burden in different professions during the final stage of the COVID-19 lockdown in China: cross-sectional survey study. J Med Internet Res. (2020) 22:e24240. doi: 10.2196/24240
40. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales. Psychology Foundation of Australia (1996).
41. Gold JA. Covid-19: adverse mental health outcomes for healthcare workers. BMJ-Brit Med J. (2020) 5:369. doi: 10.1136/bmj.m1815
42. Cheung T, Yip PSF. Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Env Res Pub He. (2015) 12:11072–100. doi: 10.3390/ijerph120911072
43. Demartini B, Nistico V, D'Agostino A, Priori A, Gambini O. Early psychiatric impact of COVID-19 pandemic on the general population and healthcare workers in italy: a preliminary study. Front Psychiatry. (2020) 11:561345. doi: 10.3389/fpsyt.2020.561345
44. Wang LQ, Zhang M, Liu GM, Nan SY Li T, Xu L, Xue Y, et al. Psychological impact of coronavirus disease (2019) (COVID-19) epidemic on medical staff in different posts in China: a multicenter study. J Psychiatr Res. (2020) 129:198–205. doi: 10.1016/j.jpsychires.2020.07.008
45. Schaufeli WB, Greenglass ER. Introduction to special issue on burnout and health. Psychol Health. (2001) 16:501–10. doi: 10.1080/08870440108405523
46. Maslach C, Jackson SE. The measurement of experienced burnout. J Occup Behav. (1981) 2:99–113. doi: 10.1002/job.4030020205
47. Duarte I, Teixeira A, Castro L, Marina S, Ribeiro C, Jacome C, et al. Burnout among Portuguese healthcare workers during the COVID-19 pandemic. BMC Public Health. (2020) 20:1–10. doi: 10.1186/s12889-020-09980-z
48. Ruiz-Fernandez MD, Ramos-Pichardo JD, Ibanez-Masero O, Cabrera-Troya J, Carmona-Rega MI, Ortega-Galan AM. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J Clin Nurs. (2020) 29:4321–30. doi: 10.1111/jocn.15469
49. Cao Y, Gao L, Fan L, Jiao M, Li Y, Ma Y. The influence of emotional intelligence on job burnout of healthcare workers and mediating role of workplace violence: A cross sectional study. Front Public Health. (2022) 10:892421. doi: 10.3389/fpubh.2022.892421
50. Xu WC, Pan ZJ, Li Z, Lu S, Zhang L. Job burnout among primary healthcare workers in rural China: a multilevel analysis. Int J Env Res Pub He. (2020) 17:727. doi: 10.3390/ijerph17030727
51. Aneshensel CS. Social stress—theory and research. Annu Rev Sociol. (1992) 18:15–38. doi: 10.1146/annurev.so.18.080192.000311
Keywords: COVID-19, healthcare worker, mental health, DASS-21, cross-sectional survey
Citation: Ning L, Jia H, Yu J, Gao S, Shang P, Cao P and Yu X (2022) Mental health among healthcare workers during the prolonged COVID-19 pandemic: A cross-sectional survey in Jilin Province in China. Front. Public Health 10:1030808. doi: 10.3389/fpubh.2022.1030808
Received: 29 August 2022; Accepted: 30 September 2022;
Published: 17 October 2022.
Edited by:
Lawrence T. Lam, University of Technology Sydney, AustraliaReviewed by:
Susan Ka Yee Chow, Tung Wah College, Hong Kong, Hong Kong SAR, ChinaDavid C. N. Wong, Tung Wah College, Hong Kong, Hong Kong SAR, China
Copyright © 2022 Ning, Jia, Yu, Gao, Shang, Cao and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xihe Yu, eGh5dUBqbHUuZWR1LmNu