 Yu Xiao1,2*
Yu Xiao1,2* Ting-ting Chen3Shao-yi Zhu4Ling Zong5Na Du1Chun-ya Li1Hao-fei Cheng1
Ting-ting Chen3Shao-yi Zhu4Ling Zong5Na Du1Chun-ya Li1Hao-fei Cheng1 Qi Zhou6Li-shi Luo1Juan Jia1
Qi Zhou6Li-shi Luo1Juan Jia1- 1Psychosomatic Medical Center, The Fourth People's Hospital of Chengdu, Chengdu, China
- 2Psychosomatic Medical Center, The Clinical Hospital of Chengdu Brain Science Institute, MOE Key Lab for Neuroinformation, University of Electronic Science and Technology of China, Chengdu, China
- 3Nursing School, Chengdu University of Traditional Chinese Medicine, Chengdu, China
- 4Department of Psychiatry, Shantou University Mental Health Center, Shantou, China
- 5Department of Judicial Expertise, Zhongshan Third People's Hospital, Zhongshan, China
- 6Institute (College) of Integrative Medicine, Dalian Medical University, Dalian, China
Objectives: Patient-initiated hospital violence is a global problem which threatens the safety of health professionals and is indicative of doctor-patient tensions, impeding health system quality and access. The current study aimed to improve the understanding of medical workplace violence (WPV) in China, using authoritative and nationally representative judgment records, and to approach violence prevention strategies.
Methods: All litigation records relating to violence against health professionals between 2013 and 2021 were extracted from the China Judgment Online System. Basic case information, victim characteristics, perpetrator characteristics and the nature of the violence were collated. The relationship between different treatment outcomes and violence was also explored.
Results: Numbers of cases of hospital violence gradually increased from 2013 to a peak in 2016 before gradually decreasing in the following years. The most common perpetrators were patients' relatives (58.2%), followed by patients themselves (38.2%). Only 9 perpetrators had a confirmed history of mental illness and only two were intoxicated with alcohol. More than half of the cases (52.5%) occurred in rural areas and this percentage is even greater for primary health care institutions (71.4%) and secondary hospitals (73.5%). On a departmental level, the highest incidence of medical WPV was found in the emergency (18.9%), pediatrics (13.2%) and obstetrics (11.5%) departments. Violent behaviors, such as stalking, mass occupation of the ward and sharp instrument injury were significantly related to cases not involving patient death (p < 0.05). Disruptive behavior, such as hanging banners, blocking hospital passages, placing flower wreaths and burning paper money were significantly correlated with cases involving patient death (p < 0.01). The interval between a patient's death and the ensuing violence was short, happening on the same day in 54.8% of cases.
Conclusions: A comprehensive overview of medical WPV in China is presented and may have utility for the formulation of prevention strategies.
Introduction
Health care workplace violence (WPV) may be defined as physical or psychological incidents in which health professionals are abused, threatened or attacked at work (1). Threats to the safety, health or well-being of health workers may be explicit or implicit. Medical WPV is an occupational hazard faced by health professionals the world over and has caused concern both before and after the COVID-19 outbreak (2, 3). A 70–74% proportion of workplace attacks occur in medical facilities in the US (3) and 15% of health professionals responding to the 2019 UK annual survey reported experience of at least one physical violence incident from patients, relatives or other members of the public in the preceding 12 months (4). Most evidence of medical WPV has traditionally come from North America and Europe but has aroused attention as an increasing problem in developing countries. More than 30 South African hospitals reported serious safety incidents in just 5 months in a 2019 survey by the South African Medical Association (5) and 57% of medical ward staff in India experienced violence from patients or visitors (6). The prevalence of WPV against Chinese medical staff has steadily increased over the past decade to become a serious social problem (7). A national survey of Chinese healthcare workers gave the incidence of hospital violence as 65.8% (8).
A separate phenomenon of “Yi Nao” (medical disturbance or medical mobs) whereby patients express their dissatisfaction with an adverse outcome by protest and/or violence in hospitals has also been recorded (9, 10). Medical disturbance represents an organized and extreme form of WPV during which patients, relatives and even hired gangs attack health workers, disrupt the running of hospitals and damage hospital facilities in order to elicit monetary compensation. Yi Nao relating to patient death represents the lack of acceptance by the patient's family and may involve the holding of funerals, placing of flower wreaths, setting up of mourning halls and the burning of paper money on hospital premises with the disruption of normal service (11). More than 17,000 “medical troubles” took place in 2010, an increase of 7,000 compared with 5 years previously, according to Chinese health department statistics (11). WPV may result in physical and mental harm to health workers (8), including death, anxiety, depression and post-traumatic stress disorder (2, 12). It also translates into short-term and long-term economic costs to the workplace and reduces the quality of patient care (13). WPV has caused many Chinese health workers to leave the medical profession and has reduced the integrity of the doctor-patient relationship (14).
Previous studies on medical WPV in China have usually involved media searches, questionnaires or qualitative interviews (15–17). The shortcomings of such studies include the cross-sectional nature and the failure to follow up on violence resolution. A better understanding of the consequences of violence would aid policymakers in the formulation of prevention strategies. A second disadvantage is that media reports often tend to involve eye-catching cases (18) and under-report the total number of incidents, failing to give the whole picture. The third disadvantage is a focus on hospitals in a certain province and the failure to be nationally representative (19).
Litigation records relating to medical malpractice have been used as a comprehensive and reliable data source in developed countries (20) but such an approach is of limited utility in developing countries. The current study used authoritative national judgment documents to evaluate medical WPV and a discussion of the formulation of violence prevention strategies in China is presented. To the best of our knowledge, the current study will be the most up-to-date exploration of medical WPV in China.
Methods
Database
Data was downloaded from the China Judgment Online System (CJOS) which is managed by the Supreme People's Court of China and represents the most reliable and comprehensive national database of judgment documents (21). Case judgments of all courts in 31 Chinese provinces may be accessed via CJOS. Judgment documents have been routinely published within 7 days of sentencing since 2013 and the online system accommodated more than 100 million judgment documents by the end of 2021.
Search strategy and exclusion criteria
All criminal judgment documents reported the date of occurrence of the crime and the date of sentencing by the court. All cases of medical WPV were included from the date of CJOS inception, January 1st, 2013, to the latest date for complete annual records, December 31st, 2021.
Three key phrases were initially used to screen judgment documents: “medical institutions”, “criminal cases” and “health care workers”. An advanced search was conducted using “criminal cases” and the other two phrases were used as keywords for the whole text. The following more specific terms, including “criminal cases”, “hospital”, “clinic”, “health room”, “health center”, “maternal and child health hospital”, “community health center”, “doctor”, “physician”, “nurse”, “radiographer”, “pharmacist”, “technician”, “laboratorian” and “health worker” were used to identify further cases involving medical WPV. The preliminary search returned 54,618 criminal cases.
All judgment documents were manually screened by four researchers and irrelevant cases in which there was no violence against health professionals deleted. A total of 21,745 cases were retained. In cases where more than one hearing was held, such as an initial hearing followed by an appellate court hearing, only the latter was included to avoid duplication. Exclusion criteria were as follows: 1) the victim was not a health professional; 2) the perpetrator was not the patient, a member of the patient's family or the patient's friend; 3) the violence was not related to the medical care received. A final total of 364 non-repetitive cases were included. Figure 1 shows a flow chart detailing the process of document extraction.
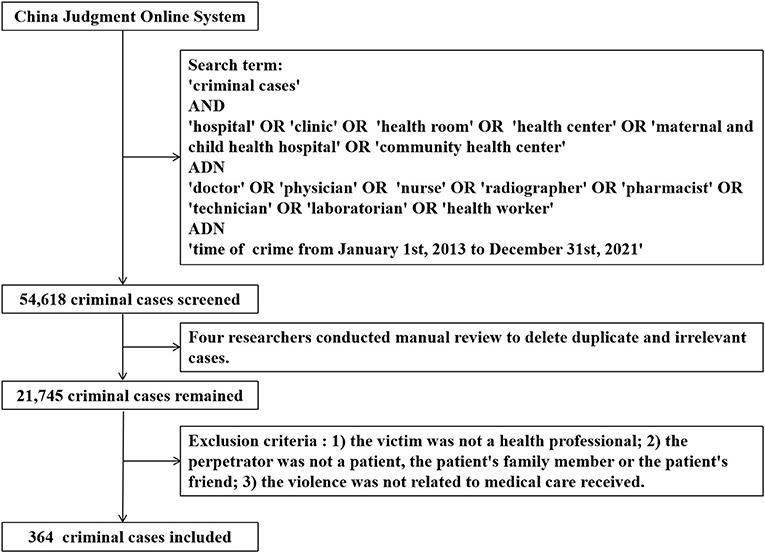
Figure 1. Flow chart of judgment document extraction.
Variable coding and statistical analysis
Judgment files were encoded into four groups of numerical and string variables in standard data format, as follows: (1) Basic case information, including court level, crime date and document number; (2) Characteristics of health professionals, including work department and occupation (e.g., doctor), type and location of health care facilities and whether the death of a health professional was involved; (3) Characteristics of perpetrators, including gender, age, occupation, educational level, relationship with patient, assumption of criminal responsibility, history of mental illness or alcohol intoxication and whether medical malpractice technical authentication had been conducted; (4) Characteristics of the violence, including type, whether patient death was involved and the interval between patient death and the violence.
In cases involving more than one defendant, the first defendant's information was taken to represent that of all defendants. Original data was input simultaneously by two researchers to establish inter-rater reliability. Four researchers completed independent reviews of the variable codes to account for potential variation among coders. Discrepancies in variable coding were resolved by team discussion to achieve consensus.
Researchers produced a descriptive statistical analysis of the characteristics of medical WPV and cases involving patient deaths were investigated as representing the most serious adverse consequence. The time interval between the occurrence of the adverse outcome, such as patient death, and violence was considered and the possibility that a death deemed unacceptable by the patient's family might precipitate the seeking of revenge. Cases involving patient death were compared with those where no death occurred and the correlation between violence and the patient's dead/alive status assessed by Fisher's exact test with IBM SPSS 22.0. Health facilities were categorized according to the Chinese Health Statistics Yearbook 2021 (22). All descriptive statistical analyses and testing of hypotheses were conducted by Microsoft Excel 2019 and IBM SPSS 22.0 with a value of p < 0.05 considered to indicate statistical significance.
Results
A total of 364 cases related to medical WPV were tried by Chinese courts between 2013 and 2021. A trend of increasing hospital violence, followed by a decrease can be seen over the last 10 years (Figure 2). The incidence of WPV cases showed a year-on-year increase from 2013 (n = 35), reaching a peak in 2016 (n = 73) and gradually decreasing in the following years. By the end of the timeframe of interest, the rate had dropped to the lowest level (n = 10), less than one-third of the rate in 2013. The distribution of medical WPV cases by province can be seen in Figure 3, in which greater numbers of cases are represented by darker colors. The following five provinces/municipalities had the most cases of WPV: Guangdong, 53 (14.6%); Hunan, 29 (8.0%); Beijing, 27 (7.4%); Jiangsu, 26 (7.1%) and Zhejiang, 23 (6.3%). The majority of medical WPV cases were concentrated in Eastern regions with the highest numbers in Guangdong (Eastern) and Hunan (central) provinces and no cases were reported from the Western provinces of Qinghai (n = 0) or Tibet (n = 0).
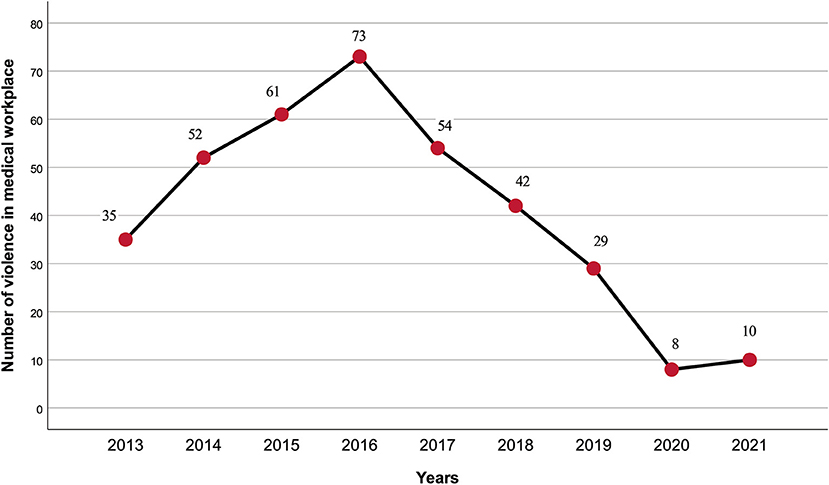
Figure 2. The frequency of medical workplace violence between 2013 and 2021.
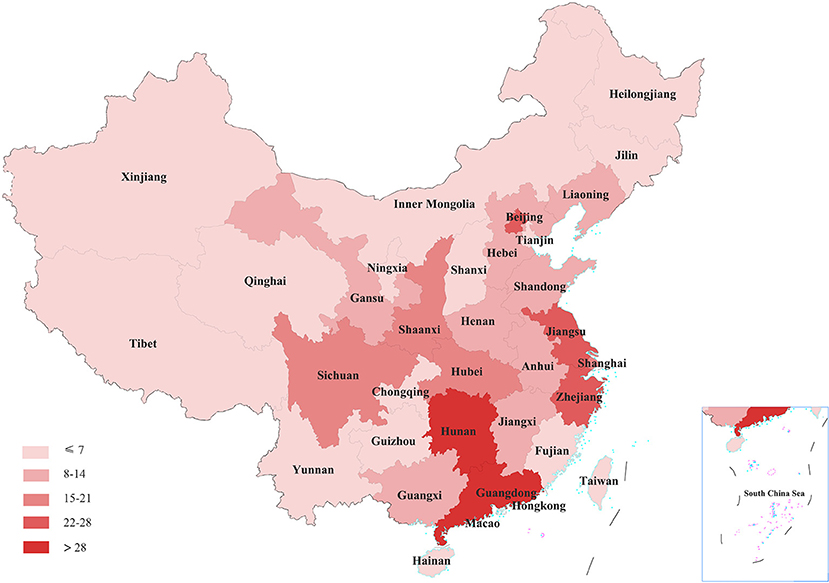
Figure 3. The distribution of medical workplace violence cases in different provinces of China.
Information about the perpetrators
Demographic characteristics of perpetrators are shown in Table 1. Most perpetrators were male (n = 239; 81.8%), aged between 18 and 47 (68.8%), had not finished high school education (66.7%) and 80.9% were farmers or unemployed. The most common perpetrators were members of patients' families (58.2%), followed by patients themselves (38.2%). The vast majority of perpetrators bore full criminal responsibility (n = 353; 96.9%) with only 9 (2.5%) having a history of mental illness and only two being intoxicated with alcohol. No records of intoxication with illegal drugs were found.
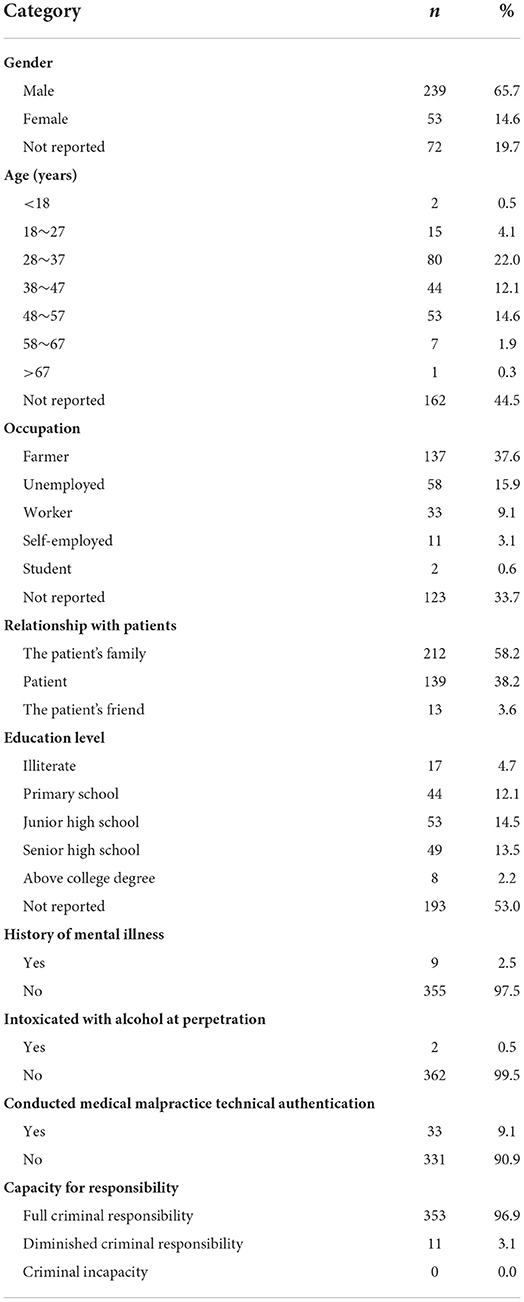
Table 1. Demographic characteristics of perpetrators.
Information about the victims
The occupational categories of victims included doctors, nurses, laboratory technicians or radiographers and others (e.g., security personnel). The vast majority of cases concerned doctors (59.9%), followed by nurses (26.1%). Secondary hospitals were the sites of 24.2% of cases, primary health care institutions of 13.5% and tertiary hospitals of 12.9% (Table 2). Violent incidents also took place in other types of hospitals, such as Chinese medicine hospitals (9.3%), specialist hospitals (8.2%) and private hospitals (6.0%). More than half of the cases (52.5%) occurred in rural areas with this percentage being even greater where primary health care institutions (71.4%) and secondary hospitals (73.5%) were involved. Of hospital-based WPV, teaching hospitals accounted for 74.7% (n = 272) of incidents and non-teaching hospitals for 20.6%. Cases showed a wide distribution across 10 clinical departments but the three with the highest incidences were the emergency (18.9%), pediatrics (13.2%) and obstetrics (11.5%) departments. Seven health care workers were murdered.
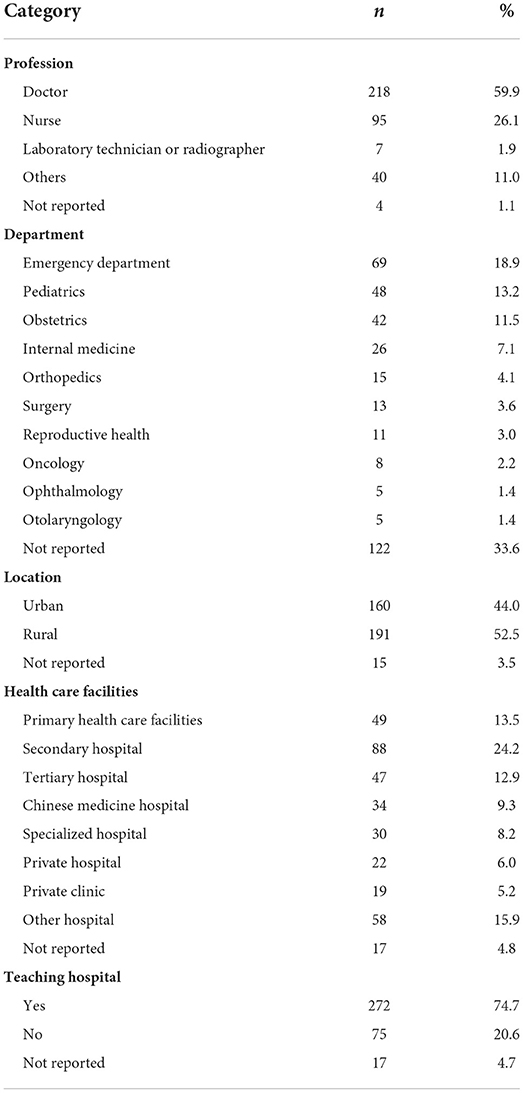
Table 2. Information about the victims.
Information about violence
Overview of various types of violence in criminal cases
The various types of violence detailed by judgment records are summarized in Table 3 and are divided into 3 categories: psychological violence, physical violence and medical disturbance (“Yi Nao”). Verbal abuse amounting to psychological violence occurred in 28.3% of cases, and 18.1% involved threats. Physical violence ranged in severity from pushing to bombing. Beating accounted for the highest proportion (43.1%), followed by pushing (30.5%) and 14.0% involved injury by a sharp instrument, such as a dagger. The four most common modes of “Yi Nao” included hanging banners (36.3%), destroying hospital equipment (34.3%), blocking hospital passages (31.0%) and burning mock paper money (26.4%).
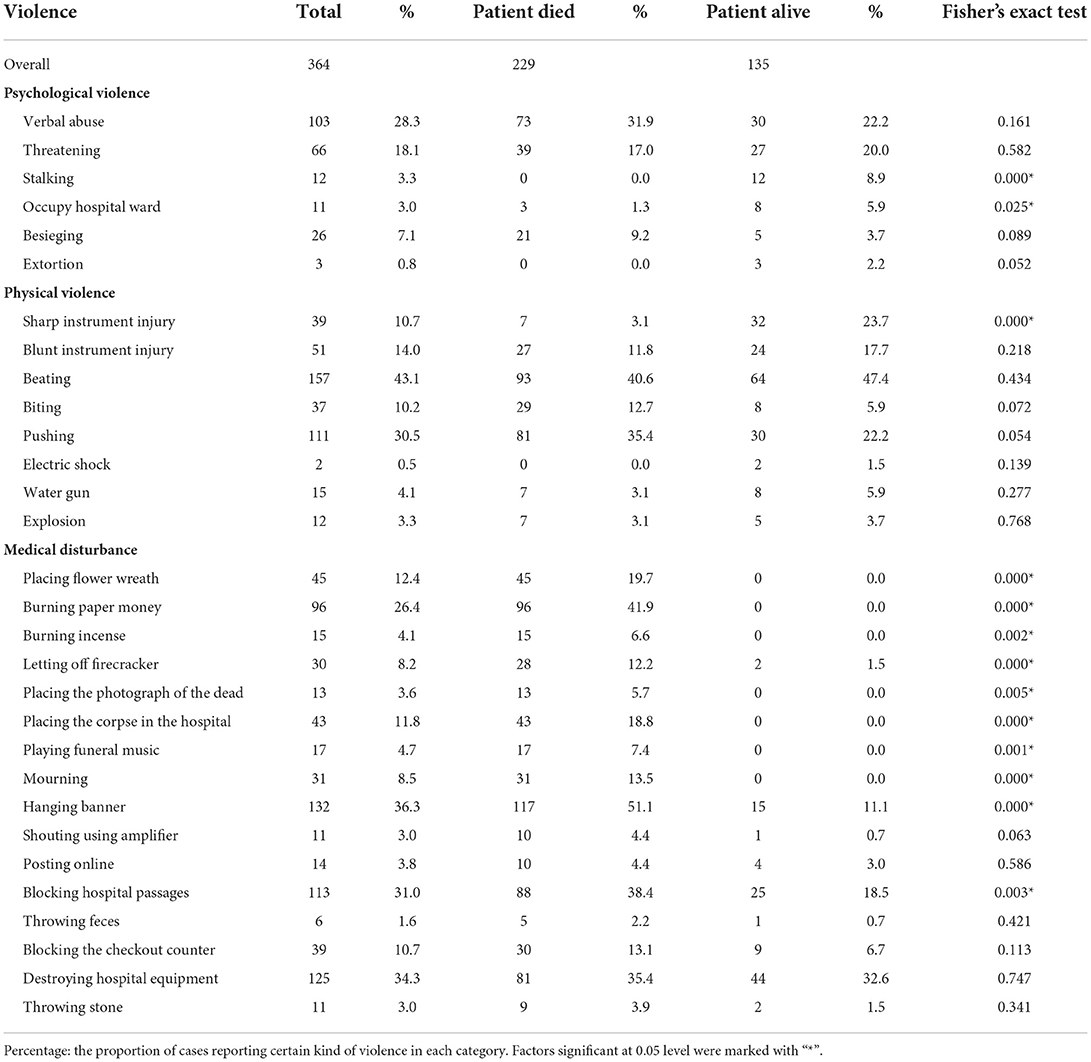
Table 3. Types of violence in the judgement records.
The relationship between violence and treatment outcome of patients (dead or alive)
Records of WPV cases showed that 229 relevant patients died and 135 patients did not. Forms of violence, such as stalking (p < 0.01), refusing to leave wards (p < 0.05) and blunt instrument injury (p < 0.01), showed a significant association with cases that did not involve patient death (Table 3). By contrast, hanging banners, blocking hospital passages, placing flower wreaths, burning paper money and placing the corpse in the hospital were significantly correlated with cases involving patient death (p < 0.01). Verbal abuse and blunt instrument injury showed no relationship with patient death.
Other features of medical WPV
Violence followed patient death with a much shorter time interval than for cases not involving the death of patients. Among the cases of violence following patient death, 54.8% occurred on the same day as the dispute happened, and 22.6% occurred within 1 week. Only in 21 cases was technical authentication of medical malpractice, requiring a third-party medical association to assess whether the adverse results were due to negligence, implemented. The court determined that 14 cases were due to medical malpractice. Four people were sentenced to death for murder as a result of medical WPV although most (82.4%) have been sentenced to fixed-term imprisonment. It is noteworthy that the police were attacked by angry patients or their families while maintaining order in 68 cases (18.7%).
Discussion
The purpose of the present study was to employ the underutilized data source of public litigation records to analyze medical WPV. Litigation records are a valuable asset for research into health policy in developing countries and have many advantages. Firstly, judgment documents are more nationally representative than previous surveys conducted in some Chinese provinces. Secondly, previous investigations into hospital violence have been conducted from the perspective of health professionals and have neglected to focus on patients and their families (perpetrators). The judgment record gives offender characteristics that previous studies have failed to capture, such as the assumption of criminal responsibility and whether a medical malpractice suit has been brought. Thirdly, our research includes medical disturbance or “Yi Nao” as an alternative form of violence which has rarely been mentioned in international literature. Collation of judgment documents has allowed us to contribute information on perpetrators to the existing literature which would otherwise have been excluded from a cross-sectional study or media search. Pre-existing challenges faced by Chinese medical institutions in dealing with WPV have been exposed in such a way as to facilitate the design of prevention strategies.
WPV was found to rise sharply in 2013 before declining after 2016, perhaps due to the revision of the Criminal Law of the People's Republic of China in 2015 (23). A legal amendment allowed courts to impose more than 3 years' imprisonment on criminals who gather people to disturb hospital order, causing heavy losses (23). The availability of severe legal punishments has previously been shown to act as a deterrent, decreasing the cost of crime and reducing the incidence of hospital violence (18). However, the number of relevant cases in 2021 was slightly higher than that in 2020 and the COVID-19 epidemic may be partly responsible. A recent systematic review demonstrated an increase in the incidence of WPV during the COVID-19 epidemic with prevalence rates ranging between 5.8 and 44.4% for physical and 9.6–97.6% for verbal violence (2). Thus, the heavy workload, stressful work conditions and inadequate human and material healthcare resources that accompanied the pandemic may have increased the vulnerability of health professionals to WPV. The spread of SARS-CoV-2 around the world continues and governments of the USA, China, India and Algeria have introduced emergency laws to protect health professionals (24). A regional variation in medical WPV was revealed with incidents more likely to take place in medical institutions of the Eastern and central regions between 2013 and 2021 than those located in the Western provinces. Population size and the number of institutional visits have been identified as contributory factors (23) but health care policy and the medical system, including healthcare financing and regulation, should also be considered.
Doctors were found to be more likely to experience WPV than nurses. Previous studies have shown that nurses receive more verbal violence than doctors (25) and doctors are more often victims of physical violence in the workplace (26). These results indicate that the most serious incidents of WPV may be caused by major problems, such as diagnosis and treatment decisions, which are usually taken by doctors. WPV was found to occur widely in health care facilities at all levels, with tertiary hospitals accounting for only 12.9%, consistent with previous conclusions (27). More than half of the medical WPV incidents occurred in rural primary health care institutions or secondary hospitals. By contrast, Ma et al. (23) used media reports from 2004 to 2018 and concluded that serious WPV was largely restricted to cities (90.2%), usually occurring in tertiary hospitals (67.9%). There are two possible explanations for these differences. Tertiary hospitals are the highest-ranking hospitals in China, usually with more qualified doctors and a higher quality of care whereas lower-level hospitals tend to provide lower-quality care, leading to serious patient dissatisfaction and more frequent WPV against medical staff (28). Higher profile tertiary hospitals are usually located in big cities and violent cases are more likely to be reported by the media (18). However, the current findings suggest that medical WPV in low-level facilities and rural areas may have been underestimated. The graded diagnosis and treatment system currently being introduced in China (29) may funnel more patients into primary medical institutions, necessitating further research in the future.
It is noteworthy that many more WPV cases occurred in teaching hospitals than in non-teaching hospitals. Many doctors in Chinese teaching hospitals undertake scientific research and teaching, reducing the time available for clinical duties (28). Routine inpatient service is often performed by postgraduate students, resident trainees and further educational doctors who have less experience in interacting with patients and fewer medical skills which may increase the possibility of involvement in medical disputes (30). Staff in the emergency, obstetrics and pediatrics departments were the most vulnerable to WPV, a finding consistent with those of other studies (23, 31). However, a specific specialization was not reported for many cases meaning that this result should be interpreted with caution.
Studies from abroad have shown that drug abuse is a common trigger of violence and the impulsiveness of drunken patients or companions also poses a threat to the safety of doctors and nurses (32). Chinese health professionals are often warned to be wary of “high-risk” tourists, who may be drunk or have mental disorders (3). However, the current results showed that very few perpetrators suffered from mental illness nor were alcohol or drugs precipitating factors. Intoxication and mental illness do not seem to be the main characteristics of perpetrators (27). Perpetrators were often relatives of patients rather than patients themselves, a phenomenon that has been reported across different time periods, including the COVID-19 pandemic, and different cultures (2, 33). Family members may suffer psychological stress and have to deal with complicated medical procedures, expenses and other issues, generating more quarrels (31). Perpetrators were found to be generally poorly educated and many were farmers or unemployed, consistent with previous studies (7, 31). The level of medical knowledge of patients or their family members with the above characteristics is likely to be low and may be accompanied by unreasonable treatment expectations. If expectations are not met, violence may become a way to vent dissatisfaction (34). Health policymakers might consider promoting medical literacy education to enhance the public's understanding of medicine (35).
Different treatment outcomes were found to be related to different types of violence. Where patient death was not involved, stalking and blunt instrument injury were more common forms of violence. Where patient death occurred, medical disturbances, such as the burning of paper money, hanging of banners and blocking of hospital passages, were more likely to follow. Medical disturbance is a phenomenon unique to China and constitutes a form of hospital violence (17, 20), being categorized as a public order offense in criminal law since 2015 (11). However, medical disturbance is on the increase as a result of hospital managers fearing damage to the reputation and performance of hospitals from adverse treatment outcomes and the consequent payment of monetary compensation to resolve conflicts quickly (11). This suggests that tedious medical malpractice suits may not be the first choice for hospitals and patients. In addition, verbal abuse was the most common psychological violence experienced by health professionals and beating was the most common physical violence. Preservation of the mental health of those in high-pressure working environments and self-defense are challenges that deserve attention (2).
More than half of violent incidents consequent on a patient's death occurred within 1 day and more than 76% within 1 week. Death was clearly the trigger of violence (17, 36), reflecting the supremacy of life in Chinese culture and the difficulty that family members often have in accepting the sudden death of a patient. Perpetrators desired either compensation or revenge to assuage their dissatisfaction (20). A similar phenomenon has been reported in India (37) with disgruntled patients preferring violent revenge rather than a legal resolution. Chinese medical education tends to lack instruction in human interaction or in communication skills (14). Instruction in notifying the family of a patient's death and explaining the circumstances would be beneficial. Police officers were sometimes attacked while maintaining order and may also benefit from instruction in self-protection when dealing with hospital violence and in preventing the spread of violence.
Two recent policy responses to medical WPV have been put forward. In 2013, China's Ministry of Health issued the “Guideline on Strengthening Security Systems in Hospitals” (38) which recommended the allocation of one security guard for every 20 beds. Since 2020, Beijing has strengthened hospital security checks to prevent admission of visitors carrying knives (39). However, some scholars have condemned these policies as “treating the symptom but not the disease” since the focus is on strengthening security, rather than correcting the underlying social factors and the structure of the health system (9).
The current study fills knowledge gaps left by previous research based on questionnaires, media reports or interviews and informs China's prevention strategies. We find that merely tightening security in hospitals is insufficient to address medical WPV, a result which has been confirmed by other studies (2, 11, 18). Better strategies to solve cultural and organizational factors in the workplace and better cooperation between occupational and public health stakeholders are necessary to improve the occupational safety of health professionals (2). Multi-department cooperation, strengthening of doctor-patient communication, improving the legal system of medical malpractice authentication and establishing a complete hospital violence crisis management system are suggested to be appropriate future directions.
Limitations
We acknowledge some limitations to the current study. First, only pre-existing data is included since information of ongoing cases was not available. Second, only adjudicated litigation cases were included and those settled or mediated out of court were not. Out-of-court cases tend to be less serious, so we concentrated on the more serious cases. Third, demographic information on perpetrators was incomplete in some cases due to inconsistent record keeping. Only available data could be analyzed and results should be interpreted on that cautionary basis. Fourth, a single data source was used and this could be seen as a limitation. However, the CJOS is a reliable and underutilized data source in China. Fifth, the focus on criminal judgment records means that emphasis was put on physical violence and medical disputes. Psychological violence against health workers may have long-term impact and merits more research in the future. Finally, under the unique cultural background of China, different forms of medical disturbance often influence each other. Therefore, the relationship between these violence variables and WPV is very complex and needs further study in the future.
Conclusion
Characteristics of violence against health professionals in China were collated from litigation records and the formulation of violence prevention policies is discussed. Doctors were more vulnerable to WPV than nurses and violence occurred in all types of health institutions in both urban and rural areas. Very few perpetrators suffered from mental illness or were intoxicated with alcohol or drugs nor was medical malpractice authentication often involved. In addition, perpetrators were often the patients' relatives not the patients themselves. Different forms of violence followed different treatment results and patient death was found to be a significant trigger. It is recommended that China's current policies on violence prevention should extend beyond the tightening of hospital security. Coordination of structural, organizational and individual participatory interventions is required to ameliorate the situation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
Data curation: YX, ND, LZ, and C-yL. Investigation: H-fC, QZ, L-sL, and JJ. Writing—original draft: YX. Writing—review and editing: T-tC and S-yZ. All authors contributed to the article and Approved the submitted version.
Acknowledgments
The authors appreciate the editor and the reviewers for their insightful and helpful comments and remarks. Besides, the authors would like to express their gratitude to EditSprings (https://www.editsprings.cn) for the expert linguistic services provided.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
WPV, Workplace Violence; CJOS, China Judgment Online System.
References
1. ILO/ICN/WHO/PSI Joint Programme on Workplace Violence in the Health Sector. Framework guidelines for addressing workplace violence in the health sector. (2002). Available online at: https://apps.who.int/iris/handle/10665/42617 (accessed March 2, 2022).
2. Chirico F, Afolabi AA, Ilesanmi OS, Nucera G, Ferrari G, Szarpak L, et al. Workplace violence against healthcare workers during the COVID-19 pandemic: a systematic review. J Health Soc Sci. (2022) 7:14–35.
3. Vento S, Cainelli F, Vallone A. Violence against healthcare workers: a worldwide phenomenon with serious consequences. Front Public Health. (2020) 8:570459. doi: 10.3389/fpubh.2020.570459
4. Andy Cowper,. Violence Against NHS Staff: A Special Report by HSJ Unison. (2018). Available online at: https://guides.hsj.co.uk/5713.guide (accessed March 2, 2022).
5. More than 30 SA Hospitals Report Serious Security Incidents in Past 5 Months,. (2019). Available online at: https://www.medicalbrief.co.za/archives/30-sa-hospitals-report-serious-security-incidents-pas-5-months/ (accessed March 2, 2022).
6. McKay D, Heisler M, Mishori R, Catton H, Kloiber O. Attacks against health-care personnel must stop, especially as the world fights COVID-19. Lancet. (2020) 395:1743–5. doi: 10.1016/S0140-6736(20)31191-0
7. Zhang X, Li Y, Yang C, Jiang G. Trends in workplace violence involving health care professionals in China from 2000 to 2020: a review. Med Sci Monit. (2021) 27:e928393. doi: 10.12659/MSM.928393
8. Shi L, Zhang D, Zhou C, Yang L, Sun T, Hao T, et al. A cross-sectional study on the prevalence and associated risk factors for workplace violence against Chinese nurses. BMJ Open. (2017) 7:e013105. doi: 10.1136/bmjopen-2016-013105
9. Tucker JD, Cheng Y, Wong B, Gong N, Nie JB, Zhu W, et al. Patient-physician mistrust and violence against physicians in Guangdong Province, China: a qualitative study. BMJ Open. (2015) 5:e008221. doi: 10.1136/bmjopen-2015-008221
10. Jiao M, Ning N, Li Y, Gao L, Cui Y, Sun H, et al. Workplace violence against nurses in Chinese hospitals: a cross-sectional survey. BMJ Open. (2015) 5:e006719. doi: 10.1136/bmjopen-2014-006719
11. Li N, Wang Z, Dear K. Violence against health professionals and facilities in China: evidence from criminal litigation records. J Forensic Leg Med. (2019) 67:1–6. doi: 10.1016/j.jflm.2019.07.006
12. Chirico F. Is burnout a syndrome or an occupational disease? Instructions for occupational physicians. Epidemiol Prev. (2017) 41:294–8. doi: 10.19191/EP17.5-6.P294.089
13. Aguglia A, Belvederi Murri M, Conigliaro C, Cipriani N, Vaggi M, Di Salvo G, et al. Workplace violence and burnout among mental health workers. Psychiatr Serv. (2020) 71:284–8. doi: 10.1176/appi.ps.201900161
14. Xiao Y, Du N, Zong L, Chen S. It's time to ease the doctor-patient relationship in China. Fam Pract. (2021) 38:848–9. doi: 10.1093/fampra/cmab051
15. Tan L, Yuan S, Cheng P, Ning P, Gao Y, Xiao W, et al. Media reports about violence against medical care providers in China. Int J Environ Res Public Health. (2021) 18:2922. doi: 10.3390/ijerph18062922
16. Ma Y, Wang L, Wang Y, Li Z, Zhang Y, Ni X. Causes of hospital violence, characteristics of perpetrators, and prevention and control measures: a case analysis of 341 serious hospital violence incidents in China. Front Public Health. (2022) 9:783137. doi: 10.3389/fpubh.2021.783137
17. Wu D, Wang Y, Lam KF, Hesketh T. Health system reforms, violence against doctors and job satisfaction in the medical profession: a cross-sectional survey in Zhejiang Province, Eastern China. BMJ Open. (2014) 4:e006431. doi: 10.1136/bmjopen-2014-006431
18. Xiao Y, Du N, Chen J, Li YL, Qiu QM, Zhu SY. Workplace violence against doctors in China: a case analysis of the Civil Aviation General Hospital incident. Front Public Health. (2022). 10:978322. doi: 10.3389/fpubh.2022.978322
19. Sun P, Zhang X, Sun Y, Ma H, Jiao M, Xing K, et al. Workplace violence against health care workers in north chinese hospitals: a cross-sectional survey. Int J Environ Res Public Health. (2017) 14:96. doi: 10.3390/ijerph14010096
20. Studdert DM, Mello MM, Gawande AA, Gandhi TK, Kachalia A, Yoon C, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. (2006) 354:2024–33. doi: 10.1056/NEJMsa054479
21. China Judgment Online System. Available online at: http://wenshu.court.gov.cn/ (accessed March 2, 2022).
22. National Health Family Planning Commission. List of tertiary and secondary hospitals. (2022). Available online at: https://www.yearbookchina.com/navibooklist-n3022013080-1.html (accessed March 2, 2022).
23. Ma J, Chen X, Zheng Q, Zhang Y, Ming Z, Wang D, et al. Serious workplace violence against healthcare providers in China Between 2004 and 2018. Front Public Health. (2021) 8:574765. doi: 10.3389/fpubh.2020.574765
24. Devnani M. Covid-19 and laws for workplace violence in healthcare. BMJ. (2021) 375:n2776. doi: 10.1136/bmj.n2776
25. Perkins M, Wood L, Soler T, Walker K, Morata L. Novotny A„ et al. Inpatient nurses' perception of workplace violence based on specialty. J Nurs Adm. (2020) 50:515–20. doi: 10.1097/NNA.0000000000000927
26. Anand T, Grover S, Kumar R, Kumar M, Ingle GK. Workplace violence against resident doctors in a tertiary care hospital in Delhi. Natl Med J India. (2016) 29:344–8.
27. Cai R, Tang J, Deng C, Lv G, Xu X, Sylvia S, et al. Violence against health care workers in China, 2013-2016: evidence from the national judgment documents. Hum Resour Health. (2019) 17:103. doi: 10.1186/s12960-019-0440-y
28. Xiao Y, Qiu QM, Huang YX, Zhu SY. Patients gather in large hospitals: the current situation of Chinese hospitals and the direction of medical reform. Postgrad Med J. (2021). [published online ahead of print] doi: 10.1136/postgradmedj-2021-140147
29. Xiao Y, Wu XH, Chen J, Xie FF. Challenges in establishing a graded diagnosis and treatment system in China. Fam Pract. (2022) 39:214–6. doi: 10.1093/fampra/cmab089
30. Kumar M, Verma M, Das T, Pardeshi G, Kishore J, Padmanandan A, et al. Study of workplace violence experienced by doctors and associated risk factors in a tertiary care hospital of South Delhi, India. J Clin Diagn Res. (2016) 10:LC06–10. doi: 10.7860/JCDR/2016/22306.8895
31. Jia C, Han Y, Lu W, Li R, Liu W, Jiang J. Prevalence, characteristics, and consequences of verbal and physical violence against healthcare staff in Chinese hospitals during 2010–2020. J Occup Health. (2022) 64:e12341. doi: 10.1002/1348-9585.12341
32. Boz B, Acar K, Ergin A, Erdur B, Kurtulus A, Turkcuer I, et al. Violence toward health care workers in emergency departments in Denizli, Turkey. Adv Ther. (2006) 23:364–9. doi: 10.1007/BF02850142
33. Arafa A, Shehata A, Youssef M, Senosy S. Violence against healthcare workers during the COVID-19 pandemic: a cross-sectional study from Egypt. Arch Environ Occup Health. (2022) 77:621–7. doi: 10.1080/19338244.2021.1982854
34. Zhou C, Mou H, Xu W, Li Z, Liu X, Shi L, et al. Study on factors inducing workplace violence in Chinese hospitals based on the broken window theory: a cross-sectional study. BMJ Open. (2017) 7:e016290. doi: 10.1136/bmjopen-2017-016290
35. Zhang L, Stone TE, Zhang J. Understanding the rise of Yinao in China: a commentary on the little known phenomenon of healthcare violence. Nurs Health Sci. (2017) 19:183–7. doi: 10.1111/nhs.12311
36. He AJ, Qian J. Explaining medical disputes in Chinese public hospitals: the doctor-patient relationship and its implications for health policy reforms. Health Econ Policy Law. (2016) 11:359–78. doi: 10.1017/S1744133116000128
37. Ambesh P. Violence against doctors in the Indian subcontinent: a rising bane. Indian Heart J. (2016) 68:749–50. doi: 10.1016/j.ihj.2016.07.023
38. National Health and Family Planning Commission of China. Guidelines of Strengthening Security Systems in Hospitals. (2013). Available online at: https://law.lawtime.cn/d699041704135.html (accessed March 2, 2022).
39. Standing Committee of Beijing Municipal People's Congress. Beijing Hospital Safety Order Management Regulations. (2020). Available online at: http://politics.people.com.cn/n1/2020/0622/c1001-31754516.html (accessed March 2, 2022).
Keywords: health policy, health professionals, hospital violence, occupational safety, criminal judgment record, workplace violence
Citation: Xiao Y, Chen T-t, Zhu S-y, Zong L, Du N, Li C-y, Cheng H-f, Zhou Q, Luo L-s and Jia J (2022) Workplace violence against Chinese health professionals 2013–2021: A study of national criminal judgment documents. Front. Public Health 10:1030035. doi: 10.3389/fpubh.2022.1030035
Received: 28 August 2022; Accepted: 05 October 2022;
Published: 19 October 2022.
Edited by:
Andrea Aguglia, University of Genoa, ItalyReviewed by:
Jacksaint Saintila, Peruvian Union University, PeruJianxiong Hu, Guangdong Provincial Center for Disease Control and Prevention, China
Copyright © 2022 Xiao, Chen, Zhu, Zong, Du, Li, Cheng, Zhou, Luo and Jia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Xiao, eGlhb3kzQG91dGxvb2suY29t