
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 25 November 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1026489
This article is part of the Research TopicMathematical and statistical modeling of infection and transmission dynamics of viral diseasesView all 13 articles
 Pei Yuan1,2†
Pei Yuan1,2† Yi Tan1,2†
Yi Tan1,2† Liu Yang1,2,3†
Liu Yang1,2,3† Elena Aruffo1,2†Nicholas H. Ogden2,4Jacques Bélair2,5Julien Arino2,6
Elena Aruffo1,2†Nicholas H. Ogden2,4Jacques Bélair2,5Julien Arino2,6 Jane Heffernan2,7
Jane Heffernan2,7 James Watmough2,8
James Watmough2,8 Hélène Carabin9,10,11,12
Hélène Carabin9,10,11,12 Huaiping Zhu1,2*
Huaiping Zhu1,2*Background: The monkeypox outbreak in non-endemic countries in recent months has led the World Health Organization (WHO) to declare a public health emergency of international concern (PHEIC). It is thought that festivals, parties, and other gatherings may have contributed to the outbreak.
Methods: We considered a hypothetical metropolitan city and modeled the transmission of the monkeypox virus in humans in a high-risk group (HRG) and a low-risk group (LRG) using a Susceptible-Exposed-Infectious-Recovered (SEIR) model and incorporated gathering events. Model simulations assessed how the vaccination strategies combined with other public health measures can contribute to mitigating or halting outbreaks from mass gathering events.
Results: The risk of a monkeypox outbreak was high when mass gathering events occurred in the absence of public health control measures. However, the outbreaks were controlled by isolating cases and vaccinating their close contacts. Furthermore, contact tracing, vaccinating, and isolating close contacts, if they can be implemented, were more effective for the containment of monkeypox transmission during summer gatherings than a broad vaccination campaign among HRG, when accounting for the low vaccination coverage in the overall population, and the time needed for the development of the immune responses. Reducing the number of attendees and effective contacts during the gathering could also prevent a burgeoning outbreak, as could restricting attendance through vaccination requirements.
Conclusion: Monkeypox outbreaks following mass gatherings can be made less likely with some restrictions on either the number and density of attendees in the gathering or vaccination requirements. The ring vaccination strategy inoculating close contacts of confirmed cases may not be enough to prevent potential outbreaks; however, mass gatherings can be rendered less risky if that strategy is combined with public health measures, including identifying and isolating cases and contact tracing. Compliance with the community and promotion of awareness are also indispensable to containing the outbreak.
Monkeypox, a zoonosis, has been recorded since early May 2022 in at least 30 non-endemic countries including Spain, the United States, Germany, the United Kingdom, France, and Canada (1). As of 21 July 2022, the cumulative number of confirmed cases exceeded 15,000 globally (2). On 23 July 2022, the World Health Organization (WHO) declared monkeypox a Public Health Emergency of International Concern (PHEIC) due to outbreaks in multiple countries and continents (3). The Public Health Agency of Canada (PHAC) reported 1,410 cases of monkeypox as of 14 October 2022, mostly occurring in Quebec, Ontario, and British Columbia (4). The unusual outbreak emerged in non-endemic areas of the world associated with transmission among gay, bisexual, and other men who have sex with men (gbMSM) (5). Although at the time of writing this paper, the epidemic was declining, there remains a pressing need to understand the epidemic and potential control methods (5–7).
Monkeypox virus, which is closely related to smallpox, is an enveloped double-stranded DNA virus, with two clades, the Central African clade and the West African clade (7, 8). The former is more virulent with reported fatality rates in Africa of 10% for the Central Africa clade and 3.6% for the West African clade (7). The incubation period ranges from 5 to 21 days, after which infected individuals may initially have flu-like symptoms, then, 1–3 days later, a characteristic skin rash develops. The recovery period may take 2–4 weeks (8). In the recent outbreak, there are atypical clinical observations. The majority of the patients are gbMSM who reported genital lesions which subsequently develop into skin lesions on other body sites, although with more limited distribution than reported in the previous outbreaks (9).
In Canada, control is based on vaccines and non-pharmaceutical interventions including recommendations for testing and isolation of cases, and, where possible, tracing of contacts (10). In June 2022, the National Advisory Committee on Immunization (NACI) released a guideline on using an orthopoxvirus (Imvamune®) vaccine with potential efficacy against monkeypox (11). The guideline recommends pre-exposure prophylaxis (PrEP) vaccination for adults at high risk of exposure (occupational or otherwise) and also post-exposure prophylaxis (PEP).
After 2 years of restrictions on gatherings due to the control and prevention of the COVID-19 pandemic, mass gatherings related to festivals and ceremonies are now allowed with no attendance limitations (12). In many Canadian provinces, local festivals recorded attendance close to the pre-pandemic level (12–15), which has led to concerns about the spread and possible outbreaks of monkeypox. WHO also expressed concerns that more infections could arise in Europe and elsewhere (16) due to private and social gatherings during festivals, parties, and holidays. In fact, in the United States, many cases were reported linked to large social gatherings, such as pride events, pool parties, and bathhouses (17, 18). Consequently, it is essential to assess the effect of gathering events on monkeypox transmission to inform public health on the most effective control measures.
Transmission risk at a gathering is mainly associated with the gathering size (19) and is proportional to the population density at the gathering place (20). Using an individual-based model, Moritz et al. (21) showed that for a mass gathering event (MGE) with 200,000 participants, there is a 23.6% increase in positive cases attributed to MGE for the transmission of COVID-19. Also, the effect of increased density of contacts during Hajj was estimated to generate a 78-fold increase in meningococcal infection that impacts not only pilgrims but also the local population (22).
To investigate the dynamics of monkeypox and provide information to public health for prevention and control, especially at gatherings, we established a SEIR modeling framework to assess the effect of the vaccination and other control methods. The vaccination in a high-risk group and ring vaccination strategy along with testing and isolation of cases and contact tracing, as well as the possible interventions during gathering events, are also considered. We mainly focused on assessing the effectiveness of public health control measures, including preventive vaccination or vaccination post-exposure, to simulate the scenarios of gathering with different numbers of attendees and different levels of interventions to inform public health decision-making. Our findings suggested that reactive ring vaccination may itself not be enough; however, if close contacts of cases can be identified, vaccinated, and isolated, an outbreak after MGEs may be prevented.
The vast majority of reported cases occurring in the recent outbreaks in non-endemic areas have been linked to specific high-risk locations and populations. Hence, to better capture the infection dynamics within different risk settings, we considered the population to be divided into two subgroups: a low-risk population (LRG), which is defined as individuals who behave in such a way that their possibility of becoming infected is reduced, and a high-risk population (HRG), which is defined as individuals whose behavior makes them at higher risk of acquiring the infection. For simplicity, henceforth, we use subscript 1 for the LRG and subscript 2 for the HRG. Those two groups interact between and within groups as represented by a contact matrix (cij, i, j = 1, 2), defined using the assumptions in Yuan et al. (23). We assumed that there is no movement of population between the risk groups unless there is a gathering event such that a proportion of LRG people may become part of the HRG.
The infection dynamic follows the SEIR framework, which is extended to include the prodromal stage, vaccinated (partially, fully), and quarantined (tested and confirmed, vaccinated, and susceptible). Susceptible (S) individuals become infected, and move to the exposed compartment (E), after encountering an infectious individual from either LRG or HRG, assuming that the latter group is with higher susceptibility than the first group. After a latent period, the prodromal stage (P) begins, and during this phase no symptoms are apparent, but the individual can shed the virus (24). This period is then followed by the symptomatic infectious stage (I) and then recovery (R) occurs. Infectious individuals with symptoms may be tested, then quarantined (Q), while their contacts, which might be susceptible, exposed, or pre-symptomatic, can be vaccinated and quarantined (Qs or Qv) to prevent any further spread of the infection. Although the model does not include demographics, we assumed that infection-related death might occur among infectious individuals. Isolated individuals who develop infection will remain isolated until recovery. Individuals in both prodromal and symptomatic infectious stages can transmit the infection; however, infections in the prodromal phase are assumed to be less infectious than those in the symptomatic phase. The population structure and flow diagram of the disease are shown in Figure 1.
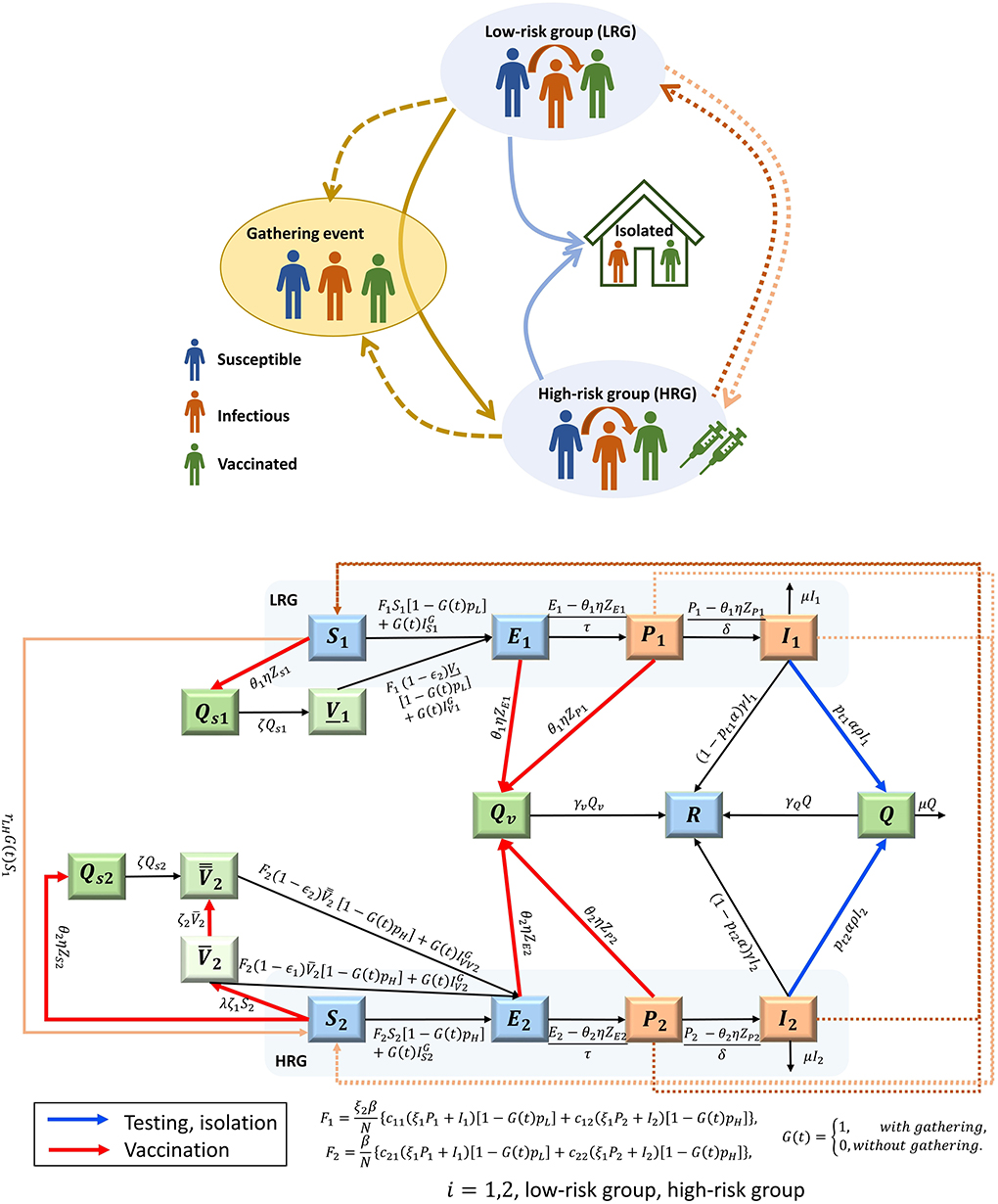
Figure 1. Schematic diagram (A) and flow chart (B) of the MPX transmission among the population classified with low-risk group (LRG, i = 1) and high-risk group (HRG, i = 2), considering the gathering event. In groups i: Susceptible (Si), Exposed (Ei), infectious, prodromal phase (Pi), infectious, acute phase, with rash symptom (Ii), Recovered R; Quarantined (Q), Quarantined and vaccinated (Qv); Quarantined and Susceptible (Qsi); partially vaccinated HRG individuals, , fully vaccinated HRG individuals , fully vaccinated LRG individuals (born before 1972), V1. The individuals in the orange compartments are infectious, while those in dark green compartments are quarantined and hence not involved in the transmission. The compartments of partially and fully vaccinated are presented with light and middle green colors respectively. The arrow with red color represents the process of vaccinating the HRG individuals and the exposures from contact tracing, while the arrow with blue color represents the testing and isolation of symptomatic infections. The dash lines show the transmission routes between the LRG and HRG. The description of the parameters shown in the flow diagram can be found in Tables 3, 4.
We included the current vaccination process in Canada (11) to explore its effectiveness by assuming that only high-risk people and close contacts of confirmed cases will be vaccinated. We also examined the public health measures of testing and isolating cases. Model assumptions, variables, and parameters are summarized in Tables 1–5, and the model equations are presented in Supplementary material S1.

Table 1. Model assumptions.
We used the assumptions of Yuan et al. (23) on the transmission of the monkeypox virus. The probability of transmission per contact was assumed to vary between 12.2 and 24.5% among the HRG and between 0.37 and 0.74%, among LRG, as calculated from the basic reproduction number R0 derived from our simplified model without public health control measures (see Supplementary material S2 for details) and all the other parameters being fixed (Tables 3, 4).
On 10 June 2022, NACI issued interim guidance on the use of Imvamune® in the context of monkeypox outbreaks in Canada (11). Imvamune, initially developed for the prevention of smallpox, is a two-dose vaccine with the second dose administered 28 days after the first one. The immune response is detectable by week 2 after the first dose and peaked at week 6 after dose 2 in a randomized, open-label trial designed to compare the effectiveness of Imvamune with the second-generation replicating smallpox vaccine (11). Given the recent emergence of cases and the use of vaccines, there are no available data indicating the effectiveness of Imvamune vaccination against monkeypox infection; however, studies of vaccine effectiveness (VE) of smallpox vaccine may provide a general estimation. In the context of PEP, the median effectiveness in preventing smallpox disease with vaccination at 1–3 days after exposure was estimated at 80% (30). There are a lot of uncertainties about the effectiveness of Imvamune against monkeypox infection, although some observational studies suggested an efficacy of about 85% among fully vaccinated individuals (11). Hence, in our model, we assumed that the efficacy of the first and second doses ranges between 40 and 60%, and 70 and 85%, respectively.
For simplification, given the extensive vaccine campaign against smallpox until 1972, we assumed that all individuals born before that year are fully vaccinated and therefore protected in the model. We defined here that partially and fully vaccinated represent the individuals who received one or two doses of vaccine, respectively.
Post-Exposure Prophylaxis with Contact Tracing (PEPCT) in our model means that individuals (without symptoms) with exposure to any confirmed case of monkeypox may be traced, vaccinated, and then quarantined. The effect of the vaccine in PEPCT is not significant as the individuals with exposure will be required to isolate and quarantine until fully recovered.
The proportion of PEPCT is represented by θi, (i = 1, 2), which should be the product of the vaccination proportion of the traced close contact and the proportion of contacts that could be traced. Also, it takes time to trace and isolate which in fact can be modeled by the parameter 1/η, the average time from exposure to becoming vaccinated and isolated.
We denote by MI1(t) and MI2(t) the number of new daily confirmed monkeypox cases in the LRG and HRG at time t, respectively, and are defined as follows:
where 1/ρ is the average number of days infectious individuals spend between showing rash symptoms and being tested and confirmed.
Following Yuan et al. (23), the number of close contacts of newly confirmed cases in the LRG, who are in the exposed state ZE1(t) and the prodromal phase ZP1(t) at time t can be calculated as
Similarly, we obtained the number of close contacts of newly confirmed cases in the HRG, who are in the exposed state ZE2(t) and the prodromal phase ZP2(t), as
Also, the number of close contacts of newly confirmed cases that are susceptible in the LRG and HRG is
Pre-exposure prophylaxis in HRG (PrEPH) refers to administering the vaccine to individuals at high risk of exposure to the virus. Hence, in our model, vaccination is only administered to those in HRG. Since people born before 1972 have been vaccinated with the smallpox vaccine, therefore, in the initial state in the model, a proportion of the LRG and HRG populations is considered fully vaccinated for simplicity.
Testing and isolation are crucial steps to detect monkeypox infections and stop the virus from spreading. Individuals with clinical illnesses where monkeypox is suspected should be tested and proceeded for self-isolation before the negative test result is received, while individuals with positive test results should isolate at home until they recover. However, it can take several days from when infected individuals develop symptoms to seek medical help and then get tested, with large variations depending on the individuals' behaviors. In addition, the recovery period takes 2–4 weeks, and with respect to the isolation strategy may not be total, hence compliance with the isolation strategy for those tested and confirmed monkeypox cases are also included in our model.
Gathering events, here refer to mass gatherings, are defined by the WHO as “more than a specified number of persons at a specific location for a specific purpose for a defined period of time” (31). Gatherings may contribute significantly to the spread of infectious diseases, as was extensively studied during the SARS-CoV-2 pandemic (19–21).
Not only will individuals from HRG attend the gathering event, but also individuals in the LRG will join and some of them may transit to the HRG; therefore, facilitating virus spreading and posing the risk of a possible outbreak. In our model, we denote G(t) as an indicator parameter if there is a gathering event.
The daily transition rate from the low-risk susceptible individuals to the high-risk ones is rLH days−1. During the period of gathering events, we assume that the total number of attendees is NG and the proportion of attendees from LRG and HRG is pGL and pGH, respectively. The proportion of LRG and HRG individuals attending the gathering event on day t is calculated as
respectively, and the number of infectious attendees during the gathering on day t is given by
where N1(t) = S1(t) + E1(t) + P1(t) + I1(t) + V1(t) and . Note that the number of recovered individuals is small and not included for simplicity.
Following Champredon et al. (19), we calculated the expected minimum probability of transmissions per attendee that will occur during the gathering, considering the vaccination of attendees, yielding
where cG is the number of effective contacts with an infectious individual during the gathering. An effective contact is defined as a contact where there is physical contact and enough exposure time between individuals which may result in the transmission of monkeypox. Hence, the number of LRG-susceptible individuals infected during the gathering is,
and the number of fully vaccinated LRG individuals infected during the gathering is,
Similarly, we obtained the number of susceptible, partially vaccinated, and fully vaccinated individuals from HRG infected during the gathering as,
respectively.
The expected minimum number of transmissions that will occur during the gathering is thus,
If public health interventions, including vaccination strategy, are applied at the gathering event to prevent the transmission, we assumed that only the fully vaccinated individuals are allowed to attend the gathering, which includes both vaccinated individuals and the individuals vaccinated but not effectively protected (infected, and in the prodromal state). Hence, the proportion of attendance in the qualified LRG and HRG on day t is
where and
are the number of individuals in the prodromal state who are fully vaccinated but not effectively protected in the LRG and HRG, respectively.
Hence, the number of infectious attendees during the gathering on day t, which can only include the fully vaccinated individuals and those infected but in the prodromal stage, is
Since only fully vaccinated individuals are allowed to attend the gathering, the minimum probability of transmissions per attendee will become
Hence, the expected minimum number of transmissions that will occur during the gathering is
respectively.
We conducted numerical simulations with the setting of the hypothetical metropolitan city, starting on 1 May 2022, and the model was run for 2 years (730 days). The vaccination started to be administered in HRG individuals on 10 June 2022 (28). The initial values, parameters with fixed values, and the range of some parameters used for simulations are presented in Tables 2–4. We investigated five different scenarios listed in Table 6 by presenting the projection of daily new infections in LRG and HRG (per 100,000 individuals). In scenarios 1–3, the projection of mean and 95% confidence interval of daily new infections are obtained from 5,000 parameter sets sampling from the prior distribution (uniform) of parameters, by the Latin hypercube sampling (LHS) method (32, 33). We only present the mean of all the simulations in scenarios 2 and 3 for an intuitive interpretation of the results. We explored the proportion of vaccination coverage needed to prevent transmission under different assumptions in scenarios 4 and 5, where other parameters are fixed at the values presented in Tables 3, 4. The analyses were conducted using MATLAB (R2020a) (34).
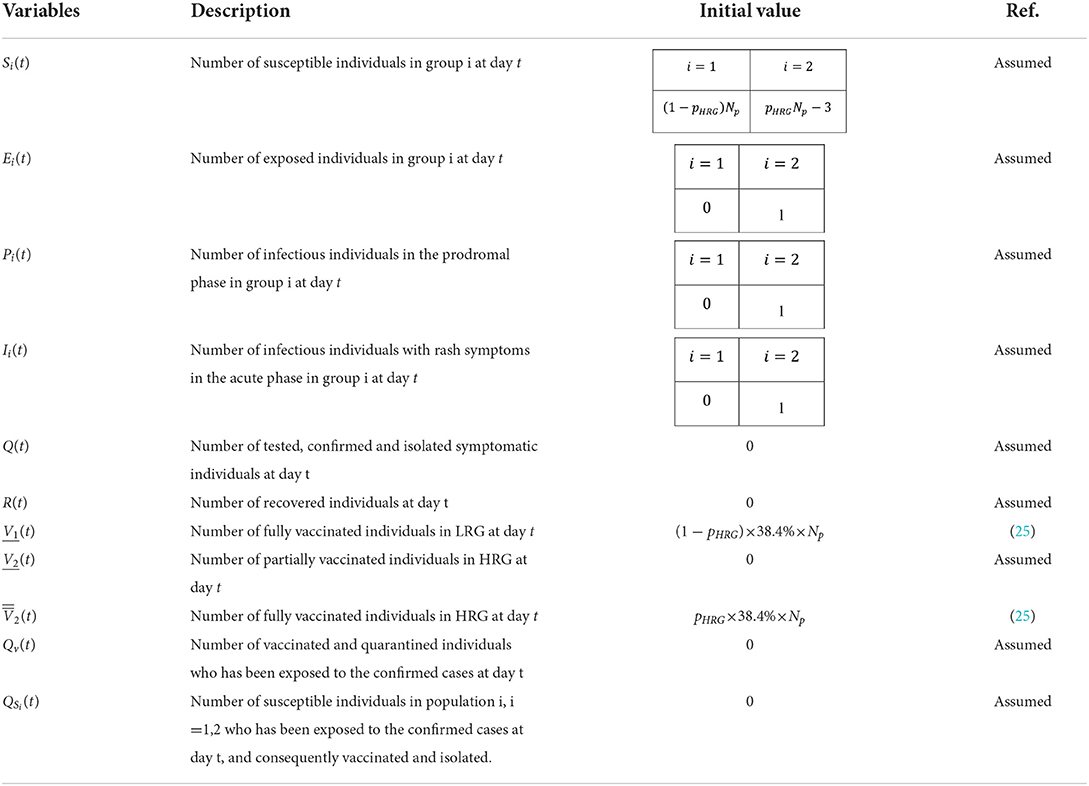
Table 2. Variables used in the modeling of monkeypox transmission and their assumed initial values.
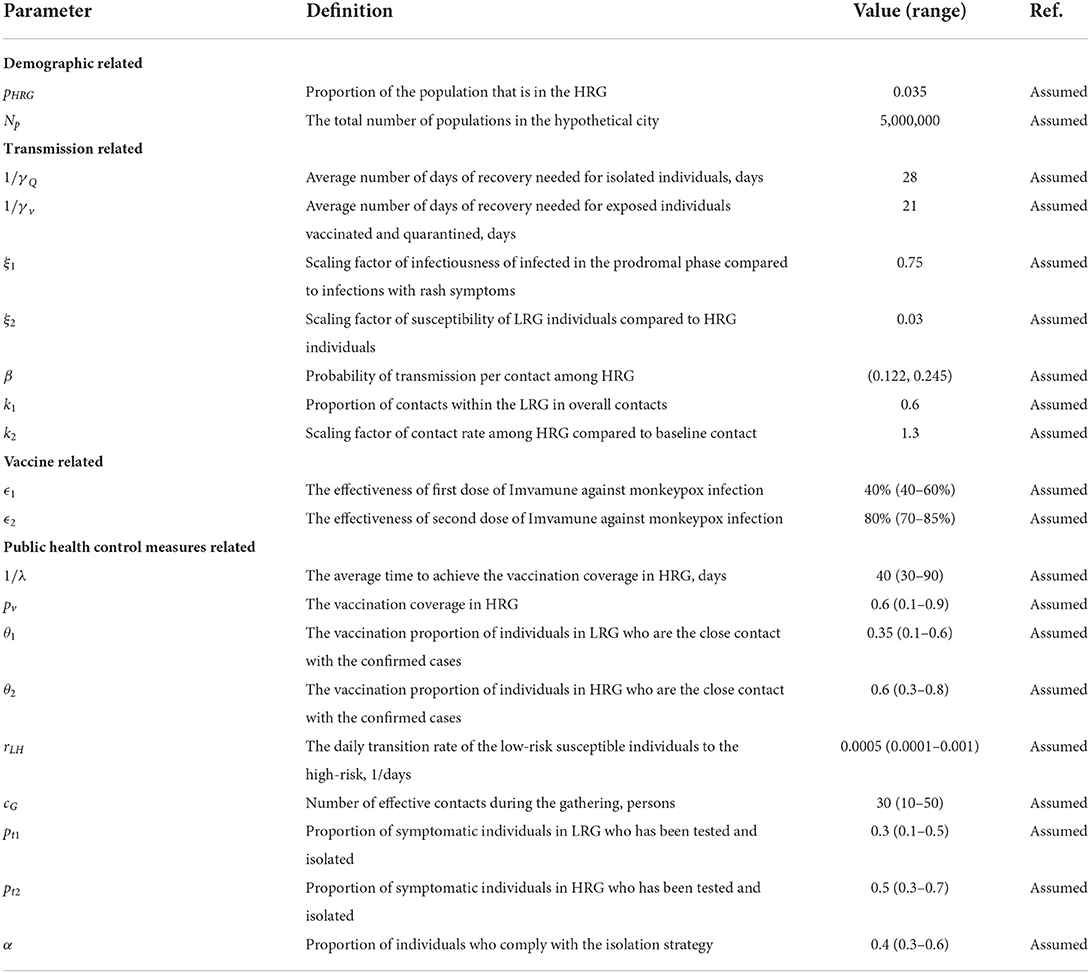
Table 3. Parameters used in the modeling of monkeypox transmission (assumed).
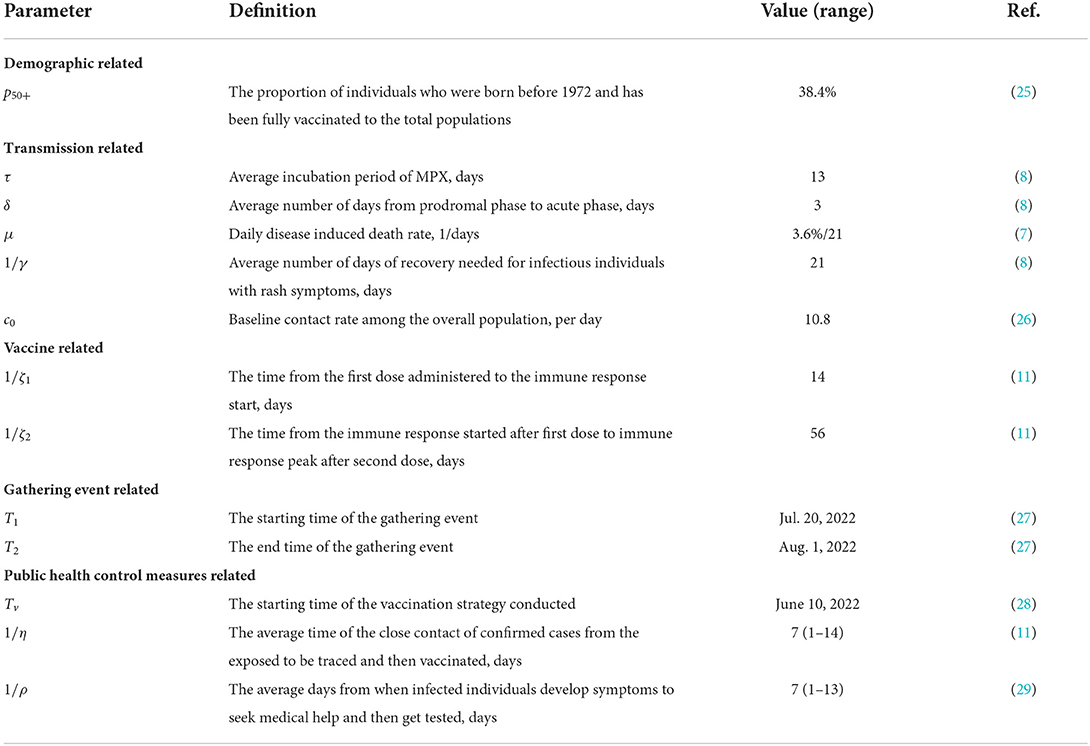
Table 4. Parameters used in the modeling of monkeypox transmission (from literature).

Table 5. Parameters defined in the modeling of monkeypox transmission.
Sensitivity analyses were conducted to address the uncertainty of the parameters through the LHS and the partial rank correlation coefficient (PRCC) method (32). We generated 5,000 samples of parameters related to vaccination strategy, including the efficacy of the vaccine, the vaccination coverage in HRG, the days needed to achieve the vaccination coverage, and the vaccination proportion of close contacts of confirmed cases in HRG and LRG, and the parameters associated with gathering events, including the number of attendees of gathering, the effective contacts in the gathering, the proportion of attendees from LRG individuals. The ranges of parameters used in the sensitivity analysis are reported in Supplementary Table S1. We calculated the value of PRCC to investigate the relationship between the parameters and the model outputs of cumulative cases, which above 0.5 were considered to be significant.
We projected the daily new infections in LRG and HRG when the MGE occurred between 20 July and 1 August 2022 (Figure 2, Scenario 1 described in Table 6). We varied the number of participants and transmissibility levels of the monkeypox virus, under the assumption that public health control measures are not in place. A large outbreak of cases follows MGEs, with the number of cases increasing as the number of attendees and probability of transmission increase, raising the transmission. However, with the lowest number of participants and lower value of R0, the outbreak shows the beginning of an increasing trend 400 days after the gathering. For a gathering with 10,000 daily attendees, the risk of a monkeypox outbreak is low if the transmission probability per contact among the HRG individuals of the monkeypox virus is 12.2% (R0 = 1.5). On the other hand, we could observe a large outbreak if the number of participants increases to 100,000, with an average peak of daily new infections in HRG of around 150 per 100,000 people. If R0 = 3 and attendance increases to 100,000, the outbreak will immediately follow the gathering event, with a larger peak size of infections (500 per 100,000).
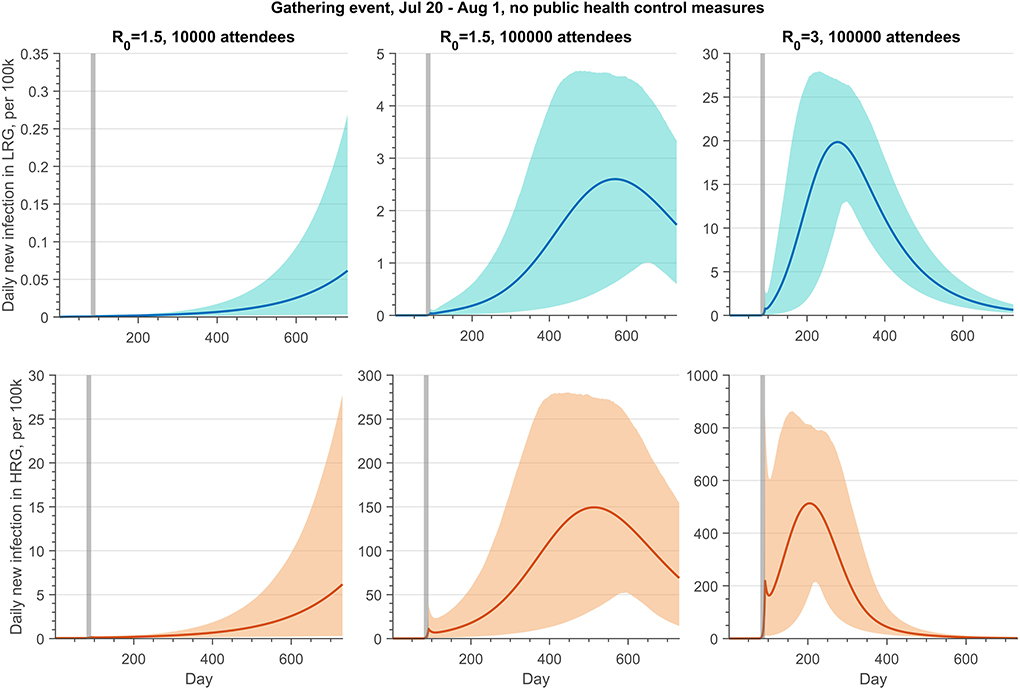
Figure 2. Projections of daily new infections (per 100 k) in the LRG and HRG without public health control measures if there is a gathering event from 20 July to 1 August 2022, with 10,000 or 100,000 daily attendees. The reproduction number of monkeypox transmission is 1.5 or 3. The gray shaded bar represents the gathering event occurring. The detailed setting can be found in Table 6, scenario 1.
Table 6. Lists of settings of scenarios to projections of monkeypox infection.
Figures 3, 4 (Scenario 2 and 3 described in Table 6) show the impact of PEPCT and PrEPH strategies under the possibility of a mass gathering with 100,000 attendees and relatively high transmission efficiency of the monkeypox virus (R0 = 3). Overall, if testing and isolation of symptomatic cases are in place, and contact tracing is effective, the PEPCT strategy is more beneficial to the control of monkeypox outbreaks, compared to the PrEPH strategy, and this is expected given the time needed to develop an immune response and the low vaccine coverage in the overall population in the simulations. With the implementation of the PEPCT strategy, tracing, vaccinating, and isolating 60 and 30% of close contacts of confirmed monkeypox cases in HRG and LRG, respectively, and maximum effective contacts in the gathering, the average peak of daily new infection in HRG was below 4 per 100,000 attendees (Figure 3, second panel). However, this number exceeds 90 per 100,000 if 90% of HRG individuals received at least 1 dose of vaccine before the gathering event started, but without PEPCT (Figure 3, fourth panel).
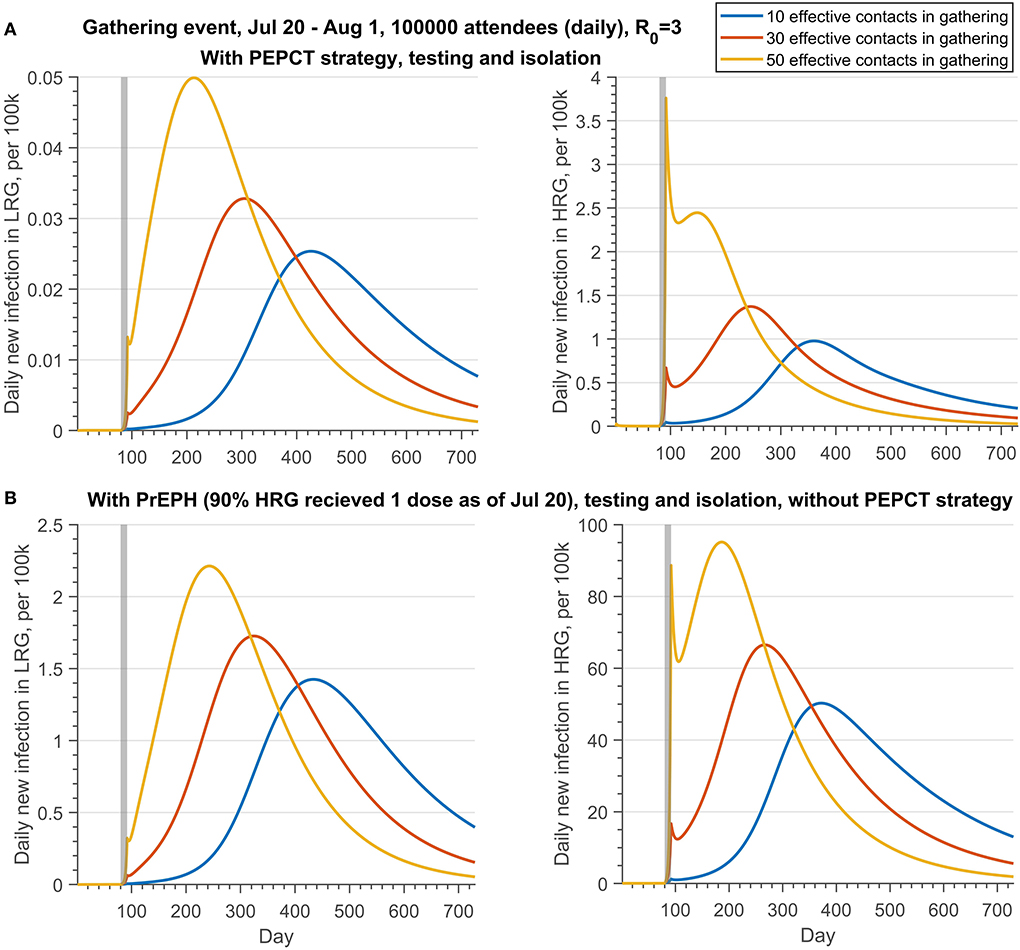
Figure 3. Projections of daily new infections (per 100 k) in the LRG and HRG with different public health control strategies under the different effective contacts in the gathering if there is a gathering event occurring from 20 July to 1 August 2022, with daily 100,000 attendees. (A) With PEPCT, testing and isolation, but without PrEPH; (B) with PrEPH, testing and isolation, but without PEPCT. Note that the reproduction number of monkeypox transmission is 3. The testing proportion of symptomatic infection in HRG and LRG is 50 and 30%, respectively. The PEPCT strategy represents that we vaccinated the 60% close contacts in HRG and 30% close contact in LRG. The gray shaded bar represents the gathering event occurring. The detailed setting can be found in Table 6, scenario 2.
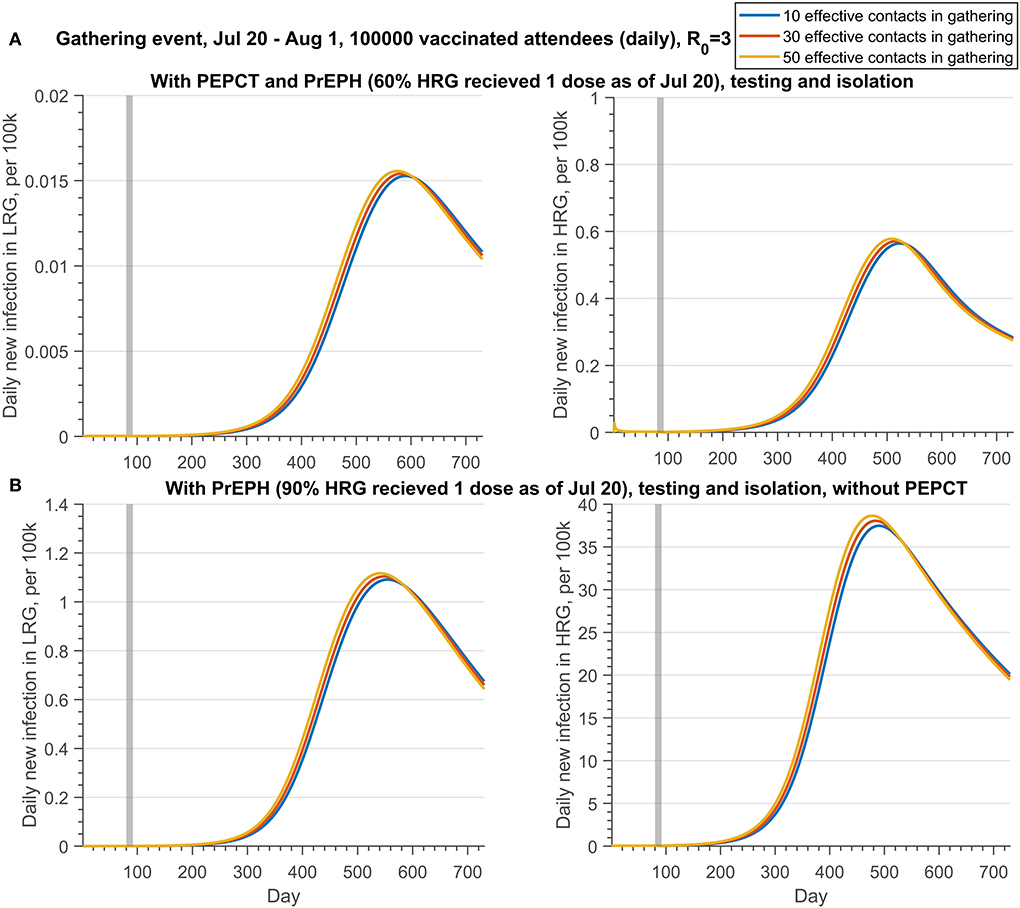
Figure 4. Projections of daily new infections (per 100 k) in the LRG and HRG with different public health control strategies under the different effective contacts in the gathering if there is a gathering event occurring from 20 July to 1 August 2022, with daily 100,000 attendees who has been fully vaccinated. (A) With PrEPH (60% HRG received 1 dose before 20 July) and PEPCT, testing and isolation; (B) with PrEPH (90% HRG received 1 dose before 20 July), testing and isolation, but without PEPCT. Note that the reproduction number of monkeypox transmission is 3. The testing proportion of symptomatic infection in HRG and LRG is 50 and 30%, respectively. The PEPCT strategy represents that we vaccinated the 60% close contacts in HRG and 30% close contact in LRG. The gray shaded bar represents the gathering event occurring. The detailed setting can be found in Table 6, scenario 3.
Similar results were obtained if all attendees of the gathering event are fully vaccinated (Figure 4). If the PEPCT strategy is implemented and the effective contacts during the gathering are 50, the mean peak of daily infection in HRG is below 1 per 100,000, although only 60% of individuals were administered 1 dose of vaccine before the gathering. Conversely, with only 10 effective contacts in the gathering, the mean peak of daily new infection in HRG exceeds 35 per 100, 000, if vaccinating 90% of HRG individuals with 1 dose before the gathering but without a PEPCT strategy. Regardless of whether there was a vaccination requirement for the attendance of gathering events, PEPCT strategies are critical to containing monkeypox transmission arising from gatherings.
Results for LRG follow the same trends of HRG, but with a smaller magnitude.
The peak size of the monkeypox outbreak is significantly associated with the number of effective contacts in the gathering if there are no restrictions on the gathering activities (Figure 3). Thus, the public health control measures aiming at constraining effective contacts during the gathering are essential to prevent the possible outbreak under this circumstance.
However, contact during the gathering would have a slight effect on the progression of the monkeypox transmission if only fully vaccinated individuals are allowed to attend the gathering (Figure 4). Moreover, whether there is a vaccination requirement for the attendees of gathering activities or not, public health control measures, such as PEPCT, are needed to prevent an outbreak resulting from MGEs.
Figure 5 shows a contour plot of peak infection in LRG and HRG under Scenario 4 (described in Table 6), when effective contacts and vaccine coverage (one dose by July 20) are varied. These results permit the determination of the vaccination coverage in HRG and constraints of contacts in gathering needed to prevent monkeypox transmission if the gathering event occurs. In this scenario, testing and isolation (30 and 50% of symptomatic infections in LRG and HRG) are included. As illustrated in Figure 5, public health interventions on constraining contacts during the gathering are more beneficial to contain the transmission, compared to the strategy of increasing vaccination coverage in HRG shortly before the event. The infection in the LRG could be kept below 1 per 100,000 if the effective contacts in the gathering are 46. However, the contacts should be < 15 to maintain a low prevalence (10 per 100,000) in HRG.
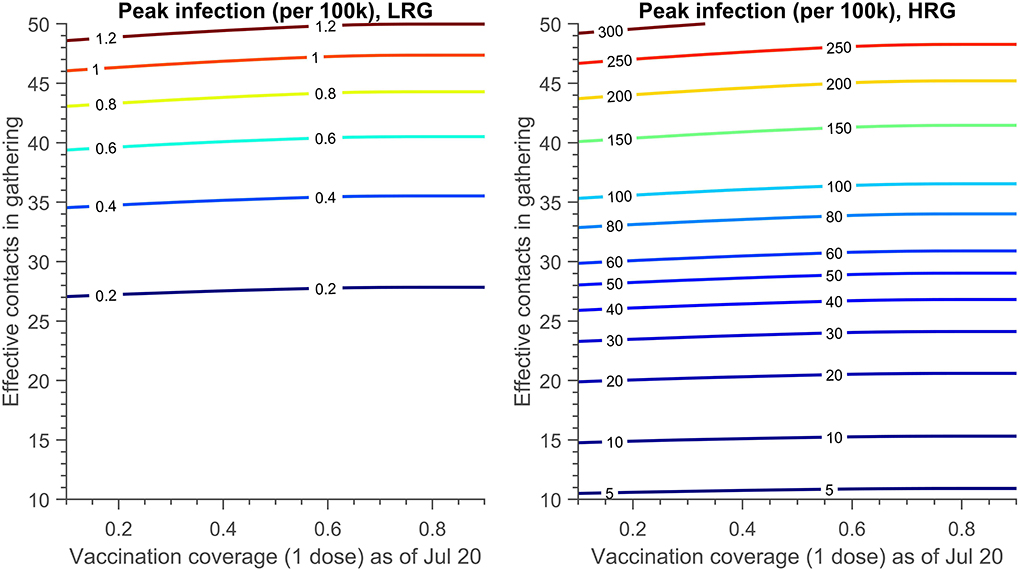
Figure 5. The contour plot of peak infection in LRG and HRG (per 100 k) with different effective contacts in the gathering and the vaccination coverage achieved (1 dose) on 20 July. There is no PEPCT strategy and the testing proportion of symptomatic infection in HRG and LRG is 50 and 30% respectively. The detailed setting can be found in Table 6, scenario 4.
The contour plot of peak infection in LRG and HRG with varying vaccination proportions of PEPCT and PrEPH is shown in Figure 6, if all the individuals were allowed to attend the mass gathering events (100,000 attendees), along with assumptions listed in Table 6 (Scenario 5). If vaccination coverage of 1 dose in HRG as of 20 July is 10%, to maintain the infection in LRG below 1 per 100,000, at least 38% of close contact of confirmed cases in HRG should be traced, vaccinated, and isolated. However, this proportion needs to increase to 75% to keep the infection in HRG below 1 per 100,000.
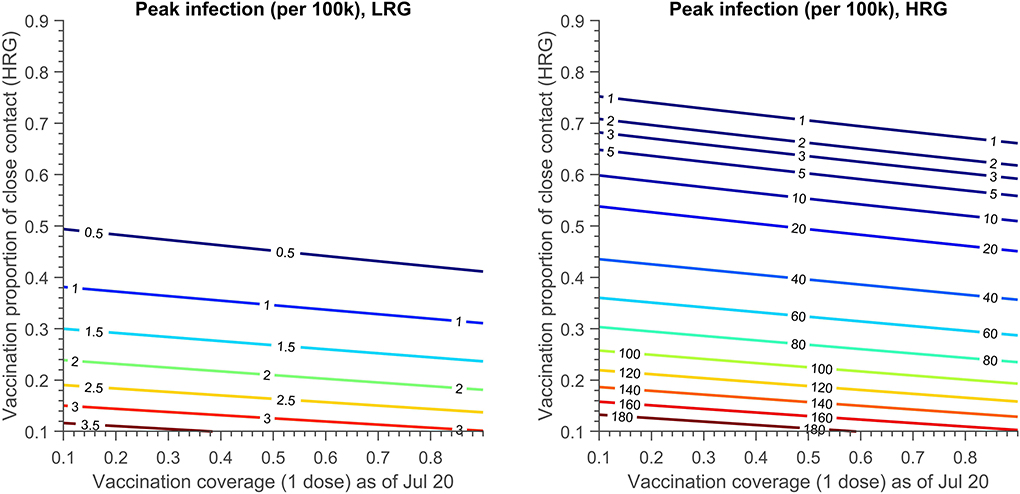
Figure 6. The contour plot of peak infection in LRG and HRG (per 100 k) with vaccination proportion of close contact in HRG and the vaccination coverage achieved (1 dose) on 20 July. The testing proportion of symptomatic infection in HRG and LRG is 50 and 30%, respectively. A total of 30% close contact of confirmed cases in LRG are traced, vaccinated and quarantined. The detailed setting can be found in Table 6, scenario 5.
The observed number of attendees, the number of effective contacts, and the transition rate from LRG to HRG during the gathering are significantly positively correlated with the cumulative cases (Figure 7A). On the other hand, the proportion of attendees from the LRG is negatively correlated to the cumulative cases, but not significant, which indicates a possibility of the dilution effect of the LRG attendees on the gathering events in consideration of the fact that they have a lower possibility to transmit the virus to the LRG community.

Figure 7. The PRCC plots of (A) gathering event-related (B) transmission and vaccine-related (C) public health control strategy-related parameters on cumulative cases.
The sensitivity analysis also showed that the efficacy of the second dose and the vaccine coverage of close contact with confirmed cases in HRG and LRG present a negative correlation with cumulative cases (Figure 7B). Nevertheless, the first dose efficacy and its coverage in HRG, and the daily vaccination rate in HRG are not significant to the cumulative cases, due to the small proportion of HRG individuals in the total population (Figure 7C).
The sensitivity analysis confirmed that the PEPCT strategy and the interventions in the gathering activities are crucial to curb monkeypox spreading at gatherings. Moreover, the efforts of case detection, testing and isolation, and contact tracing, of symptomatic monkeypox cases affect the progression of the disease significantly (Figure 7C).
The classification of the monkeypox outbreak as a PHEIC by WHO underlines its global seriousness (3). In this study, we employed a mathematical modeling approach to explore how vaccinations and other public health measures can be implemented, in a hypothetical metropolitan city, to prevent the spread of monkeypox in human populations after mass gatherings events. Our results suggested that the risk of a monkeypox outbreak after gatherings is high, especially if the number of attendees was large and public health measures were not in place. However, effective public health measures can support the containment of monkeypox transmission at mass gatherings by a combination of constraints on effective contact at the gatherings, implementation of PrEPH, testing and isolation of symptomatic cases, and contact tracing and PEP (here studied as one process PEPCT). Vaccination requirements for participants in mass gathering events could play a crucial role in curbing the spreading of viruses. In addition, tracing, vaccinating, and isolating the close contacts who are exposed to cases was more beneficial to contain monkeypox transmission compared to a PrEP vaccination campaign in HRG individuals that begins shortly before the event.
Our novel model structure, with consideration of saturation of contacts at gatherings, allowed us to assess the monkeypox transmission risk on the occasion that gathering activities occur. Our results suggested that ring vaccination, along with efficient contact tracing and isolation, can be a powerful tool to halt the spread of the monkeypox virus linked to mass gathering events. Either limiting the gathering size and density, requiring the vaccination of attendees, or both may be essential for safe social gathering events. Additional measures were also required, such as a high level of effort to test and isolate confirmed cases and PEPCT, which required rigorous contact tracing and compliance with isolation policies.
In these simulations, the containment effect of PEPCT was determined by the vaccine efficacy, the proportion of contacts traced, the days needs to trace the exposures and vaccination, and the compliance with the quarantine after vaccination. Hence, PEPCT may not work as expected due to the uncertainty of efficacy and availability of the vaccine, as well as the difficulty in identifying the people who are most at risk from infection (35). Moreover, the significant containment effect of the PEPCT strategy mainly results from the transmission cut-off due to the contact tracing and isolation of the exposures. In reality, there is considerable difficulty in identifying contacts with cases, thus limiting the PEPCT strategy. Containing the spreading of monkeypox by ring vaccination protocol is also greatly dependent on the willingness of inoculation of the individual with exposure and compliance with the quarantine after vaccination.
In addition, the precise effectiveness of the smallpox vaccine against monkeypox infection in the human population remains unclear, although initial studies begin to suggest high effectiveness (36). The rollout of the vaccine campaign in HRG, or extending the eligibility to individuals with a moderate risk, requires the support of enough stockpiles of the vaccine. Given the limited vaccine capacity, the public health sector should prioritize vaccines for the communities at risk (37). However, targeting specific communities or groups of people may deepen stigma and hinder tracing, vaccination, and identification of cases (5, 35, 38). Also, only vaccinating the individuals with high risk was not enough to prevent the outbreak in a scenario with an increased transmission efficiency of the virus (possibly due to accelerated evolution) and there may be increased spillover from HRG to LRG (Supplementary Figure S1).
Although our modeling scenario simulations are conducted in a hypothetical metropolitan city with parameters from literature regarding Canadian cities, our model can be easily applied to any jurisdictions and areas where data are available, with the refinement of key parameters like the efficacy of vaccines to inform public health decision making. But the specific numbers required to halt the transmission need to be re-examined in a given region with local data. Besides, it is known that animals are a reservoir and part of the transmission to the human population, but this is not included in our work as we are focusing on the effect of vaccination and gathering events, and it can underestimate the transmission risk (23). We will include it in further study.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
HZ, PY, YT, LY, EA, and NO: conceptualization. YT, LY, and PY: data curation. LY, PY, YT, and HZ: formal analysis. PY, YT, LY, EA, and HZ: methodology and writing—original draft. PY and YT: software, validation, and visualization. JB, JA, JH, JW, NO, HC, EA, PY, YT, LY, and HZ: writing—review and editing. HZ, JA, JB, JH, JW, and HC: funding acquisition. HZ: supervision. All authors contributed to the article and approved the submitted version.
This research was supported by the Natural Sciences and Engineering Research Council of Canada OMNI-REUNI network for the Emerging Infectious Disease Modeling Initiative (NSERC EIDM) (JB, JA, JH, JW, HC, and HZ), Public Health Agency of Canada (HZ), and by the York Research Chair Program (HZ).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1026489/full#supplementary-material
1. World Health Organization. Multi-Country Monkeypox Outbreak in Non-Endemic Countries: Update. (2022). Available online at: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON388 (accessed July 21, 2022).
2. Our World in Data. Monkeypox. (2022). Available online at: https://ourworldindata.org/monkeypox (accessed July 26, 2022).
3. World Health Organization. Second Meeting of the International Health Regulations (2005) (IHR) Emergency Committee Regarding the Multi-country Outbreak of Monkeypox. (2022). Available online at: https://www.who.int/news/item/23-07-2022-second-meeting-of-the-international-health-regulations-(2005)-(ihr)-emergency-committee-regarding-the-multi-country-outbreak-of-monkeypox (accessed July 26, 2022).
4. Government of Canada. Monkeypox: Outbreak Update. (2022). Available online at: https://www.canada.ca/en/public-health/services/diseases/monkeypox/outbreak-update.html (accessed October 18, 2022).
5. The New York Times. Monkeypox and the Gay Community. (2022). Available online at: https://www.nytimes.com/2022/06/24/briefing/monkeypox-gay-community.html (accessed July 31, 2022).
6. Kozlov M. Monkeypox vaccination begins-can the global outbreaks be contained? Nature. (2022) 606:444–5. doi: 10.1038/d41586-022-01587-1
7. Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, Baer LR, et al. The changing epidemiology of human monkeypox—a potential threat? a systematic review. PLOS Negl Trop Dis. (2022) 16:e0010141. doi: 10.1371/journal.pntd.0010141
8. World Health Organization. Monkeypox. World Health Organization. (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed June 2, 2022).
9. Lum FM, Torres-Ruesta A, Tay MZ, Lin RTP, Lye DC, Rénia L, et al. Monkeypox: disease epidemiology, host immunity and clinical interventions. Nature Reviews Immunology. (2022) 22:597–613. doi: 10.1038/s41577-022-00775-4
10. Government of Canada. Interim Guidance on Infection Prevention and Control for Suspect, Probable or Confirmed Monkeypox Within Healthcare Settings. (2022). Available online at: https://www.canada.ca/en/public-health/services/diseases/monkeypox/health-professionals/interim-guidance-infection-prevention-control-healthcare-settings.html (accessed July 21, 2022).
11. Government of Canada. NACI Rapid Response: Interim Guidance on the Use of Imvamune® in the Context of Monkeypox Outbreaks in Canada. (2022). Available online at: https://www.canada.ca/en/public-health/services/immunization/national-advisory-committee-on-immunization-naci/guidance-imvamune-monkeypox.html (accessed July 15, 2022).
12. Mccarthy Tetrault. COVID-19: Recovery Re-opening Tracker. (2022). Available online at: https://www.mccarthy.ca/en/insights/articles/covid-19-recovery-and-re-opening-tracker (accessed July 21, 2022).
13. CBC News. 'Back in the saddle': 2022 Calgary Stampede Winds Down with Near Pre-Pandemic Numbers. (2022). Available online at: https://www.cbc.ca/news/canada/calgary/calgary-stampede-2022-near-pre-pandemic-numbers-1.6523589 (accessed August 01, 2022).
14. The Globe Mail. Summer Festival Sales to Hit New Heights in 2022. (2022). Available online at: https://www.theglobeandmail.com/life/article-summer-festival-sales-to-hit-new-heights-in-2022/ (accessed August 01, 2022).
15. CTV News. Hundreds of thousands celebrate return of Toronto Pride parade to downtown streets. (2022). Available online at: https://toronto.ctvnews.ca/hundreds-of-thousands-celebrate-return-of-toronto-pride-parade-to-downtown-streets-1.5963641 (accessed July 21, 2022)
16. CTV News. How Concerned Should We Be About Monkeypox?. (2022). Available online at: https://www.ctvnews.ca/health/how-concerned-should-we-be-about-monkeypox-1.5914385 (accessed July 21, 2022).
17. NBC Bay Area. SF's LGBTQ Community on Alert After Monkeypox Cases Linked to Pride Parties. (2022). Available online at: https://www.nbcbayarea.com/news/local/san-francisco/san-francisco-pride-monkeypox/2937348/ (accessed July 31, 2022).
18. CNN Health. Monkeypox Spreading in ‘Cluster Events,’ But Vaccines Can Help Stop it, Local Health Officials Say. (2022). Available online at: https://www.cnn.com/2022/07/21/health/monkeypox-clusters-local-officials/index.html (accessed July 31, 2022).
19. Champredon D, Fazil A, Ogden N H. Simple mathematical modelling approaches to assessing the transmission risk of SARS-CoV-2 at gatherings. CCDR. (2021) 47:184–94. doi: 10.14745/ccdr.v47i04a02
20. Liu C, Huang J, Chen S, Wang D, Zhang L, Liu X, et al. The impact of crowd gatherings on the spread of COVID-19. Environ Res. (2022) 213:113604. doi: 10.1016/j.envres.2022.113604
21. Moritz S, Gottschick C, Horn J, Popp M, Langer S, Klee B, et al. The risk of indoor sports and culture events for the transmission of COVID-19. Nat Commun. (2021) 12:1–9. doi: 10.1038/s41467-021-25317-9
22. Coudeville L, Amiche A, Rahman A, Arino J, Tang B, Jollivet O, et al. Disease transmission and mass gatherings: a case study on meningococcal infection during Hajj. BMC Infect Dis. (2022) 22:1–10. doi: 10.1186/s12879-022-07234-4
23. Yuan P, Tan Y, Yang L, Aruffo E, Ogden NH, Belair J, et al. Assessing transmission risks and control strategy for monkeypox as an emerging zoonosis in a metropolitan area. J Med Virol. (2022) 1–15. doi: 10.1101/2022.06.28.22277038. [Epub ahead of print].
24. European Center for Disease Prevention Control. Considerations for Contact Tracing During the Monkeypox Outbreak in Europe, 2022. (2022). Available online at: https://www.ecdc.europa.eu/sites/default/files/documents/Considerations-for-Contact-Tracing-MPX_June%202022.pdf (accessed July 31, 2022).
25. Statista. Resident Population of Canada in 2021, by Age. (2022). Available online at: https://www.statista.com/statistics/444868/canada-resident-population-by-age-group/ (accessed August 01, 2022).
26. Brankston G, Merkley E, Fisman DN, Tuite AR, Poljak Z, Loewen PJ, et al. Quantifying contact patterns in response to COVID-19 public health measures in Canada. BMC Public Health. (2021) 21:1–10. doi: 10.1186/s12889-021-12080-1
27. Fashion Magazine. All the Pride Events Happening Across Canada this Summer. (2022). Available online at: https://fashionmagazine.com/flare/pride-events-calendar-canada-2022/ (accessed August 01, 2022).
28. GovernmentofCanada. Summary of National Advisory Committee on Immunization (NACI) Rapid Response of June 10, 2022. (2022). Available online at: https://www.canada.ca/content/dam/phac-aspc/documents/services/immunization/national-advisory-committee-on-immunization-naci/guidance-imvamune-monkeypox/summary-june-10-2022/summary-june-10-2022-en.pdf (accessed July 31, 2022).
29. Adler H, Gould S, Hine P, Snell LB, Wong W, Houlihan CF, et al. Clinical features and management of human monkeypox: a retrospective observational study in the UK. Lancet Infect Dis. (2022) 22:1153–62. doi: 10.1016/S1473-3099(22)00228-6
30. Massoudi MS, Barker L, Schwartz B. Effectiveness of postexposure vaccination for the prevention of smallpox: results of a delphi analysis. J Infect Dis. (2003) 188:973–6. doi: 10.1086/378357
31. World Health Organization: Public Health for Mass Gatherings: Key Considerations. (2022). Available online at: https://www.who.int/publications/i/item/public-health-for-mass-gatherings-key-considerations (accessed October 16, 2022).
32. Mckay MD, Beckman RJ, Conover WJ. A comparison of three methods for selecting values of input variables in the analysis of output from a computer code. Technometrics. (2000) 21:239–45. doi: 10.1080/00401706.2000.10485979
33. Yuan P, Aruffo E, Tan Y, Yang L, Ogden NH, Fazil A, et al. Projections of the transmission of the Omicron variant for Toronto, Ontario, and Canada using surveillance data following recent changes in testing policies. Infect Dis Model. (2022) 7:83–93. doi: 10.1016/j.idm.2022.03.004
34. Math Works. Matlab for Artificial Intelligence. (2022). Available online at: https://www.mathworks.com (accessed July 10, 2022).
35. Kupferschmidt K. Monkeypox vaccination plans take shape amid questions. Science. (2022) 376:1142–3. doi: 10.1126/science.add3743
36. Payne AB, Ray LC, Kugeler KJ, Fothergill A, White EB, Canning M, et al. Incidence of monkeypox among unvaccinated persons compared with persons receiving ≥ 1 JYNNEOS vaccine dose−32 US jurisdictions, July 31–September 3, 2022. MMWR Morb Mortal Wkly Rep. (2022) 71:1278–82. doi: 10.15585/mmwr.mm7140e3
37. Knight J, Tan D, Mishra S. Maximizing the impact of limited vaccine supply under different epidemic conditions: a two-city monkeypox modelling analysis. medRxiv. [Preprint]. (2022). doi: 10.1101/2022.08.18.22278949
Keywords: monkeypox, vaccination strategy, ring vaccination, gatherings, testing, modeling, control
Citation: Yuan P, Tan Y, Yang L, Aruffo E, Ogden NH, Bélair J, Arino J, Heffernan J, Watmough J, Carabin H and Zhu H (2022) Modeling vaccination and control strategies for outbreaks of monkeypox at gatherings. Front. Public Health 10:1026489. doi: 10.3389/fpubh.2022.1026489
Received: 24 August 2022; Accepted: 31 October 2022;
Published: 25 November 2022.
Edited by:
Pierre Magal, Université de Bordeaux, FranceReviewed by:
Jun Han, Chinese Center for Disease Control and Prevention, ChinaCopyright © 2022 Yuan, Tan, Yang, Aruffo, Ogden, Bélair, Arino, Heffernan, Watmough, Carabin and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huaiping Zhu, aHVhaXBpbmdAeW9ya3UuY2E=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.