
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 10 January 2023
Sec. Family Medicine and Primary Care
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1023431
 Sandra Parisi1*
Sandra Parisi1* Nina Lehner1
Nina Lehner1 Hanna Schrader1Leonard Kierer1Anna Fleischer2
Hanna Schrader1Leonard Kierer1Anna Fleischer2 Olga Miljukov3Gabor Borgulya1Gernot Rüter4Annika Viniol5Ildikó Gágyor1
Olga Miljukov3Gabor Borgulya1Gernot Rüter4Annika Viniol5Ildikó Gágyor1Objectives: Although the vast majority of COVID-19 cases are treated in primary care, patients' experiences during home isolation have been little studied. This study aimed to explore the experiences of patients with acute COVID-19 and to identify challenges after the initial adaptation of the German health system to the pandemic (after first infection wave from February to June 2020).
Methods: A mixed-method convergent design was used to gain a holistic insight into patients experience. The study consisted of a cross-sectional survey, open survey answers and semi-structured telephone interviews. Descriptive analysis was performed on quantitative survey answers. Between group differences were calculated to explore changes after the first infection wave. Qualitative thematic analysis was conducted on open survey answers and interviews. The results were then compared within a triangulation protocol.
Results: A total of 1100 participants from all German states were recruited by 145 general practitioners from August 2020 to April 2021, 42 additionally took part in qualitative interviews. Disease onset varied from February 2020 to April 2021. After the first infection wave, more participants were tested positive during the acute disease (88.8%; 95.2%; P < 0.001). Waiting times for tests (mean 4.5 days, SD 4.1; 2.7days, SD 2.6, P < 0.001) and test results (mean 2.4 days, SD 1.9; 1.8 days, SD 1.3, P < 0.001) decreased. Qualitative results indicated that the availability of repeated testing and antigen tests reduced insecurities, transmission and related guilt. Although personal consultations at general practices increased (6.8%; 15.5%, P < 0.001), telephone consultation remained the main mode of consultation (78.5%) and video remained insignificant (1.9%). The course of disease, the living situation and social surroundings during isolation, access to health care, personal resilience, spirituality and feelings of guilt and worries emerged as themes influencing the illness experience. Challenges were contact management and adequate provision of care during home isolation. A constant contact person within the health system helped against feelings of care deprivation, uncertainty and fear.
Conclusions: Our study highlights that home isolation of individuals with COVID-19 requires a holistic approach that considers all aspects of patient care and effective coordination between different care providers.
The novel coronavirus Sars-CoV2 has led to an unprecedented pandemic situation, affecting global economies, mobility and lives. As of November 2022, more than 6.6 million deaths have been attributed to COVID-19 (1). In addition to physical symptoms, COVID-19 leads to psychological distress and mental health consequences (2, 3). These can also be present in patients with non-severe COVID-19 (4, 5). Living through COVID-19 has been described as a stressful event and crisis (6).
The experience of people affected by COVID-19 could contribute to a holistic understanding of individuals‘ illness experience, but has (surprisingly) scarcely been studied (7). Most studies exploring experiences during the pandemic focus on non-infected individuals (8–10). The few studies exploring COVID-19 patients' experience often focus on vulnerable groups e.g., with comorbidities (11) or hospitalized patients (12–15). Both, comorbidities and hospitalization during COVID-19 may, however, significantly influence the illness experience (11–15). Hospital-based isolation is, for example, associated with post-traumatic stress disorder (PTSD) (16). While most patients experience a mild or moderate course of disease, little is known about the illness experience of the broader COVID-19 population in primary care.
During the course of the pandemic, health care systems had to prove resilience (17) finding new ways to ensure COVID-19 diagnosis and care, while adapting to hygiene, quarantine and isolation measures enforced to combat the spread of the disease. The adapted health structure included new modes of care and stakeholders: Telehealth services were rapidly expanded (18–20). In Germany, public health services (Öffentlicher Gesundheitsdienst) gained more influence and became a central player in patient management and implementing COVID-19 related policies (21) alongside general practitioners (GPs) who traditionally coordinate patient-centered prevention and care. Home isolation and care became an important element of the new health structure. While it has been postulated that isolation at home might be less burdensome than isolation in a hospital (22), home confinement during lockdowns has been shown to be a stressful event in the general population across countries (23). The influence of home isolation and the living situation during the pandemic on the individual illness experience is unknown (22). Moreover, there is a lack of evidence on how new modes of care, such as telehealth services, were perceived by patients, particularly within primary health care (24). The experience of people affected by COVID-19 with the new health care structures might help to identify remaining challenges and inform future policies.
Thus, the aim of this study was to explore the experiences of people affected by acute COVID-19 during diagnosis, course and care of disease. We also aimed to explore patients experience with the new health care structures and home isolation, as well as to identify remaining challenges after the initial adaptation of the health care system.
We conducted a mixed-methods study consisting of a survey with both structured and open-ended questions and qualitative interviews. Mixed methods can combine the strength of both quantitative and qualitative research and add additional value when studying complex phenomena (25). We chose the design to gain a holistic insight into patients' experience, combining different methods to identify and compare emerging aspects. To increase credibility and validity of the results we used a large data set as well as methodological, data and investigator triangulation (11, 26).
We used a convergent mixed-parallel design, collecting quantitative and qualitative data at the same time, with both methods equally weighted (27). The analysis of the different datasets was carried out independently and the results were then integrated for interpretation. We used an iterative approach (28) during data collection to fully explore aspects relevant to participants: Initial survey response and themes emerging within the open-ended survey questions were deepened within qualitative interviews (Figure 1).
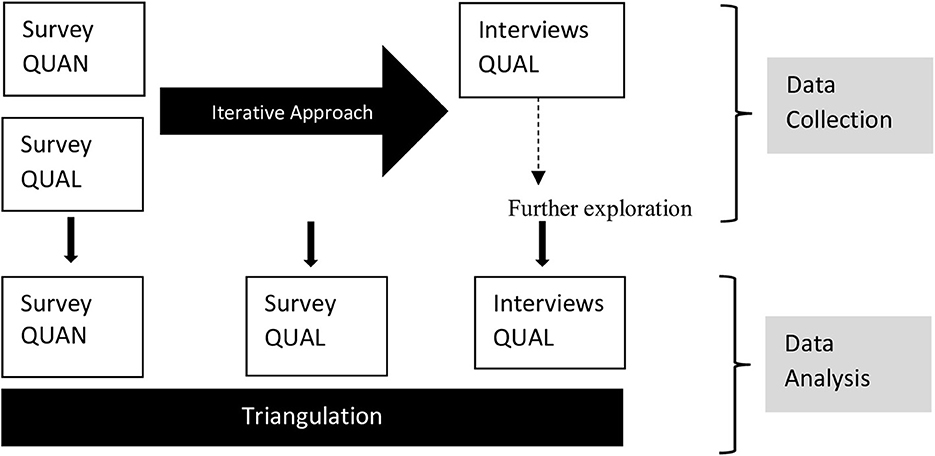
Figure 1. Mixed methods convergent design using parallel data collection with an iterative approach.
The main findings arising within each component were then compared within a triangulation protocol (see also Supplementary material S1) for agreement, partial agreement, silence (complementing information, not present in all data sources) and disagreement (29, 30). This manuscript focusses on the experiences of patients during the acute disease whereas other issues we explored will be published elsewhere.
Recruitment of patients took place through their GPs, who maintain the basic medical care for the population in the German health care system. GPs see the whole range of diseases courses and their patients holistically, within their lived reality during the COVID-19 pandemic.
All adult individuals who had ever experienced COVID-19 were eligible to participate. Due to the lack of access to diagnosis in the early phase of the pandemic, we also included patients without a positive PCR test, based on the early German case definitions (Robert Koch Institute (RKI) guidelines, Supplementary material S2). Exclusion criteria were living in a nursing home, alternative diagnosis (e.g., influenza) and not being able to fill out the survey by oneself (e.g., language constraints).
Study recruitment lasted from August 2020 to April 2021 to include the experience of participants during the so-called 2nd and 3rd infection waves in autumn and winter 20/21, when the German health care system had overcome its initial adaptation process to the pandemic situation. We invited GPs through various channels: a national online forum for GPs, practice based research networks, workshops and congresses, networks of GPs engaged in COVID-19 prevention. Moreover, we reached out to general practices in all German states through letters, using registered addresses publicly available on the internet. We estimate that we reached between 2.000–2.500 GPs in total.
Participating GPs were asked to contact all eligible patients and to pass along the study documents. The survey was then sent back directly to the department of General practice in Würzburg or filled out online using a link provided. Participants were asked to avoid any personal, identifiable information on the survey or envelops. Participants that additionally wanted to participate in telephone interviews directly contacted the study team. They received additional study information including informed consent. Qualitative sampling was by convenience, including all participants until a broad range of participants and illness experiences was covered, and no new themes emerged (data saturation). After finalization of recruitment, GPs were contacted to assess how many study documents they had effectively passed along to their patients for a clearer estimate of the response rate (Figure 2).
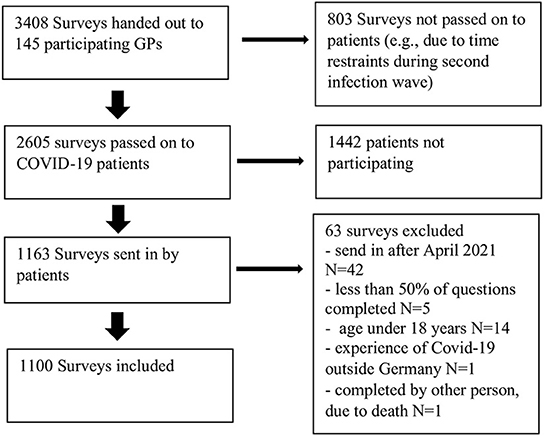
Figure 2. Flowchart of study recruitment.
All documents and tools were tested and adapted during a pilot phase in a community of Würzburg in June/July 2020. A total of 15 patients recruited by 1 non-participating GP completed the survey during the pilot phase. Survey responses were checked and adapted in detail for consistency and misunderstandings. The participants provided written feedback on the survey structure, length and comprehensibility of questions and were asked to propose better suiting answers if appropriate.
The 52-items survey (Supplementary material S3) included sociodemographic variables, comorbidities and risk factors for severe COVID-19, alongside questions on the course and duration of symptoms, as well as on patients' experience during the process of diagnosis and care. Several questions were partially categorized, with the option of multiple choices and the option “others” that could then be specified. Partially categorized questions enable simplified data collection by easier coding of frequently expected answers, without forcing divergent answers into pre-defined categories and thus distorting the results (31). They can moreover help to identify additional aspects relevant to the patients' experience.
Paper-based survey data was entered manually into REDCap electronic data capture tools hosted at [University of Würzburg] (32) with 10% of surveys being randomly selected for independent double data entry (NL, SP) to rule out systematic errors. Both, paper and online databases were then imported into SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) and merged. Respondents that did not meet the eligibility criteria and surveys with < 50% of questions answered, were excluded.
Descriptive analysis of all variables, graphs and bar charts served for database exploration using (33, 34). Comments specified within the option “other” in partially categorized questions were either categorized or explored through qualitative methods. To assess differences in experiences and to identify remaining challenges after the initial adaptation of the health care system to the pandemic, a dichotomous variable for the first infection wave was created (0 = first infection wave, 1 = after first wave). We used the cutoff date for the first infection wave specified in the official reports from RKI (35) (including reporting week 25/20, 21st June 2020). Between group differences were calculated using Kruskal-Wallis (ordinal variables), t-tests, Chi Square or Fisher's exact tests, where appropriate.
Qualitative survey data included responses written within free spaces for comments on the experience during the diagnostic process and any relevant aspects related to the illness experience. Participants also added written side notes or used the option “other” in the section of illness and care for longer comments, e.g., related to health care deprivation. We decided to include those comments into qualitative thematic analysis.
Interviews were conducted via telephone, audio-recorded and transcribed verbatim using a semi-structured interview guide (Supplementary material S3), which was adapted during the process according to new or saturated themes. Thematic analysis with a content-structuring approach aligned to Kuckartz (36) was performed in MAXQDA 2020 (VERBI Software 2019) (37). Main categories were identified deductive-inductively on the ground of the interview guideline and study objectives. After coding all transcripts into those main categories, sub-categories were identified inductively. Two researchers (NL, LK, both thesis students) conducted and coded approximately half of the interviews. SP (MD, MScIH, experienced in mixed-methods research) then built a final coding structure by merging both frameworks and re-coding the data using consensual coding and discussing differences within the research team. IG (MD, senior researcher) supervised the process.
Key findings were identified within each data set and listed within a triangulation protocol (S1). Quantitative findings were reframed into qualitative statements for comparison. Three researchers then independently compared those key findings for agreement, partial agreement, silence or disagreement (SP, NL, KL). Differences were resolved by discussion.
The idea for the study emerged within an online forum of German GPs (Allgemeinmedizinischer Listserver) (38) and was then elaborated by the research team and a member of the forum (GR). Both GPs and patients were involved in the initial design and adaptation of the study and its tools. Several forums were used to engage GPs and patients in this process: (1) Patients gave written and oral feedback on the tools and missing topics they considered important before and after the pilot phase. (2) Initial results were discussed and compared to experiences of local GPs during a workshop. (3) Some authors had also their own experiences with COVID-19.
The study was approved by the ethical committee of the university hospital Würzburg (Nr. 135/20 opinion dated 24th of June 2020). The survey was anonymous. Written informed consent was provided by all participants of qualitative interviews.
A total of 145 GPs supported the study by handing out 2605 surveys to their respective patients from August 2020 to April 2021. From 1163 completed surveys, 1100 were included in the analysis, (90.8% paper based, 9.2% online). The response rate was 44.6%. Figure 2 depicts the flowchart of study recruitment. Figure 3 shows the distribution of survey participants per federal state.
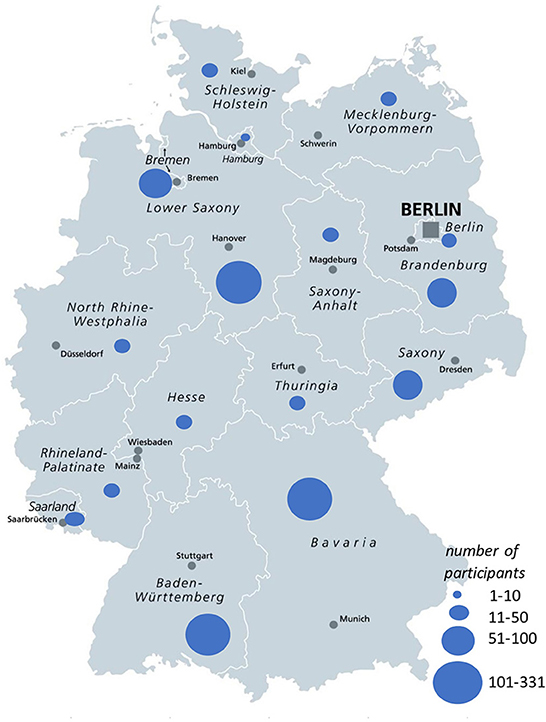
Figure 3. Distribution of survey participants per federal state. Adapted by NL from Peter Hermes Furian–shutterstock.com, with permission.
Survey participants were aged 18–93 years (mean 51.0, SD 16.0, median 53.0) and 56.9% were female; 21.5% worked in health care. Disease onset varied between February 2020 and April 2021. Table 1 depicts the main characteristics of survey participants. Of these, 42 participants (26 female) attended qualitative interviews via telephone (detailed description of interview participants in Supplementary material S4).
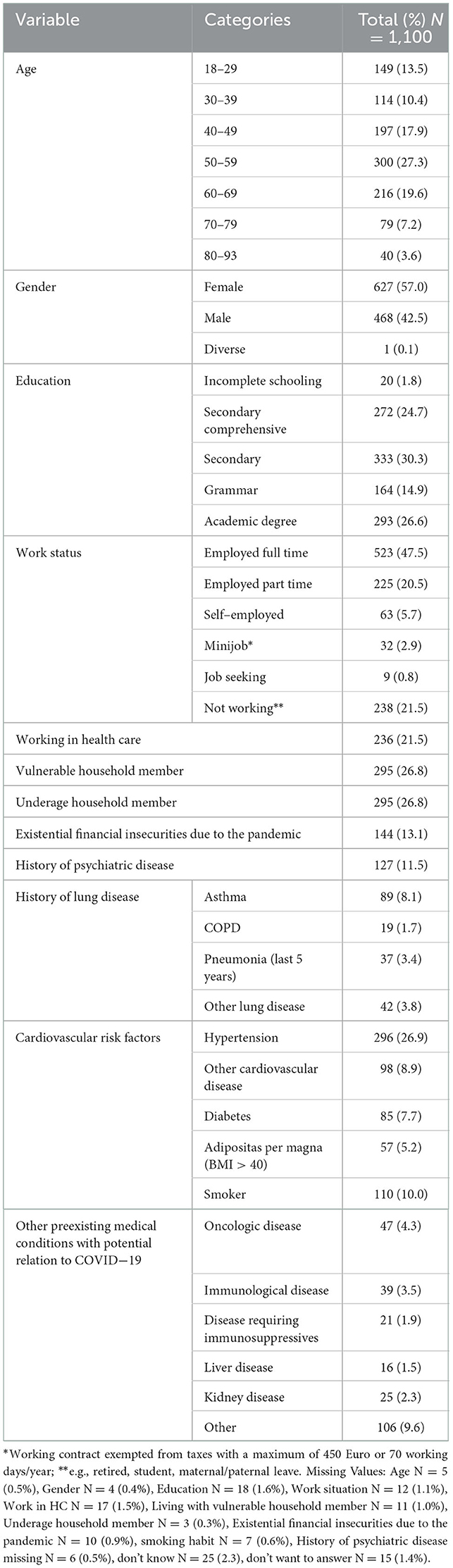
Table 1. Sociodemographic characteristics of the survey population.
Most participants (79.7%) had actively sought diagnosis, mainly due to the occurrence of symptoms (52.8%) and the majority had received a diagnostic test (95.5%), with 93.3% of these being positive. Every fifth participant had later undergone serologic testing, with 78.4% being positive. After the first infection wave there were significantly more positive test results (P < 0.001). There was a decrease in the time span between developing symptoms and tests (P < 0.001) and waiting for test results (P < 0.001) (Table 2).
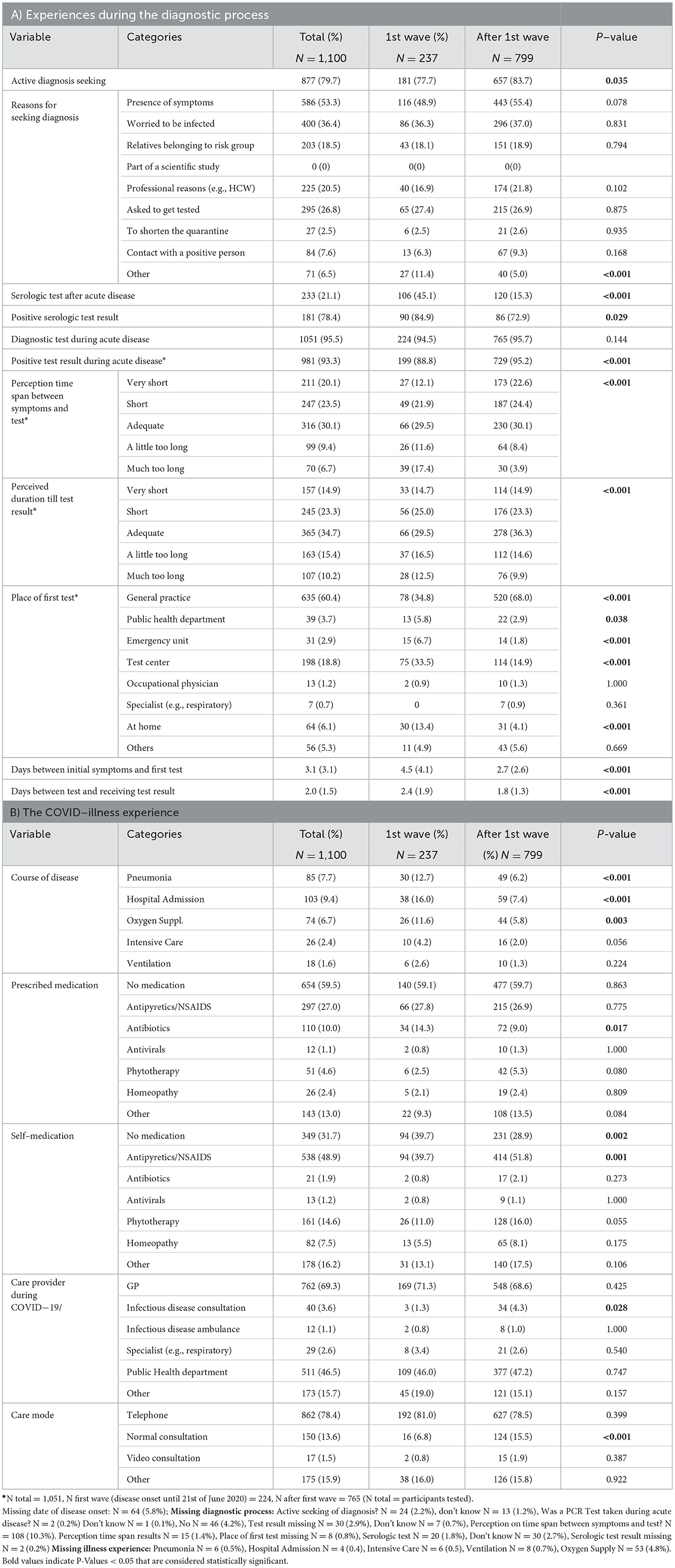
Table 2. Experiences of people affected by acute COVID−19, summary of quantitative results.
Accessing diagnosis ranged from smooth testing (VS1) to nerve-wrecking experiences (VS2-4). Reasons for not being tested were not complying with test criteria (e.g., high fever, positive contact, work within health care) (VS5-7), misdiagnosis (VS8), denial by health authorities and GPs (VS9-11), prioritization due to the scarcity of tests (VS12-14) and problems getting to the test site while feeling sick (VS15-16). Dedicated GPs, focal points for COVID-19 and working within healthcare were facilitators for early testing and early information of results, even outside of working hours (VS17-21). Referenced verbatims (VS) can be found in Supplementary materials S5, S6.
Long waiting times for test results led to insecurities among participants (VS22-23), household members, contacts and superiors (VS24-26) and were connected to putting other people unnecessarily at risk (VS27-28) and to the ongoing high Sars-CoV2 incidence (VS29). Later, the availability of antigen tests and possibilities to repeated testing decreased these insecurities (VS30-32).
The efforts to obtain diagnosis and access barriers were similar to qualitative survey answers (VS33-36). Some participants highlighted creative solutions among their GPs to assure early diagnosis (VS37-39), while others perceived lack of expertise (VS40) or felt denied diagnosis (VS41). Participants also stressed the logistic tasks associated with COVID-19 (VS42) and difficulties organizing the diagnosis of household members (VS43) and contacts (VS44). Public authorities were often perceived overstrained (VS45-46), with difficulties in managing early diagnosis and transmission control, also due to the lack of coordination and digitalization (VS47-49).
The emotional reaction to being diagnosed with COVID-19 ranged from disbelief (VS50-51) and shock (VSVS52-53) to staying calm (VS54) or feeling relief of finally being sure about the diagnosis (VS55). Diagnosis led to rumination and distress about prior contact behavior (VS56-58).
The most cited symptoms of acute COVID-19 were fatigue (70.3%), body aches (60.8%), headaches (60.4%), cough (57.9%), dysosmia (55.7%) and dysgeusia (53.6%) being present in more than half of the study population (Supplementary material S7). Participants with COVID-19 experience during the first wave, more often reported a severe course of disease (Table 2).
GPs (69.3 %) and the public health department (46.5%) were cited as the main care providers. While diagnosis and personal consultations at general practices increased after the first wave (6.8%; 15.5%, P < 0.001), telephone consultation remained (78.5%) the main mode of care and video consultation remained insignificant (1.9%). Some participants (6.1% of total study population) emphasized within the option “other” that they had received no or inadequate health care, without a significant decrease after the first infection wave (P = 0.571). The option “other” also included privately organized or complementary care. Survey responses on prescribed and self-medication are depicted in Table 2.
Disease progression and symptoms: Participants reported a wide range of disease severity (VS 59-61). Severe courses of disease, leading to hospitalization (VS62), but also the unexpected intensity and duration of common symptoms such as pain (VS63-64), fever (VS62), cough (VS65) and especially weakness (VS60, 66-67) impaired the participants‘ illness experience. The unpredictability of COVID-19, with sudden changes in symptoms and severity and the undulating recovery process was perceived difficult (VS63, 68-69).
The mental burden caused by COVID-19: Several participants described panic attacks and constant fear (VS70-72). The focus of media and politicians on severe COVID-19 (VS73) and belonging to a risk group (VS74) contributed to the mental burden. Isolation led to problems with caring for vulnerable family member and worries (VS75-76). Participants described loneliness, imprisonment and difficulties coping with their symptoms, especially when living alone (VS75-77).
Access to health care was often described difficult, both in person and by phone (VS78-80). Perceived health care deprivation during isolation led to feelings of being left alone (VS81-83), helplessness (VS83-84) and insecure (VS85). Insecurities also emerged from the perceived lack of expertise among health staff (VS86-87). A lack of coordination among health care providers resulted in contradicting information and increased the organizational burden on participants (VS88-91). There were, however, also participants with positive experiences (VS92) and participants who reported no need for further care (VS93). Moreover, several participants highlighted their family practice as supporting pillar (VS94-95). Other identified themes are summarized in Table 3.
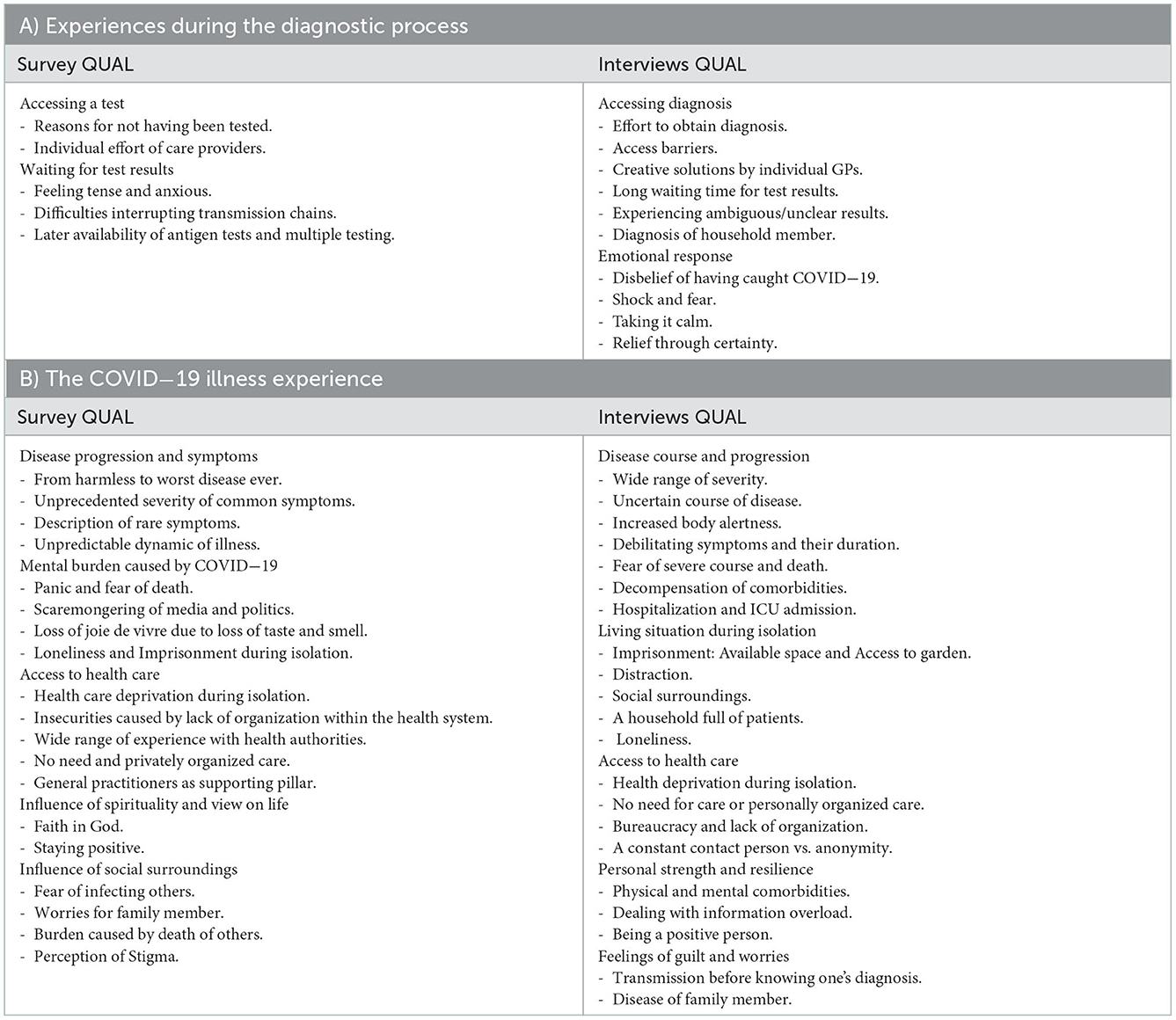
Table 3. Experiences of people affected by acute COVID−19, summary of qualitative results.
Disease course and progression: The intensity (VS96-99), duration (VS99-101) and combination (VS100-101) of pain, weakness, fever, shortness of breath, chest pains (VS102-103), psychotic delusions (VS104), near death experiences (VS105) and the decompensation of chronic comorbidities (VS106-108) were related to a troublesome illness experience. The suddenness and unpredictability of changes in symptoms (VS109-113), the medial focus on severe COVID-19 (VS113-114) and excessive time spent in isolation (VS115) contributed to increased body alertness. Worries of relatives and the fear of not seeing them again impacted the illness experience during hospitalization (VS116-118). Some participants were afraid of or declined hospitalization (VS119-120).
Living Situation: Long isolation and extensions were burdensome (VS121-124). Available space, access to a garden, sunshine and distraction were protective against feelings of imprisonment (VS125-129). Parents described exhaustion due to family management, handling bad moods and social distancing while feeling sick (VS130-136), but also enjoying time together (VS127,137). Loneliness was often described as the worst aspect of COVID-19 (VS138-141). While many participants highlighted support from their social surroundings (VS142), the ban on visits led to a lack of care and support for people in need, e.g., unable to cook for themselves (VS143). Moreover, some patients had experienced stigma including from health staff (VS144-147).
Access to health care: Perceived health care deprivation during isolation was linked to unclear contact persons, busy hotlines, helplessness and anxiety (VS147-151). Health professionals among family and friends, pharmacists and complementary care providers and pulseoxymeters were important resources (VS152-155).
Personal strength and resilience: Having a health or scientific background helped (VS156), whereas previous trauma and mental health conditions impacted the illness experience and the handling of information overload from the media (VS157-159). A pragmatic or positive attitude and experience of handling stressful situations was considered important (VS160-161).
Feelings of guilt and worries: Several participants expressed constantly rethinking their contact behavior prior to knowing about their disease (VS162). Transmission led to feelings of guilt (VS163-165). Worries for infected family members also impacted the illness experience (VS164-166).
The key findings (N = 28) across all data sources can be found within the triangulation protocol (supplementary material S1). There was a high number of agreements between qualitative data sources (27 agreement, 1 partial agreement, 0 dissonance). Between the qualitative and quantitative data sources there was mostly silence (22 silence, 6 agreements, 0 dissonance), indicating that respondents often used the free space and notes to complement the information provided within survey questions.
To the best of our knowledge, this is the first large-scale mixed-methods study using surveys and interviews to explore the experience of people affected by COVID-19 within primary health care. Our results show that diagnostic barriers decreased after the initial adaptation of the health system to the pandemic; however, challenges in the area of contact management remained. Delayed diagnosis was related to worries and guilt of infecting others. The patients‘ illness experience was influenced by the course of the disease, the living situation and social surroundings during isolation, access to health care, personal resilience, spirituality and feelings of guilt and worries. A constant contact person within the health care system and coordinated information provision between different health care providers were identified as essential against feelings of health care deprivation and fear. Triangulation of results demonstrated a high agreement between key findings of the qualitative survey and interview data. Survey participants used the free space to complement these aspects relevant to their experience, whenever not covered by quantitative questions.
In many countries worldwide, including Germany, where this study was carried out, early diagnosis and isolation formed an essential pillar of the strategy for transmission control (39). This could explain the experienced improvements during the diagnostic process. Repeated testing and POC- antigen tests were confirmed as viable tools to reduce insecurities caused by long waiting times and initial false negative PCR results (40, 41). Our study, however, identified remaining challenges within the process of contact management, despite the massive training of containments scouts (without a necessary professional background in health) that served to encompass human resource constraints within Germany‘s public health system (39). Participants often perceived health authorities overburdened and uncoordinated, also due to the already described bureaucracy and lack of digitalization (42). Similar problems in coordination and communication have also been described in other countries (43, 44). COVID-19 diagnosis has previously been linked to rumination about prior contact behavior (45). Organizational problems during the process of diagnosis and contact management led to feelings of guilt and anger of having exposed others to an unnecessary risk and significantly impacted the illness experience.
In line with our study, narratives of patients in Prokop et al. (46) described common symptoms such as body- and headaches, as well as fatigue in a severity never experienced before. This unprecedented severity might be related to several pathophysiologic mechanisms, such as autoimmune responses, direct impairment of nerves or muscles or activation of nociceptive neurons (47). The unpredictable character of COVID-19 has been linked to a burdensome, undulating recovery process (48). In our study this unpredictability moreover led to an increased body alertness and fear, expecting symptoms to decline at any time. Comorbidities were confirmed as important modifiers of illness experience that should be carefully monitored (49). The mental burden caused by acute COVID-19 was furthermore increased by scaremongering media reports and one-sided political communication (50).
In agreement with hospital-based studies (16, 22), the physical environment (e.g., space and access to a garden) significantly influenced the illness experience during isolation. Loneliness has been described as a relevant theme during and after acute COVID-19, especially in older patients (51) and separation from children very difficult (52). We, however, found no studies identifying family management and conflicts, the bureaucratic burden linked to COVID-19 and organizing care for vulnerable family member outside the own household as additional stressors.
Continuity of care by GPs can lead to better general health outcomes (53). Studies from other countries moreover identified, that physicians at times experienced a closer relationship with their patients during the pandemic (43, 54). Our study identified a constant contact person within the health system as important pillar while experiencing COVID-19. Participants lacking a trusted contact person often described feeling left alone and “kafkaesk” while trying to get help and feared a worsening condition without anybody noticing. Apart from GPs, other care providers can play that role. Coordination between different stakeholders and clear guidance to patients should be assured to reduce stress caused by contradicting information (55).
In contrast to the possibilities highlighted in the literature (56–60), and the rapid expansion of telehealth in other countries (18, 20, 24, 61), surprisingly, video consultations were only reported by 1.5% of participants. In line with findings from Australia the telehealth tool mostly used by GPs in our study was the telephone (24). This could be explained by the lack of previous investments in further digitalization within the German Health Care system which hampered a rapid integration of other digital tools into GP practice (62, 63). The German health care system is currently developing strategies to expand home-based care in order to decrease the burden placed upon the hospital sector (64). Remote home monitoring models could reassure patients during home based isolation and care (19, 65), but more studies are needed to generate evidence for appropriate care (66) and the utility of different tools, such as pulseoxymetry (56, 66, 67). We showed that special attention should be placed on people living alone, with preexisting comorbidities or of old age. The same vulnerable groups have been identified in studies in the field of telehealth (18–20, 24, 65, 68). In line with our results, continuity of staff and a trusted relationship with the telehealth provider have been identified as important to patients (18).
Our study results need to be interpreted considering some limitations: (1) The cross-sectional study design does not allow to gain sufficient data reflecting changes during the course of the pandemic. Moreover, emerging qualitative themes such as “loneliness” and “health care deprivation” were not assessed within quantitative variables to test for improvements after the first wave. They however kept emerging in qualitative interviews throughout the study. (2) A recall bias could play a role, particularly among participants who had experienced COVID-19 during the first wave. (3) Participants with a troublesome illness experience (due to either severe COVID-19 or other aspects influencing the experience) could have been more prone to participate and might be overrepresented. (4) Participating GPs were sampled by convenience and the results are therefore not representative. A selection bias of GPs more interested in patient-centered care and COVID-19 might also play a role and lead to an overestimation of the role in patient care played by individual GPs.
On the other hand, the recruitment through a large number of GPs and an adequate response rate compared to surveys in literature (69–71) allowed an inclusion of participants from all German states with a broad range of COVID-19 disease courses, comparable to the expected overall disease severity within the population (35). Although the lack of randomization does not allow representativeness, the geographic coverage, large data set and the methodological, data and investigator triangulation help to gain an idea of patients‘ experiences during acute COVID-19.
Our study might contribute to a better understanding of home isolation as a new care setting, which will continue to play an important role in the context of the current and future health crises. The frequency of zoonotic disease outbreaks is likely to increase due to changes in climate and land-use, as well as livestock production and wildlife trade (72). While home isolation is a viable—and often preferred—option to hospitalization (18, 65), more studies are needed to generate evidence for appropriate care (66). Isolation should be as short as possible and not be prolonged without a strictly necessary reason (55). To provide and maintain patient care during isolation, the patient's condition, environment and responsibilities should be taken into account holistically. Patients of old age, with comorbidities or living alone should be followed up and support for basic needs must be assured. Isolated patients might also need support when in charge of care for other family members. Our study furthermore identified remaining challenges in the context of contact management, as well as coordination and information provision at the interface of GPs and health authorities that need to be addressed. Lastly, proactively signaling availability and clear guidance on what to do in case of worsening symptoms (52) (instead of waiting for patients to seek help) was an easy and very effective way of GPs to reduce the burden caused by acute COVID-19.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study involving human participants was reviewed and approved by Ethical Committee of the University Hospital Würzburg (N.135/20 opinion dated 24th of June 2020). Survey participation was completely anonymous without any possibility to trace identities. The participants self-registered and provided their written informed consent to participate in qualitative interviews.
SP, IG, and GR conceptualized the initial study and together with HS and AV, developed the study protocol and tools. SP, NL, LK, IG, AV, and GR were involved in study recruitment. NL and LK conducted qualitative interviews and transcribed the narratives. SP, GB, OM, and AF were involved in elaborating and carrying out the quantitative analysis. SP, NL, and LK conducted qualitative analysis and triangulation. IG supervised all processes. SP drafted the initial manuscript. All authors contributed during the process of reviewing and adapting the manuscript and approved the current version for submission.
The study was financed with institutional funds from the Department of General Practice, Würzburg.
We thank participating GPs and patients for supporting the study and their valuable input. We also thank the team of the Departments of General Practice at the Universities of Würzburg and Marburg as well as Anna Grau for her support with the database.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1023431/full#supplementary-material
2. Khraisat B, Toubasi A, AlZoubi L, Al-Sayegh T, Mansour A. Meta-analysis of prevalence: the psychological sequelae among COVID-19 survivors. Int J Psychiatry Clin Pract. (2022) 26:234–43. doi: 10.1080/13651501.2021.1993924
3. Bo HX Li W, Yang Y, Wang Y, Zhang Q, Cheung T, et al. Posttraumatic stress symptoms and attitude toward crisis mental health services among clinically stable patients with COVID-19 in China. Psychol Med. (2021) 51:1052–3. doi: 10.1017/S0033291720000999
4. Moradi Y, Mollazadeh F, Karimi P, Hosseingholipour K, Baghaei R. Psychological reactions of COVID-19 patients to the stress caused by the disease crisis: a descriptive phenomenological study. Perspect Psychiatr Care. (2021) 57:1719–26. doi: 10.1111/ppc.12741
5. Landsman JA, Verheij NP, Alma MA, van den Boogaard J, Luning-Koster M, Evenboer KE, et al. COVID-19: Recovering at Home is not Easy. Ned Tijdschr Geneeskd. (2020) 164:D5358.
6. Moradi Y, Mollazadeh F, Karimi P, Hosseingholipour K, Baghaei R. Psychological disturbances of survivors throughout COVID-19 crisis: a qualitative study. BMC Psychiatry. (2020) 20:594. doi: 10.1186/s12888-020-03009-w
7. Missel M, Bernild C, Christensen SW, Dagyaran I, Berg SK. It's not just a virus! lived experiences of people diagnosed with COVID-19 infection in Denmark. Qual Health Res. (2021) 31:822–34. doi: 10.1177/1049732321990360
8. von Mackensen S, Halimeh S, Siebert M, Wermes C, Hassenpflug W, Holstein K, et al. Impact of COVID-19 pandemic on mental health of patients with inherited bleeding disorders in Germany. Haemophilia. (2020) 26:e272–e81. doi: 10.1111/hae.14130
9. Younger E, Smrke A, Lidington E, Farag S, Ingley K, Chopra N, et al. Health-related quality of life and experiences of sarcoma patients during the COVID-19 pandemic. Cancers (Basel). (2020) 12:288. doi: 10.3390/cancers12082288
10. Levy I, Sharf G, Norman S, Tadmor T. The impact of COVID-19 on patients with hematological malignancies: the mixed-method analysis of an Israeli national survey. Support Care Cancer. (2021) 29:7591–9. doi: 10.1007/s00520-021-06324-4
11. Philip KEJ, Buttery S, Williams P, Vijayakumar B, Tonkin J, Cumella A, et al. Impact of COVID-19 on people with asthma: a mixed methods analysis from a UK wide survey. BMJ Open Respir Res. (2022) 9:1056. doi: 10.1136/bmjresp-2021-001056
12. Mukhtar NB, Abdullahi A, Abba MA, Mohammed J. Views and experiences of discharged COVID-19 patients in Kano, Nigeria: a qualitative study. Pan Afr Med J. (2020) 37:38. doi: 10.11604/pamj.supp.2020.37.1.26609
13. Venturas M, Prats J, Querol E, Zabalegui A, Fabrellas N, Rivera P, et al. Lived experiences of hospitalized COVID-19 patients: a qualitative study. Int J Environ Res Public Health. (2021) 18:958. doi: 10.3390/ijerph182010958
14. Roberts ME, Knestrick J, Resick L. The lived experience of COVID-19. J Nurse Pract. (2021) 17:828–32. doi: 10.1016/j.nurpra.2021.04.013
15. Sun W, Chen WT, Zhang Q, Ma S, Huang F, Zhang L, et al. Post-traumatic growth experiences among COVID-19 confirmed cases in China: a qualitative study. Clin Nurs Res. (2021) 30:1079–87. doi: 10.1177/10547738211016951
16. Vottero B, Rittenmeyer L. The hospitalised patients' experience of being in protective/source isolation: a systematic review of qualitative evidence. JBI Libr Syst Rev. (2012) 10:935–76. doi: 10.11124/jbisrir-2012-63
17. Legido-Quigley H, Asgari N, Teo YY, Leung GM, Oshitani H, Fukuda K, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet. (2020) 395:848–50. doi: 10.1016/S0140-6736(20)30551-1
18. Walton H, Vindrola-Padros C, Crellin NE, Sidhu MS, Herlitz L, Litchfield I, et al. Patients' experiences of, and engagement with, remote home monitoring services for COVID-19 patients: a rapid mixed-methods study. Health Expect. (2022) 25:2386–404. doi: 10.1111/hex.13548
19. Hoffmann M, Stengel S, Szecsenyi J, Peters-Klimm F. Health care professionals' perspectives on the utilisation of a remote surveillance and care tool for patients with COVID-19 in general practice: a qualitative study. BMC Primary Care. (2022) 23:254. doi: 10.1186/s12875-022-01863-z
20. Teng K, Russo F, Kanuch S, Caron A. Virtual care adoption-challenges and opportunities from the lens of academic primary care practitioners. J Public Health Manag Pract. (2022) 28:599–602. doi: 10.1097/PHH.0000000000001548
21. Arnold L, Teichert U. Politischer Reformprozess im Zuge der COVID-19-pandemie: der Pakt für den Öffentlichen Gesundheitsdienst. Public Health Forum. (2021) 29:47–50. doi: 10.1515/pubhef-2020-0130
22. Shaban RZ, Nahidi S, Sotomayor-Castillo C, Li C, Gilroy N, O'Sullivan MVN, et al. SARS-CoV-2 infection and COVID-19: The lived experience and perceptions of patients in isolation and care in an Australian healthcare setting. Am J Infect Control. (2020) 48:1445–50. doi: 10.1016/j.ajic.2020.08.032
23. Ammar A, Mueller P, Trabelsi K, Chtourou H, Boukhris O, Masmoudi L, et al. Psychological consequences of COVID-19 home confinement: the ECLB-COVID19 multicenter study. PLoS One. (2020) 15:e0240204. doi: 10.1371/journal.pone.0240204
24. Toll K, Spark L, Neo B, Norman R, Elliott S, Wells L, et al. Consumer preferences, experiences, and attitudes towards telehealth: Qualitative evidence from Australia. PLoS ONE. (2022) 17:e0273935. doi: 10.1371/journal.pone.0273935
25. Creswell JW, Klassen AC, Plano Clark VL, Smith KC. Best practices for mixed methods research in the health sciences. Bethesda (Maryland). (2011) 2013:541–5. doi: 10.1037/e566732013-001
26. Noble H, Heale R. Triangulation in research, with examples. Evid Based Nurs. (2019) 22:67–8. doi: 10.1136/ebnurs-2019-103145
27. Demir SB, Pismek N. A convergent parallel mixed-methods study of controversial issues in social studies classes: a clash of ideologies. Educational Sci: Theory Pract. (2018) 18:119–49. doi: 10.12738/estp.2018.1.0298
28. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. (2013) 48:2134–56. doi: 10.1111/1475-6773.12117
29. O'Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ. (2010) 341:c4587. doi: 10.1136/bmj.c4587
30. Tonkin-Crine S, Anthierens S, Hood K, Yardley L, Cals JWL, Francis NA, et al. Discrepancies between qualitative and quantitative evaluation of randomised controlled trial results: achieving clarity through mixed methods triangulation. Implementation Science. (2016) 11:66. doi: 10.1186/s13012-016-0436-0
31. Unite for Sight. Survey Methodology. (2021). Available online at: http://www.uniteforsight.org/global-health-university/survey-methodologies (accessed December 21, 2022).
32. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
34. Microsoft Corporation. Microsoft Excel. Microsoft Corporation (2016). Available online at: https://office.microsoft.com/excel
35. Schilling J, Lehfeld A-S, Schumacher D, Diercke M, Buda S, Haas W, et al. Krankheitsschwere der ersten COVID-19-Welle in Deutschland basierend auf den Meldungen gemäß Infektionsschutzgesetz. J Health Monitor. (2020) S11:1–20. doi: 10.25646/7170
36. Kuckartz U. Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung 69 469 Weinheim: Beltz Verlagsgruppe. (2018).
37. MAXQDA 2020 (VERBI Software 2019). VERBI Software. MAXQDA 2020, computer program, VERBI Software, Berlin (2019). Available online at: https://www.maxqda.com/blogpost/how-to-cite-maxqda
38. DEGAM. Allgemeinmedizinischer Listserver: German College of General Practitioners and Family Physicians. (2022). Available online at: https://www.degam.de/allgemeinmed-listserver (accessed December 21, 2022).
39. Said D, Brinkwirth S, Taylor A, Markwart R, Eckmanns T. The containment scouts: first insights into an initiative to increase the public health workforce for contact tracing during the COVID-19 pandemic in Germany. Int J Environ Res Public Health. (2021) 18:9325. doi: 10.3390/ijerph18179325
40. Arevalo-Rodriguez I, Buitrago-Garcia D, Simancas-Racines D, Zambrano-Achig P, Del Campo R, Ciapponi A, et al. False-negative results of initial RT-PCR assays for COVID-19: a systematic review. PLoS ONE. (2020) 15:e0242958. doi: 10.1371/journal.pone.0242958
41. Dinnes J, Deeks JJ, Berhane S, Taylor M, Adriano A, Davenport C, et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev. (2021) 3:Cd013705. doi: 10.1002/14651858.CD013705
42. Roßmann K, Wegner H, Stark H, Großmann G, Jansen A, Frangoulidis D. COVID-19 Pandemic & bureaucracy: the crisis inside the crisis. Front Public Health. (2021) 9:665323. doi: 10.3389/fpubh.2021.665323
43. Kurotschka PK, Serafini A, Demontis M, Serafini A, Mereu A, Moro MF, et al. General practitioners' experiences during the first phase of the COVID-19 pandemic in Italy: a critical incident technique study. Front Public Health. (2021) 9:623904. doi: 10.3389/fpubh.2021.623904
44. Roehr B. Covid-19 is threatening the survival of US primary care. BMJ. (2020) 369:m2333. doi: 10.1136/bmj.m2333
45. Sun N, Wei L, Wang H, Wang X, Gao M, Hu X, et al. Qualitative study of the psychological experience of COVID-19 patients during hospitalization. J Affect Disord. (2021) 278:15–22. doi: 10.1016/j.jad.2020.08.040
46. Prokop J, Reid C, Palmateer B. Experiences with COVID-19. Nurs Res. (2022). doi: 10.1097/NNR.0000000000000583
47. Meyer-Frießem CH, Gierthmühlen J, Baron R, Sommer C, Üçeyler N, Enax-Krumova EK. Pain during and after COVID-19 in Germany and worldwide: a narrative review of current knowledge. Pain Rep. (2021) 6:e893. doi: 10.1097/PR9.0000000000000893
48. Buttery S, Philip KEJ, Williams P, Fallas A, West B, Cumella A, et al. Patient symptoms and experience following COVID-19: results from a UK-wide survey. BMJ Open Respir Res. (2021) 8:75. doi: 10.1136/bmjresp-2021-001075
49. Wang T, Du Z, Zhu F, Cao Z, An Y, Gao Y, et al. Comorbidities and multi-organ injuries in the treatment of COVID-19. Lancet. (2020) 395:e52. doi: 10.1016/S0140-6736(20)30558-4
50. Ogbodo JN, Onwe EC, Chukwu J, Nwasum CJ, Nwakpu ES, Nwankwo SU, et al. Communicating health crisis: a content analysis of global media framing of COVID-19. Health Promot Perspect. (2020) 10:257–69. doi: 10.34172/hpp.2020.40
51. Heiberg KE, Jøranson N, Heggestad AKT, Breievne G, Lausund H, Myrstad M, et al. “This path I must walk alone”. Challenges experienced by older patients while recovering from severe COVID-19– a qualitative study. BMC Geriatr. (2022) 22:253. doi: 10.1186/s12877-022-02959-y
52. Verberk JDM, Anthierens SA, Tonkin-Crine S, Goossens H, Kinsman J, de Hoog MLA, et al. Experiences and needs of persons living with a household member infected with SARS-CoV-2: a mixed method study. PLoS ONE. (2021) 16:e0249391. doi: 10.1371/journal.pone.0249391
53. Sandvik H, Hetlevik Ø, Blinkenberg J, Hunskaar S. Continuity in general practice as predictor of mortality, acute hospitalisation, and use of out-of-hours care: a registry-based observational study in Norway. Br J Gen Pract. (2022) 72:e84–90. doi: 10.3399/BJGP.2021.0340
54. Gao B, Dong J. Does the Impact of COVID-19 Improve the doctor-patient relationship in China? Am J Med Sci. (2020) 360:305–6. doi: 10.1016/j.amjms.2020.05.039
55. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
56. Greenhalgh T, Knight M, Inda-Kim M, Fulop NJ, Leach J, Vindrola-Padros C. Remote management of covid-19 using home pulse oximetry and virtual ward support. BMJ. (2021) 372:n677. doi: 10.1136/bmj.n677
57. Due TD, Thorsen T, Andersen JH. Use of alternative consultation forms in Danish general practice in the initial phase of the COVID-19 pandemic–a qualitative study. BMC Fam Pract. (2021) 22:108. doi: 10.1186/s12875-021-01468-y
58. Johnsen TM, Norberg BL, Kristiansen E, Zanaboni P, Austad B, Krogh FH, et al. Suitability of video consultations during the COVID-19 pandemic lockdown: cross-sectional survey among norwegian general practitioners. J Med Internet Res. (2021) 23:e26433. doi: 10.2196/26433
59. Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: a call to action. JMIR Public Health Surveill. (2020) 6:e18810. doi: 10.2196/18810
60. Danchin M, Biezen R, Manski-Nankervis JA, Kaufman J, Leask J. Preparing the public for COVID-19 vaccines: How can general practitioners build vaccine confidence and optimise uptake for themselves and their patients? Aust J Gen Pract. (2020) 49:625–29. doi: 10.31128/AJGP-08-20-5559
61. DePuccio MJ, Gaughan AA, Shiu-Yee K, McAlearney AS. Doctoring from home: Physicians' perspectives on the advantages of remote care delivery during the COVID-19 pandemic. PLoS ONE. (2022) 17:e0269264. doi: 10.1371/journal.pone.0269264
62. Hughes G, Moore L, Maniatopoulos G, Wherton J, Wood GW, Greenhalgh T, et al. Theorising the shift to video consulting in the UK during the COVID-19 pandemic: analysis of a mixed methods study using practice theory. Soc Sci Med. (2022) 311:115368. doi: 10.1016/j.socscimed.2022.115368
63. Bratan T, Schneider D, Heyen NB, Pullmann L, Friedewald M, Kuhlmann D, et al. E-Health in Deutschland: Entwicklungsperspektiven und internationaler Vergleich, No 12–2022, Studien zum deutschen Innovationssystem, Expertenkommission Forschung und Innovation (EFI) – Commission of Experts for Research and Innovation. Berlin. (2022).
64. Aerzteblatt. Krankenhausreform: Lauterbach will mehr ambulante Behandlungen. Deutsches Aerzteblatt. (2022). Available online at: https://www.aerzteblatt.de/nachrichten/138206/Krankenhausreform-Lauterbach-will-mehr-ambulante-Behandlungen (accessed December 21, 2022).
65. Van Grootven B, Irusta LA, Christiaens W, Mistiaen P, De Meester C, Cornelis J, et al. Experiences with the implementation of remote monitoring in patients with COVID-19: a qualitative study with patients and healthcare professionals. J Nurs Scholarsh. (2022). doi: 10.1111/jnu.12814. [Epub ahead of print].
66. Donno DR, Grattagliano I, Rossi A, Lora Aprile P, Medea G, Lagolio E, et al. How to treat COVID-19 patients at home in the Italian context: an expert opinion. Infect Dis Rep. (2021) 13:251–8. doi: 10.3390/idr13010028
67. Alboksmaty A, Beaney T, Elkin S, Clarke JM, Darzi A, Aylin P, et al. Effectiveness and safety of pulse oximetry in remote patient monitoring of patients with COVID-19: a systematic review. Lancet Digital Health. (2022) 4:e279–e89. doi: 10.1016/S2589-7500(21)00276-4
68. Ufholz K, Sheon A, Bhargava D, Rao G. Telemedicine preparedness among older adults with chronic illness: survey of primary care patients. JMIR Form Res. (2022) 6:e35028. doi: 10.2196/35028
69. Aerny-Perreten N, Domínguez-Berjón MF, Esteban-Vasallo MD, García-Riolobos C. Participation and factors associated with late or non-response to an online survey in primary care. J Eval Clin Pract. (2015) 21:688–93. doi: 10.1111/jep.12367
70. Harrison S, Henderson J, Alderdice F, Quigley MA. Methods to increase response rates to a population-based maternity survey: a comparison of two pilot studies. BMC Med Res Methodol. (2019) 19:65. doi: 10.1186/s12874-019-0702-3
71. McKernan SC, Reynolds JC, McInroy B, Damiano PC. Randomized experiment on the effect of incentives and mailing strategy on response rates in a mail survey of dentists. J Public Health Dent. (2022) 82:484–90. doi: 10.1111/jphd.12510
Keywords: COVID-19, patients' experience, illness experience, mixed methods, general practice, home isolation, Germany, telehealth
Citation: Parisi S, Lehner N, Schrader H, Kierer L, Fleischer A, Miljukov O, Borgulya G, Rüter G, Viniol A and Gágyor I (2023) Experiencing COVID-19, home isolation and primary health care: A mixed-methods study. Front. Public Health 10:1023431. doi: 10.3389/fpubh.2022.1023431
Received: 19 August 2022; Accepted: 12 December 2022;
Published: 10 January 2023.
Edited by:
Suneela Garg, University of Delhi, IndiaReviewed by:
Daisy Volmer, University of Tartu, EstoniaCopyright © 2023 Parisi, Lehner, Schrader, Kierer, Fleischer, Miljukov, Borgulya, Rüter, Viniol and Gágyor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sandra Parisi,  UGFyaXNpX1NAdWt3LmRl
UGFyaXNpX1NAdWt3LmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.