 Hong Guo
Hong Guo- Department of Public Health, Shihezi University School of Medicine, Xinjiang, China
Background: To study the corresponding strategies for controlling cancer in older adults aged 60 and above in China, a comprehensive assessment of disease burden is required. Therefore, we will introduce the cancer epidemiological characteristics of older adults in China over a recent 12 year period.
Methods: The age-period-cohort model was constructed using the cancer incidence data from the Chinese Cancer Registry Annual Report published in 2008–2019. The annual change percentage (APC) was estimated by log-linear regression to reflect the time trend. The data from the GLOBOCAN 2020 database was selected for worldwide comparative analysis.
Results: The cancer incidence in older adults aged 60 and above in China showed a decreasing trend (APC = −0.73%, P = 0.009). The urban/rural ratio of cancer incidence increased from 0.94 to 1.07 (t = 3.52, P < 0.05), while the sex ratio (male/female) showed a significant decreasing trend only in rural areas (t = −6.77, P < 0.05), and the ratio decreased from 2.02 to 1.72. The results of the age-period-cohort model showed that the cancer incidence increased with age in both males and females, urban and rural areas. The RR of period effect increased from 2005 to 2010, then decreased from 2010 to 2015, and the downward trend was more obvious. The RR of the later-born cohort was lower than that of the earlier-born cohort in rural areas. Lung, gastric, colorectal, esophageal, liver, and breast cancers were common cancers in Chinese older adults. Lung cancer incidence ranked first in males, and it decreased with time in the 75–79 and 80–84 age groups (APC75 − 79 = −1.10%, APC80 − 84 = −0.88%, all P < 0.05). Breast cancer incidence ranked first among female in the 60–64 age group and showed an increasing trend (APC60 − 64 = 1.52%, P < 0.05).
Conclusions: The cancer incidence in Chinese older adults aged 60 and above showed a decreasing trend, but it was still at a relatively high level. The key targets of prevention and treatment should be males, urban areas, younger people, older adults aged 60–69, lung, gastrointestinal, and breast cancers in the future.
Introduction
Global aging is increasingly serious. Take France, which was the first to enter an aging society, as an example. In 2015, the number of people aged 60 and above in France exceeded that of 0–14 years. If fertility remains low, France's population will fall by 13.5% in 2050. With the reversal of the age structure of the French population, the median age will rise to an unprecedented age of 45–50, and France will enter the era of an inverted population pyramid (1). Japan, which is quite similar to China in social and cultural aspects, has an aging situation. It is estimated that in 2030, more than 40% of Japan's working population will be 60 or older. Long-term ultra-low fertility rate and rising life expectancy will lead to slow population decline and aging in these decades, and the growth of Gross Domestic Product (GDP) and per-capita GDP will slow down (2). Obviously, the impact of aging is not limited to changes in the proportion of older adults, but will reshape the age structure of various countries' populations and bring a series of social problems.
China has become an aging society, at an exponential rate. In the past decade, the aging rate of China has surpassed that of Japan (3). In 1999, older adults aged 60 above accounted for 10% of the total population, marking that China has officially entered an aging society (4). Since then, China has entered a period of rapid development of population aging. The number of people aged over 60 in China has reached 264 million in 2020, accounting for 19% of the total population (5). Meanwhile, it is estimated that by 2030, people aged 60 years or above will exceed 25% (6). As the population ages, society and families are facing significant issues. How to deal with the aging population and improve the quality of life of older adults has become a prominent topic in recent studies. According to the study, the cancer incidence in elders in China from 2006 to 2010 was 8.18 times that of the young and middle-aged groups, and the risk of cancer was also higher (7). Furthermore, in a review of the death causes of Chinese older adults between 1990 and 2019, cancer was the second leading cause (8). The prevention and control of cancers in older people have become one of the important public health problems in China.
Concurrently, China has issued policy documents such as the Healthy China Action (2019–2030) and Outline of the Healthy China 2030 Plan, which regard the prevention and control of cancers as one of the 15 key special actions, and older adults as one of the key groups. The purpose of this study was to construct an age-period-cohort model and estimate the APC by log-linear regression to conduct a comprehensive study on the epidemic characteristics of cancers among older adults aged 60 and above in China from 2005 to 2016, so as to provide a reference basis for the prevention and control of cancers in China.
Methods
Data sources
In this study, the cancer incidence data among older adults aged 60 and above in China from 2005 to 2016 were selected from the Chinese Cancer Registry Annual Report compiled by the National Cancer Center (NCC) published in 2008–2019 (9–20). During this period, the number of cancer registries in China increased from 45 in 2008 to 682 in 2019, with a coverage rate of 27.60%.
The regional distribution of this study was based on the classification criteria in the Chinese Cancer Registry Annual Report: cities above prefecture level were urban areas, and counties and county-level cities were rural areas.
The cancer incidence data in the world and countries with different Human Development Index (HDI) were selected from the GLOBOCAN 2020 database for comparative analysis (21).
Analysis index
According to the international classification of diseases (ICD-10) (22), the incidence, age-specific incidence rate, constituent ratio (%), sex incidence ratio (male/female, SIR), regional incidence ratio (urban/rural, RIR), age-standardized rate (ASR), age-standardized incidence rate of the world (ASRW) and annual percent change (APC) of all cancers (C00–C96) was calculated.
APC was used to describe the trend of cancers in older adults for 12 years. The natural logarithm of the incidence rate (r) is represented by y, that is, y = ln(r). Then, with y as the dependent variable and x (year) as the independent variable, a regression linear model is fitted: y = α+βx+ε, where α is a constant term, β is a regression coefficient, and ε is a random error term.
If the trend of incidence does not change, that is, APC = 0 (invalid hypothesis), the statistical test of APC can be based on whether β is equal to 0 or not. The 95% confidence interval (CI) of APC is estimated to be:
Statistical methods
Stratification was carried out according to different regions (urban and rural), sex, age groups (60–64, 65–69, 70–74, 75–79, 80–84, and ≥85 years) and time (2005–2016). Assuming that the cancer cases in the population follow the Poisson distribution, the SAS statistical software Genmod module was used to fit the Poisson regression, with the log of the population as an offset variable, the dependent variable was the incidence, and the independent variables were sex, urban and rural. The annual RIR, SIR and its 95%CI (adjusted region and sex) were calculated, and the linear regression was used to test the ratio trend (23).
The time trend of cancer incidence was analyzed by APC and its 95%CI. With the log of cancer incidence as the dependent variable, the regression coefficient β of log-linear regression was used to estimate the APC (24, 25). “Increase” or “decrease” was used to describe a statistically significant trend.
The expression of the age-period-cohort model was as follows:
where R is the outcome variable of an event, such as incidence (/105); P represents the population of age group i in the period group j; u stands for intercept term of incidence; α, β, γ represent age, period and cohort effect at all levels, respectively, and ε is residual. The relative risk (RR) is the exponential value of the coefficient (26, 27).
To avoid expanding the scope of the birth cohort and affecting the time accuracy of disease risk description, the age-specific data of 2005, 2010, and 2015 were selected to simulate the age-period-cohort model (28). For the collinearity problem existing in the classical age-period-cohort model, the intrinsic estimator approach was used to solve the collinearity problem in the age-period-queue model (29, 30), and the fitting superiority of the Comprehensive Evaluation Model based on the Akaike information criterion.
Results
Overall situation
In 2005–2016, there were 3,478,089 cases of cancers in Chinese people aged 60 and above, and the median incidence was 1,057.56/105 (range, 997.89/105 ~ 1,123.32/105). The cancer incidence showed a decreasing trend during this period (APC = −0.73%, P = 0.009) (Table 1).
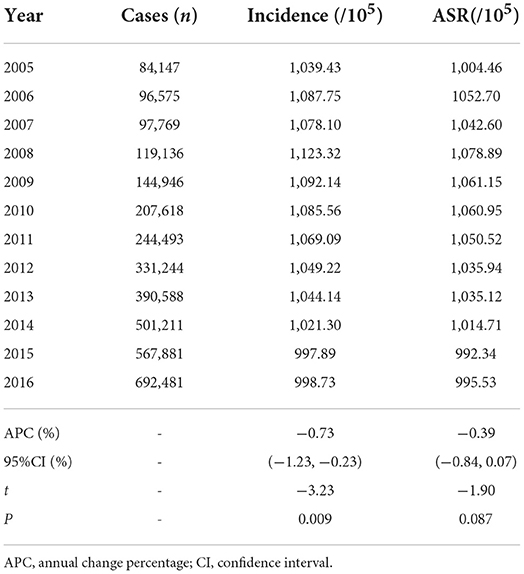
Table 1. Cancer incidence in Chinese older adults aged 60 and above from 2005 to 2016.
In 2016, a total of 692,480 cases occurred. Among them, the proportion of each age group was: 23.6% for 60–64 years (163,727 cases), 21.7% for 65–69 years (149,994 cases), 18.5% for 70–75 years (128,171 cases), 16.6% for 75–79 years (115,125 cases), 12.3% for 80–84 years (84,953 cases), and 7.3% for ≥ 85 years (50,510 cases). The cancer cases of males accounted for 61.0% (422,399 cases), that of females accounted for 39.0% (270,081 cases). The proportion for urban and rural areas were 53.9% (373,176 cases) and 46.1% (319,304 cases), respectively.
Sex-specific
The cancer incidence showed a decreasing trend in males and females, and the trend was more obvious in males (APCmales = −1.00%, APCfemales = −0.63%, all P < 0.05). For different regions, the cancer incidences of males and females in urban were stable (all P > 0.05), however, that of rural males showed a decreasing trend (APC = −2.10%, P < 0.05) (Table 2). The SIR of older adults in China and urban areas was stable (all P > 0.05). However, the SIR in rural areas decreased from 2.02 in 2005 to 1.72 in 2016 (P < 0.05) (Table 3).
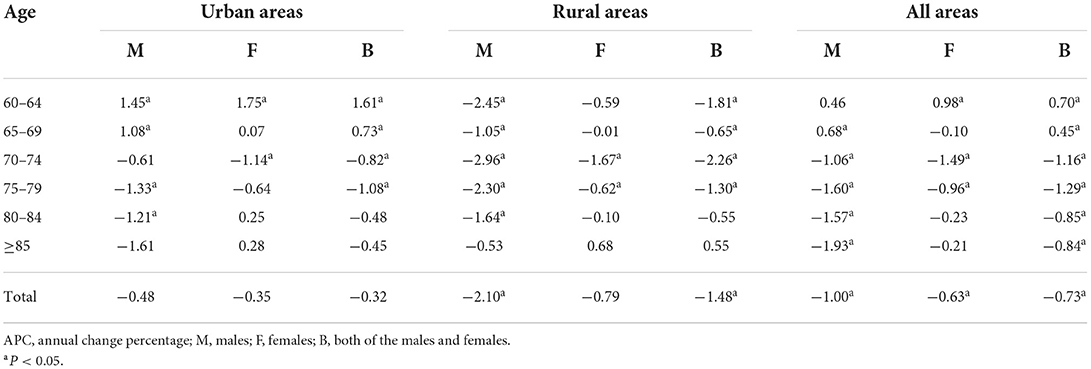
Table 2. The APC of cancer incidence in Chinese older adults aged 60 and above with different characteristics from 2005 to 2016 (%).
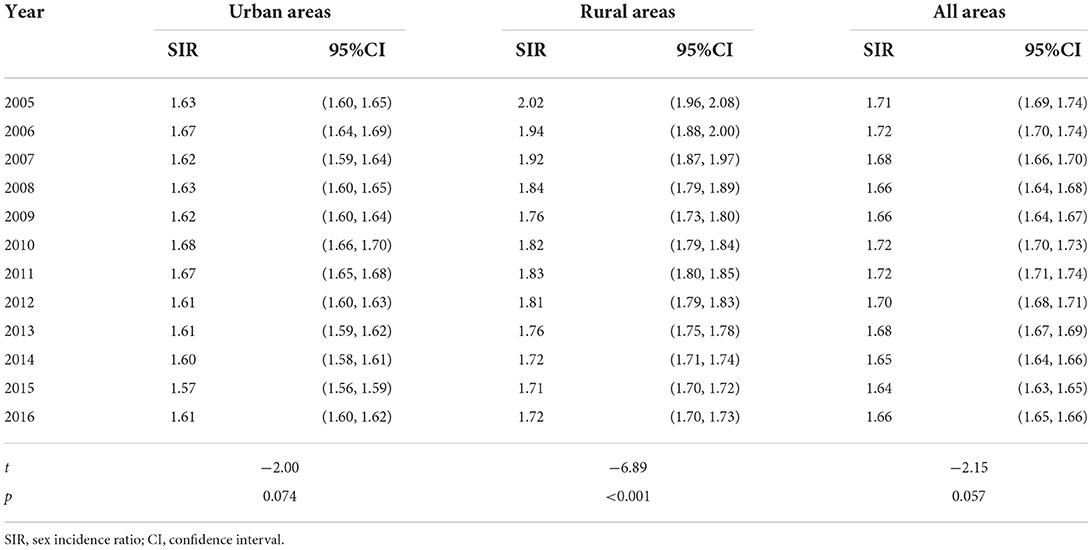
Table 3. The sex (male/female) incidence ratio in Chinese older adults aged 60 and above from 2005 to 2016.
Region-specific
According to the data of the GLOBOCAN2020 database, the cancer incidences among older adults in United States, Britain, Japan, South Korea and China were 1,386.4/105, 2,061.0/105, 1,829.7/105, 1,615.0/105, 1,156.8/105, 1,060.2/105, respectively. The cancer incidence in Chinese older adults was lower than that in countries with very high HDI and the world average level (Figure 1).
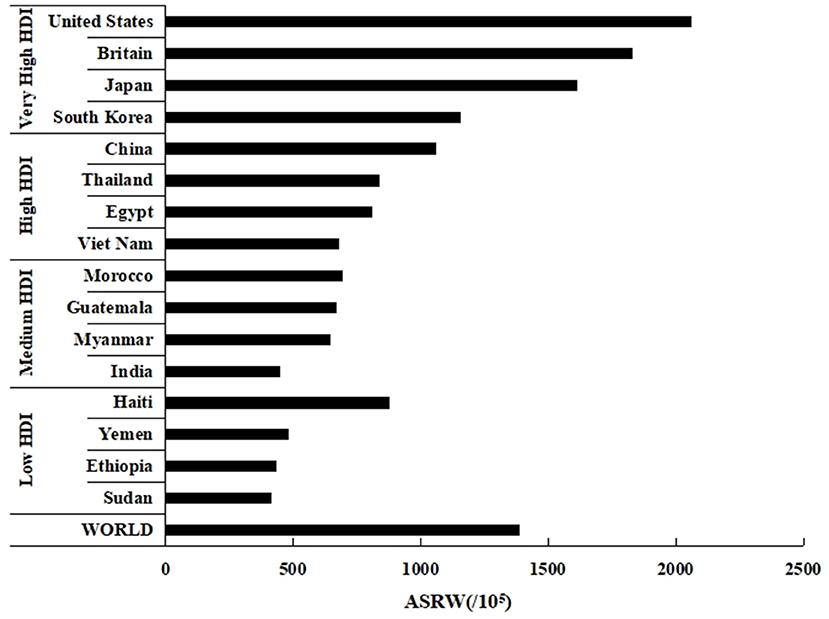
Figure 1. Estimated age-standardized incidence rates of cancers in older adults aged 60 and above in countries with different HDI in 2020 (Date source: GLOBOCAN 2020, https://gco.iarc.fr/today/).
The cancer incidence among older adults in urban areas was stable (P > 0.05), while in rural areas it showed a decreasing trend (APC = −1.48%, P < 0.05) (Table 2). In 2005, the RIR was 0.94 among Chinese older adults. By 2016, the RIR increased to 1.07 (P < 0.05). The RIR among females was stable (P > 0.05). However, the RIR among males increased from 0.86 in 2005 to 1.04 in 2016 (P < 0.05) (Table 4).
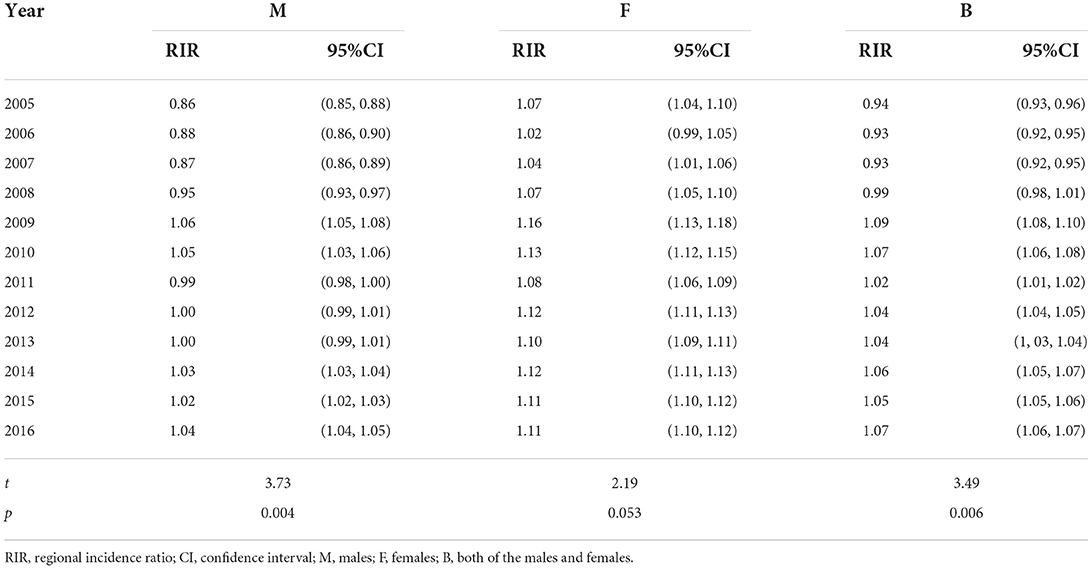
Table 4. The regional (urban/rural) incidence ratio in Chinese older adults aged 60 and above from 2005 to 2016.
Age-period-cohort analysis
Age effect: among the Chinese older adults aged 60 and above, whether males or females, urban or rural areas, the cancer incidence increased first and then decreased with age, reaching a peak in the 80–84 age group.
Period effect: for males and females, the RR increased from 2005 to 2010, then decreased from 2010 to 2015, and the downward trend was more obvious. The RR in rural areas decreased from 2005 to 2015.
Cohort effect: for males, females, and urban areas, the RR decreased in birth-cohorts born from 1935 to 1949 and increased in birth-cohorts born from 1950 to 1959. In rural areas, the RR deceased in birth-cohorts born from 1935 to 1959 (Figures 2A–D).
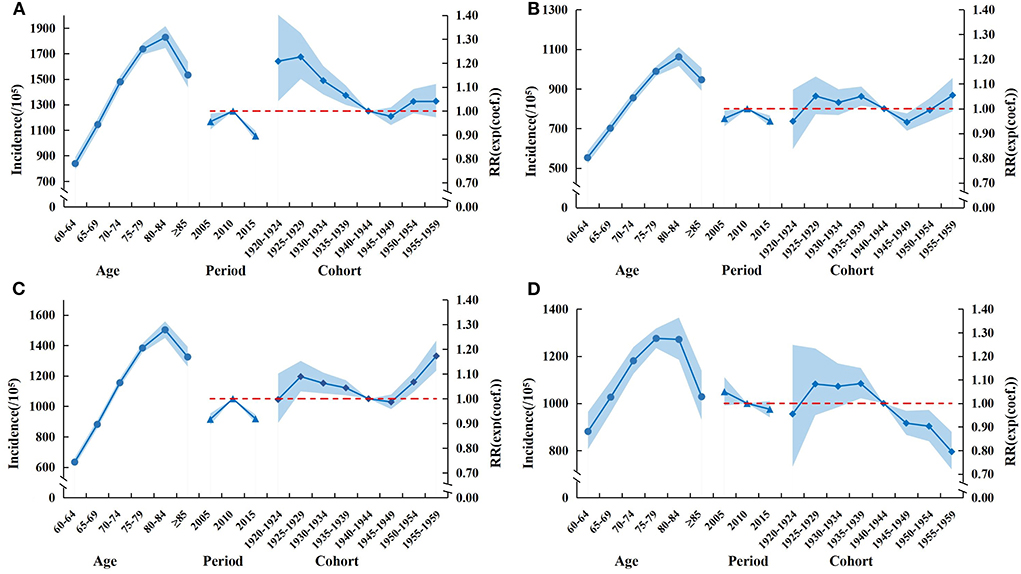
Figure 2. Age-period-cohort model of cancer incidence in Chinese older adults aged 60 and above from 2005 to 2016. (A) Male. (B) Female. (C) Urban. (D) Rural.
Cancer composition
Lung cancer ranked first among Chinese older adults from 2005 to 2016, with a total of 844,286 cases, and followed by gastric, colorectal, esophageal, liver, breast, prostate, pancreatic, bladder cancers and lymphoma, the top 10 cancer cases accounted for about 81.6% of all cancers. Similarly, for males and females, the lung cancer ranked first, with 567,608 cases and 276,678 cases, respectively. It was followed by gastric, colorectal, esophageal, liver, prostate, bladder, pancreatic, lymphoma and oral cavity and pharynx cancer in males. The top 10 cancer cases accounted for 89.1% of all male cancers. In females, the incidence of lung cancer was followed by those of colorectal, gastric, breast, esophageal, liver, pancreatic, gallbladder, brain and nervous system, corpus uteri and uterus unspecified cancer, the top 10 cancers accounted for about 80.1% of all cancers (Figures 3A–C).
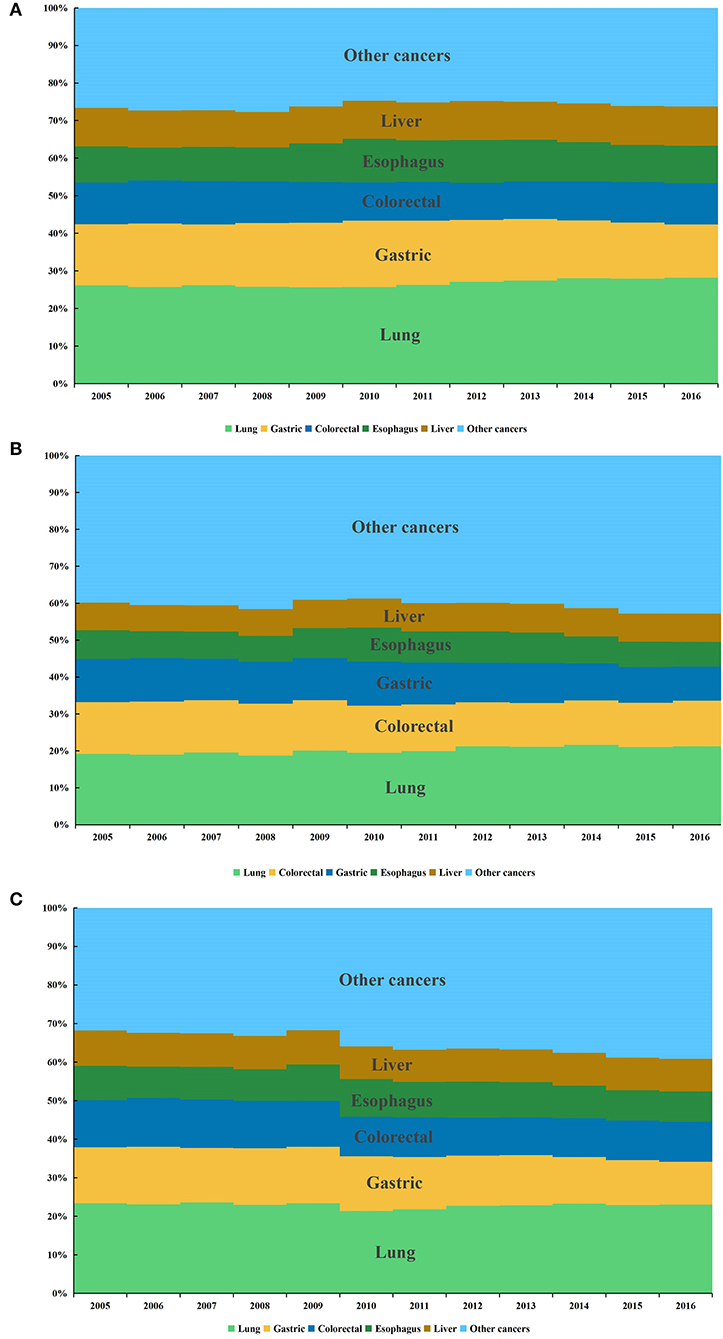
Figure 3. Composition of cancers in Chinese older adults aged 60 and above from 2005 to 2016. (A) Male. (B) Female. (C) Both.
Time trend of the top five cancers in different sexes and ages
For males: lung cancer incidence ranked first in all age groups and it increased with time in 60–64 and 65–69 age groups (APC60 − 64 = 2.22%, APC65 − 69 = 1.87%, all P < 0.05), while it decreased in 75–79 and 80–84 age groups (APC75 − 79 = −1.10%, APC80 − 84 = −0.88%, all P < 0.05). Gastric cancer incidence showed a decreasing trend in 60–64, 70–74, 75–79, and 80–84 age groups (APC60 − 64 = −1.94%, APC70 − 74 = −1.87%, APC75 − 79 = −2.02%, APC80 − 84 = −1.95%, all P < 0.05). Colorectal cancer incidence increased in 60–64 age group (APC60 − 64 = 1.07%, P < 0.05), while it decreased in 70–74, 75–79, 80–84 and ≥85 age groups (APC70 − 74 = −2.72%, APC75 − 79 = −2.51%, APC80 − 84 = −1.89%, APC≥85 = −2.12%, all P < 0.05). Liver cancer incidence increased in 65–69 age group (APC65 − 69 = 0.76%, P < 0.05), while it decreased in 75–79 and 80–84 age groups (APC75 − 79 = −1.18%, APC80 − 84 = −1.43%, all P < 0.05) (Figure 4A).
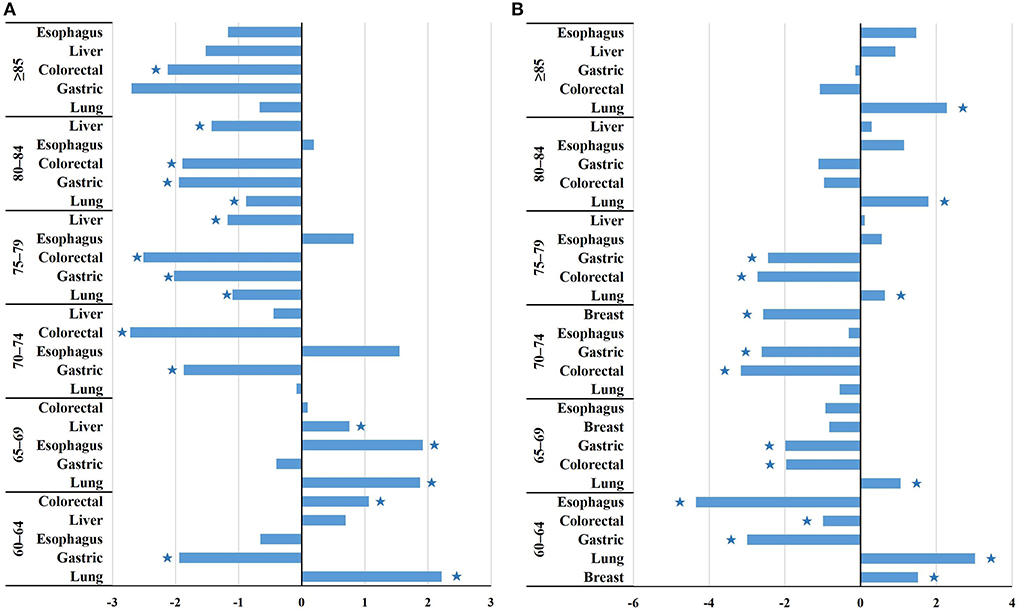
Figure 4. The changing trend of the incidence of the top five cancers among Chinese older adults aged 60 and above of different genders and different age groups from 2005 to 2016. *P < 0.05. (A) Male. (B) Female.
For females: breast cancer ranked first in 60–64 age group and increased with time (APC60 − 64 = 1.52%, P < 0.05), while it decreased in 70–74 age group (APC70 − 74 = −2.58%, P < 0.05). Lung cancer incidence ranked first among older females except for the 60–64 age group and showed an increasing trend in 60–64, 65–69, 80–84 and ≥85 age groups (APC60 − 64 = 3.02%, APC65 − 69 = 1.06%, APC80 − 84 = 1.79%, APC≥85 = 2.28%, all P < 0.05). Gastric cancer incidence decreased in 60–64, 65–69, 70–74 and 75–79 age groups (APC60 − 64 = −3.00%, APC65 − 69 = −1.99%, APC70 − 74 = −2.61%, APC75 − 79 = −2.45%, all P < 0.05). Similar to gastric cancer, colorectal cancer decreased in 60–64, 65–69, 70–74 and 75–79 age groups (APC60 − 64 = −0.99%, APC65 − 69 = −1.97%, APC70 − 74 = −3.16%, APC75 − 79 = −2.73%, all P < 0.05). Esophagus cancer incidence showed a decreasing trend in 60–64 age group (APC60 − 64 = −4.35%, P < 0.05) (Figure 4B).
Discussion
Based on the cancer incidence data collected by the NCC from 2005 to 2016, the present study analyzed the cancer epidemic characteristics in Chinese older adults aged 60 years and above over a recent 12 year period. The results showed a decreasing trend in the cancer incidence of older adults from 2005 to 2016, but the incidence was still at a high level. The most economical strategy to reduce the cancer incidence should be primary prevention. The Chinese government has implemented a number of health promotion initiatives, including the national cancer prevention and control plan (1986–2000 years) and the programme of cancer prevention and control in China (2004–2010 years) (31, 32). The reduction in cancer incidence among Chinese older adults may be consistent with the implementation of these initiatives.
Numerous studies have shown that smoking may increase the risk of more than 15 cancers, including lung, esophageal, gastric and liver cancer (33, 34). China has been making efforts to reduce tobacco use, including increasing fees and outlawing smoking in enclosed public spaces (35). Although the benefits of these initiatives have started to be felt, they are insufficient. Studies have shown that in 2019, the smoking prevalence in China was 24.3%, of which 49.7% for male and 3.54% for female. Compared with 32.7% of the global male smoking prevalence, the prevalence of Chinese male smoking was at a higher level, which was also significantly higher than that in very high HDI countries, such as the United States (19.9%), Britain (21.7%) and Japan (33.4%) (36).
However, this study found that the cancer incidence in Chinese older adults was lower than that in countries with very high HDI, such as the United States, Britain, South Korea, Japan. Some studies found that the smoking-caused respiratory and circulatory diseases [Respiratory and circulatory diseases accounted for 85.1% of Chinese older adults suffering from chronic diseases in 2016 (37), and the prevalence was higher than that in countries with very high HDI (8, 38, 39)] may reduce the proportion of Chinese older adults to accept cancer screening and their willingness to seek medical advice (40, 41), this phenomenon could mask the true cancer incidence of Chinese older adults. For example, we known that a national cancer screening program was launched by the Chinese government in 2005, covering eight common cancers, including lung, breast and colorectal cancer (42). But studies have shown that people with comorbidities were 0.79, 0.62, and 0.93 times likely to be screened for lung, breast and colorectal cancer than those without chronic conditions, respectively (43, 44). And a study of lung cancer patients showed that patients with chronic obstructive pulmonary disease (COPD) took twice as long to consult with lung cancer symptoms (45). Therefore, China should continue to take strong measures to control the smoking prevalence in order to reduce the occurrence of respiratory and other diseases, increase the likelihood of participating in cancer screening, and reduce the disease burden.
In addition, the cancer incidence among older people in a country is also related to factors such as the number and life expectancy of older adults (46, 47). The relatively lower life expectancy in China compared to countries with very high HDI may also contribute to the low cancer incidence in Chinese older adults (48). In 2019, the coverage rate of China's cancer registry was 27.60%, while as of July 2019, the coverage rate of the US cancer registration system was 96%, and that of the United Kingdom and South Korea was close to 100% (49). Incomplete coverage of cancer registries may lead to the low incidence among Chinese older adults. Therefore, improving the construction of China's cancer registration system, making full use of big data and new information technology and achieving accurate monitoring of cancers are prerequisites for understanding the epidemic trend of cancers among Chinese older adults (50).
From the perspective of the differences between urban and rural areas in China, the cancer incidence among older adults in rural areas was decreased, while the incidence in urban areas was stable. There has been a reversal of the incidence ratio between urban and rural areas in China. In 2005, the incidence in rural areas was 6% higher than that in urban areas; by 2016, the incidence in urban areas was 7% higher than that in rural areas. This may be due to differences in living habits, eating habits, and environmental pollution between urban and rural areas (51). The large number of rural migrant elderly people choosing to seek medical treatment in cities and the growing awareness of cancer prevention among rural residents may also contribute to this phenomenon (52–54). For example, China launched a major national health care reform project “early diagnosis and early treatment of cancer in rural areas” in 2009 and launched screening work for high-risk groups such as lung cancer in rural areas (55). Moreover, the decreasing trend in cancer incidence among rural older adults was mainly reflected in male with more serious morbidity, and the sex ratio dropped from 2.02 in 2005 to 1.72 in 2016. This may be related to the cancer control strategy taken for male high-risk groups in China.
Aging is a risk factor for cancer. Theoretically, the cancer incidence increases with age. Countries with very high HDI levels, such as the United States and Japan, have shown this trend (56, 57). However, the results of this study showed that the cancer incidence in older people aged 85 years and above was lower than that in the 75–79 and 80–84 groups, which may be due to the competitive death of diseases such as the circulatory and respiratory systems after 80 years of age (8). This may also be due to the decrease in the possibility of seeing a doctor in the group aged ≥ 85 years, which could lead to missed diagnosis (58).
The cohort effect is regarded as the interaction between age growth and period change, which shows that after suffering specific historical events, the change of exposure risk factors affects all age groups at the same time, and different birth cohorts often have different risks (59). In this study, whether male or female, urban or rural areas, the RR decreased in birth-cohorts born from 1935 to 1949. It indicated that people born during this period experienced a lower risk of cancer. Environmental improvements may reduce the risk of cancer (60). With China's industrial reforms in 1920 (61), air pollution began to improve, and environmental change could have a lasting impact on people born between 1935 and 1949, which may promote cancer prevention. Therefore, environment management should be continued to prevent cancer.
In terms of the cancer composition, lung, gastric, and colorectal cancers were the main cancers that threaten the health of Chinese older adults, among which lung cancer ranked first in both male and female. The top 10 cancers in Chinese older adults were the same as those in countries with very high HDI, but the order was different. China had a high incidence of lung cancer and digestive system cancers, such as liver, gastric, and esophageal cancers, whereas countries with very high HDI in Europe and the United States had a high incidence of thyroid, breast, and prostate cancers (62–64). The difference between the cancer spectrum in China and that in countries with very high HDI has caused a serious disease burden in China. China should expand the screening of cancers and vigorously perform health education to reduce the incidence of related cancers among older adults. Lung cancer showed an increasing trend among Chinese older females except the 70–74 and 75–79 age groups, however, it decreased among males aged 75–79 and 80–84 age groups. The different trends may be related to the change in the concept of smoking, the decrease in smoking prevalence in males with age, and the increase in females (65, 66). Females' exposure to second-hand smoke, outdoor air pollution and the use of indoor solid fuels for heating and cooking may also contribute to an increased incidence of lung cancer (67, 68). Breast cancer ranked first in older females aged 60–64 years, and showed an increasing trend, suggesting that older females of 60–64 years should be considered as the key object of prevention and treatment of breast cancer. Although the incidence of gastric cancer and colorectal cancer in Chinese older adults showed an overall decreasing trend, gastrointestinal cancers still had a high incidence. Screening and treatment of gastrointestinal cancers should be strengthened to reduce the disease burden.
In summary, the cancer incidence in Chinese older adults showed a decreasing trend, but it was still high. The incidence of Chinese older males was higher than that of females, and the incidence of urban elderly was higher than that in rural areas. The cancer incidence increased with age in both males and females, urban and rural areas. The RR of the later-born cohort was lower than that of the earlier-born cohort in rural areas. In the future, China should regard males, urban, and low-age elderly as the key population for the prevention and treatment of cancer, and focus on the control of lung, gastrointestinal, breast, and other major cancers that threaten the health of Chinese older adults. In addition, more attention should be paid to prevention and treatment of cancer in the younger population, which may reduce the cancer risk in the old age and may even reduce the cancer incidence in the population as a whole.
Data availability statement
The original contributions presented in the study are included in the article/supplementary files, further inquiries can be directed to the corresponding authors.
Author contributions
YY, HG, and KL initiated the study. HG, KL, KY, ZM, and MC collected and processed the data. HG and KL performed the statistical analysis, visualization, and drafted the manuscript. YH and YY revised the manuscript. All authors read, contributed to the framework construction, result interpretation, manuscript revision, and approved the final version of the manuscript.
Funding
This study was funded by the Shihezi University High-Level Talent Project (No. RCZK2021B28) and the Shihezi Science and self-Funded project of ShiHezi University (No. ZZZC202125).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
GDP, Gross Domestic Product; NCC, National Cancer Center; HDI, Human Development Index; APC, annual change percentage; SIR, sex incidence ratio; RIR, regional incidence ratio; ASR, age-standardized rate; ASRW, age-standardized incidence rate of the world; CI, confidence interval; RR, relative risk; M, males; F, females; B, both of the males and females.
References
1. Chesnais J-C. The inversion of the age pyramid and the future population decline in France: implications and policy responses. New York: United Nations. (2002).
2. Clark RL, Ogawa N, Kondo M, Matsukura R. Population decline, labor force stability, and the future of the Japanese economy. Eur J Popul. (2009) 26:207–27. doi: 10.1007/s10680-009-9179-9
3. Tao T, Wang NL, Zhang HQ. Identical Origin Point Ageing Path and Socio-Economic Impacts: A Multiple-Country Comparison. Populat Res. (2019) 43:28–42.
4. Pan JY, Xu T, Xuan Y. Population aging, human capital and economic growth. Inq Econom Issu. (2022) 7:74–89.
5. National Bureau of Statistics of the People's Republic of China. China's National Population Census. (2022). Available online at: http://www.stats.gov.cn/tjsj/pcsj/ (accessed March 16, 2022).
6. United Nations. World Population Prospects. (2017). Available online at: https://esa.un.org/unpd/wpp/ (accessed April 15, 2017).
7. Zhang XF, Yan YZ, Pang LJ, Guo SX, Niu Q, Xu SZ, et al. Cancer disease burden of older adults in China. Chin J Gerontol. (2017) 37:5325–9.
8. Ma MH, Han YH. Analysis of death causes of the elderly in different regions of china since 1990. Chin Heal standard management. (2021) 12:16–9.
9. Zhao P, Chen WQ. 2008 China Tumor Registration Annual Report. (2009). Beijing: Military Medical Sciences Press.
10. Zhao P, Chen WQ. 2009 China Tumor Registration Annual Report. (2010). Beijing: Military Medical Sciences Press.
11. Zhao P, Chen WQ. 2010 China Tumor Registration Annual Report. (2011). Beijing: Military Medical Sciences Press.
12. He J, Zhao P, Chen WQ. 2011 China Tumor Registration Annual Report. (2012). Beijing: Military Medical Sciences Press.
13. He J, Chen WQ. 2012 China Tumor Registration Annual Report. (2013). Beijing: Military Medical Sciences Press.
14. He J, Chen WQ. 2013 China Tumor Registration Annual Report. (2017). Beijing: Tsinghua University Publishing House.
15. He J, Chen WQ. 2014 China Tumor Registration Annual Report. (2017). Beijing: Tsinghua University Publishing House.
16. He J, Chen WQ. 2015 China Tumor Registration Annual Report. (2017). Beijing: Tsinghua University Publishing House.
17. He J, Chen WQ. 2016 China Tumor Registration Annual Report. (2017). Beijing: Tsinghua University Publishing House.
18. He J, Chen WQ. 2017 China Tumor Registration Annual Report. (2018). Beijing: People's Medical Publishing House.
19. He J, Chen WQ. 2018 China Tumor Registration Annual Report. (2019). Beijing: People's Medical Publishing House.
20. He J, Chen WQ. 2019 China Tumor Registration Annual Report. (2021). Beijing: People's Medical Publishing House; 2021.
21. Global Cancer Observatory. International Agency for Research on Cancer 2022. (2022). Available online at: https://gco.iarc.fr/today/ (accessed February 03, 2022).
22. Freyberger H, Schulte-Markwort E, Dilling H, WHO. Crosswalk for the tenth revision of the international classification of diseases, chapter V (F): ICD-10 vs. ICD-9. Fortschr Neuro Psyc. (1993) 61:128–128. doi: 10.1055/s-2007-999082
23. Chen WQ, Zheng RS, Zeng HM, Zhang SW. Trend analysis of the changes of male/female,urban/rural incidences and average age of cancer patients in China 1989–2008. Chin J Oncol. (2014) 36:796–800.
24. Khazaei S, Soheilyzad M, Molaeipoor L, Khazaei Z, Rezaeian S, Khazaei S. Trend of smear-positive pulmonary tuberculosis in Iran during 1995–2012: a segmented regression model. Int J Prev Med. (2016) 7:86. doi: 10.4103/2008-7802.184317
25. Wang DZ, Wang C, Shen CF, Zhang Y, Zhang H, Song GD, et al. Comparison of application of Cochran-Armitage trend test and linear regression analysis forrate trend analysis in epidemiology study. Chin J Epidemiol. (2017) 38:684–7.
26. Yang Y, Schulhofer-Wohl S, Fu WJ. Land KCJAJoS. The intrinsic estimator for age-period-cohort analysis: what it is and how to use it. Am. J Sociol. (2008) 113:1697–736. doi: 10.1086/587154
27. Shi TT, Liu ZQ, Fan H, Zhang PY, Yu SZ, TJ. Z. Analysis on incidence trend of liver cancer in China, 2005-2016. Chin J Epidemiol. (2022) 43:330–5.
28. Cai Jie, Chen HD, Lu M, Zhang YH, Lu B, You L, et al. Trend analysis on morbidity and mortality of pancreatic cancer in China, 2005-2015. Chin J Epidemiol. (2021) 42:794–800.
29. Chernyavskiy P, Little MP, Rosenberg PS, A. unified approach for assessing heterogeneity in age–period–cohort model parameters using random effects. Methods Med Res. (2019) 28:20–34. doi: 10.1177/0962280217713033
30. Chen L, Xu JR, Wang M, Zhang M, Rang WQ. Analysis for mortality trend and age-period-cohort of kidney cancer in China from 1990 to 2019. Chin J Dis Control Prev. (2021) 25:1026–033.
31. Ministry of Health of the People's Republic of China. Program of cancer prevention and control in China (2004–2010). China Cancer. (2004) 13:65–8.
32. Sun D, Li H, Cao M, He S, Lei L, Peng J, et al. Cancer burden in China: trends, risk factors and prevention. Cancer Biol Med. (2020) 17:879. doi: 10.20892/j.issn.2095-3941.2020.0387
33. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Tobacco smoke and involuntary smoking. IARC Monogr Eval Carcinog risks Hum. (2004) 83:1–1438.
34. Centers for Disease Control and Prevention (US) National Center for Chronic Disease Prevention and Health Promotion (US) Office Office on Smoking and Health. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta, GA: Centers for Disease Control and Prevention (2010).
35. Yang G, Wang Y, Wu Y, Yang J, Wan X. The road to effective tobacco control in China. Lancet. (2015) 385:1019–28. doi: 10.1016/S0140-6736(15)60174-X
36. Reitsma MB, Kendrick PJ, Ababneh E, Abbafati C, Abbasi-Kangevari M, Abdoli A, et al. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990–2019: a systematic analysis from the Global Burden of Disease Study 2019. Lancet. (2021) 39710292:2337–60. doi: 10.1016/S0140-6736(21)01169-7
37. Zhu K. Analysis of the prevalence and influencing factors of chronic diseases in the elderly in China under the background of population aging. Nanjing University of Posts and Telecommunications. (2021).
38. Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. (2016) 388:1545–602. doi: 10.1016/S0140-6736(16)31678-6
39. Dong Y, Wang H, Tan C, Zhang G. Epidemic status of four major chronic diseases of elderly and influence of DALYs. Med Society. (2019) 32:59–61+65.
40. Renzi C, Kaushal A, Emery J, Hamilton W, Neal RD, Rachet B, et al. Comorbid chronic diseases and cancer diagnosis: disease-specific effects and underlying mechanisms. Nat Rev Clin Oncol. (2019) 16:746–61. doi: 10.1038/s41571-019-0249-6
41. Salika T, Lyratzopoulos G, Whitaker KL, Waller J, Renzi C. Do comorbidities influence help-seeking for cancer alarm symptoms? A population-based survey in England. J Public Health (Oxf). (2017) 2:340–9. doi: 10.1093/pubmed/fdx072
42. Cao MM Li H, Sun DQ, He SY Yu YW, Li J, et al. Cancer screening in China: the current status, challenges, and suggestions. Cancer Lett. (2021) 506:120–7. doi: 10.1016/j.canlet.2021.02.017
43. Klabunde CN, Zheng YY, Quinn VP, Beaber EF, Rutter CM, Halm EA, et al. Influence of age and comorbidity on colorectal cancer screening in the elderly. Am J Prev Med. (2016) 51:e67–75. doi: 10.1016/j.amepre.2016.04.018
44. Guilcher SJ, Lofters A, Glazier RH, Jaglal SB, Voth J, Bayoumi AM. Level of disability, multi-morbidity and breast cancer screening: does severity matter? Prevent Med. (2014) 67:193–8. doi: 10.1016/j.ypmed.2014.07.025
45. Smith SM, Campbell NC, MacLeod U, Lee AJ, Raja A, Wyke S, et al. Factors contributing to the time taken to consult with symptoms of lung cancer: a cross-sectional study. Thorax. (2009) 64:523–31. doi: 10.1136/thx.2008.096560
46. Chen WQ, Zheng RS, Zhang SW, Zou HMZN, He J. Analysis of cancer incidence and mortality in elderly population in China, 2013. Chin J Oncol. (2017) 39:60–6. doi: 10.1016/j.canlet.2017.04.024
47. Varghese F, Wong J. Breast cancer in the elderly. Surgical Clinics. (2018) 98:819–33. doi: 10.1016/j.suc.2018.04.002
48. Wang W, Yin P, Wang LJ, Liu YN, Liu JM Qi JL, et al. Analysis on all-cause mortality rate and life expectancy in China, 2005-2018. Chin J Epidemiol. (2021) 42:1420–8.
49. Wei W, Zeng H, Zheng R, Zhang S, An L. Chen R„ et al. Cancer registration in China and its role in cancer prevention and control. Lancet Oncol. (2020) 21:e342–9. doi: 10.1016/S1470-2045(20)30073-5
50. Wei WQ, He J. Cancer registration in China and its role in cancer prevention and control. Chin J Oncol. (2019) 41:15–8.
51. Islami F, Chen W, Yu X, Lortet-Tieulent J, Zheng R, Flanders W, et al. Cancer deaths and cases attributable to lifestyle factors and infections in China, 2013. Ann Oncol. (2017) 28:2567–74. doi: 10.1093/annonc/mdx342
52. He NF, Pu YJ Li ZQ, Shi H, Zhao HF Li YY, et al. Influencing factors and Fairness of Health status of floating elderly population in China. Chin J Gerontol. (2021) 41:4398–401.
53. Huo TQ, Yan X, Guo J, Guo QF, Xiao GX. Prevalence and healthcare-seeking for common diseases and associated factors in elderly migrants in China. Chin Gen Pract. (2021) 24:2785–92.
54. Zheng YH, Hao XN. Rearch on medical orientation and influnce factors of elderly floating population. Chinese Health Economics. (2021) 40:56–9.
55. Li X, Gao S. Trend analysis of the incidence,morbidity and mortality of lung cancer in China from 1990 to 2019. Chin J Prev Control Chronic Non-Commun Dis. (2021) 29:821–6.
56. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
57. International Agency for Research on Cancer. Cancer incidence in five continents. (2021). Available online at: https://ci5.iarc.fr (accessed June 28, 2021).
58. Zheng RS, Sun KX, Zhang SW, Zeng HM, Zou XN, Chen R, et al. Report of cancer epidemiology in China, 2015. Chin J Oncol. (2019) 41:19–28.
59. Fletcher JM. The effects of in utero exposure to the 1918 influenza pandemic on family formation. Econ Hum Biol. (2018) 30:59–68. doi: 10.1016/j.ehb.2018.06.004
60. Santibáñez-Andrade M, Chirino YI, González-Ramírez I, Sánchez-Pérez Y, García-Cuellar CM. Deciphering the code between air pollution and disease: The effect of particulate matter on cancer hallmarks. Int J Mol Sci. (2019) 21:136. doi: 10.3390/ijms21010136
61. Guo F. The study on the early health enterprise in Nanjing National Government, Master's Thesis. Guilin, China: Guangxi Normal Univers. (2010).
62. Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang X-S, et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet Oncol. (2015) 385:977–1010. doi: 10.1016/S0140-6736(14)62038-9
63. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. (2022) 72:7–33. doi: 10.3322/caac.21708
64. Xia C, Dong X, Li H, Cao M, Sun D, He S, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. (2022) 135:584–90. doi: 10.1097/CM9.0000000000002108
65. Yang SS. An epidemiologic study on changes and patterns of smoking behavior and its genetic score in an older adults: The General Hospital of the People's Liberation Army. (2015).
66. Crocetti E, Paci E. What gender differences in cancer incidence changed during the last 10 years in central Italy? Tumori. (2002) 88:13–7. doi: 10.1177/030089160208800401
67. Mu L, Liu L, Niu R, Zhao B, Shi J, Li Y, et al. Indoor air pollution and risk of lung cancer among Chinese female non-smokers. Cancer Causes Control. (2013) 24:439–50. doi: 10.1007/s10552-012-0130-8
Keywords: cancer, epidemiology, aged, age-period-cohort model, log-linear regression
Citation: Guo H, Lin K, Yang K, Ma Z, Cao M, Hu Y and Yan Y (2022) Trends of cancer incidence among Chinese older adults from 2005 to 2016: A log-linear regression and age-period-cohort analysis. Front. Public Health 10:1023276. doi: 10.3389/fpubh.2022.1023276
Received: 19 August 2022; Accepted: 03 October 2022;
Published: 18 October 2022.
Edited by:
Xuan Li, University of Mississippi Medical Center, United StatesReviewed by:
Peter D. Baade, Cancer Council Queensland, AustraliaNatasa Krsto Rancic, University of Niš, Serbia
Copyright © 2022 Guo, Lin, Yang, Ma, Cao, Hu and Yan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yunhua Hu, huyunhua1019@sina.com; Yizhong Yan, erniu19880215@sina.com
†These authors have contributed equally to this work