 Dianjiang Li
Dianjiang Li Yuhui Ruan3,4†
Yuhui Ruan3,4† Qi Kang
Qi Kang Chao Rong
Chao Rong- 1Department of Social Medicine and Health Education, School of Public Health, Nanjing Medical University, Nanjing, China
- 2Research Center for Social Risk Governance for Major Public Health Events, Nanjing Medical University, Nanjing, China
- 3School of Politics and Public Administration, Soochow University, Suzhou, China
- 4Institute of Public Health, Soochow University, Suzhou, China
- 5Department of Health Policy Research, Shanghai Health Development Research Center (Shanghai Medical Information Center), Shanghai, China
- 6Department of Health Service and Management, School of Humanities and Management, Zhejiang Chinese Medical University, Hangzhou, China
Objective: To investigate the gender-specific associations between exposure to urbanization and psychological stress in China experiencing rapid urbanization.
Methods: Data were obtained from the 2015 China Health and Nutrition Survey. A total of 4,388 men and 5,098 women aged at least 18 years were obtained from 288 communities across 12 provinces and municipalities. Tertiles of the urbanization index, summarizing 12 urbanization dimensions at the community level, were used to define low, medium, and high levels of urbanization. The psychological stress was measured based on the 10-item Perceived Stress Scale. The gender-stratified multilevel analysis (Level-1: Individuals, Level-2: Communities, and Level-3: provinces/municipalities) was used to estimate the association between exposure to urbanization and psychological stress.
Results: After controlling for age, education status, marital status, work status, household income per capita, current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions, the urbanization index was negatively associated with psychological stress in women (Ptrend = 0.017) but not men (Ptrend = 0.476). More specifically, a one-standard deviation increase in the score of community population density (β = −0.329, P = 0.329), modern markets (β = −0.247, P = 0.044), education (β = −0.448, P = 0.002), and housing (β = −0.380, P = 0.005) was negatively associated with psychological stress only in women, separately.
Conclusion: Our data revealed that living in the most urbanized communities is associated with lower levels of psychological stress for women but not men. Thus, this study can help empower decision-makers to accurately target vulnerable communities and plan effective strategies to address psychological outcomes.
Introduction
Urbanization involves the change in size, density, and heterogeneity in places (1), and is widely recognized as a driver of the main health-relevant changes to humanity (2). Currently, more than 55% of the global population is living in urban areas. This proportion will increase to nearly 70% by 2050, with at least 50% of the population living in cities of more than 500,000 inhabitants (3). Rapid urbanization generated opportunities for improved sanitation, infrastructure, education, communication networks, and better health care services. Nevertheless, it resulted in traffic congestion, sedentary lifestyles, and environmental pollution (4–6). These factors can independently and synergistically influence individuals' health (7–9). A better understanding of their relationships may help us identify interventions that effectively promote health status in countries undergoing rapid urbanization.
China has witnessed unprecedented urbanization and associated rural depopulation over the past 40 years, along with a huge increase in the total population (10, 11). The rapid migration and urbanization process in China has led to pronounced changes in community composition and its characteristics (12), evoking great scholarly interest in the effects of urbanization on mental health for Chinese people (13–18). Most studies suggested an inverse relationship between urbanization and mental health (14, 16, 19), with urban living related to a lower prevalence of developing mental health problems (such as schizophrenia, dementia, cognitive impairment, and mood disorders) (14, 16, 17). Especially residence in highly urbanized areas was associated with lower depressive symptoms (20). However, few studies examined the association between exposure to urbanization and psychological stress in China. Psychological stress refers to the real or perceived environmental demands that exceed an individual's adaptive capacity in daily life (21, 22) and is considered the most well-established risk factor for mental disorders (23–25). It is, therefore, vital to obtain a comprehensive view of the complex and evolving relationship between urbanization and psychological stress for sustainable urbanization that can be deployed to protect mental health.
Moreover, rapid urbanization affects women and men in fundamentally different patterns (8, 26). Women and men may perceive, be exposed to, and respond differently to a growing urbanized environment (27). Meanwhile, gender affects each element in the stress process as much as the input by deciding whether a situation will be stressful at the output (28). Previous epidemiological studies have revealed that women are more likely to suffer from higher psychological stress than men (29–31) and develop greater mental health problems (14, 16, 17). Therefore, these observations suggest the possibility of gender-specific differences in the effects of urbanization on psychological stress. Thus, this study aimed to use data from the China Health and Nutrition Survey (CHNS) to explore the gender-specific association between urbanization and psychological stress, with a multidimensional index assessment at the community level.
Materials and methods
Study population and design
This study used data from CHNS, a longitudinal study that began in 1989 and has been repeated every 2–4 years through 2015 in 10 waves. The CHNS used a multistage, random cluster process to draw the sample surveyed in nine provinces (Liaoning, Heilongjiang, Jiangsu, Shandong, Henan, Hubei, Hunan, Guangxi, and Guizhou) (32). The sample was designed to represent rural and urban areas of varying geography, economy, and public resources, and to focus on the overall health during urbanization and economic transitions (32). In 2011, three municipalities (Beijing, Chongqing, and Shanghai) directly under the Central Government were added to the study. The scientific rationale and design of the CHNS have been reported in detail elsewhere (33).
For the analysis, we included 20,899 participants over 18 years old from the 10th survey of the CHNS carried out in 2015, which measured psychological stress for the first time. Participants who had missing information on urbanization (n = 36), psychological stress (n = 1,413), or control variables including household income (n = 7,345), current smoking (n = 969), alcohol drinking (n = 4), sleep duration (n = 125), height (n = 1,512), or chronic conditions (n = 9) were excluded. Thus, 9,486 subjects (4,388 men and 5,098 women) from 288 communities across 12 provinces and municipalities were included in the final analysis.
Assessment of urbanization
We evaluated the urbanization level of the 288 sampled communities using an urbanization index developed by Jones-Smith and Popkin (34). Specifically, the urbanization index was applied to 12 multidimensional components at a community level: communications (e.g., television, mobile, post, and cinema), population density, economic activity, housing (i.e., availability of electricity, indoor tap water, and flushing toilets), traditional markets (i.e., types, distances, and business hours of food and fuel markets), modern markets (i.e., the quantity of supermarkets and modern eating establishments), social services, transportation, education (i.e., average educational level among adults above 21 years old), diversity (i.e., community variance in education and income levels), health infrastructure, and sanitation. Each component was scaled from 0 to 10, weighted equally in the overall index, and added together for an overall maximum possible score of 120. Higher scores reflected more urban characteristics across multiple domains. The urbanization index was explicitly developed for the CHNS and had adequate reliability and validity in previous studies (32, 35). The indicators measuring the proportion of households were derived from the household responses and the remaining indicators were collected from the community-level survey offered to community officials. The detailed construction procedure has been described elsewhere (34, 36, 37). Similar to prior studies, the urbanization index is categorized into tertiles representing low (<63.52), medium (63.52–84.07), and high (>84.07) urbanization levels.
Assessment of psychological stress
The Perceived Stress Scale-10 (PSS-10) was designed to measure the degree to which situations in one's life are appraised as stressful (38) and has been verified to assess psychological stress in a large community-based general population in China (24, 39). The PSS-10 is divided into two subscales: negative and positive. The negative subscale assesses the lack of control in life and negative affective reactions (perceived distress), while the positive subscale measures the ability to cope with current stressors (coping capacity) (38, 40). The participants rated each item on a 5-point Likert scale ranging from “0 = never” to “4 = very often. Positively framed questions (items 6, 7, 9, and 10) were reverse scored (“4 = never” to “0 = very often”), and all 10-item scores were then summed to create a total score. The total score ranged from 0 to 40 (Cronbach's α = 0.744 in the present study), with higher scores indicating higher levels of psychological stress.
Assessment of control covariates
Trained interviewers collected individual information on sociodemographics, lifestyle parameters, and medical history with a structured questionnaire. The education status was divided into three categories (primary school and below, junior school, or senior school and above), and the marital status was categorized as married or others (including divorced, widowed, separated, or never married). The work status was divided into two categories (yes or no). The annual household income per capita (yuan) was calculated as the sum of the self-reported annual income of all adult family members divided by household size. Lifestyle factors included in the analysis were current smoking (yes or no), alcohol drinking (yes or no), and sleeping. Sleep duration was obtained by asking how many hours a person sleeps every day, including daytime and night time, and was categorized as ≤6 h, 7–8 h, or ≥9 h. The body mass index (BMI) was calculated as the weight (kg) divided by height (m) squared and was divided into four categorical groups based on the criteria recommended by the Working Group on Obesity in China (41): underweight (< 18.5 kg/m2), normal (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2), or obesity (≥28.0 kg/m2). Chronic conditions were measured by asking the respondents whether they had been diagnosed with chronic diseases (including hypertension, diabetes mellitus, stroke, myocardial infarction, or cancer) by professional doctors (yes or no).
Statistical analysis
Given that the continuous variables were of non-normal distribution, the results were presented as medians (P25, P75) for continuous variables and numbers (percentages) for categorized variables. The characteristics between men and women were compared using the Wilcoxon rank-sum test or Chi-squared test, as appropriate. Due to the prominent hierarchical characteristics of the data, individuals (level 1) nested within the community (level 2), and province/municipality (level 3) (42, 43), we used a gender-stratified multilevel (three-level) linear regression model to investigate the association between the community-level urbanization index and psychological stress. We developed two models, model 1 was unadjusted, and model 2 was adjusted for individual-level variables including age (continuous), education status, marital status, work status, household income per capita (continuous), current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions. In addition, we examined whether each of the 12 urbanization components was separately associated with psychological stress. Given collinearity between the 12 urbanization components and to better understand the pathways linking exposure to urbanization and psychological stress, we conducted a separate analysis. We incorporated each of the 12 urbanization components [in one-standard deviation (SD) increase increments] in the model while adjusting for the covariates included in model 2 and stratifying by gender.
The statistical significance was determined at a two-sided P-value < 0.05 level, and all statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) for Windows.
Results
Characteristics of the participants
Table 1 reports the characteristics of the 9,486 participants aged 18–99. The median (P25, P75) age of the total population was 53 (43, 63) years, with men having a higher median (P25, P75) age than women [54 (44, 64) vs. 53 (42, 63)]. Men were more likely to be educated, married, employed, and have higher median household income per capita, whereas women smoked and drank less and had higher levels of obesity. Men more frequently reported a history of chronic conditions than women. The median (P25, P75) score of PSS-10 was 16 (12, 19) for men and 17 (13, 19) for women.
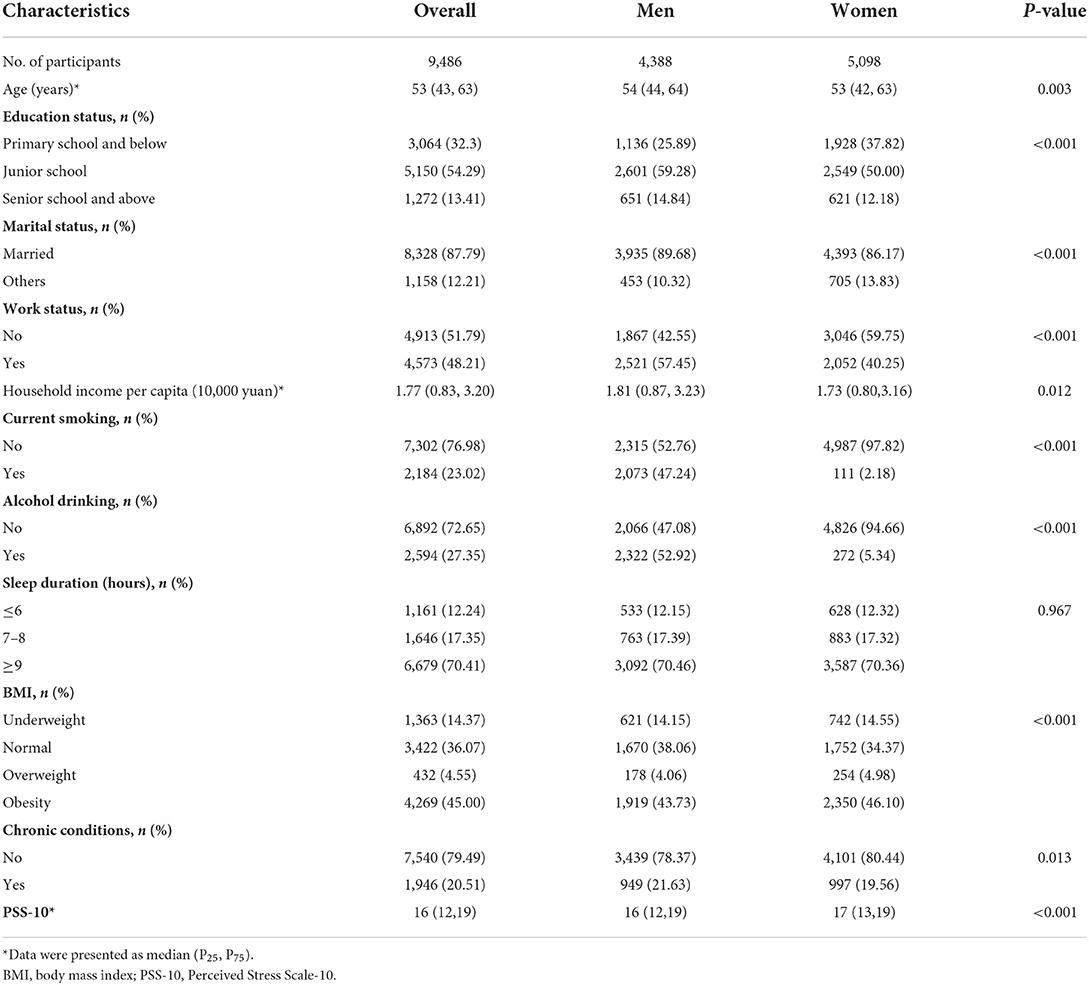
Table 1. Characteristics of the study population.
Urbanization index and psychological stress
Table 2 reports the multilevel-adjusted associations between the urbanization index and psychological stress. In men, no significant association between urbanization index and psychological stress was observed in model 1 (Ptrend = 0.209) and model 2 (Ptrend = 0.476). In women, model 1 presented a higher urbanization index associated with lower psychological stress (Ptrend = 0.001). Regarding model 2, the association reduced but remained statistically significant when adjusting for age, education status, marital status, work status, household income per capita, current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions (Ptrend = 0.017). Specifically, women were significantly more likely to report a lower psychological stress medium (β = −0.661, P = 0.034) and high (β = −0.775, P = 0.014) levels of urbanization than low urbanization in model 2.
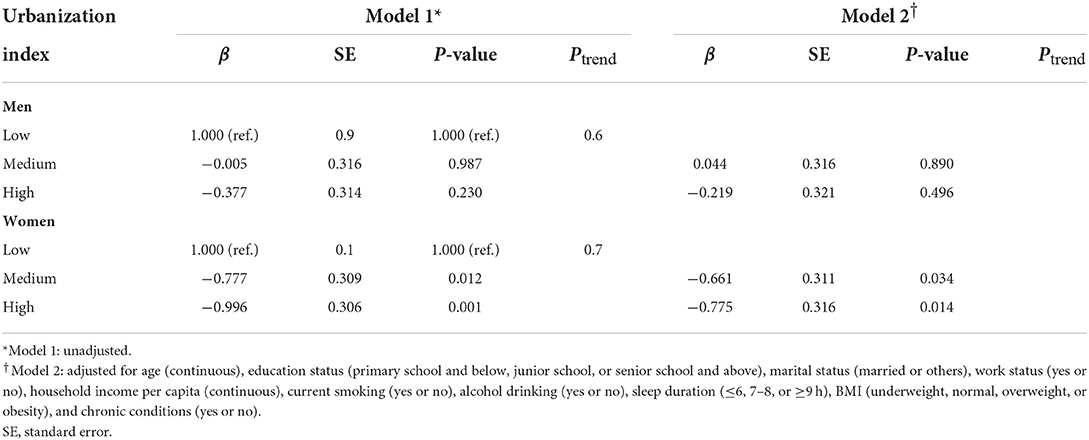
Table 2. Multilevel linear regression for the association between urbanization index and psychological stress, stratified by gender.
Urbanization components and psychological stress
The multilevel-adjusted associations of urbanization components (per one-SD increase) and psychological stress are presented in Table 3. In men, a one- SD increase in the score of education and housing at the community level was separately associated with lower psychological stress in model 1, but the associations were not statistically significant when controlling for the variables in Model 2. In women, model 1 showed that a one-SD increase in the score of community population density, social services, modern markets, transportation, economic activity, education, housing, and sanitation was separately associated with lower psychological stress. Further adjustment for age, education status, marital status, work status, household income per capita, current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions in Model 2, the increase in the score of community population density (β = −0.329, P = 0.329), modern markets (β = −0.247, P = 0.044), education (β = −0.448, P = 0.002), and housing (β = −0.380, P = 0.005) were still inversely associated with psychological stress, separately.
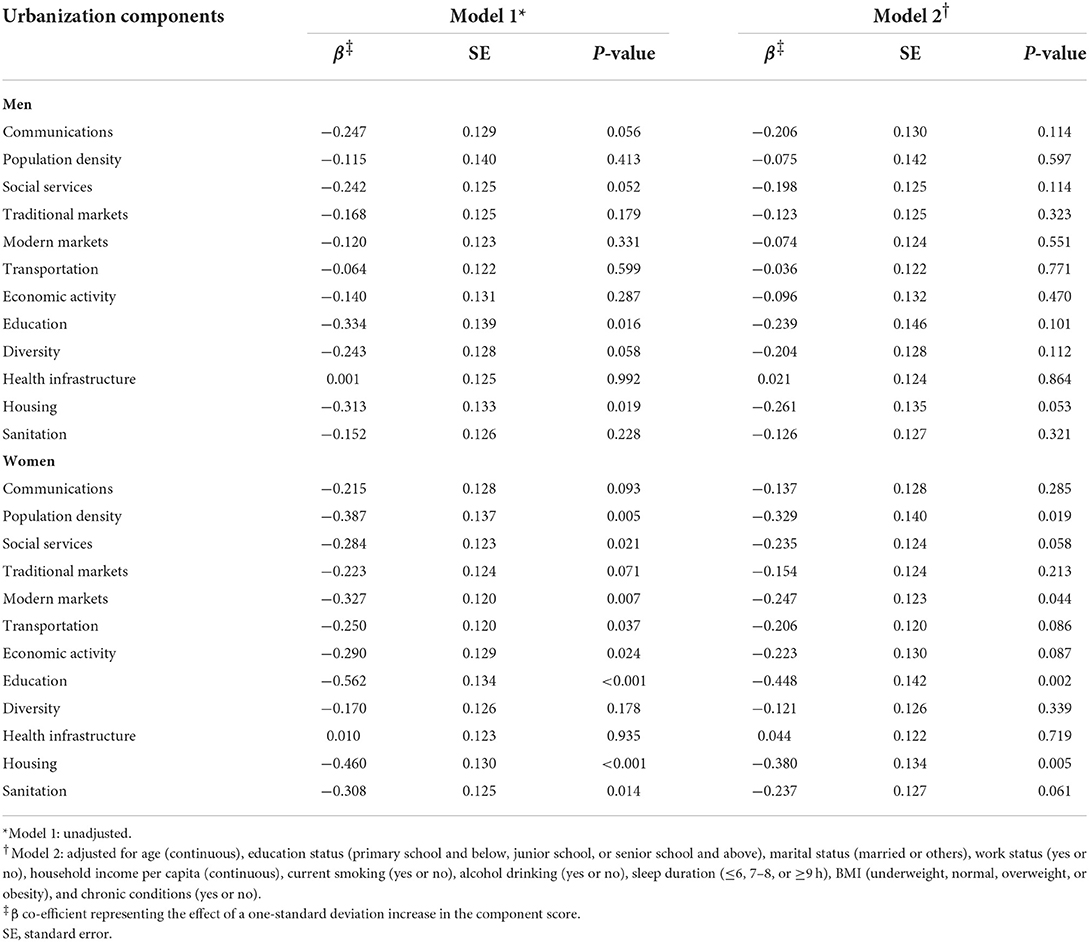
Table 3. Multilevel linear regression for the association between urbanization components and psychological stress, stratified by gender.
Discussion
To our knowledge, this study is the first to test potential gender differences in the association of urbanization with psychological stress in the CHNS data using multilevel analyses. Our gender-specific analysis showed that men and women had different patterns in the association between the urbanization index and psychological stress. By further analyzing the results, women appeared to be more sensitive to the urbanization components than men. Moreover, four urbanization components were separately and negatively associated with the levels of psychological stress in women levels after controlling for potential confounders.
This study found that the urbanization index was negatively associated with psychological stress in women but not men. Women in the most urbanized communities were likely to have lower levels of psychological stress than those in the low urbanized communities. No association was found in men, and the results for both genders remained consistent after adjusting for age, education status, marital status, work status, household income per capita, current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions. Similar to this work, prior studies have reported that living in urban areas was associated with a lower suicide rate, with a consistently lower rate in women than in men (44, 45). One potential explanation for the observed gender difference may be partly that social roles determine the range of potentially stressful experiences of women and men (28). In China, women are equally stressed by work and family, whereas men are more vulnerable to the psychological impact of work roles than family roles (46). During China's urbanization, urban women, in contrast to rural women, are more likely to strive to become financially independent by doing more market work and less housework (47, 48) and eventually win better happiness (48). In addition, the mechanisms for the observed gender differences may also be related to the different coping strategies of men and women. This is explained by studies showing that women tend to use adaptive coping skills more and are more likely to seek social support than men (49–53). For example, women tend to be relatively more willing and able to access neighborhood social resources when faced with stressful life experiences (20). In contrast, men resist receiving or seeking formal support but are more willing to accept social support from families (54). Distinct from western countries, China's urbanization was greatly intervened by government policies (55, 56) and might promote neighborhood social capital (20, 56), increasing access to social networks and supports, regulating unhealthy behaviors, and promoting adaptive coping mechanisms associated with better psychological outcomes (57).
This study first examined the pathways linking 12 components of urbanization and psychological stress. It demonstrated that one SD increase in the score of community population density, modern markets, education, and housing was negatively associated with psychological stress only in women after controlling for age, education status, marital status, work status, household income per capita, current smoking, alcohol drinking, sleep duration, BMI, and chronic conditions. Living in crowded communities is associated with decreased psychological stress since population density is one of the most widely used proxies for access to medical and mental health professionals (58, 59). Therefore, mental health service providers tend to be heavily concentrated in densely populated urban areas (60). Melis et al. found that high population density contributed to a reduced risk of depression, especially for women (61). Additionally, greater access to modern markets was associated with lower levels of psychological stress. Living in a community with easier access to modern markets promotes access to healthy foods, resulting in lower life stress (62) and better happiness (63, 64). Brown et al. reported that greater accessibility and shopping in modern supermarkets were associated with better self-rated health (64, 65). Education at a community level was inversely associated with psychological stress because the neighborhood educational attainment was considered “collective human capital” (66) and “collective efficiency” (67), which may benefit the residents' health more than the sum of their efforts (68). Wight et al. indicated that living in a low-education area was associated with low cognitive function, net of individual characteristics, including individual-level education (69). Noteworthy, a house is a crucial family asset and is regarded as a potent status symbol in China (70). This study found that better housing conditions were inversely associated with psychological stress, consistent with previous studies, showing that inadequate housing conditions are associated with worsening mental health (i.e., stress, anxiety, and depression) (71–73). Although pathways have been proposed to elucidate this association, future studies are required to validate the role of the other specific urbanization elements in improving psychological outcomes.
The strengths of this study were that the multicomponent urbanization index could capture heterogeneity in various services and infrastructures across different urbanized communities. We also evaluated how the pathways linking urbanization and psychological stress vary by gender, demonstrating a statistically significant association for women. The findings can help guide decision-makers to accurately target vulnerable communities and formulate effective policies to address psychological outcomes in China and other recently urbanized countries. However, there are several limitations to this study. First, the CHNS was not nationally representative, but encompassed communities from 12 different provincial regions in the northeast, central, and south China (27). This diversity makes this analysis possible (74). Second, the study was a cross-sectional design, limiting causality interpretations. Healthier people were more likely to migrate to more urbanized communities in search of better living conditions (20, 27, 75) because of the so-called healthy migrant effect (76). Third, this study decomposed urbanization and revealed that specific elements substantially affect psychological stress. Nevertheless, these single associations might be due to other factors associated with urbanization (77). Last, although measuring psychological stress in the CHNS has been validated (24, 39), it represents a self-reported perception of stress and is not an objective measurement. Future studies should attempt to replicate our analyses by measuring biological stress markers, such as cortisol levels (78–80).
Conclusion
The current study in a large sample of Chinese adults showed that a higher urbanization index was negatively associated with psychological stress in women but not men. More specifically, one SD increase in the score of community population density, modern markets, education and housing was separately and negatively associated with psychological stress only in women after controlling for potential confounders. These findings provide valuable insights that help guide decision-makers to accurately target vulnerable communities and allocate public resources to address psychological outcomes in the case of rapid urbanization.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://www.cpc.unc.edu/projects/china.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Committees of the Institute for Nutrition and Health of Chinese Center for Disease Control and Prevention and the University of North Carolina at Chapel Hill, USA. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DL conceived and designed the study, drafted the report, and received the final version for publication. YR conducted the statistical analysis. QK and CR revised the manuscript. All authors checked the article and approved it for publication.
Funding
This work was supported by the National Natural Science Foundation of China (Project No. 71974101), the Humanities and Social Science Research Project of Soochow University (Project No. NH33716122), and the Youth Interdisciplinary Research Project in Humanities and Social Sciences of Soochow University (Project No. NH33714622).
Acknowledgments
We sincerely thank the Institute of Nutrition and Food Safety (China Center for Disease Control and Prevention) and Carolina Population Center (University of North Carolina at Chapel Hill) for providing financial support for collecting CHNS data and analysis files.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Vlahov D, Galea S. Urbanization, urbanicity, and health. J Urban Health. (2002) 79:S1–12. doi: 10.1093/jurban/79.suppl_1.S1
2. Gruebner O, Rapp MA, Adli M, Kluge U, Galea S, Heinz A. Cities and mental health. Dtsch Arztebl Int. (2017) 114:121–7. doi: 10.3238/arztebl.2017.0121
3. Jiang L, Young MH, Hardee K. Population, urbanization and the environment. World Watch. (2008) 21:34–9.
4. Luo Y, Pang L, Guo C, Zhang L, Wang Y, Zheng X. Urbanicity and autism of children in China. Psychiatry Res. (2020) 286:112867. doi: 10.1016/j.psychres.2020.112867
5. Luo Y, Pang L, Guo C, Zhang L, Zheng X. Association of urbanicity with schizophrenia and related mortality in China. Can J Psychiatry. (2021) 66:385–94. doi: 10.1177/0706743720954059
6. Chen H, Liu Y, Li Z, Xue D. Urbanization, economic development and health: evidence from China's labor-force dynamic survey. Int J Equity Health. (2017) 16:207. doi: 10.1186/s12939-017-0705-9
7. Li X, Song J, Lin T, Dixon J, Zhang G, Ye H. Urbanization and health in China, thinking at the national, local and individual levels. Environ Health. (2016) 15(Suppl.1):32. doi: 10.1186/s12940-016-0104-5
8. Jiang TB, Deng ZW, Zhi YP, Cheng H, Gao Q. The effect of urbanization on population health: evidence from China. Front Public Health. (2021) 9:706982. doi: 10.3389/fpubh.2021.706982
9. Li X, Wang C, Zhang G, Xiao L, Dixon J. Urbanisation and human health in China: spatial features and a systemic perspective. Environ Sci Pollut Res Int. (2012) 19:1375–84. doi: 10.1007/s11356-011-0718-7
10. Zhang X, Brandt M, Tong X, Ciais P, Yue Y, Xiao X, et al. A large but transient carbon sink from urbanization and rural depopulation in China. Nat Sustain. (2022) 5:321–8. doi: 10.1038/s41893-021-00843-y
11. Yue L, Xue D. The double-edged sword of urbanization and its nexus with eco-efficiency in China. Int J Environ Res Public Health. (2020) 17:446. doi: 10.3390/ijerph17020446
12. Chen J, Chen S. Mental health effects of perceived living environment and neighborhood safety in urbanizing China. Habitat Int. (2015) 46:101–10. doi: 10.1016/j.habitatint.2014.11.002
13. Zhang J, Wang R, Wang C, Wang Y, Chen X, Mi G, et al. Prevalence of mental disorders in 21st century Shandong Province, China: a ten-year comparative study. J Affect Disord. (2021) 283:344–53. doi: 10.1016/j.jad.2021.01.068
14. Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiat. (2019) 6:211–24. doi: 10.1016/S2215-0366(18)30511-X
15. Lu J, Xu X, Huang Y, Li T, Ma C, Xu G, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiat. (2021) 8:981–90. doi: 10.1016/S2215-0366(21)00251-0
16. Jia L, Du Y, Chu L, Zhang Z, Li F, Lyu D, et al. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health. (2020) 5:e661–e71. doi: 10.1016/S2468-2667(20)30185-7
17. Sun L, Zhang Y, Cui L, Li J, Li L, Sun X, et al. Lifetime and 1-month prevalence of mental disorders in Hebei Province, China: a community-based cross-sectional study. Front Public Health. (2021) 9:759160. doi: 10.3389/fpubh.2021.759160
18. Guo X, Meng Z, Huang G, Fan J, Zhou W, Ling W, et al. Meta-analysis of the prevalence of anxiety disorders in mainland China from 2000 to 2015. Sci Rep. (2016) 6:28033. doi: 10.1038/srep28033
19. Tang T, Jiang J, Tang X. Prevalence of depressive symptoms among older adults in mainland China: a systematic review and meta-analysis. J Affect Disord. (2021) 293:379–90. doi: 10.1016/j.jad.2021.06.050
20. Wang R, Xue D, Liu Y. The relationship between urbanization and depression in China: the mediating role of neighborhood social capital. Int J Equity Health. (2018) 17:105. doi: 10.1186/s12939-018-0825-x
21. Cohen S, Janicki-Deverts D, Miller GE. Psychological stress and disease. J Am Med Assoc. (2007) 298:1685–7. doi: 10.1001/jama.298.14.1685
23. Steel Z, Marnane C, Iranpour C, Chey T, Jackson JW, Patel V, et al. The global prevalence of common mental disorders: a systematic review and meta-analysis 1980-2013. Int J Epidemiol. (2014) 43:476–93. doi: 10.1093/ije/dyu038
24. Shih S, Chan A, Yeung E, Tsang A, Chiu R, Chu M, et al. Psychometric properties and correlates of Chinese version of Perceived Stress Scale (CPSS-10) in people with common mental disorders with different employment Statuses. Hong Kong J Occup Ther. (2021) 34:103–12. doi: 10.1177/15691861211032318
25. Lindholdt L, Labriola M. Perceived stress among adolescents as a marker for future mental disorders: a prospective cohort study. Scand J Public Health. (2022) 50:412–7. doi: 10.1177/1403494821993719
26. Colvin ML. Women's health and the world's cities. J Evid Inform Soc Work. (2015) 12:1–3. doi: 10.1080/15433714.2012.759471
27. Wu J, Jiao B, Fan Y. Urbanization and systolic/diastolic blood pressure from a gender perspective: separating longitudinal from cross-sectional association. Health Place. (2022) 75:102778. doi: 10.1016/j.healthplace.2022.102778
28. Matud MP. Gender differences in stress and coping styles. Pers Indiv Differ. (2004) 37:1401–15. doi: 10.1016/j.paid.2004.01.010
29. Ishiguro A, Inoue M, Fisher J, Inoue M, Matsumoto S, Yamaoka K. Gender-based risk and protective factors for psychological distress in the midterm recovery period following the Great East Japan earthquake. Disaster Med Public Health Prep. (2019) 13:487–96. doi: 10.1017/dmp.2018.80
30. Vigna L, Brunani A, Brugnera A, Grossi E, Compare A, Tirelli AS, et al. Determinants of metabolic syndrome in obese workers: gender differences in perceived job-related stress and in psychological characteristics identified using artificial neural networks. Eat Weight Disord. (2019) 24:73–81. doi: 10.1007/s40519-018-0536-8
31. Chaplin TM, Hong K, Bergquist K, Sinha R. Gender differences in response to emotional stress: an assessment across subjective, behavioral, and physiological domains and relations to alcohol craving. Alcohol Clin Exp Res. (2008) 32:1242–50. doi: 10.1111/j.1530-0277.2008.00679.x
32. Popkin BM, Du S, Zhai F, Zhang B. Cohort Profile: the China Health and Nutrition Survey–monitoring and understanding socio-economic and health change in China, 1989-2011. Int J Epidemiol. (2010) 39:1435–40. doi: 10.1093/ije/dyp322
33. Zhang B, Zhai FY, Du SF, Popkin BM. The China health and nutrition survey, 1989–2011. Obes Rev. (2014) 15(Suppl.1):2–7. doi: 10.1111/obr.12119
34. Jones-Smith JC, Popkin BM. Understanding community context and adult health changes in China: development of an urbanicity scale. Soc Sci Med. (2010) 71:1436–46. doi: 10.1016/j.socscimed.2010.07.027
35. Cyril S, Oldroyd JC, Renzaho A. Urbanisation, urbanicity, and health: a systematic review of the reliability and validity of urbanicity scales. BMC Public Health. (2013) 13:513. doi: 10.1186/1471-2458-13-513
36. Attard SM, Herring AH, Mayer-Davis EJ, Popkin BM, Meigs JB, Gordon-Larsen P. Multilevel examination of diabetes in modernising China: what elements of urbanisation are most associated with diabetes? Diabetologia. (2012) 55:3182–92. doi: 10.1007/s00125-012-2697-8
37. Fong TCT, Ho RTH. Longitudinal measurement invariance in urbanization index of Chinese communities across 2000 and 2015: a Bayesian approximate measurement invariance approach. BMC Public Health. (2021) 21:1653. doi: 10.1186/s12889-021-11691-y
38. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. (1983) 24:385–96. doi: 10.2307/2136404
39. Huang F, Wang H, Wang Z, Zhang J, Du W, Su C, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. (2020) 20:130. doi: 10.1186/s12888-020-02520-4
40. Leung DY, Lam TH, Chan SS. Three versions of Perceived Stress Scale: validation in a sample of Chinese cardiac patients who smoke. BMC Public Health. (2010) 10:513. doi: 10.1186/1471-2458-10-513
41. Zhou BF. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. (2002) 15:83–96.
42. He T, Wang M, Tian Z, Zhang J, Liu Y, Zhang Y, et al. Sex-dependent difference in the association between frequency of spicy food consumption and risk of hypertension in Chinese adults. Eur J Nutr. (2019) 58:2449–61. doi: 10.1007/s00394-018-1797-8
43. Xue Y, He T, Yu K, Zhao A, Zheng W, Zhang Y, et al. Association between spicy food consumption and lipid profiles in adults: a nationwide population-based study. Br J Nutr. (2017) 118:144–53. doi: 10.1017/S000711451700157X
44. Wang CW, Chan CL, Yip PS. Suicide rates in China from 2002 to 2011: an update. Soc Psychiatry Psychiatr Epidemiol. (2014) 49:929–41. doi: 10.1007/s00127-013-0789-5
45. Jiang H, Niu L, Hahne J, Hu M, Fang J, Shen M, et al. Changing of suicide rates in China, 2002-2015. J Affect Disord. (2018) 240:165–70. doi: 10.1016/j.jad.2018.07.043
46. Lai G. Work and family roles and psychological well-being in urban China. J Health Soc Behav. (1995) 36:11–37. doi: 10.2307/2137285
47. Luo MS, Chui EWT. Moving from rural to urban China: how urbanization affects women's housework. Sex Roles. (2019) 81:127–39. doi: 10.1007/s11199-018-0987-4
48. Hori M, Kamo Y. Gender differences in happiness: the effects of marriage, social roles, and social support in East Asia. Appl Res Qual Life. (2018) 13:839–57. doi: 10.1007/s11482-017-9559-y
49. Wu Y, Yu W, Wu X, Wan H, Wang Y, Lu G. Psychological resilience and positive coping styles among Chinese undergraduate students: a cross-sectional study. BMC Psychol. (2020) 8:79. doi: 10.1186/s40359-020-00444-y
50. Tang W, Dai Q. Depressive symptoms among first-year Chinese undergraduates: the roles of socio-demographics, coping style, and social support. Psychiatry Res. (2018) 270:89–96. doi: 10.1016/j.psychres.2018.09.027
51. Mirkovic B, Labelle R, Guilé JM, Belloncle V, Bodeau N, Knafo A, et al. Coping skills among adolescent suicide attempters: results of a multisite study. Can J Psychiatry. (2015) 60:S37–45.
52. Xu H, Wang R, Li R, Jin Z, Wan Y, Tao F. Associations of non-suicidal self-injury and psychological symptoms with suicide attempt in adolescents: are there any gender differences? Front Psychiatry. (2022) 13:894218. doi: 10.3389/fpsyt.2022.894218
53. Copeland EP, Hess RS. Differences in young adolescents' coping strategies based on gender and ethnicity. J Early Adolescence. (1995) 15:203–19. doi: 10.1177/0272431695015002002
54. Qian Y, Kent EE. Gender differences in the association between unmet support service needs and mental health among American cancer caregivers. Support Care Cancer. (2022) 30:5469–80. doi: 10.1007/s00520-022-06966-y
55. Chaolin G, Liya W, Cook I. Progress in research on Chinese urbanization. Front Archit Res. (2012) 1:101–49. doi: 10.1016/j.foar.2012.02.013
56. Zhang L, Wang SX, Yu L. Is social capital eroded by the state-led urbanization in China? A case study on indigenous villagers in the urban fringe of Beijing China. Econ Rev. (2015) 35:232–46. doi: 10.1016/j.chieco.2014.04.005
57. Rothon C, Goodwin L, Stansfeld S. Family social support, community “social capital” and adolescents' mental health and educational outcomes: a longitudinal study in England. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:697–709. doi: 10.1007/s00127-011-0391-7
58. Karolaakso T, Autio R, Näppilä T, Leppänen H, Rissanen P, Tuomisto MT, et al. Contextual and mental health service factors in mental disorder-based disability pensioning in Finland - a regional comparison. BMC Health Serv Res. (2021) 21:1081. doi: 10.1186/s12913-021-07099-4
59. Cummings JR, Druss BG. Racial/ethnic differences in mental health service use among adolescents with major depression. J Am Acad Child Adolesc Psychiatry. (2011) 50:160–70. doi: 10.1016/j.jaac.2010.11.004
60. Holzer III CE, Goldsmith HF, Ciarlo JA. The availability of health and mental health providers by population density. J Wash Acad Sci. (2000) 86:25–33.
61. Melis G, Gelormino E, Marra G, Ferracin E, Costa G. The effects of the urban built environment on mental health: a cohort study in a large Northern Italian City. Int J Environ Res Public Health. (2015) 12:14898–915. doi: 10.3390/ijerph121114898
62. Seedat S, Stein DJ, Jackson PB, Heeringa SG, Williams DR, Myer L. Life stress and mental disorders in the South African stress and health study. S Afr Med J. (2009) 99:375–82.
63. Dubowitz T, Ghosh-Dastidar M, Cohen DA, Beckman R, Steiner ED, Hunter GP, et al. Diet and perceptions change with supermarket introduction in a food desert, but not because of supermarket use. Health Aff. (2015) 34:1858–68. doi: 10.1377/hlthaff.2015.0667
64. Brown AF, Vargas RB, Ang A, Pebley AR. The neighborhood food resource environment and the health of residents with chronic conditions: the food resource environment and the health of residents. J Gen Intern Med. (2008) 23:1137–44. doi: 10.1007/s11606-008-0601-5
65. Liu Y, Zhang F, Wu F, Liu Y, Li Z. The subjective wellbeing of migrants in Guangzhou, China: the impacts of the social and physical environment. Cities. (2017) 60:333–42. doi: 10.1016/j.cities.2016.10.008
66. Ross CE, Mirowsky J. Neighborhood socioeconomic status and health: context or composition? City Community. (2008) 7:163–79. doi: 10.1111/j.1540-6040.2008.00251.x
67. Sampson RJ, Raudenbush SW, Earls F. Neighborhoods and violent crime: a multilevel study of collective efficacy. Science. (1997) 277:918–24. doi: 10.1126/science.277.5328.918
68. Zhang W, Chen Q, McCubbin H, McCubbin L, Foley S. Predictors of mental and physical health: individual and neighborhood levels of education, social well-being, and ethnicity. Health Place. (2011) 17:238–47. doi: 10.1016/j.healthplace.2010.10.008
69. Wight RG, Aneshensel CS, Miller-Martinez D, Botticello AL, Cummings JR, Karlamangla AS, et al. Urban neighborhood context, educational attainment, and cognitive function among older adults. Am J Epidemiol. (2006) 163:1071–8. doi: 10.1093/aje/kwj176
70. Zhou Z, Ma Y, Du W, Zhou K, Qi S. Housing conditions and adolescents' socioemotional well-being: an empirical examination from China. Appl Res Qual Life. (2021) 4:1–21. doi: 10.1007/s11482-021-09998-4
71. Xie L, Zhou S, Zhang L. Associations between objective and subjective housing status with individual mental health in Guangzhou, China. Int J Environ Res Public Health. (2021) 18:30930. doi: 10.3390/ijerph18030930
72. Thomson H, Thomas S, Sellstrom E, Petticrew M. The health impacts of housing improvement: a systematic review of intervention studies from 1887 to 2007. Am J Public Health. (2009) 99(Suppl.3):S681–92. doi: 10.2105/AJPH.2008.143909
73. Wang S, Cheng C, Tan S. Housing determinants of health in urban China: a structural equation modeling analysis. Soc Indic Res. (2019) 143:1245–70. doi: 10.1007/s11205-018-2022-0
74. Attard SM, Herring AH, Zhang B, Du S, Popkin BM, Gordon-Larsen P. Associations between age, cohort, and urbanization with SBP and DBP in China: a population-based study across 18 years. J Hypertens. (2015) 33:948–56. doi: 10.1097/HJH.0000000000000522
75. Lankila T, Näyhä S, Rautio A, Koiranen M, Rusanen J, Taanila A. Health and well-being of movers in rural and urban areas–a grid-based analysis of northern Finland birth cohort 1966. Soc Sci Med. (2013) 76:169–78. doi: 10.1016/j.socscimed.2012.10.021
76. Parkin DM. Studies of cancer in migrant populations: methods and interpretation. Rev Epidemiol Sante Publique. (1992) 40:410–24.
77. Inoue Y, Howard AG, Thompson AL, Mendez MA, Herring AH, Gordon-Larsen P. The association between urbanization and reduced renal function: findings from the China Health and Nutrition Survey. BMC Nephrol. (2017) 18:160. doi: 10.1186/s12882-017-0577-7
78. Zajkowska Z, Walsh A, Zonca V, Gullett N, Pedersen GA, Kieling C, et al. A systematic review of the association between biological markers and environmental stress risk factors for adolescent depression. J Psychiatr Res. (2021) 138:163–75. doi: 10.1016/j.jpsychires.2021.04.003
79. Russell E, Koren G, Rieder M, Van Uum S. Hair cortisol as a biological marker of chronic stress: current status, future directions and unanswered questions. Psychoneuroendocrino. (2012) 37:589–601. doi: 10.1016/j.psyneuen.2011.09.009
Keywords: China, urbanization, community, psychological stress, multilevel analysis
Citation: Li D, Ruan Y, Kang Q and Rong C (2022) Gender differences in association of urbanization with psychological stress in Chinese adults: A population-based study. Front. Public Health 10:1022689. doi: 10.3389/fpubh.2022.1022689
Received: 18 August 2022; Accepted: 28 October 2022;
Published: 14 November 2022.
Edited by:
John Porter, University of London, United KingdomReviewed by:
Fanlei Kong, Shandong University, ChinaYouran Zhang, Anhui Medical University, China
Tong G. E., Shanghai Children's Medical Center, China
Zhongming Chen, Weifang Medical University, China
Xiaohua Liang, Children's Hospital of Chongqing Medical University, China
Copyright © 2022 Li, Ruan, Kang and Rong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dianjiang Li, bGlkaWFuamlhbmdAMTYzLmNvbQ==
†These authors have contributed equally to this work