 Xiaojie Hu
Xiaojie Hu Yuquan Chen
Yuquan Chen Yiting Shen1
Yiting Shen1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health, 13 October 2022
Sec. Life-Course Epidemiology and Social Inequalities in Health
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1020709
Objective: Although Hashimoto's thyroiditis is associated with cardiovascular disease and malignancy, the global status of Hashimoto's thyroiditis is not well characterized across regions. Our objective was to evaluate the prevalence and trends of Hashimoto's thyroiditis in adults in regions with different economic income levels around the world.
Methods: For this systematic review and meta-analysis, we searched PubMed, Embase, MEDLINE, Scopus, and Web of Science databases, and 48 random-effects representative studies from the inception to June 2022 were included without language restrictions to obtain the overall prevalence of Hashimoto's thyroiditis in adults worldwide. In addition, we stratified by time of publication, geographic region, economic level of the region of residence, gender, diagnostic method, etc.
Results: A total of 11,399 studies were retrieved, of which 48 met the research criteria: 20 from Europe, 16 from Asia, five from South America, three from North America, and three from Africa. Furthermore, there are two projects involving 19 countries and 22,680,155 participants. The prevalence of Hashimoto's thyroiditis was 7.5 (95%CI 5.7–9.6%), while in the low-middle-income group the prevalence was 11.4 (95%CI 2.5–25.2%). Similarly, the prevalence was 5.6 (95%Cl 3.9–7.4%) in the upper-middle-income group, and in the high-income group, the prevalence was 8.4 (95%Cl 5.6–11.8). The prevalence of Hashimoto's varied by geographic region: Africa (14.2 [95% CI 2.5–32.9%]), Oceania (11.0% [95% CI 7.8–14.7%]), South America and Europe 8.0, 7.8% (95% Cl 0.0–29.5%) in North America, and 5.8 (95% Cl 2.8–9.9%) in Asia. Although our investigator heterogeneity was high (I2), our results using a sensitivity analysis showed robustness and reliability of the findings. People living in low-middle-income areas are more likely to develop Hashimoto's thyroiditis, while the group in high-income areas are more likely to develop Hashimoto's thyroiditis than people in upper-middle-income areas, and women's risk is about four times higher than men's.
Conclusions: Global Hashimoto's thyroiditis patients are about four times as many as males, and there are discrepancies in the regions with different economic levels. In low-middle-income areas with a higher prevalence of Hashimoto's thyroiditis, especially countries in Africa, therefore local health departments should take strategic measures to prevent, detect, and treat Hashimoto's thyroiditis. At the same time, the hidden medical burden other diseases caused by Hashimoto's thyroiditis should also be done well.
Systematic review registration: https://www.crd.york.ac.uk/prospero/, identifier: CRD 42022339839.
Hashimoto's thyroiditis (HT), also known as autoimmune thyroiditis (AIT) or chronic lymphocytic thyroiditis, is an autoimmune disease of the thyroid gland, often characterized by an enlarged thyroid gland, lymphocytic infiltration, and elevated serum autoimmune antibody levels. HT is a common cause of hypothyroidism in iodine-replete settings and increases the risk of malignancy (1–3).
The prevalence of HT varies by region and socioeconomic level, ranging from 4.8–25.8% in women and 0.9–7.9% in men (4). As we all known, the prevalence of HT varies significantly depending on geographic location. Although several previous studies have systematically described the prevalence of HT, none of them reviewed global HT prevalence and trends. Current researches have shown that the global prevalence of various autoimmune diseases was increasing (5), it is worth being exploring whether the global prevalence of HT has also increased. This study aimed to quantify the possible healthcare burden and plan for the future by assessing the global prevalence and trends of HT by analyzing the prevalence of HT in different regions.
Meta-based analysis was applied in this study. Compared with traditional literature review or the emerging bibliometric analysis, systematic review and meta-analysis had a relatively broad horizon of the current hotspots and can quantitatively reflect the research status in the field (1–3). This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols guidelines (4) and is registered with the International Prospective Register of Systematic Reviews (CRD42022339839).
Five database including PubMed, Embase, MEDLINE, Scopus, and Web of Science databases were searched from inception until June 2022, with no language restrictions. The retrieval strategies included three core panels, associated with using AND connectors: (1) Hashimoto's thyroiditis, (2) Prevalence, and (3) Observational studies. The three core components are all composed of subject words and free words, which are retrieved from Pubmed's MeSH interface (Appendix 1).
The articles we included were all observational studies which reported the prevalence of HT with no interventions. We excluded articles for which full-text or original data were not available, and studies with a sample size fewer than 100 participants. Two authors (XH and YiS) independently screened eligible research records in accordance with title and abstract, respectively. And two additional authors (RT and YuS) retrieved the full text of potentially eligible articles to determine final inclusion. Inconsistent choices are resolved through discussion or third-party author participation.
Data were extracted by one author using a standardized template, cross-checked by another author, and ambiguities resolved by discussion. Extracted data included the year of publication, first author, country of publication, geographic location, study type, sample size, diagnostic method, duration, sample source, and prevalence. We used an existing checklist modified by Hoy D to assess the quality of included studies (6). The list contained a total of nine questions, each question could be answered “yes” or “no,” and answering “yes” earns one point. The final score for each study was between zero and nine. Zero to three was low quality, four to six was medium quality, and seven to nine was high quality.
We performed a meta-analysis of the extracted data and carried out statistical analysis using R software (version 4.0.3). The meta package in R software (version 4.0.3, Auckland University, USA) was mainly used for data analysis and the main outcome was assessed via single-arm analysis. For the prevalence or proportion, firstly, the normality test was conducted. If the data did not conform to the normality, it would be transformed by logarithm, logit, or double anti-sinusoidal transformation, and then, the inverse variance weighting method was used to combine.
The Cochrane Q-test and I2 value were used to test whether there was significant heterogeneity among all studies (7). According to the Meta-analysis of Observational Studies in Epidemiology guideline (8), if P > 0.10 and I2 ≤ 50%, it indicated that there was no statistical heterogeneity among the research results, and the fixed effect model was applied to analyze the results; If P ≤ 0.1 and I2 > 50%, the random effect model was used for meta-analysis. Publication bias was evaluated using Egger's test combined with a funnel plot. If there was obvious publication bias, we would use the trim-and-fill method to adjust for prospective plot asymmetry. And provided that necessary, sensitivity analysis was performed by grouping or omitting each study. Given that it was infeasible to make a quantitative synthesis and conduct a meta-analysis, a narrative approach and descriptive statistics were used. In addition, we performed subgroup analyses by income, geographic region, study type, diagnostic method, time of the study, and source of participants.
A total of 11,399 records were retrieved and identified across five databases. After removing duplicate literature, 7,989 articles were screened out. Hundred and fifty four studies were reviewed for full text, and a total of 48 studies were finally included (9–56) (Figure 1). All studies were observational (40 cross-sectional, eight cohort studies) involving 22,680,155 participants (Table 1). Thirty-seven of the 48 studies were population-based and 11 were clinical-based. Thirty-seven of the 48 studies were population-based and 11 were clinical-based. Twenty-seven studies confirmed HT was due to serum autoantibody levels, nine studies that used serum autoantibodies combined with ultrasonography to confirm the diagnosis, three studies that used serum autoantibodies to combine ultrasonography and fine needle aspiration, four studies on biopsy, only one study on ultrasonography alone, and four items not reported. Participants spanned from 1962 to 2021 and included studies published from 1966 to 2021 (Table 1). Twenty-one studies were published before 2000 and 27 studies were published after 2000. Of the 48 studies, 20 were from Europe, 16 from Asia, five from South America, three from North America, two from Africa, and two from Oceania, involving 19 countries. The quality scores of 48 articles are all six points or above, and the detailed quality assessment results are shown in Figure 2.
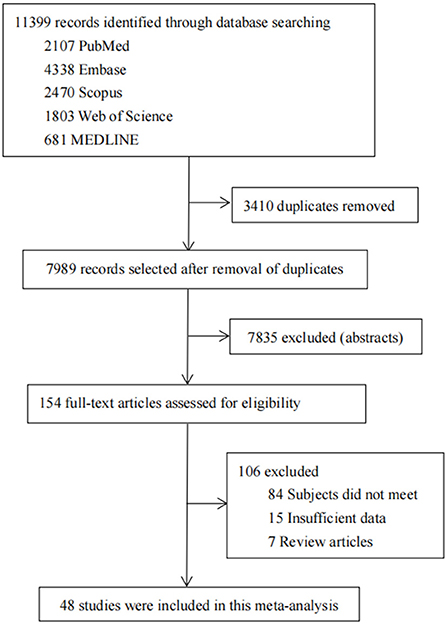
Figure 1. Study selection.

Table 1. Characteristics of included studies.
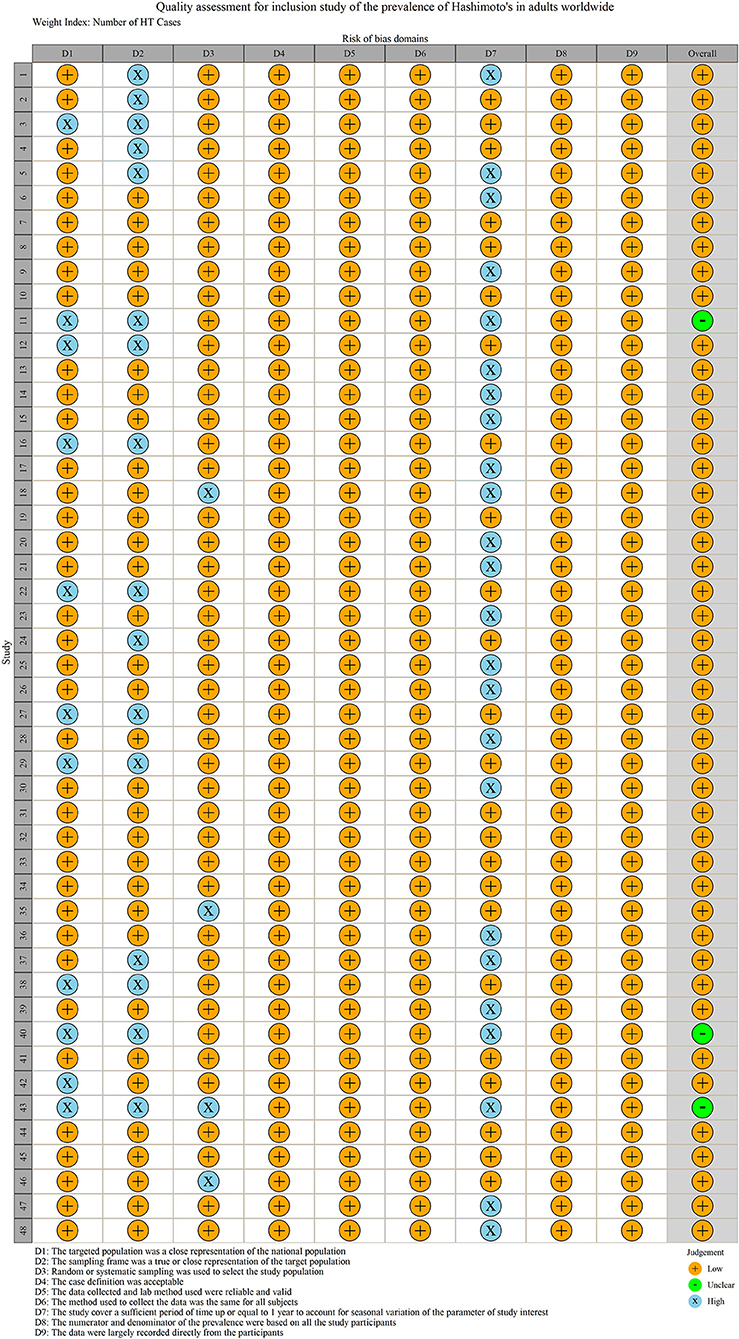
Figure 2. Literature quality assessment.
We extracted data points from 48 studies that met the inclusion criteria to form the initial data. The initial data was tested by Shapiro-Wilk (SW), P = 0.002047 < 0.05, which did not conform to the normal distribution, so we adopted Freeman-Tukey double arcsine transformation. After the transformation, the data showed a normal distribution. We executed a data pooled meta-analysis and estimated the global prevalence of HT in adults to be 7.5% (Figure 3). The prevalence of HT in adults has declined over the past 60 years, from 9% before 2000 to 6.5% after 2000 (Figure 4). HT prevalence of female adults was 3.86 adult males times (17.5 vs. 6.0%) (Figure 5). The prevalence of HT in clinical studies was 8.6% higher than in population-based studies (8.6 vs. 7.5%) (Figure 6). The prevalence of HT in adults from different continents was diverse, with the highest prevalence of HT in African adults (14.2%), followed by Oceania (11.0%), 8.0% in both South American and European adults, and 7.8% in North America. The lowest prevalence of HT in Asian adults was 5.8% (Figure 7). According to the latest income classification of the World Bank (https://datatopics.worldbank.org/world-developmentindicators/the-world-by-incomeand-region.htm), we conducted a subgroup analysis according to low-income, lower-middle-income, upper-middle-income, and high-income groups. The results showed that the prevalence of HT adults in the low-middle-income group was 11.4%, in the upper-middle-income group, the prevalence was 5.6%, and in the high-income group, the prevalence was 8.4% (Figure 8).
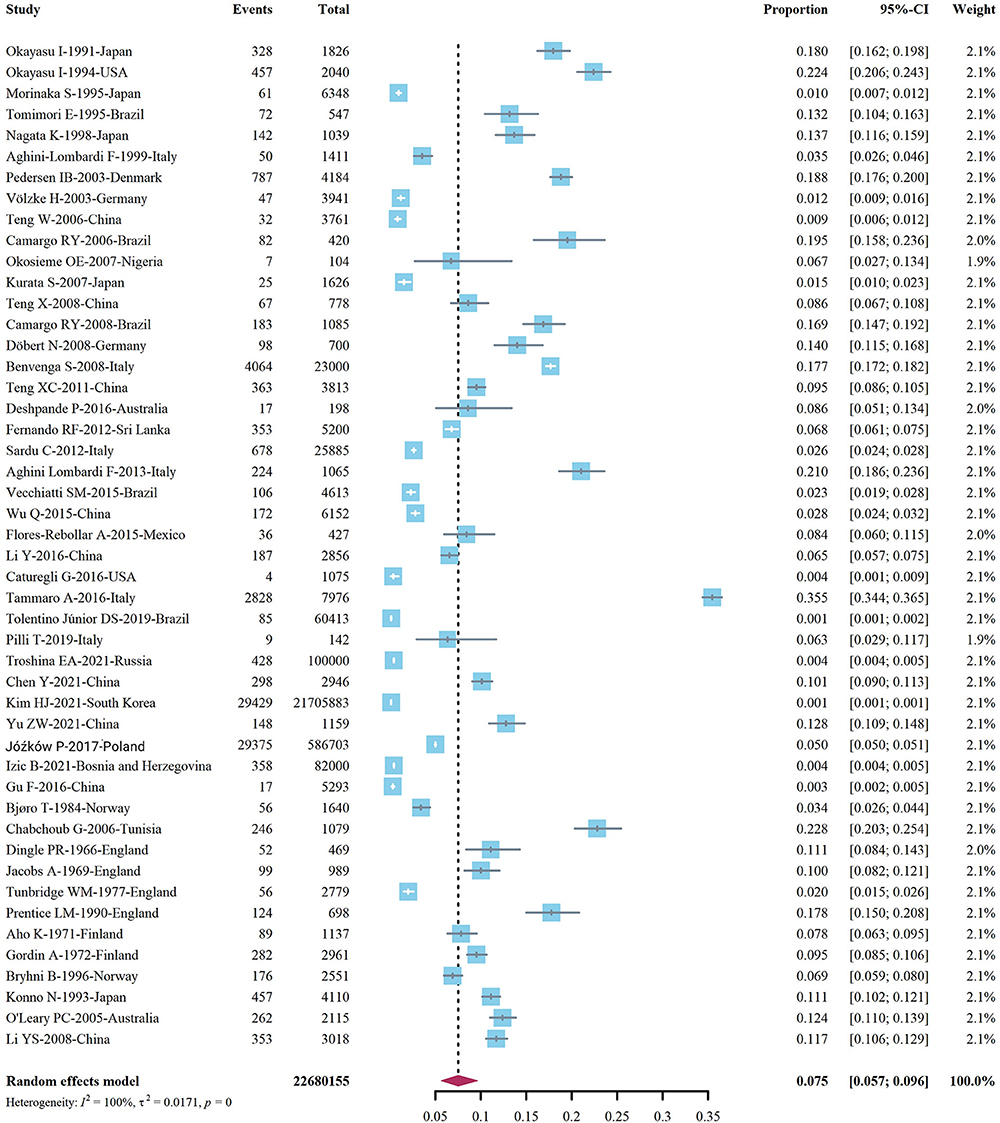
Figure 3. Global prevalence of Hashimoto's thyroiditis.
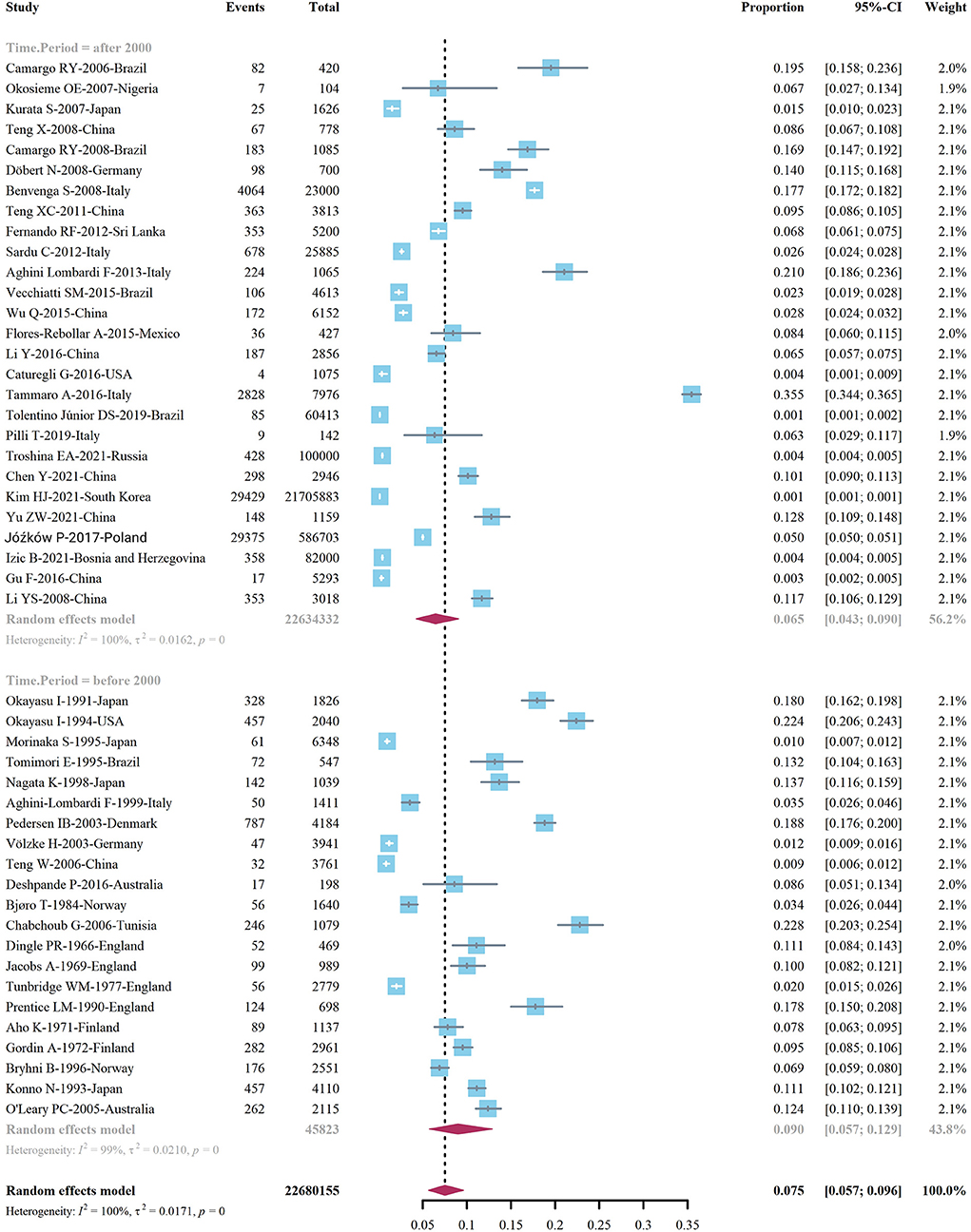
Figure 4. Global prevalence of Hashimoto's thyroiditis, by time of study implementation.
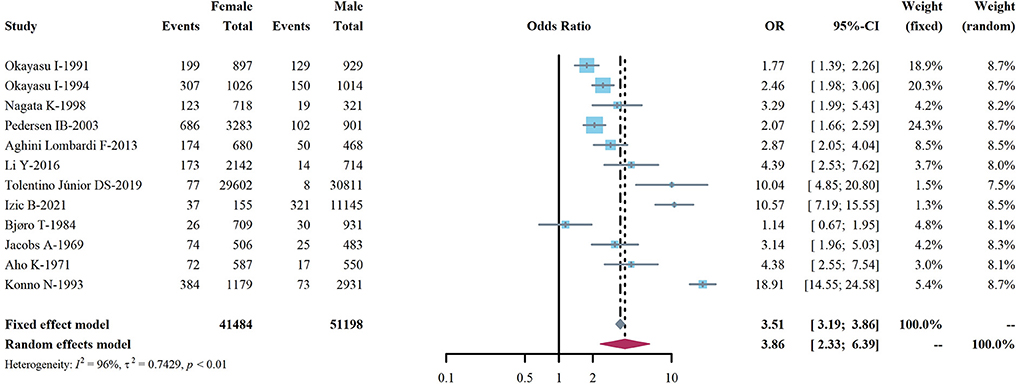
Figure 5. Global prevalence of Hashimoto's thyroiditis, by sex.

Figure 6. Global prevalence of Hashimoto's thyroiditis, by study source.
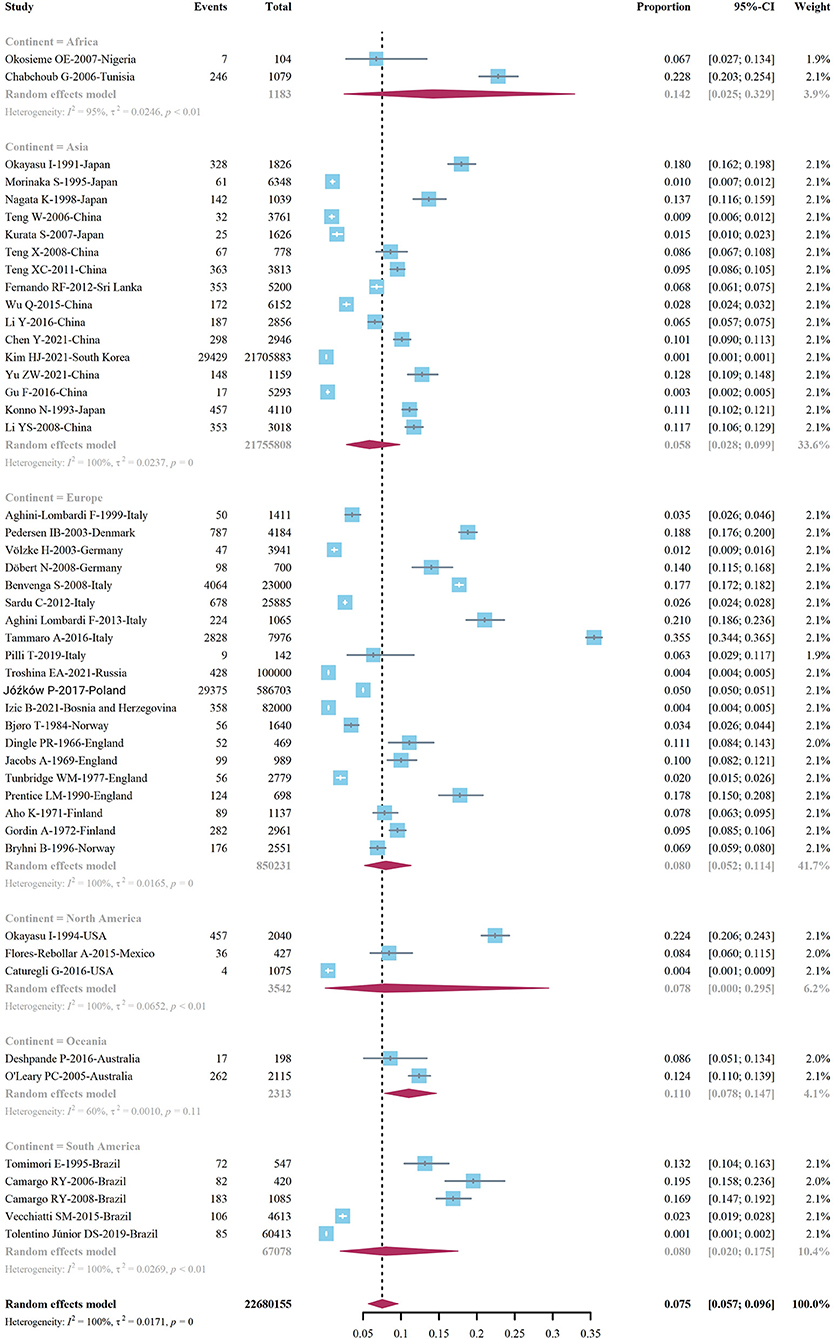
Figure 7. Global prevalence of Hashimoto's thyroiditis, by geographic location.
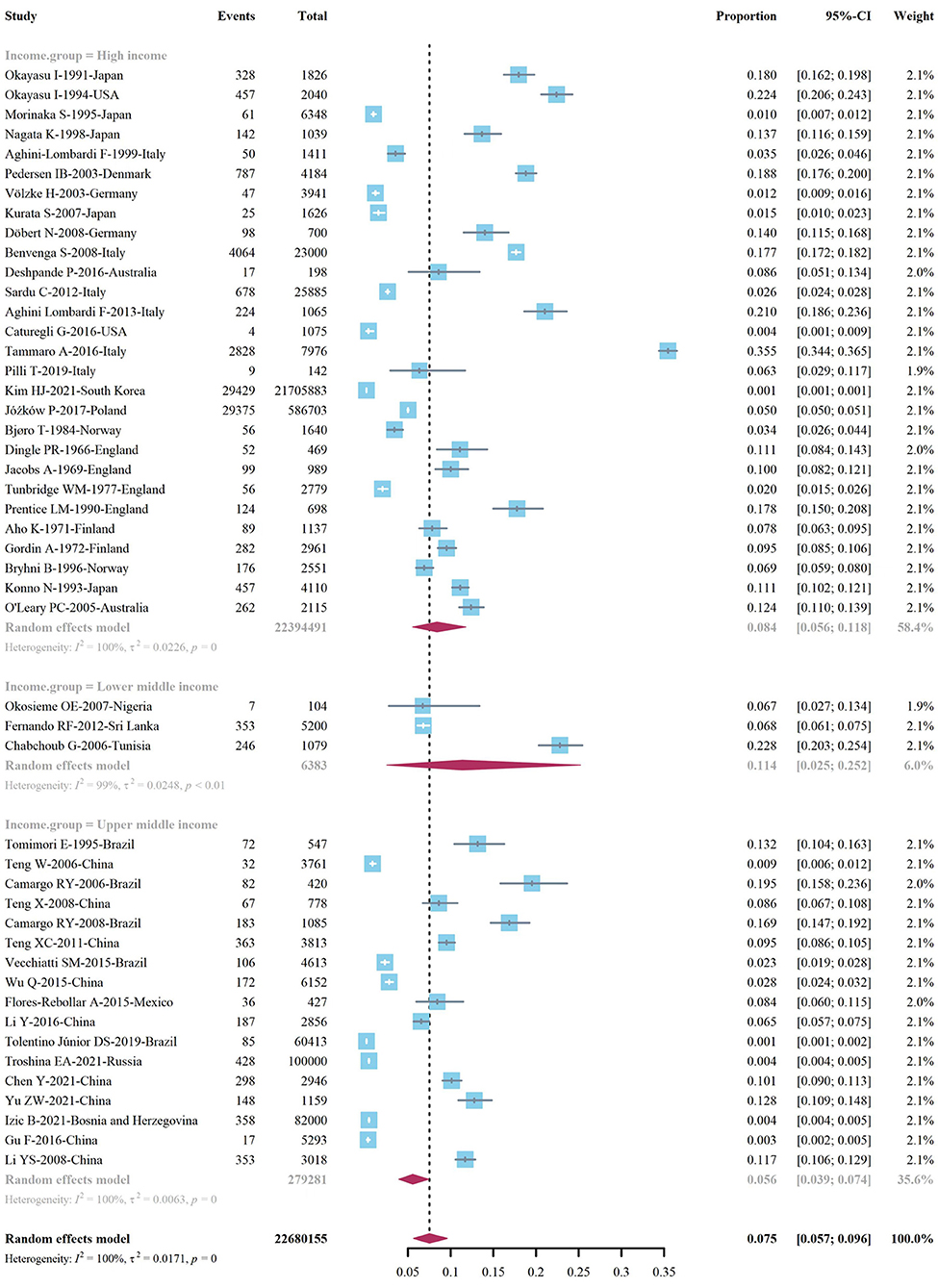
Figure 8. Global prevalence of Hashimoto's thyroiditis, by income.
We conducted a subgroup analysis according to different diagnostic methods. The results of analysis indicated that the prevalence of HT diagnosed by serum autoantibodies was 7.8 (95% Cl 5.4–10.5%), and the prevalence of HT diagnosed by ultrasonography was 13.2 (95% Cl 5.7–9.6%). Similarly, the prevalence of HT was diagnosed by pathological examination was 12.5 (95% Cl 3.3–26.5%) (Figure 9). The prevalence rate of HT diagnosed by serum autoantibody level combined with color Doppler ultrasound was 10.4 (95% Cl 5.1–17.1%), while the prevalence rate of HT diagnosed by serum autoantibody level, color Doppler ultrasonography, and fine needle aspiration (FNA) was 4.7 (95% 0.0–21.0%) (Figure 9). We performed a subgroup analysis of samples diagnosed with HT. The prevalence of HT confirmed by serum was 7.8 (95% Cl 5.8–10.1%), the prevalence of HT confirmed by serum or pathological tissue was 7.6 (95% Cl 0.0–30.2%), and the prevalence of HT confirmed by thyroid tissue alone was 14.1 (95% Cl 5.2–26.5%).
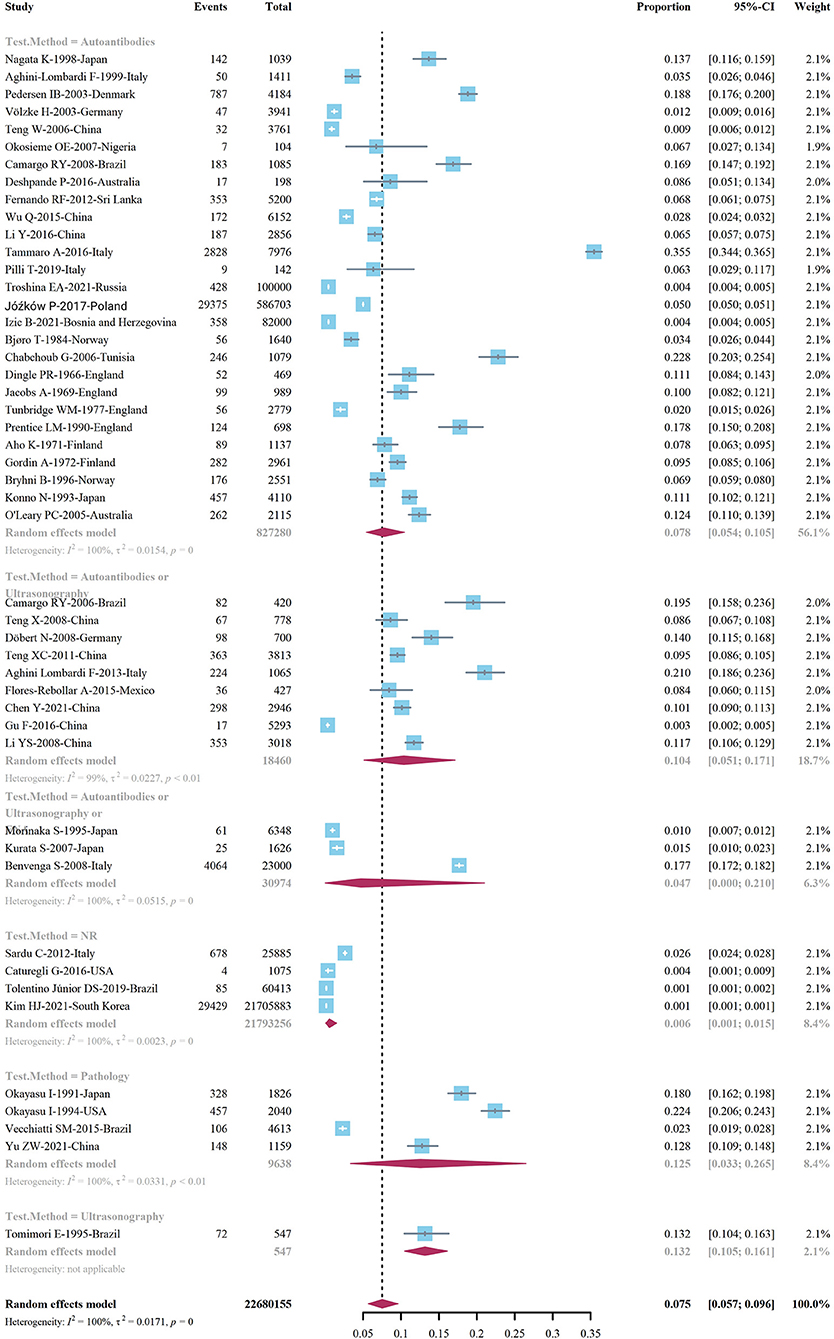
Figure 9. Subgroup analysis of diagnostic methods.
The prevalence of HT in adults varies significantly across countries, ranging as high as 22.8 (95% Cl 20.3–25.4%) in Tunisia and 18.8 (95% Cl 17.6-−20.0%) in Denmark, while the prevalence in South Korea is as low as 0.1%, and in adults in Russia and Bosnia and Herzegovina, The prevalence of HT was 0.4% (Figure 10).
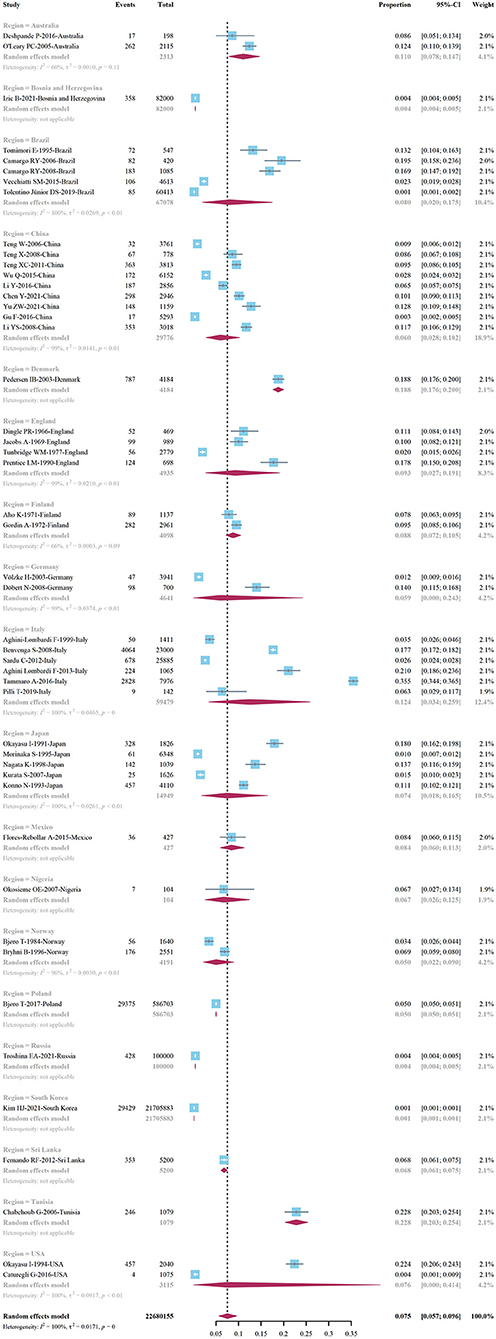
Figure 10. Prevalence of Hashimoto's thyroiditis by country.
Among the 48 observational studies, 42 studies were low risk (good quality), and 6 studies were rated as medium risk, making a risk of bears evaluation chart (Figure 11). Funnel plots and Egger's test linear regression were used to test for publication bias. There was a publication bias in each study (P < 0.05). The results are shown in the Appendix 1 (Figure 12). We used the trim-and-fill method to correct for publication bias. Sensitivity analysis showed that the literature included in this study had little impact on the results of the study analysis, and removing any one of the studies would have a small impact (Figure 13).
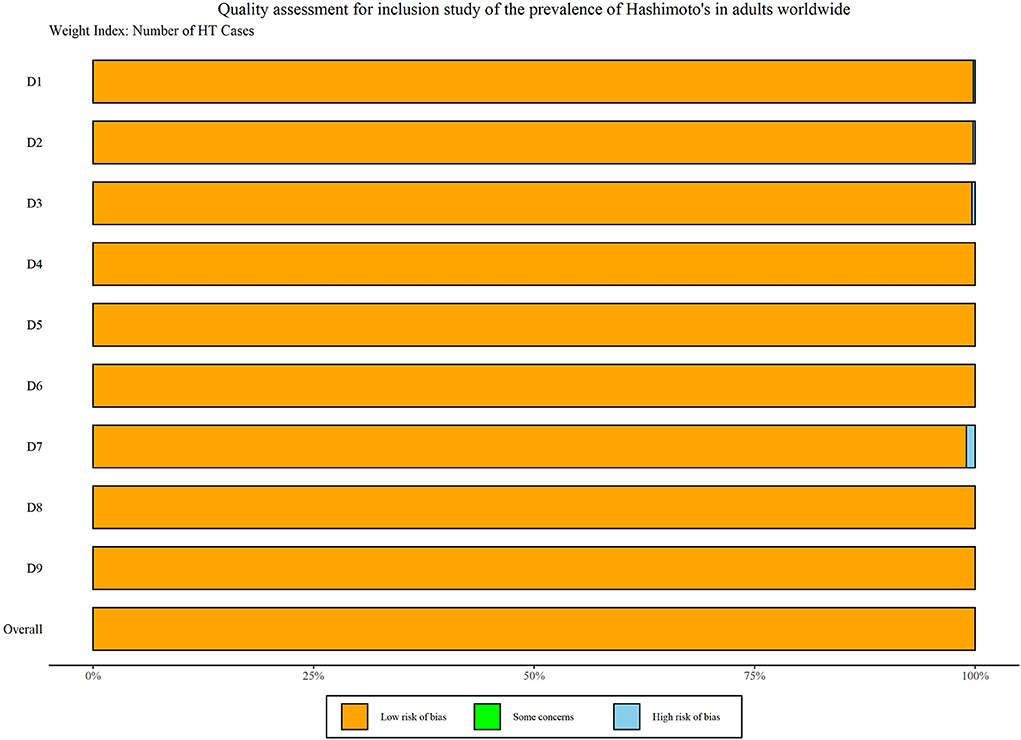
Figure 11. Literature quality risk assessment chart.
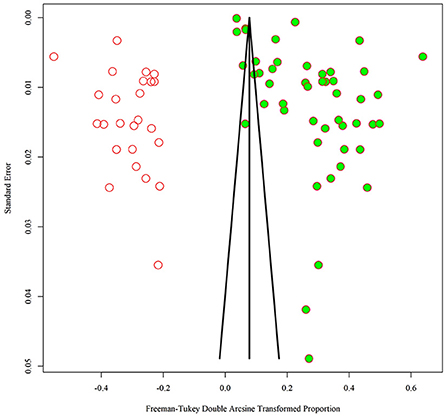
Figure 12. Trim-and-fill method to adjust for funnel plot asymmetry.
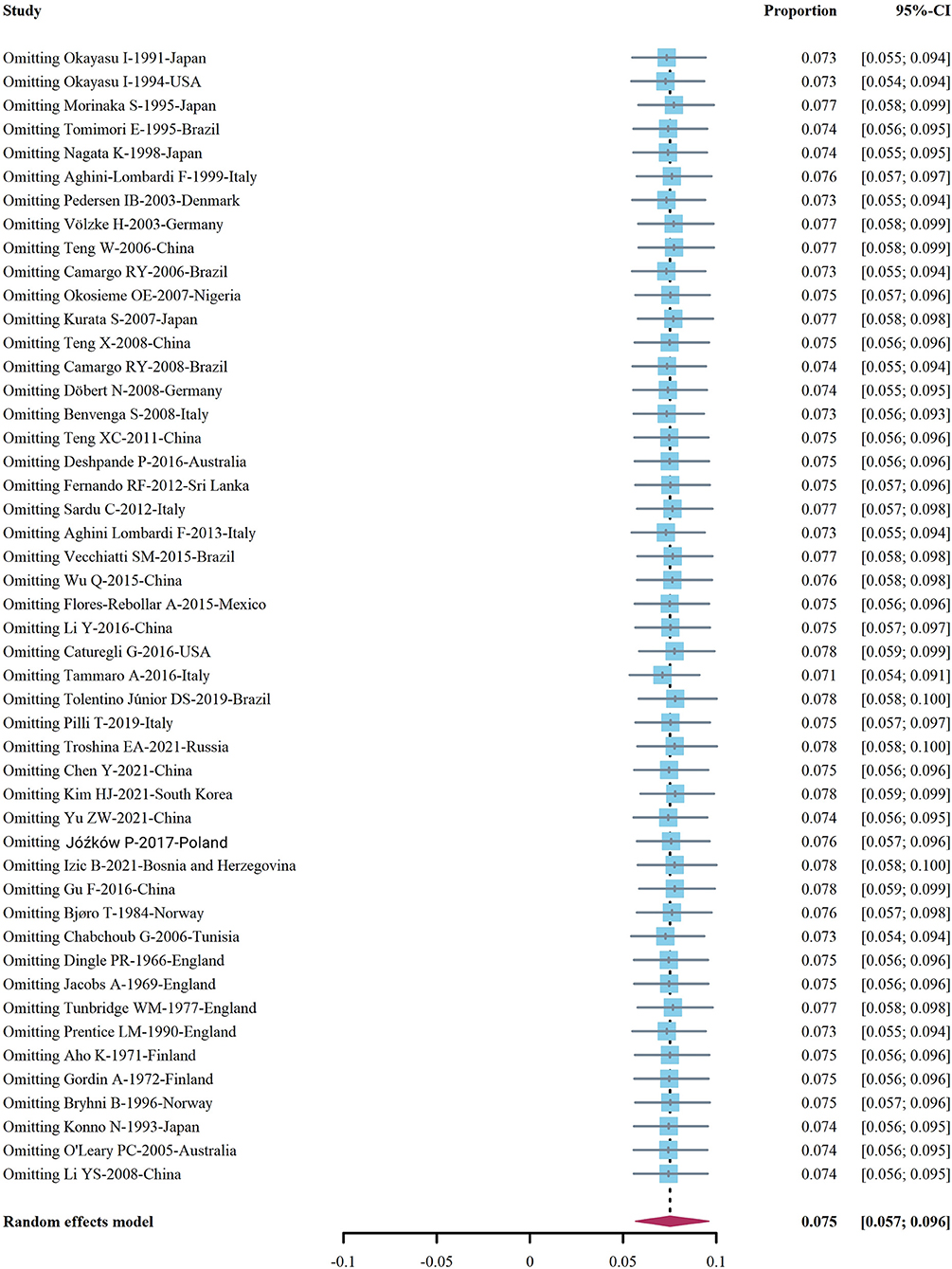
Figure 13. Sensitivity analysis chart of included studies.
This systematic review and meta-analysis provides a comprehensive assessment of the prevalence of HT in adults worldwide, which is associated with the occurrence of various malignant tumors (2, 57, 58). In total, this study pooled 48 studies involving more than 20 million adult patients with HT and performed subgroup analyses by type of study, diagnostic method, the timing of study conduct, patient source, gender, geographic location, and economic level. We found that the prevalence of HT in adults varies widely across continents. African adults have the highest prevalence of HT, more than double the prevalence in Asia. We also found that the prevalence of HT in adults decreased as time went by. Unlike previous studies (59–61), the prevalence of Hashimoto's thyroiditis in adults decreased over time.
In our study, the overall prevalence of HT in adults was 7.5%, with a prevalence of 17.5% in women and 6.0% in men. The risk of developing HT in adult women is approximately 4 times than that of adult men. Tunbridge et al. reported that in the United States, 10% of the population had thyroid antibodies, a prevalence of 14% in whites and about 5% in blacks (49). In the report, the prevalence of female HT was higher, and the ratio of female HT patients to male HT patients was 8–9:1 (60). In contrast, the prevalence of HT in the study by Gu et al. was much lower (3.2%) (24).
Our study involved 19 countries and 6 continents (Europe, Asia, South America, North America, Africa, and Oceania), and the prevalence data of HT adults in various regions of the world were aggregated to estimate the prevalence of HT in adults and development trend as far as possible. From 1960 to the present, we pooled data on adults with HT every 20 years to assess trends in the prevalence of HT in adults. We were surprised to find that the prevalence of HT in adults decreased regardless of whether we divided the study by time before and after 2000 or every 20 years. This is inconsistent with most studies. This may be related to different regions and periods, socioeconomic development, availability, and availability of medical resources. The progress of the social economy will promote people to pay more attention to physical health, increase the records of hospital visits, and also increase the chances of HT being detected and recorded. Therefore, studies in different periods in the same region have shown an increase in the prevalence of HT. Whether this is due to an increase in the prevalence of HT due to an increase in the number of people with HT or an increase in the probability of being detected is unclear. In our study, which pooled population-based and clinical-based studies separately, the prevalence of HT in adults was lower in population-based studies than in clinical studies (7.2 vs. 8.6%). This provides persuasive evidence for our hypothesis. Another reason may be that in the studies we included, the proportion of studies in different regions and different periods was different. The lowest prevalence of HT in adults (6.7%) was observed in 2000–2021, with a higher proportion of studies in Asia and Europe during this period, and a relatively high proportion of HT studies in North and South America between 1960–1981.
When we performed a subgroup analysis according to the latest income classification of the World Bank, we found an interesting phenomenon. A higher prevalence of HT among adults in low- and middle-income countries is conceivable. However, the higher prevalence of HT in adults in high-income countries than in upper-middle-income countries is indeed an interesting finding. This may be related to the pathogenesis of HT. People living in economically developed countries have increased pressure from various aspects (62), and mental health status is also an important cause of HT (61).
In our systematic review, Africa had the highest prevalence (14.2%) while Asia had the lowest prevalence (5.8%). The prevalence varies widely, which may be related to lifestyle and dietary habits. The pathogenesis of Hashimoto's thyroiditis is still unclear, and some studies have pointed out that the lack of micronutrients may be related to the pathogenesis of thyroiditis, such as vitamin D deficiency (4, 63). In Africa, some people still live a traditional way of life (gathering, hunting, nomadic animals) (64). The lack of diversification of nutrient intake due to geographic location, environmental factors, and economic level may explain the high prevalence of HT in African adults. It may also be related to the number of studies included, with 16 studies included in Asia and only two studies from Africa. We cannot rule out differences due to differences in the number of included cases. HT is a chronic inflammatory disease, and chronic inflammation increases the risk of a variety of malignancies (65–67). The studies we included were all observational studies, most of which were cross-sectional studies, only to assess the prevalence of HT, with no follow-up for later cancer risk and treatment in HT patients. Therefore, our pooled estimates of the adult prevalence of HT may underestimate the actual burden on health care.
Our study systematically evaluated the global adult prevalence of HT for the first time and includes the largest number of studies on the prevalence of HT in adults. However, our study also involves certain limitations. The period of the studies we included was large. From 1962 to 2021, there may exist differences in the diagnostic criteria and detection methods of HT in different periods. In many cases, we were unable to obtain specific information on the diagnostic criteria for HT in the studies. Although we were unable to unify the diagnostic criteria for HT, we analyzed the prevalence of HT in adults by detection method. There was considerable heterogeneity among studies, and we performed subgroup analyses where possible, but this did not reduce heterogeneity between studies. This may be related to the regional economy, dietary habits, lifestyle, and diagnostic criteria of HT in different periods of the included studies. Sensitivity analysis showed that each study included in the study had little effect on the results and had good stability. The studies we included may have some selection bias, but the information in the studies was insufficient to assess these errors. We hope that the diagnostic criteria for HT will be unified as much as possible in future research so that the research results will be more convincing.
In conclusion, we found that the prevalence of Hashimoto's thyroiditis in adult females is approximately four times that of male patients, and the prevalence of HT is relatively high in adults worldwide, especially in Africa. There are differences in the prevalence of HT among adults at different economic levels. The prevalence of HT in low- and middle-income countries is the highest, and the prevalence in high-income countries is higher than that in upper-middle-income countries. Therefore, we suggest that public health departments in low- and middle-income countries should take strategic measures to prevent, detect, and treat HT as early as possible, while high-income countries should also pay attention to the prevalence of HT and the burden of medical services.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
XH and YShen conceptualized, involved, and conducted this study. XH wrote the first draft under the guidance of HQ. YC, YShen, YSheng, and RT reviewed drafts and provided input for all versions. XH and YC accessed, verified, analyzed, and interpreted the data. All authors contributed to the article and approved the submitted version.
This project was supported by the Shanghai Key Clinical Specialty Construction Project of China (shslczdzk03801).
The authors thank YC from Institute of Medical Information/Medical Library, Chinese Academy of Medical Sciences and Peking Union Medical College for his contribution to data analysis.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ragusa F, Fallahi P, Elia G, Gonnella D, Paparo SR, Giusti C, et al. Hashimotos' thyroiditis: epidemiology, pathogenesis, clinic and therapy. Best Pract Res Clin Endocrinol Metab. (2019) 33:101367. doi: 10.1016/j.beem.2019.101367
2. Feldt-Rasmussen U. Hashimoto's thyroiditis as a risk factor for thyroid cancer. Curr Opin Endocrinol Diabetes Obes. (2020) 27:364–71. doi: 10.1097/MED.0000000000000570
3. Hu X, Wang X, Liang Y, Chen X, Zhou S, Fei W, et al. Cancer risk in Hashimoto's thyroiditis: a systematic review and meta-analysis. Front Endocrinol. (2022) 13:937871. doi: 10.3389/fendo.2022.937871
4. Mikulska AA, Karazniewicz-Łada M, Filipowicz D, Ruchała M, Główka FK. Metabolic characteristics of Hashimoto's thyroiditis patients and the role of microelements and diet in the disease management-an overview. Int J Mol Sci. (2022) 23:6580. doi: 10.3390/ijms23126580
5. Lerner A, Jeremias P, Matthias T. The world incidence and prevalence of autoimmune diseases is increasing. Int J Celiac Dis. (2015) 3:151–5. doi: 10.12691/ijcd-3-4-8
6. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. (2012) 65:934–9. doi: 10.1016/j.jclinepi.2011.11.014
7. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
8. Greeenwood DC. Meta-analysis of observational studies. In:Tu YK, Greenwood D, , editors. Modern Methods for Epidemiology. Dordrecht: Springer (2012). p. 173–89. doi: 10.1007/978-94-007-3024-3_10
9. Okayasu I, Hatakeyama S, Tanaka Y, Sakurai T, Hoshi K, Lewis PD. Is focal chronic autoimmune thyroiditis an age-related disease? Differences in incidence and severity between Japanese and British. J Pathol. (1991) 163:257–64. doi: 10.1002/path.1711630312
10. Okayasu I, Hara Y, Nakamura K, Rose NR. Racial and age-related differences in incidence and severity of focal autoimmune thyroiditis. Am J Clin Pathol. (1994) 101:698–702. doi: 10.1093/ajcp/101.6.698
11. Morinaka S. On the frequency of thyroid diseases in outpatients in an ENT clinic. Auris Nasus Larynx. (1995) 22:186–91. doi: 10.1016/S0385-8146(12)80057-5
12. Tomimori E, Pedrinola F, Cavaliere H, Knobel M, Medeiros-Neto G. Prevalence of incidental thyroid disease in a relatively low iodine intake area. Thyroid. (1995) 5:273–6. doi: 10.1089/thy.1995.5.273
13. Nagata K, Takasu N, Akamine H, Ohshiro C, Komiya I, Murakami K, et al. Urinary iodine and thyroid antibodies in Okinawa, Yamagata, Hyogo, and Nagano, Japan: the differences in iodine intake do not affect thyroid antibody positivity. Endocr J. (1998) 45:797–803. doi: 10.1507/endocrj.45.797
14. Aghini-Lombardi F, Antonangeli L, Martino E, Vitti P, Maccherini D, Leoli F, et al. The spectrum of thyroid disorders in an iodine-deficient community: the Pescopagano survey. J Clin Endocrinol Metab. (1999) 84:561–6. doi: 10.1210/jc.84.2.561
15. Pedersen IB, Knudsen N, Jørgensen T, Perrild H, Ovesen L, Laurberg P. Thyroid peroxidase and thyroglobulin autoantibodies in a large survey of populations with mild and moderate iodine deficiency. Clin Endocrinol (Oxf). (2003) 58:36–42. doi: 10.1046/j.1365-2265.2003.01633.x
16. Völzke H, Lüdemann J, Robinson DM, Spieker KW, Schwahn C, Kramer A, et al. The prevalence of undiagnosed thyroid disorders in a previously iodine-deficient area. Thyroid. (2003) 13:803–10. doi: 10.1089/105072503768499680
17. Teng W, Shan Z, Teng X, Guan H, Li Y, Teng D, et al. Effect of iodine intake on thyroid diseases in China. N Engl J Med. (2006) 354:2783–93. doi: 10.1056/NEJMoa054022
18. Camargo RY, Tomimori EK, Neves SC, Knobel M, Medeiros-Neto G. Prevalence of chronic autoimmune thyroiditis in the urban area neighboring a petrochemical complex and a control area in Sáo Paulo, Brazil. Clinics. (2006) 61:307–12. doi: 10.1590/S1807-59322006000400006
19. Okosieme OE, Taylor RC, Ohwovoriole AE, Parkes AB, Lazarus JH. Prevalence of thyroid antibodies in Nigerian patients. QJM. (2007) 100:107–12. doi: 10.1093/qjmed/hcl137
20. Kurata S, Ishibashi M, Hiromatsu Y, Kaida H, Miyake I, Uchida M, et al. Diffuse and diffuse-plus-focal uptake in the thyroid gland identified by using FDG-PET: prevalence of thyroid cancer and Hashimoto's thyroiditis. Ann Nucl Med. (2007) 21:325–30. doi: 10.1007/s12149-007-0030-2
21. Teng X, Shi X, Shan Z, Jin Y, Guan H, Li Y, et al. Safe range of iodine intake levels: a comparative study of thyroid diseases in three women population cohorts with slightly different iodine intake levels. Biol Trace Elem Res. (2008) 121:23–30. doi: 10.1007/s12011-007-8036-0
22. Camargo RY, Tomimori EK, Neves SC G S, Rubio I, Galrão AL, Knobel M, et al. Thyroid and the environment: exposure to excessive nutritional iodine increases the prevalence of thyroid disorders in Sáo Paulo, Brazil. Eur J Endocrinol. (2008) 159:293–9. doi: 10.1530/EJE-08-0192
23. Döbert N, Balzer K, Diener J, Wegscheider K, Vaupel R, Grünwald F. Thyroid sonomorphology, thyroid peroxidase antibodies and thyroid function: new epidemiological data in unselected German employees. Nuklearmedizin. (2008) 47:194–9. doi: 10.3413/nukmed-0166
24. Benvenga S, Trimarchi F. Changed presentation of Hashimoto's thyroiditis in North-Eastern Sicily and Calabria (Southern Italy) based on a 31-year experience. Thyroid. (2008) 18:429–41. doi: 10.1089/thy.2007.0234
25. Teng X, Shan Z, Chen Y, Lai Y, Yu J, Shan L, et al. More than adequate iodine intake may increase subclinical hypothyroidism and autoimmune thyroiditis: a cross-sectional study based on two Chinese communities with different iodine intake levels. Eur J Endocrinol. (2011) 164:943–50. doi: 10.1530/EJE-10-1041
26. Deshpande P, Lucas M, Brunt S, Lucas A, Hollingsworth P, Bundell C. Low level autoantibodies can be frequently detected in the general Australian population. Pathology. (2016) 48:483–90. doi: 10.1016/j.pathol.2016.03.014
27. Fernando RF, Chandrasinghe PC, Pathmeswaran AA. The prevalence of autoimmune thyroiditis after universal salt iodization in Sri Lanka. Ceylon Med J. (2012) 57:116–9. doi: 10.4038/cmj.v57i3.4702
28. Sardu C, Cocco E, Mereu A, Massa R, Cuccu A, Marrosu MG, et al. Population based study of 12 autoimmune diseases in Sardinia, Italy: prevalence and comorbidity. PLoS One. (2012) 7:e32487. doi: 10.1371/journal.pone.0032487
29. Aghini Lombardi F, Fiore E, Tonacchera M, Antonangeli L, Rago T, Frigeri M, et al. The effect of voluntary iodine prophylaxis in a small rural community: the Pescopagano survey 15 years later. J Clin Endocrinol Metab. (2013) 98:1031–9. doi: 10.1210/jc.2012-2960
30. Vecchiatti SM, Lin CJ, Capelozzi VL, Longatto-Filho A, Bisi H. Prevalence of thyroiditis and immunohistochemistry study searching for a morphologic consensus in morphology of autoimmune thyroiditis in a 4613 autopsies series. Appl Immunohistochem Mol Morphol. (2015) 23:402–8. doi: 10.1097/PAI.0000000000000094
31. Wu Q, Rayman MP, Lv H, Schomburg L, Cui B, Gao C, et al. Low population selenium status is associated with increased prevalence of thyroid disease. J Clin Endocrinol Metab. (2015) 100:4037–47. doi: 10.1210/jc.2015-2222
32. Flores-Rebollar A, Moreno-Castañeda L, Vega-Servín NS, López-Carrasco G, Ruiz-Juvera A. Prevalence of autoimmune thyroiditis and thyroid dysfunction in healthy adult Mexicans with a slightly excessive iodine intake. Nutr Hosp. (2015) 32:918–24. doi: 10.3305/nh.2015.32.2.9246
33. Li Y, Chen DN, Cui J, Xin Z, Yang GR, Niu MJ, et al. Using Hashimoto thyroiditis as gold standard to determine the upper limit value of thyroid stimulating hormone in a Chinese cohort. BMC Endocr Disord. (2016) 16:57. doi: 10.1186/s12902-016-0137-3
34. Caturegli G, Caturegli P. Disease prevalence in a rural Andean population of central Peru: a focus on autoimmune and allergic diseases. Auto Immun Highlights. (2016) 7:3. doi: 10.1007/s13317-016-0076-z
35. Tammaro A, Pigliacelli F, Fumarola A, Persechino S. Trends of thyroid function and autoimmunity to 5 years after the introduction of mandatory iodization in Italy. Eur Ann Allergy Clin Immunol. (2016) 48:77–81.
36. Tolentino Júnior DS, de Oliveira CM, de Assis EM. Population-based study of 24 autoimmune diseases carried out in a Brazilian microregion. J Epidemiol Glob Health. (2019) 9:243–51. doi: 10.2991/jegh.k.190920.001
37. Pilli T, Cardinale S, Dalmiglio C, Secchi C, Fralassi N, Cevenini G, et al. Autoimmune thyroid diseases are more common in patients with prolactinomas: a retrospective case-control study in an Italian cohort. J Endocrinol Invest. (2019) 42:693–8. doi: 10.1007/s40618-018-0972-3
38. Troshina EA, Platonova NM. Panfilova EA. Probl Endokrinol (Mosk). (2021) 67:10–9. doi: 10.14341/probl12433
39. Chen Y, Han B, Yu J, Chen Y, Cheng J, Zhu C, et al. Influence of rapid urbanization on thyroid autoimmune disease in China. Int J Endocrinol. (2021) 2021:9967712. doi: 10.1155/2021/9967712
40. Kim HJ, Kazmi SZ, Kang T, Sohn SY, Kim DS, Hann HJ, et al. Familial risk of Hashimoto's thyroiditis among first-degree relatives: a population-based study in Korea. Thyroid. (2021) 31:1096–104. doi: 10.1089/thy.2020.0213
41. Yu Z, Yu Y, Wan Y, Fan J, Meng H, Li S, et al. Iodine intake level and incidence of thyroid disease in adults in Shaanxi province: a cross-sectional study. Ann Transl Med. (2021) 9:1567. doi: 10.21037/atm-21-4928
42. Józków P, Lwow F, Słowińska-Lisowska M, Medraś M. Trends in the prevalence of autoimmune thyroiditis in the leading private health-care provider in Poland. Adv Clin Exp Med. (2017) 26:497–503. doi: 10.17219/acem/60862
43. Izic B, Custovic A, Caluk S, Fejzic H, Kundalic BS, Husejnovic MS. The Epidemiological characteristics of autoimmune thyroiditis in the Tuzla Canton in the period from 2015 to 2020. Mater Sociomed. (2021) 33:288–92. doi: 10.5455/msm.2021.33.288-292
44. Gu F, Ding G, Lou X, Wang X, Mo Z, Zhu W, et al. Incidence of thyroid diseases in Zhejiang Province, China, after 15 years of salt iodization. J Trace Elem Med Biol. (2016) 36:57–64. doi: 10.1016/j.jtemb.2016.04.003
45. Bjøro T, Gaarder PI, Smeland EB, Kornstad L. Thyroid antibodies in blood donors: prevalence and clinical significance. Acta Endocrinol (Copenh). (1984) 105:324–9. doi: 10.1530/acta.0.1050324
46. Chabchoub G, Mnif M, Maalej A, Charfi N, Ayadi H, Abid M. Etude épidémiologique des maladies autoimmunes thyroïdiennes dans le sud tunisien [Epidemiologic study of autoimmune thyroid disease in south Tunisia]. Ann Endocrinol. (2006) 67:591–5. doi: 10.1016/S0003-4266(06)73012-8
47. Dingle PR, Ferguson A, Horn DB, Tubmen J, Hall R. The incidence of thyroglobulin antibodies and thyroid enlargement in a general practice in north-east England. Clin Exp Immunol. (1966) 1:277–84.
48. Jacobs A, Entwistle CC, Campbell H, Waters WE. A random sample from Wales. IV Circulating gastric and thyroid antibodies and antinuclear factor. Br J Haematol. (1969) 17:589–95. doi: 10.1111/j.1365-2141.1969.tb01410.x
49. Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, Clark F, et al. The spectrum of thyroid disease in a community: the Whickham survey. Clin Endocrinol. (1977) 7:481–93. doi: 10.1111/j.1365-2265.1977.tb01340.x
50. Prentice LM, Phillips DI, Sarsero D, Beever K, McLachlan SM, Smith BR. Geographical distribution of subclinical autoimmune thyroid disease in Britain: a study using highly sensitive direct assays for autoantibodies to thyroglobulin and thyroid peroxidase. Acta Endocrinol. (1990) 123:493–8. doi: 10.1530/acta.0.1230493
51. Sharma D, Tuomi J. Determination of thyroglobulin antibodies in obese strain chicken sera using chromic chloride as a coupling reagent. Acta Vet Scand. (1973) 14:651–6. doi: 10.1186/BF03547393
52. Gordin A, Heinonen OP, Saarinen P, Lamberg BA. Serum-thyrotrophin in symptomless autoimmune thyroiditis. Lancet. (1972) 1:551–4. doi: 10.1016/S0140-6736(72)90353-4
53. Bryhni B, Aanderud S, Sundsfjord J, Rekvig OP, Jorde R. Thyroid antibodies in northern Norway: prevalence, persistence and relevance. J Intern Med. (1996) 239:517–23. doi: 10.1046/j.1365-2796.1996.488823000.x
54. Konno N, Yuri K, Taguchi H, Miura K, Taguchi S, Hagiwara K, et al. Screening for thyroid diseases in an iodine sufficient area with sensitive thyrotrophin assays, and serum thyroid autoantibody and urinary iodide determinations. Clin Endocrinol. (1993) 38:273–81. doi: 10.1111/j.1365-2265.1993.tb01006.x
55. O'Leary PC, Feddema PH, Michelangeli VP, Leedman PJ, Chew GT, Knuiman M, et al. Investigations of thyroid hormones and antibodies based on a community health survey: the Busselton thyroid study. Clin Endocrinol. (2006) 64:97–104. doi: 10.1111/j.1365-2265.2005.02424.x
56. Li Y, Teng D, Shan Z, Teng X, Guan H, Yu X, et al. Antithyroperoxidase and antithyroglobulin antibodies in a five-year follow-up survey of populations with different iodine intakes. J Clin Endocrinol Metab. (2008) 93:1751–7. doi: 10.1210/jc.2007-2368
57. Jackson D, Handelsman RS, Farrá JC, Lew JI. Increased incidental thyroid cancer in patients with subclinical chronic lymphocytic thyroiditis. J Surg Res. (2020) 245:115–8. doi: 10.1016/j.jss.2019.07.025
58. Uhliarova B, Hajtman A. Hashimoto's thyroiditis - an independent risk factor for papillary carcinoma. Braz J Otorhinolaryngol. (2018) 84:729–35. doi: 10.1016/j.bjorl.2017.08.012
59. McLeod DS, Cooper DS. The incidence and prevalence of thyroid autoimmunity. Endocrine. (2012) 42:252–65. doi: 10.1007/s12020-012-9703-2
60. Hollowell JG, Staehling NW, Flanders WD, Hannon WH, Gunter EW, Spencer CA, et al. Serum TSH, T, and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab. (2002) 87:489–99. doi: 10.1210/jcem.87.2.8182
61. Ajjan RA, Weetman AP. The pathogenesis of Hashimoto's thyroiditis: further developments in our understanding. Horm Metab Res. (2015) 47:702–10. doi: 10.1055/s-0035-1548832
62. Dunlap LJ, Han B, Dowd WN, Cowell AJ, Forman-Hoffman VL, Davies MC, et al. Behavioral health outcomes among adults: associations with individual and community-level economic conditions. Psychiatr Serv. (2016) 67:71–7. doi: 10.1176/appi.ps.201400016
63. Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al. Prevalence of vitamin D deficiency in Africa: a systematic review and meta-analysis. Lancet Glob Health. (2020) 8:e134-e142. doi: 10.1016/S2214-109X(19)30457-7
64. Luxwolda MF, Kuipers RS, Kema IP, van der Veer E, Dijck-Brouwer DA, Muskiet FA. Vitamin D status indicators in indigenous populations in East Africa. Eur J Nutr. (2013) 52:1115–25. doi: 10.1007/s00394-012-0421-6
65. Hussain SP, Harris CC. Inflammation and cancer: an ancient link with novel potentials. Int J Cancer. (2007) 121:2373–80. doi: 10.1002/ijc.23173
66. Khandia R, Munjal A. Interplay between inflammation and cancer. Adv Protein C hem Struct Biol. (2020) 119:199–245. doi: 10.1016/bs.apcsb.2019.09.004
67. Ohnishi S, Ma N, Thanan R, Pinlaor S, Hammam O, Murata M, et al. DNA damage in inflammation-related carcinogenesis and cancer stem cells. Oxid Med Cell Longev. (2013) 2013:387014. doi: 10.1155/2013/387014
Literature search strategies.
Pubmed: ((((epidemiology[Title/Abstract])) OR (incidence[Title/Abstract])) OR (prevalence[Title/Abstract])) AND ((”Hashimoto Disease“[Mesh]) OR ((((((((((((((((((((((((Disease, Hashimoto[Title/Abstract])) OR (Hashimoto Struma[Title/Abstract])) OR (Hashimoto Thyroiditis[Title/Abstract])) OR (Hashimoto Thyroiditides[Title/Abstract])) OR (Thyroiditides, Hashimoto[Title/Abstract])) OR (Thyroiditis, Hashimoto[Title/Abstract])) OR (Hashimoto's Syndrome[Title/Abstract])) OR (Hashimoto Syndrome[Title/Abstract])) OR (Hashimoto's Syndromes[Title/Abstract])) OR (Hashimotos Syndrome[Title/Abstract])) OR (Syndrome, Hashimoto's[Title/Abstract])) OR (Syndromes, Hashimoto's[Title/Abstract])) OR (Hashimoto's Struma[Title/Abstract])) OR (Chronic Lymphocytic Thyroiditis[Title/Abstract])) OR (Chronic Lymphocytic Thyroiditides[Title/Abstract])) OR (Lymphocytic Thyroiditides, Chronic[Title/Abstract])) OR (Lymphocytic Thyroiditis, Chronic[Title/Abstract])) OR (Thyroiditides, Chronic Lymphocytic[Title/Abstract])) OR (Thyroiditis, Chronic Lymphocytic[Title/Abstract])) OR (Hashimoto's Disease[Title/Abstract])) OR (Disease, Hashimoto's[Title/Abstract])) OR (Hashimotos Disease[Title/Abstract])) OR (Autoimmune thyroiditis[Title/Abstract]))).
Keywords: Hashimoto's thyroiditis, global prevalence, epidemiological trends, systematic review, meta-analysis
Citation: Hu X, Chen Y, Shen Y, Tian R, Sheng Y and Que H (2022) Global prevalence and epidemiological trends of Hashimoto's thyroiditis in adults: A systematic review and meta-analysis. Front. Public Health 10:1020709. doi: 10.3389/fpubh.2022.1020709
Received: 16 August 2022; Accepted: 29 September 2022;
Published: 13 October 2022.
Edited by:
Masoud Dadashi, Alborz University of Medical Sciences, IranReviewed by:
Mengli Guo, Guangzhou First People's Hospital, ChinaCopyright © 2022 Hu, Chen, Shen, Tian, Sheng and Que. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huafa Que, aHVhZmFxdWVAMTI2LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.