
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health , 13 January 2023
Sec. Public Health and Nutrition
Volume 10 - 2022 | https://doi.org/10.3389/fpubh.2022.1016819
 Álvaro González-Domínguez1
Álvaro González-Domínguez1 Jesús Domínguez-Riscart1,2
Jesús Domínguez-Riscart1,2 María Millán-Martínez3,4
María Millán-Martínez3,4 Alfonso María Lechuga-Sancho1,2,5
Alfonso María Lechuga-Sancho1,2,5 Raúl González-Domínguez1*
Raúl González-Domínguez1*Diet is one of the most important modifiable lifestyle factors for preventing and treating obesity. In this respect, the Mediterranean diet (MD) has proven to be a rich source of a myriad of micronutrients with positive repercussions on human health. Herein, we studied an observational cohort of children and adolescents with obesity (N = 26) to explore the association between circulating blood trace elements and the degree of MD adherence, as assessed through the KIDMED questionnaire. Participants with higher MD adherence showed better glycemic/insulinemic control and a healthier lipid profile, as well as raised plasma levels of selenium, zinc, cobalt, molybdenum, and arsenic, and increased erythroid content of selenium. Interestingly, we found that these MD-related mineral alterations were closely correlated with the characteristic metabolic complications behind childhood obesity, namely hyperglycemia, hyperinsulinemia, and dyslipidemia (p < 0.05, |r| > 0.35). These findings highlight the pivotal role that dietary trace elements may play in the pathogenesis of obesity and related disorders.
Obesity is a condition characterized by an excessive accumulation of body fat, which may have significant negative repercussions on health and raise the risk of developing other chronic diseases. The main driver of obesity is an imbalance between total energy intake and expenditure within the framework of a complex interplay involving multiple players, including genetic, metabolic, environmental, and behavioral factors (1). In this context, diet is well-recognized to be one of the most important modifiable lifestyle factors in the prevention and treatment of obesity and related disorders. On the one hand, the over-consumption of calories is the most likely cause of the obesity epidemic, mainly because of the loss of traditional dietary patterns and the increasingly frequent intake of energy-dense foods (e.g., high-fat foods) and added sugar-containing foods (2). Moreover, the adherence to unhealthy diets has also been linked to deficiencies of multiple micronutrients, including vitamins, carotenoids, and trace elements, which in turn may contribute and aggravate the pathogenic events behind obesity (3). Trace elements are essential micronutrients that are primarily acquired through the diet and participate in a myriad of primary biological process, including the antioxidant defense, immune system, hormonal regulation, and many others. In particular, growing evidence points to essential and toxic metals as pivotal regulators of a myriad of biological processes underlying the development and progression of obesity and its comorbidities (4). For instance, it has been repeatedly reported that numerous trace elements (e.g., zinc, chromium, vanadium, molybdenum, cobalt) play central roles in the synthesis, storage, and action of insulin, and consequently influence carbohydrate and lipid metabolism (5). Their correct homeostasis, both in terms of potentially pro-oxidant species (e.g., iron, copper) and elements participating in the antioxidant defense (e.g., selenium, manganese), is also crucial to maintain an adequate redox status (6, 7). Furthermore, it is noteworthy that metals and the immune system are bidirectionally interrelated, being mineral deficiencies associated with impaired immune function, whereas the inflammatory response (e.g., secretion of cytokines) can modulate the metabolism and bioavailability of trace elements and other nutrients (8). On the other hand, the exposure to toxic heavy metals (e.g., cadmium, mercury, lead) has been demonstrated to disrupt the endocrine system and to induce chronic inflammation and oxidative stress (9).
A few authors have previously studied the influence of diet determinants on the levels of specific metals among healthy children (10, 11), but this remains unexplored in obese populations. Obesity is nowadays the most prevalent chronic disease among children and adolescents, which can be often accompanied by different comorbidities related to abnormal insulin-mediated glucose control (e.g., insulin resistance, impaired fasting glucose, impaired glucose tolerance) and dyslipidemia (12). As mentioned above, insulin, glucose, and lipid metabolisms are tightly regulated by essential elements and may be impaired by exposure to toxic heavy metals. Accordingly, investigating the interplay between dietary habits, the homeostasis of trace elements, and the characteristic metabolic complications concurring with obesity is crucial to get new insights into the pathogenesis of this disorder. In this study, we aimed to explore the association between circulating trace elements and the degree of adherence to a Mediterranean diet (MD), as assessed through the Mediterranean Diet Quality Index for children and adolescents (KIDMED), in a Spanish observational cohort of children and adolescents with obesity. To this end, we applied multi-elemental analysis to plasma and erythrocyte samples with the aim of comprehensively characterizing the biodistribution of trace elements in peripheral blood. Furthermore, we also investigated the association between blood metals and other biochemical variables (e.g., glycemia, insulinemia, lipid profile) to better understand the role of diet-related micronutrient alterations in the pathogenic events behind childhood obesity.
The study design consisted of an observational cohort of children and adolescents with obesity recruited at “Hospital Universitario Puerta del Mar” (Cádiz, Spain), who underwent an oral glucose tolerance test (OGTT) under medical prescription. The inclusion criteria were children and adolescents of both sexes, aged between 6 and 14 years, presenting a body mass index (BMI) over two standard deviations above the mean of the reference population, adjusted for sex and age (13). Subjects with other known chronic systemic diseases or suffering of acute infectious processes were not eligible for the study. Using a sample size of 26 children and considering an alpha risk of 0.05, the statistical power of our comparisons was above 80%, as calculated using the GRANMO 7.12 webtool. The study was performed in accordance with the principles contained in the Declaration of Helsinki. The Ethical Committee of “Hospital Universitario Puerta del Mar” (Cádiz, Spain) approved the study protocol (Ref. PI22/01899), and all participants and/or legal guardians provided written informed consent.
From all participants, venous blood samples were obtained by venipuncture of the antecubital region using an intravenous catheter, BD Vacutainer tubes, and Advance vacuum system. All baseline blood samples were collected in the morning after overnight fasting to minimize the influence of the circadian rhythm and dietary factors. Additional blood samples were collected at the different time points along the OGTT curve (i.e., 30, 60, 90, and 120 min) to evaluate glycemia- and insulinemia-related variables. After withdrawal, blood tubes were gently inverted several times and placed horizontally on ice to prevent red cell lysis and to reduce protease activity. Then, blood samples were centrifuged at 1,500 g for 10 min at 4°C to separate the plasma. Finally, the resulting pellets were washed with cold saline solution (9 g/L NaCl, 4°C) and centrifuged at 1,500 g for 5 min at 4°C (three times) to obtain the erythrocyte fraction. The plasma and erythrocyte samples were aliquoted and stored at −80°C until analysis.
Anthropometric variables (i.e., weight, height, BMI, and waist circumference) were evaluated by pediatric endocrinologists (J.D.-R. and A.M.L.-S.). The height was measured using a fixed wall stadiometer, whereas weight was determined in a SECA 5,000 balance. Blood glucose and insulin concentrations along the OGTT curve (i.e., 0, 30, 60, 90, and 120 min), as well as the fasting lipid profile, were measured using an Alinity automatic analyzer (Abbot, Spain) located at the Clinical Analysis Laboratory of the “Hospital Universitario Puerta del Mar.” Briefly, plasma levels of glucose and insulin were determined using the hexokinase method (CV <3%) and an electrochemiluminescence microparticle immunoassay (CV <2.2%), respectively. Enzymatic colorimetric assays were applied to quantify total cholesterol (TC, CV <1.4%), high-density lipoprotein cholesterol (HDL-C, CV <2.1%), low-density lipoprotein cholesterol (LDL-C, CV <1.7%), and triglycerides (TG, CV <1.1%). The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated by applying the following formula: HOMA-IR = (Glc0 × Ins0) × 0.055/22.5, where Glc0 and Ins0 refer to the fasting plasma levels of glucose (mg/dL) and insulin (μU/mL), respectively.
The adherence to a MD of the study participants was assessed using the updated version of the Mediterranean Diet Quality Index for children and adolescents (KIDMED) (14, 15). This dietary questionnaire consists of 16 dichotomous items (i.e., yes/no), of which 12 questions denote a positive connotation with respect to the MD (e.g., consumption of fruits, vegetables, fish, pulses, pasta or rice, cereals, nuts, olive oil, cereals, dairy products) and 4 questions denote a negative connotation (e.g., consumption of fast food, baked goods, sweets, skipping breakfast). Items with a positive connotation were assigned a value of +1, and those with a negative connotation a value of −1. The total KIDMED score is obtained by summing these individual values, which allows classifying subjects into three different groups according to their degree of MD adherence: very low diet quality (≤3), improvement needed to adjust intake to Mediterranean patterns (4–7), and optimal MD (≥8). For further analyses, these categories were collapsed into low MD adherence (“improvement needed to adjust intake to Mediterranean patterns” and “very low diet quality”) or high MD adherence (“optimal MD”) (16). This dietary assessment was conducted via interview by pediatric endocrinologists (J.D.-R.).
Trace elements (i.e., vanadium, chromium, manganese, iron, cobalt, copper, zinc, arsenic, selenium, molybdenum, cadmium, and lead) were determined by diluting aliquots of 150 μL of plasma or 50 μL of the erythrocyte fraction to a final volume of 3 mL using an alkaline solution containing 2% 1-butanol (w/v), 0.05% EDTA (w/v), 0.05% Triton X-100 (w/v), and 1% NH4OH (w/v) (17). As the internal standard, rhodium was added to sample extracts to reach a final concentration of 1 μg/L. Samples were filtered through 0.45 μm pore size hydrophilic PTFE filters before analysis. Then, multi-elemental determinations were performed using an Agilent 7,900 inductively coupled plasma mass spectrometer (ICP-MS) equipped with collision/reaction cell system and with nickel sampling and skimmer cones (Agilent Technologies, Tokyo, Japan). High-purity grade helium (>99.999%) was employed as the collision gas. The ICP-MS working conditions were set as follows (18): sampling depth, 7 mm; forward power, 1,550 W; plasma gas, 15 L/min; auxiliary gas, 1 L/min; carrier gas, 1 L/min; make-up gas, 0.10 L/min; collision gas, 5 mL/min. The isotopes monitored were 51V, 52Cr, 53Cr, 55Mn, 56Fe, 57Fe, 59Co, 63Cu, 66Zn, 75As, 77Se, 78Se, 82Se, 95Mo, 98Mo, 103Rh, 111Cd, and 208Pb, using a dwell time of 0.3 s per isotope. Multi-elemental calibration curves were prepared within the concentration range 0.5–2,500 μg/L, containing 1 μg/L rhodium as the internal standard.
Data normality and skewness was first tested by inspecting normal probability plots and by performing the Kolmogorov–Smirnov test. Clinical, biochemical, and dietary variables were subjected to Mann-Whitney U test (continuous variables) and chi-square test (dichotomous variables) to compare the study groups. The pre-processing and statistical analysis of the multi-elemental data were performed using the MetaboAnalyst 5.0 web tool (https://www.metaboanalyst.ca/), as follows. First, variables with more than 20% missing values were removed, and the remaining missing values were imputed using the kNN algorithm. Then, the data were log transformed and Pareto scaled. To look for differences between the study groups, data were subjected to Mann-Whitney U test. Finally, correlation analysis was applied to look for associations between trace elements and the KIDMED scores, as well as between trace elements and other biochemical variables (i.e., glucose, insulin, lipids). P-Values below 0.05 were considered as statistically significant.
In our study population of children and adolescents with obesity, the demographic and anthropometric characteristics were similar between participants with low and high MD adherence as assessed through the KIDMED questionnaire (Table 1). Evidently, the average KIDMED scores significantly differed between the study groups (low MD adherence: 5.2, high MD adherence: 8.3), and similar results were observed for the frequency of consumption of some of the individual items conforming the questionnaire (e.g., Q2: consumption of fruits; Q9: consumption of cereals). Furthermore, it should be noted that subjects reporting higher KIDMED scores showed lower blood levels of glucose and insulin along the OGTT curve, as well as lower fasting levels of total cholesterol.
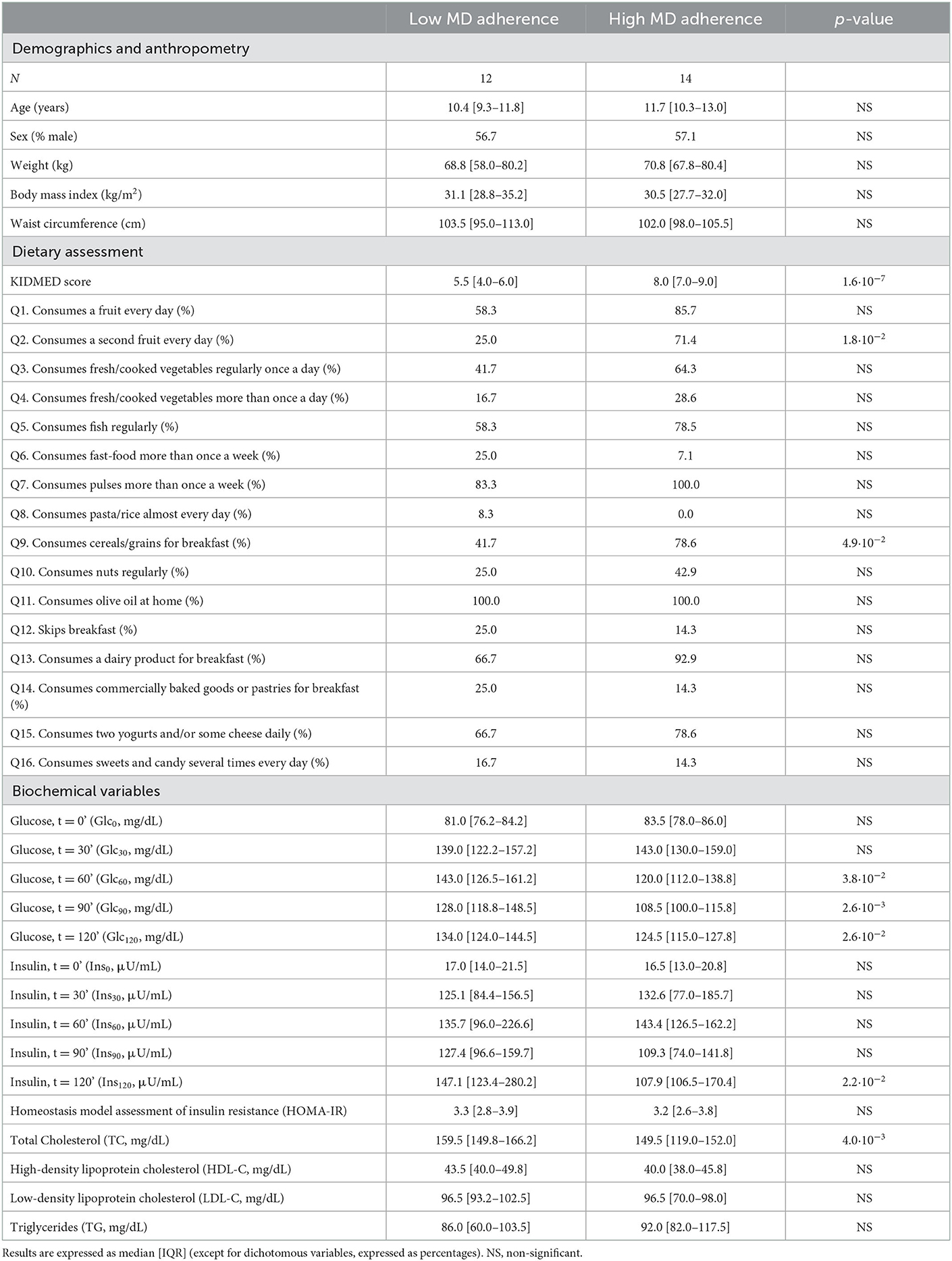
Table 1. Demographic, anthropometric, dietary, and biochemical characterization of the study population.
The degree of adherence to a MD also had a significant influence on the multi-elemental profile of plasma and erythrocyte samples of the study participants, as shown in Table 2. The plasma contents of selenium, zinc, cobalt, molybdenum, and arsenic were higher among subjects adhering to an optimal MD, and the same trend was observed for other trace elements without reaching statistical significance (e.g., chromium, manganese, iron). Similarly, increased erythroid selenium was observed in children and adolescents from the high MD adherence group, but no significant differences were found for the rest of elements under investigation. These findings were further corroborated in a large extent through correlation analyses. The KIDMED index was found to be positively associated with plasma levels of selenium (r = 0.58), zinc (r = 0.57), molybdenum (r = 0.40), and arsenic (r = 0.39) (Figure 1A). Furthermore, circulating trace elements were also correlated with the frequency of consumption of some of the individual items conforming the KIDMED questionnaire (Supplementary Figure 1). A consistent negative association was observed between unhealthy dietary habits (e.g., consumption of fast food, baked goods, sweets) and the plasma contents of zinc and/or molybdenum. On the other hand, the intake of food products with a healthy connotation with respect to the MD was positively associated with a myriad of plasmatic micronutrients: the consumption of a second fruit with molybdenum and iron, fish with selenium and arsenic, pulses with molybdenum, and dairy products with copper. Conversely, correlation analysis between dietary intake data and erythroid mineral profiles yielded less robust results, with only a few individual food items being significantly associated with copper (e.g., consumption of a second vegetable, cereals) and zinc (e.g., consumption of pasta/rice) levels (Supplementary Figure 2).
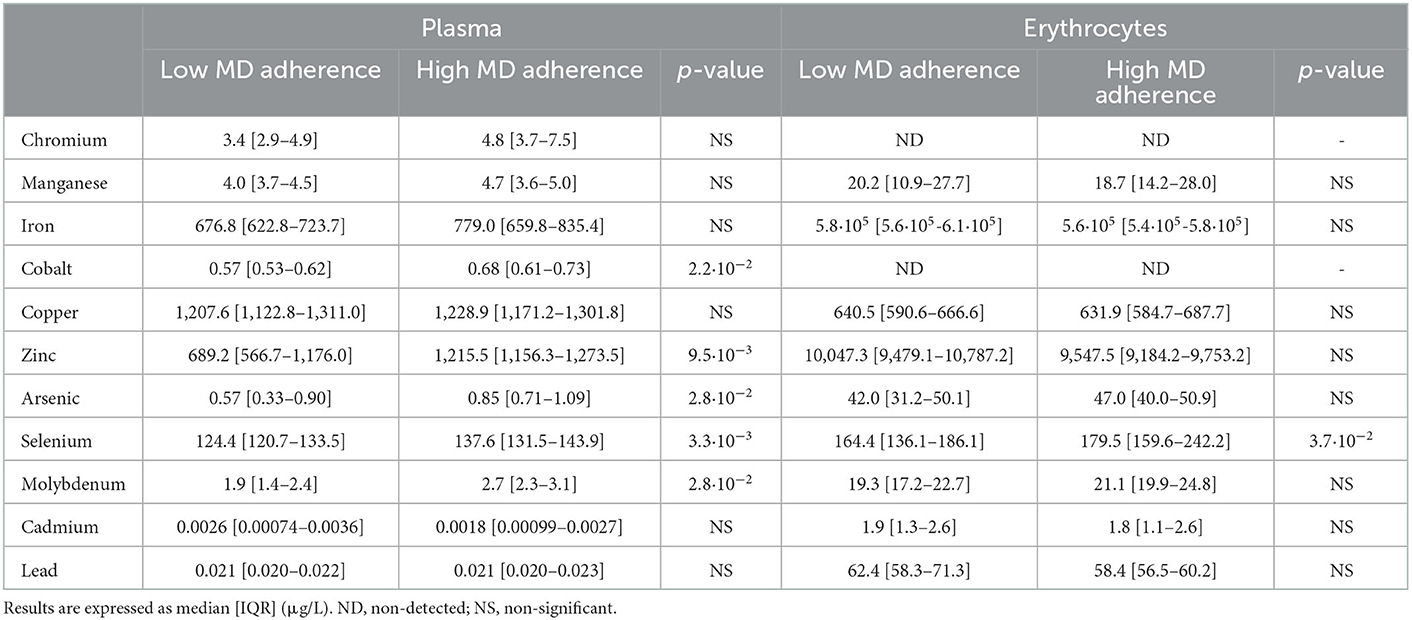
Table 2. Plasma and erythroid concentrations of trace elements in the two study groups.
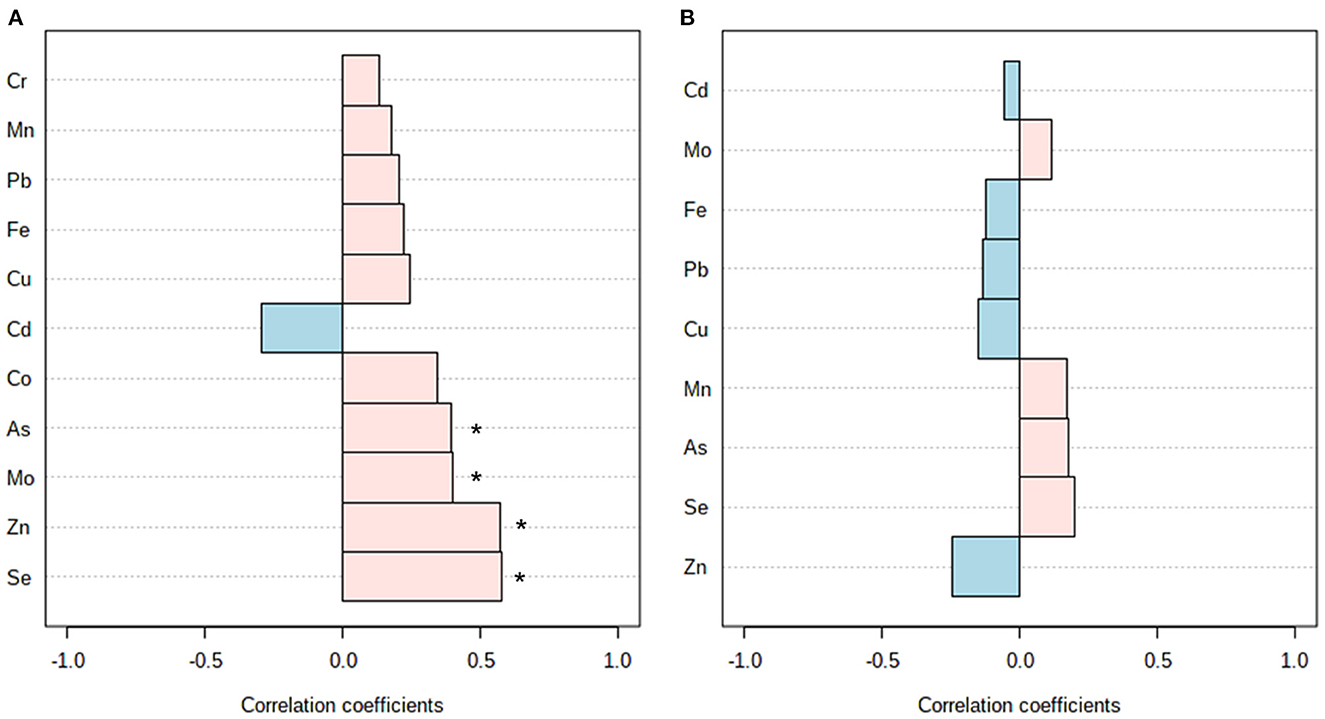
Figure 1. Correlation analysis between the KIDMED score and multi-elemental data from plasma (A) and erythrocytes (B). *Denotes significant correlation (p < 0.05).
Finally, Pearson's correlations were computed between multi-elemental and biochemical variables with the aim of investigating the relationship between diet-related micronutrient alterations and the typical metabolic complications behind childhood obesity (Figure 2). Glucose and insulin concentrations along the OGTT, as well as the HOMA-IR scores, showed a consistent negative association with selenium (r = −0.36 with Glc0, r = −0.43 with Glc60, r = −0.45 with Glc120, r = −0.50 with Ins0, r = −0.54 with HOMA-IR) and a positive association with cadmium (r = 0.35 with Glc60, r = 0.35 with Glc90, r = 0.38 with Glc120) in plasma. The same trend of association was observed for erythroid selenium (r = −0.37 with Glc30, r = −0.38 with Glc90) and cadmium (r = 0.37 with Ins0, r = 0.37 with HOMA-IR). Similarly, erythroid levels of manganese were negatively correlated to the HOMA-IR score (r = −0.48). Regarding lipid parameters, various plasmatic trace elements, including iron, cobalt, chromium, arsenic, and lead, were negatively associated with LDL-C (r = −0.38 with Fe, r = −0.63 with Co, r = −0.51 with As, r = −0.54 with Pb) and/or TC (r = −0.34 with Fe, r = −0.53 with Co, r = −0.40 with Cr, r = −0.53 with As, r = −0.38 with Pb) levels. Conversely, a positive association was found between TGs and plasma iron (r = 0.48), zinc (r = 0.38), and lead (r = 0.42).
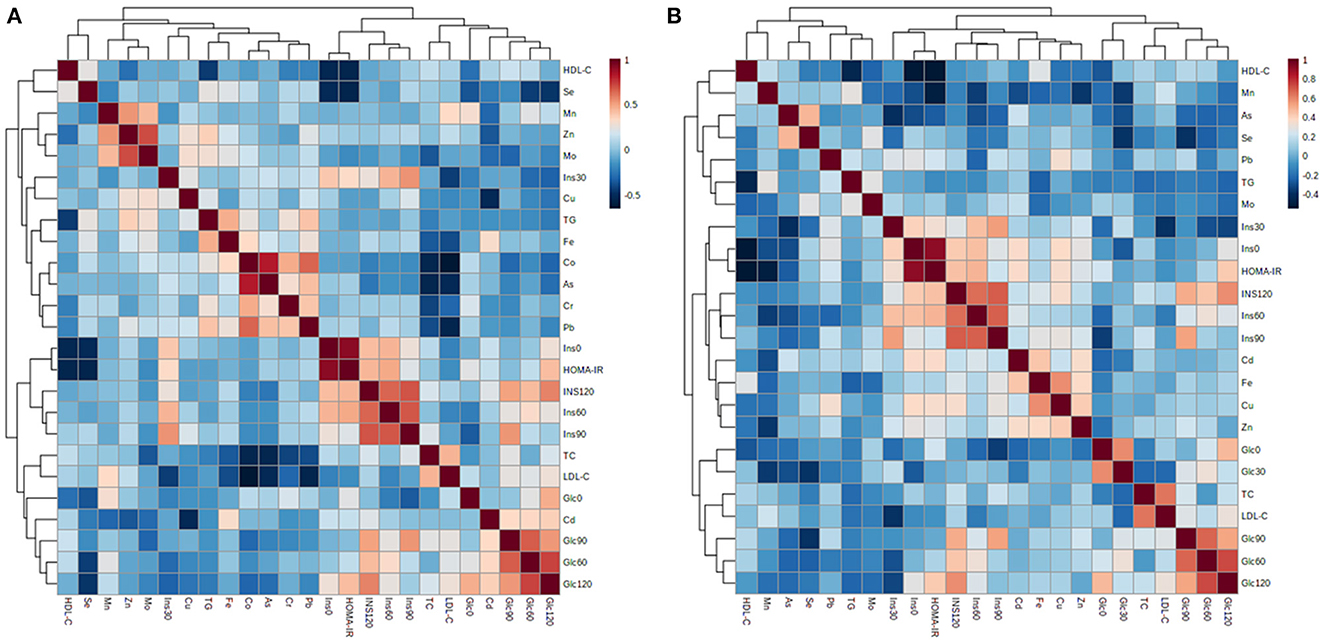
Figure 2. Pearson's correlation matrix between biochemical variables and multi-elemental data from plasma (A) and erythrocytes (B).
Dietary assessment through self-reporting methods (e.g., food frequency questionnaires, dietary recalls) has repeatedly evidenced a positive association between the adherence to a MD, micronutrient intake, and nutritional adequacy in young (19, 20), adult (21), and older populations (22). However, the measurement of dietary biomarkers in biological matrices has emerged in recent years as a more reliable strategy to get a closer and more objective understanding of the crosstalk between diet and health within the complex meshwork of bioavailability, metabolism, biodistribution, and excretion processes. In this respect, some observational studies have previously reported that subjects adhering to a MD usually have increased blood levels of multiple micronutrients, including vitamins (23), lipid-soluble compounds (e.g., carotenoids, tocopherols) (24), n-3 polyunsaturated fatty acids (25), and other essential food bioactives. To get a more comprehensive exploration about the influence of nutrition on human health, other authors have proposed the application of wide-coverage metabolomics approaches for identifying food intake biomarkers and biomarkers of adherence to specific dietary patterns (26, 27). Nevertheless, the number of studies relying on the determination of trace elements are still scarce (28), and normally focused on investigating single food items rather than complex dietary patterns (10, 11, 29).
In the present study, we have demonstrated for the first time that circulating blood trace elements can reflect the degree of MD adherence, as assessed through the KIDMED index, among children and adolescents with obesity. Herein, we found that subjects reporting higher KIDMED scores showed increased selenium, zinc, cobalt, molybdenum, and arsenic in plasma, as well as increased erythroid levels of selenium (Table 2). These findings could be explained by the rich content of minerals present in the major food products that conform the traditional MD, including vegetables, fruits, cereals, and fish (30). Indeed, nutritional interventions with heathy dietary habits (e.g., MD) have proven to significantly raise the serum concentrations of various essential minerals (31). Further correlation analyses corroborated our results (Figure 1) and shed more light on the specific food items that could contribute the most to the characteristic multi-elemental profiles observed among participants with optimal MD adherence (Supplementary Figures 1, 2). Circulating contents of essential trace elements (e.g., selenium, iron, molybdenum, copper) were positively correlated with the frequency of consumption of healthy food products, such as fruits, vegetables, fish, pulses, and dairy products, in line with previous data (29, 32). Conversely, plasma levels of zinc and molybdenum were negatively associated with unhealthy dietary habits, such as the intake of fast foods, baked goods, and sweets. Therefore, we hypothesize that metal differences between the study groups could be regarded as a direct reflection of the MD adherence, since participants consuming heathy diets are expected to have higher circulating levels of minerals than subjects who replace healthy food items with micronutrient-poor ones. Altogether, these results highlight the crucial role that diet may play on maintaining an adequate micronutrient status. Nevertheless, it is worth mentioning here that levels of metal elements may be influenced by many exogenous (e.g., diet, pollution, smoking, medications) and endogenous factors (e.g., sex, age, hormonal factors) (33), which considerably limits their reliability as sensitive and specific dietary biomarkers.
To conclude, it should also be noted that participants with the higher MD adherence showed better glycemic and insulinemic control (i.e., lower blood levels of glucose and insulin along the OGTT curve) and a healthier lipid profile (i.e., lower fasting TC levels) compared to those reporting lower KIDMED scores. For this reason, we decided to explore possible associations between the MD-related mineral profile and the pathogenic hallmarks behind childhood obesity, namely abnormal insulin-mediated carbohydrate metabolism and dyslipidemia (Figure 2). On the one hand, we found a strong negative association between selenium and manganese levels (this latter only in erythrocytes) and different variables related to hyperglycemia and hyperinsulinemia. In this respect, other authors have previously reported reduced activity of selenium- and manganese-dependent antioxidant enzymes, such as glutathione peroxidase (34, 35) and manganese superoxide dismutase (36), in children with obesity. This exacerbated oxidative stress may in turn perturb insulin secretion in pancreatic β cells (5), which could explain the direction of association between the above-mentioned trace elements and glycemia/insulinemia-related variables. Conversely, the association was positive with plasma and erythroid contents of cadmium, plausibly because of its capacity to disrupt the endocrine system, provoke insulin resistance, and consequently increase the circulating concentrations of insulin and glucose (9). In line with previous studies describing the involvement of trace elements and heavy metals in the development of dyslipidemia factors, we found a negative correlation between various blood cholesterol fractions (e.g., TC, LDL-C) and plasmatic minerals (e.g., iron, cobalt, chromium, arsenic, lead). This could be attributed to the essential roles that trace elements seem to play in ameliorating atherogenic dyslipidemia through a myriad of mechanisms (e.g., lipid β-oxidation, expression of peroxisome proliferator-activated receptors), and particularly by interfering with cholesterol metabolism (37–39). Surprisingly, a positive association was found between plasma TG, iron, zinc, and lead, which could be due to their dietary co-occurrence (e.g., animal-based products).
Herein, we have demonstrated that the degree of MD adherence, as assessed through the KIDMED score, has a significant impact on the biochemical profile and trace element status among children and adolescents with obesity. Subjects adhering to an optimal MD showed better glycemic/insulinemic control and a healthier lipid profile, as well as increased metal contents in plasma (selenium, zinc, cobalt, molybdenum, arsenic) and erythrocytes (selenium). Further correlation analyses evidenced close interrelationships between these diet-related mineral alterations and the typical metabolic complications behind childhood obesity (i.e., abnormal insulin-mediated carbohydrate metabolism, dyslipidemia), thereby highlighting the crucial role that diet might play on health through maintaining an adequate micronutrient status.
The main limitation of the present study was the relatively small sample size of the population under investigation and the lack of an independent cohort for validation purposes. Although this pilot exploration lays the foundation for better understanding the interplay between dietary habits, homeostasis of trace elements, and obesity-related pathogenic events, future studies are needed in larger cohorts to further validate our findings. In this respect, the analysis of other complementary biological matrices could be of great interest to investigate short-term (e.g., urine) and long-term (e.g., hair, nails) exposure.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethical Committee of “Hospital Universitario Puerta del Mar” (Cádiz, Spain). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
RG-D: conceptualization, project administration, and supervision. ÁG-D and RG-D: data curation and roles/writing–original draft. ÁG-D, MM-M, and RG-D: formal analysis. RG-D and AL-S: funding acquisition and resources. ÁG-D, MM-M, JD-R, AL-S, and RG-D: investigation and writing–review and editing. MM-M and RG-D: methodology. All authors have read and agreed to the published version of the manuscript.
This research was partially funded by the Spanish Government through Instituto de Salud Carlos III- (PI22/01899). ÁG-D was supported by an intramural grant from the Biomedical Research and Innovation Institute of Cádiz (LII19/16IN-CO24), and RG-D was recipient of a “Miguel Servet” fellowship (CP21/00120) funded by Instituto de Salud Carlos III.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1016819/full#supplementary-material
1. Lin X, Li H. Obesity: epidemiology, pathophysiology, and therapeutics. Front Endocrinol. (2021) 12:706978. doi: 10.3389/fendo.2021.706978
2. Speakman JR. The roles of different macronutrients in regulation of appetite, energy intake and adiposity. Curr Opin Endocr Metab Res. (2022) 22:100297. doi: 10.1016/j.coemr.2021.100297
3. Lapik IA, Galchenko AV, Gapparova KM. Micronutrient status in obese patients: a narrative review. Obes Med. (2020) 18:100224. doi: 10.1016/j.obmed.2020.100224
4. González-Domínguez Á, Millán-Martínez M, Domínguez-Riscart J, Mateos RM, Lechuga-Sancho AM, González-Domínguez R. Altered metal homeostasis associates with inflammation, oxidative stress, impaired glucose metabolism, and dyslipidemia in the crosstalk between childhood obesity and insulin resistance. Antioxidants. (2022) 11:2439. doi: 10.3390/antiox11122439
5. Barra NG, Anhê FF, Cavallari JF, Singh AM, Chan DY, Schertzer JD. Micronutrients impact the gut microbiota and blood glucose. J Endocrinol. (2021) 250:R1–R21. doi: 10.1530/JOE-21-0081
6. González-Domínguez Á, Visiedo-García FM, Domínguez-Riscart J, González-Domínguez R, Mateos RM, Lechuga-Sancho AM. Iron metabolism in obesity and metabolic syndrome. Int J Mol Sci. (2020) 21:5529. doi: 10.3390/ijms21155529
7. Köhrle J. Selenium in endocrinology-selenoprotein-related diseases, population studies, and epidemiological evidence. Endocrinology. (2021) 162:bqaa228. doi: 10.1210/endocr/bqaa228
8. Elmadfa I, Meyer AL. The role of the status of selected micronutrients in shaping the immune function. Endocr Metab Immune Disord Drug Targets. (2019) 19:1100–15. doi: 10.2174/1871530319666190529101816
9. González-Villalva A, Colín-Barenque L, Bizarro-Nevares P, Rojas-Lemus M, Rodríguez-Lara V, García-Pelaez I, et al. Pollution by metals: is there a relationship in glycemic control? Environ Toxicol Pharmacol. (2016) 46:337–43. doi: 10.1016/j.etap.2016.06.023
10. Garí M, Grimalt JO, Torrent M, Sunyer J. Influence of socio-demographic and diet determinants on the levels of mercury in preschool children from a Mediterranean island. Environ Pollut. (2013) 182:291–8. doi: 10.1016/j.envpol.2013.07.022
11. Jain RB. Contribution of diet and other factors for urinary concentrations of total arsenic and arsenic species: data for US children, adolescents, and adults. Environ Sci Pollut Res Int. (2021) 28:50094–116. doi: 10.1007/s11356-021-14230-9
12. De Spiegeleer M, De Paepe E, Van Meulebroek L, Gies I, De Schepper J, Vanhaecke L. Paediatric obesity: a systematic review and pathway mapping of metabolic alterations underlying early disease processes. Mol Med. (2021) 27:145. doi: 10.1186/s10020-021-00394-0
13. Hernández M, Castellet J, Narvaiza JL, Rincón JM, Ruiz I, Sánchez E, et al. Curvas y tablas de crecimiento. Instituto de Investigación sobre Crecimiento y Desarrollo, Fundación Faustino Orbegozo. Madrid: Editorial Garsi (2018).
14. Serra-Majem L, Ribas L, Ngo J, Ortega RM, García A, Pérez-Rodrigo C, et al. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. (2004) 7:931–5. doi: 10.1079/PHN2004556
15. Altavilla C, Caballero-Pérez P. An update of the KIDMED questionnaire, a Mediterranean diet quality index in children and adolescents. Public Health Nutr. (2019) 22:2543–7. doi: 10.1017/S1368980019001058
16. Dominguez-Riscart J, Buero-Fernandez N, Garcia-Zarzuela A, Morales-Perez C, Garcia-Ojanguren A, Lechuga-Sancho AM. Adherence to Mediterranean diet is associated with better glycemic control in children with type 1 diabetes: a cross-sectional study. Front Nutr. (2022) 9:813989. doi: 10.3389/fnut.2022.813989
17. Lu Y, Kippler M, Harari F, Grander M, Palm B, Nordqvist H, et al. Alkali dilution of blood samples for high throughput ICP-MS analysis-comparison with acid digestion. Clin Biochem. (2015) 48:140–7. doi: 10.1016/j.clinbiochem.2014.12.003
18. González-Domínguez Á, Millán-Martínez M, Sánchez-Rodas D, Lechuga-Sancho AM, González-Domínguez R. Characterization of the plasmatic and erythroid multielemental biodistribution in childhood obesity using a high-throughput method for size fractionation of metal species. In:González-Domínguez R, , editor. Mass Spectrometry for Metabolomics. Methods in Molecular Biology. New York, NY: Humana (2023) 2571. doi: 10.1007/978-1-0716-2699-3_12
19. Peng W, Berry EM, Goldsmith R. Adherence to the Mediterranean diet was positively associated with micronutrient adequacy and negatively associated with dietary energy density among adolescents. J Hum Nutr Diet. (2019) 32:41–52. doi: 10.1111/jhn.12602
20. Serra-Majem L, Ribas L, Garcia A, Pérez-Rodrigo C, Aranceta J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur J Clin Nutr. (2003) 57:S35–9. doi: 10.1038/sj.ejcn.1601812
21. Serra-Majem L, Bes-Rastrollo M, Roman-Vinas B, Pfrimer K, Sánchez-Villegas A, Martínez-González MA. Dietary patterns and nutritional adequacy in a Mediterranean country. Br J Nutr. (2009) 101:S21–8. doi: 10.1017/S0007114509990559
22. Feart C, Alles B, Merle B, Samieri C, Barberger-Gateau P. Adherence to a Mediterranean diet and energy, macro-, and micronutrient intakes in older persons. J Physiol Biochem. (2012) 68:691–700. doi: 10.1007/s13105-012-0190-y
23. Aparicio-Ugarriza R, Cuenca-García M, Gonzalez-Gross M, Julián C, Bel-Serrat S, Moreno LA, et al. Relative validation of the adapted Mediterranean Diet Score for Adolescents by comparison with nutritional biomarkers and nutrient and food intakes: the healthy lifestyle in Europe by nutrition in adolescence (HELENA) study. Public Health Nutr. (2019) 22:2381–97. doi: 10.1017/S1368980019001022
24. Aumueller N, Boushey CJ, Franke AA, Cooney RV, Monroe KR, Haiman CA, et al. Diet quality measured by four a priori-defined diet quality indices is associated with lipid-soluble micronutrients in the Multiethnic Cohort Study (MEC). Eur J Clin Nutr. (2019) 73:703–13. doi: 10.1038/s41430-018-0272-1
25. Féart C, Torrès MJM, Samieri C, Jutand MA, Peuchant E, Simopoulos AP, et al. Adherence to a Mediterranean diet and plasma fatty acids: data from the Bordeaux sample of the three-city study. Br J Nutr. (2011) 106:149–58. doi: 10.1017/S0007114510005805
26. Playdon MC, Moore SC, Derkach A, Reedy J, Subar AF, Sampson JN, et al. Identifying biomarkers of dietary patterns by using metabolomics. Am J Clin Nutr. (2017) 105:450–65. doi: 10.3945/ajcn.116.144501
27. Castellano-Escuder P, González-Domínguez R, Vaillant MF, Casas-Agustench P, Hidalgo-Liberona N, Estanyol-Torres N, et al. Assessing adherence to healthy dietary habits through the urinary food metabolome: results from a European two-center study. Front Nutr. (2022) 9:880770. doi: 10.3389/fnut.2022.880770
28. Sánchez C, Fente C, Barreiro R, López-Racamonde O, Cepeda A, Regal P. Association between breast milk mineral content and maternal adherence to healthy dietary patterns in Spain: a transversal study. Foods. (2020) 9:659. doi: 10.3390/foods9050659
29. Sánchez C, López-Jurado M, Aranda P, Llopis J. Plasma levels of copper, manganese and selenium in an adult population in southern Spain: influence of age, obesity and lifestyle factors. Sci Total Environ. (2010) 408:1014–20. doi: 10.1016/j.scitotenv.2009.11.041
30. Mesías M, Seiquer I, Navarro P. Chapter 18 - the Mediterranean diet and mineral composition. In: The Mediterranean Diet An Evidence-Based Approach. (2015), p. 185-198.
31. Paz-Tal O, Canfi A, Marko R, Katorza E, Karpas Z, Schwarzfuchs D, et al. Dynamics of magnesium, copper, selenium and zinc serum concentrations for 2-year dietary intervention. e-SPEN J. (2013) 8:e100–7. doi: 10.1016/j.clnme.2013.04.001
32. Lombardi-Boccia G, Aguzzi A, Cappelloni M, Di Lullo G, Lucarini M. Total-diet study: dietary intakes of macro elements and trace elements in Italy. Br J Nutr. (2003) 90:1117–21. doi: 10.1079/BJN2003997
33. Grandjean P, Nielsen GD, Jørgensen PJ, Hørder M. Reference intervals for trace elements in blood: significance of risk factors. Scand J Clin Lab Invest. (1992) 52:321–37. doi: 10.1080/00365519209088366
34. González-Domínguez Á, Visiedo F, Domínguez-Riscart J, Ruiz-Mateos B, Saez-Benito A, Lechuga-Sancho AM, et al. Blunted reducing power generation in erythrocytes contributes to oxidative stress in prepubertal obese children with insulin resistance. Antioxidants. (2021) 10:244. doi: 10.3390/antiox10020244
35. Fontenelle LC, Cardoso de Araújo DS, da Cunha Soares T, Clímaco Cruz KJ, Henriques GS, Marreiro DDN. Nutritional status of selenium in overweight and obesity: A systematic review and meta-analysis. Clin Nutr. (2022) 41:862–84. doi: 10.1016/j.clnu.2022.02.007
36. Mohseni R, Sadeghabadi ZA, Goodarzi MT, Teimouri M, Nourbakhsh M, Azar MR. Evaluation of Mn-superoxide dismutase and catalase gene expression in childhood obesity: its association with insulin resistance. J Pediatr Endocrinol Metab. (2018) 31:727–32. doi: 10.1515/jpem-2017-0322
37. Genchi G, Lauria G, Catalano A, Carocci A, Sinicropi MS. The double face of metals: the intriguing case of chromium. Appl Sci. (2021) 11:638. doi: 10.3390/app11020638
38. Kawakami T, Hanao N, Nishiyama K, Kadota Y, Inoue M, Sato M, et al. Differential effects of cobalt and mercury on lipid metabolism in the white adipose tissue of high-fat diet-induced obesity mice. Toxicol Appl Pharmacol. (2012) 258:32–42. doi: 10.1016/j.taap.2011.10.004
Keywords: childhood obesity, trace elements, Mediterranean diet, KIDMED, multi-elemental analysis
Citation: González-Domínguez Á, Domínguez-Riscart J, Millán-Martínez M, Lechuga-Sancho AM and González-Domínguez R (2023) Exploring the association between circulating trace elements, metabolic risk factors, and the adherence to a Mediterranean diet among children and adolescents with obesity. Front. Public Health 10:1016819. doi: 10.3389/fpubh.2022.1016819
Received: 11 August 2022; Accepted: 27 December 2022;
Published: 13 January 2023.
Edited by:
Dong-Xing Guan, Zhejiang University, ChinaReviewed by:
Andrea Paola Rojas Gil, University of Peloponnese, GreeceCopyright © 2023 González-Domínguez, Domínguez-Riscart, Millán-Martínez, Lechuga-Sancho and González-Domínguez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raúl González-Domínguez,  cmF1bC5nb256YWxlekBpbmliaWNhLmVz
cmF1bC5nb256YWxlekBpbmliaWNhLmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.