 Naohisa Shobako
Naohisa Shobako- Division of Food Science and Biotechnology, Graduate School of Agriculture, Kyoto University, Uji, Japan
It is everyone's desire to seek the sound growth of children through food education and there is a critical need for fostering an environment for this purpose. Health policies are important for this support. To the present, the Japanese society has been greatly disrupted by COVID-19 pandemic. “Stay at home”, “mokusyoku (silent eating)”, and mask wearing were encouraged in nationwide campaigns as public health measures to combat COVID-19. There are some papers reporting negative effects of “stay at home” and lockdowns such as weight gain, decrease in physical activities and change in eating habits. In Japan, while benefits and advantages of food education during mealtime were previously well studied, the “mokusyoku” rule may directly run counter to this food education. Moreover, there are several reports showing that nutrients might contribute to prevention of infectious diseases. Japanese children were also encouraged to wear masks all day long. The results of the clinical research, especially randomized control trials, show limited protective effect of masks. On the other hand, negative outcomes of the masks were reported in various scenes. This review focuses on these topics and arousing reconsideration for a better environment for children.
Introduction
Eating, learning, and playful behaviors are essential for healthy development of children. Societies around the world, including Japan, have been severely affected by the COVID-19 pandemic. It was well announced that Japan had controlled the infection successfully without draconian lockdowns or other harsh restrictions which unduly limit private rights of citizens.
However, the environment in which children eat, learn and play has greatly been affected by health policies in Japan. While no proven effect of school closures against spread of COVID-19 has been reported (1), a few schools are still taking temporary closure measures (2). Though most schools were opened, children were strongly encouraged to follow the “mokusyoku” rule of eating lunch silently during the lunch time (3). Although the Ministry of Education, Culture, Sports, Science and Technology (MECSST) has modified the guideline of mask wearing in schools to clarify that mask wearing is not necessary in physical education classes as long as the social distance (1–2 m) is maintained, the ministry still recommended to continue the mask wearing rule in schools (4). Typical events related to COVID-19 and children are summarized in Table 1. As shown, novel Coronavirus Response Headquarters present the basic policies for COVID-19 prevention, and each ministry announces relevant basic policies (5). MECSST presents guidelines describing the basic policy of countermeasures that the schools should take. Since most of them are only written recommendations, each municipality's board of education and school finally decide what kind of countermeasures to request for children. So, children were forced to comply with many kinds of measures. Examples of such measures are shown in Figure 1. As shown in the figure, children were forced to follow “The New Lifestyle (New Normal Lifestyle)” in the name of public health.
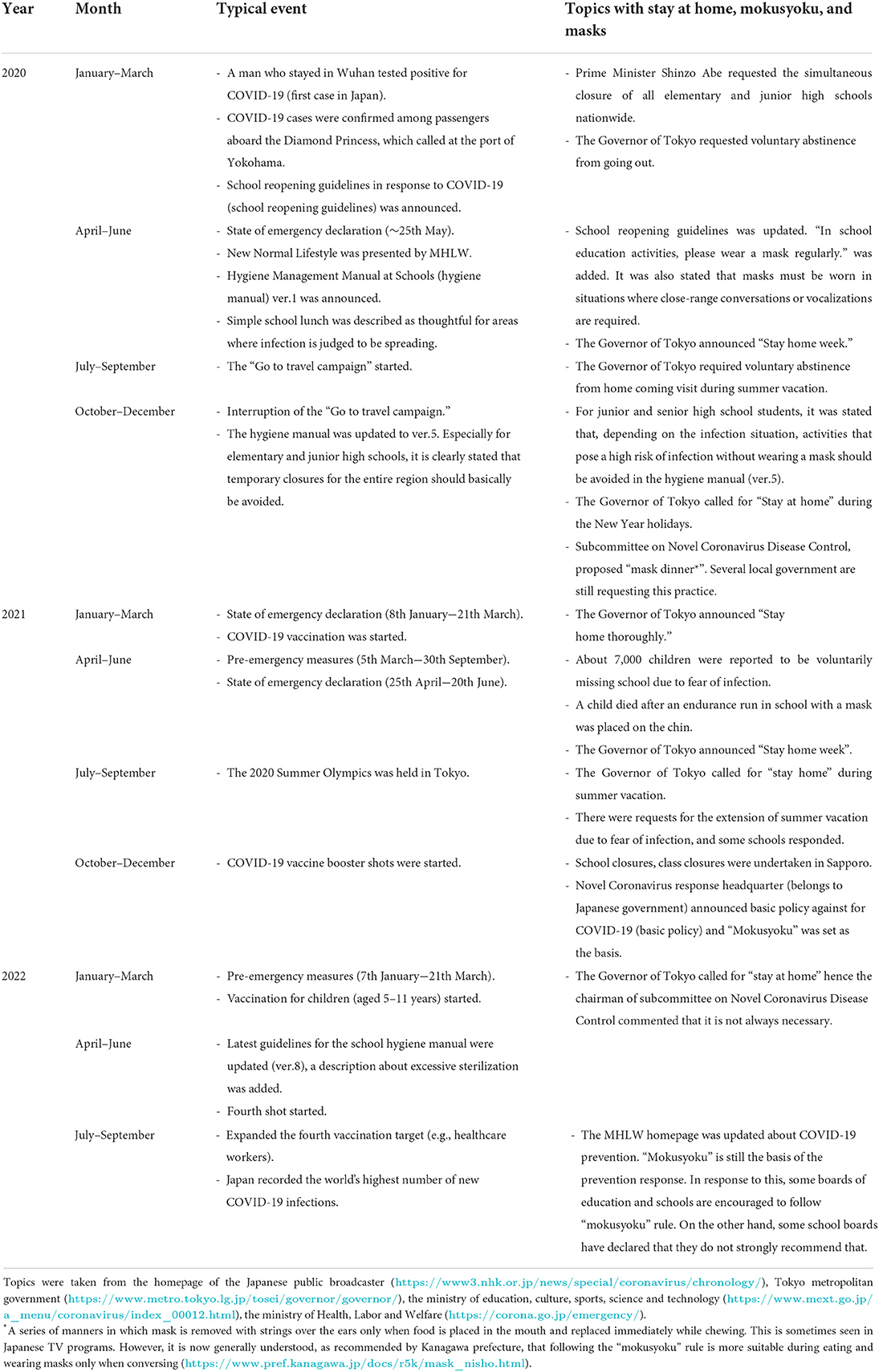
Table 1. Typical events about history of COVID-19 pandemic in Japan.
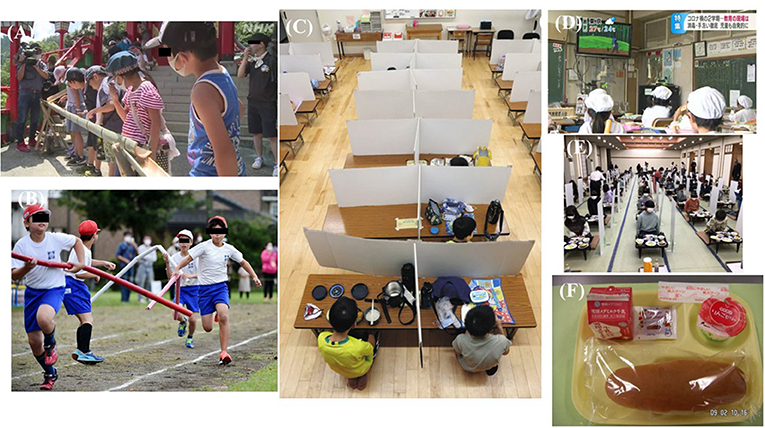
Figure 1. Example of “Infectious disease counter measures” for children taken for Japanese Children. (A) Children watching “somen (Japanese traditional noodle) flow” with their mask on in silence in summer. Under ordinary circumstances, children eat somen noodles flowing in front of them. (B) Special care is taken to keep “Physical distance” in a relay race of a school sport festival. The length of the baton was 2 meters. (C) Children are taking lunch following “mokusyoku rule”. (D) Children are watching TV program during lunch time to follow mokusyoku rurle. (E) “The New way of lifestyle” adopted in a school excursion. Children must follow “mokusyoku rule”. (F) Example of “Simple school lunch”. These pictures were taken from the following websites: (A) “Watch over them without eating. Somen flow in Tsuwano city preventing COVID-19 infection. 8/9/2020” Japan Broadcasting Corporation https://www3.nhk.or.jp/news/html/20200809/k10012560081000.html. (B) “2 meter baton, shouts on paper, broadcast on TV sports festival under COVID-19 pandemic. 9/27/2020” Mainichi Shimbun https://mainichi.jp/articles/20200927/k00/00m/040/122000c. (C) “Infection for children is increasing in COVID-19 seventh wave. What are the characteristics of the symptoms? What measures are needed for the new semester? 8/26/2022” Tokyo shimbun https://sukusuku.tokyo-np.co.jp/education/59471/. (D) “A strategy to follow mokusyoku rule by showing animated films during lunch time. In the second semester of the COVID-19 epidemic at an elementary school, the educational scene is undergoing a trial-and-error process for infection prevention measures. Nagano city. 9/1/2022” Shin-etsu broadcasting https://newsdig.tbs.co.jp/articles/sbc/140832?display=1. (E) “Dinner with mokusyoku rule and infection control measures 11/25/2021” Official Blog of Onohara east primary school http://www.kamisu.ed.jp/onoharanishi/19314.html. (F) Fuji News Network “Zero side dishes painful choice “simple school lunch” to prevent COVID-19 infection, 1.2 times the amount of hot dog buns, and concerns about nutritional deficiencies. 9/8/2021” https://www.fnn.jp/articles/-/235832. For privacy, part of the face is hidden. All sites were accessed at September 19th, 2022.
An object of this paper is to summarize the findings about the result of health policies taken in Japan and looking back the challenges of science-based policy making.
“Stay at home” campaign
Draconian lockdowns were enforced in many regions in the world such as China and Europe to prevent the wide-spread of COVID-19. “Stay at home” campaign was also strongly promoted in Japan even though Japan did not adopt any lockdown with severe restrictions. During the campaign, while adults were not subject to commuting restrictions, children were forced to stay at home due to the long-term school closures. Some negative effects of the lockdowns and “Stay at home” campaign were previously reported. In Japan, during the state of emergency, schools were closed and a “stay-at home order” was issued. As a consequence, it was reported that children had higher body fat percentage, shorter single leg standing time, and a larger number of falls per month compared with children before the pandemic (6). Abe also reported that fundamental movement skills, especially for object control skills were impeded during this pandemic (7). In low-income households, children's consumption of sweets, soft drinks, and ready-to-eat foods was increased (8). Horikawa et al. also reported children eating a balanced diet of meat or fish and vegetables at least twice a day decreased during the period (9). Horikawa's research also revealed the importance for the support of low-income households. Changes in eating habit was also observed in Kosaka's study and interfaced with feeling enervation and mental stress (10). Longer periods for video games were also reported in this study. Ueda et al. reported about half of children, participated in the research, experienced sleep pattern change during the period and its change was predicted by a high level of depression (11). In Nakachi et al. study, change tendency in sleep pattern was also observed in junior and high school students (12). Psychological problems were observed in lower grade of elementary school; they easily cried and complained, were unable to keep calm, and were dependent on parents and family members.
Similar results were reported outside Japan, where stronger behavioral restrictions have been imposed. For example, in China, significant increase in total food intake, especially snacks and drinks, and decrease in physical activities were reported (13). Negative effects of weight gain were also reported in research in U.S. (14, 15). Changes in eating habits and lifestyle during lockdowns were also reported (16, 17). Increased risk in type 2 diabetes was also reported (18). The restrictive lifestyle and weight gain due to the lockdown are considered be the causes of the increased risk in type 2 diabetes. The survey conducted on children also showed a significant increase in the consumption of potato chips, red meat, and sugary drinks, and a significant decrease in time spent in sports (19). The studies presented in this section are summarized in Table 2A.
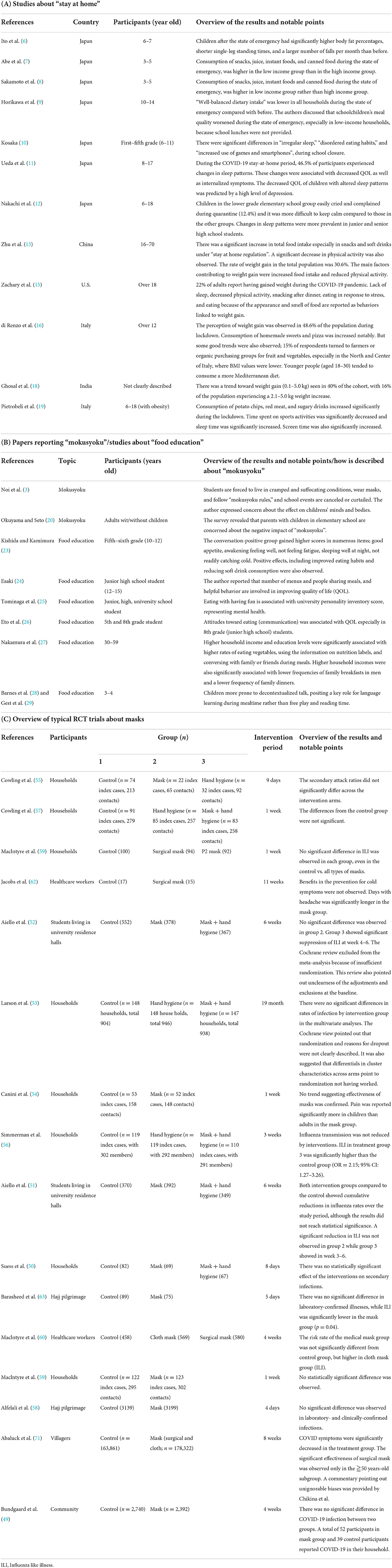
Table 2. The typical studies about stay at home (A), mokusyoku and food education (B), and RCTs about mask-wearing (C).
“Mokusyoku rule” and food education
The “Mokusyoku rule” is prohibition of conversation during meals in schools, working spaces, and restaurants (3, 20). The novel Coronavirus Response Headquarters announced “mokusyoku” as a basic policy for COVID-19 prevention (5), and the Japanese government and industry groups are promoting this health policy by spreading awareness (21). As described in Section Introduction, the final decision relies on each municipality; some local governments relaxed the “mokusyoku rule” in schools, while others continue to instruct children to follow. In order to ensure the rule implementation, each school is trying to search for the best way, such as using partition or TV animation even in 2022 (Figures 1C,D). In the early stage of the pandemic, droplet infection was thought highly threatening, and measures aimed at an assumed droplet pathogen were over-emphasized (22). The mokusyoku rule was thought to be a remnant of that time, the same as surrounding individuals with panels (Figures 1C,E). There are no reports on the benefits of the “mokusyoku rule,” and several Japanese articles have expressed worry about or negatively commented on its impact on children (20).
The importance of conversations during meals for children has been well studied in Japan. Kishida and Kamimura reported conversation positive group (group with frequent conversation) gained higher scores for good appetite, not feeling fatigue, sleeping well, and not readily catching cold (23). There are also reports of positive effects on eating habits and reducing soft drink consumption. Esaki reported frequent conversation during meals has positive relation with meal-related quality of life (QOL) (24). Previous studies also showed that Japanese children who had conversations during meals had better dietary attitudes, eating behavior and mental QOLs (25–27). Surveys outside Japan have also reported that conversations during meals in pre-kindergarten are effective for vocabulary acquisition because out-of-context conversations occur uniquely (28, 29). Although some papers suggest that people have indeed contracted COVID while eating in restaurants, such risk can be minimized by ventilation which is an important factor in preventing COVID (30, 31). As described above, conversations during meals are important for children to foster healthy minds and eating habits. Thus, it will be necessary to reconsider the “Mokusyoku rule” that would adversely affect physical and mental development and abolish the rule by taking measures such as sufficient ventilation. Articles describing mokusyoku and food education are summarized in Table 2B.
Some schools introduced “simple school lunch” with insufficient nutrition for fear of contact infection at the time of serving the meal (Figure 1F). This has been described as thoughtful for areas where the infection is judged to be spreading, as per the first version of hygiene management manual at schools to the latest version, established by MECSST (4, 32). Tanaka et al.'s survey showed simple school lunch was served in a certain number (55/205 schools for 10–40 days) of schools (33). The relationship between nutrients and infectious disease has been well studied (34). Vitamin D (VD) is probably the most well studied nutrient which has been reported to have a protective effect against COVID-19 infection (35). It is reported that serum 25-hydroxyvitamin D [25(OH)D] of <20 ng/mL is one of the risk factors of deficiency and according to a survey in South Korea, serum 25-hydroxyvitamin D [25(OH)D] of about the half of the 6–12 years old children was 20 ng/mL or less (36, 37). Not only from the diet, but also exposure to sunlight is important for vitamin D synthesis. During the pandemic, children's serum 25(OD)D concentration was significantly decreased. It was discussed that school closures and lockdowns were associated with this decrease (38). In the Turkey observational study for children under 18 years old, VD deficiency was significantly high in the COVID-19 patient group compared with the control group (39). Vitamin C (VC) and omega-3 fatty acids were also considered to prevent or reduce COVID-19 infection by cytokine modulation such as IL6, TNFα, and IL1β reduction and IL10 upregulation (40). Although some sufficient clinical observations have been reported, there are few data supporting active intervention especially for children (41). The situation of Vitamin E, considered as a natural killer cell and a T cell activator, was similar to VC (42). For children, there are a few RCTs showing positive effects of Vitamin A for preventing respiratory infections. However, the results of meta-analyses did not support active intervention (43). Zinc is well known for its important role for the development and maintenance of immune and other cells (44). Previous studies revealed that low zinc status is a risk factor of pneumonia infection for children (45). RCT studies for children also support the importance of Zinc (46). It was also reported that low selenium status is associated with COVID infection (47). Simple school lunch might be leading to opportunity loss of taking these nutrients.
Horikawa et al. discussed that school lunches play an important role in continuing well-balanced eating habits (9). Detailed research about the nutrition of simple school lunches and their effect has not been performed, but Kojima reported that it might not provide necessary nutrients compared to regular school lunch, while there was an apparent effort in the areas where a state of emergency was declared for a long time (48).
Mask rules (mandate): Review of its effectiveness
Wearing surgical masks was strongly recommended in Japan even for children in school, on the way to and from school, and even in the house (so called “family mask” in Japanese; Yamanashi Center for Infectious Disease Control and Prevention). Randomized control trials (RCTs) with appropriate sample sizes have reported the limited effectiveness of surgical masks for infectious diseases, COVID-19 and influenza (49–63). Especially, RCT demonstrated by Simmerman et al. showed significantly opposite effect in Influenza like illness (56) and demonstrated by Jacobs showed only significantly prolonged the duration of the headache (62) (Table 2C).
Significant effectiveness of masks for COVID-19 prevention was reported in numerous observational studies (64–70) and “Bangladesh study” (71). Regarding the “Bangladesh study”, there are some points to be noted in the interpretation of the results. First, the total sample size was too large to conduct proper evaluation (N = 342,183), and subgroup analysis revealed that no significant prevalence intervention ratio was observed in the age 50 subgroup for surgical mask. Second, increase of the physical distance was observed in mask group but not in the control group. Third, monetary reward was provided for participants. Chikina et al. recently reported the re-analysis results and pointed out potential biases that cannot be ignored (72). In support of this view, based on the results of meta-analysis of RCTs, the universal mask policy especially in community settings is not strongly recommended (73–75). While many observational studies reported on the effectiveness of face mask, Davies et al. pointed out that most of them were based on self-reporting, and <0.2% of studies studied the behavior in question objectively (76). Particularly, the frequency of hand washing tends to vary greatly between the actual and self-reported values, which might be the reason for overestimating mask-wearing effectiveness. Frequency of self-report mask use was also reported to differ from actual. Thus, we should carefully consider this when determining the effectiveness of personal protective equipment by observational studies. Given the sample size and results of RCTs, it may be necessary to reconsider overestimation of mask effectiveness for scientific integrity.
Effectiveness of the mask mandate should have been reconsidered as well. The survey in Europe and Texas state revealed that the mas mandate has no effect against COVID-19 infection, hospitalization, and mortality (77, 78). In Kansas, counties with mask mandate had significantly higher case fatality rates than counties without mask mandate, with a risk ratio of 1.85 for COVID-19-related deaths. The mechanism of this adverse effect is propounded as “Foegen effect” (79). This effect was supported by in vitro examinations. In the manikin model, favorable results of viral titer or viral RNA detection were observed when the receiver was not wearing a mask (80). It will be necessary to consider what happens if the simulation is continued for more than 20 min, extended from the experimented time. This paper also points out an important issue. The droplets captured by the mask might be transformed into aerosols and were floated in a chamber. Penetration and secondary atomization of droplets impacted on the surgical masks were also well studied (81, 82). People wear masks for a long period of time and, it is considered that, due to the deposition of respiratory droplets released through multiple respiratory events, mask matrix becomes wet and secondary atomization of the droplets was promoted to produce aerosol. Contamination of the mask due to wearing for the prolonged period should also be considered. Park reported the result of culturing bacteria and fungi from outer and inner layers of the masks wore by 109 Japanese people, and it was found that the mean colony counts were 13.4-times higher on the face-side of masks (83). To sum up, the effectiveness of masks, especially universal masking, seems to be limited based on the evidence described above. Regarding this point, the effectiveness of mask rules in schools has not been proven as well. For example, upon comparison of two cities, it was found that recommendation of face mask use in schools for pupils aged 10–12 didn't lower the number of COVID-19 infections (84). Similar results were also reported in school settings in various countries such as Norway (85), U.K (86), and Spain (87).
Mask rules (mandate): Review of side effects
Further, we should more deeply consider side effects of universal masking for children. Watanabe previously alerted mask addiction (88). Although wearing of masks makes it more difficult to read emotions and provides a temporary sense of security, the continued wearing of masks may diminish this sense of security, leading to a risk of worsening social anxiety.
Not only mental but also physical side effects of masks were well studied. Prolonged mask use is reported to cause headache and impaired cognition (89). Koseoglu et al. also reported increases in dyspnea, itching, ear pain, and headache induction (90). Ou et al. reported negative impact on the ventilation function of exercise with mask on in young healthy subjects (91). It is also important point that the weight of the surgical mask increased during the exercise (92). This means that masks were wet by evaporation of sweat. As described in the previous section, we should consider the accumulation of contaminated droplets for long periods and their release as aerosols. Children's modified Borgi score, an indicator of breath shortness, was significantly increased by the simple exercise with surgical mask compared to not wearing a mask (93).
Difficultly in recognition of emotion is also an important issue when considering universal masking for children. Ruba and Pollak reported aged 7–13 children have significant difficultly in reading emotion (94). In particular, mask inhibited accurate reading of fear emotion <25% (median value). Gori et al. also reported that masks inhibited reading of emotion of toddlers and children (95). Studies reported by Grahlow et al. was like this, and face masks inhibited all kinds of emotion from the face (96). When does emotional development reach adult levels? There are several scientific reports on this issue. Cohen et al. showed that cognitive abilities in emotional situations may be developing even in teenagers and young adults (97). Research on emotional understanding and prosocial behavior have been actively conducted in Japan, and some Japanese papers have been published. For example, Toda reported a significant correlation between emotional cognition and prosocial behavior in young children (98).
Discussion
Health policies during the COVID pandemic has changed our daily life especially in children in Japan. Children were encouraged to comply with “new way of life” which requires “stay at home”, “mokusyoku”, and wearing a mask all day long. This review summarized the scientific research related to these health policies.
First, I reviewed lockdown and “Stay at home” campaign. The relationship between COVID-19 and obesity in childhood was well reviewed (99). We should have to critically reflect on this health policy has caused changes in eating and exercise habits that increased obesity. The importance of nutritional education to prevent obesity is well studied (100). Dietary intervention programs to prevent body weight gain have also been developed (101). It will be important in the future to use these programs to develop health policies to prevent obesity during pandemic.
Second, I reviewed “mokusyoku rule” and food education and simple school lunch. Close contact is exactly risk factor of COVID infection (102) but for example, hand hygiene could reduce infection (103). In Japan, in-depth research has revealed the beneficial effects of food education and conversation during meals. Nutrients which are effective in preventing infectious diseases are also well studied. Health policies should be developed so that children can take enough these nutrients.
Third, I reviewed the mask rule. There was no mask obligation with penalties in Japan. However, mask wearing was strongly demanded. Over estimation of the effectiveness of mask might be impeding science-based health policy making and infection control. Psychological and physical adverse effect of prolonged mask wearing was also reviewed. As Thomson pointed out, any negative impact on mental or emotional wellbeing experienced by children who are required to wear masks may vary according to age and ability factors and which may yet be established, may be inconsistent with the WHO constitution (104). In the future, it will be necessary to proactively take less burdensome and less legally complex measures, such as adequate hand washing and ventilation.
Vaccination might have one of the key roles of the public health. The efficacy and safety of vaccination for children have been also well studied (105). However, the amount of spike protein synthesized in the body after vaccination has only been measured in adults and there is a discrepancy between the report of Ogata et al. which is in the pico-order (106), and the Cognetti and Miller in the micro-order (107). We should carefully consider the risk and benefits of vaccination and ensure that everyone's judgment is respected. In a recent survey, some parents (8.2%) answered that they intended to vaccinate their children because pediatricians might think less of them if they do not do so (108). This result might suggest that more thorough informed consent is needed. It is a matter of course that misleading media coverage focused only on the benefits or harms of vaccination should be refrained from, as such coverage only contributes to vaccine hesitancy.
As described in Section Introduction, Japan is a unique country that confronts the pandemic without measures with legal binding force, and administrative organs stayed with “recommendation” and avoided orders in most cases. It is reported that most Japanese people think “everyone should be responsible for their health” (109, 110) and should refrain from outside recreation during the pandemic (111). They wear masks (112) and wash their hands (113) voluntarily because they value peer pressure and are afraid of being left out of the community. Television broadcasts, which repeatedly report excessively about facemasks, might also play a part in the formation of the public opinion that it is acceptable to condemn not wearing a mask. Before the pandemic, immoral post for social network service (SNS) by healthcare workers were sometimes came to an issue (114). In the pandemic period, there were not a few posts on SNS by healthcare workers denigrating those who do not want to wear masks and such opinion also might have an influence. Public opinion formed by the accumulation of these factors might influence, sometimes excessively, societal pandemic measures, including in schools.
Health policy should be developed based on multifaced scientific evidence and respect for individual values. Even if the measures have no legal binding force, sometimes measures with greater disadvantages, like those reviewed in this paper, are enforced, especially for children. It is important to regularly receive feedback from schools and review measures from multiple perspectives, including not only the opinion of public health experts but also experts in nutrition science, food education, psychology, and of course, children's opinion and rights.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
NS reviewed the literature and drafted the perspective.
Acknowledgments
The author would like to thanks all journalists, scientists, lawyers, translators, and all people, who have continued to examine excessive health policies, despite criticism from the general public in Japan. Their continued activities were a great encouragement for the author to write this manuscript.
Conflict of interest
Author NS is also employed by the company Nissin Foods Holdings. The company was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fukumoto K, McClean CT, Nakagawa K. No causal effect of school closures in Japan on the spread of COVID-19 in spring 2020. Nat Med. (2021) 27:2111–9. doi: 10.1038/s41591-021-01571-8
2. Ministry of Education Culture Sports Science Technology. Results of the Survey on Temporary Closure of Public School Due to New Coronavirus Infection. Available online at: https://www.mext.go.jp/content/20220913-mxt_kouhou01-000004520_01.pdf (accessed September 17, 2022).
3. Noi S, Shikano A, Nakajima R, Shimosato S, Matsumoto R. The concern of childcare and education site about the “abnormalities in physical function” among children based on the results of ‘The questionnaire about physical function of children in 2020.' Ann Report Jpn Soc School Health Educ. (2022) 29:3–17. doi: 10.32314/educationalhealth.29.0_3
4. Ministry of Education Culture Sports Science Technology. Hygiene Management Manual at Schools (ver.8). Available online at: https://www.mext.go.jp/content/20220404-mxt_kouhou01-000004520_01.pdf (accessed September 19, 2022).
5. Novel, Coronavirus Response Headquarters. Basic Policy on Countermeasures against New Coronavirus Infections. Available online at: https://www.kantei.go.jp/jp/singi/novel_coronavirus/th_siryou/kihon_r2_040908.pdf (accessed September 17, 2022).
6. Ito T, Sugiura H, Ito Y, Noritake K, Ochi N. Effect of the COVID-19 emergency on physical function among school-aged children. Int J Environ Res Public Health. (2021) 18:9620. doi: 10.3390/ijerph18189620
7. Abe T, Kitayuguchi J, Fukushima N, Kamada M, Okada S, Ueta K, et al. Fundamental movement skills in preschoolers before and during the COVID-19 pandemic in Japan: a serial cross-sectional study. Environ Health Prev Med. (2022) 27:26. doi: 10.1265/ehpm.22-00049
8. Sakamoto T, Nozue M, Okabe T, Yoshioka Y, Saito S, Takahashi T, et al. Association between household income and dietary changes in young children during the COVID-19 state of emergency in Japan from April to May 2020. J Jpn Soc Health Educ Promot. (2022) 1:14–25. doi: 10.11260/kenkokyoiku.30.14
9. Horikawa C, Murayama N, Kojima Y, Tanaka H, Morisaki N. Changes in selected food groups consumption and quality of meals in Japanese school children during the covid-19 pandemic. Nutrients. (2021) 13:2743. doi: 10.3390/nu13082743
10. Kosaka Y. Parental perception of the relationship between stress responses and the changes in lifestyle habits of elementary school students during a temporary leave of absence for COVID-19. Shinrigaku Kenkyu. (2021) 92:408–16. doi: 10.4992/jjpsy.92.20040
11. Ueda R, Okada T, Kita Y, Ozawa Y, Inoue H, Shioda M, et al. Psychological status associated with low quality of life in school-age children with neurodevelopmental disorders during COVID-19 stay-at-home period. Front Psychiatry. (2021) 12:676493. doi: 10.3389/fpsyt.2021.676493
12. Nakachi K, Kawabe K, Hosokawa R, Yoshino A, Horiuchi F, Ueno- ichi S. Differences in psychological and behavioral changes between children following school closure due to COVID-19. Psychiatry J. (2021) 2021:5567732. doi: 10.1155/2021/5567732
13. Zhu Q, Li M, Ji Y, Shi Y, Zhou J, Li Q, et al. “Stay-at-home” lifestyle effect on weight gain during the COVID-19 outbreak confinement in China. Int J Environ Res Public Health. (2021) 18:1–13. doi: 10.3390/ijerph18041813
14. Seal A, Schaffner A, Phelan S, Brunner-Gaydos H, Tseng M, Keadle S, et al. COVID-19 pandemic and stay-at-home mandates promote weight gain in US adults. Obesity. (2022) 30:240–8. doi: 10.1002/oby.23293
15. Zachary Z, Brianna F, Brianna L, Garrett P, Jade W, Alyssa D, et al. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes Res Clin Pract. (2020) 14:210–6. doi: 10.1016/j.orcp.2020.05.004
16. di Renzo L, Gualtieri P, Pivari F, Soldati L, Attinà A, Cinelli G, et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J Transl Med. (2020) 18:229. doi: 10.1186/s12967-020-02399-5
17. Sidor A, Rzymski P. Dietary choices and habits during COVID-19 lockdown: experience from Poland. Nutrients. (2020) 12:1657. doi: 10.3390/nu12061657
18. Ghosal S, Arora B, Dutta K, Ghosh A, Sinha B, Misra A. Increase in the risk of type 2 diabetes during lockdown for the COVID19 pandemic in India: a cohort analysis. Diabetes Metabolic Synd Clin Res Rev. (2020) 14:949–52. doi: 10.1016/j.dsx.2020.06.020
19. Pietrobelli A, Pecoraro L, Ferruzzi A, Heo M, Faith M, Zoller T, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity. (2020) 28:1382–5. doi: 10.1002/oby.22861
20. Okuyama J, Seto S. Physical activity and mental health of children and adolescents in prolonged COVID-19 pandemic. Stress Sci Res. (2021) 36:3–11. doi: 10.5058/stresskagakukenkyu.2021002
21. Ministry of Health Labor Welfare. Announcement for Cooperation in Preventing the Spread of Infection Disease. Available online at: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kansentaisaku.html (accessed September 17, 2022).
22. Greenhalgh T, Ozbilgin M, Tomlinson D. How COVID-19 spreads: narratives, counter narratives, and social dramas. BMJ. (2022) 378:e069940. doi: 10.1136/bmj-2022-069940
23. Kishida N, Kamimura Y. Relationship of conversation during meal and health and dietary life of school children. In the case of 5th and 6th graders in Urban District, Hiroshima. Jpn J Nutr Dietetics. (1993) 51:23–30. doi: 10.5264/eiyogakuzashi.51.23
24. Esaki Y. Predictors of meal-related quality of life. Jpn J Educ Psychol. (2017) 65:239–47. doi: 10.5926/jjep.65.239
25. Tominaga M, Kodama MK, Sato TK. Relationship between life style focusing on eating habits and mental health of junior and high school students, and university students. J Home Econ Jpn. (1997) 52:499–510.
26. Eto K, Nakanishi A, Takemi Y. Associations between family dinner frequency and voluntary mealtime communication with dietary attitudes, dietary behaviors, and quality of life: a cross-sectional and longitudinal study of 5th and 8th grade students. Jpn J Nutr Dietetics. (2014) 72:113–25. doi: 10.5264/eiyogakuzashi.72.113
27. Nakamura S, Inayama T, Hata K, Matsushita M, Takahashi M, Harada K, et al. Association of household income and education with eating behaviors in Japanese adults: a cross-sectional study. BMC Public Health. (2016) 16:1–14. doi: 10.1186/s12889-016-2748-z
28. Barnes EM, Grifenhagen JF, Dickinson DK. Mealtimes in head start pre-k classrooms: examining language-promoting opportunities in a hybrid space. J Child Lang. (2020) 47:337–57. doi: 10.1017/S0305000919000199
29. Gest SD, Holland-Coviello R, Welsh JA, Eicher-Catt DL, Gill S. Language development subcontexts in head start classrooms: Distinctive patterns of teacher talk during free play, mealtime, and book reading. Early Educ Dev. (2006) 17:293–315. doi: 10.1207/s15566935eed1702_5
30. Lu J, Gu J, Li K, Xu C, Su W, Lai Z, et al. COVID-19 outbreak associated with air conditioning in restaurant, Guangzhou, China, 2020. Emerg Infect Dis. (2020) 26:1628–31. doi: 10.3201/eid2611.203774
31. Zhang N, Chen X, Jia W, Jin T, Xiao S, Chen W, et al. Evidence for lack of transmission by close contact and surface touch in a restaurant outbreak of COVID-19. J Infect. (2021) 83:207–16. doi: 10.1016/j.jinf.2021.05.030
32. Ministry of Education Culture Sports Science Technology. Hygiene Management Manual at Schools (ver.1). Available online at: https://www.pref.shiga.lg.jp/file/attachment/5178754.pdf (accessed September 19, 2022).
33. Tanaka H, Kojima Y, Horikawa C, Murayama N, Morisaki N. A nationwide survey on school lunch provision during the COVID-19 pandemic. J Natl Inst Public Health. (2021) 70:579–86. doi: 10.20683/jniph.70.5_579
34. Iddir M, Brito A, Dingeo G, del Campo SSF, Samouda H, la Frano MR, et al. Strengthening the immune system and reducing inflammation and oxidative stress through diet and nutrition: considerations during the covid-19 crisis. Nutrients. (2020) 12:1562. doi: 10.3390/nu12061562
35. Mercola J, Grant WB, Wagner CL. Evidence regarding vitamin d and risk of covid-19 and its severity. Nutrients. (2020) 12:3361. doi: 10.3390/nu12113361
36. Roh YE, Kim BR, Choi WB, Kim YM, Cho MJ, Kim HY, et al. Vitamin D deficiency in children aged 6 to 12 years: single center's experience in busan. Ann Pediatr Endocrinol Metab. (2016) 21:149–54. doi: 10.6065/apem.2016.21.3.149
37. Tamaki J, Iki M, Sato Y, Kajita E, Nishino H, Akiba T, et al. Total 25-hydroxyvitamin D levels predict fracture risk: results from the 15-year follow-up of the Japanese Population-based Osteoporosis (JPOS) Cohort Study. Osteoporosis Int. (2017) 28:1903–13. doi: 10.1007/s00198-017-3967-6
38. Beyazgül G, Bag Ö, Yurtseven I, Coşkunol F, Başer S, Çiçek D, et al. How vitamin D levels of children changed during COVID-19 pandemic: a comparison of pre-pandemic and pandemic periods. J Clin Res Pediatr Endocrinol. (2022) 14:188–95. doi: 10.4274/jcrpe.galenos.2022.2021-10-6
39. Alpcan A, Tursun S, Kandur Y. Vitamin D levels in children with COVID-19: a report from Turkey. Epidemiol Infect. (2021) 149:e180. doi: 10.1017/S0950268821001825
40. Shakoor H, Feehan J, al Dhaheri AS, Ali HI, Platat C, Ismail LC, et al. Immune-boosting role of vitamins D, C, E, zinc, selenium and omega-3 fatty acids: could they help against COVID-19? Maturitas. (2021) 143:1–9. doi: 10.1016/j.maturitas.2020.08.003
41. Milani GP, Macchi M, Guz-Mark A. Vitamin C in the treatment of COVID-19. Nutrients. (2021) 13:1172. doi: 10.3390/nu13041172
42. Saeed H, Osama H, Abdelrahman MA, Madney YM, Harb HS, Abdelrahim MEA, et al. Vitamins and other immune-supportive elements as cofactors for passing the COVID-19 pandemic. Beni Suef Univ J Basic Appl Sci. (2021) 10:1–8. doi: 10.1186/s43088-021-00163-2
43. Chen H, Zhuo Q, Yuan W, Wang J, Wu T. Vitamin A for preventing acute lower respiratory tract infections in children up to seven years of age. Cochrane Database Syst Rev. (2008). doi: 10.1002/14651858.CD006090.pub2
44. Alexander J, Tinkov A, Strand TA, Alehagen U, Skalny A, Aaseth J. Early nutritional interventions with zinc, selenium and vitamin D for raising anti-viral resistance against progressive COVID-19. Nutrients. (2020) 12:1–12. doi: 10.3390/nu12082358
45. Saleh NY, Abo El Fotoh WMM. Low serum zinc level: the relationship with severe pneumonia and survival in critically ill children. Int J Clin Pract. (2018) 72:e13211. doi: 10.1111/ijcp.13211
46. Bhatnagar S, Aneja S, Dutta AK, Chandra J, Rath B, Sharma M, et al. Zinc as adjunct treatment in infants aged between 7 and 120 days with probable serious bacterial infection: a randomised, double-blind, placebo-controlled trial. Lancet. (2012) 379:2072–8. doi: 10.1016/S0140-6736(12)60477-2
47. Moghaddam A, Heller RA, Sun Q, Seelig J, Cherkezov A, Seibert L, et al. Selenium deficiency is associated with mortality risk from COVID-19. Nutrients. (2020) 12:1–13. doi: 10.3390/nu12072098
48. Kojima Y, Murayama N, Horikawa C, Tanaka H, Morisaki N. Impact of declaration of a state of emergency due to the COVID-19 pandemic on school lunches: a nationwide survey. Jpn J Nutr Dietetics. (2022) 80:116–25. doi: 10.5264/eiyogakuzashi.80.116
49. Bundgaard H, Bundgaard JS, Raaschou-Pedersen DET, von Buchwald C, Todsen T, Norsk JB, et al. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS-CoV-2 infection in Danish mask wearers a randomized controlled trial. Ann Intern Med. (2021) 174:335–43. doi: 10.7326/M20-6817
50. Suess T, Remschmidt C, Schink SB, Schweiger B, Nitsche A, Schroeder K, et al. The role of facemasks and hand hygiene in the prevention of influenza transmission in households: results from a cluster randomised trial; Berlin, Germany, 2009-2011. BMC Infect Dis. (2012) 12:26. doi: 10.1186/1471-2334-12-26
51. Aiello AE, Perez V, Coulborn RM, Davis BM, Uddin M, Monto AS. Facemasks, hand hygiene, and influenza among young adults: a randomized intervention trial. PLoS ONE. (2012) 7:e29744. doi: 10.1371/journal.pone.0029744
52. Aiello AE, Murray GF, Perez V, Coulborn RM, Davis BM, Uddin M, et al. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. (2010) 201:491–8. doi: 10.1086/650396
53. Larson EL, Ferng YH, Wong-McLoughlin J, Wang S, Haber M, Morse SS. Impact of non-pharmaceutical interventions on URIs and influenza in crowded, urban households. Public Health Rep. (2010) 125:178–91. doi: 10.1177/003335491012500206
54. Canini L, Andréoletti L, Ferrari P, Angelo DR, Blanchon T, Lemaitre M, et al. Surgical mask to prevent influenza transmission in households: a cluster randomized trial. PLoS ONE. (2010) 5:e13998. doi: 10.1371/journal.pone.0013998
55. Cowling BJ, Fung ROP, Cheng CKY, Fang VJ, Chan KH, Seto WH, et al. Preliminary findings of a randomized trial of non-pharmaceutical interventions to prevent influenza transmission in households. PLoS ONE. (2008) 3:e2101. doi: 10.1371/journal.pone.0002101
56. Simmerman JM, Suntarattiwong P, Levy J, Jarman RG, Kaewchana S, Gibbons R v, et al Findings from a household randomized controlled trial of hand washing and face masks to reduce influenza transmission in Bangkok, Thailand. Influenza Other Respir Viruses. (2011) 5:256–67. doi: 10.1111/j.1750-2659.2011.00205.x
57. Cowling BJ, Chan KH, Fang VJ, Cheng CKY, Fung ROP, Wai W, et al. Facemasks and hand hygiene to prevent influenza transmission in households. Ann Intern Med. (2009) 151:437–46. doi: 10.7326/0003-4819-151-7-200910060-00142
58. Alfelali M, Haworth EA, Barasheed O, Badahdah AM, Bokhary H, Tashani M, et al. Facemask against viral respiratory infections among Hajj pilgrims: a challenging cluster-randomized trial. PLoS ONE. (2020) 15:e0240287. doi: 10.1371/journal.pone.0240287
59. MacIntyre CR, Zhang Y, Chughtai AA, Seale H, Zhang D, Chu Y, et al. Cluster randomised controlled trial to examine medical mask use as source control for people with respiratory illness. BMJ Open. (2016) 6:e012330. doi: 10.1136/bmjopen-2016-012330
60. MacIntyre CR, Seale H, Dung TC, Hien NT, Nga PT, Chughtai AA, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. (2015) 5:e006577. doi: 10.1136/bmjopen-2014-006577
61. Maclntyre CR, Cauchemez S, Dwyer DE, Seale H, Cheung P, Browne G, et al. Face mask use and control of respiratory virus transmission in households. Emerg Infect Dis. (2009) 15:233–41. doi: 10.3201/eid1502.081166
62. Jacobs JL, Ohde S, Takahashi O, Tokuda Y, Omata F, Fukui T. Use of surgical face masks to reduce the incidence of the common cold among health care workers in Japan: a randomized controlled trial. Am J Infect Control. (2009) 37:417–9. doi: 10.1016/j.ajic.2008.11.002
63. Barasheed O, Heron L, Haworth E, Almasri N, Badahdah AM, Taylor J, et al. Pilot randomised controlled trial to test effectiveness of facemasks in preventing influenza-like illness transmission among Australian Hajj Pilgrims in 2011 on behalf of the Hajj Research Team. Infect Disord Drug Targets. (2014) 14:110–6. doi: 10.2174/1871526514666141021112855
64. Guo X, Wang J, Hu D, Wu L, Gu L, Wang Y, et al. Survey of COVID-19 disease among orthopaedic surgeons in Wuhan, People's Republic of China. J Bone Joint Surg Am. (2020) 102:847–54. doi: 10.2106/JBJS.20.00417
65. Kumar S, Kumar A, Kirtana J, Singh A, Shankar S, Khan M, et al. Risk factors and outcome among COVID-19 exposed and quarantined healthcare workers: a study on the status of existing practices of standard precautions. J Family Med Prim Care. (2020) 9:5355. doi: 10.4103/jfmpc.jfmpc_1579_20
66. Lio CF, Cheong HH, Lei CI, Lo IL, Yao L, Lam C, et al. Effectiveness of personal protective health behaviour against COVID-19. BMC Public Health. (2021) 21:1. doi: 10.1186/s12889-021-10680-5
67. Xu H, Gan Y, Zheng D, Wu B, Zhu X, Xu C, et al. Relationship between COVID-19 infection and risk perception, knowledge, attitude, and four nonpharmaceutical interventions during the late period of the COVID-19 epidemic in China: online cross-sectional survey of 8158 adults. J Med Internet Res. (2020) 22:e21372. doi: 10.2196/21372
68. Hendrix MJ, Walde C, Findley K, Trotman R. Absence of apparent transmission of SARS-CoV-2 from two stylists after exposure at a hair salon with a universal face covering policy – springfield, missouri, May 2020. MMWR Morb Mortal Wkly Rep. (2020) 69:930–32. doi: 10.15585/mmwr.mm6928e2
69. Doung-Ngern P, Suphanchaimat R, Panjangampatthana A, Janekrongtham C, Ruampoom D, Daochaeng N, et al. Case-control study of use of personal protective measures and risk for SARS-CoV 2 infection, Thailand. Emerg Infect Dis. (2020) 26:2607–16. doi: 10.3201/eid2611.203003
70. Khalil MdM, Alam MM, Arefin MK, Chowdhury MR, Huq MR, Chowdhury JA, et al. Role of personal protective measures in prevention of COVID-19 spread among physicians in Bangladesh: a multicenter cross-sectional comparative study. SN Compr Clin Med. (2020) 2:1733–9. doi: 10.1007/s42399-020-00471-1
71. Abaluck J, Kwong LH, Styczynski A, Haque A, Kabir MA, Bates-Jeffery E, et al. Impact of community masking on COVID-19: a cluster-randomized trial in Bangladesh. Science. (2021) 375:6577. doi: 10.1126/science.abi9069
72. Chikina M, Pegden W, Recht B. Re-analysis on the statistical sampling biases of a mask promotion trial in Bangladesh: a statistical replication. Trials. (2022) 23:786. doi: 10.1186/s13063-022-06704-z
73. Kim MS, Seong D, Li H, Chung SK, Park Y, Lee M, et al. Comparative effectiveness of N95, surgical or medical, and non-medical facemasks in protection against respiratory virus infection: a systematic review and network meta-analysis. Rev Med Virol. (2022) 32:e2336 doi: 10.1002/rmv.2336
74. Nanda A, Hung I, Kwong A, Man VCM, Roy P, Davies L, et al. Efficacy of surgical masks or cloth masks in the prevention of viral transmission: systematic review, meta-analysis, and proposal for future trial. J Evid Based Med. (2021) 14:97–111. doi: 10.1111/jebm.12424
75. Jefferson T, del Mar CB, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst Rev. (2020) 2011:CD006207. doi: 10.1002/14651858.CD006207.pub4
76. Davies R, Mowbray F, Martin AF, Smith LE, Rubin GJ. A systematic review of observational methods used to quantify personal protective behaviours among members of the public during the COVID-19 pandemic, and the concordance between observational and self-report measures in infectious disease health protection. BMC Public Health. (2022) 22:1436. doi: 10.1186/s12889-022-13819-0
77. Spira B. Correlation between mask compliance and COVID-19 outcomes in Europe. Cureus. (2022) 14:e24268. doi: 10.7759/cureus.24268
78. April MD, Naylor JF, Long B. Analysis of the effects of a texas state-wide mask mandate (Executive Order GA-29) on case load, hospitalizations, and mortality. South Med J. (2022) 115:175–80. doi: 10.14423/SMJ.0000000000001368
79. Fögen Z. The Foegen effect: a mechanism by which facemasks contribute to the COVID-19 case fatality rate. Medicine. (2022) 101:E28924. doi: 10.1097/MD.0000000000028924
80. Ueki H, Furusawa Y, Iwatsuki-Horimoto K, Imai M, Kabata H, Nishimura H, et al. Effectiveness of face masks in preventing airborne transmission of SARS-CoV-2. mSphere. (2020) 5:e00637–20. doi: 10.1128/mSphere.00637-20
81. Sharma S, Pinto R, Saha A, Chaudhuri S, Basu S. On secondary atomization and blockage of surrogate cough droplets in single-and multilayer face masks. Sci Adv. (2021) 7:eabf0452. doi: 10.1126/sciadv.abf0452
82. Bagchi S, Basu S, Chaudhuri S, Saha A. Penetration and secondary atomization of droplets impacted on wet facemasks. Phys Rev Fluids. (2021) 6:110510. doi: 10.1103/PhysRevFluids.6.110510
83. Park AM, Khadka S, Sato F, Omura S, Fujita M, Hashiwaki K, et al. Bacterial and fungal isolation from face masks under the COVID-19 pandemic. Sci Rep. (2022) 12:11361. doi: 10.1038/s41598-022-15409-x
84. Juutinen A, Sarvikivi E, Laukkanen-Nevala P, Helve O. Use of face masks did not impact COVID-19 incidence among 10–12-year-olds in Finland. medRxiv [Preprint]. (2022). doi: 10.1101/2022.04.04.22272833
85. Rotevatn TA, Larsen VB, Bjordal Johansen TK, Astrup E, Surén P, Greve-Isdahl M, et al. Transmission of SARS-CoV-2 in Norwegian schools: A population-wide register-based cohort study on characteristics of the index case and secondary attack rates. medRxiv [Preprint]. (2021). doi: 10.1101/2021.10.04.21264496
86. Marchant E, Griffiths L, Crick T, Fry R, Hollinghurst J, James M, et al. COVID-19 mitigation measures in primary schools and association with infection and school staff wellbeing: an observational survey linked with routine data in Wales, UK. PLoS ONE. (2022) 17:e0264023. doi: 10.1371/journal.pone.0264023
87. Coma E, Català M, Méndez-Boo L, Alonso S, Hermosilla E, Alvarez-Lacalle E, et al. Unravelling the role of the mandatory use of face covering masks for the control of SARS-CoV-2 in schools: A quasi-experimental study nested in a population-based cohort in Catalonia (Spain). SSRN Elec J. (2022). Available online at: https://www.ssrn.com/abstract=4046809 (accessed September 19, 2022).
88. Watanabe N. Mask addiction. Stress Sci Res. (2018) 33:15–20. doi: 10.5058/stresskagakukenkyu.2018006
89. Elisheva R. Adverse effects of prolonged mask use among healthcare professionals during COVID-19. J Infect Dis Epidemiol. (2020) 6:130. doi: 10.23937/2474-3658/1510130
90. Koseoglu S, Caklcl K, Demirtaş M, Gokdogan O, Ucuncu H. Ear nose and throat symptoms of mask-earing in the COVID era. J Laryngol Otol. (2022) 136:645–8. doi: 10.1017/S0022215122000676
91. Ou H, Zheng Y, Li M, Liang J, Chen H, Lang S, et al. The impacts of surgical mask in young healthy subjects on cardiopulmonary function and muscle performance: a randomized crossover trial. Arch Public Health. (2022) 80:1. doi: 10.1186/s13690-022-00893-4
92. Roberge RJ, Kim JH, Benson SM. Absence of consequential changes in physiological, thermal and subjective responses from wearing a surgical mask. Respir Physiol Neurobiol. (2012) 181:29–35. doi: 10.1016/j.resp.2012.01.010
93. Reychler G, Standaert M, Audag N, Caty G, Robert A, Poncin W. Effects of surgical facemasks on perceived exertion during submaximal exercise test in healthy children. Eur J Pediatr. (2022) 181:2311–7. doi: 10.1007/s00431-022-04430-x
94. Ruba AL, Pollak SD. Children's emotion inferences from masked faces: implications for social interactions during COVID-19. PLoS ONE. (2020) 15:e0243708. doi: 10.1371/journal.pone.0243708
95. Gori M, Schiatti L, Amadeo MB. Masking emotions: face masks impair how we read emotions. Front Psychol. (2021) 12:669432. doi: 10.3389/fpsyg.2021.669432
96. Grahlow M, Rupp CI, Derntl B. The impact of face masks on emotion recognition performance and perception of threat. PLoS ONE. (2022) 17:e0262840. doi: 10.1371/journal.pone.0262840
97. Cohen AO, Breiner K, Steinberg L, Bonnie RJ, Scott ES, Taylor-Thompson KA, et al. When is an adolescent an adult? Assessing cognitive control in emotional and nonemotional contexts. Psychol Sci. (2016) 27:549–62. doi: 10.1177/0956797615627625
98. Toda S. The relation between understanding of other people's emotion and prosocial behavior in preschoolers. J Hokkaido Univ Educ Kushiro. (2003) 35:95–105. Available online at: http://s-ir.sap.hokkyodai.ac.jp/dspace/handle/123456789/1291
99. Nogueira-de-Almeida CA, del Ciampo LA, Ferraz IS, del Ciampo IRL, Contini AA, da Ued FV. COVID-19 and obesity in childhood and adolescence: a clinical review. J Pediatr. (2020) 96:546–58. doi: 10.1016/j.jped.2020.07.001
100. Yu HJ, Li F, Hu YF, Li CF, Yuan S, Song Y, et al. Improving the metabolic and mental health of children with obesity: a school-based nutrition education and physical activity intervention in Wuhan, China. Nutrients. (2020) 12:194. doi: 10.3390/nu12010194
101. Nakazeko T, Shobako N, Hirano Y, Nakamura F, Honda K. Novel dietary intervention program “COMB meal program” approaching health and presenteeism: two pilot studies. J Funct Foods. (2022) 92:105050. doi: 10.1016/j.jff.2022.105050
102. Alsohime F, Temsah MH, Al-Nemri AM, Somily AM, Al-Subaie S. COVID-19 infection prevalence in pediatric population: etiology, clinical presentation, and outcome. J Infect Public Health. (2020) 13:1791–6. doi: 10.1016/j.jiph.2020.10.008
103. Lotfinejad N, Peters A, Tartari E, Fankhauser-Rodriguez C, Pires D, Pittet D. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect. Dis. (2021) 21:e209–21. doi: 10.1016/S1473-3099(21)00383-2
104. Thomson S. Mask mandates for children during the COVID-19 pandemic: an international human rights perspective. Scand J Public Health. (2022) 50:683–5. doi: 10.1177/14034948221081087
105. Olson SM, Newhams MM, Halasa NB, Price AM, Boom JA, Sahni LC, et al. Effectiveness of BNT162b2 vaccine against critical Covid-19 in adolescents. New Engl J Med. (2022) 386:713–23. doi: 10.1056/NEJMoa2117995
106. Ogata AF, Cheng CA, Desjardins M, Senussi Y, Sherman AC, Powell M, et al. Circulating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccine antigen detected in the plasma of mRNA-1273 vaccine recipients. Clin Infect Dis. (2022) 74:715–8. doi: 10.1093/cid/ciab465
107. Cognetti JS, Miller BL. Monitoring serum spike protein with disposable photonic biosensors following SARS-CoV-2 vaccination. Sensors. (2021) 21:5857. doi: 10.3390/s21175857
108. Ruiz JB, Bell RA. Parental COVID-19 vaccine hesitancy in the United States. Public Health Rep. (2022). doi: 10.1177/00333549221114346
109. Burgess A, Horii M. Risk, ritual and health responsibilisation: Japan's “safety blanket” of surgical face mask-wearing. Sociol Health Illn. (2012) 34:1184–98. doi: 10.1111/j.1467-9566.2012.01466.x
110. Nakayachi K, Ozaki T, Shibata Y, Yokoi R. Why do Japanese people use masks against COVID-19, even though masks are unlikely to offer protection from infection? Front Psychol. (2020) 11:1918. doi: 10.3389/fpsyg.2020.01918
111. Tanaka K, Inagaki T, Iwata K, Onishi M, Kanda Y, Kii M, et al. Basic survey of attitudes and behaviors under state of emergency by COVID-19 in Japan. J Jpn Soc Civil Engin. (2021) 77:129–40. doi: 10.2208/jscejipm.77.2_129
112. Yoshizawa H, Yoshizawa E. Examination of motivations for college students to wear masks in COVID-19 pandemic. J Appear Adornment Stud. (2022) 1:20–8.
113. Nakayachi K, Ozaki T, Shibata Y, Yokoi R. Determinants of hand-washing behavior during the infectious phase of COVID-19. Shinrigaku Kenkyu. (2021) 92:327–31. doi: 10.4992/jjpsy.92.20314
Keywords: food education, stay at home, masks, COVID-19, pandemic, health policy
Citation: Shobako N (2022) Lessons from the health policies for children during the pandemic in Japan. Front. Public Health 10:1015955. doi: 10.3389/fpubh.2022.1015955
Received: 10 August 2022; Accepted: 21 September 2022;
Published: 06 October 2022.
Edited by:
Pier Luigi Sacco, University of Studies G. D'Annunzio Chieti and Pescara, ItalyReviewed by:
Tatsui Otsuka, Tohoku University, JapanTetsuhiro Kidokoro, Nippon Sport Science University, Japan
Copyright © 2022 Shobako. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Naohisa Shobako, c2hvYmFrby5uYW9oaXNhLjJ4QGt5b3RvLXUuYWMuanA=