 Mohammed Noushad1*
Mohammed Noushad1* Samer Rastam2
Samer Rastam2 Mohammad Zakaria Nassani1Inas Shakeeb Al-Saqqaf3Mudassir Hussain4
Mohammad Zakaria Nassani1Inas Shakeeb Al-Saqqaf3Mudassir Hussain4 Ali Ango Yaroko5Mohammed Arshad6
Ali Ango Yaroko5Mohammed Arshad6 Abdullahi Musa Kirfi7Pradeep Koppolu1Fayez Hussain Niazi1Ali Elkandow8Mahmoud Darwish2Ahmad Salim Abdalla Nassar9Sami Osman Abuzied Mohammed10Nasser Hassan Abdalrady Hassan11Ghadah Salim Abusalim12Abdulaziz Samran1Anas B Alsalhani2Amir Mohiddin Demachkia13Renata Marques de Melo13Norhayati Luddin14Adam Husein14Adnan Habib15
Abdullahi Musa Kirfi7Pradeep Koppolu1Fayez Hussain Niazi1Ali Elkandow8Mahmoud Darwish2Ahmad Salim Abdalla Nassar9Sami Osman Abuzied Mohammed10Nasser Hassan Abdalrady Hassan11Ghadah Salim Abusalim12Abdulaziz Samran1Anas B Alsalhani2Amir Mohiddin Demachkia13Renata Marques de Melo13Norhayati Luddin14Adam Husein14Adnan Habib15 Firas Suleyman16
Firas Suleyman16 Hussein Ali Osman17
Hussein Ali Osman17 Mohammed Sadeg Al-Awar18Mohiddin R. Dimashkieh1Lingam Amara Swapna1Ali Barakat1Ali Alqerban12
Mohammed Sadeg Al-Awar18Mohiddin R. Dimashkieh1Lingam Amara Swapna1Ali Barakat1Ali Alqerban12- 1Dar Al Uloom University, Riyadh, Saudi Arabia
- 2Vision Colleges, Riyadh, Saudi Arabia
- 3University Sains Malaysia, Penang, Malaysia
- 4Karachi Medical and Dental College, Karachi, Pakistan
- 5Usman Danfodiyo University Teaching Hospital, Sokoto, Nigeria
- 6Kannur Dental College, Kerala, India
- 7Abubakar Tafawa Balewa University Teaching Hospital, Bauchi, Nigeria
- 8Hamad Medical Corporation, Doha, Qatar
- 9Ministry of Health, Amman, Jordan
- 10King Abdullah Medical City, Makkah, Saudi Arabia
- 11King Faisal Medical Complex, Taif, Saudi Arabia
- 12Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
- 13São Paulo State University (UNESP), São José dos Campos, São Paulo, Brazil
- 14Universiti Sains Malaysia, Kelantan, Malaysia
- 15College of Dentistry, Aleppo University, Aleppo, Syria
- 16University of Health Sciences, Istanbul, Turkey
- 17Umma University, Kajiado, Kenya
- 18Al-Razi University, Sana'a, Yemen
Objectives: Even though several effective vaccines are available to combat the COVID-19 pandemic, wide disparities in vaccine distribution, and vaccine acceptance rates between high- and low-income countries appear to be major threats toward achieving population immunity. Our global descriptive study aims to inform policymakers on factors affecting COVID-19 vaccine acceptance among healthcare workers (HCWs) in 12 countries, based on income index. We also looked for possible predictors of vaccine acceptance among the study sample.
Methods: A structured questionnaire prepared after consultation with experts in the field and guided by the “Report of the SAGE working group on vaccine hesitancy” was administered among 2,953 HCWs. Upon obtaining informed consent, apart from demographic information, we collected information on trust in vaccines and health authorities, and agreement to accept a COVID-19 vaccine.
Results: Although 69% of the participants agreed to accept a vaccine, there was high heterogeneity in agreement between HCWs in low and lower-middle income countries (L-LMICs) and upper-middle- and high-income countries (UM-HICs), with acceptance rates of 62 and 75%, respectively. Potential predictors of vaccine acceptance included being male, 50 years of age or older, resident of an UM-HIC, updating self about COVID-19 vaccines, greater disease severity perception, greater anxiety of contracting COVID-19 and concern about side effects of vaccines.
Conclusions: COVID-19 vaccine acceptance among HCWs in L-LMICs was considerably low as compared to those from UM-HICs. The lowest vaccine acceptance rates were among HCWs from the African continent. This underlines the need for the implementation of country-specific vaccine promotion strategies, with special focus on increasing vaccine supply in L-LMICs.
Introduction
The SARS-CoV-2 that causes COVID-19 has been responsible for millions of deaths worldwide. Although preventive measures have been able to limit mortality and morbidity, any laxity therein, or the introduction of new mutations have usually been shown to cause recurring waves of infections, many a times even more destructive than the first one (1). As of Sepember 2021, at least eight notable mutations including the highly transmissible Delta variant has been identified, causing global concern, and forcing countries to impose repeated border restrictions (2). Therefore, unlike endemic diseases, pandemics being global in nature require collective global action to translate to global population immunity.
Two pathways exist that could lead to population immunity, either through previous infection or through immunization. According to the World Health Organisation (WHO), immunization programs prevent an estimated 2–3 million deaths every year globally (3). Since aiming for population immunity to COVID-19 through previous infection could lead to excess mortality and morbidity, and a huge socio-economic burden, especially as a consequence of the emerging mutations, the ideal strategy would be to attain it through mass immunization programs (1, 4). However, two major hurdles exist: vaccine hesitancy, a delay in acceptance, or refusal of vaccination despite availability of vaccination services, and vaccine inequality or lack of access to vaccines, a trend that has crippled mostly low and lower middle-income nations (L-LMICs) (5). As of 30 September 2021, <1% of people in low-income countries (LICs), and just 10% in lower-middle-income countries (LMICs) are fully vaccinated, compared with more than half in high-income countries (HICs) (6). Therefore, attaining global population immunity necessitates a two-pronged approach; combating vaccine hesitancy and promoting vaccine equality.
Although vaccine inequality is a complex issue that must be dealt with by policymakers and stakeholders, vaccine acceptance is mostly based on individual preferences. It is context, time and geographic location specific, and could be due to complacency around the disease, availability, ease of access and safety concern of vaccines, etc. (7). Since attitudes toward vaccines could be multifactorial, determining the predictors of vaccine acceptance could guide policymakers in formulating appropriate healthcare strategies for targeting vulnerable populations. This becomes all the more important in light of the anti-vaccine movements and protests across several countries, sometimes even supported by healthcare workers (HCWs) (8, 9).
Although, most of the focus in L-LMICs has been on vaccine inequality, lack of access and infrastructure, inefficient cold storage facilities, etc., information on vaccine acceptance, especially among HCWs is lacking. Our study aims to fill this gap by comparing vaccine acceptance in a sample of six L-LMICs and six upper middle income and high-income countries (UM-HICs) with wide geographic coverage, spanning over Asia, Africa, Europe, and South America.
Since HCWs form the frontline combatants against disease outbreaks, and are one of the most vulnerable groups, they have rightly been prioritized to receive vaccination against COVID-19. As of 24 May 2021, the WHO has estimated 115,000 HCWs to have died due to COVID-19 (10). Nonetheless, studies have shown wide variations of vaccine acceptance among HCWs, from as high as 95 percent to as low as 28 percent (11, 12). Since HCWs could act as messengers to the general public in vaccine promotion, we found it appropriate to determine the predictors of vaccine acceptance among them. Our study aimed to explore intention to accept COVID-19 vaccines among HCWs and to identify potential predictors of vaccine acceptance among them in 12 countries grouped on the basis of income index.
Materials and Methods
Study Design
A cross-sectional online self-administered survey was conducted among HCWs in 12 countries (Sudan, Pakistan, Nigeria, Kenya, India, Egypt, Turkey, Qatar, Malaysia, Saudi Arabia, Jordan, and Brazil) from February to the middle of April 2021. We grouped the countries into six L-LMICs and six UM-HICs (13). The ‘Report of the SAGE working group on vaccine hesitancy' and opinions from experts in the field were used in preparing the questionnaire (14). A pilot study was initially carried out on 10 participants, after which expert opinion was taken from four specialists in the field. The survey questionnaire developed on Google Forms was distributed online. The questionnaire required <5 min to complete. Participation was voluntary and the participants provided informed consent on the survey platform before proceeding to the survey items. The participants' anonymity was guaranteed during the data collection process. Participants were reminded only once, on failure to complete the survey form.
This study was approved by the Research Committee of College of Dentistry, Dar Al Uloom University, Saudi Arabia (COD/IRB/2020/2).
Sample
Participants (n = 2,963) included HCWs from various specialties from twelve countries. HCWs expected to come in contact with patients were only included in the study. Students who had entered the clinical training level in their fields of study were also included in the study. Other students in the healthcare field were excluded from the study. Participants below the age of 18 years were not included in the study. Participants were not compensated for participation in the study. The survey form was designed in such a way that only completed forms would qualify for submission.
Measures
Trust in Vaccines, Vaccine Manufacturers, and Health Authorities
General attitudes toward vaccines were measured using a set of 6 items. First, participants were asked if vaccines were really necessary to overcome the pandemic. Assessment questions on perceived trust in vaccine manufacturers included, whether participants trusted vaccines of only specific companies, whether vaccine manufacturers followed recommended development and production guidelines, concerns of commercial profiteering, risk of side effects of vaccines and whether manufacturers were open about disclosing the side effects of vaccines. Responses were rated on a five-point scale from 1 “strongly agree” to 5 “strongly disagree.” Participants' attitudes toward health care system were measured using a set of 2 items. Participants were asked if they were happy with the health authorities' handling of the pandemic, and their management of vaccination campaigns. Responses were rated on a five-point scale from 1 “strongly agree” to 5 “strongly disagree.”
Intention to Vaccinate
The vaccine intention was measured using a set of 7 items. First, participants were asked if vaccines should be made mandatory and if the participant intended to get vaccinated. Further questions included fear of the vaccine, care for others who would be in greater need for the vaccine, intention to protect others with weaker immunity, willingness/unwillingness to take the vaccine if required to pay for it, and fear of side effects from second dose. Responses were rated on a six-point scale from 1 “strongly agree” to 5 “strongly disagree.”
Exploratory Variables
Socio-demographic factors included age group, sex, nationality, region of current work/study place, type of work/study (governmental/private/both), and profession. Participants' report on chronic medical condition (e.g., asthma, diabetes, hypertension, heart disease, and/or cancer) was used to indicate the presence or absence of pre-existing co-morbidity. Other variables included, participants' self-updating on COVID-19 vaccine development, prior infection with COVID-19, perception of COVID-19 severity, compliance with government COVID-19 guidelines and anxiety toward contracting COVID-19.
Statistical Analysis
The main outcome of this study was intention to vaccinate. Sample statistics for each country and for the totals of low- and high-income countries were expressed as numbers and percentages for different socio-economical, health and COVID-19 vaccination parameters (Table 1). Details of responses for all questionnaire items among all countries were expressed as number and percentages (Table 2).
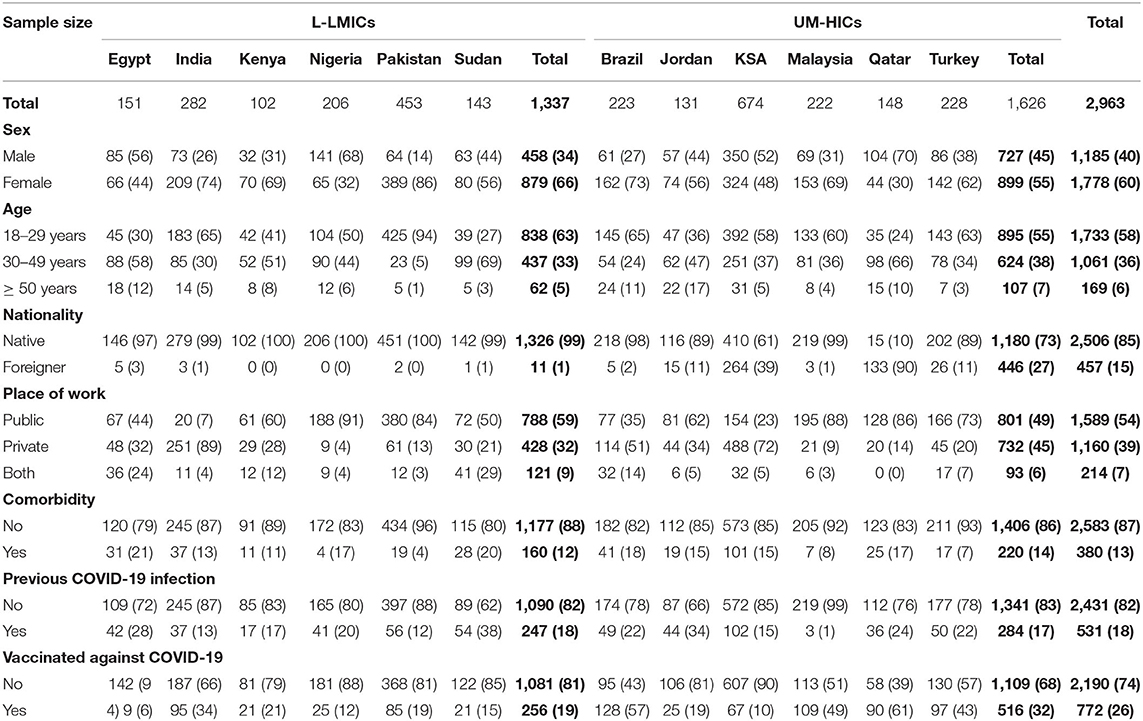
Table 1. Sample characteristics: Data are presented as n (%).
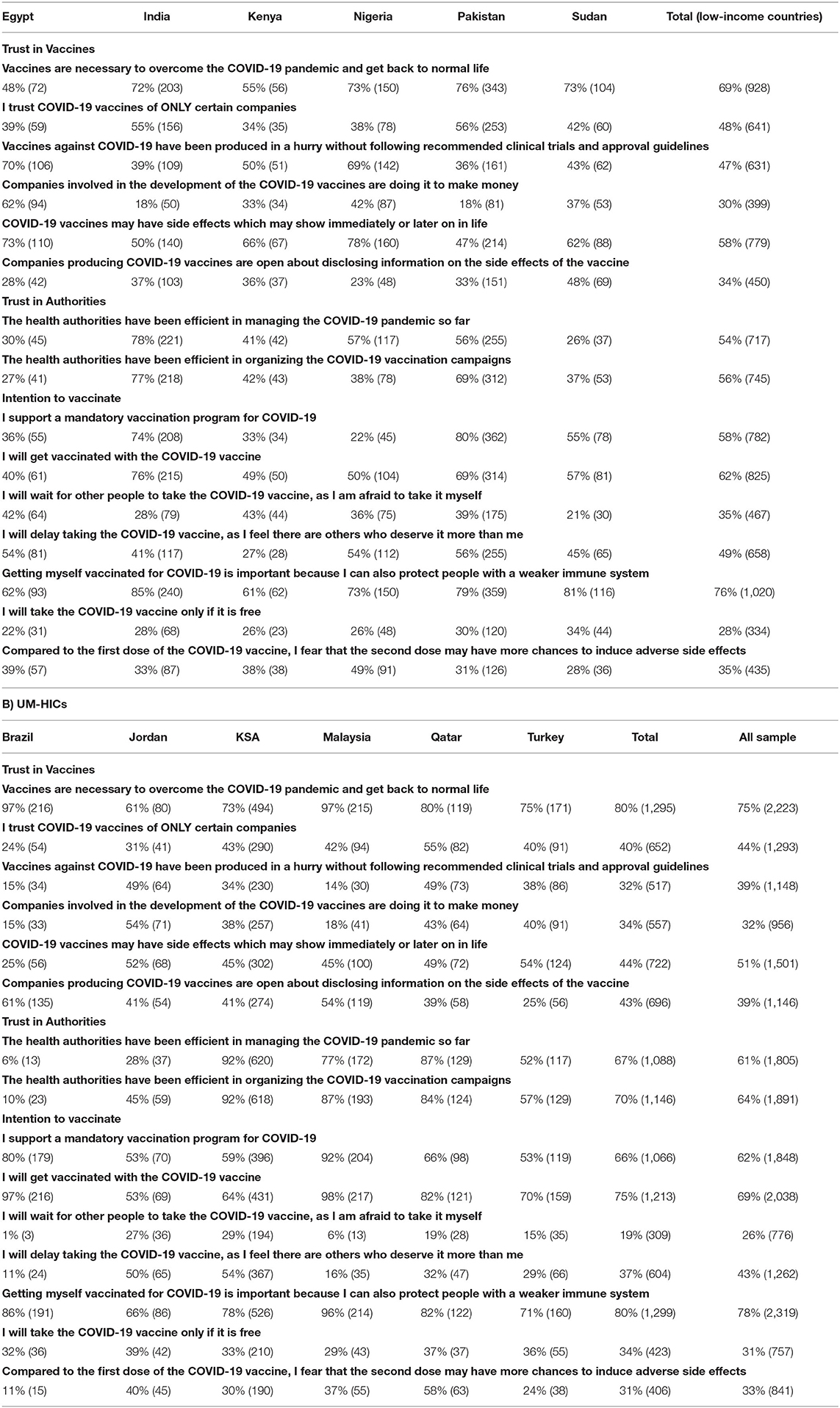
Table 2. Agreement to different survey questions—Data are presented as % (n): L-LMICs.
Bivariate statistical analysis of the relationship between the income of the countries and various questionnaire items were conducted using Chi-squared test for trend for ordinal factors, and the Chi-squared test for categorical variables (Table 3).
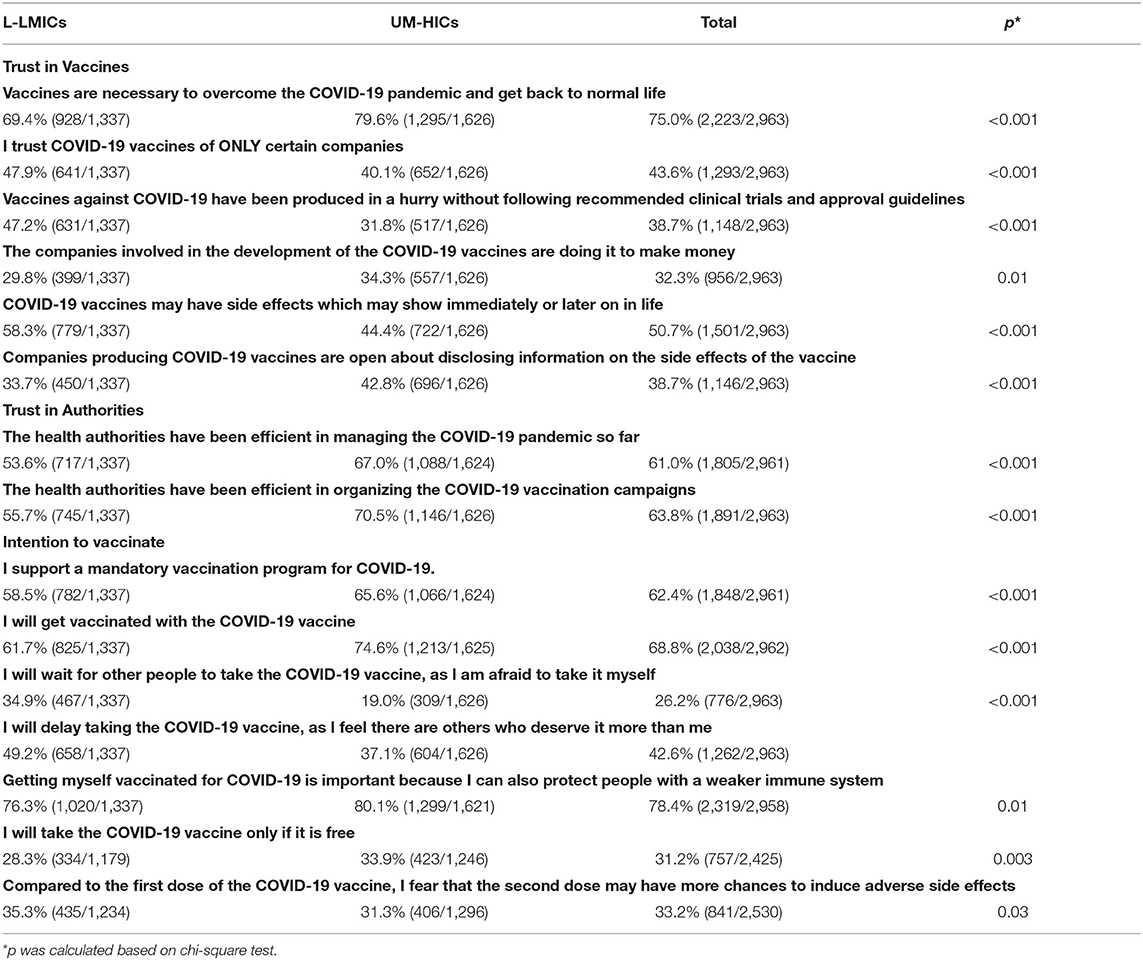
Table 3. Comparison of responses to different survey questions between L-LMICs and UM-HICs– Data are presented as % (n).
In this study we considered the participant as willing to accept a COVID-19 vaccine if he/she agreed or strongly agreed on the item “I will get vaccinated with the Covid-19 vaccine,” or if he/she had already taken the vaccine. Intention to vaccinate and its 95% confidence interval for each country are presented in Figure 1.
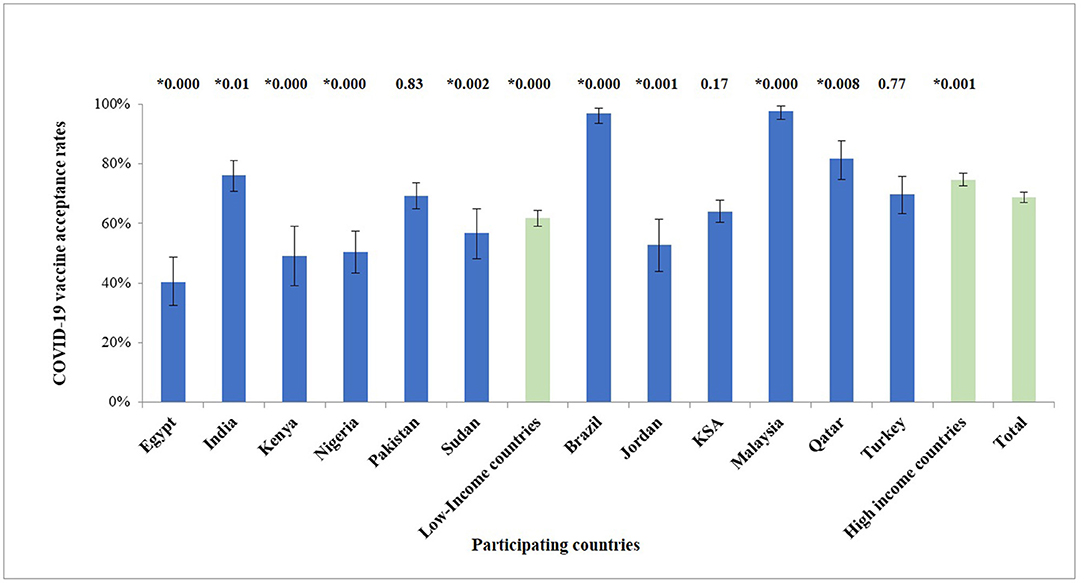
Figure 1. Agreement to accept a COVID-19 vaccine (proportion ± 95% confidence interval) among HCWs in different countries. Numbers above each bar represent the p-value for the differences between the intention to vaccinate in each country compared to the total of all the countries (0.000 means p < 0.001). *Denotes significant difference (p < 0.05).
Bivariate statistical analyses were conducted between “intention to vaccinate” and possible demographical, health and behavioral factors, and also between L-LMICs and UM-HICs by using Chi-squared test for trend for ordinal factors, and the Chi-squared test for categorical variables (Tables 4, 5).
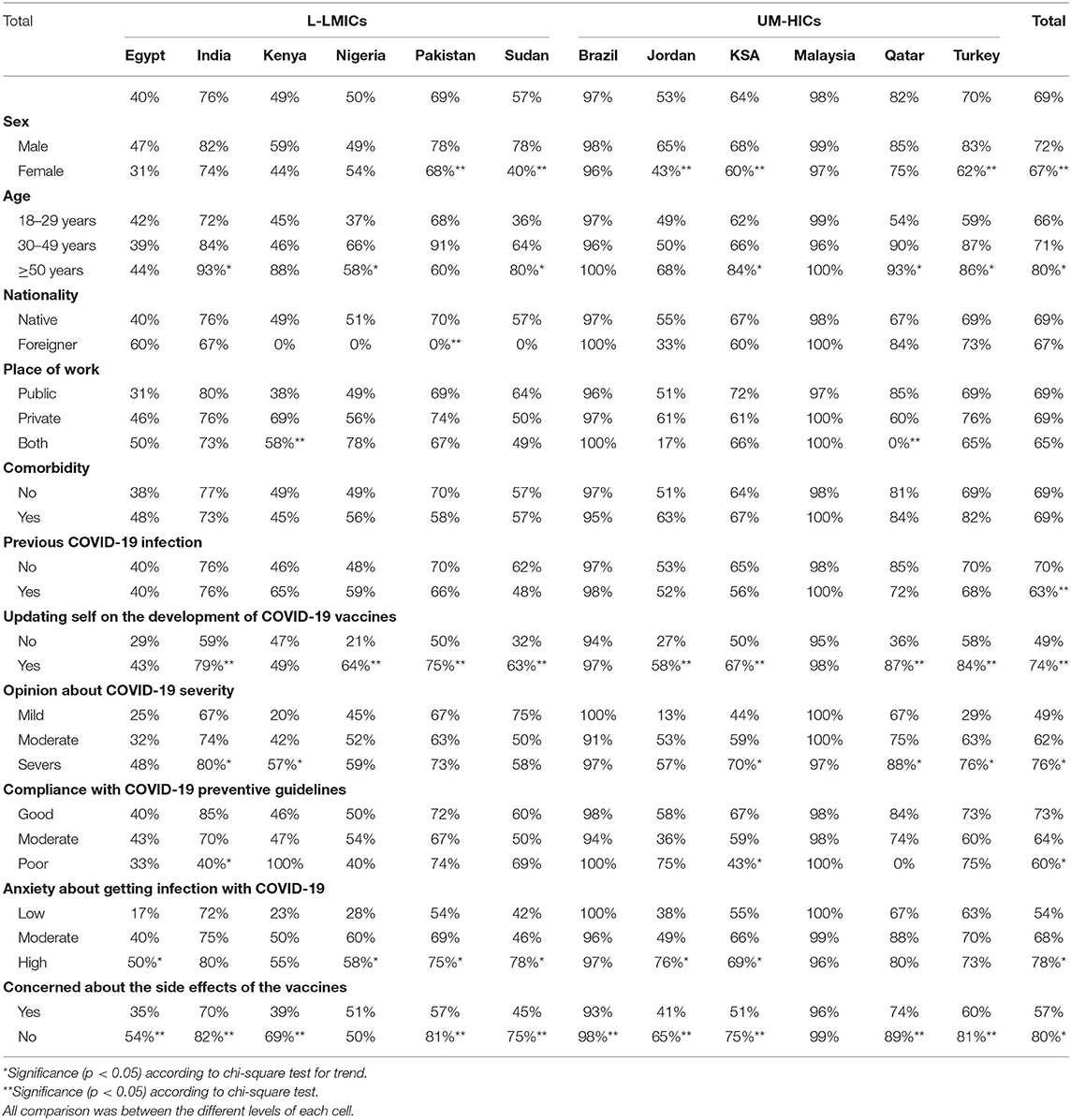
Table 4. Agreement among HCWs in different countries to accept a COVID-19 vaccine - Data are presented as %.
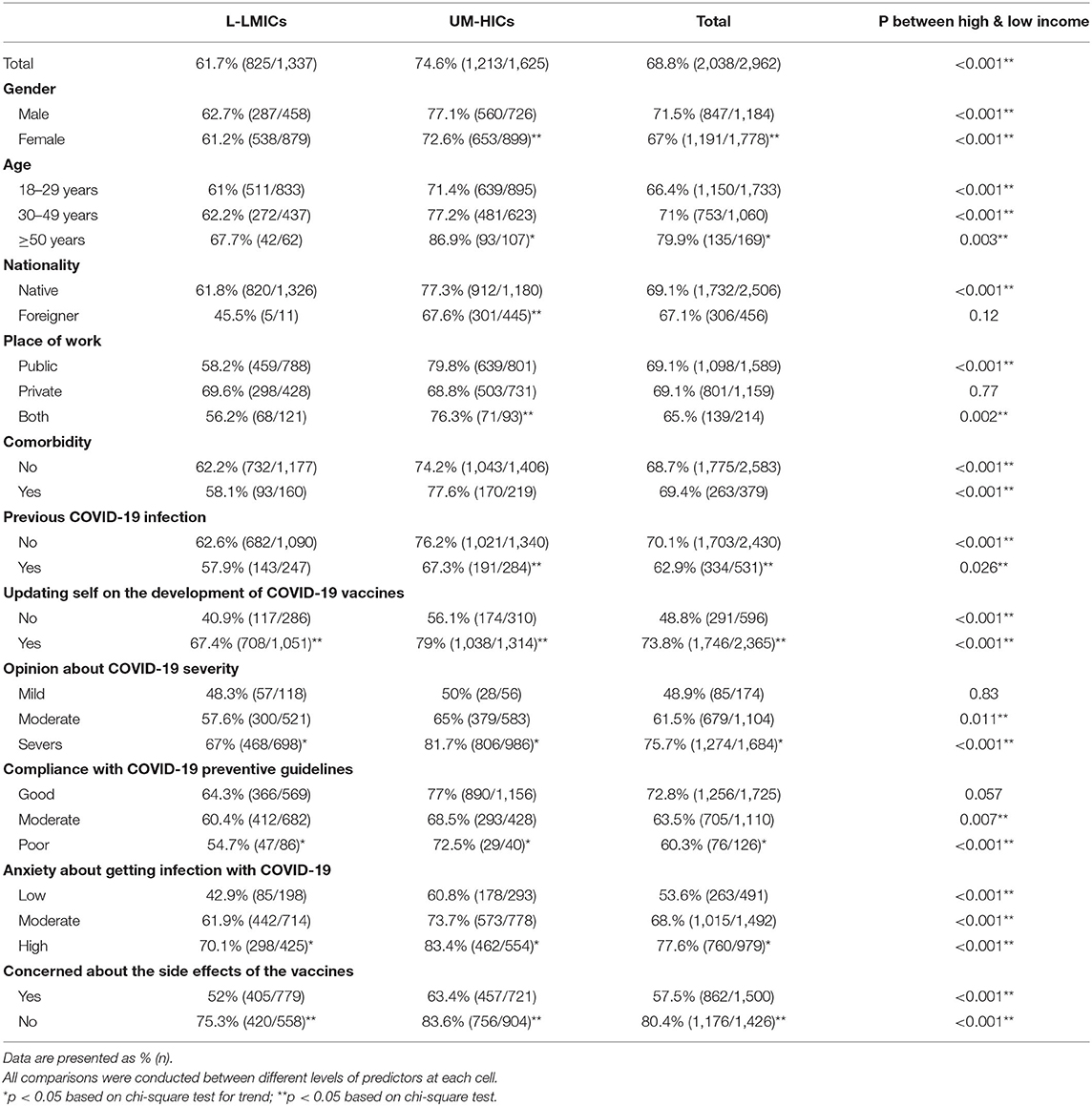
Table 5. Agreement among HCWs in L-LMICs and UM-HICs to accept a COVID-19 vaccine.
A multivariate binary logistic regression model was used to determine the predictors of vaccine acceptance. Age groups, sex, nationality, presence of any medical condition, previous infection with COVID-19, following updates on the development of vaccines against COVID-19, opinion about the severity of COVID-19, compliance with COVID-19 preventive guidelines, concern about side effects of COVID-19 vaccines and anxiety about contracting COVID-19 were included in the model and then step wisely eliminated using Wald statistic. Odds ratio and their 95% confidence interval (95% CI) are presented in Table 6.
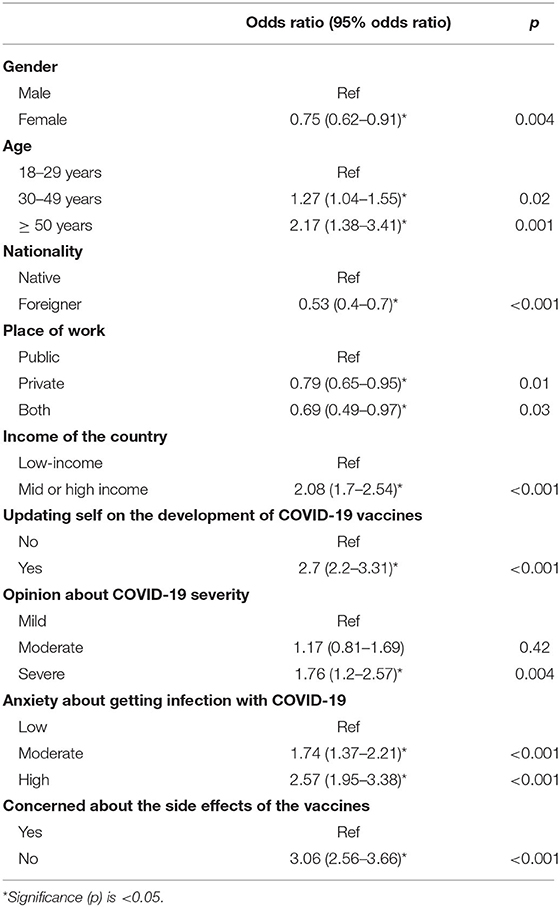
Table 6. Predictors of agreement to accept a COVID-19 vaccine.
All statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. IBM Corp, Armonk, NY, USA). The significance level was set at p < 0.05.
Results
Of the 2,963 HCWs from 12 countries that participated in the current survey, 1,337 HCWs were from six L-LMICs, and 1,626 from six UM-HICs. Table 1 shows the demographics and characteristics of the study sample. Table 2 illustrates the country-wise proportions of HCWs who agreed to various survey questions. It can be noted that the majority of the study population (75%) agreed that vaccines are necessary to overcome the COVID-19 pandemic and get back to normal life. However, distribution of the agreement was wide ranging, from 48% in Egypt to 97% in Brazil and Malaysia. Of the Nigerian HCWs, 78% believed that COVID-19 vaccines may have side effects. This figure decreased tremendously to 25% among HCWs from Brazil. Overall, almost half of the HCWs (51%) believed that COVID-19 vaccines may have immediate or delayed side effects. Trust of HCWs in health authorities and their management of the COVID-19 pandemic varied among countries, from as high as 92% in Saudi Arabia to as low as 6% in Brazil.
Agreement to accept the COVID-19 vaccine was apparent among the majority of the study population (69%). While, HCWs from Brazil and Malaysia indicated the highest figures for vaccine acceptance (97, 98% respectively), those from Egypt showed the lowest (40%) (Table 2, Figure 1). Association between survey questions and income of the country indicated clear impact for country income classification on the trust in COVID-19 vaccines, trust in health authorities and vaccine acceptance (Table 3). Vaccine acceptance and trust in health authorities were significantly higher among HCWs from UM-HICs (p < 0.001). On the other hand, concern about side effects from COVID-19 vaccines was significantly higher among HCWs from L-LMICs (p < 0.001) (Table 3). Table 4 demonstrates COVID-19 vaccine intention among HCWs according to country and demographics. It is noteworthy that vaccine acceptance was higher among male HCWs across all the surveyed countries. Moreover, older HCWs had significantly greater intention to accept the COVID-19 vaccine compared to younger HCWs. Similarly, the acceptance was higher among HCWs who were previously infected with SARS-CoV-2, updated themselves on the development of vaccines against COVID-19, perceived COVID-19 to be a severe disease, complied well with COVID-19 preventive guidelines, those who were highly anxious about contracting COVID-19 and those who feared about the side effects of the vaccines (Table 4).
Table 5 indicates significant association between COVID-19 vaccine acceptance and income of the country. Notably, HCWs from UM-HICs had significantly higher intention to be vaccinated compared to those from L-LMICs (75% vs. 62%, p < 0.001). This trend was almost dominant across the various demographics of this survey (Table 5).
Logistic regression statistics identified nine predictors of vaccine acceptance among the study population. Greater acceptance can be anticipated among male HCWs, those 50 years of age or older, native HCWs and HCWs from the UM-HICs. Additionally, HCWs who were not previously infected with COVID-19, those who followed the updates about COVID-19 vaccines, those who perceived COVID-19 to be a severe disease, those with higher levels of anxiety about contracting COVID-19 and those who had safety concerns about the vaccines indicated greater intention to be vaccinated against COVID-19 (Table 6).
Discussion
The success in the fight against COVID-19 rests largely on successful global vaccination coverage. Our study contributes to the literature on potential global COVID-19 vaccine acceptance among HCWs in six L-LMICs and six UM-HICs across four continents. Although 69% of the participants in our study indicated vaccine acceptance, our findings indicate high heterogeneity between the two groups of nations and within each group. Even though, 75% of the participants from UM-HICs indicated their agreement to accept the vaccine, only 62% from L-LMICs agreed to do so. Participants from Malaysia and Brazil, both UM-HICs, indicated the greatest acceptance rates at 98 and 97%, respectively, whereas those from L-LMICs in the African continent, including Egypt, Kenya, Nigeria and Sudan indicated the lowest with 40, 49, 50, and 57% acceptance rates, respectively. Among the L-LMICs, India and Pakistan showed better acceptance rates of 69 and 76%, respectively. Our results indicate an overall acceptance rate of 69%, which could be just enough to attain population immunity. However, the far-from-universal willingness is definitely a cause for concern and stresses the need for implementation of country- and culture-specific strategies.
Currently, there is inadequate information on vaccine acceptance among HCWs in L-LMICs, especially in the African continent. Two studies in the African continent before the start of vaccination campaigns indicated wide ranging acceptance rates of 79 and 40% (15). A study in the Democratic Republic of Congo in the early phase of the pandemic indicated that only 28 percent of the HCWs were willing to accept a vaccine against COVID-19 (12). Our results represent attitudes following the implementation of the vaccination campaigns, indicating low acceptance rates, as reported in other studies (16, 17). Reasons for this could be the lower number of reported infections and deaths in L-LMICs as compared to UM-HICs, mistrust in authorities, lack of access to vaccines, etc. (18).
Although the pace of vaccine roll-out has been slow in the L-LMICs, as of 30 September 2021, more than 60% of the population in all surveyed UM-HICs, except Jordan, has received at least one dose of the vaccine. Interestingly, in our study, among the UM-HICs, only participants from Jordan indicated very low vaccine acceptance rates (53%). The lack of trust in health authorities (only 28%) could be a major reason for this as suggested in other large-scale studies in Jordan indicating similar acceptance rates (19, 20). This could also be the case in L-LMICs in the African continent, where trust in healthcare authorities was low, due to their mishandling of the pandemic and laxity in procurement of vaccines, indicating the need for a bottom-up rather than a top-down approach. Since mistrust in authorities could translate to vaccine hesitancy or even denial, community engagement through local, tribal and religious leaders would be a viable option in L-LMICs. Surprisingly, even though Brazil indicated the lowest trust in health authorities among all the surveyed countries (only 10%), their vaccine acceptance rate was high (97%) as reported in other studies (17, 21, 22). This could be due to the high infection and mortality rate in Brazil throughout the pandemic and an increase during the study period (23).
Even though vaccine inequality in L-LMICs is a major barrier toward attaining population immunity, it could also be a reason for the low acceptance rates (24). Results from our study suggest that a higher percentage of participants from L-LMICs preferred out of fear of vaccines (35%) or consideration for others (49%), to wait for others to get vaccinated before accepting it themselves, as compared to those from UM-HICs (19 and 37%, respectively). This could be an indication of potential future increase in vaccine acceptance in L-LMICs if policymakers can address safety concerns and misinformation effectively and promote trust in health authorities. It is of concern, that some rich countries have begun giving out third doses while several L-LMICs have exhausted the limited vaccines supplied to them through the COVAX facility (25). For example, Rwanda administered 96% of the doses given to it in March within the first 2 weeks, and in June, Nigeria exhausted all of the 3.9 million doses it was given in the first phases of vaccination (26). Currently COVAX has shifted its goal of delivering two billion doses from this year to 2022 (6). Therefore, an impending challenge more serious than vaccine hesitancy in L-LMICs, that will need to be addressed by policymakers is increasing supply to meet a potential increase in demand. However, even if sufficient vaccines are supplied, lack of access or inconvenience in getting vaccinated could also translate to hesitancy. Therefore, strategies aimed at addressing hesitancy must also include making vaccines easily accessible in safe and convenient locations.
After performing logistic regression analysis, we came out with several predictors of global vaccine acceptance in the overall sample, with the income of the country being one of them. Interestingly, bivariate analysis among the two groups of countries also indicate similar significant associations between the intention to vaccinate and the parameters, but with variations in the margins of association. For example, consistent with other studies on HCWs and the general population, we found higher vaccine acceptance among males than in females, with the margin being comparatively lower in L-LMICs (27, 28). This could probably be due to the greater perception of COVID-19 severity, lower belief in conspiracy theories surrounding the disease and the vaccines, and greater access to vaccines among males. The initially reported greater risk of blood clots with certain vaccines in females and their safety concerns in pregnant ladies could also have created a negative attitude toward vaccines among them (28–30). Apart from educating females on the safety of the vaccines, policymakers should pay particular attention to providing them easy access to vaccines, especially in L-LMICs. Higher age was shown to be directly proportional to vaccine acceptance, with people over 50 years of age being most likely to accept the vaccine. Numerous studies on a global scale have reported a similar trend (31). The reason could again be the greater probability of disease severity in older individuals. On a similar note, individuals who had one or more comorbidities were more likely to accept a vaccine than those who didn't, probably due to their fear of a greater likelihood of the disease to advance to critical stage or even death.
An interesting finding in our study is the strong association between the intention to accept the vaccine and participants who updated themselves on its development. This underlines the importance of incorporating wide ranging educative strategies, on the development, safety profile and efficiency of the vaccines, through social media, public signboards and by involving respected community figures. As suggested in numerous studies, the strongest predictor of vaccine acceptance in our study is the concerns on the safety profile and side effects from the vaccines (11, 18, 32). Since our study was conducted at a time when reports of specific vaccine related adverse events, even though rare, were being widely reported in social and mass media, we find this association logical.
An emerging threat to vaccine acceptance and attaining population immunity is the increasing reports of COVID-19 vaccine breakthrough infections in fully vaccinated people (33). Although a majority of them are asymptomatic or mild, they could cause hesitant individuals to deny vaccines altogether. Another stumbling block is the provision of third vaccine doses in HICs, which could widen vaccine disparity, thereby jeopardizing vulnerable populations in L-LMICs. Although the WHO has called for a moratorium on countries giving out third doses, several countries, including the USA, have disregarded that call (34). These concerns should be appropriately addressed by the concerned authorities.
Although global vaccine distribution has skewed heavily toward higher-income countries, the modest levels of vaccine acceptance we identify in L-LMICs suggest that apart from educating the public on the necessity to accept vaccines, prioritizing distribution to them may be an efficient way to achieve immunity on a global scale and prevent novel variants from emerging. Vaccine hesitancy is one dilemma affecting most countries, if not all. However, L-LMICs are facing additional hurdles like lack of access to vaccines. Since there is a possibility that the vaccine acceptance rates may increase if access to vaccines is increased, especially in L-LMICs, governments of L-LMICs, policymakers, donor nations and NGOs like the WHO and COVAX should use every opportunity to increase supply to L-LMICs to meet the needs of their populations. The concerned authorities should work inclusively with governments of L-LMICs to focus on converting positive intentions into uptake by also investing in local supply chains and delivery. Educating health workers and community leaders and engaging them to deliver information and messaging focused on vaccine effectiveness and safety will go a long way in addressing vaccine hesitancy.
Our study has a few limitations. Since there could be a number of HCWs, especially in L-LMICs who would be willing to get vaccinated but do not have access to a COVID-19 vaccine, there is a possibility of bias. Our results represent the attitudes of HCWs at a particular point in time and is expected to change as the vaccination campaigns gather pace, depending on several factors, including rate of disease transmission and mortality, first-hand information from vaccinated friends and relatives, change in perception of disease severity and trust in authorities, etc. (35, 36). Therefore, more studies are necessary to collect snapshots at different points in time to capture changes in mass behavior and prioritize vulnerable populations accordingly. Such studies will be useful during possible future outbreaks as well. During our study period there were several reports of vaccine related serious adverse events forcing governments to put on hold, opt out or halt the use of specific vaccines (37). However, the decline in the reported adverse events and the assurances by concerned authorities have helped in gaining back public trust and combating vaccine hesitancy. Another limitation is that our results are not representative of the population at large, as we used convenience sampling. However, they do serve as a guide to policymakers and stakeholders. Yet another limitation is the mode of study. Since we used a web-based self-administration mode of survey, there could be potential bias among the participants in responding to the survey questions. However, due to the restrictions related to the pandemic, this was the best mode currently available.
Data Availability Statement
The questionnaire used in the current study is not publicly available due to certain restrictions. However, it is available from the corresponding author (Mohammed Noushad) on reasonable request.
Ethics Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Committee of College of Dentistry, Dar Al Uloom University, Saudi Arabia (COD/IRB/2020/2). The participants provided their consent to participate in this study.
Author Contributions
MN and MZN: conceptualization, methodology, and writing—original draft. MN, SR, MZN, IA-S, MH, AY, MA, AK, PK, FN, AE, MD, ASA, SA, NA, GA, AS, ABA, AD, RM, NL, AHu, AHa, FS, HO, MA-A, MRD, LS, AB, and AA: investigation and data collection and writing—review for important intellectual content and editing. MN, MZN, and SR: data analysis. All authors contributed to the article and approved the submitted version.
Conflict of Interest
Author AE is employed by Hamad Medical Corporation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors extend their appreciation to the Deanship of Postgraduate and Scientific Research at Dar Al UIoom University for their support for this work.
References
1. Mallapaty S. Delta threatens rural regions that dodged earlier COVID waves. Nature. (2021) 596:325–6. doi: 10.1038/d41586-021-02146-w
2. Mahase E. Covid-19: how many variants are there, and what do we know about them? BMJ. (2021) 374:n1971. doi: 10.1136/bmj.n1971
3. WHO. Vaccines and Immunization. World Health Organisation (2020). Available online at: https://www.who.int/health-topics/vaccines-and-immunization
4. Alagoz O, Sethi AK, Patterson BW, Churpek M, Safdar N. Effect of timing of and adherence to social distancing measures on COVID-19 burden in the United States. Ann Intern Med. (2021) 174:50–57. doi: 10.7326/M20-4096
5. MacDonald NE the the SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. (2015) 33:4161–4. doi: 10.1016/j.vaccine.2015.04.036
6. Maxmen A. The fight to manufacture COVID vaccines in lower-income countries. Nature. (2021) 597:455–7. doi: 10.1038/d41586-021-02383-z
7. Robertson E, Reeve KS, Niedzwiedz CL, Moore J, Blake M, Green M, et al. Predictors of COVID-19 vaccine hesitancy in the UK household longitudinal study. Brain Behav Immun. (2021) 94:41–50. doi: 10.1016/j.bbi.2021.03.008
8. Zadrozny B, Collins B. As vaccine mandates spread, protests follow — some spurred by nurses. NBCNews. (2021). Available online at: https://www.nbcnews.com/tech/social-media/vaccine-mandates-spread-protests-follow-spurred-nurses-rcna1654 (accessed September 20, 2021).
9. Waterson J. Anti-vaccine protesters occupy ITV News and Channel 4 headquarters. The Guardian. (2021, August 23). Available online at: https://www.theguardian.com/media/2021/aug/23/anti-vaccine-protesters-occupy-itv-nnews-and-channel-4-london-headquarters (accessed September 20, 2021).
10. World Health Organization. Director-General's Opening Remarks at the World Health Assembly - 24 May, 2021. WHO (2021). Available online at: https://www.who.int/director-general/speeches/detail/director-general-s-opening-remarks-at-the-world-health-assembly-−24-may-2021 (accessed September 20, 2021).
11. Chew NWS, Cheong C, Kong G, Phua K, Ngiam JN, Tan BYQ, et al. An Asia-Pacific study on healthcare workers' perceptions of, and willingness to receive, the COVID-19 vaccination. Int J Infect Dis. (2021) 106:52–60. doi: 10.1016/j.ijid.2021.03.069
12. Kabamba Nzaji M, Kabamba Ngombe L, Ngoie Mwamba G, Banza Ndala DB, Mbidi Miema J, Luhata Lungoyo C, et al. Acceptability of vaccination against COVID-19 among healthcare workers in the democratic republic of the Congo. Pragmat Obs Res. (2020) 11:103–9. doi: 10.2147/POR.S271096
13. The World Bank. World Bank Country and Lending Groups. (2021). Available online at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519 (accessed January 29, 2021).
14. Sage Working Group,. Report of the Sage Working Group on Vaccine Hesitancy' Was Used as a Guide in Preparing the Questionnaire. (2014). Available online at: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_ GROUP_vaccine_hesitancy_final.pdf (accessed January 10, 2021).
15. Seydou A,. Who Wants COVID-19 Vaccination? In 5 West African Countries, Hesitancy Is High, Trust Low. Afrobarometer (2021). Available online at: https://afrobarometer.org/sites/default/files/publications/Dispatches/ad432-covid-19_vaccine_hesitancy_high_trust_low_in_west_africa-afrobarometer-8march21.pdf (accessed September 22, 2021).
16. El-Sokkary RH, El Seifi OS, Hassan HM, Mortada EM, Hashem MK, Gadelrab MRMA, et al. Predictors of COVID-19 vaccine hesitancy among Egyptian healthcare workers: a cross-sectional study. BMC Infect Dis. (2021) 21:762. doi: 10.1186/s12879-021-06392-1
17. Bono SA, Villela E FdM, Siau CS, Chen WS, Pengpid S, Hasan MT et al. Factors affecting COVID-19 vaccine acceptance: an international survey among low- and middle-income countries. Vaccines. (2021) 9:515. doi: 10.3390/vaccines9050515
18. Solís Arce JS, Warren SS, Meriggi NF, Scacco A, McMurry N, Voors M, et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat Med. (2021) 27:1385–94. doi: 10.1038/s41591-021-01454-y
19. El-Elimat T, AbuAlSamen MM, Almomani BA, Al-Sawalha NA, Alali FQ. Acceptance and attitudes toward COVID-19 vaccines: a cross-sectional study from Jordan. PLoS ONE. (2021) 16:e0250555. doi: 10.1371/journal.pone.0250555
20. Sallam M, Dababseh D, Eid H, Al-Mahzoum K, Al-Haidar A, et al. Taim High rates of COVID-19 vaccine hesitancy and its association with conspiracy beliefs: a study in Jordan and Kuwait among other Arab countries. Vaccines. (2021) 9:42. doi: 10.3390/vaccines9010042
21. Taylor L. Covid-19: vaccine corruption allegations spart protests across Brazil. BMJ. (2021) 374:n1724. doi: 10.1136/bmj.n1724
22. Moore DCBC, Nehab MF, Kamacho KG, Reis AT, Junqueira-Marinho MdF, Abramov DM et al. Low COVID-19 vaccine hesitancy in Brazil. Vaccine. (2021) 39:6262–8. doi: 10.1016/j.vaccine.2021.09.013
23. WHO. WHO Health Emergency Dashboard. WHO COVID-19 Homepage. (2021). Available online at: https://covid19.who.int/region/amro/country/br (accessed September 22, 2021).
24. Liu R, Li GM. Hesitancy in the time of coronavirus: temporal, spatial, and sociodemographic variations in COVID-19 vaccine hesitancy. SSM Popul Health. (2021) 15:100896. doi: 10.1016/j.ssmph.2021.100896
25. Rogawski McQuade ET, Breskin A. Longer intervals and extra doses of ChAdOx1 nCoV-19 vaccine. Lancet. (2021) 398:933–5. doi: 10.1016/S0140-6736(21)01817-1
26. Jerving S. The long road ahead for COVID-19 vaccination in Africa. Lancet. (2021) 398:827–28. doi: 10.1016/S0140-6736(21)01967-X
27. Sallam M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccines. (2021) 9:160. doi: 10.3390/vaccines9020160
28. Robinson E, Jones A, Lesser I, Daly M. International estimates of intended uptake and refusal of COVID-19 vaccines: a rapid systematic review and meta-analysis of large nationally representative samples. Vaccine. (2021) 39:2024–34. doi: 10.1016/j.vaccine.2021.02.005
29. Sessa M, Kragholm K, Hviid A, Andersen M. Thromboembolic events in younger women exposed to Pfizer-BioNTech or Moderna COVID-19 vaccines. Expert Opin Drug Saf. (2021) 26:1–3. doi: 10.1080/14740338.2021.1955101
30. Ciapponi A, Bardach A, Mazzoni A, Alconada T, Anderson SA, Argento FJ, et al. Safety of components and platforms of COVID-19 vaccines considered for use in pregnancy: a rapid review. Vaccine. (2021) 39:5891–908. doi: 10.1016/j.vaccine.2021.08.034
31. Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. (2021) 27:225–8. doi: 10.1038/s41591-020-1124-9
32. Fares S, Elmnyer MM, Mohamed SS, Elsayed R. COVID-19 vaccination perception and attitude among healthcare workers in Egypt. J Prim Care Community Health. (2021) 12:21501327211013303. doi: 10.1177/21501327211013303
33. Brown CM, Vostok J, Johnson H, Burns M, Gharpure R, Sami S, et al. Outbreak of SARS-CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings - Barnstable County, Massachusetts, July 2021. MMWR Morb Mortal Wkly Rep. (2021) 70:1059–62. doi: 10.15585/mmwr.mm7031e2
34. WHO. WHO Director-General's Opening Remarks at the Media Briefing on COVID-19 - 4 August, 2021. WHO (2021). Available online at: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-4-august-2021 (accessed September 22, 2021).
35. Kitro A, Sirikul W, Piankusol C, Rirermsoonthorn P, Seesen M, Wangsan K, et al. Acceptance, attitude, and factors affecting the intention to accept COVID-19 vaccine among Thai people and expatriates living in Thailand. Vaccine. (2021) 39:7554–61. doi: 10.1016/j.vaccine.2021.11.031
36. Carlson SJ, McKenzie L, Roberts L, Blyth CC, Attwell K. Does a major change to a COVID-19 vaccine program alter vaccine intention? A qualitative investigation. Vaccine. (2021) 40:594–600. doi: 10.1016/j.vaccine.2021.12.021
Keywords: COVID-19, vaccine acceptance, low-income countries, population immunity, vaccine inequality
Citation: Noushad M, Rastam S, Nassani MZ, Al-Saqqaf IS, Hussain M, Yaroko AA, Arshad M, Kirfi AM, Koppolu P, Niazi FH, Elkandow A, Darwish M, Abdalla Nassar AS, Abuzied Mohammed SO, Abdalrady Hassan NH, Abusalim GS, Samran A, Alsalhani AB, Demachkia AM, de Melo RM, Luddin N, Husein A, Habib A, Suleyman F, Osman HA, Al-Awar MS, Dimashkieh MR, Swapna LA, Barakat A and Alqerban A (2022) A Global Survey of COVID-19 Vaccine Acceptance Among Healthcare Workers. Front. Public Health 9:794673. doi: 10.3389/fpubh.2021.794673
Received: 02 November 2021; Accepted: 30 December 2021;
Published: 08 February 2022.
Edited by:
Constantinos Tsioutis, European University Cyprus, CyprusReviewed by:
Nikolas Dietis, University of Cyprus, CyprusChristopher Holzmann-Littig, Technical University of Munich, Germany
Copyright © 2022 Noushad, Rastam, Nassani, Al-Saqqaf, Hussain, Yaroko, Arshad, Kirfi, Koppolu, Niazi, Elkandow, Darwish, Abdalla Nassar, Abuzied Mohammed, Abdalrady Hassan, Abusalim, Samran, Alsalhani, Demachkia, de Melo, Luddin, Husein, Habib, Suleyman, Osman, Al-Awar, Dimashkieh, Swapna, Barakat and Alqerban. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammed Noushad, aW55YTExM0B5YWhvby5jb20=