
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health, 23 December 2021
Sec. Public Health and Nutrition
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.789535
This article is part of the Research TopicThe Obesity Epidemic: Causes, Context, PreventionView all 15 articles
 Mariam Mandoh1*
Mariam Mandoh1* Julie Redfern1,2Seema Mihrshahi3,4Hoi Lun Cheng5,6Philayrath Phongsavan4
Julie Redfern1,2Seema Mihrshahi3,4Hoi Lun Cheng5,6Philayrath Phongsavan4 Stephanie R. Partridge1,4
Stephanie R. Partridge1,4Background: Traditionally, adolescent participation in research has been tokenistic. Adolescents are rarely afforded the opportunity to influence decision-making in research designed to prevent obesity. Engaging adolescents in meaningful decision-making may enhance research translation. This review aimed to analyze the current modes and nature of adolescent participation in obesity prevention research decision-making.
Methods: A systematic scoping review was conducted using Arksey and O'Malley's six-stage framework. Six major databases were searched for peer-reviewed primary research studies with adolescent participation related to obesity, physical activity, and diet. Modes of adolescent participation were categorized based on the Lansdown-UNICEF conceptual framework for measuring outcomes of adolescent participation. The framework outlines three modes of meaningful participation: (i) consultative, which involves taking opinions and needs into consideration; (ii) collaborative, where adolescents are partners in the decision-making process; and (iii) adolescent-led participation where adolescents have the capacity to influence the process and outcomes. The degree of involvement in research cycles was classified based on the National Health and Medical Research Council consumer engagement framework. Five stages of the research cycle were determined: identify, design and develop, conduct, analyze and disseminate.
Results: In total, 126 papers describing 71 unique studies were identified. Of these, 69% (49/71) took place in the USA, and 85% (52/61) were conducted in minority or underserved communities, while males were more likely to be under-represented. In 49% (35/71) of studies, participation was consultative and 9% (6/71) of studies involved an adolescent-led approach. Furthermore, 87% (62/71) of studies incorporated adolescent participation in one or more of the research cycle's formative phases, which involve eliciting views, opinions and idea generation. Only 11% of studies engaged adolescents in all five stages of the research cycle where adolescents could have more influence over the research process.
Conclusion: Meaningful adolescent participation in the obesity prevention research cycle is limited. Empowering and mobilizing equal partnership with adolescents should be at the forefront of all adolescent-related obesity prevention research.
Overweight and obesity is a global health crisis affecting 340 million young people (5–19 years) worldwide (1). Despite common misconceptions and gender-based stereotypes, obesity is more likely to affect adolescent boys than girls in 60% of countries, with this trend most apparent in high and upper-middle-income nations (2). The prevalence of overweight and obesity in young people continues to increase and has quadrupled in this cohort from 4 to 18% in the last three decades (3). The incidence of overweight and obesity has plateaued in several high-income countries while simultaneously escalating at a 10-fold rate in lower-income countries across Asia and Africa (4). Overweight and obesity are significant risk factors for developing lifestyle-related chronic diseases such as cardiovascular disease, diabetes mellitus, hypertension, some cancers, muscular-skeletal, and mental health disorders (5).
An unhealthy diet and insufficient physical activity are modifiable risk factors for obesity. Social equity challenges, such as income, education, and food insecurity strongly influence these risk factors (6, 7). An increasing body of evidence demonstrates the relationship between diet and physical activity behaviors in adolescence and the association between obesity and chronic disease development in adulthood (8–11). Yet, globally, there is inconsistent evidence regarding the effectiveness of diet or physical activity interventions or a combination of both to reduce the risk of obesity and its related co-morbidities in adolescents (12–14). Obesity prevention research is further complicated by ethical and psychosocial health concerns such as weight stigmatization, eating disorder risk, low self-esteem, body dissatisfaction, anxiety, and depression (15–18). Emerging research demonstrates how supervised obesity treatment can improve psychosocial health for adolescents; however, there is limited research regarding obesity prevention initiatives (19). Engaging adolescents in the design and development of obesity prevention interventions can address social equity challenges and ethical and psychosocial health concerns (20). It is therefore crucial that adolescents from all backgrounds are engaged in obesity prevention research (21).
Current evidence syntheses have focused on determining the efficacy and effectiveness of obesity prevention interventions (12, 14); the conclusions are limited mainly to factors related to intervention outcomes (22). This finding suggests little attention has been given to understanding meaningful adolescent participation in the research decision-making process beyond passive engagement as research participants. Currently, no review has focused on understanding adolescents' engagement in the research cycle and relationships to intervention efficacy and effectiveness.
In recent years, there has been a growing call to prioritize the voice of adolescents in societal decision-making (23). Meaningful adolescent participation is a fundamental human right as articulated in the Convention on the Rights of the Child (24). The importance of adolescent participation is further expanded on in the Lansdown-UNICEF framework for adolescent participation (25). The framework acknowledges that meaningful participation involves adolescents articulating their views and being involved in the decision-making process to impact matters of importance to them. Meaningful participation varies in mode and is subject to the evolving capacity of adolescents as they transition from early adolescence through to young adulthood.
Theoretical youth engagement models such as UNICEFs Adolescent and Youth Engagement Strategic Framework (26), Hart's Ladder (27), and Shier's pathway (28), among others, have been developed to guide organizations on the components of effective and ethical consumer or stakeholder engagement. Such models aim to amplify adolescent voices and improve their confidence and feelings of empowerment, which are fundamental to meaningful participation and decision-making in research and ultimately to research translation (25, 26).
Additionally, practical and transparent frameworks allow researchers to monitor meaningful participation where stakeholders and consumers can be involved effectively throughout the research process. Examples of such are the United Kingdom's National Institute for Health Research (NIHR) INVOLVE Public and Patient Involvement Framework (29, 30), and the Australian National Health and Medical Research Council (NHMRC) Consumer Engagement Framework (31), which provide a detailed outline of the stages and strategies necessary to achieve meaningful participation. Such frameworks offer foundational measures for researchers to assess the degree of engagement expected throughout the research cycle.
Despite the increasing call to effectively engage adolescents in society and consumers in research, there is yet to be meaningful convergence. To date, reviews in the field of participatory research have tended to focus specifically on specific methodological approaches such as Participatory Action Research (PAR) (32, 33), Youth advisory (34), Patient Engagement (PE) (35), or Community Based Participatory Research (CBPR) (36). The demographic of interest also varies significantly between published reviews with researchers specifically investigating children (37) or children grouped with adolescents, youth, or young people and results for such populations analyzed together despite their significantly different needs and abilities (32, 33, 36, 38). Moreover, current evidence syntheses are looking broadly at participatory approaches (32, 33, 36), how they influence social determinants (32), general health and well-being (34, 35, 38), or health policy (39). Currently, comprehensive evidence syntheses are lacking to evaluate the participatory approaches for adolescent consumers in obesity prevention research.
Mental health researchers have recognized that engaging adolescents in meaningful participation is a crucial component of effective research and intervention development (40, 41). Adolescents have unique insight into their own lived experiences and needs; therefore meaningful participation involving adolescent consumers in the decision-making is a potentially vital link to tailor obesity and chronic disease prevention interventions to this demographic. In this scoping review, we aim to address this gap in the literature by broadly assessing how and to what extent adolescents are meaningfully participating in the co-design and decision-making in research studies that target overweight, obesity, physical activity, and dietary interventions specifically for adolescents. Secondly, we aim to provide recommendations on optimal modes of participation in obesity and chronic disease prevention research.
The following research questions guided this scoping review:
i) Is there evidence of the effectiveness of adolescent participation in peer-reviewed primary research studies?
ii) What are the components, processes, or conceptual frameworks of effective peer-reviewed primary research studies involving adolescent participation?
iii) Are there any identified barriers or facilitators, or evidence gaps for adolescent participation?
A scoping review was determined to be the most suitable form of evidence synthesis for the research question as it allowed for a broad and thorough examination of the existing literature (42). The scoping review methodology was informed by the Arksey and O'Malley six-stage framework (43), Levac et al.'s (44) recommendations, and the Joanna Briggs Institute (45–47) guidelines for scoping reviews. The review was reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist (see Supplementary File 1) (48). As per scoping review guidelines, no quality assessment is required (47, 48). The research questions were formulated, followed by the identification of criteria for the inclusion of relevant studies. Next, studies were selected based on the pre-defined criteria, and relevant data from the included studies were extracted. Collating, summarizing, and reporting the results followed. The scoping review protocol contains full details of the study methodology and search strategy (49). The protocol is registered with Joanna Briggs Institute and Open Science Framework, doi: 10.17605/OSF.IO/E3S64. A brief description of the methods is provided below.
The term “adolescent” is defined by the World Health Organization (WHO) as a person aged 10–19 years old, and “youth” as one between the age of 15–24 years old (50). However, within the published peer-reviewed literature, these terms are used synonymously. To broadly examine the literature and in line with the Lancet Child and Adolescent health definition of an adolescent (51), this scoping review assessed published peer-reviewed literature engaging adolescents or youth aged 10–24 years.
Meaningful participation refers to participation in which adolescents have some level of influence over the research and development decision-making. The mode of meaningful participation is dependent on the degree of influence adolescents impart on the research process (Table 1). Furthermore, meaningful participation is dependent on the methods and strategies used at various points within the research cycle (31). All modes of participation can be valid and effective if conducted within an enabling environment where participatory outcomes are based on empowerment and the degree of influence is measured and achieved (25).

Table 1. Working definitions to classify mode and degree of adolescent participation.
Based on key concepts emerging from the research questions, the research team developed a search strategy in consultation with an academic liaison librarian. All qualitative and quantitative peer-reviewed primary research studies published from 1995 to December 2020 were considered for inclusion; reviews were excluded. Peer-reviewed papers of all languages with an abstract in English were considered. Studies involved participants aged 10–24 years involved in obesity or chronic disease prevention, nutrition or physical activity research decision-making. Youth participation was the primary outcome sought hence inclusion of broad search terminologies such as Youth-PAR, CBPR, youth involvement, and youth engagement. Medical subject heading (MeSH) terms were selected accordingly. An example search strategy is presented in Supplementary Table 1.
Systematic searches of six scientific databases, Medline (PubMed), Embase, CINAHL, Scopus, Global health, and CENTRAL, were conducted. Publications identified up to the first of December 2020 were considered. Additional sources were identified through hand searching, reference list examination, and citation chaining. Results were pooled and duplicates removed, remaining results were uploaded to the Covidence systematic review software. A two-part study selection process followed, first a title and abstract review by one reviewer (MM) and secondly a full-text review by two reviewers (MM and SRP). Any discrepancies were resolved by consensus with a third reviewer (JR).
Data extraction table variables were iteratively developed to broadly encompass the scope of adolescent participation in the obesity and chronic disease research cycle. Relevant data were extracted and tabulated by one reviewer (MM) (see Supplementary Table 2). Key outcomes extracted included social and environmental variables, the degree of adolescent participation in the research cycle, modes of participation, participatory outcomes, and chronic disease-associated outcomes. Corresponding authors were contacted via email where necessary data was missing or not reported. A second reviewer (SRP) cross-checked 20% of studies for consistency in data extraction.
Data presented were based on active (meaningful) adolescent participation in the research and decision-making process, where adolescents were engaged as consumers rather than passive study participants. Data were assessed based on key modes of participation (consultative, collaborative and, adolescent-led) and alignment with participatory outcomes from the Lansdown-UNICEF conceptual framework for adolescent participation (25). After the protocol publication, the NHMRC framework for effective consumer and community engagement in research was selected to contextualize the data within the phases of the research cycle (31). The framework was deemed necessary for data analysis and was the only protocol deviation.
Chronic disease outcomes associated with improved health status or obesity and chronic disease risk factor prevention were established based on emerging categories founded on preliminary searching. Reported chronic disease outcomes were classified into the following categories: (i) increased awareness of family, peers and adolescents; (ii) program or intervention development; (iii) policy change; (iv) environmental change, relating to changes in the physical surroundings in which adolescents live; (v) behavior change specifically changes in diet and physical activity behaviors; and (iv) health status or risk factor change, including but not limited to change in body mass index, weight status, waist circumference, and blood pressure. Qualitative analysis of the data revealed emerging trends and themes. Data were reported by descriptive numerical analysis and in narrative form.
The search strategy generated a total of 1,212 results, including an additional 53 papers through hand searching, which were subsequently pooled, and duplicates removed, leaving 902 unique papers (Figure 1). The 902 papers were assessed by title and abstract screening for inclusion; 736 were excluded. The full text of the remaining 166 papers were reviewed, and a further 40 papers were excluded and reasons documented. In total, 126 full-text peer-reviewed papers (52–175) describing 71 unique studies were included in the review.
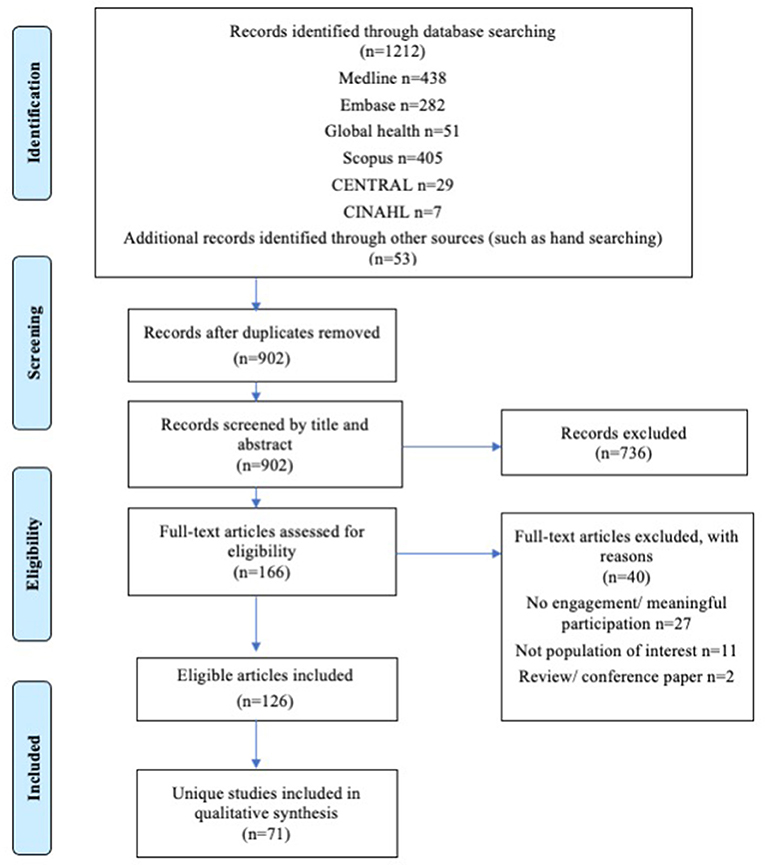
Figure 1. Prisma flow diagram: adolescent participation in research for obesity prevention.
The studies identified varied broadly in their target demographic and scope. Various socioeconomic and ecological characteristics were analyzed (Table 2).
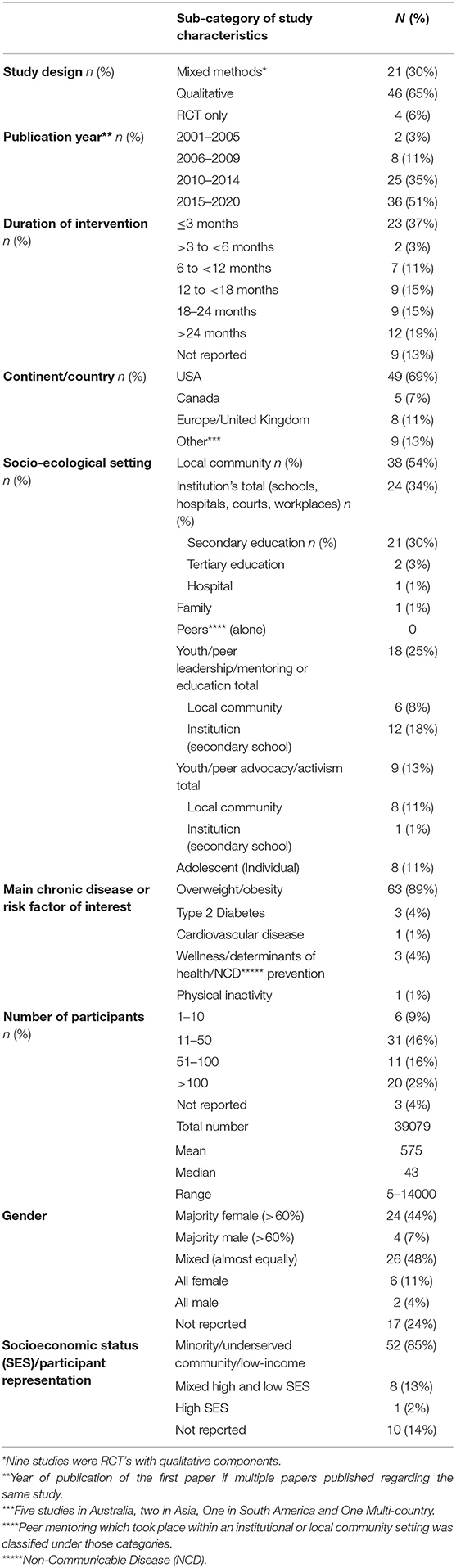
Table 2. Summary of study characteristics.
Of the 71 unique studies identified, 65% (46/71) were qualitative, and a further 30% (21/71) employed a mixed-methods approach. Thirteen studies (18%, 13/71) were randomized controlled trials (RCT).
Publication dates ranged from 2003 to 2020, with >50% (n = 36) of studies publishing their first paper between 2015 and 2020. Studies varied in duration from 30-min to 6 years, the mean study duration being 3 months or less in duration (23/71), followed by intervention durations >12 months (12/71).
Most studies (76%, 54/71) were conducted in North America, with a total of 49 in the USA and five in Canada. Eight studies took place in Europe (Netherlands, United Kingdom, Belgium, Spain, France) and five studies in Australia. Furthermore, two studies were conducted in Asia (Republic of Korea, Vietnam), one in South America (Peru), and one multi-country (Australia, New Zealand, Fiji, and Tonga) study.
The most common socioecological setting targeted was the local community (54%, 38/71), followed by secondary education institutions (30%, 21/71). Eight studies targeted the adolescent (individual), and one study specifically targeted the family unit. Peer leadership, mentoring, or education were components of 18 studies, with six targeting the local community and 12 targeting secondary education institutions. Similarly, youth or peer advocacy was a component of nine studies, eight of which targeted the local community and one targeting a secondary education institution.
Socioeconomic status (SES) was described in 61/71 studies (86%), of those reporting SES, 52 studies (85%) were conducted in a minority or underserved community, and one study took place in an affluent (high SES) setting.
Overweight and obesity was the most common chronic disease or chronic disease risk factor targeted in the included studies, with 89% (63/71) of studies reporting this to be the main purpose for the study. The remaining eight studies investigated the prevention of obesity-related co-morbidities such as type 2 diabetes and cardiovascular disease.
Of the 71 studies, the total number of participants involved in a meaningful participatory method ranged from 5 to 14,000 participants (Supplementary Table 2), with a median of 43 participants. Thirty-one studies (46%) had between 11 and 50 participants; three studies did not report the number of adolescent participants. The gender of adolescent participants was not reported in 24% of studies (17/71). In 26 (48%) of the studies which reported gender, gender was evenly distributed. Still, in the studies that remained, males were more likely to be under-represented [24 (44%) or not represented at all six (11%), while females were under-represented in four (7%) studies and not represented in a further three (4%)].
In 87% (62/71) of studies, adolescents participated in at least one of the two formative phases of the research cycle (identification of the topic or design or development), and in 11% (8/71) of studies, participation took place in all five stages of the research process (Table 3). The mode of participation was almost equally distributed between consultative (49%, 35/71) and collaborative (41%, 29/71) approaches. An adolescent-led mode of participation was identified in six studies (9%).

Table 3. Adolescent participation, theoretical frameworks used and outcomes of participation in the research cycle.
The number and type of participatory methods used by researchers in the included studies significantly varied. Results revealed that a combination of methods was commonly employed in each study. Approaches ranged from one participatory method per study to a maximum of four methods, with a mean of two participatory methods per study. Adolescent-led participatory approaches were more likely to employ a greater number of participatory methods (mean of three methods per study) to achieve their outcomes.
Overall, the most common single method used was focus groups in 55% (39/71) of studies, followed by questionnaires and surveys (38%, 27/71) and interviews (38%, 27/71). These were more commonly employed in consultative studies either alone or combination with other methods. Furthermore, other methods such as photovoice (n = 10), needs and community assessments (n = 5), discussion groups, and community forums (n = 3) were also used in a smaller proportion of studies. These methods have in common that they elicit views, opinions and uncover the needs of adolescents and their community which is a fundamental element of formative work. Youth advisory groups (n = 2) and peer leadership and advocacy activities were a component of 25% of studies (18/71). The studies that used these approaches were typically studies that employed a collaborative (n = 13) or adolescent-led (n = 3) mode of participation. A social marketing approach was used in six studies (8%), four of which were collaborative, and two were adolescent-led. Additionally, co-design or co-creation activities (sessions) were specified in 7% (n = 5) of studies; these were a component of one consultative study and four studies that used a collaborative approach.
Overall, studies varied significantly in their theoretical basis, with 9 theoretical models and 15 complex models and frameworks reported. Table 3 presents the most common models, theories and frameworks used. A significant number of studies used multiple theories or models (49%, 35/71). Overall, 48% (34/71) of studies reported a participatory design, of which 74% (25/34) used CBPR principles to guide their project. Moreover, other theories which complement but do not explicitly promote a participatory approach were identified. Thirty-four (48%) studies reported a social component, with social-cognitive theory reported to inform 22/71 (31%) of studies, and socio-ecological theories informed seven studies. Of the multi-theory models employed, which did specifically involve a participatory component, the transtheoretical model of behavior change (n = 5) and the PRECEDE-PROCEED model (n = 4) were the most reported. Empowerment theory was used in seven studies; however, participatory outcomes which measure empowerment and influence were only measured in five studies. Of the studies labeled participatory, 32% (11/34) involved adolescents in at least four research cycle stages. A collaborative approach was employed in more than half (18/34, 53%) of participatory studies.
Chronic disease outcomes were largely based on outcomes of obesity prevention research. The most common chronic disease-related outcomes of adolescent participation were “increased awareness among family and peers” (49/71, 69%) and “program or intervention development” (45/71, 63%). It is also important to note that two studies (69, 135) were in progress, and therefore, information on outcomes was not available or incomplete.
Overall, 12 studies (17%, 12/71) reported four or more chronic disease outcomes; these studies tended to be 12 months or longer in duration, and five of these studies (41%) involved adolescents in four or more stages of the research cycle. Nine of the 12 studies (75%) used a mixed-methods interventional design, with seven studies (58%) involving an RCT component and another two (17%) studies using a quasi-experimental design. Of these 12 studies, 11 (92%) employed a collaborative mode of adolescent participation. Moreover, seven studies (58%) were supported by multiple theoretical frameworks, and six (50%) had a participatory agenda. While 8/12 (67%) studies used youth or peer leadership or advocacy practice, only 33% (4/12) were also described as participatory. In contrast, all seven RCTs involved youth or peer-leadership or advocacy regardless of whether they declared the usage of a participatory model or not. Overall, participatory outcomes were measured in 5/71 (7%) studies but were more likely to be reported in studies with four or more chronic disease outcomes measured 3/12 (25%).
Due to the broad range of study designs and aims, chronic disease outcomes as per the established categories were not within the aim or scope of many of the studies reviewed and, as such, were not reported. This was particularly the case in qualitative studies that employed a consultative participatory mode, usually focus groups, discussion groups, questionnaires, surveys, or interviews. In these instances, the researchers were seeking opinions and preferences. Therefore changes in weight, diet, or physical activity levels were not measured as they would be outside the scope of the study. A total of 91% (29/32) of consultative studies described <3 chronic disease outcomes. Similarly, all six studies (82, 86, 114, 133, 173) that used an adolescent-led participation mode achieved no more than three chronic disease outcomes despite all except one (145) meeting the aims of their respective projects. Furthermore, adolescent-led studies described outcomes related to increased awareness (82, 86, 133, 173), program/intervention development (86, 114, 133, 173), or environmental changes (86, 133) and did not report anthropometric, behavioral changes, or changes in health status associated with obesity and chronic disease development.
Differences in the study designs and methodologies of the studies analyzed meant that data reporting differed. Quantitative measures were often not measured/ or sought in many studies included within this review. Still, 22 studies (31%) reported an improvement in one or more obesity risk factors. Data on anthropometric measures as well as behavioral measures such as physical activity and dietary intake were analyzed.
Eight studies (11%) reported an improvement in one or more anthropometric measures such as BMI (57, 62, 76, 91, 158, 169), weight (161), waist circumference (158), or adiposity (142) albeit not always statistically significant (161, 169). Methodological components which were common between these studies included use of an RCT (57, 62, 76, 91, 142, 169) in 75% (6/8) of studies, a collaborative (62, 76, 91, 158, 161, 169) mode of adolescent participation in 75% (6/8) of studies and inclusion of a peer-component (57, 62, 76, 91, 169) in 63% (5/8) of studies.
Improvements in physical activity and fitness behaviors were reported in 12 studies (54, 93, 96, 101, 105, 126, 142, 149, 161, 164, 165, 169), five of these involved an RCT (101, 142, 164, 165, 169), seven employed a collaborative (54, 93, 96, 105, 161, 165, 169) mode of adolescent participation and seven involved a peer-component (93, 96, 105, 126, 149, 164, 169).
Encouraging changes in dietary behaviors were reported in 17 studies, as an improvement in dietary intake or nutrition behaviors (61, 91, 96, 101, 105, 112, 126, 149, 161, 164, 165, 169), increased fruit (93) and vegetable consumption (121), reduced caloric intake (99), reduction in sugar sweetened beverage intake (108) or an increase in water consumption (54). Overall studies involving improvements in dietary behaviors had in common that they were more likely to be collaborative (9/17) (54, 91, 93, 96, 105, 108, 161, 165, 169) and involve a peer-component (10/17) (61, 91, 93, 96, 105, 108, 126, 149, 164, 169). Studies which reported an improvement in dietary behaviors were almost evenly of qualitative (7/17) (54, 93, 105, 112, 121, 126, 149) or RCT (6/17) design (91, 101, 108, 164, 165, 169).
Understanding barriers and facilitators to adolescent engagement are essential in improving meaningful adolescent participation in the obesity prevention research cycle. Of the studies analyzed, school, family, and work commitments were the most common barriers suggested. Facilitators to participation included compensation for the time spent participating, peer-support, leaderships opportunities, and adolescent-led participatory methods (such as photovoice and youth advisory groups), which gave the youth a voice and influence. Furthermore, incorporating meaningful participation into supportive and trusted environments such as the local community or school setting was suggested to facilitate engagement.
Overall, barriers and facilitators to adolescent participation when documented were usually reported as general observations rather than concrete data. Barriers and facilitators to participation were seldom an outcome measured in the studies reviewed and is in line with lacking measurements of participatory outcomes in general.
This is the first review investigating adolescent participation in the obesity prevention literature to the best of our knowledge. Overall, findings from our review indicate that adolescent participation in research is a complex yet adaptable construct that may be a vital link between obesity prevention research and practice.
Our review detailed the new and emerging field of adolescent participatory research in obesity prevention, with more than 50% of the studies identified having published their first paper in the last 5 years. We found that despite obesity and its associated co-morbidities affecting populations broadly (176), the use of participatory research methods were not equitably deployed. Of the studies which reported socioeconomic characteristics, we found that 85% targeted minority or underserved communities in mostly affluent western nations. Only four studies took place in middle-income nations, where adolescents represent a greater proportion of the total population (177) and where obesity has surpassed undernutrition as a leading cause of morbidity (4). The lack of participatory research for adolescents in LMICs may be attributable to low resources and challenges in health research allocation and implementation. Funders and the global community often expect LMICs to direct research and funds to the most acute public health challenges (178). Furthermore, our finding suggests adolescent participation in obesity prevention research appears to be gender-biased with studies involving predominantly adolescents identifying as female. Adolescents identifying as male were either not represented at all or underrepresented in 55% of the included studies, while “no representation” or underrepresentation of adolescents identifying as female-only occurred in only 11% of studies. This finding may be explained by sociocultural factors and gender-based ideals, particularly in higher-income countries, with females more likely to be concerned with weight compared to their male counterparts (2). Girls are also more likely to partake in disordered eating behaviors and calls for further public health attention (179).
Our review revealed that over the last decade there has been a gradual increase in the awareness of the need to involve adolescents in the dialogue and decision-making processes to make progress on matters affecting youth, such as the global obesity crisis. This finding is consistent with the WHO-UNICEF-Lancet commission report (180), which recommends that youth be placed at the center of Sustainable Development Goals (SDGs). The commission states that “children should be given high-level platforms to share their concerns and ideas and to claim their rights to a healthy future” (180). Insights from our review indicate that meaningful participation not only upholds adolescents' fundamental right to participation but also allows for the development of interventions that are tailored to the unique needs of this demographic.
Results of our review suggest that meaningful adolescent participation is limited within obesity and chronic disease prevention research. Our results indicate that when adolescents are engaged, they are more likely to be involved in the formative stages of the research cycle in activities such as relationship building, needs assessment, research idea development, and project design (34). Nevertheless, only 11% of the included studies reported meaningful participation in all stages of the research cycle. Further, our review determined that to date, participatory research with young people has been predominantly consultative in nature, using methods such as surveys, focus groups, and interviews to elicit views and opinions. At the same time, an adolescent-led mode of participation was described in only 9% of the 71 studies examined. We found that methods that engage adolescents more meaningfully in research such as YAGs, youth advocacy, and peer leadership were a common component of the few adolescent-led participatory studies. Furthermore, studies that involved a youth-led component reported improvements in capacity building markers of empowerment and influence, enhanced confidence, and gave adolescents a voice in research that concerns their lives. The use of YAGs exemplifies a novel (181) yet practical and effective strategy to meaningfully engage adolescents in an adolescent-led approach throughout the entirety of the research cycle (114, 130). Similarly, in a recent scoping review investigating the use of YAGs in health research, Sellars et al. determined that YAGs are a valuable yet underutilized method of involving young people in effective research development and translation globally (34). Moreover, Sellars et al. also found an underutilization of YAGs was more apparent in research conducted in low and middle-income countries (LMICs), where socioeconomic and cultural factors such as lack of resources and age discrimination limited the use of such engagement strategies (34). This finding is consistent with the findings of our review, which found few participatory-focused research studies for adolescent obesity prevention in LMICs.
Findings from our review indicate significant variability in the scope of reported outcomes of meaningful adolescent participation. We found that participatory outcomes are rarely evaluated, and chronic disease outcomes are inconsistently reported. Nevertheless, similarly to Larsson et al. (38), our review provided evidence that increasing adolescent involvement in the advisory, co-design, and decision-making processes contributed to more meaningful obesity and chronic disease prevention associated outcomes. Chronic disease outcomes described within the studies analyzed included increased awareness of obesity, its risk factors and prevention, obesity prevention interventions and program development, environmental modifications to promote healthier lifestyle habits, behavioral changes including diet and physical activity, and improvements in anthropometric measures such as BMI and weight. Furthermore, we identified that meaningful participation contributes to the development of research and leadership skills as well participatory outcomes of empowerment and influence (82, 86). Although participatory outcomes were rarely evaluated in the 71 studies included within this review, there were reports of improved outcomes for the participating youth (97) and their peers (57, 62, 96). Additionally, DeBar et al. reported in their multi-center RCT, that meaningful participation alone (regardless of the amount) was the main factor driving a positive effect on outcomes, with peer-leadership and commitment contributing to a significant improvement in dietary behavior outcomes as well as a reduction in BMI compared to controls (76).
Our review revealed that current research is failing to take into consideration the dynamic context in which adolescents live, participate and the associated social, economic, cultural, political and health policy influences (182). Most included studies in our scoping review (87%) involved adolescent participation within a single socio-ecological setting, namely, local communities and secondary education institutions. However, studies that also included a “peer” context component in the form of YAGs, leadership, advocacy, or peer education were found to be more likely to achieve a wider range of positive chronic disease outcomes. Moreover, findings from our review reinforced that adolescents as individuals live within a complex and intertwined socio-ecological sphere, which often impacts their opportunity for health equity (6, 25). In each context, adolescents experienced barriers and facilitators to their diet and lifestyle choices, and decision-making (183). Engaging adolescents in meaningful obesity prevention research across socio-ecological domains may allow for more efficient identification of risk factors that contribute to global adolescent health inequalities resulting in more dynamic intervention development and implementation (184–186). A study by Livingood et al. provided an exemplar model of how to engage adolescents in meaningful participation in research (114). Youth were engaged in a multi-method adolescent-led approach throughout the entirety of the research cycle. Youth developed and facilitated a youth advisory board and used methods such as photovoice and focus groups to identify needs, concerns and preferences. Youth analyzed and presented their findings, which ultimately led to the development of a digital communication (mHealth) obesity prevention intervention that was tailored to the specific needs of youth. However, although obesity prevention was indicated as an objective of the aforementioned study, chronic disease-related outcomes such as anthropometric measures were not taken and hence it is unclear what impact the development of this youth-led intervention will have on obesity incidence within the community (114).
Despite our best efforts, this scoping review has several limitations and challenges to note. Overall, it was recognized that due to the lack of standardized measures and reporting, measuring and documenting participatory and chronic disease outcomes were predominantly subjective in nature. Furthermore, the term “participation” is routinely used to refer to participants taking part in a study and not necessarily participating in a meaningful way as per participatory frameworks (25). This made it difficult to decipher if meaningful participation was a component of the research processes. Additionally, participatory approaches were often included in methodology sections of reported studies and hence were often not components of the outcomes measured.
Furthermore, scoping reviews have innate limitations of importance to consider. By design scoping reviews are broad in scope and aim to map the literature therefore, the included studies were heterogenous in range of study methodologies and designs. This made direct comparisons between studies challenging. Furthermore, although search terms used were broad and the search strategy was systematic, as with any review, it is possible that some studies were missed. Moreover, studies were limited to those with abstracts published in English; this self-selection limitation may have inadvertently excluded perspectives from non-English speaking countries. Finally, as per the scoping review guidelines, it is not necessary to rate the quality of the data or conduct a critical appraisal of the evidence used in scoping reviews; this may have implications for practice (47).
For research to translate effectively into practice and to address health equity challenges faced by minority and underserved communities, more effort needs to be placed on making participatory research gender-balanced and inclusive. Future research should endeavor to identify why high-risk groups such as males in high and high-middle-income countries are underrepresented in obesity prevention participatory research and work toward facilitating equal representation between genders. Furthermore, future participatory obesity prevention research should aim for a broad representation of young people from different socio-economic backgrounds as well as cultural and social groups. Additionally, funding bodies and researchers should direct attention and resources to the growing adolescent obesity concerns in LMICs, where meaningful adolescent participation in obesity prevention research is remarkably lacking. Also, for participatory research to truly capture the voice and needs of adolescents, it is necessary for researchers to engage young people in an increasingly collaborative or adolescent-led capacity throughout all stages of research and development processes. Researchers should also take into consideration the diverse and dynamic socio-ecological settings in which adolescents and their peers connect. Finally, to adequately measure participatory outcomes and make comparisons between studies we recommend standardized and universal tools to measure participatory outcomes in adolescent obesity-related participatory research.
Findings from our review indicate that adolescents globally are not being engaged sufficiently in obesity prevention research decision-making to uphold the recommendations of the WHO-UNICEF-Lancet commission. The limited number of studies identified from this review that engaged adolescents to a greater capacity within the research process highlights a key opportunity for enhancing obesity prevention research and practice. Meaningful engagement of adolescents in an inclusive and fair manner builds their capacity to contribute throughout the obesity prevention research process. Addressing the unique needs of adolescents requires adolescents to be afforded increased opportunities to collaborate and lead stages of the decision-making, research and translation process.
MM, SM, HC, PP, JR, and SP: conceptualization, methodology, investigation, and writing—review and editing. MM: writing—original draft preparation. JR and SP: supervision. All authors have read and agreed to the published version of the manuscript.
This research was supported by a National Health and Medical Research Council/National Heart Foundation Early Career Fellowship (Grant Number APP1157438) awarded to SP. While JR was funded by a National Health and Medical Research Council Career Development Fellowship (Grant Number APP1143538).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
This research was conducted as part of MM's PhD project and supervised by SP and JR. The authors wish to thank the academic liaison librarians at the University of Sydney, Tess Aiken and Kanchana Ekanayake for their support developing the search strategy.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.789535/full#supplementary-material
Supplementary File 1. Prisma Scoping Review Checklist.
Supplementary Table 1. Medline Search Strategy.
Supplementary Table 2. Data extraction table of included studies.
USA, United States of America; UNICEF, United Nations Children's Fund; NIHR, National Institute for Health Research; NHMRC, National Health and Medical Research Council; PAR, Participatory Action Research; PE, Patient Engagement; CBPR, Community Based Participatory Research; PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews; MeSH, Medical Subject Headings; CINAHL, Cumulative Index of Nursing and Allied Health Literature; CENTRAL, Cochrane Controlled Register of Trials; RCT, Randomized Control Trial; SES, Socioeconomic Status; BMI, Body Mass Index; WHO, World Health Organization; SDGs, Sustainable Development Goals; YAG, Youth Advisory Group; LMICs, Low- and Middle-Income Countries.
1. WHO. Obesity and Overweight: Key Facts. (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed May 05, 2021).
2. Shah B, Tombeau Cost K, Fuller A, Birken CS, Anderson LN. Sex and gender differences in childhood obesity: contributing to the research agenda. BMJ Nutr Prev Health. (2020) 3:387–90. doi: 10.1136/bmjnph-2020-000074
3. WHO. Obesity. (2021). Available online at: https://www.who.int/health-topics/obesity#tab=tab_1 (accessed May 10, 2021).
4. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
5. WHO. Controlling the Global Obesity Epidemic. (2021). Available online at: https://www.who.int/activities/controlling-the-global-obesity-epidemic (accessed July 07, 2021).
6. Kumanyika SK. A framework for increasing equity impact in obesity prevention. Am J Public Health. (2019) 109:1350–7. doi: 10.2105/AJPH.2019.305221
7. WHO. Social Determinants of Health World Health Organization. (2021). Available online at: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed August 10, 2021).
8. Afshin A, Sur PJ, Fay KA, Cornaby L, Ferrara G, Salama JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2019) 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
9. Cheng HL, Medlow S, Steinbeck K. The health consequences of obesity in young adulthood. Curr Obes Rep. (2016) 5:30–7. doi: 10.1007/s13679-016-0190-2
10. McNaughton SA, Ball K, Mishra GD, Crawford DA. Dietary patterns of adolescents and risk of obesity and hypertension. J Nutr. (2008) 138:364–70. doi: 10.1093/jn/138.2.364
11. Karnik S, Kanekar A. Childhood obesity: a global public health crisis. Int J Prev Med. (2012) 3:1–7.
12. Brown T, Moore THM, Hooper L, Gao Y, Zayegh A, Ijaz S, et al. Interventions for preventing obesity in children. Cochrane Datab Syst Rev. (2019) 7:CD001871. doi: 10.1002/14651858.CD001871.pub4
13. Kornet-van der Aa DA, Altenburg TM, van Randeraad-van der Zee CH, Chinapaw MJM. The effectiveness and promising strategies of obesity prevention and treatment programmes among adolescents from disadvantaged backgrounds: a systematic review. Obesity Rev. (2017) 18:581–93. doi: 10.1111/obr.12519
14. Kobes A, Kretschmer T, Timmerman G, Schreuder P. Interventions aimed at preventing and reducing overweight/obesity among children and adolescents: a meta-synthesis. Obesity Rev. (2018) 19:1065–79. doi: 10.1111/obr.12688
15. Puhl R, Suh Y. Health consequences of weight stigma: implications for obesity prevention and treatment. Curr Obes Rep. (2015) 4:182–90. doi: 10.1007/s13679-015-0153-z
16. Holm JC, Nowicka P, Farpour-Lambert NJ, O'Malley G, Hassapidou M, Weiss R, et al. The ethics of childhood obesity treatment - from the childhood obesity task force (COTF) of European Association for the Study of Obesity (EASO). Obes Facts. (2014) 7:274–81. doi: 10.1159/000365773
17. Russell-Mayhew S, McVey G, Bardick A, Ireland A. Mental health, wellness, and childhood overweight/obesity. J Obes. (2012) 2012:281801. doi: 10.1155/2012/281801
18. Perryman ML, Sidoti KA. Ethical considerations in the treatment of childhood obesity. Medicol Bioeth. (2015) 5:17–26. doi: 10.2147/MB.S63710
19. Jebeile H, Cardel MI, Kyle TK, Jastreboff AM. Addressing psychosocial health in the treatment and care of adolescents with obesity. Obesity. (2021) 29:1413–22. doi: 10.1002/oby.23194
20. Hoare E, Fuller-Tyszkiewicz M, Skouteris H, Millar L, Nichols M, Allender S. Systematic review of mental health and well-being outcomes following community-based obesity prevention interventions among adolescents. BMJ Open. (2015) 5:e006586. doi: 10.1136/bmjopen-2014-006586
21. Puhl RM, Heuer CA. Obesity stigma: important considerations for public health. Am J Public Health. (2010) 100:1019–28. doi: 10.2105/AJPH.2009.159491
22. Thomas H. Obesity prevention programs for children and youth: why are their results so modest? Health Educ Res. (2006) 21:783–95. doi: 10.1093/her/cyl143
23. Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. (2016) 387:2423–78. doi: 10.1016/S0140-6736(16)00579-1
24. UNICEF. Convention on the Rights of the Child. New York, NY: UN general assembly New York City: The United Nations Population Fund (1989).
25. Lansdown G. Conceptual Framework for Measuring Outcomes of Adolescent Participation. New York, NY: UNICEF (2018).
28. Shier H. Pathways to participation: Openings, opportunities and obligations. Children & society. (2001) 15:107–17. doi: 10.1002/chi.617
30. INVOLVE. Involving Children and Young People in Research: Top Tips and Essential Key Issues for Researchers. Southampton: INVOLVE (2019).
31. NHMRC. Expectations and Value- Framework for Effective Consumer and Community Engagement in Research. Canberra: NHMRC (2019).
32. Anyon Y, Bender K, Kennedy H, Dechants J. A systematic review of youth participatory action research (YPAR) in the United States: methodologies, youth outcomes, and future directions. Health Educ Behav. (2018) 45:865–78. doi: 10.1177/1090198118769357
33. Shamrova DP, Cummings CE. Participatory action research (PAR) with children and youth: An integrative review of methodology and PAR outcomes for participants, organizations, and communities. Child Youth Serv Rev. (2017) 81:400–12. doi: 10.1016/j.childyouth.2017.08.022
34. Sellars E, Pavarini G, Michelson D, Creswell C, Fazel M. Young people's advisory groups in health research: scoping review and mapping of practices. Arch Dis Child. (2020) 106, 698–704. doi: 10.1136/archdischild-2020-320452
35. Flynn R, Walton S, Scott SD. Engaging children and families in pediatric Health Research: a scoping review. Res Invol Engag. (2019) 5:32. doi: 10.1186/s40900-019-0168-9
36. Jacquez F, Vaughn LM, Wagner E. Youth as partners, participants or passive recipients: a review of children and adolescents in community-based participatory research (CBPR). Am J Community Psychol. (2013) 51:176–89. doi: 10.1007/s10464-012-9533-7
37. Vaughn LM, Wagner E, Jacquez F. A review of community-based participatory research in child health. MCN Am J Matern Child Nurs. (2013) 38:48–53. doi: 10.1097/NMC.0b013e31826591a3
38. Larsson I, Staland-Nyman C, Svedberg P, Nygren JM, Carlsson IM. Children and young people's participation in developing interventions in health and well-being: a scoping review. BMC Health Serv Res. (2018) 18:507. doi: 10.1186/s12913-018-3219-2
39. Njelesani J, Hunleth J. Youth participatory research evidence to inform health policy: a systematic review protocol. BMJ Open. (2020) 10:e036522. doi: 10.1136/bmjopen-2019-036522
40. Hawke LD, Relihan J, Miller J, McCann E, Rong J, Darnay K, et al. Engaging youth in research planning, design and execution: Practical recommendations for researchers. Health Expect. (2018) 21:944–9. doi: 10.1111/hex.12795
41. Hawke LD, Darnay K, Relihan J, Khaleghi-Moghaddam M, Barbic S, Lachance L, et al. Enhancing researcher capacity to engage youth in research: researchers' engagement experiences, barriers and capacity development priorities. Health Expect. (2020) 23:584–92. doi: 10.1111/hex.13032
42. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
43. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
44. Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:69. doi: 10.1186/1748-5908-5-69
45. JBI. The JBI Reviewer's Manual: Joanna Briggs Institute. (2019). Available online at: https://wiki.joannabriggs.org/display/MANUAL/11.2.3$+$Introduction (accessed April 03, 2021).
46. Peters M, Godfrey C, Khalil H, McInerney P, Soares C, Parker D. Guidance for the Conduct of JBI Scoping Reviews. Adelaide: JBI (2017).
47. Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping Reviews (2020 version). JBI Manual for Evidence Synthesis. (2020). Available online at: https://synthesismanual.jbi.global (accessed April 10, 2021). doi: 10.46658/JBIMES-20-12
48. Andrea C, Tricco EL, Wasifa Zarin, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018). 169:467–73. doi: 10.7326/M18-0850
49. Mandoh M, Mihrshahi S, Cheng HL, Redfern J, Partridge SR. Adolescent participation in research, policies and guidelines for chronic disease prevention: a scoping review protocol. Int J Environ Res Public Health. (2020) 17:8257. doi: 10.3390/ijerph17218257
50. WHO. Health for the World's Adolescents: A Second Chance in the Second Decade. World Health Organization (2014). Available online at: https://www.who.int/maternal_child_adolescent/documents/second-decade/en/ (accessed July 08, 2021).
51. Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health. (2018) 2:223–8. doi: 10.1016/S2352-4642(18)30022-1
52. Aceves-Martins M, Llauradó E, Tarro L, Moriña D, Papell-Garcia I, Prades-Tena J, et al. A school-based, peer-led, social marketing intervention to engage Spanish adolescents in a healthy lifestyle (“we are cool”–Som la Pera Study): a parallel-cluster randomized controlled study. Childhood Obesity. (2017) 13:300–13. doi: 10.1089/chi.2016.0216
53. Anselma M, Altenburg T, Chinapaw M. Kids in action: the protocol of a youth participatory action research project to promote physical activity and dietary behaviour. BMJ Open. (2019) 9:e025584. doi: 10.1136/bmjopen-2018-025584
54. Anselma M, Altenburg TM, Emke H, van Nassau F, Jurg M, Ruiter RAC, et al. Co-designing obesity prevention interventions together with children: intervention mapping meets youth-led participatory action research. Int J Behav Nutr Phys Act. (2019) 16:130. doi: 10.1186/s12966-019-0891-5
55. Anselma M, Chinapaw M, Altenburg T. “Not only adults can make good decisions, we as children can do that as well” evaluating the process of the youth-led participatory action research ‘kids in action’. Int J Environ Res Public Health. (2020) 17:625. doi: 10.3390/ijerph17020625
56. Anselma M, Chinapaw MJM, Altenburg TM. Determinants of child health behaviors in a disadvantaged area from a community perspective: a participatory needs assessment. Int J Environ Res Public Health Electronic Resource. (2018) 15:31. doi: 10.3390/ijerph15040644
57. Arlinghaus KR, Moreno JP, Reesor L, Hernandez DC, Johnston CA. Companeros: high school students mentor middle school students to address obesity among hispanic adolescents. Prev Chronic Dis. (2017) 14:E92. doi: 10.5888/pcd14.170130
58. Bailey J, Davies C, McCrossin T, Kiernan M, Skinner R, Steinbeck K, et al. Fit4YAMs: Structuring a lifestyle intervention for rural overweight and obese young adult males using participatory design. J Adolesc Health. (2018) 62:S65–71. doi: 10.1016/j.jadohealth.2017.06.019
59. Balvanz P, Dodgen L, Quinn J, Holloway T, Hudspeth S, Eng E. From voice to choice: african american youth examine childhood obesity in rural North Carolina. Prog Commun Health Partner. (2016) 10:293–303. doi: 10.1353/cpr.2016.0036
60. Bardwell G, Morton C, Chester A, Pancoska P, Buch S, Cecchetti A, et al. Feasibility of adolescents to conduct community-based participatory research on obesity and diabetes in rural Appalachia. Clin Transl Sci. (2009) 2:340–9. doi: 10.1111/j.1752-8062.2009.00155.x
61. Bindler RC, Goetz S, Butkus SN, Power TG, Ullrich-French S, Steele M. The process of curriculum development and implementation for an adolescent health project in middle schools. J Sch Nurs. (2011) 28:13–23. doi: 10.1177/1059840511424414
62. Bogart LM, Cowgill BO, Elliott MN, Klein DJ, Hawes-Dawson J, Uyeda K, et al. A randomized controlled trial of Students for Nutrition and exercise: a community-based participatory research study. J Adolesc Health. (2014) 55:415–22. doi: 10.1016/j.jadohealth.2014.03.003
63. Bogart LM, Elliott MN, Cowgill BO, Klein DJ, Hawes-Dawson J, Uyeda K, et al. Two-year BMI outcomes from a school-based intervention for nutrition and exercise: a randomized trial. Pediatrics. (2016) 137:2493. doi: 10.1542/peds.2015-2493
64. Bogart LM, Elliott MN, Uyeda K, Hawes-Dawson J, Klein DJ, Schuster MA. Preliminary healthy eating outcomes of SNaX, a pilot community-based intervention for adolescents. J Adolesc Health. (2011) 48:196–202. doi: 10.1016/j.jadohealth.2010.06.004
65. Bogart LM, Fu CM, Eyraud J, Cowgill BO, Hawes-Dawson J, Uyeda K, et al. Evaluation of the dissemination of SNaX, a middle school-based obesity prevention intervention, within a large US school district. Transl Behav Med. (2018) 8:724–32. doi: 10.1093/tbm/ibx055
66. Briançon Briançon S, Bonsergent E, Agrinier N, Tessier S, Legrand K, Lecomte E, et al. PRALIMAP: study protocol for a high school-based, factorial cluster randomised interventional trial of three overweight and obesity prevention strategies. Trials. (2010) 11:119. doi: 10.1186/1745-6215-11-119
67. Brown B, Noonan C, Harris KJ, Parker M, Gaskill S, Ricci C, et al. Developing and piloting the journey to native youth health program in northern plains Indian communities. Diabetes Educ. (2013) 39:109–18. doi: 10.1177/0145721712465343
68. Brown BD, Harris KJ, Harris JL, Parker M, Ricci C, Noonan C. Translating the diabetes prevention program for northern plains Indian youth through community-based participatory research methods. Diab Educ. (2010) 36:924–35. doi: 10.1177/0145721710382582
69. Cassidy O, Sbrocco T, Vannucci A, Nelson B, Jackson-Bowen D, Heimdal J, et al. Adapting interpersonal psychotherapy for the prevention of excessive weight gain in rural African American girls. J Pediatr Psychol. (2013) 38:965–77. doi: 10.1093/jpepsy/jst029
70. Chae SM, Yeo JY, Hwang JH, Lee JH, Lim J, Kwon I. Weight control in adolescents: focus groups with korean adolescents and their teachers. J Pediatr Nurs. (2017) 33:4–9. doi: 10.1016/j.pedn.2016.12.003
71. Christianson J, Kattelmann K, Riggsbee K, Moret L, Vilaro MJ, Olfert MD, et al. Promoting wellness on college campuses: identifying and addressing the wellness needs of college students. Top Clin Nutr. (2019) 34:125–37. doi: 10.1097/TIN.0000000000000169
72. Correa N, Rajaraman D, Swaminathan S, Vaz M, Jayachitra KG, Lear SA, et al. Perceptions of healthy eating amongst Indian adolescents in India and Canada. Appetite. (2017) 116:471–9. doi: 10.1016/j.appet.2017.05.029
73. Cueva K, Speakman K, Neault N, Richards J, Lovato V, Parker S, et al. Cultural connectedness as obesity prevention: indigenous youth perspectives on feast for the future. J Nutr Educ Behav. (2020). 52:632–9. doi: 10.1016/j.jneb.2019.11.009
74. Cullen KW, Thompson D, Boushey C, Konzelmann K, Chen TA. Evaluation of a web-based program promoting healthy eating and physical activity for adolescents: teen choice: food and fitness. Health Educ Res. (2013) 28:704–14. doi: 10.1093/her/cyt059
75. de Vet E, de Wit JB, Luszczynska A, Stok FM, Gaspar T, Pratt M, et al. Access to excess: how do adolescents deal with unhealthy foods in their environment? Eur J Public Health. (2013) 23:752–6. doi: 10.1093/eurpub/cks185
76. Debar LL, Schneider M, Drews KL, Ford EG, Stadler DD, Moe EL, et al. Student public commitment in a school-based diabetes prevention project: impact on physical health and health behavior. BMC Public Health. (2011) 11:711. doi: 10.1186/1471-2458-11-711
77. DeBar LL, Schneider M, Ford EG, Hernandez AE, Showell B, Drews KL, et al. Social marketing-based communications to integrate and support the HEALTHY study intervention. (2005). (2009) 33(Suppl. 4):S52–9. doi: 10.1038/ijo.2009.117
78. Dennisuk LA, Coutinho AJ, Suratkar S, Surkan PJ, Christiansen K, Riley M, et al. Food expenditures and food purchasing among low-income, Urban, African-American Youth. Am J Prev Med. (2011) 40:625–8. doi: 10.1016/j.amepre.2011.02.015
79. Diez-Canseco F, Boeren Y, Quispe R, Chiang ML, Miranda JJ. Engagement of adolescents in a health communications program to prevent noncommunicable diseases: multiplicadores Jovenes, Lima, Peru 2011. Prev Chronic Dis. (2015) 12:E28. doi: 10.5888/pcd12.140416
80. Edwardson CL, Harrington DM, Yates T, Bodicoat DH, Khunti K, Gorely T, et al. A cluster randomized controlled trial to investigate the effectiveness and cost effectiveness of the ‘Girls Active’ intervention: a study protocol. BMC Public Health. (2015) 15:526. doi: 10.1186/s12889-015-1886-z
81. Ewan L, McLinden D, Biro F, DeJonckheere M, Vaughn L. Mapping the views of adolescent health stakeholders. J Adolesc Health. (2015) 56:S68–S9. doi: 10.1016/j.jadohealth.2014.10.137
82. Findholt NE, Michael YL, Davis MM. Photovoice engages rural youth in childhood obesity prevention. Public Health Nurs. (2011) 28:186–92. doi: 10.1111/j.1525-1446.2010.00895.x
83. Foley BC, Shrewsbury VA, Hardy LL, Flood VM, Byth K, Shah S. Evaluation of a peer education program on student leaders' energy balance-related behaviors. BMC Public Health. (2017) 17:695. doi: 10.1186/s12889-017-4707-8
84. Fotu KF, Moodie MM, Mavoa HM, Pomana S, Schultz JT, Swinburn BA. Process evaluation of a community-based adolescent obesity prevention project in Tonga. BMC Public Health. (2011) 11:284. doi: 10.1186/1471-2458-11-284
85. Frerichs L, Brittin J, Robbins R, Steenson S, Stewart C, Fisher C, et al. SaludABLEOmaha: improving readiness to address obesity through healthy lifestyle in a Midwestern Latino Community, 2011-2013. Prevent Chronic Dis. (2015) 12:328. doi: 10.5888/pcd12.140328
86. Frerichs L, Brittin J, Stewart C, Robbins R, Riggs C, Mayberger S, et al. SaludableOmaha: development of a youth advocacy initiative to increase community readiness for obesity prevention, 2011-2012. Prev Chronic Dis. (2012) 9:E173. doi: 10.5888/pcd9.120095
87. Frerichs L, Hassmiller Lich K, Young TL, Dave G, Stith D, Corbie-Smith G. Development of a systems science curriculum to engage rural African American teens in understanding and addressing childhood obesity prevention. Health Educ Behav. (2018) 45:423–34. doi: 10.1177/1090198117726570
88. Garcia ML, Gatdula N, Bonilla E, Frank GC, Bird M, Rascon MS, et al. Engaging intergenerational hispanics/latinos to examine factors influencing childhood obesity using the PRECEDE-PROCEED Model. Matern Child Health J. (2019) 23:802–10. doi: 10.1007/s10995-018-02696-y
89. Garnett BR, Wendel J, Banks C, Goodridge A, Harding R, Harris R, et al. Challenges of data dissemination efforts within a community-based participatory project about persistent racial disparities in excess weight. Prog Commun Health Partner. (2015) 9:289–98. doi: 10.1353/cpr.2015.0047
90. Gittelsohn J, Anderson Steeves E, Mui Y, Kharmats AY, Hopkins LC, Dennis D. B'More healthy communities for kids: design of a multi-level intervention for obesity prevention for low-income African American children. BMC Public Health. (2014) 14:942. doi: 10.1186/1471-2458-14-942
91. Gittelsohn J, Dennisuk LA, Christiansen K, Bhimani R, Johnson A, Alexander E, et al. Development and implementation of Baltimore Healthy Eating Zones: a youth-targeted intervention to improve the urban food environment. Health Educ Res. (2013) 28:732–44. doi: 10.1093/her/cyt066
92. Goh Y, Bogart LM, Sipple-Asher BK, Uyeda K, Hawes-Dawson J, Olarita-Dhungana J, et al. Using community-based participatory research to identify potential interventions to overcome barriers to adolescents' healthy eating and physical activity. J Behav Med. (2009) 32:491–502. doi: 10.1007/s10865-009-9220-9
93. Green B, Ralston PA, Young-Clark I, Waryoba C, Smith S, Harris CM, et al. A youth health leadership program: feasibility and initial outcomes. J Commun Health. (2020) 45:228–38. doi: 10.1007/s10900-019-00707-9
94. Grignard S, Bourguignon JP, Born M, Mairiaux P, Vandoorne C. Characteristics of adolescent attempts to manage overweight. Patient Educ Counsel. (2003) 51:183–9. doi: 10.1016/S0738-3991(02)00217-3
95. Group HS, Hirst K, Baranowski T, DeBar L, Foster GD, Kaufman F, et al. HEALTHY study rationale, design and methods: moderating risk of type 2 diabetes in multi-ethnic middle school students. Int J Obesity. (2009) 33(Suppl. 4):S4–20. doi: 10.1038/ijo.2009.112
96. Hagedorn RL, White JA, Franzen-Castle L, Colby SE, Kattelmann KK, White AA, et al. Teens implementing a childhood obesity prevention program in the community: feasibility and perceptions of a partnership with HSTA and iCook 4-H. Inter J Environ Res Public Health Electronic Resource. (2018) 15:07. doi: 10.3390/ijerph15050934
97. Hannay J, Dudley R, Milan S, Leibovitz PK. Combining photovoice and focus groups: engaging latina teens in community assessment. Am J Prevent Med. (2013) 44(Suppl. 3):S215–24. doi: 10.1016/j.amepre.2012.11.011
98. Harrington DM, Davies MJ, Bodicoat DH, Charles JM, Chudasama YV, Gorely T, et al. Effectiveness of the ‘Girls Active’ school-based physical activity programme: A cluster randomized controlled trial. Int J Behav Nutr Phys Act. (2018) 15:40. doi: 10.1186/s12966-018-0664-6
99. Hunsberger M, McGinnis P, Smith J, Beamer BA, O'Malley J. Calorie labeling in a rural middle school influences food selection: findings from community-based participatory research. J Obes. (2015) 2015:531690. doi: 10.1155/2015/531690
100. Jackson CJ, Mullis RM, Hughes M. Development of a theater-based nutrition and physical activity intervention for low-income, urban, African American adolescents. Prog Community Health Partnersh. (2010) 4:89–98. doi: 10.1353/cpr.0.0115
101. Kattelmann KK, Bredbenner CB, White AA, Greene GW, Hoerr SL, Kidd T, et al. The effects of young adults eating and active for health (YEAH): a theory-based web-delivered intervention. J Nutr Educ Behav. (2014) 46:S27–41. doi: 10.1016/j.jneb.2014.08.007
102. Kattelmann KK, White AA, Greene GW, Byrd-Bredbenner C, Hoerr SL, Horacek TM, et al. Development of young adults eating and active for health (YEAH) internet-based intervention via a community-based participatory research model. J Nutr Educ Behav. (2014) 46:S10–25. doi: 10.1016/j.jneb.2013.11.006
103. Knoblock-Hahn AL, Wray R, LeRouge CM. Perceptions of adolescents with overweight and obesity for the development of user-centered design self-management tools within the context of the chronic care model: a qualitative study. J Acad Nutr Dietet. (2016) 116:957–67. doi: 10.1016/j.jand.2015.08.022
104. Kong AS, Farnsworth S, Canaca JA, Harris A, Palley G, Sussman AL. An adaptive community-based participatory approach to formative assessment with high schools for obesity intervention. J Sch Health. (2012) 82:147–54. doi: 10.1111/j.1746-1561.2011.00678.x
105. Kramer L, Schwartz P, Cheadle A, Borton JE, Wright M, Chase C, et al. Promoting policy and environmental change using photovoice in the kaiser permanente community health initiative. Health Promot Pract. (2010) 11:332–9. doi: 10.1177/1524839909341555
106. Kramer L, Schwartz P, Cheadle A, Rauzon S. Using photovoice as a participatory evaluation tool in Kaiser Permanente's community health initiative. Health Promot Pract. (2013) 14:686–94. doi: 10.1177/1524839912463232
107. Lane HG, Driessen R, Campbell K, Deitch R, Turner L, Parker EA, et al. Development of the PEA-PODS (perceptions of the environment and patterns of diet at school) survey for students. Prevent Chronic Dis. (2018) 15:561. doi: 10.5888/pcd15.170561
108. Lane HG, Porter KJ, Hecht E, Harris P, Zoellner JM. A participatory process to engage appalachian youth in reducing sugar-sweetened beverage consumption. Health Promot Pract. (2019) 20:258–68. doi: 10.1177/1524839918762123
109. Lems E, Hilverda F, Broerse JEW, Dedding C. ‘Just stuff yourself’: Identifying health-promotion strategies from the perspectives of adolescent boys from disadvantaged neighbourhoods. Health Expect. (2019) 22:1040–9. doi: 10.1111/hex.12913
110. LeRouge C, Durneva P, Sangameswaran S, Gloster A-M. Design guidelines for a technology-enabled nutrition education program to support overweight and obese adolescents: qualitative user-centered design study. J Med Inter Res. (2019) 21:e14430. doi: 10.2196/14430
111. LeRouge CM, Hah H, Deckard GJ, Jiang H. Designing for the co-use of consumer health technology in self-management of adolescent overweight and obesity: mixed methods qualitative study. JMIR Mhealth Uhealth. (2020) 8:e18391. doi: 10.2196/18391
112. Lewis RK, Lee FA, Brown KK, LoCurto J, Stowell D, Maryman J, et al. Youth empowerment implementation project evaluation results: a program designed to improve the health and well-being of low-income African-American adolescents. J Prev Interv Community. (2018) 46:28–42. doi: 10.1080/10852352.2018.1385954
113. Linton LS, Edwards CC, Woodruff SI, Millstein EA, Moder C. Youth advocacy as a tool for environmental and policy changes that support physical activity and nutrition: an evaluation study in San Diego County. Prevent Chronic Dis. (2014) 11:321. doi: 10.5888/pcd11.130321
114. Livingood WC, Monticalvo D, Bernhardt JM, Wells KT, Harris T, Kee K, et al. Engaging adolescents through participatory and qualitative research methods to develop a digital communication intervention to reduce adolescent obesity. Health Educ Behav. (2017) 44:570–80. doi: 10.1177/1090198116677216
115. Llaurado E, Aceves-Martins M, Tarro L, Papell-Garcia I, Puiggros F, Arola L, et al. A youth-led social marketing intervention to encourage healthy lifestyles, the EYTO (European Youth Tackling Obesity) project: a cluster randomized controlled trial in Catalonia, Spain. BMC Public Health. (2015) 15, 607–619. doi: 10.1186/s12889-015-1920-1
116. Llauradó E, Aceves-Martins M, Tarro L, Papell-Garcia I, Puiggròs F, Prades-Tena J, et al. The “Som la Pera” intervention: sustainability capacity evaluation of a peer-led social-marketing intervention to encourage healthy lifestyles among adolescents. Transl Behav Med. (2018) 8:739–44. doi: 10.1093/tbm/ibx065
117. Loman DG. Promoting physical activity in teen girls: insight from focus groups. Mcn. Am J Maternal Child Nurs. 33:294–9; quiz 300-1 (2008). doi: 10.1097/01.NMC.0000334896.91720.86
118. Marcus MD, Hirst K, Kaufman F, Foster GD, Baranowski T. Lessons learned from the HEALTHY primary prevention trial of risk factors for type 2 diabetes in middle school youth. Curr Diab Rep. (2013) 13:63–71. doi: 10.1007/s11892-012-0333-0
119. Martin Romero MY, Francis LA. Youth involvement in food preparation practices at home: A multi-method exploration of Latinx youth experiences and perspectives. Appetite. (2020) 144:104439. doi: 10.1016/j.appet.2019.104439
120. Mathews LB, Moodie MM, Simmons AM, Swinburn BA. The process evaluation of It's Your Move!, an Australian adolescent community-based obesity prevention project. BMC Public Health. (2010) 10:448. doi: 10.1186/1471-2458-10-448
121. Mauriello LM, Ciavatta MMH, Paiva AL, Sherman KJ, Castle PH, Johnson JL, et al. Results of a multi-media multiple behavior obesity prevention program for adolescents. Prevent Med. (2010) 51:451–6. doi: 10.1016/j.ypmed.2010.08.004
122. Mauriello LM, Driskell MM, Sherman KJ, Johnson SS, Prochaska JM, Prochaska JO. Acceptability of a school-based intervention for the prevention of adolescent obesity. J Sch Nurs. (2006) 22:269–77. doi: 10.1177/10598405060220050501
123. Maynard M, Baker G, Harding S. Exploring childhood obesity prevention among diverse ethnic groups in schools and places of worship: Recruitment, acceptability and feasibility of data collection and intervention components. Prevent Med Rep. (2017) 6:130–6. doi: 10.1016/j.pmedr.2017.02.019
124. Maynard MJ, Baker G, Rawlins E, Anderson A, Harding S. Developing obesity prevention interventions among minority ethnic children in schools and places of worship: The DEAL (DiEt and Active Living) study. BMC Public Health. (2009) 9:480. doi: 10.1186/1471-2458-9-480
125. McGee BB, Richardson V, Johnson G, Johnson C. Perceptions of food intake, physical activity, and obesity among African-American children in the lower mississippi delta. Am J Health Promot. (2017) 31:333–5. doi: 10.4278/ajhp.130611-ARB-296
126. McKinney C, Bishop V, Cabrera K, Medina R, Takawira D, Donate N, et al. NuFit: nutrition and fitness CBPR program evaluation. J Prev Interv Community. (2014) 42:112–24. doi: 10.1080/10852352.2014.881180
127. McPherson AC, Lindsay S. How do children with disabilities view ‘healthy living’? A descriptive pilot study. Disabil Health J. (2012) 5:201–9. doi: 10.1016/j.dhjo.2012.04.004
128. Millar L, Kremer P, de Silva-Sanigorski A, McCabe MP, Mavoa H, Moodie M, et al. Reduction in overweight and obesity from a 3-year community-based intervention in Australia: the ‘It's Your Move!’ project. Obes Rev. (2011) 12(Suppl. 2):20–8. doi: 10.1111/j.1467-789X.2011.00904.x
129. Millstein RA, Woodruff SI, Linton LS, Edwards CC, Sallis JF. Development of measures to evaluate youth advocacy for obesity prevention. Int J Behavioral Nutr Phys Activity. (2016) 13:84. doi: 10.1186/s12966-016-0410-x
130. Morales-Campos DY, Parra-Medina D, Esparza LA. Picture this!: using participatory photo mapping with Hispanic girls. Fam Community Health. (2015) 38:44–54. doi: 10.1097/FCH.0000000000000059
131. Mosavel M, Gough MZ, Ferrell D. Using asset mapping to engage youth in community-based participatory research: the WE project. Prog Commun Health Partner. (2018) 12:223–36. doi: 10.1353/cpr.2018.0042
132. Muturi N, Kidd T, Daniels AM, Kattelmann KK, Khan T, Lindshield E, et al. Examining the role of youth empowerment in preventing adolescence obesity in low-income communities. J Adolesc. (2018) 68:242–51. doi: 10.1016/j.adolescence.2018.08.001
133. Necheles JW, Chung EQ, Hawes-Dawson J, Ryan GW, Williams SB, Holmes HN, et al. The Teen photovoice project: a pilot study to promote health through advocacy. Prog Commun Health Partner. (2007) 1:221–9. doi: 10.1353/cpr.2007.0027
134. Nguyen NM, Dibley MJ, Tang HK, Alam A. Perceptions and practices related to obesity in adolescent students and their programmatic implications: qualitative evidence from Ho Chi Minh City, Vietnam. Matern Child Health J. (2017) 21:2199–208. doi: 10.1007/s10995-017-2340-x
135. Partridge SR, Raeside R, Latham Z, Singleton AC, Hyun K, Grunseit A, et al. Not to be harsh but try less to relate to ‘the teens and you'll relate to them more’: Co-designing obesity prevention text messages with adolescents. Int J Environ Res Public Health. (2019) 16:887. doi: 10.3390/ijerph16244887
136. Partridge SR, Raeside R, Singleton AC, Hyun K, Latham Z, Grunseit A, et al. Text message behavioral intervention for teens on eating, physical activity and social wellbeing (TEXTBITES): protocol for a randomized controlled trial. JMIR Res Protoc. (2020) 9:e16481. doi: 10.2196/16481
137. Perry C, Hoffman B. Assessing tribal youth physical activity and programming using a community-based participatory research approach. Public Health Nurs. (2010) 27:104–14. doi: 10.1111/j.1525-1446.2010.00833.x
138. Power TG, Bindler RC, Goetz S, Daratha KB. Obesity prevention in early adolescence: Student, parent, and teacher views. J Sch Health. (2010) 80:13–9. doi: 10.1111/j.1746-1561.2009.00461.x
139. Rajaraman D, Correa N, Punthakee Z, Lear SA, Jayachitra KG, Vaz M, et al. Perceived benefits, facilitators, disadvantages, and barriers for physical activity amongst south asian adolescents in India and Canada. J Phys Act Health. (2015) 12:931. doi: 10.1123/jpah.2014-0049
140. Rawlins E, Baker G, Maynard M, Harding S. Perceptions of healthy eating and physical activity in an ethnically diverse sample of young children and their parents: the DEAL prevention of obesity study. J Hum Nutr Diet. (2013) 26:132–44. doi: 10.1111/j.1365-277X.2012.01280.x
141. Renzaho AM, Halliday JA, Mellor D, Green J. The healthy migrant families initiative: development of a culturally competent obesity prevention intervention for African migrants. BMC Public Health. (2015) 15:272. doi: 10.1186/s12889-015-1628-2
142. Robbins LB, Gretebeck KA, Kazanis AS, Pender NJ. Girls on the move program to increase physical activity participation. Nurs Res. (2006) 55:206–16. doi: 10.1097/00006199-200605000-00007
143. Robbins LB, Pender NJ, Kazanis AS. Barriers to physical activity perceived by adolescent girls. J Midwifery Womens Health. (2003) 48:206–12. doi: 10.1016/S1526-9523(03)00054-0
144. Ruggiero CF, Poirier L, Trude ACB, Yang T, Schwendler T, Gunen B, et al. Implementation of B'More Healthy Communities for Kids: process evaluation of a multi-level, multi-component obesity prevention intervention. Health Educ Res. (2018) 33:458–72. doi: 10.1093/her/cyy031
145. Saez L, Legrand K, Alleyrat C, Ramisasoa S, Langlois J, Muller L, et al. Using facilitator-receiver peer dyads matched according to socioeconomic status to promote behaviour change in overweight adolescents: a feasibility study. BMJ Open. (2018) 8:e019731. doi: 10.1136/bmjopen-2017-019731
146. Sato PM, Steeves EA, Carnell S, Cheskin LJ, Trude AC, Shipley C, et al. A youth mentor-led nutritional intervention in urban recreation centers: a promising strategy for childhood obesity prevention in low-income neighborhoods. Health Educ Res. (2016) 31:195–206. doi: 10.1093/her/cyw011
147. Schultz J, Utter J, Mathews L, Cama T, Mavoa H, Swinburn B. The pacific OPIC project (obesity prevention in communities): action plans and interventions. Pac Health Dialog. (2007) 14:147–53.
148. Schwarte L, Samuels SE, Capitman J, Ruwe M, Boyle M, Flores G. The central California regional obesity prevention program: changing nutrition and physical activity environments in California's heartland. Am J Public Health. (2010) 100:2124–8. doi: 10.2105/AJPH.2010.203588
149. Shah S, Foley BC, Molinari I, Lim KS, Shrewsbury VA. The students as lifestyle activists (SALSA) program. Br J Sports Med. (2017) 51:1445–6. doi: 10.1136/bjsports-2016-097219
150. Shah S, Patching van der Sluijs C, Lagleva M, Pesle A, Lim KS, Bittar H, et al. A partnership for health - working with schools to promote healthy lifestyle. Aust Fam Physician. (2011) 40:1011–3.
151. Shepherd LM, Neumark-Sztainer D, Beyer KM, Story M. Should we discuss weight and calories in adolescent obesity prevention and weight-management programs? Perspectives of adolescent girls. J Am Dietetic Assoc. (2006) 106:1454–8. doi: 10.1016/j.jada.2006.06.012
152. Sherman J, Macdonald ME, Carnevale F, Vignola S. The development and implementation of a type 2 diabetes prevention program for youth in the Algonquin community of Rapid Lake, Quebec. Pimatisiwin. J Aborig Indigenous Commun Health. (2011) 9:219–44.
153. Shin A, Surkan PJ, Coutinho AJ, Suratkar SR, Campbell RK, Rowan M, et al. Impact of Baltimore healthy eating zones: an environmental intervention to improve diet among African American Youth. Health Educ Behav. (2015) 42:97S−105S. doi: 10.1177/1090198115571362
154. Siega-Riz AM, El Ghormli L, Mobley C, Gillis B, Stadler D, Hartstein J, et al. The effects of the HEALTHY study intervention on middle school student dietary intakes. Int J Behav Nutr Phys Activity. (2011) 8:7. doi: 10.1186/1479-5868-8-7
155. Spaulding CJ, McNeal CJ, Coppin JD, Shimek C, Field L, Murano PS. Engaging inner city middle school students in development of an energy expenditure food label. J Prev Interv Community. (2015) 43:123–34. doi: 10.1080/10852352.2014.973272
156. Steele MM, Daratha KB, Bindler RC, Power TG. The relationship between self-efficacy for behaviors that promote healthy weight and clinical indicators of adiposity in a sample of early adolescents. Health Educ Behav. (2011) 38:596–602. doi: 10.1177/1090198110387514
157. Surkan PJ, Coutinho AJ, Christiansen K, Dennisuk LA, Suratkar S, Mead E, et al. Healthy food purchasing among African American youth: associations with child gender, adult caregiver characteristics and the home food environment. Public Health Nutr. (2011) 14:670–7. doi: 10.1017/S136898001000251X
158. Sussman AL, Montoya C, Werder O, Davis S, Wallerstein N, Kong AS. An adaptive CBPR approach to create weight management materials for a school-based health center intervention. J Obesity. (2013) 2013:978482. doi: 10.1155/2013/978482
159. Swanson M, Schoenberg NE, Davis R, Wright S, Dollarhide K. Perceptions of healthful eating and influences on the food choices of Appalachian Youth. J Nutr Educ Behav. (2013) 45:147–53. doi: 10.1016/j.jneb.2011.07.006
160. Swinburn B, Pryor J, McCabe M, Carter R, de Courten M, Schaaf D, et al. The pacific OPIC project (obesity prevention in communities) – objectives and designs. Pac Health Dialog. (2007) 14:139–46.
161. Swinburn BA, Millar L, Utter J, Kremer P, Moodie M, Mavoa H, et al. The pacific obesity prevention in communities project: project overview and methods. Obes Rev. (2011) 12(Suppl. 2):3–11. doi: 10.1111/j.1467-789X.2011.00921.x
162. Tang HK, Nguyen N-M, Dibley MJ, Nguyen THHD, Alam A. Improving the lifestyle of adolescents through peer education and support in vietnam: protocol for a pilot cluster randomized controlled trial. JMIR Res Protoc. (2020) 9:e15930. doi: 10.2196/15930
163. Tarro L, Aceves-Martins M, Papell-Garcia I, Arola L, Giralt M, Llauradó E, et al. A youth-led, social marketing intervention run by adolescents to encourage healthy lifestyles among younger school peers (EYTO-Kids Project): a protocol for pilot cluster randomized controlled trial (Spain). Int J Environ Res Public Health. (2017) 14:923. doi: 10.3390/ijerph14080923
164. Tarro L, Llauradó E, Aceves-Martins M, Moriña D, Papell-Garcia I, Arola L, et al. Impact of a youth-led social marketing intervention run by adolescents to encourage healthy lifestyles among younger school peers (EYTO-Kids project): a parallel-cluster randomized controlled pilot study. J Epidemiol Community Health. (2019) 73:324–33. doi: 10.1136/jech-2017-210163
165. Thompson D, Cullen KW, Boushey C, Konzelmann K. Design of a website on nutrition and physical activity for adolescents: results from formative research. J Med Internet Res. (2012) 14:85–99. doi: 10.2196/jmir.1889
166. Utter J, Warbrick J, Scragg R, Denny S, Schaaf D. Design, development, and achievements of a youth-led nutrition and physical activity intervention in a Pacific community in New Zealand. J Am Diet Assoc. (2010) 110:1634–7. doi: 10.1016/j.jada.2010.08.014
167. Uyeda K, Bogart LM, Hawes-Dawson J, Schuster MA. Development and implementation of a school-based obesity prevention intervention: lessons learned from community-based participatory research. Prog Commun Health Partner. (2009) 3:249–55. doi: 10.1353/cpr.0.0085
168. Vangeepuram N, Carmona J, Arniella G, Horowitz CR, Burnet D. Use of focus groups to inform a youth diabetes prevention model. J Nutr Educ Behav. (2015) 47:532–9.e1. doi: 10.1016/j.jneb.2015.08.006
169. Vangeepuram N, Williams N, Constable J, Waldman L, Lopez-Belin P, Phelps-Waldropt L, et al. TEEN HEED: design of a clinical-community youth diabetes prevention intervention. Contemp Clin Trials. (2017) 57:23–8. doi: 10.1016/j.cct.2017.03.010
170. Venditti EM, Elliot DL, Faith MS, Firrell LS, Giles CM, Goldberg L, et al. Rationale, design and methods of the HEALTHY study behavior intervention component. Int J Obesity. (2009) 33:116. doi: 10.1038/ijo.2009.116
171. Werkhoven T, Cotton W, Dudley D. Australian tertiary students' attitudes towards youth obesity in educational institutions. Eur Phys Educ Rev. (2018) 24:181–93. doi: 10.1177/1356336X16675774
172. Woodgate RL, Leach J. Youth's perspectives on the determinants of health. Qual Health Res. (2010) 20:1173–82. doi: 10.1177/1049732310370213
173. Woodgate RL, Sigurdson CM. Building school-based cardiovascular health promotion capacity in youth: a mixed methods study. BMC Public Health. (2015) 15:421. doi: 10.1186/s12889-015-1759-5
174. Wordell D, Daratha K, Mandal B, Bindler R, Butkus SN. Changes in a middle school food environment affect food behavior and food choices. J Acad Nutr Diet. (2012) 112:137–41. doi: 10.1016/j.jada.2011.09.008
175. Pfeiffer KA, Robbins LB, Ling J, Sharma DB, Dalimonte-Merckling DM, Voskuil VR, et al. Effects of the girls on the move randomized trial on adiposity and aerobic performance (secondary outcomes) in low-income adolescent girls. Pediatr Obes. (2019) 14:e12559. doi: 10.1111/ijpo.12559
176. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128 9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42.
177. UNFPA. The Power of 1.8 Billion- Adolescents, Youth and the Transformation of the Future. New York, NY: The United Nations Population Fund (2014).
178. McGregor S, Henderson KJ, Kaldor JM. How are health research priorities set in low and middle income countries? A systematic review of published reports. PLoS ONE. (2014) 9:e108787. doi: 10.1371/journal.pone.0108787
179. Neumark-Sztainer D, Story M, Hannan PJ, Perry CL, Irving LM. Weight-related concerns and behaviors among overweight and nonoverweight adolescents: implications for preventing weight-related disorders. Arch Pediatr Adolesc Med. (2002) 156:171–8. doi: 10.1001/archpedi.156.2.171
180. Clark H, Coll-Seck AM, Banerjee A, Peterson S, Dalglish SL, Ameratunga S, et al. A future for the world's children? Lancet. (2020) 395:605–58. doi: 10.1016/S0140-6736(19)32540-1
181. Tsang VWL, Fletcher S, Thompson C, Smith S. A novel way to engage youth in research: evaluation of a participatory health research project by the international children's advisory network youth council. Int J Adolesc Youth. (2020) 25:676–86. doi: 10.1080/02673843.2020.1716817
182. Dover DC, Belon AP. The health equity measurement framework: a comprehensive model to measure social inequities in health. Int J Equity Health. (2019) 18:36. doi: 10.1186/s12939-019-0935-0
183. Cardel M, Lee A, Dillard J, Dilip A, Miller D, Theis R, et al. Perceived barriers and facilitators to healthy lifestyles and weight loss among adolescents with overweight and obesity: a qualitative study. Curr Dev Nutr. (2020) 4(Suppl. 2):1614. doi: 10.1093/cdn/nzaa063_012
184. Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
185. Australia UY. Australian Youth Representative Consultation Report. New York, NY: United Nations (2019).
Keywords: adolescent, youth, participation, engagement, decision-making, obesity, overweight, prevention
Citation: Mandoh M, Redfern J, Mihrshahi S, Cheng HL, Phongsavan P and Partridge SR (2021) Shifting From Tokenism to Meaningful Adolescent Participation in Research for Obesity Prevention: A Systematic Scoping Review. Front. Public Health 9:789535. doi: 10.3389/fpubh.2021.789535
Received: 05 October 2021; Accepted: 30 November 2021;
Published: 23 December 2021.
Edited by:
Dickson Amugsi, African Population and Health Research Center (APHRC), KenyaReviewed by:
Anniza De Villiers, South African Medical Research Council, South AfricaCopyright © 2021 Mandoh, Redfern, Mihrshahi, Cheng, Phongsavan and Partridge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariam Mandoh, bWFyaWFtLm1hbmRvaEBzeWRuZXkuZWR1LmF1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.