 Ana Maria Nogales Vasconcelos
Ana Maria Nogales Vasconcelos Lenice Ishitani2
Lenice Ishitani2- 1Department of Statistics, University of Brasilia, Brasilia, Brazil
- 2Epidemiology and Health Assessment Research Group (GPEAS), Federal University of Minas Gerais, Belo Horizonte, Brazil
- 3Graduate Program in Public Health, School of Medicine and Epidemiology and Health Assessment Research Group (GPEAS), Federal University of Minas Gerais, Belo Horizonte, Brazil
Objective: This study aimed to analyze the chain of events and contributing causes associated with COVID-19 adult mortality (30–69 years old), based on qualified data on CoD from three Brazilian capitals cities, Belo Horizonte, Salvador, and Natal, in 2020.
Methods: Data of all deaths among residents in the three capitals in 2020 were provided by these municipalities' routine Mortality Information System (SIM). Mentions B34.2 with the markers U07.1 and U07.2 in the death certificate identified COVID-19 deaths. We used a multiple-cause-of-death approach better to understand the complexity of the morbid process of COVID-19. Conditions that appeared more frequently in the same line or above the COVID-19 mentions in the death certificate were considered a chain-of-event. Conditions that occurred more often after the codes for COVID-19 were considered as contributing.
Results: In 2020, 7,029 records from COVID-19 as the underlying cause of death were registered in SIM in the three capitals. Among these, 2,921 (41.6%) were deceased between 30 and 69 years old, representing 17.0% of deaths in this age group. As chain-of-events, the most frequent conditions mentioned were sepsis (33.4%), SARS (32.0%), acute respiratory failure (31.9%), unspecified lower respiratory infections (unspecified pneumonia) (20.1%), and other specified respiratory disorders (14.1%). Hypertension (33.3%), diabetes unspecified type (21.7%), renal failure (12.7%), obesity (9.8%), other chronic kidney diseases (4.9%), and diabetes mellitus type 2 (4.7%) were the most frequent contributing conditions. On average, 3.04 conditions were mentioned in the death certificate besides COVID-19. This average varied according to age, place of death, and capital.
Conclusion: The multiple-cause analysis is a powerful tool to better understand the morbid process due to COVID-19 and highlight the importance of chronic non-communicable diseases as contributing conditions.
Introduction
The importance of vital statistics to support the planning, evaluation, and monitoring of health programs and policies is widely recognized (1, 2). In the current scenario of the COVID-19 pandemic, the availability of vital statistics data is essential to follow the evolution and characteristics of cases and deaths (3). This information must be timely and with a satisfactory level of quality for its use. In Brazil, the Mortality Information System (SIM) from the Ministry of Health (MS) provides data on mortality for the whole country since 1976. SIM is a decentralized system in which each municipality (5,570 in total) is responsible for collecting and inputting data from the death certificate that the physician must sign (4). Although recent studies have shown that SIM has a high completeness level, there are still problems with the quality of information on causes of death (CoD) (5).
Several initiatives to improve the quality of information have been adopted, including physician training to improve the certification of the cause of death. The investigation of deaths with underlying cause classified as garbage code (CG) was carried out in 2017 in 60 municipalities in the five regions of the country, an initiative coordinated by the MS, in partnership with the Federal University of Minas Gerais (UFMG) and with support from Vital Strategies, through the Bloomberg Foundation. The investigation resulted in the reclassification for specific causes of 58% of deaths with GC (6).
In 2019, to promote the sustainability of the previous improvements achieved in selected municipalities in Brazil, a new initiative proposed to work more deeply with only three cities, Belo Horizonte with 2.5 million inhabitants, Salvador, 2.9, and Natal, 0.9 (7). The first municipality is in the Southeast region and the two others in the Northeast. Due to the emergence of the new Coronavirus (COVID-19), the initiative in these three cities changed its former aim and focused on an investigation to correctly identify deaths from COVID-19.
COVID-19 epidemic has led to an overload on the health system in Brazil, with a negative impact on all health programs (8). It has significantly compromised the achievement of Goal 3 of the Sustainable Development Objectives (SDG), more specifically, the target 3.4 of SDG that pointed, by 2030, a reduction of one-third premature mortality (adults under 70 years old) from non-communicable diseases (NCD) (9).
Non-communicable diseases are the leading causes of death (CoD) for adults and the elderly (10). They are also the main comorbidities that contribute to the severity of COVID-19 (11). As death is not a single event, the multiple-cause-of-death approach can contribute to understanding the complexity of the morbid process of COVID-19 since the traditional focus on underlying CoD statistics is insufficient in facing the challenges posed by this epidemic (12).
To better describe and understand the morbid process of COVID-19 mortality and its association with NCD, the present study aims to analyze the chain of events and contributing causes associated with COVID-19 adult mortality (30–69 years old), based on qualified data on CoD from the three capitals cities in 2020. Although these three capitals do not represent the entire country, they can provide essential information about the morbid process caused by COVID-19 and its contributing causes.
Materials and Methods
Data
We used data of all deaths among residents in the three capitals (Belo Horizonte, Salvador, and Natal) that occurred in 2020, provided by these municipalities' routine Mortality Information System (SIM). The available database contains information on the characteristics of the deceased, the circumstance of death, causes of death (underlying cause and associated causes), and the investigation process. For this study we selected deaths from 30 to 69 years old that correspond to premature mortality, according to the WHO Global Action Plan for the prevention and control of non-communicable diseases (13, 14).
Cause of Death Statistics
Even though to statistical purpose, for each death, only one CoD is tabulated, certifier physicians must fill the death certificate with all conditions considered to have caused or contributed to the death. The order that all causes are mentioned in the death certificate can show the sequence of events that caused the death. In that sequence, the underlying cause of death (UCoD) will be (a) the disease or injury that initiated the train of events leading directly to death, or (b) the circumstances of the accident or violence that produced the fatal injury.
This sequence results from a complex pathological process. Thus, the UCoD approach underestimates mortality from diseases not selected as the underlying cause but contributing to death, as with chronic conditions. Using the multiple-cause-of-death approach, all causes present in the morbid process and informed by the certifying physician can be analyzed.
Medical Certification and ICD Mortality Coding of COVID-19
The first step in this work was to understand the medical certification and ICD mortality coding of COVID-19 in Brazil. For the codification of the COVID-19 death, Ministry of Health guidelines (15) established the use of ICD-10 code B34.2 with markers U07.1 (COVID-19, virus identified) and U07.2 (COVID-19, virus not identified). The markers would help the investigation of the cause of death process, specifying if the diagnosis of COVID-19 was confirmed or not. At the beginning of the pandemic, coders used the U04.9 code that refers to severe acute respiratory syndrome (SARS) to identify deaths from COVID-19 in the country. In July 2020, the MH issued a note informing that the codification of deaths with a mention of COVID-19 should be revised (16). The U04.9 code would only remain in the SIM if the SARS was part of the events chain that led to death.
Then, to identify the deaths due to COVID-19, we considered the mentions B34.2 with the markers U07.1 and U07.2 in the death certificate.
Multiple Cause of Death Analysis
To proceed with the analysis of causes associated with COVID-19 mortality, we used a multiple-cause-of-death approach, including all conditions, diseases, and injuries mentioned on the death certificate. Considering the significant number of possible conditions informed in the DC for this analysis, we decided to group the ICD-10 codes into groups with similar diagnoses. The initial classification was based on the Global Burden of Diseases study (GBD 2017) (17) and adapted to the Brazilian epidemiological profile. The Supplementary Table A presents the Group of conditions analyzed and respective ICD-10 codes.
We classified the conditions into two categories: chain-of-event or contributing. In Part I of the death certificate, we considered conditions that appeared more frequently (60% or more) in the same line or above the mentions B34.2, U0.7.1, U07.2, as a chain-of-event of COVID-19 mortality. Conditions that appeared more frequently (60% or more) after the codes for COVID-19 in Part I or, mainly, in Part II, were considered a contributing condition. Conditions that did not meet the requirements above or mentioned in <0.5% of the analyzed death certificates were not classified.
Statistical Analysis
Other than the cause of death, we consider age, gender, and race/color as characteristics of the deceased and local of death.
All data were analyzed using R-Studio with libraries readxl, foreign, tidyverse, and writexl.
Ethics
The analyzed data were in the public domain, preserving anonymity. Therefore, the project was approved by the Research Ethics Committee of the Federal University of Minas Gerais (COEP/UFMG) under number 4749326.
Results
In 2020, 7,029 records from COVID-19 as the underlying cause of death (UCoD) were registered by the routine SIM in the three Brazilian capitals cities (Belo Horizonte, Salvador, and Natal) (Figure 1). Of these, 62.5% were investigated to confirm the COVID-19 diagnosis and complete information about causes of death. The three capitals presented different investigation rates for COVID-19 mortality: 93.4% in Belo Horizonte (n = 2,018), 48.2% in Salvador (n = 1,812), and 51.9% in Natal (n = 571).
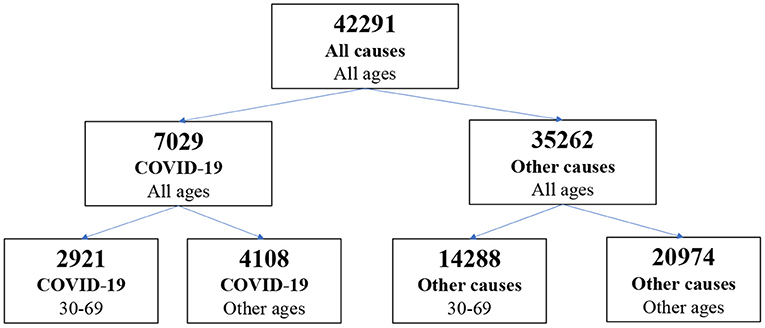
Figure 1. Number of death certificates according to age and cause of death, in three Brazilian capitals, 2020.
Among the deaths from COVID-19 as UCoD, 2,921 (41.6%) were from deceased between 30 and 69 years old, representing 17.0% of deaths in this group of ages. The virus SARS-COV2 was identified in 85.8% of deaths (U07.1), and for 14%, the COVID-19 diagnosis was clinical or epidemiological (U07.2).
Table 1 shows the distribution of COVID-19 deaths according to some characteristics and the proportion in relation to the total number of deaths in each category. Firstly, the number of deaths is concentrated in older ages: 50.2% of deaths are in the 60–69 age group. Likewise, the proportion of COVID-19 deaths increases with age: from 11% (IC 95% 9.5–12.4%) in the 30–39 age group to 19.2% (IC 95% 18.3–20.1%) in the 60–69 age group.
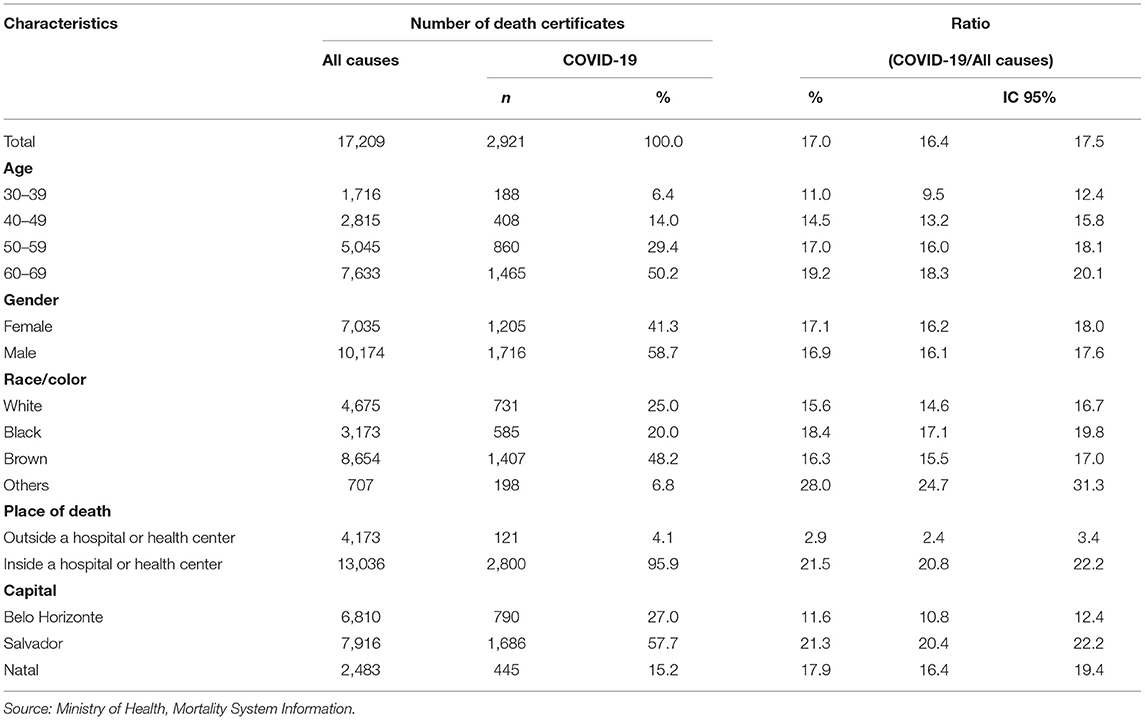
Table 1. Number of death certificates due to COVID-19 and all causes of death according to characteristics of the deceased and local of death, at ages 30–69 years, in three Brazilian capitals, 2020.
Although the number of deaths from COVID-19 is higher among men (58.7%), the proportion of deaths from COVID-19 in the total number of deaths is very similar between men and women, between 30 and 69 years (17.1 among women and 16.9 among men).
Regarding race/color categories, 68.2% of death from COVID-19 are of blacks or browns in these three capitals. We can also observe that the proportion of COVID-19 deaths among whites (15.6–IC 95% 14.3–16.7%) is lower than among blacks (18.4–IC 95% 17.1–19.8%). Among the “others” category of race/color, the proportion of deaths by COVID-19 is much higher (25.5–IC 95% 24.7–31.3%).
Concerning the place of occurrence of the death, we found that 95.9% of deaths occurred in hospitals or health centers. Thus, the proportion of COVID-19 deaths in total hospital deaths is much higher than that among deaths occurring outside hospital units (21.5 vs. 2.9%).
Considering the distribution of deaths among the three capitals, we observed that Salvador concentrated 57.7% of COVID-19 deaths in 2020. The proportion of COVID-19 deaths in the total number of deaths in Salvador is much higher than in the other two capitals [21.3% (20.4–22.2%) in Salvador vs. 17.9% (16.4–19.4%) and 11.6% (10.8–12.4%) in Natal and Belo Horizonte, respectively].
Table 2 shows the conditions mentioned in at least 0.5% of the death certificates where COVID-19 was the UCoD, and their classification as chain-of-events, contributing condition or not classified. Supplementary Table B presents all conditions mentioned classified as chain-of-events and contributing conditions. In 98.4% of DC with COVID-19 as UCoD (n = 2,843), there was at least one condition mention besides the COVID-19 diagnosis.
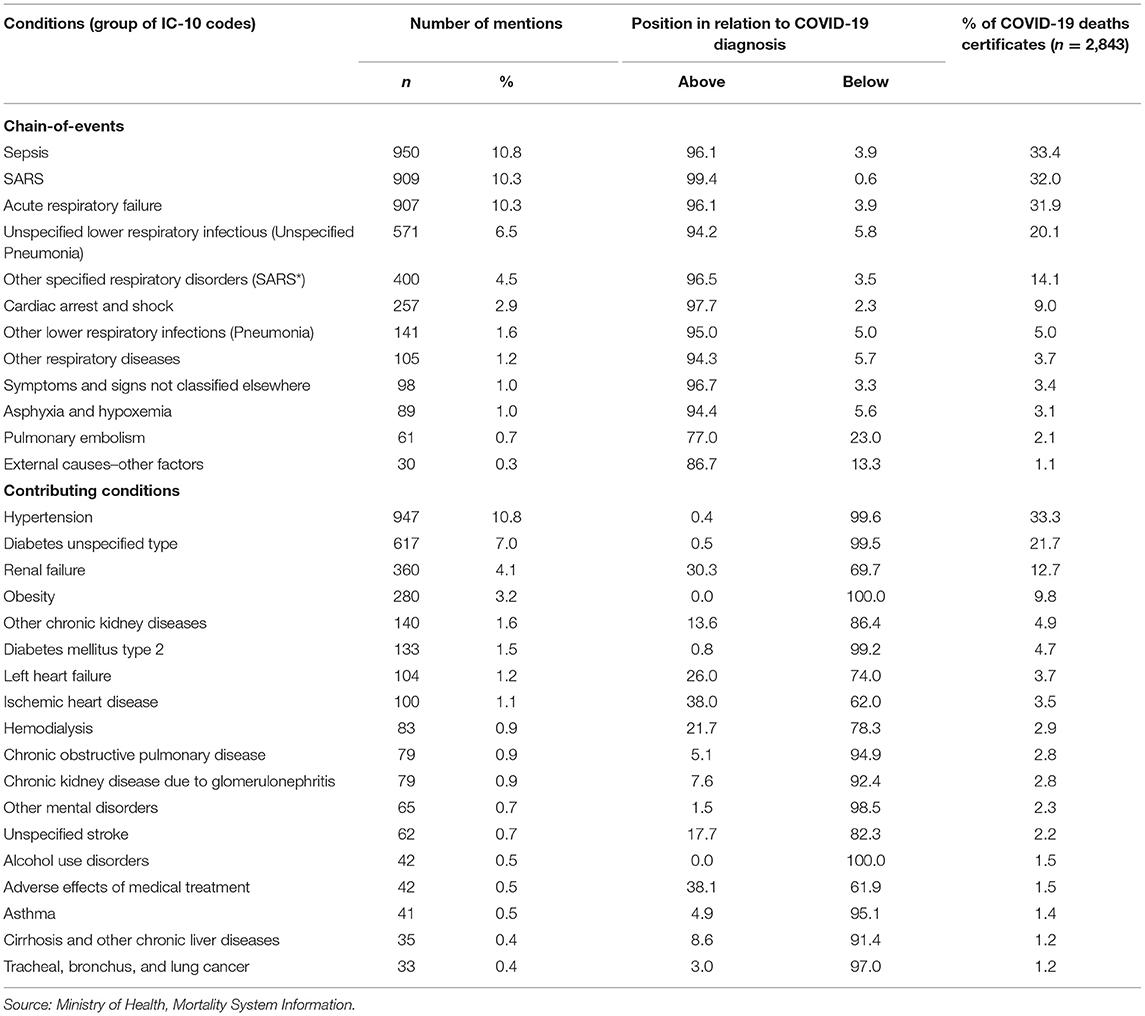
Table 2. Most frequent conditions listed in death certificates by position in relation to COVID-19 diagnosis, at ages 30–69 years, in three Brazilian capitals, 2020.
As chain-of-events, the most frequent conditions mentioned on the death certificate were sepsis (33.4%), SARS (32.0%), acute respiratory failure (31.9%), unspecified lower respiratory infections (unspecified pneumonia) (20.1%), and other specified respiratory disorders (14.1%). These five conditions corresponded to 42.4% of all conditions mentioned in DC analyzed.
Among the other conditions in the chain of events, we highlight the external cause–other factors condition mentioned in 1.1% of DC. A more detailed analysis showed that the most frequent code in this group (77%) corresponds to Y95, nosocomial condition.
As contributing conditions, hypertension (33.3%), diabetes unspecified type (21.7%), renal failure (12.7%), obesity (9.8%), other chronic kidney diseases (4.9%), and diabetes mellitus type 2 (4.7%) were the most frequent conditions mentioned in DC. These six conditions corresponded to 28.1% of all conditions mentioned in DC analyzed.
Among the other contributing conditions, we have mentions related to cardiovascular diseases, as left heart failure (3.7%), ischemic heart disease (3.5%), and unspecified stroke (1.5%), related to kidney diseases, as hemodialysis (2.9%) and chronic kidney disease due to glomerulonephritis (2.8%), related to respiratory diseases, as chronic obstructive pulmonary disease (2.8%) and asthma (1.4%), related to mental disorders, as alcohol use disorders (1.5%) and other mental disorders (2.3%). Related to neoplasms, the condition most frequent was tracheal, bronchus, and lung cancer (1.2%).
Still, we have external causes as the adverse effects of medical treatment in 1.5% of DC as contributing conditions.
Conditions not classified as chain-of-events or contributing were the group of injuries (0.8%), gastrointestinal bleeding (0.8%), flutter and fibrillation (0.7%), and hepatic failure (0.7%), among others less frequently mentioned.
Table 3 shows the distribution of death certificates according to the type of conditions associated with COVID-19. In general, 64.1% of DC present the two kinds of conditions: chain-of-events and contributing. This proportion varies according to (1) the age, from 51.6% in the 30–39 age group to 66.1% in the 60–69; (2) the gender, 67.8% among women and 61.5% among men; (3) the place of death, 64.4% for deaths occurred inside a hospital or health center, and 56.2% for deaths occurred elsewhere; (4) the capitals, 64.1 and 66.2% in Belo Horizonte and Salvador, against 56.2% in Natal.
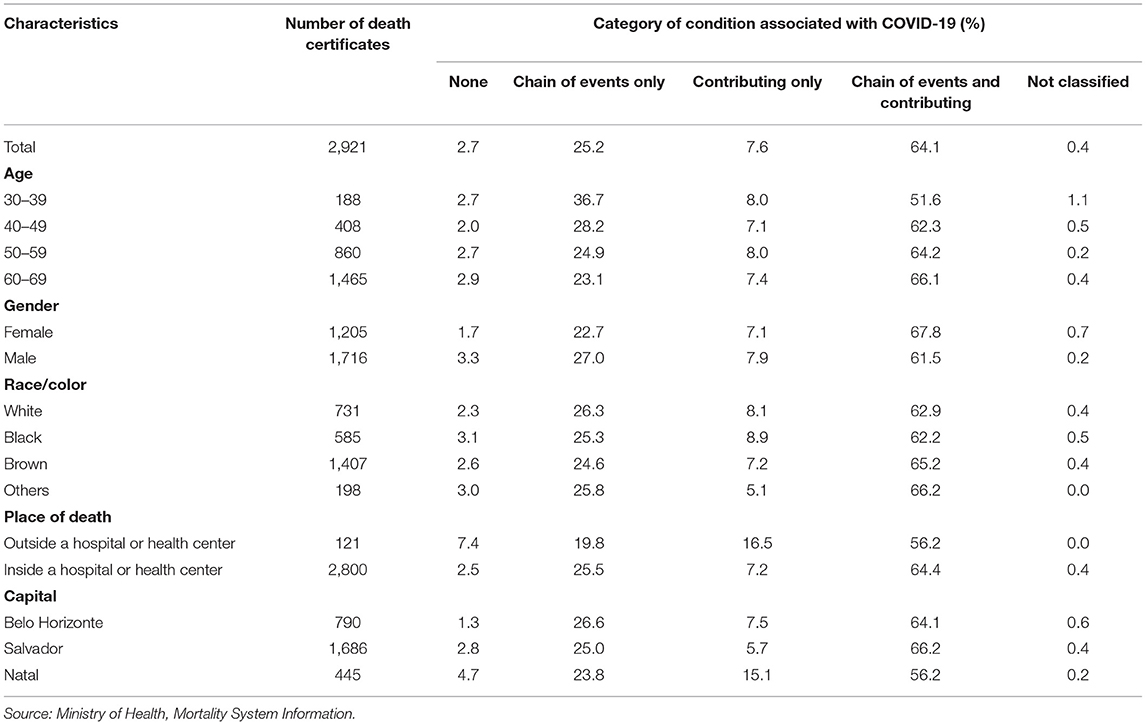
Table 3. Distribution of conditions associated with COVID-19 by category according to characteristics of the deceased and local of death, at ages 30–69 years, in three Brazilian capitals, 2020.
We can note that deaths that occurred outside a hospital or health center are more likely to have no other condition mentioned in DC besides COVID-19 (7.4%) or contributing only (16.5%). We observe the same for deaths registered in the city of Natal. We also note that deaths in the 30–39 age group are more likely to present only chain-of-events conditions (36.7%) than other groups of ages. We observe the same for men (27.0%) in comparison to women (22.7%).
For all death certificates analyzed, we have 3.04 (IC 95%: 2.99–3.10) conditions mentioned on average in Table 4. Nevertheless, this average varied according to age, place of death, and capital. For the first characteristic, we observe that the mean number of conditions increases with age. From 2.48 mentions (IC 95%: 2.30–2.66) on average for the age group 30–39 to 3.16 mentions (IC 95%: 3.08–3.24) for 60–69. Deaths that occurred inside a hospital or health center present a higher number of conditions mentioned on average than deaths that occurred elsewhere (3.07 vs. 2.53). Belo Horizonte presents a higher number of conditions mentioned on average than the other two capitals. In Belo Horizonte, the mean number of conditions mentioned was 3.39 (IC 95%: 3.28–3.50) against 2.94 (IC 95%: 2.87–3.01) and 2.81 (IC 95%: 2.68–2.94) for Salvador and Natal, respectively.
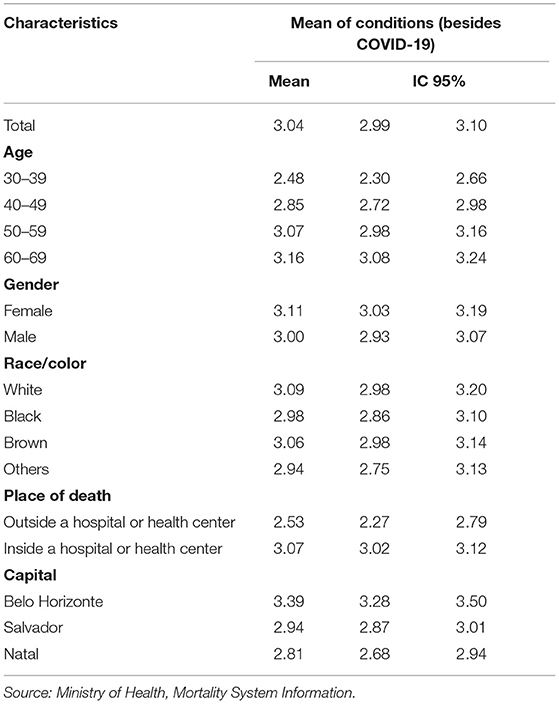
Table 4. Mean number of conditions mentioned in death certificate according to characteristics of the deceased and local of death, at ages 30–69 years, in three Brazilian capitals, 2020.
Discussion
This study provided important information on the chain of events and contributing causes of COVID-19 adult mortality (30–69 years old) from the three Brazilian capitals cities in 2020. Three aspects were highlighted from this analysis: first, the quality of medical certification of the COVID-19 mortality; second, the importance of the process of codification of all mentions declared in the death certificate and the role of the process of investigation of the cause of death in detailing the chain of events; third, the large concentration of mentions in just a few different causes or groups of causes highlights problems in-hospital care in patients with severe COVID-19 infection, on the one hand, and the relevance of non-communicable chronic diseases as contributing conditions to the worsening of COVID-19 infection.
Regarding the first aspect, we observed that 64% of 2,921 deaths certificated with COVID-19 have the documented chain-of-event and contributing conditions. Causes mentioned as chain-of-event or contributing are in accordance with other studies (18, 19), revealing the quality of death certificates filled out by physicians in these municipalities.
The number of causes mentioned on the death certificate also indicates the quality of filling in the medical certification, reporting possible multi-morbidity, and revealing the probable access to diagnostic procedures (20, 21). On average, there were 3.04 additional conditions in death certificates with COVID-19 as UCoD. However, data showed differences among the capitals. Belo Horizonte presented a significative higher mean number of mentions than the other two capitals. These differences may be associated with the different conditions of medical care given to COVID-19 patients, the different working conditions of physicians during the pandemic, and the different cultures of medical certification of the cause of death (21). In this sense and to clarify the reasons for these differences, it is essential to carry out more in-depth research that raises the factors mentioned above and describes the process of medical certification of the cause of death by COVID-19, compared to non- COVID-19 deaths. As a background for these differences, one must consider the social and economic inequalities that distinguish the three capitals, with Belo Horizonte located in an economically more favored region than Salvador and Natal (22).
Concerning the second aspect, we must remember that the quality of cause of death statistics also depends on the coding and investigation of the cause of death process carried out by the municipality's health departments and how the guidelines from the Ministry of Health were proposed and implemented locally. In Brazil, the automatic Underlying Cause Selection System (SCB–“Seletor de Causa Básica,” in Portuguese) used in the SIM, initially code U04.9 as a marker of the COVID-19 pandemic. Subsequently and following the WHO recommendation, all death records in which the code U04.9 appeared as a pandemic marker of COVID-19 should go through the SIM update process to include the new recommended COVID-19 codes (B34.2 with the markers U07.1 or U07.2) (15, 16).
A problem with the SARS (severe acute respiratory syndrome) diagnosis mentioned in the death certificate emerged with the updated coding guidelines. Following the guidelines, the SIM would retain U04.9 (ICD-10 code for SARS) only if SARS was mentioned in the death certificate. Nevertheless, preceding these guidelines, the Ministry of Health recommended code J98.8 (other specified respiratory disorders in ICD-10) when SARS was mentioned as a single cause or accompanied by an ill-defined condition in Part I, and with no additional condition in Part II of the death certificate.
How the local coders interpreted these recommendations and guidelines and carried out a review of the codes used to identify deaths from COVID-19 is a factor that impacts the number of mentions of causes reported to the System. Thus, in the analysis of the multiple causes of death approach, it is essential to consider that, in situations such as the SARS in COVID-19 deaths, the number of codes may be higher than the mentions of diagnoses informed by the physician. In some cases, excluding diagnostic duplicity is necessary when there is more than one diagnosis meaning the same cause or more than one code for the same diagnosis.
In this study, we chose to separately present the two codes used for SARS diagnosis (U04.9 and J98.8) and emphasize the influence of coding rules and recommendations in the count of the number of diagnoses mentioned in the death certificates. A more detailed analysis to verify the co-occurrence of the two codes in the death certificates should be carried out to, eventually, correct the number of different diagnoses of causes reported by the physician.
About the investigation process, it is important to consider that the three municipalities' health departments carried out an epidemiological investigation for most of the death certificates with COVID-19 as UCoD (62.5%). However, the quality of the investigation and the information collected during this procedure also will determine the quality of cause of death statistics. Advancing this analysis to other causes would bring crucial contributions to the elucidation of the differences of number of conditions mentioned in the death certificates among the three capitals and understand the role of the codification and investigation process in improving the quality of mortality statistics.
Concerning the third aspect, more than 70% of all causes mentioned in the medical certificate in the three capitals concentrated on five conditions classified as the chain of events and six as contributing causes. As conditions that describe the chain of events that led to death by COVID-19, different respiratory complications were often mentioned as SARS, unspecified pneumonia, and acute respiratory failure. Nevertheless, the high proportion of sepsis concerns and the mention of nosocomial conditions (Y95) may be associated with the quality of the health attention in-hospital during the pandemic. An analysis of this question goes beyond the objectives of this study. This finding suggests further new studies on sepsis, such as the trend (23) and association with other causes of death through more specific multiple cause of death analysis.
As contributing conditions, there is sufficient evidence that patients with non-communicable diseases (NCD) are at higher risk of worse consequences if they contract COVID-19 (12, 24, 25). Our study also observed that the most frequent contributing conditions are hypertension, diabetes, obesity, and complications related to kidney diseases. Our results were consistent with other studies about COVID-19 associated outcomes (18). Nevertheless, it is important to note that deaths from COVID-19 are closely related to the presence of chronic conditions for the old ages (26–28). In contrast, in adults under 50, this situation is less common (19).
Considering that the situation is worse in low- and middle-income countries due to the interaction between socioecological and biological factors (29, 30), the high prevalence of NCD, the accelerated demographic transition process and the great social inequality (31) contribute to a challenging scenario in the Brazilian context of the COVID-19 pandemic.
The information obtained through this study provides essential insight on how these three capitals and other Brazilian cities need support to respond quickly and effectively to COVID-19. Also, it will be vital to ensure primary health assistance for NCD after the pandemic (24, 25, 32, 33).
However, some significant limitations of the study must be addressed. The first refers to the classification of conditions associated with COVID-19 into a chain of events and contributing. Our classification observed only the position in which the cause appeared on the death certificate. Thus, our classification depends on the accuracy with which physicians report all conditions of the morbid process and how they fill out death certificates. A second limitation is the codification process of the causes associated with COVID-19, which changed throughout 2020.
Nevertheless, the multiple-cause-of-death approach provides a starting point for the identification of other conditions that might contribute to adult mortality, considering lesser-known conditions that are not yet understood to be associated with or contribute to death from COVID-19.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data can be found at: https://datasus.saude.gov.br/transferencia-de-arquivos/.
Ethics Statement
The analyzed data were in the public domain, preserving anonymity. Therefore, the project was approved by the Research Ethics Committee of the Federal University of Minas Gerais (COEP/UFMG) under number 4749326.
Author Contributions
AN performed data analysis and interpretation. LI, DA, and EF proposed the grouping of causes. All authors made substantial contributions to the content, writing of this paper, conceived the study, made substantial intellectual contributions to several drafts, and approved the final version of the manuscript.
Funding
This work was supported by Vital Strategies-GGP-CRVS Brazil Data for Health/ n. 23998 Fundep. This article is, in part, an output of the Bloomberg Philanthropies Data for Health Initiative. AN was supported in part by CNPq-Brazil (Bolsa de produtividade em pesquisa, 309944/2018-0).
Author Disclaimer
The views expressed are not necessarily those of the Philanthropies.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors expressly acknowledged the contributions of Mathews de Noronha Silveira Lisboa e Luana Gonçalves Barreto in statistical data analysis.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.788932/full#supplementary-material
References
1. AbouZahr C, de Savigny D, Mikkelsen L, Setel PW, Lozano R, Nichols E, et al. Civil registration and vital statistics: progress in the data revolution for counting and accountability. Lancet. (2015) 386:1373–85. doi: 10.1016/S0140-6736(15)60173-8
2. World Health Organization (WHO). University of Queensland. Improving the Quality and Use of Birth, Death and Cause-of-Death Information: Guidance for a Standards-Based Review of Country Practices. Geneva: World Health Organization (2010). Available online at: http://whqlibdoc.who.int/publications/2010/9789241547970_eng.pdf (accessed July 15, 2020).
3. AbouZahr C, Bratschi MW, Cercone E, Mangharam A, Savigny D, Dincu I, et al. The COVID-19 pandemic: effects on civil registration of births and deaths and on availability and utility of vital events data. Am J Public Health. (2021) 111:1123–31. doi: 10.2105/AJPH.2021.306203
4. Mello Jorge MHP, Laurenti R, Gotlieb SLD. Análise da qualidade das estatísticas vitais brasileiras: a experiência de implantação do SIM e do SINASC [Quality analysis of Brazilian vital statistics: the experience of implementing the SIM and SINASC systems]. Cien Saude Colet. (2007) 12:643–4. doi: 10.1590/S1413-81232007000300014
5. Teixeira RA, Ishitani L, França E, Pinheiro PC, Lobato MM, Malta DC. Mortality due to garbage codes in Brazilian municipalities: differences in rate estimates by the direct and Bayesian methods from 2015 to 2017. Rev Bras Epidemiol. (2021) 24:e210003. doi: 10.1590/1980-549720210003.supl.1
6. Marinho MF, França EB, Teixeira RA, Ishitani LH, Cunha CC, Santos MR, et al. Data for health: impact on improving the quality of cause-of-death information in Brazil. Rev Bras Epidemiol. (2019) 22(Suppl. 3):e19005.supl.3. doi: 10.1590/1980-549720190005.supl.3
7. IBGE. Estimativas de população. Available online at: https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de-populacao.html?edicao=28674&t=resultados (accessed September 25, 2021).
8. Moreira G, Canedo AC, Mello RGB. SARS-COV-2: the first wave of disease outbreak and its barriers to chronic diseases management. Geriatr Gerontol Aging. (2020) 14:149–51. doi: 10.5327/Z2447-21232020v14n3EDT1
9. World Health Organization. Regional Office for the Western Pacific. Sustainable Development Goals (SDGs): Goal 3. Target 3.4: By 2030, By 2030, Reduce by One Third Premature Mortality From Non-communicable Diseases Through Prevention and Treatment and Promote Mental Health and Wellbeing. (2016). Available online at: https://apps.who.int/iris/handle/10665/208282 (accessed September 25, 2021).
10. World Health Organization. Global Status Report on Non-communicable Diseases 2014. (2014). Available online at: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf (accessed September 25, 2021).
11. Palmer K, Monaco A, Kivipelto M, Onder G, Maggis S, Michel J-P et al. The potential long-term impact of the COVID-19 outbreak on patients with non-communicable diseases in Europe: consequences for healthy ageing. Aging Clin Exp Res. (2020) 32:1189–94. doi: 10.1007/s40520-020-01601-4
12. Nikoloski Z, Alqunaibet AM, Alfawaz RA, Almudarra SS, Herbst CH, El-Saharty S, et al. Covid-19 and non-communicable diseases: evidence from a systematic literature review. BMC Public Health. (2021) 21:1068. doi: 10.1186/s12889-021-11116-w
13. World Health Organization. WHO Global Action Plan for the Prevention and Control Of Noncommunicable Diseases 2013-2020. Available online at: https://www.who.int/publications/i/item/9789241506236 (accessed November 25, 2021).
14. Cardoso LSM, Teixeira RA, Ribeiro ALP, Malta DC. Premature mortality due to non-communicable diseases in Brazilian municipalities estimated for the three-year periods of 2010 to 2012 and 2015 to 2017. Rev Bras Epidemiol. (2021) 24(suppl 1):e210005. doi: 10.1590/1980-549720210005.supl.1
15. Brasil Ministério da Saúde,. Orientações para a codificação das causas de morte no contexto da COVID-19. (2020). Available online at: http://plataforma.saude.gov.br/cta-br-fic/codificacao-Covid-19.pdf (accessed September 25, 2021).
16. Brasil. Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Análise de Situação de Saúde e Vigilância de Doenças não Transmissíveis. Orientações sobre causas de mortes no contexto da covid-19: respostas às perguntas mais frequentes. (2020). Available online at: https://www.gov.br/saude/pt-br/coronavirus/publicacoes-tecnicas/guias-e-planos/af_orientacoes-causa-morte-respostas_13set21_finalb.pdf/view (accessed September 25, 2021).
17. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/S0140-6736(18)32203-7
18. Gundlapalli AV, Lavery AM, Boehmer TK, Beach MJ, Walke HT, Sutton PD, et al. Death Certificate–Based ICD-10 Diagnosis Codes for COVID-19 Mortality Surveillance — United States, January–December 2020. MMWR Morb Mortal Wkly Rep. (2021) 70:523–7. doi: 10.15585/mmwr.mm7014e2
19. Grippo F, Navarra S, Orsi C, Manno V, Grande E, Crialesi R, et al. The role of COVID-19 in the death of SARS-CoV-2–positive patients: a study based on death certificates. J Clin Med. (2020) 9:3459. doi: 10.3390/jcm9113459
20. Santo AH. Potencial epidemiológico da utilização das causas múltiplas de morte por meio de suas menções nas declarações de óbito, Brasil, 2003 [Epidemiological potential of multiple-cause-of-death data listed on death certificates, Brazil, 2003]. Rev Panam Salud Publica. (2007) 22:178–86. doi: 10.1590/S1020-49892007000800004
21. Campbell Annie,. Quality of Mortality Data During the Coronavirus Pandemic, England Wales: 2020. Office for National Statistics (2020). Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/qualityofmortalitydataduringthecoronaviruspandemicenglandandwales/2020 (accessed September 29, 2021).
22. Silva SA. Regional inequalities in brazil: divergent readings on their origin and public policy design. EchoGéo. (2017) 41:15060. doi: 10.4000/echogeo.15060
23. Prest J, Sathananthan M, Jeganathan N. Current trends in sepsis-related mortality in the United States. Crit Care Med. (2021) 49:1276–84. doi: 10.1097/CCM.0000000000005017
24. World Health Organization. The Impact of the COVID-19 Pandemic on Non-communicable Disease Resources and Services: Results of a Rapid Assessment. (2020). Available online at: https://apps.who.int/iris/bitstream/handle/10665/334136/9789240010291-eng.pdf (accessed January 4, 2021).
25. Stefan N, Birkenfeld AL, Schulze MB. Global pandemics interconnected - obesity, impaired metabolic health and COVID-19. Nat Rev Endocrinol. (2021) 17:135–49. doi: 10.1038/s41574-020-00462-1
26. Niquini RP, Lana RM, Pacheco AG, Cruz OG, Coelho FC, Carvalho LM, et al. Description and comparison of demographic characteristics and comorbidities in SARI from COVID-19, SARI from influenza, and the Brazilian general population. Cad Saude Publica. (2020) 36:e00149420. doi: 10.1590/0102-311x00149420
27. Silva PVD, Oliveira SB, Escalante JJC, Almiron M, Tsuha DH, Sato HK, et al. Risk factors for death among 120,804 hospitalized patients with confirmed COVID-19 in São Paulo, Brazil. Am J Trop Med Hyg. (2021) 105:88–92. doi: 10.4269/ajtmh.20-1598
28. Salzberger B, Buder F, Lampl B, Ehrenstein B, Hitzenbichler F, Holzmann T, et al. Epidemiology of SARS-CoV-2. Infection. (2021) 49:233–9. doi: 10.1007/s15010-020-01531-3
29. Yadav UN, Rayamajhee B, Mistry SK, Parsekar SS, Mishra SK. A syndemic perspective on the management of noncommunicable diseases amid the COVID-19 pandemic in low- and middle-income countries. Front Public Health. (2020) 8:508. doi: 10.3389/fpubh.2020.00508
30. Hacker KA, Briss PA, Richardson L, Wright J, Petersen R. COVID-19 and chronic disease: the impact now and in the future. Prev Chronic Dis. (2021) 18:E62. doi: 10.5888/pcd18.210086
31. Mesenburg MA, Hallal PC, Menezes AMB, Barros AJD, Horta BL, Barros FC, et al. Chronic non-communicable diseases and COVID-19: EPICOVID-19 Brazil results. Rev Saude Publica. (2021) 55:38. doi: 10.11606/s1518-8787.2021055003673
32. Chang AY, Cullen MR, Harrington RA, Barry M. The impact of novel coronavirus COVID-19 on non-communicable disease patients and health systems: a review. J Intern Med. (2021) 289:450–62. doi: 10.1111/joim.13184
Keywords: COVID-19, multiple cause of death, non-communicable diseases, Brazil, mortality
Citation: Nogales Vasconcelos AM, Ishitani L, Abreu DMX and França E (2022) Covid Adult Mortality in Brazil: An Analysis of Multiple Causes of Death. Front. Public Health 9:788932. doi: 10.3389/fpubh.2021.788932
Received: 03 October 2021; Accepted: 14 December 2021;
Published: 17 January 2022.
Edited by:
Carla Sofia e Sá Farinha, New University of Lisbon, PortugalReviewed by:
Precil Neves, University of São Paulo, BrazilLivia Vinhal Frutuoso, Ministry of Health, Brazil
Copyright © 2022 Nogales Vasconcelos, Ishitani, Abreu and França. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Maria Nogales Vasconcelos, bm9nYWxlc0B1bmIuYnI=