 Ren Wang
Ren Wang Lizhi Zhang
Lizhi Zhang Ting Tang
Ting Tang Fei Yan1
Fei Yan1- 1School of Finance, Hunan University of Technology and Business, Changsha, China
- 2College of Science, Hunan University of Technology and Business, Changsha, China
- 3Hunan Aerospace Hospital, Changsha, China
There have been considerable concerns regarding the effects of air pollution on health and economy over the past decades across the world. As insurance coverage has been closely related to household welfare, we aim to investigate the influence of air pollution, in particular, the sulfur dioxide (SO2) pollution on household purchases of commercial health insurance using data from the 2017 China Household Financial Survey (CHFS). The results show that the rise in SO2 emission has a significant positive association with tendency of residents to participate in commercial health insurance. The possibility of household commercial health insurance purchasing increases by 4% per 1,000 tons of SO2 emission. In addition, the proportion of commercial health insurance expenditure in household annual income increases by 29% per 1,000 tons of SO2 emission. The effects are also found to differ among resident groups. Residents in eastern parts of China are more likely to buy commercial health insurance facing SO2 pollution compared to those in western parts of China; people with higher income are more likely to be affected compared to those with lower income; families with the household head being female are more likely to be affected compared to those with the household head being male. This research provides baseline information on the formulation and implementation of future operation strategy in commercial health insurance companies of China.
Introduction
Air pollution is one of the leading issues threatening human health. As the WHO suggested in 2016, almost 91% of people over the world lived in areas with major air pollutants higher than the WHO standard, and outdoor air pollution caused nearly 3.7 million deaths. In China, this problem is also concerning. Although the Chinese government has made persistent efforts on promoting air pollution control, like supporting the development of eco-industry park and green innovation (1, 2). Chinese residents were still exposed to fine particulate matter (PM2.5) three times higher than the standard stipulated in the WHO guideline. This situation mentioned above gives great significance in studying the health effect of air pollution. Existing research works provide numerous evidence that air pollution has a close association with the increasing morbidity of various diseases (3–6). Accompanied with rapid economic growth in the emerging economies is the severe ecological deterioration (7). In developing countries like China, the health effect of air pollution has attracted a lot of interest for their facing more serve environmental threats. China's efforts on reducing air pollutants emission is proved to be effective in lowering the premature death rates by 12.6% from 2013 to 2017 (8). Besides, air pollution is also found to have a negative effect on people's mental health in China (9). Sulfur dioxide (SO2) is one of the major air pollutants worldwide. Short-term exposure to SO2 is also proved to result in higher morbidity of cardiovascular diseases and increased hospitalization due to respiratory diseases including chronic obstructive pulmonary diseases and so on (10). It is also suggested that SO2 pollution notably correlates with a greater risk of acute myocardial infarction (11). The effect of SO2 pollution on the morbidity of diseases varies across the world due to differences in the concentration of the pollutant, lifestyles of residents, etc. In China, the morbidity of diabetes is found to increase by 3.835% with the concentration of SO2 raising every 10 μg/m (12). However, the risk of diabetes due to exposure to SO2 in the US is roughly 1.15 times that in China (13). In addition, exposure to SO2 also affects health expenditures of residents. According to the health investment model and the health capital depreciation theory developed by Grossman (14), the outside shock aroused by exposure to air pollutants including SO2 would accelerate the depreciation of health capital stock of residents. To maintain their health status, residents should expand their health expenditures. Therefore, many scholars have discussed the relationship between air pollution and medical cost of residents (15). Air pollution would significantly increase medical costs and healthcare costs of residents (16). Moreover, the effect of air pollution differs across regions in China. There exists a positive association between air pollution and medical expense in eastern and central regions, but a non-linear threshold effect is detected in the western region of China. Based on the micro-data of Chinese residents, it is found that fine PM2.5 has a positive association with medical care cost, hospitalization spending, and self-payed healthcare costs of residents (17). Furthermore, the study reveals that young people are more sensitive to the detrimental effect and the long-term effect is smaller. Other scholars study the effect in different regions over the world. In Iran, air pollution increases the healthcare cost either in the short run or in the long run (18). In Korea, the improvement in air quality is suggested to gain potential health benefits with the air quality index, which includes five major air pollutants being the indicator (19). A series of studies above confirm that air pollution would drive residents to increase their healthcare expenses. However, few researches focus on how to cope with this side effect that air pollution brought, which is of great necessity to improve people's well-being and promote public health.
For another, commercial health insurance is an important approach for residents to reduce their self-paid healthcare costs and hence relieve their economic burden of relevant diseases, which is helpful for improving household welfare. The earliest study on the effect of air pollution on the purchase and cancellation of commercial insurance contracts is conducted to analyze motives of consumers to purchase insurance and reveals a positive relationship, which is inconsistent with behavioral economics. Besides, evidence shows that the health and economic loss brought by air pollution can be reduced by taking avoidance response and medical insurance is found to be an effective measure (20). Health insurance could also effectively reduce the mortality rate, which therefore is of significance for residents to maintain fitness (21). Under the Patient Protection and Affordable Care Act, almost 90% of American citizens are covered by health insurance or something similar (22). Facing the debate over healthcare policies, Woolhandler et al. (21) summarize the evidence on the association between insurance coverage and mortality. The evidence shows that health insurance is helpful to reduce mortality.
In conclusion, considering that commercial health insurance could assist people in improving health conditions, it is meaningful to study the effects of SO2 pollution on household insurance purchasing, particularly for those developing countries that are still encountering serious environmental problems. Commercial health insurance purchasing could be an effective way to cope with the adverse health effects of air pollution on the local residents. Under the background of the “Healthy China Plan”, more efforts should be made to focus on public health, to provide health services of better quality, and to improve the existing public healthcare system. Therefore, this paper is intended to focus on the effects of SO2 pollution on household insurance purchasing from the micro-perspective and to provide necessary information on the benign operation of commercial health insurance companies of China. By matching the individual data from China Household Financial Survey (CHFS) with the provincial annual SO2 emission data in China, this study examines whether SO2 pollution would drive people to take avoidance actions, which increase their possibility and degree of commercial health insurance purchasing. Since insurance purchasing is a complicated process affected by many factors, to reach convincible results, besides common control variables like demographic characteristics, more specific individual factors are fixed including financial literacy, social trust, etc. Last but not least, considering the characteristics of our indicators and data, the Probit and Tobit models are adopted to capture the effects of SO2 pollution on household insurance purchasing.
Materials and Methods
Data
This paper focuses on the associations between levels of SO2 pollution and household commercial health insurance purchasing based on micro-data from the 2017 CHFS, which covers 400,011 interviewees from 29 provincial-level regions in China excluding Tibet, Xinjiang, Hong Kong, Macao, and Taiwan. The survey provides abundant data on household and individual characteristics including income and asset conditions, age, gender, risk attitudes, etc. Therefore, it provides necessary data for our empirical research considering that insurance purchase behavior is also affected by various household and individual factors. The data on SO2 pollution is from China Statistical Yearbook (2017). The pollution data are matched with micro-data through the provincial code listed in the dataset of the CHFS.
Data Description
Dependent Variable
This paper analyzes the impact of SO2 pollution on household commercial health insurance purchasing from two aspects: the possibility of purchasing commercial health insurance and the degree of their purchase behavior. For defining household commercial health insurance purchasing, a household with at least one member covered by commercial health insurance is defined as a household covered by commercial health insurance. Therefore, we construct a dummy variable Insurance to indicate whether a household is covered by commercial health insurance, whose value is 1 when its members purchased commercial health insurance and is 0 when its members did not. For another, the degree of their purchase behavior is quantified by their proportion of commercial health insurance cost in household income. The data on the commercial health insurance cost is also obtained from the survey.
Independent Variable
The annual emission of SO2 pollutants is used as the core independent variable to measure the degree of SO2 pollution. The major air pollutants are including fine PM2.5, inhalable particles (PM10), SO2, nitrogen dioxide (NO2), carbon monoxide (CO), and ozone (O3). Some studies employ the Air Pollution Index (API) and Air Quality Index (AQI) released by the Ministry of Ecology and Environment of the People's Republic of China to quantify the air pollution in China. However, API is abolished in 2015 and AQI covers only 74 cities across China. In addition, the open average annual statistics on PM2.5, PM10, NO2, CO, and O3 are seldom collected. Considering that this paper is based on annual data, although the AQI, which is reported on a daily basis, could be more comprehensive, it would be difficult to be incorporated into our analysis. Therefore, this paper uses SO2 emission to quantify the degree of air pollution and focuses on the effect of SO2 pollution on the commercial health insurance purchase behavior of households.
Control Variable
To focus on the effect of SO2 pollution on household insurance purchasing as possible, it would be important to include a series of comprehensive control variables in the regression models. Insurance purchasing is a sophisticated process affected by many factors. People's health factors and other factors like financial literacy are necessary to be considered. According to the relevant studies, this paper includes various factors affecting commercial health insurance purchasing (23, 24). The control variables include two parts. First of all, the household characteristics are fixed including annual income, total assets, the proportion of medical expenditure in annual income, the proportion of children under 14 in the household, the proportion of the elder over 60 in the household, and residential background. The other part is the characteristics of the household head including age, gender, health conditions, marital status, education level, financial literacy, risk attitude, social health insurance, social trust, etc.
Several control variables are processed to eliminate potential data bias. First of all, the anomalous data with the values of annual income and total assets equal to or <0 is omitted. In addition, to eliminate the outliers, the indicators of annual income and total assets are winsorized at the upper and lower limit of 1% and then logarithmically processed. Second, based on the three questions about interest rate calculation, understanding of inflation rate, and knowledge of investment risks in the survey, this paper constructs three dummy variables, respectively, whose value is 1 if the answer is correct and is 0 if not. Those dummy variables are utilized to measure the financial literacy of the interviewee by employing factor analysis. All the variables are shown in Table 1.
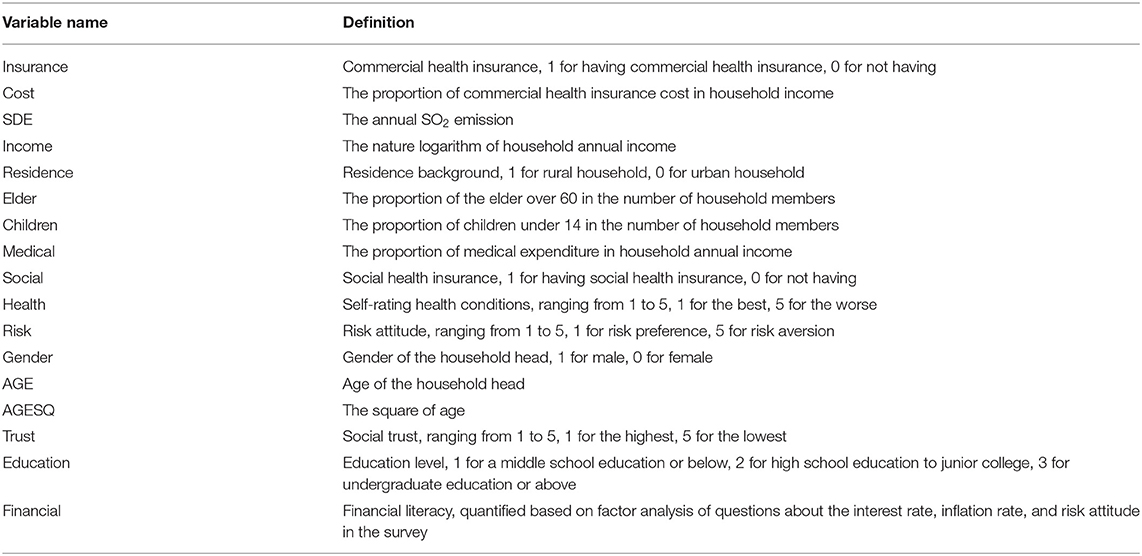
Table 1. Variable definition.
Model Specification
Considering whether a household purchase commercial health insurance is a dummy variable, the Probit model is used to analyze the effect of SO2 pollution on the possibility of a household purchasing commercial health insurance. The estimation equation is shown as follow:
The variable Insurance reflects whether a household has purchased commercial health insurance or not, whose value is 1 for households covered by commercial health insurance and is 0 for those not covered by commercial health insurance. The variable SDE is measured by SO2 emission volume. X represents all the control variables and ε is the error term.
Furthermore, this paper studies that to what degree SO2 pollution affects household commercial health insurance purchasing, which is measured by their proportion of commercial health insurance cost in household annual income. However, the commercial health insurance cost is zero for those households not purchasing commercial health insurance. That is to say, the variable cost is truncated. Therefore, this paper uses the Tobit model to analyze the association between SO2 pollution and the degree of household commercial health insurance purchasing. The estimation equation is listed as below:
The variable Cost is the proportion of commercial health insurance cost in household annual income. The variables SDE and X are the same as those in equation (3).
Empirical Analysis
Geographic Characteristics of SO2 Emission in China
The changes in annual SO2 emissions of each province in China from 2015 to 2017 are shown in Figure 1 by ArcGIS. It is shown that annual SO2 emissions of every province appeared to decline from 2015 to 2017, which suggests that the overall air quality in China is improving. However, the annual SO2 emissions of several provinces were still at a high level, and the total annual SO2 emission in the eastern region was higher than that in the western region in 2017, which might be due to the disparity in the levels of economic development and industry agglomeration (25). In addition, improvement in reducing SO2 emission differed across provinces. The top three provinces in an effort to reduce SO2 emission were Henan, Shandong, and Inner Mongolia, which decreased annual SO2 emission by over 600,000 tons. The improvement was relatively nominal in the provinces where the annual SO2 emission was at a low level over the past few years like Tibet and Hainan. In general, from 2015 to 2017, the SO2 emission of provinces in China decreased significantly, which indicates that the Chinese government is committed to improving the atmosphere environment.
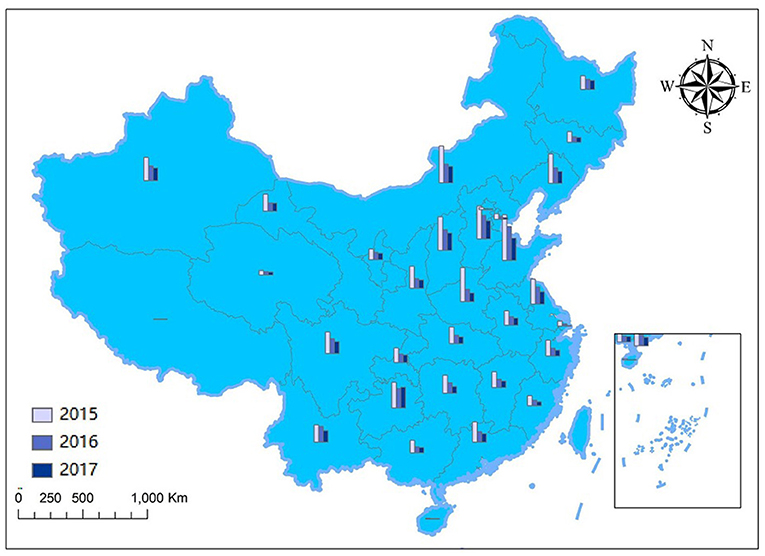
Figure 1. Changes in the SO2 emissions across provinces and regions from 2015 to 2017.
The geographic distribution of SO2 emissions over provinces in 2017 is shown in Figure 2. It shows that there observed notable spatial differences in annual SO2 emission across provinces. The highest annual SO2 emission amounted to 739,100 tons, whereas the lowest annual emission was only 3,500 tons. Particularly, the annual SO2 emissions of several provinces exceeded 400,000 tons, which might have posed a severe threat to the local atmosphere environment and the health of residents, including Shandong, Guizhou, Hebei, Shanxi, Inner Mongolia, and Xinjiang. In comparison, the annual SO2 emissions of some provinces and regions were at a lower level <100,000 tons like Beijing, Tianjin, Shanghai, Hainan, and Qinghai.
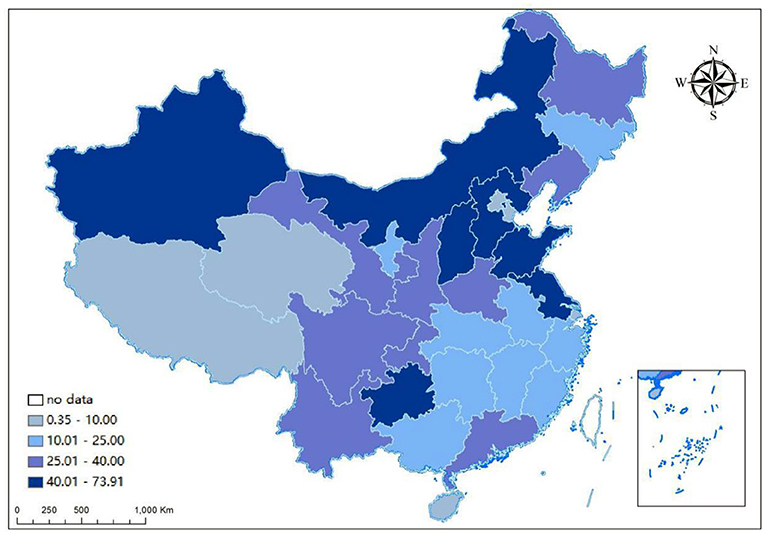
Figure 2. The geographic distribution of SO2 emissions across provinces and regions in 2017.
Figure 3 is the perspective view of the geographic distribution of SO2 emissions over provinces and regions in 2017, which reflects the spatial distribution of the provincial SO2 emissions and their overall trend. The X-axis indicates the east–west direction in China, and the Y-axis indicates the north–south direction. The Z-axis measures the provincial annual SO2 emission. The fitted curves in the X–Z plane and Y–Z plane show the geographic distribution of provincial annual SO2 emission in the east–west direction and the north–south direction, respectively. Figure 3 shows that the fitted curve in the X–Z plane is inverted U-shaped and the fitted curve in the Y–Z plane is like an arc, which indicates that the 2017 provincial annual SO2 emissions in China were spatially uneven. Specifically, the annual SO2 emission in the central region of China was higher than that in the eastern and western regions, and the annual SO2 emission in the eastern region was relatively higher than that in the western region. As for the difference between the south and north, the annual SO2 emission in the northern part of China was higher than that in the southern part.
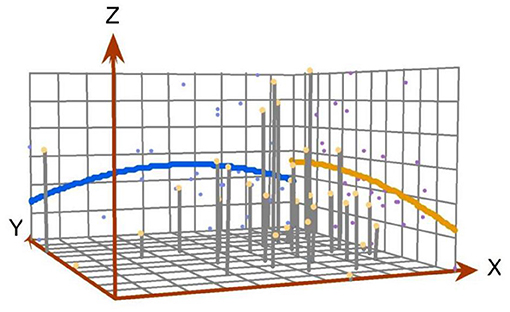
Figure 3. The perspective view of the geographic distribution of SO2 emissions in China.
Summary Statistics
After omitting the missing value and outliers, 20,100 valid observations are acquired in total as the sample for the empirical analysis. The sample is divided into two groups by whether a household had purchased commercial health insurance or not. Table 2 shows the mean and SD for the main variables in the empirical analysis. It shows that the annual SO2 emissions are unevenly distributed across regions. The average proportion of households with commercial health insurance in the sample is 5.07%. Moreover, there exist apparent differences in household characteristics among the observations. The average annual income and total assets of households with commercial health insurance are higher than those of households without commercial health insurance. For those households without commercial health insurance, their average proportion of medical insurance in annual income is also higher than their counterpart, which suggests that medical costs could be a heavy economic burden for them to bear. As for the other variables, it is also shown that the average performance of households with commercial health insurance is better than that of households without commercial health insurance in education level, health conditions, social trust, risk attitude, and social trust.
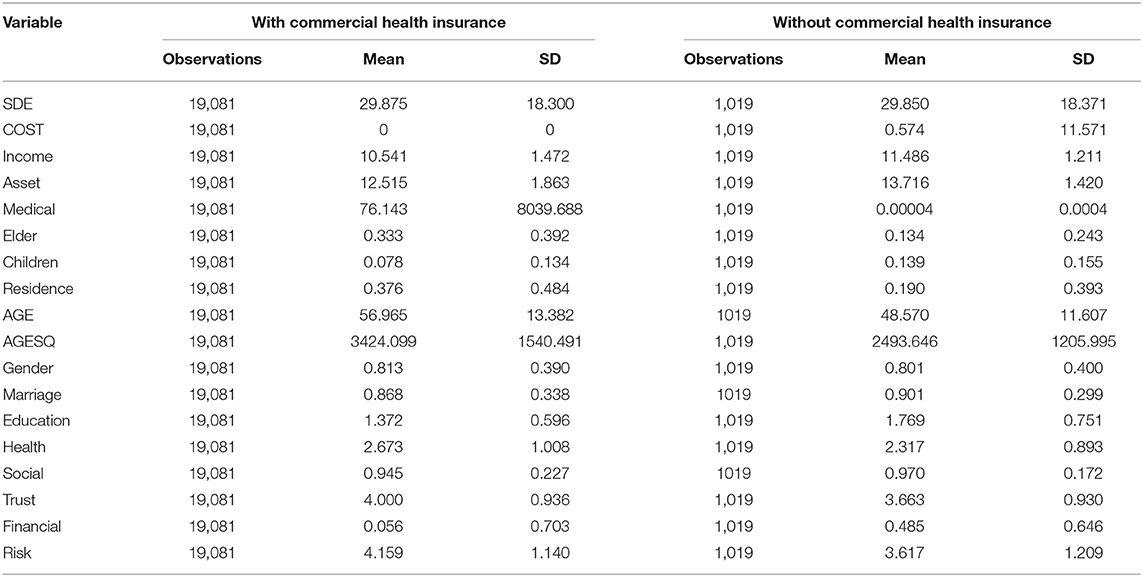
Table 2. Summary statistics.
Results
The results of our empirical analysis are shown in Table 3. In order to reveal the effect of SO2 pollution on household commercial health insurance purchasing and its degree, this paper employs the Probit and Tobit models as mentioned above, which are denoted by model 1 and model 2, respectively. For the regression results using the Probit model, it is shown that there exists a significant association between SO2 pollution and household commercial health insurance purchasing with the value of coefficient being 0.004, which suggests that SO2 pollution would raise the possibility of a household purchasing commercial health insurance. As for the regression results using the Tobit model, the coefficient value of the SDE is 0.0029, which proves that SO2 pollution would drive a household with commercial health insurance to increase the investment in health insurance.
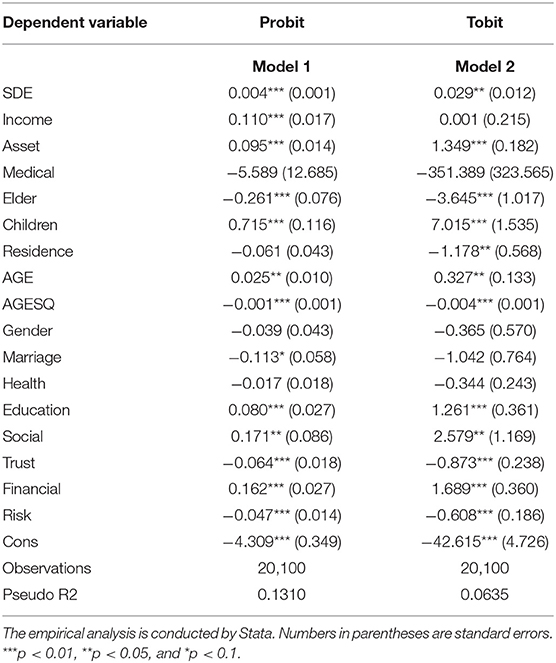
Table 3. Empirical results.
The regression results of the control variables indicate that the annual income of a household and total asset have a significant effect on its commercial health insurance purchase behavior, and the proportion of expenditure on commercial health insurance in annual income expands as the scale of total asset enlarges. The coefficients of the proportion of medical expenditure are insignificant in both models, which may be attributed to the crowding-out effect of medical expenditure on commercial health insurance expenditure. The proportions of the elder and children in the number of household members are significant. However, the coefficient of Elder is negative, whereas the coefficient of children is positive. This indicates that demand for commercial health insurance might decrease as the situation of the aging population gets more severe in China, whereas the increase in the proportion of younger people might boost the demand. The coefficient of Residence is insignificant, which suggests that there exists no apparent distinction between the demand of urban residents and rural residents for commercial health insurance. This situation might occur because commercial health insurance has not been popularized in China. As for the variables of individual characteristics, the effects of AGE, Education, Social, Trust, Financial, and Risk are significant, whereas the effects of Gender and Health are insignificant. Particularly, the effects of AGE on the possibility of a household purchasing commercial health insurance and its degree takes on inverted U-shaped, which means that the demand for commercial health insurance would increase at first and then decrease as the age of household head increases. The existence of adverse selection and moral hazard might exclude those people with a poor health condition from the commercial health insurance market, which could lead to the insignificant effect of health conditions on household commercial health insurance purchasing.
Heterogeneity Effects
It is mentioned that purchase decision of households on insurance is affected by various household and individual factors. Therefore, it is necessary to analyze its heterogeneous effects. This paper analyzes the heterogeneous effects of SO2 pollution on household commercial health insurance purchasing from four aspects including residential background, region, income level, and gender. All the results are shown in Table 4.
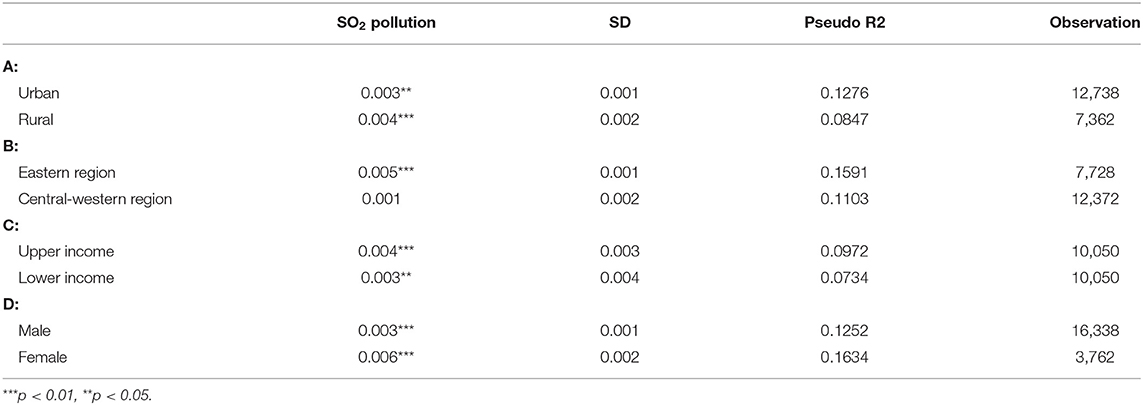
Table 4. Results of heterogeneity effect.
After dividing the sample into two groups by whether they are urban or rural residents, it is shown that the effect of SO2 pollution on household commercial health insurance purchasing is still significant for both groups. As for the effects on the residents in different regions, it suggests that there exists a positive association between SO2 pollution and household commercial health insurance purchasing in the eastern region and the central-northern region. However, the effect in the eastern region is still significant, whereas the effect in the central-northern region turns into insignificant. This indicates that the willingness of residents in eastern regions is stronger to address the outside shock of SO2 pollution by investing in commercial health insurance. After dividing the sample into two groups by the median annual household income, it is found that the effect is more notable for those with higher income. The households with higher annual income have more disposable income, so they are more likely to purchase commercial health insurance facing the SO2 pollution. Last but not least, considering gender differences, the result shows that women are more likely to depend on commercial health insurance to cope with the adverse effect of SO2 pollution compared to men.
Robustness Test
The effectiveness of our empirical results above might be mainly affected by two types of endogeneity including omitted variables and reverse causality. To address potential endogeneity, this paper employs the two-stage least squares (2SLS) method with an instrumental variable. A valid instrumental variable should satisfy two preconditions. First, the instrumental variable must be independent of the error term, which could be denoted by cov(IV, ε) = 0. In other words, the instrumental variable must be exogenous. Second, the instrumental variable must be highly related to the major dependent variable. According to a relevant study, this paper utilizes the annual precipitation amount at the provincial level as the instrument variable (26). For one thing, it is found that the precipitation could directly influence air pollutants like SO2 and hence is highly correlated to SO2 pollution (27–29). For another, considering that precipitation is a natural phenomenon, it is exogenous. Furthermore, precipitation is considered to have nothing to do with the health condition of residents, let alone their commercial health insurance behavior.
The regression results using an instrumental variable are shown in Table 5. The F-value in the first-stage least square regression is over 10, which indicates that the instrumental variable precipitation passes the Cragg–Donald test and is not a weak instrumental variable. In the 2SLS regression, the positive effect of SO2 pollution on commercial health insurance purchase behavior of households is also significant, and the value of its coefficient increases. It indicates that the effects of SO2 pollution on household purchases of commercial health insurance might be underestimated in our empirical analysis above due to endogeneity. The regression results with an instrumental variable are inconsistent with our empirical results, which suggests that our evidence on the positive association between SO2 pollution and households commercial health insurance purchasing is robust.
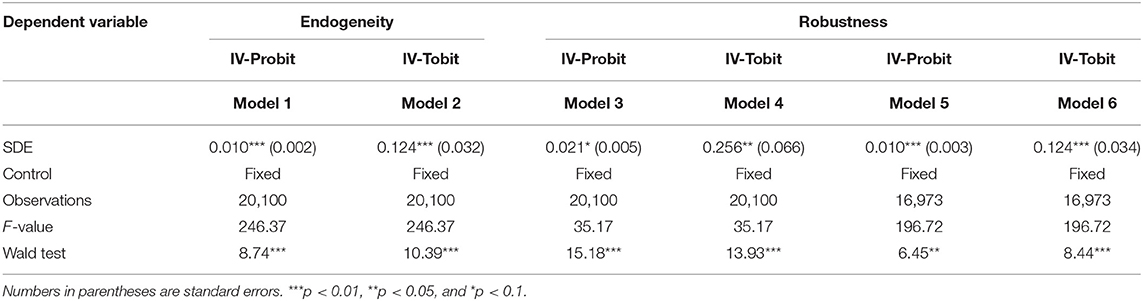
Table 5. Results of robustness test.
Considering that using the indicator of SO2 pollution only might result in measurement bias, To overcome potential selection bias, and test the robustness of our results the indicator of SO2 pollution is substituted with the annual emission of nitrogen oxide (NOx) to conduct a robustness test. The results are shown in Table 5 in the volumes of models 3 and 4. It shows that the coefficients of the effect are 0.021 and 0.256, respectively, which are both significant. The regression results after changing the indicator of air pollution shock also prove the robustness of our empirical results. In addition, considering that commercial health insurance purchase behavior of households is particularly affected by age, the regression results might be biased including those with the age of household head being too higher. Therefore, this paper conducts re-estimation based on the sample without observations with the age of household head over 70. The results are shown in Table 5 in the volumes of model 5 and model 6. After omitting parts of the observations, the results are still inconsistent with those in our empirical results above. In conclusion, the deepening of SO2 pollution has a significant positive association with the tendency of residents to participate in commercial health insurance, and the results are robust.
Discussion
The air pollution aroused by nature and human activities poses a great threat to the health status of human beings, which leads to increased morbidity of various diseases including lung diseases, respiratory diseases, heart diseases, and specifically childhood diseases (30, 31). Although air pollution damages the health of people (32), investing in commercial health insurance might be an effective approach to fight against this kind of adverse effect. Therefore, the aggravation of air pollution might have associations with the possibility of a household purchasing commercial health insurance. Based on the micro-data from the 2017 CHFS, this paper studies the effects of SO2 pollution on household commercial health insurance purchasing with a perspective from exposome. Our empirical results prove that SO2 pollution has a significant positive effect on household commercial health insurance purchasing. The possibility of a household purchasing commercial health insurance and its expenditure on commercial health insurance increase as SO2 pollution gets worse.
There exist some research works on the effects of air pollution on medical cost (33, 34), but few study the association between air pollution and household demand for health insurance. Moreover, previous studies on this topic are conducted from a macro-perspective. To the best of our knowledge, Chang et al. (35) first study on the effect of air pollution on the demand for commercial insurance from a micro-perspective. Based on the transaction data from a large insurance company in China, they found that for each SD increase in the Air Quality Index, the sales of insurance contracts would rise by 7.2%. Their research is remarkable but still has some limitations. Compared to our study, their data are from a single company, which might lead to sample bias. In addition, they do not take the individual factors into consideration, which might lead to omitted variable bias. Therefore, this study includes a series of household and individual factors affecting the insurance purchase behavior of people based on the micro-data from the 2017 CHFS which makes it possible for us to better reveal the effects of SO2 pollution on households' health insurance purchasing.
Our empirical results show that there are positive associations between SO2 pollution and household commercial health insurance purchasing, which is inconsistent with the previous studies. According to a similar study on the effects of air pollution on the demand of people for insurance, it also finds that air pollution would significantly increase the possibility of a household buying insurance and its insurance expenditure, and the effect is more apparent for health insurance compared with life insurance (23). The mechanism of the effect of air pollution on household commercial health insurance purchasing could be explained from two perspectives. For one thing, the investment of consumers in commercial health insurance is in fact to fulfill their demand for health. People increase their investment in health capital and transfer their potential health risks through commercial health insurance. The influences of air pollution on the health conditions of people received great attention in the past two decades (36). And it is found that frequent exposure to air pollutants like SO2 is linked to higher morbidity of respiratory diseases (37). According to the Grossman model, the outside shock from air pollution would accelerate the depreciation of health capital stock of people, which would drive them to increase their investment in health capital to cover the loss. As a result, their demand for commercial health insurance would expand. For another, air pollution makes people feel a sense of anxiety and unsafe (38, 39). For Residents with long-term exposure to air pollution, their anxiety would last and accumulate. Under this circumstance, people would tend to seek insurance to cover their potential loss as Maslow's needs theory suggest that insurance meets the need for security of people.
The heterogeneous factors are also considered in this study. First of all, it is found that urban and rural residents react differently to SO2 pollution. Second, regional heterogeneity also exists. Third, the effect of SO2 pollution also varies among households at different income levels. Last but not least, the gender of the household head affects the effect of SO2 pollution as well. Previous studies also provide some evidence on the heterogeneous effects. Geruso (40) reveals that the demand for health insurance differs between younger and elder consumers, and between men and women considering their difference in the potential medical expenditure. Other scholars experiment on the effect of risk attitude on the behavior of people for selecting health insurance (41). They find that the demand for health insurance of people is also affected by their risk attitude, and people are more likely to transfer their potential risk through insurance as risk awareness increase. In summary, besides regional disparity in air pollution degree, more individual factors should be considered to gain reasonable regression results of the effect.
To our knowledge, there are few studies on the effects of air pollution on household commercial health insurance purchasing. This paper conducts an empirical analysis based on the data from a micro database, which enriches the relevant studies of the exposome field. Furthermore, considering the regional disparity in the level of air pollution (42), the demand for commercial health insurance differs across regions. Insurance companies should consider environmental factors when pricing their products. Therefore, commercial health insurance with a reasonable price could be popularized by market forces and then help to promote public health. For another reason, facing the differences in individual characteristics, insurance companies should also tailor their products to meet specific health needs of people.
There are also some limitations in this paper. First of all, since there is a lack of data on air pollution, this paper selects the annual emission of SO2 pollutants only being the indicator of air pollution and mainly focuses on the effect of SO2 pollution on the commercial health insurance purchase behavior of households. However, SO2 is just one of the major air pollutants and it cannot reveal the whole effect of air pollution. Second, for privacy consideration, CHFS does not open its data on the location information of interviewee under provincial level. Therefore, this study has to define SO2 pollution at the provincial level, which might encounter measurement bias. Future researches on this topic could be conducted through the following directions. More air pollutants and their spatial factors should be considered to reach comprehensive and robust findings. How to establish an effective commercial insurance mechanism balancing its for-profit nature and its ability to promote public welfare could also be a far-reaching direction for future works.
Conclusion
In conclusion, based on the data from the 2017 CHFS, this paper employs a combination of the Probit and Tobit models to reveal the influence of air pollution, in particular, the SO2 pollution on household purchase of insurance. To address potential endogeneity issues, an instrumental variable of precipitation is utilized to conduct a 2SLS regression. Furthermore, considering insurance purchase behavior affected by multiple individual factors, we also perform a heterogeneity analysis to test the effects of SO2 pollution on different groups of residents. It is found that SO2 pollution has a significant positive effects on household commercial health insurance purchasing. Furthermore, the heterogeneity analysis shows that the effects differ across households with different characteristics including residential background, living regions, income level, and education level.
Data Availability Statement
All data generated or analyzed during this study will be made available by the authors. Further inquiries can be directed to the corresponding author.
Author Contributions
RW conceived of the presented idea and supervised the findings. LZ, TT, FY, and DW collected data and performed the computations. LZ and TT prepared the manuscript. All authors have made a substantial and intellectual contribution to this paper and approved it for publication.
Funding
This research was funded by the National Social Science Foundation of China (Grant No. 19BJY161), Key Program Provincial Education Department of Hunan Province (Grant No. 20A122), and Natural Science Foundation of Hunan Province (Grant No. 2021JJ30197).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We gratefully acknowledge the helpful suggestions of the reviewers, which have improved the paper.
References
1. Zeng H, Chen X, Xiao X, Zhou Z. Institutional pressures, sustainable supply chain management, and circular economy capability: empirical evidence from Chinese eco-industrial park firms. J Cleaner Prod. (2017) 155:54–65. doi: 10.1016/j.jclepro.2016.10.093
2. Chen X, Yi N, Zhang L, Li D. Does institutional pressure foster corporate green innovation? Evidence from China's top 100 companies. J Cleaner Prod. (2018) 188:304–11. doi: 10.1016/j.jclepro.2018.03.257
3. Fotourehchi Z. Health effects of air pollution: an empirical analysis for developing countries. Atmos Pollut Res. (2016) 7:201–6. doi: 10.1016/j.apr.2015.08.011
4. Liu W, Xu Z, Yang T. Health effects of air pollution in China. Int J Environ Res Public Health. (2018) 15:1471. doi: 10.3390/ijerph15071471
5. Anderson ML. As the wind blows: the effects of long-term exposure to air pollution on mortality. J Eur Econ Assoc. (2020) 18:1886–927. doi: 10.1093/jeea/jvz051
6. Li H, Chen R, Meng X, Zhao Z, Cai J, Wang C, et al. Short-term exposure to ambient air pollution and coronary heart disease mortality in 8 Chinese cities. Int J Cardiol. (2015) 197:265–70. doi: 10.1016/j.ijcard.2015.06.050
7. Li D, Cao C, Zhang L, Chen X, Ren S, Zhao Y. Effects of corporate environmental responsibility on financial performance: The moderating role of government regulation and organizational slack. J Cleaner Prod. (2017) 166:1323–34. doi: 10.1016/j.jclepro.2017.08.129
8. Zou B, You J, Lin Y, Duan X, Zhao X, Fang X, et al. Air pollution intervention and life-saving effect in China. Environ Int. (2019) 125:529–41. doi: 10.1016/j.envint.2018.10.045
9. Yang Z, Song Q, Li J, Zhang Y, Yuan XC, Wang W, et al. Air pollution and mental health: the moderator effect of health behaviors. Environ Res Lett. (2021) 16:44005. doi: 10.1088/1748-9326/abe88f
10. Gharehchahi E, Mahvi AH, Amini H, Nabizadeh R, Akhlaghi AA, Shamsipour M, et al. Health impact assessment of air pollution in Shiraz, Iran: a two-part study. J Environ Health Sci Eng. (2013) 11:1–8. doi: 10.1186/2052-336X-11-11
11. Khaniabadi YO, Daryanoosh SM, Hopke PK, Ferrante M, De Marco A, Sicard P, et al. Acute myocardial infarction and COPD attributed to ambient SO2 in Iran. Environ Res. (2017) 156:683–7. doi: 10.1016/j.envres.2017.04.028
12. Wu C, Yan Y, Chen X, Gong J, Guo Y, Zhao Y, et al. Short-term exposure to ambient air pollution and type 2 diabetes mortality: a population-based time series study. Environ Pollut. (2021) 289:117886. doi: 10.1016/j.envpol.2021.117886
13. Williams AD, Kanner J, Grantz KL, Ouidir M, Sheehy S, Sherman S, et al. Air pollution exposure and risk of adverse obstetric and neonatal outcomes among women with type 1 diabetes. Environ Res. (2021) 197:111152. doi: 10.1016/j.envres.2021.111152
14. Grossman M. On the concept of health capital and the demand for health. J Politic Econ. (1972) 80:223–55. doi: 10.1086/259880
15. Yang J, Zhang B. Air pollution and healthcare expenditure: implication for the benefit of air pollution control in China. Environ Int. (2018) 120:443–55. doi: 10.1016/j.envint.2018.08.011
16. Shen JS, Wang Q, Shen HP. Does industrial air pollution increase health care expenditure? Evidence from China. Front Public Health. (2021) 9:632. doi: 10.3389/fpubh.2021.695664
17. Liao L, Du M, Chen Z. Air pollution, health care use and medical costs: evidence from China. Energy Econ. (2021) 95:105132. doi: 10.1016/j.eneco.2021.105132
18. Yazdi SK, Khanalizadeh B. Air pollution, economic growth andhealth care expenditure. Ekonomska Istraivanja. (2017) 30:1181–90. doi: 10.1080/1331677X.2017.1314823
19. An J, Heshmati A. The relationship between air pollutants and healthcare expenditure: empirical evidence from south korea. Environ Sci Pollut Res Int. (2019) 26:31730–51. doi: 10.1007/s11356-019-06145-3
20. Graff Zivin J, Neidell M. Environment, health, human capital. J Econ Literat. (2013) 51:689–730. doi: 10.1257/jel.51.3.689
21. Woolhandler S, Himmelstein DU. The relationship of health insurance and mortality: is lack of insurance deadly? Ann Intern Med. (2017) 167:424–31. doi: 10.7326/M17-1403
23. Zhao W. Effect of air pollution on household insurance purchases. evidence from China household finance survey data. PLoS One. (2020) 15:e0242282. doi: 10.1371/journal.pone.0242282
24. Chen F, Chen Z. Air pollution and avoidance behavior: a perspective from the demand for medical insurance. J Cleaner Product. (2020) 259:120970. doi: 10.1016/j.jclepro.2020.120970
25. Kou D. Industrial specialization agglomeration, diversified agglomeration and environmental pollution: an empirical analysis based on panel data of 285 cities in China. J Yunnan Univ Finance Econ. (2020) 36:3–17. doi: 10.16537/j.cnki.jynufe.000622
26. Chen R, Huang W, Wong CM, Wang Z, Thach TQ, Chen B, et al. Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: the China air pollution and health effects study (CAPES). Environ Res. (2012) 118:101–6. doi: 10.1016/j.envres.2012.07.003
27. Andronache C. Estimated variability of below-cloud aerosol removal by rainfall for observed aerosol size distributions. Atmos Chem Phys. (2002) 2:133–45. doi: 10.5194/acpd-2-2095-2002
28. Chate DM, Murugavel P, Ali K, Tiwari S, Beig G. Below-cloud rain scavenging of atmospheric aerosols for aerosol deposition models. Atmos Res. (2011) 99:528–36. doi: 10.1016/j.atmosres.2010.12.010
29. Tai A, Mickley LJ, Jacob DJ. Correlations between fine particulate matter (PM2.5) and meteorological variables in the United States: implications for the sensitivity of PM2.5 to climate change. Atmos Environ. (2010) 44:3976–84. doi: 10.1016/j.atmosenv.2010.06.060
30. Kampa M, Castanas E. Human health effects of air pollution. Environ Pollut. (2008) 151:362–7. doi: 10.1016/j.envpol.2007.06.012
31. Chen X, Wang X, Huang JJ, Zhang LW, Song FJ, Mao HJ, et al. Nonmalignant respiratory mortality and long-term exposure to PM10 and SO2: a 12-year cohort study in northern China. Environ Pollut. (2017) 231:761–7. doi: 10.1016/j.envpol.2017.08.085
32. Gu H, Cao Y, Elahi E, Jha SK. Human health damages related to air pollution in China. Environ Sci Pollut Res Int. (2019) 26:13115–25. doi: 10.1007/s11356-019-04708-y
33. Deschenes O, Greenstone M, Shapiro JS. Defensive investments and the demand for air quality: evidence from the NOx budget program. Am Econ Rev. (2017) 107:2958–89. doi: 10.1257/aer.20131002
34. Yang T, Liu W. Does air pollution affect public health and health inequality? Empirical evidence from China. J Cleaner Product. (2018) 203:43–52. doi: 10.1016/j.jclepro.2018.08.242
35. Chang TY, Huang W, Wang Y. Something in the air: pollution and the demand for health insurance. Rev Econ Stud. (2018) 85:1609–34. doi: 10.1093/restud/rdy016
36. Brunekreef B, Holgate ST. Air pollution and health. Lancet. (2002) 360:1233–42. doi: 10.1016/S0140-6736(02)11274-8
37. Chen TM, Kuschner WG, Gokhale J, Kuschner WG. Outdoor air pollution: nitrogen dioxide, sulfur dioxide, and carbon monoxide health effects. Am J Med Sci. (2007) 333:249–56. doi: 10.1097/MAJ.0b013e31803b900f
38. Xue T, Zhu T, Zheng Y, Zhang Q. Declines in mental health associated with air pollution and temperature variability in China. Nat Commun. (2019) 10:2165. doi: 10.1038/s41467-019-10196-y
39. Tzivian L, Winkler A, Dlugaj M, Schikowski T, Vossoughi M, Fuks K, et al. Effect of long-term outdoor air pollution and noise on cognitive and psychological functions in adults. Int J Hyg Environ Health. (2015) 218:1–11. doi: 10.1016/j.ijheh.2014.08.002
40. Geruso M. Demand heterogeneity in insurance markets: implications for equity and efficiency. Quantit Econ. (2017) 8:929–75. doi: 10.3982/QE794
41. Kairies-Schwarz N, Kokot J, Vomhof M, Wessling J. How Do Consumers Choose Health Insurance?-An Experiment on Heterogeneity in Attribute Tastes and Risk Preferences. An Experiment on Heterogeneity in Attribute Tastes and Risk Preferences (December 17, 2014). Ruhr Economic Paper. (2014). doi: 10.2139/ssrn.2579733
Keywords: SO2 pollution, commercial health insurance, residential health behavior, micro-data, discrete model
Citation: Wang R, Zhang L, Tang T, Yan F and Jiang D (2021) Effects of SO2 Pollution on Household Insurance Purchasing in China: A Cross-Sectional Study. Front. Public Health 9:777943. doi: 10.3389/fpubh.2021.777943
Received: 16 September 2021; Accepted: 08 October 2021;
Published: 25 November 2021.
Edited by:
Ruixue Huang, Central South University, ChinaReviewed by:
Shih-Chieh Chang, National Chengchi University, TaiwanYuan Zheng, Anhui University of Finance and Economics, China
Copyright © 2021 Wang, Zhang, Tang, Yan and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ting Tang, dGFuZ3Rpbmc2MjhAMTYzLmNvbQ==