 Li-Li Zhou1†
Li-Li Zhou1† Shu-E Zhang2†
Shu-E Zhang2† Jiao Liu3Hong-Ni Wang4
Jiao Liu3Hong-Ni Wang4 Li Liu5
Li Liu5 Jing-Jing Zhou6Zhi-Hua Bu5
Jing-Jing Zhou6Zhi-Hua Bu5 Yu-Fang Gao7
Yu-Fang Gao7 Tao Sun4*†
Tao Sun4*† Bei Liu8*†
Bei Liu8*†- 1Department of Urology, The Second Affiliated Hospital, Harbin Medical University, Harbin, China
- 2Department of Health Management, School of Health Management, Harbin Medical University, Harbin, China
- 3Department of Respiratory Medicine, Third Affiliated Hospital, Harbin Medical University, Harbin, China
- 4Department of Health Policy and Management, School of Public Health, Hangzhou Normal University, Hangzhou, China
- 5Department of Nephrology, Second Affiliated Hospital of Harbin Medical University, Harbin, China
- 6Department of Endocrinology, Second Affiliated Hospital of Harbin Medical University, Harbin, China
- 7Institute of Hospital Management, Qingdao University, Qingdao, China
- 8Department of Inspection, School of Public Health, Peking University, Beijing, China
Background: To investigate the prevalence of burnout syndrome among Chinese female nurses during the controlled coronavirus disease 2019 (COVID-19) period and explore its associated socio-demographic factors and job characteristics.
Methods: With the multistage, stratified sampling method, a cross-sectional online survey was conducted from September to October 2020 in China. The survey tool included revised Maslach Burnout Inventory (MBI) with 15 items, socio-demographic and job characteristics. Univariate logistic regression analysis and multivariate factor logistic regression analysis were used to identify the risk factors for burnout of female nurses.
Results: During controlled COVID-19 period in China, the overall prevalence of burnout symptoms among Chinese female nurses was 60.2% with a breakdown in severity as follows: 451 (39.8 %) mild, 163 (14.4%) moderate, and 68 (6.0%) severe burnout. Little variance was reported for burnout symptoms according to job tenure (Waldχ2 = 14.828, P < 0.05,odds ratio [OR] <1), monthly salary income (Waldχ2 = 12.460, P < 0.05, OR <1), and night shift (Waldχ2 = 3.821, P < 0.05, OR > 1).
Conclusion: Burnout symptoms among Chinese female nurses were prevalent and associated with job tenure, monthly salary income, and night shift. Female nurses who were with shorter job tenure, worked at night shifts, and had lower monthly salaries tended to exhibit increasing high-level burnout than their counterparts. This study serves as an implication for administrators and policy-makers to improve the work conditions of nurses for promoting overall healthcare service quality.
Background
Recently, WHO declared burnout as an “occupational phenomenon” in the International Classification of Diseases 11th revision (ICD-11), recognizing burnout as a new public health concern (1). A previous study confirmed (2) that burnout affected the physical and mental health of nurses, quality of nursing care, and conditions and recovery of patients. Burnout is described as a psychological syndrome involving feelings of emotional fatigue, depersonalization (DA), a sense of reduced personal accomplishment (PA), and poor self-efficacy secondary to occupational stress (3, 4). According to Maslach et al., burnout consists of three dimensions involving emotional exhaustion (EE), DA and cynicism, and reduced PA (3). EE refers to the feelings of being overextended emotionally and physically and depleted of personal energy (3). DA means a cynical and distant attitude toward one's duties and tasks. Reduced PA is the tendency to negatively evaluate their own achievements at work (3).
The concept of burnout originated from the field of human service in which professionals contact with other people as the majority of their tasks and which can become a source of stress (5, 6). In recent years, nursing staff regarded as a high-risk and particularly vulnerable population for suffering burnout, are experiencing exceptional challenges worldwide within the current turbulent healthcare system due to these dilemmas, such as limited health resources, staff shortages, overworked, and overloaded (7). Moreover, tense nurse-patient relationships, frequent nurse-patient conflicts, and workplace violence contribute to extensive depressive symptoms and occupational stress for nurses and further resulting in suffering burnout (8). Various studies have been undertaken to evaluate the prevalence of burnout in high-income countries among nurses ranged from 33 to 50% (2, 9–11). The latest evidence found that the prevalence of burnout among nurses has been increasing at an alarming rate in low-income and moderate-income countries, with a previous study reported exceeding 60% in China (12, 13).
Particularity, the coronavirus disease 2019 (COVID-19) outbreak became a public health emergency of international concern (PHEIC) on January 30, 2020 (14). Being the largest part of the healthcare workforce against the epidemic, the hospital industry is facing greater challenges as a result of the increased work stress, highest risk, and heavier workload during the COVID-19 epidemic (15), which potentially contribute to the increased high risk of burnout. However, actions and behaviors of nurses toward the COVID-19 epidemic have attracted intense approval from the public and the media (16), as social support, which may contribute to a positive function related to alleviate the intensive relationship between nurses and patients and increase professional identity and calling of nurses, thereby resulting in decreased nurses burnout. Unfortunately, the limited available literature reported the prevalence of burnout among nurses is still conflicting (17). During the initial and the most severe phase of the COVID-19 epidemic in China, one study reported a high-level prevalence of burnout among Chinese front-line nurses against the epidemic (18). Contrarily, another survey conducted in China showed that nurses who worked in COVID-19 wards had lower burnout symptom than those worked in usual wards (19). The generalizability of findings regarding the prevalence of burnout is inconsistent, since the study was conducted on different stages of the COVID-19 epidemic, and a convenience sample of participating by social media, and varied working demands (20, 21). Therefore, this study believes that the prevalence of burnout of Chinese nurses is of worry and needs to be assessed further during different stages of the COVID-19 epidemic.
Previous studies widely confirmed that burnout was associated with negative attitudes toward work and life (22), such as generating physical symptoms of fatigue, anxiety, and so on, resulting in various forms of job withdrawal behavior and affecting work engagement and quality of nursing care (23) and even fundamental functionality of healthcare systems (24). Given that the mass potentially negative impacts of burnout on both the health and quality of patient care, the driving factors of the rising burnout issue had been paid more attention. Based on previous literature, several demographic and job characteristics were suggested to be associated with burnout among medical staffs, such as age (25), sex (25), job tenure, work hours education level (26), professional titles (27), and so on. However, overall evidence on demographic and job factors of burnout among nurses was inconclusive (28) in different space-time settings and deserves a wide range of attention.
Moreover, the study of gender differences has been historically controversial in previous scientific research (29, 30). Female has changed the role of women in society through progressively entering the workforce and expanding their aspirations in different settings (31). Nursing is a female-subjugated profession with undergoing common work-family conflict and high workload (32). Female nurses are more vulnerable to burnout and psychological distress (33), which tend to cause direct and indirect negative consequences for both patients and themselves. Therefore, it is significant and valuable to explore burnout in female nursing viewpoint, especially in the COVID-19 special period. In relation to burnout specifically, experienced difference between males and female is existent. A meta-analysis showed that females were more likely to be emotionally exhausted than men, whereas males were more likely to report DA than females (29). A previous study drew attention to recognize the differences in burnout between sexes and then required different help and organizational support strategies in dealing with burnout issues (29). In fact, data concerning burnout of female nurse are inconclusive (29). Therefore, considering that gender role interferes with burnout assessment and females are over-represented in disorders, the current study focuses on the prevalence of burnout syndrome of female nurses and tries to accurately identify its association with social-demographic factors and job characteristics. Besides, the COVID-19 period as a special contextual factor is also discussed in the study.
Aim
The major aims of the present study were to (1) address the prevalence of burnout syndrome among Chinese female nurses during the controlled COVID-19 period and (2) to explore its association with socio-demographic factors and job characteristics.
Methods
Subjects and Procedures
We used both multistage-stratified sampling and convenient sampling methods to collect data, a total of 100 cities and 1,740 nurses were randomly selected. The Chinese mainland consists of 32 provinces, which were divided into five regions according to geographical location: eastern, western, southern, northern, and central regions. In each region, 20 cities were randomly selected. An anonymous online survey was completed by a representative group of nurses across 100 cities in 31 provinces in China from September to October 2020 (a controlled COVID-19 period in China). In the second stage of sampling, the nurses who were originally selected were appointed to deliver the questionnaires to other nurses. The selected nurse was invited to click on a webpage link to access a self-administered questionnaire (https://www.wenjuan.com/). Subsequently, the web page link was sent by the deliverers to other nurses via mobile phones. The investigation purpose and significance of this study are shown on the front page of the self-administered questionnaire. The progress of the survey was monitored by the authors. Eventually, we checked the accuracy and completeness of the data and excluded the questionnaire. All data were checked for consistency by the two authors. A total of 1,740 nurses completed their questionnaires, resulting in 1,133 valid questionnaires, with an effective completion rate of 70.13%. The distribution of demographic variables (gender, age, and level of education) of the representative nurses is comparable to the general population of the Chinese registered nurses. The inclusion criteria were recognized as (1) being a registered nurse; (2) being currently enrolled in nursing; (3) gender is female; and (4) consent and voluntary participation in our study.
Measures
Measurement of Demographic Characteristics
In the current study, five demographic variables were collected, such as gender, age, marital status, education level, and parental status. Marital status was divided into three categories: unmarried, married, and divorced or loss of a spouse. In China, one is qualified as a nurse only if who has at least a technical secondary education from a nursing school and has passed Nurse Professional Qualification Examination. Thus, options for educational level included “technical secondary school”, “college degree”, “bachelor's degree”, and “master's degree or above”. Parental status was divided into four categories “no child”, “0–5 years”, “6–18 years”, “19 and above years”.
Measurement of Job Characteristics
In the current study, four variables were utilized to assess job characteristics, such as monthly salary income, professional categories, job tenure, and work shift. Professional categories were divided into “nurse”, “senior nurse”, “nurse-in-charge”, and “associate professor of nursing/professor of nursing”. Both “nurse” and “nurse practitioner” are defined as the primary professional title, “nurse-in-charge” as the intermediate professional title, and associate professor of nursing/professor of nursing as the senior professional title in China. Nursing students are graduated from technical secondary nursing school or are graduated from senior high school entrance exam, educational system is divided into 3, 4 years, two kinds of graduates are eligible to become a certified registered nurse after graduation.
The night shift was divided into “yes” or “no”. Monthly income (RMB) was categorized as “3,000 or below”, “3,001–5,000 yuan”, “5,001–7,000 yuan”, “7,001–9,000 yuan”, and “9,001 or above yuan” (1 Yuan ≈ 0.1566 Dollar, 0.1139 Pound, 0.1345 Euro, in October 2021). Using the domestic working-hour standard in China as the cut point, weekly work time was divided into ≤ 40 hours/week and >40 hours/week. Job tenures were divided into categories, such as “1–3”, “4–5”, “6–10”, and “11–20” years. Consider that the employees are more likely to be troubled by stressors (34) even leave their first job (35) in the early career. The demanding and overwhelming experience and work-life interference are important factors influencing new graduate nurse burnout (34, 35). Thus, Relationship between job tenures and burnout is more sensitive to terms. Participants with 1–3 years of job tenures should be considered as new nurses who are a particular group with little working experience, who are prone to have a greater risk of suffering burnout. In comparison, as a similar group with shorter job tenure, participants with 4–5 working experiences should have possessed vocational adaptability.
Measurement of Burnout
The MBI (6) with 15 revised items was used to measure the three dimensions of burnout (EE, DA, and reduced PA) translated by Li et al. (36). Items were scored on a seven-point Likert scale ranging from 0 (totally disagree) to 6 (totally agree) where higher scores represented a higher degree of burnout. This burnout inventory in medical settings was demonstrated to have good reliability and validity in the Chinese context. The Chinese version of Maslach's cut-off scores (37) for EE, DA, and PA is 25, 11, and 16, respectively. According to the scores for these three dimensions, the model then divides burnout into four levels in Table 1. In the current study, reliability measured by Cronbach's alpha coefficient for the whole burnout, EE, DA, and reduced PA in this study were 0.928, 0.985, 0.938, and 0.900, respectively.
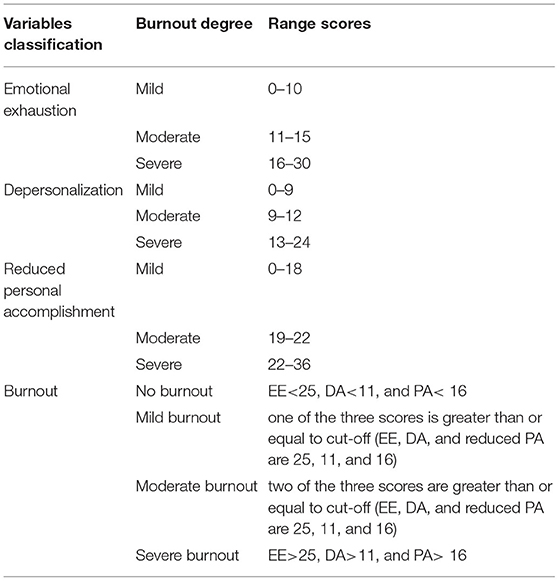
Table 1. The cut-off scores for burnout three dimensions.
Statistical Analysis
Statistical significance was considered as a two-tailed p-value < 0.05. All analyses were conducted using SPSS version 22.0 (IBM, BM SPSS Statistics for Windows). Demographic factors and job characteristics had been defined as independent variables, and total burnout had been defined as a dependent variable. Univariate and multivariate logistic regression analyses as the main statistical analysis methods were performed in the current study.
Results
Demographic Information for Samples
The age of the participants ranged from 20 to 55 years. Most (77.00%) participants had bachelor's degree and above. Of the 1,133 sampled nurses, 45.1% of them were unmarried, approximately 53.3% were married, and 1.6% were divorced or had loss of a spouse. Approximately 27.7% of them belonged to the primary professional category. Furthermore, a total of 529 nurses (46.7%) worked less than 6 years. Moreover, 74.8 and 32.2% of them experienced night-shifts work and worked 40 hours/week, respectively. Moreover, 27.19% had a monthly income within 2,001–5,000 RMB, as shown in Table 2.
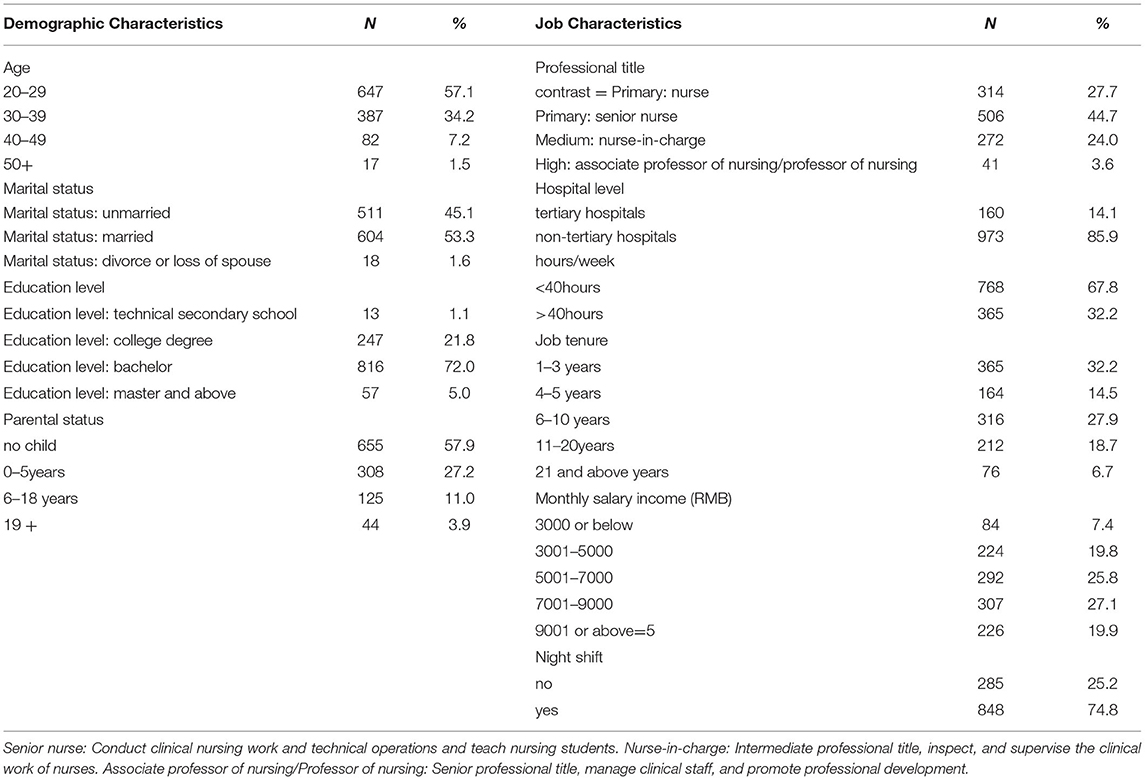
Table 2. The list of demographic and job characteristics of the participants.
The Incidence of Burnout and the Three Dimensions
The status of burnout of female nurses is shown in Table 3. Among 1,133 participating Chinese female nurses, a total of 782 reported experiencing varying degrees of burnout over the 2 weeks. The overall prevalence of all degrees of burnout was 60.20%, and the breakdown according to severity is as follows: 451 (39.8 %) mild, 163 (14.4%) moderate, and 68 (6.0%) severe burnout.
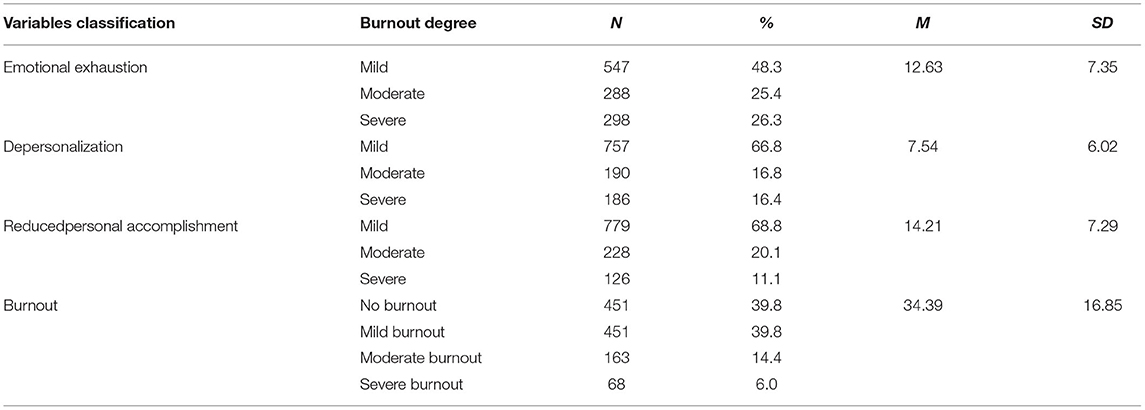
Table 3. Values are numbers (percentages) of respondents regarding burnout (n = 1,133).
Total Burnout-Univariate Analysis
The analysis of the factors influencing burnout of Chinese female nurse is shown in Tables 4, 5. One of the classification variables was intentionally set as a “dummy” variable. Univariate logistic regression analysis of the development dataset included in the equation was as follows: (1) burnout as dependent variable (never = 0, exist = 1); (2) age of nurse (20–29 = 1, 30–39 = 2, 40–49 = 3, 50+ = 4); (3) marital status (unmarried = 1, married = 2, divorced or loss of a spouse = 3); (4) education level (technical secondary school= 1, college degree = 2, bachelors = 3, master degree, or above = 4); (5) parental status was divided into four categories (no child = 1, 0–5years = 2, 6–18 years = 3, 19, and above years = 4). (6) Professional title (primary: nurse = 1, primary: senior nurse = 2, medium: nurse-in-charge = 3, high: associate professor of nursing/professor of nursing = 4); (7) hospital level (tertiary hospitals = 1, non-tertiary hospitals = 2); and (8) hours/week (≤ 40 hours/week = 1, >40 hours/week = 2). (9) Job tenure (1–3 years = 1, 4–5 years = 2, 6–10 years = 3, 11–20 years = 4, 21, and above years = 5); (10) monthly salary income (RMB) (3,000 or below = 1, 3,001–5,000 = 2, 5,001–7,000 = 3, 7,001–9,000 = 4, 9,001 or above = 5); (11) night shifts (no = 1, yes = 2). According to our results, most female nurses (61.20%) exhibited varying degrees of burnout. Compared to female nurses aged 20–29 years old, female nurses aged 40–49 were not as prone to burnout. Age (Waldχ2 = 14.562, P < 0.01, OR <1), parental status (Waldχ2 = 17.688, P < 0.05, OR <1), professional title (Waldχ2 = 12.748, P < 0.01, OR <1), working hours (Waldχ2= 4.466, P < 0.05, OR > 1), job tenure (Waldχ2 = 28.826, P < 0.05, OR > 1), monthly salary income (RMB) (Waldχ2 = 13.692, P < 0.05, OR > 1), and night shifts (Waldχ2 = 5.341, P < 0.05, OR > 1) were the factors associated with burnout. These seven factors were then entered into the multivariate logistic regression model.
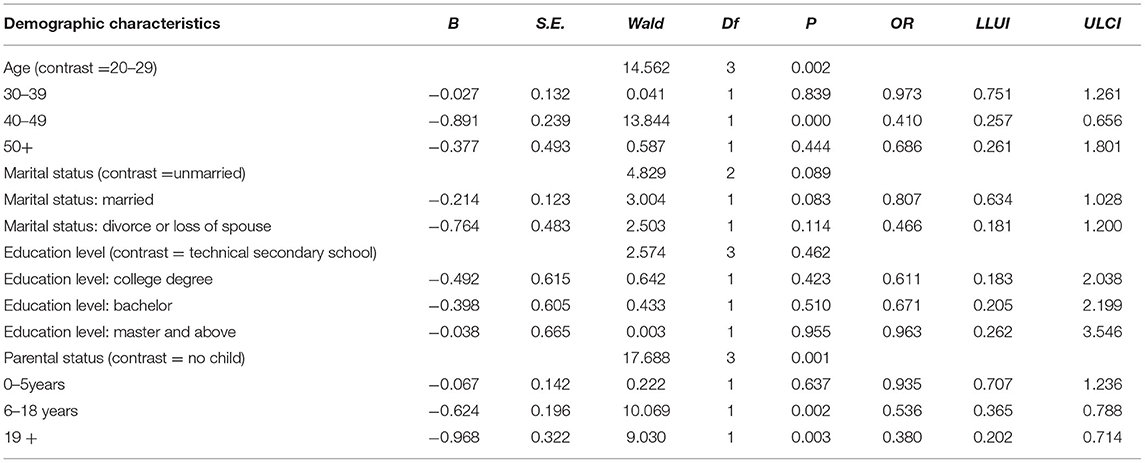
Table 4. Univariate logistic regression analysis of respondents (n = 1,133).
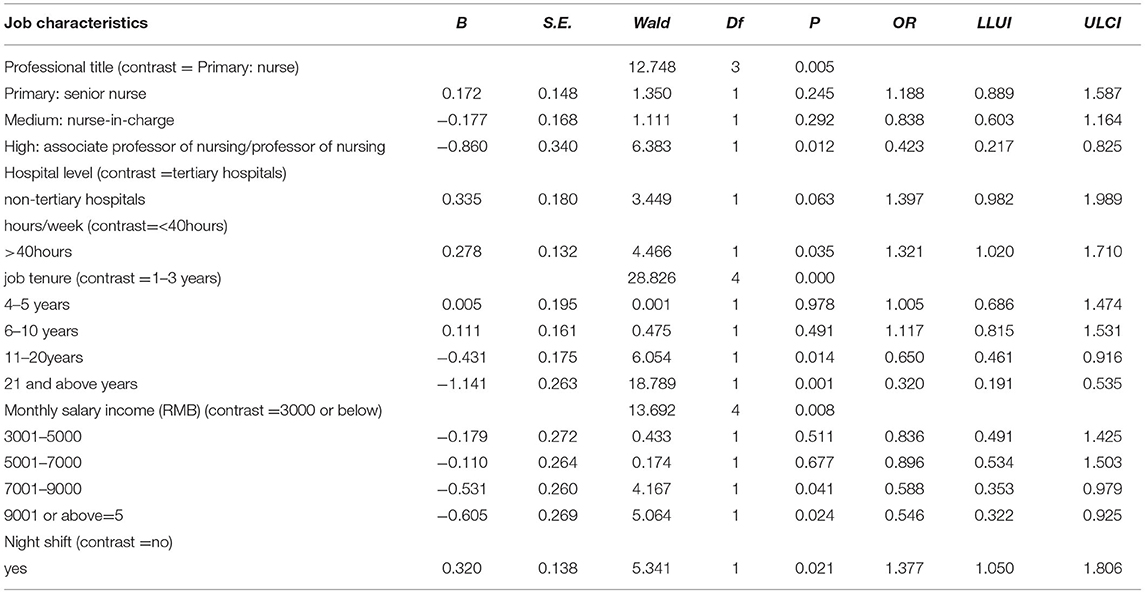
Table 5. Univariate logistic regression analysis of respondents (n = 1,133).
Total Burnout-Multivariate Analysis
Further screening of the seven factors influencing burnout of female nurses is shown in Table 6. We analyzed the four factors selected by the univariate logistic regression analysis using multivariate factor logistic regression analysis. According to Table 4, the result of the significance test of the whole regression model is X2 = 60.991 (P = 0.001, P < 0.01), while the result of the Hosmer-Lemeshow test is 2.132 (P = 0.459, P > 0.05); therefore, these regression models were optimal. As shown in Table 4, the results of the tests concerning the variables of job tenure (Waldχ2 = 14.828, P < 0.05, OR <1), night shift (Waldχ2 = 3.821, P < 0.01, OR > 1), and monthly salary income (RMB) (Waldχ2 = 12.460, P < 0.01, OR <1) were significant, suggesting that these factors are the significant predictors of burnout among female nurses.
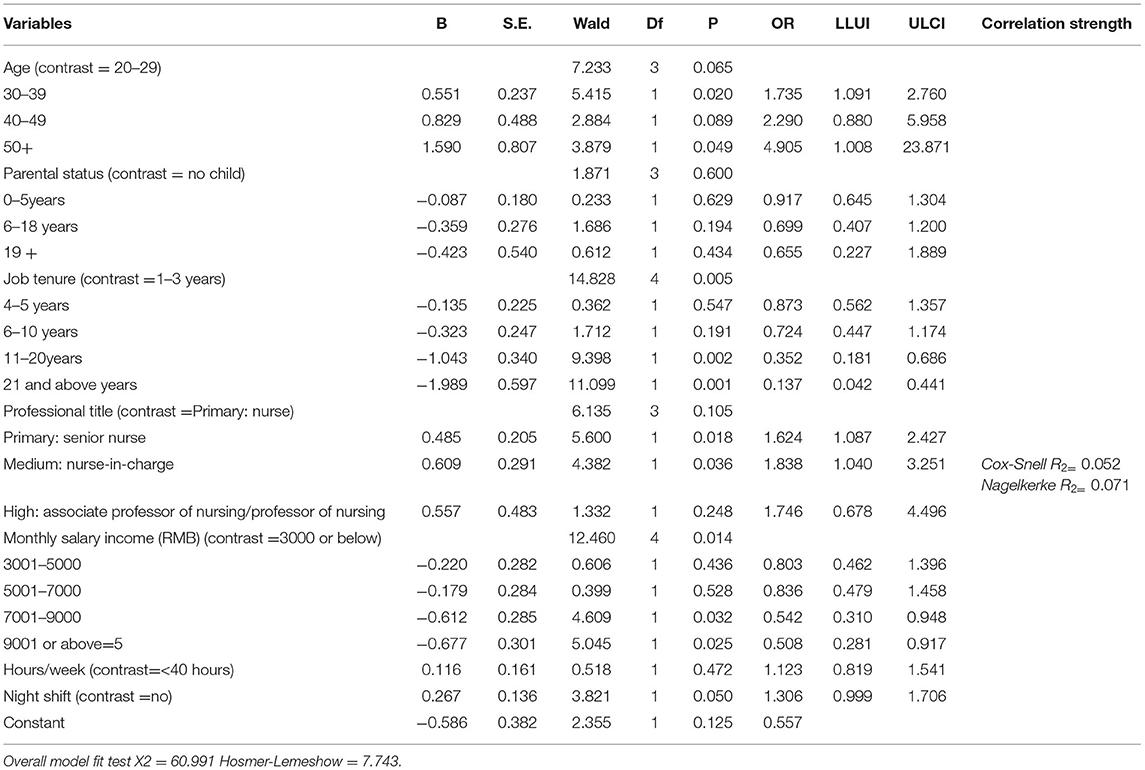
Table 6. Multivariate logistic regression analysis of respondents (n = 1,133).
Discussion
Prevalence of Burnout Among Chinese Female Nurses During the Controlled COVID-19 Period
The burnout incidence in female nurses during the controlled COVID-19 period was 60.20%, with a breakdown in severity as follows: 451 (39.8 %) mild, 163 (14.4%) moderate, and 68 (6.0%) severe burnout, which was slightly lower than the initial stage of COVID-19 outbreak and slightly lower than that of predating COVID-19 ones (13). The current study on burnout in Chinese female nurses reported that 26.3% with high EE, 16.4% with high levels of DA, and 11.1% with low levels of personal achievement respectively among the participates. During the period of the COVID-19 outbreak, the anti-epidemic efforts of female nurses were positively evaluated by the public and media in China, which heartened the sense of achievement, career identity, and high-level self-recognition of female nurses, thus showing a decreased EE and less DA but more PA (38). Compared with Chinese doctors (21, 39), the overall prevalence of burnout of female nurses was lower involved less EE and less DA but more personal accomplishment. The study supports the view that burnout is still a common prevalence and worrying phenomenon in female nursing. In China, due to the increased contradictions between nursing care and expectation of patients (40), the exceeding work-family conflicts and work stress have been increasing especially in female nurses (41), resulting in a variety of potentially fatigued or hazardous circumstances for female nurses. Therefore, strategies, such as increasing job resources (42), designedly allocated to female nurses and establishing a supportive work environment (43) and organizational culture should be encouraged to prevent burnout among female nurses in China.
Risk Factors Influencing Burnout of Chinese Female Nurse
A previous study showed that age, gender, marital status, parental status, and professional title affected the incidence of burnout of female nurses (44). However, our study found that job characteristics, such as job tenure, monthly salary income, and night shift, were closely linked to the level of burnout, rather than age, marital status, and other demographic characteristics. The current study further confirmed that female nurses with shorter job tenure showed a greater vulnerability toward suffering burnout than those with longer job tenure. Compared to broad experienced female nurses, new female nurses may initially feel inadequately prepared for their occupational role, especially at the early stages of a career that often be known as the most stressful, frustrating, discouraging, and disillusioning stage for individual employees, which is also the process of ongoing professional role adaptation and identity crisis (45, 46). For female nurses with shorter job tenure, the experience of transition from school-based experience to professional practice can be stressful compounded by entrenched systemic issues, such as working irregular hours, rotating shifts, and under staffing (45). Being shorter job tenure, those nurses do not yet possess solid interpersonal and workplace relationships that are conducive to destroy intrapersonal psychological capital against burnout (47). Therefore, much more attention should be paid to that new female nurse is suffering from high-level burnout.
A previous study proved that inadequate sleep was associated with increasing burnout in shift working occupations (48). The current findings showed that working on night shifts is also one risk factor for female nurses suffering burnout rather than their weekly work hours. As an inevitable work type for providing in-patient nursing care, night shifts for female nurses were associated with more reports of heavy burnout symptoms (49, 50). A nurse working irregular shifts was more likely to lead to inadequate sleep (51), irregular habits and lifestyles (52), and change in sleep blood pressure (50), which in turn may explain the increased overall burnout risk among female nurses compared with those working daily (50). Inadequate sleep caused by irregular shifts might destroy accessibility and ability of female nurses to recover from fatigue caused by heavy duty and workplace demands, potentially resulting in the heightened burnout risk in those reporting irregular shifts (48). Unlike the western countries, the shortage of nurses in China is more serious due to the huge China population base and inefficient health service systems (53), thereby the nurses have been encountered heavier workload and more frequent irregular shifts, resulting in a range of serious consequences, such as sleep disorder and physical damage for a long time (54). Although shift work is unavoidable for a nursing career, it is valuable for a manager that optimizing shift arrangement in relation to control over overtime should be explored as one of the key intervention to prevent the high-level burnout among female nurses, thereby concentrating on improved health and wellness for female nurses and in turn enhanced patient care quality.
Female nurses with lower monthly salary income were more likely to report severe burnout than that those with higher monthly salary income, which seems to be at coherent with previous findings (55). To some extent, low salary is one of the key predictor for a high risk of burnout among female nurses might as a result of perceived disproportion between job resources and demands (56, 57). Perceived unreasonable revenue as an important determinant factor for female nurses is likely to lead to decreased motivation and job satisfaction and then resulting in high-level burnout (58), which also reversely interpreted that the participating female nurses in this study who reported high-level salary tend to feel less emotionally exhausted and less depersonalized but more personally accomplished. Besides, another reason might be that the general judgment indicator of PA of female nurses was determined by the money their earn (59). Previous studies revealed that Chinese nurses are dissatisfied with their salary (60), working environment, and nurse-patient relationships. Moreover, compared to the pre-COVID-19 epidemic stage, work pattern and workflow of nurse are completely different from the usual during controlling the COVID-19 epidemic. According to the current study, the finding suggested that 32.2% of the participants had hours/week more than 40 hours/week, indicating that nearly a third of the participants had complained the long working hours during the controlled COVID-19 period. In this stage, Chinese nurses are facing various huge challenges, such as increased the long working hours, extra effort, heavily workload, stress, new risk, and so on (20, 53). Except for front-line wards nurses, the majority of Chinese nurse's salary did not increase due to decreased hospital economic benefit during a fight against the COVID-19 epidemic period, which contributes to the effort-reward imbalance at work being more serious. Therefore, it is important for nurse administrators and managers to enable female nurses to alleviate work-related burnout symptoms through matching reasonably economic, physical, and emotional resources (61). The last evidence from The Dresden Burnout Study (DBS) is a 12-year longitudinal cohort study that aims to provide a description of the burnout syndrome on the basis of time and symptom criteria with a special focus on the search for biomarkers (62) indicated that providing work environments where high efforts are always linked with high rewards, such as economic, physical, and emotional resources, have to be considered an important issue for avoiding burnout (63).
Limitations
In the current study, the findings need to be discussed with respect to certain limitations. First, data were collected through an online survey, which is prone to lead to response bias due to social desirability or negative effect. Second, although these efforts had been tried to ensure a representative sample and although there were no significant differences across data collection regions, we must acknowledge that the effective response rate was not ideal. Third, a cross-sectional design cannot determine a cause-effect relationship among the studied variables. Further experimental design is needed to test the cause-effect relationships across different cultural contexts. Forth, due to the substantial existence of income differences between the eastern and western areas in China, the categories of monthly salary incomes in our study only represent ordinal variables, which cannot explain the impact of the differences of real income between regions on burnout. Fifth, the multicollinearity problem is a substantial existence in our study, which potentially leads to skewed or misleading results when the current study attempts to determine how well each independent variable can be used most effectively to predict or understand the dependent variable in a statistical model. Last, burnout among nurses is constantly changing during the epidemic, but our study only focuses on a single time point in China from September to October 2020.
Conclusions
This study revealed the prevalence of burnout syndrome among female nurses (60.02%) during the controlled COVID-19 period. Female nurses reported that more of them were likely to experience higher incidence and more severity of EE than that of DA and reduced PA. Given the growing number of female nurses entering the field of healthcare service, much attention should be paid to their EE dimension. Furthermore, the interventions and prevention measures direct at female burnout should be strengthened and improved, especially during the controlled COVID-19 period, further rather than that be ignored. Females bring many innate qualities to their work as nurse, which affects burnout due to differentiated socio-demographic characters. Socio-demographic factors of female nurses, such as job tenure, salary income, and night shifts, accounted for only a small proportion of variance in the burnout of nurses in Chinese nurses during the controlled COVID-19 period. Shorter-tenure female nurses experienced a much higher level of burnout symptoms than that those with longer job tenure. Female nurses who worked at night shifts and had lower monthly salary tend to exhibit an increasing high risk of burnout. The current study suggests that hospital administrators and decision-makers should provide positive psychological support to avert and alleviate the burnout symptoms of female nurses during the controlled COVID-19 period, especially focusing on nurses who are younger, have lower salary, and have night shift.
Data Availability Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request from aHlkc3VudGFvQDEyNi5jb20=.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Harbin Medical University (ECHMU). Due to the anonymous survey approach, written informed consent could not be obtained. A verbal informed consent form was included at the beginning of the questionnaire. And the ECHMU had approved verbal consent for this study. Completing the questionnaire regarded as a verbal consent was therefore considered ‘informed consent' for participation in the survey. A verbal informed consent has been obtained from the participants to publish this paper.
Author Contributions
L-LZ, S-EZ, and TS conceived and designed the experiments. JL, H-NW, LL, Y-FG, J-JZ, and Z-HB performed the experiments. S-EZ and BL analyzed the data. JL, H-NW, and Y-FG contributed reagents, materials, analysis tools. L-LZ and S-EZ wrote the paper. BL and TS approved the final manuscript for publication. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We sincerely thank all participants who had contributed, particularly those who helped in collecting data, distributing questionnaires, and participated in our research.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.757113/full#supplementary-material
References
1. Krueger RB, Reed GM, First MB, Marais A, Kismodi E, Briken P. Proposals for paraphilic disorders in the international classification of diseases and related health problems, eleventh revision (ICD-11). Arch Sex Behav. (2017) 46:1529–45. doi: 10.1007/s10508-017-0944-2
2. Woo T, Ho R, Tang A, Tam W. Global prevalence of burnout symptoms among nurses: a systematic review and meta-analysis. J Psychiatr Res. (2020) 123:9–20. doi: 10.1016/j.jpsychires.2019.12.015
3. Maslach C, Leiter MP. The truth about burnout: how organizations cause personal stress and what to do about it. Psychiatr Rehabil J. (1997) 23:194. doi: 10.1037/h0095170
4. Pines A, Maslach C. Characteristics of staff burnout in mental health settings. Hosp Commun Psychiatr. (1978) 29:233–7. doi: 10.1176/ps.29.4.233
6. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. (2001) 52:397–422. doi: 10.1146/annurev.psych.52.1.397
7. Wang L, Chen H, Wan Q, Cao T, Dong X, Huang X, et al. Effects of self-rated workload and nurse staffing on work engagement among nurses: a cross-sectional survey. J Nurs Manag. (2021) 29:1329–37. doi: 10.1111/jonm.13274
8. Shi Y, Guo H, Zhang S, Xie F, Wang J, Sun Z, et al. Impact of workplace incivility against new nurses on job burn-out: a cross-sectional study in China. BMJ Open. (2018) 8:e020461. doi: 10.1136/bmjopen-2017-020461
9. Owuor RA, Mutungi K, Anyango R, Mwita CC. Prevalence of burnout among nurses in sub-Saharan Africa: a systematic review. JBI Evid Synth. (2020) 18:1189–207. doi: 10.11124/JBISRIR-D-19-00170
10. Dugani S, Afari H, Hirschhorn LR, Ratcliffe H, Veillard J, Martin G, et al. Prevalence and factors associated with burnout among frontline primary health care providers in low- and middle-income countries: a systematic review. Gates Open Res. (2018) 2:4. doi: 10.12688/gatesopenres.12779.1
11. Li H, Cheng B, Zhu XP. Quantification of burnout in emergency nurses: a systematic review and meta-analysis. Int Emerg Nurs. (2018) 39:46–54. doi: 10.1016/j.ienj.2017.12.005
12. Wang QQ, Lv WJ, Qian RL, Zhang YH. Job burnout and quality of working life among Chinese nurses: a cross-sectional study. J Nurs Manag. (2019) 27:1835–44. doi: 10.1111/jonm.12884
13. Hu Z, Wang H, Xie J, Zhang J, Li H, Liu S, et al. Burnout in ICU doctors and nurses in mainland China-A national cross-sectional study. J Crit Care. (2021) 62:265–70. doi: 10.1016/j.jcrc.2020.12.029
14. Dhama K, Khan S, Tiwari R, Sircar S, Bhat S, Malik YS, et al. Coronavirus disease 2019–COVID-19. Clin Microbiol Rev. (2020) 33:e00028–20. doi: 10.1128/CMR.00028-20
15. Huang L, Lin G, Tang L, Yu L, Zhou Z. Special attention to nurses' protection during the COVID-19 epidemic. Crit Care (London, England). (2020) 24:120. doi: 10.1186/s13054-020-2841-7
16. He Q, Li T, Su Y, Luan Y. Instructive messages and lessons from chinese countermarching nurses of caring for COVID-19 patients: a qualitative study. J Transcult Nurs. (2021) 32:96–102. doi: 10.1177/1043659620950447
17. Lasalvia A, Amaddeo F, Porru S, Carta A, Tardivo S, Bovo C, et al. Levels of burn-out among healthcare workers during the COVID-19 pandemic and their associated factors: a cross-sectional study in a tertiary hospital of a highly burdened area of north-east Italy. BMJ Open. (2021) 11:e045127. doi: 10.1136/bmjopen-2020-045127
18. Hu D, Kong Y, Li W, Han Q, Zhang X, Zhu LX, et al. Frontline nurses' burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. E Clin Med. (2020) 24:100424. doi: 10.1016/j.eclinm.2020.100424
19. Wu Y, Wang J, Luo C, Hu S, Lin X, Anderson AE, et al. A comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J Pain Symptom Manage. (2020) 60:e60–5. doi: 10.1016/j.jpainsymman.2020.04.008
20. Zhang X, Wang J, Hao Y, Wu K, Jiao M, Liang L, et al. Prevalence and factors associated with burnout of frontline healthcare workers in fighting against the COVID-19 pandemic: evidence from china. Front Psycho. (2021) 12:680614. doi: 10.3389/fpsyg.2021.680614
21. Zhang S, Wang J, Xie F, Yin D, Shi Y, Zhang M, et al. A cross-sectional study of job burnout, psychological attachment, and the career calling of Chinese doctors. BMC Health Serv Res. (2020) 20:193. doi: 10.1186/s12913-020-4996-y
22. Dyrbye LN, West CP, Kelsey EA, Gossard AA, Satele D, Shanafelt T. A national study of personal accomplishment, burnout, and satisfaction with work-life integration among advance practice nurses relative to other workers. J Am Assoc Nurse Pract. (2020) 33:896–906. doi: 10.1097/JXX.0000000000000517
23. Ambani Z, Kutney-Lee A, Lake ET. The nursing practice environment and nurse job outcomes: a path analysis of survey data. J Clin Nurs. (2020) 29:2602–14. doi: 10.1111/jocn.15283
24. Salyers M, Bonfils K, Luther L, Firmin R, White D, Adams E, et al. The relationship between professional burnout and quality and safety in healthcare: a meta-analysis. J Gen Intern Med. (2016) 32:475–82. doi: 10.1007/s11606-016-3886-9
25. Vévodová Š, Vevoda J, Grygová B. Mobbing, subjective perception, demographic factors, and prevalence of burnout syndrome in nurses. Cent Eur J Public Health. (2020) 28:61–68. doi: 10.21101/cejph.a6211
26. Xu W, Pan Z, Li Z, Lu S, Zhang L. Job burnout among primary healthcare workers in rural China: a multilevel analysis. Int J Environ Res Public Health. (2020) 17:727. doi: 10.3390/ijerph17030727
27. Zhang Y, Wang C, Pan W, Zheng J, Gao J, Huang X, et al. Stress, burnout, and coping strategies of frontline nurses during the COVID-19 epidemic in Wuhan and Shanghai, China. Front Psychiatry. (2020) 11:565520. doi: 10.3389/fpsyt.2020.565520
28. Dall'Ora C, Ball J, Reinius M, Griffiths P. Burnout in nursing: a theoretical review. Hum Resour Health. (2020) 18:41. doi: 10.1186/s12960-020-00469-9
29. Purvanova RK, Muros RP. Gender differences in burnout: a meta-analysis. J Vocat Behav. (2010) 77:168–85. doi: 10.1016/j.jvb.2010.04.006
30. Schadenhofer P, Stummer H. Gender differences in the vulnerability to burnout in the health and nursing care. Heilberufe Sci. (2011) 2:42–7. doi: 10.1007/s16024-011-0235-0
31. Fountaine S. Women in management worldwide: progress and prospects. Gender Manage. (2012) 27:214–6.
32. Hussain G, Javed N, Irshad W. Work-family role conflicts and its relationship with job performance of female nurses working in public hospitals of lahore corresponding author. Pakistan Soc Sci Rev. (2020) 4. doi: 10.35484/pssr.2020(4-III)49
33. Adebayo S, Chineye O. Gender differences in burnout among health workers in the Ekiti State University Teaching Hospital Ado-Ekiti. Int J Soc Behavioural Sci. (2013) 1:112–21.
34. Eckerson CM. The impact of nurse residency programs in the United States on improving retention and satisfaction of new nurse hires: AN evidence-based literature review. Nurse Educ Today. (2018) 71:84–90. doi: 10.1016/j.nedt.2018.09.003
35. Kovner CT, Brewer CS, Fatehi F, Jun J. What does nurse turnover rate mean and what is the rate? Policy Polit Nurs Pract. (2014) 15:64–71. doi: 10.1177/1527154414547953
36. Li CP, Shi K. The influence of distributive justice and procedural justice on job burnout. Acta Psychol Sin. (2003) 35:677–84. doi: 10.1023/A:1022289509702
37. Long-Fei L, Xiu-Xian Y, Fei W, Xiao-Hui Q, Zheng-Xue Q, Lin W, et al. Study on job burnout and personality characteristics of teachers. Chin Primary Health Care. (2013) 27:27–8. doi: 10.3969/j.issn.1001-568X.2013.01.012
38. Gao B, Jiayu Dong BS. Does the impact of COVID-19 improve the doctor-patient relationship in China? Science Direct. Am J Med Sci. (2020) 360:305–6. doi: 10.1016/j.amjms.2020.05.039
39. Li H, Yuan B, Meng Q, Kawachi I. Contextual factors associated with burnout among Chinese primary care providers: a multilevel analysis. Int J Environ Res Public Health. (2019) 16:3555. doi: 10.3390/ijerph16193555
40. Gu B, Tan Q, Zhao S. The association between occupational stress and psychosomatic wellbeing among Chinese nurses: a cross-sectional survey. Medicine. (2019) 98:e15836. doi: 10.1097/MD.0000000000015836
41. Wang Y, Chang Y, Fu J, Wang L. Work-family conflict and burnout among Chinese female nurses: the mediating effect of psychological capital. BMC Public Health. (2012) 12:915. doi: 10.1186/1471-2458-12-915
42. Hansen N, Sverke M, Näswall K. Predicting nurse burnout from demands and resources in three acute care hospitals under different forms of ownership: a cross-sectional questionnaire survey. Int J Nurs Stud. (2008) 46:95–106. doi: 10.1016/j.ijnurstu.2008.08.002
43. Brooks Carthon JM, Hatfield L, Brom H, Houton M, Kelly-Hellyer E, Schlak A, et al. System-level improvements in work environments lead to lower nurse burnout and higher patient satisfaction. J Nurs Care Qual. (2021) 36:7–13. doi: 10.1097/NCQ.0000000000000475
44. Zeng LN, Zhang JW, Zong QQ, Chan SW, Browne G, Ungvari GS, et al. Prevalence of burnout in mental health nurses in China: a meta-analysis of observational studies. Arch Psychiatr Nurs. (2020) 34:141–8. doi: 10.1016/j.apnu.2020.03.006
45. De Vos JA, Brouwers A, Schoot T, Pat-El R, Verboon P, Näring G. Early career burnout among Dutch nurses: a process captured in a Rasch model. Burnout Research. (2016) 3:55–62. doi: 10.1016/j.burn.2016.06.001
46. Lin YE, Tseng CN, Wang MF, Wu SV, Jane SW, Chien LY. Anxiety and work stress among newly employed nurses during the first year of a residency programme: a longitudinal study. J Nurs Manag. (2020) 28:1598–606. doi: 10.1111/jonm.13114
47. Dwyer PA, Hunter Revell SM, Sethares KA, Ayotte BJ. The influence of psychological capital, authentic leadership in preceptors, and structural empowerment on new graduate nurse burnout and turnover intent. Appl Nurs Res. (2019) 48:37–44. doi: 10.1016/j.apnr.2019.04.005
48. Peterson SA, Wolkow AP, Lockley SW, O'Brien CS, Qadri S, Sullivan JP, et al. Associations between shift work characteristics, shift work schedules, sleep and burnout in North American police officers: a cross-sectional study. BMJ Open. (2019) 9:e030302. doi: 10.1136/bmjopen-2019-030302
49. Chico-Barba G, Jiménez-Limas K, Sánchez-Jiménez B, Sámano R, Rodríguez-Ventura AL, Castillo-Pérez R, et al. Burnout and metabolic syndrome in female nurses: an observational study. Int J Environ Res Public Health. (2019) 16:1993. doi: 10.3390/ijerph16111993
50. Nascimento J, Santos JD, Meira KC, Pierin A, Souza-Talarico JN. Shift work of nursing professionals and blood pressure, burnout and common mental disorders. Rev Esc Enferm USP. (2019) 53:e03443. doi: 10.1590/s1980-220x2018002103443
51. Gómez-García T, Ruzafa-Martínez M, Fuentelsaz-Gallego C, Madrid JA, Rol MA, Martínez-Madrid MJ, et al. Nurses' sleep quality, work environment and quality of care in the Spanish National Health System: observational study among different shifts. BMJ Open. (2016) 6:e012073. doi: 10.1136/bmjopen-2016-012073
52. Pepłońska B, Nowak P, Trafalska E. The association between night shift work and nutrition patterns among nurses: a literature review. Med Pr. (2019) 70:363–76. doi: 10.13075/mp.5893.00816
53. Gao X, Jiang L, Hu Y, Li L, Hou L. Nurses' experiences regarding shift patterns in isolation wards during the COVID-19 pandemic in China: a qualitative study. J Clin Nurs. (2020) 29:4270–80. doi: 10.1111/jocn.15464
54. Dong H, Zhang Q, Zhu C, Lv Q. Sleep quality of nurses in the emergency department of public hospitals in China and its influencing factors: a cross-sectional study. Health Qual Life Outcomes. (2020) 18:116. doi: 10.1186/s12955-020-01374-4
55. Su Y, Wang Z, Bian YD, Peng YB. A Survey on Nurses' Job Burnout and Factors Analysis in Tangshan Private Hospitals. Appl Mech Mater. (2011) 50:939–43. doi: 10.4028/www.scientific.net/AMM.50-51.939
56. Panagiotis Z, Fotios A, Panagiota S. Burnout in medical residents: a study based on the job demands-resources model. Sci World J. (2014) 2014:673279. doi: 10.1155/2014/673279
57. Schaufeli W. Job demands, job resources, and their relationship with burnout and engagement: a multi-sample study. J Organ Behav. (2004) 25:293–315. doi: 10.1002/job.248
58. Vevoda J, Vévodová Á. The impact of burnout on nurses' work satisfaction. Eur J Public Health. (2020) 50:113–4. doi: 10.1093/eurpub/ckaa165.307
59. Özdemir B, Demir A. Romantic relationship satisfaction, age, course load, satisfaction with income and parental status as predictors of instructors' burnout: evidence from a correlational study. Curr Psychol. (2019) 38:1–16. doi: 10.1007/s12144-017-9724-3
60. Zhang LF, You LM, Liu K, Zheng J, Fang JB, Lu MM, et al. The association of Chinese hospital work environment with nurse burnout, job satisfaction, and intention to leave. Nurs outlook. (2014) 62:128–37. doi: 10.1016/j.outlook.2013.10.010
61. Van der Heijden B, Brown Mahoney C, Xu Y. Impact of job demands and resources on nurses' burnout and occupational turnover intention towards an age-moderated mediation model for the nursing profession. Int J Environ Res Public Health. (2019) 16:2011. doi: 10.3390/ijerph16112011
62. Penz M, Wekenborg MK, Pieper L, Beesdo-Baum K, Walther A, Miller R, et al. The Dresden Burnout Study: Protocol of a prospective cohort study for the bio-psychological investigation of burnout. Int J Methods Psychiatr Res. (2018) 27:e1613. doi: 10.1002/mpr.1613
Keywords: female nurses, burnout, factors, a cross-section, controlled COVID-19 period
Citation: Zhou L-L, Zhang S-E, Liu J, Wang H-N, Liu L, Zhou J-J, Bu Z-H, Gao Y-F, Sun T and Liu B (2022) Demographic Factors and Job Characteristics Associated With Burnout in Chinese Female Nurses During Controlled COVID-19 Period: A Cross-Sectional Study. Front. Public Health 9:757113. doi: 10.3389/fpubh.2021.757113
Received: 11 August 2021; Accepted: 08 November 2021;
Published: 06 January 2022.
Edited by:
Joanne Nicholson, Brandeis University, United StatesReviewed by:
Xiaoyan Liao, Southern Medical University, ChinaChing-Hui Sia, National University of Singapore, Singapore
Copyright © 2022 Zhou, Zhang, Liu, Wang, Liu, Zhou, Bu, Gao, Sun and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bei Liu, MTg4MjczODA3MTdAMTYzLmNvbQ==; Tao Sun, aHlkc3VudGFvQDEyNi5jb20=
†These authors have contributed equally to this work