
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 30 November 2021
Sec. Public Health Education and Promotion
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.753867
 Abdurezak Umer1*
Abdurezak Umer1* Kedir Abdella1
Kedir Abdella1 Yared Tekle1
Yared Tekle1 Addisalem Debebe1
Addisalem Debebe1 Tsegahun Manyazewal2
Tsegahun Manyazewal2 Mohammed Yuya3
Mohammed Yuya3 Hussen Mohammed1,2
Hussen Mohammed1,2Background: There is a global concern that coronavirus disease 2019 (COVID-19) cannot be addressed without the integration and active engagement of communities. We aimed to investigate the knowledge, attitude, and practices (KAP) of the residents in Eastern Ethiopia toward COVID-19.
Method: A community-based cross-sectional study was conducted on May 1–30, 2020 among the residents of Dire Dawa, Eastern Ethiopia. Data were collected using a structured questionnaire on the awareness, knowledge, attitudes, and preventive practices toward COVID-19. We used random sampling to select the participants. Data was entered into the statistics and data (STATA) version for data cleaning and analysis. Binary logistic regression models with 95% CI were used to conduct bivariable [crude odds ratio (COR)] and multivariable [adjusted odds ratio (AOR)] analyses.
Result: A total of 415 community residents responded to the questionnaire. Of those participants, 52.5% (95% CI 47.7–57) had adequate knowledge, 31.6% (95% CI 27–36) had favorable attitudes, and 49% (95% CI 45–50) had good practice toward the precautionary measures of COVID-19. Adequate knowledge had a significant association with urban residence (AOR = 5, 95% CI 3.1–8.4) and literacy (AOR = 3.1, 95% CI 1.5–6.7). Good preventions practices had a significant association with place of residence (AOR = 4.1, 95% CI 2.3–7.2), literacy (AOR = 2.9, 95% CI: 1,2–7.4), adequate knowledge (AOR = 3.5, 95% CI 2.3–5.8), and favorable attitude (AOR = 2.3, 95% CI 1.4–3.8) about the disease.
Conclusion: The overall COVID-19-related KAP was inadequate in the majority of the residents of Dire Dawa that occupy irregular migration flows. These call for robust community-centered behavioral communication strategies that could bridge the gaps and help prevent and control COVID-19 and other future pandemics in their community.
Coronavirus disease 2019 continues to be a global pandemic and public health crisis. More than 200 million people were infected by the disease and 2% of these people died, globally (1). Ethiopia reported its first coronavirus disease 2019 (COVID-19) case on March 13, 2020; since then, the disease has spread over all parts of the country and infected over 300,000 people, of whom 1.59% died (1). The majority of the secondary cases reported in Ethiopia were acquired through community transmission (2). Currently, there are some specific antiviral treatments recommended for COVID-19 infection (3). Individuals with COVID-19 often receive medical care to relieve symptoms. Recently, a high number of COVID-19 cases were reported in Ethiopian communities, even though the Federal Government of Ethiopia and its national regional states and city administrations took steps to prevent the spread of the disease (4). The outbreak still has the potential for greater loss of life in Ethiopia if the community is unable to shape their regular behavioral and sociocultural norms that would favor the spread of the disease. The knowledge, attitude, and practices (KAP) of the community toward COVID-19 have a significant impact on the battle against the disease. Previous studies conducted elsewhere around KAP documented cognitive factors as major drivers of behavioral change (5, 6) and the KAP of the disease was the major behavioral determinant that directly influenced the activities of human beings, behaviors, understanding, and habits of a given community (7). There have been some studies conducted in Ethiopia to know how the KAPs toward COVID-19 at the community level influenced the transmissions of the disease (8, 9); however, their primary focus had been on the general knowledge of COVID-19 or knowledge that the general public can have along with the misconception of COVID-19.
The Dire Dawa administration is an industrial hub, in which cars, railways, and airline transportations are available, and a border with Djibouti that favors the transmission of COVID-19. There has been no research conducted in Dire Dawa to know the KAP of the community toward COVID-19 and this has been a missed opportunity to mitigate the disease in its earliest stages. In the absence of adequate treatments and vaccines in the place, the strict implementation of disease prevention and control measures, and harnessing the awareness of communities toward these measures are the most powerful tools that local governments need to pursue. In this case, it is necessary to assess the KAPs, beliefs, rumors, and misconceptions of a given community to know the appropriate interventions.
Therefore, the present study aimed to investigate the current KAP of the residents in the Dire Dawa administration, Eastern Ethiopia, toward COVID-19.
A community-based, cross-sectional study was conducted in the Dire Dawa Administration. The Dire Dawa administration is situated in the Eastern part of Ethiopia, 315 km from Addis Ababa, the capital city of Ethiopia. The Dire Dawa administration has different sorts of transportations from land, railway, and an international airport, and it is only 300 km away from Djibouti, thus is susceptible to cross-border transmission of COVID-19. The administration has two government hospitals and 15 health centers that provide healthcare services to more than 500,000 of the population (10).
The source population was all the residents of the Dire Dawa administration, and the study population was all selected adults in the selected kebeles (lowest administrative unit) in the urban and rural kebeles. The following inclusion criteria were applied in this study: adults (i.e., older than 18 years of age) of any sex, formal residents of Dire Dawa, and willing to participate and sign the informed consent of the study.
The sample size estimation was calculated using a single population formula with a 5% margin of error and 95% confidence level. We considered that 50% of the population have adequate KAP based on the sample collection procedure at the times that there is no study to refer to (11). With this, a minimum of 384 participants was required. A further 10% was added to account for non-respondents and this increased the sample size to 422.
Random sampling was used to select the study participants. In the Dire Dawa administration, there are urban and rural kebeles (lowest administration unit). Three urban and six rural kebeles were selected using simple random sampling (SRS). Finally, the sampling with population proportional to the size was calculated for the study participants at each selected kebeles to attain the total sample size by using the proportionate allocation formula.
The data were obtained from the consenting participants through face-to-face interviews using a structured questionnaire on the KAP toward COVID-19. The questionnaire was adopted from previous studies (12, 13) and pre-tested. It had five distinct sections that deal with sociodemographic data, KAP, awareness toward the disease, and the belief, rumors, and stigma associated with COVID-19 in the community. The data were collected from May 1–30, 2020.
On the survey instrument, omit or skip patterns were utilized to properly direct respondents to answer items that are relevant to them. A codebook was employed to input and organize the data appropriately. Data verification processes, including the spot-checking of the questionnaire at the data-gathering sites, were implemented to ensure the accuracy of the row data. The questionnaire was pre-tested on 5% of the total sample size.
The data were double-entered in Epi-Info™ (version 3.5.1, CDC, Atlanta, Georgia, United States), and analyzed by Stata 14 (College Station, Texas, United States). A Kolmogorov-Smirnov test was used to check for the normal distribution of data. The reliability of the questionnaire was tested using Cronbach's alpha. Binary logistic regression models with 95% CI were used to conduct bivariable [crude odds ratio (COR)] and multivariable analysis [adjusted odds ratio (AOR)]. From the multivariable analysis (AOR), variables significantly associated with p-value < 0.05 were declared as factors for good prevention practices.
The knowledge of the respondents about COVID-19 was assessed using a 31-item questionnaire developed by Zhong et al. and adopted by other similar studies (12, 13). The questionnaire included the clinical characteristics of the disease (i.e., primary symptoms, availability and effectiveness of treatment, and severity), addressed transmission (i.e., infection through contact with animals and transmission through respiratory droplets), and prevention and control (i.e., wearing medical masks for prevention). All respondents could respond with “Yes,” “No,” or “Don't know.” The knowledge scores were calculated by assigning one point to each correct question, and an aggregate score was calculated (range 0–21). It is measured by calculating the mean score of the 21 items. This was categorized as knowledgeable, if a participant scored ≥ the mean score of the correctly answered questions, or not knowledgeable, if the participant scored < the mean score of the correctly answered questions
To measure attitudes related to COVID-19, we examined the perceived risk of COVID-19 infection comprising perceived susceptibility, which signifies the beliefs of an individual about their possibility of infection, and perceived severity of the infection. The respondents answered how dangerous they think COVID-19 is, how they describe their risk of infection with COVID-19, and how effective the state of emergency was to control the spread of COVID-19. The responses were rated on a 5-point Likert-type scale, with “1 = very low, 3 = neither low nor high, and 5 = very high” which is finally merged.
The prevention practice behaviors were measured using three items that covered the following two categories: (1) preventive measures (i.e., wearing facial masks and practicing hand hygiene) and social distancing (i.e., avoiding crowded places). The respondents self-reported the frequency of the practices they performed during the previous week at the time of the survey, using yes “1” and no “0”).
The study protocol was reviewed and approved by the ad-hoc Committee for Ethical Review of Human Study of the Dire Dawa University. A letter of support was written to the concerned body. Participation was voluntary and each participant was asked to give consent after a clear explanation of the research objectives. The participants were assured that all responses would remain confidential. The right to withdraw from the study was respected.
Out of the 422 community residents that the study reached, 415 participants consented and responded to the questionnaire, with a respondent rate of 98%. For their place of residence, 371 (89.4%) were from urban areas. The mean age of the participants was 32.83 ± 8.78 SD. The majority of the participants were male [268 (64.6%)] and government employees [113 (27.2%)]. Regarding their educational status, 66 (15.9%) cannot read and write and 158 (38.1%) have attended college and above (Table 1).
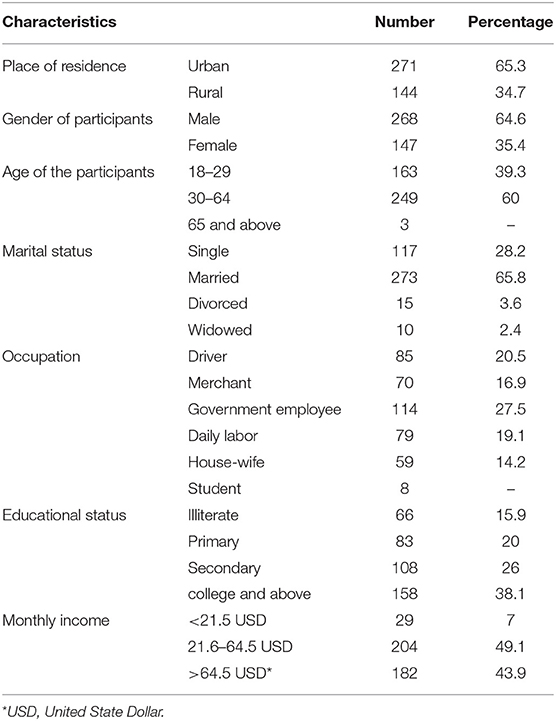
Table 1. Demographic characteristic of study participants on the assessment of the risk of COVID-19 among Dire Dawa administration residents, Eastern Ethiopia, May 2020 (N = 415).
Almost all the participants (99.9%) have heard about COVID-19, 356 (85.8%) were aware that COVID-19 is a virus that causes a disease, and 52 (12.5%) perceived COVID-19 as futile propaganda from the government. Regarding the source of information, 359 (86.5%) of the participants have heard of the disease from television, with 273 (65.8%) and 88 (21.2%) perceiving television and social media as the ideal source of information, respectively. In the study, 228 (54.9%) of the participants reported that there is a stigma toward COVID-19 (Figure 1).
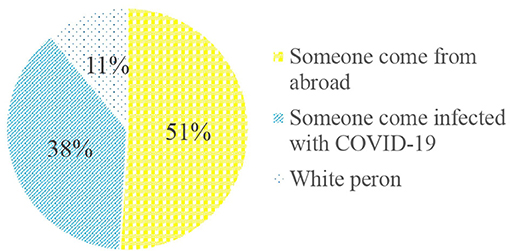
Figure 1. Stigmatized group during the COVID-19 pandemic among the Dire Dawa Administration residents, Eastern Ethiopia, September 2020.
A total of 21 questions were used to measure the knowledge of the study participants toward COVID-19 where the mean knowledge score was 14.29 (SD= 4.7, range 3–26). Two hundred forty-six (59.3%) of the participants knew that people who had contact with an infected person should be immediately isolated for 14 days as per the national guideline. Regarding social interaction, 395 (95.2%) of the participants perceived that shaking hands and hugging may result in the contract of COVID-19. Regarding preventive measures, 360 (86.7%) and 267 (64.3%) of the participants perceived that washing hands with soap and wearing a mask in crowded areas, respectively, prevent COVID-19 transmission (Table 2).
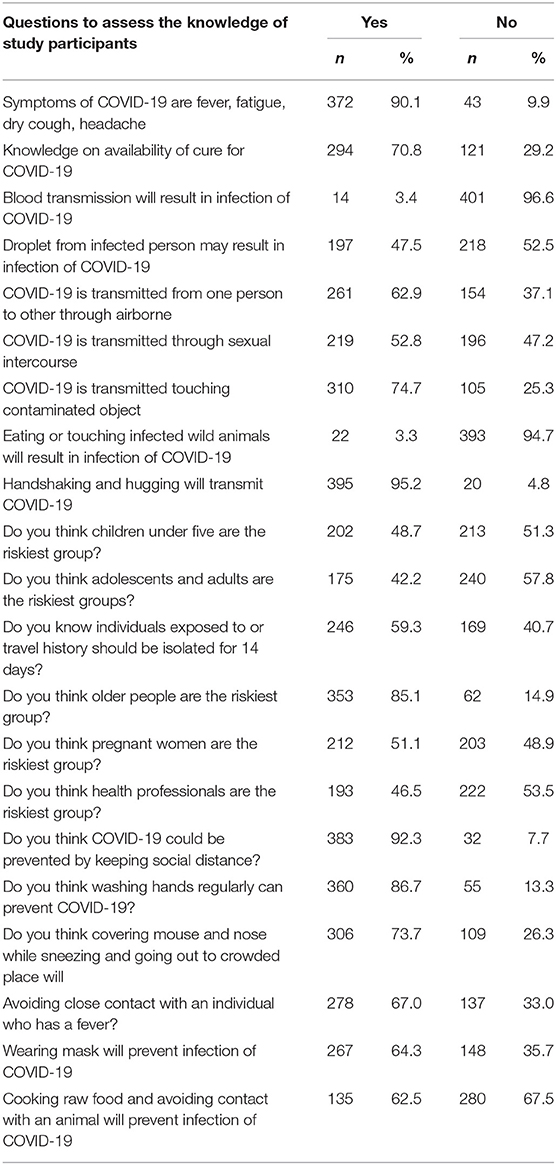
Table 2. Frequency of respondent's knowledge on coronavirus, Dire Dawa administration, Eastern Ethiopia, May 2020 (N = 415).
A total of four questions were used to assess the attitudes of the participants toward COVID-19. These included questions if they perceive COVID-19 as a serious disease, perceive the State of Emergency of the government as effective in controlling COVID-19, if complete lockdown helps to control COVID-19 in their community, and if they perceive that they will become infected with COVID-19 without their personal preventive measures. With these, 271 (65.3%) of the participants perceived COVID-19 as a very serious disease; 144 (34.7%) perceived that the State of Emergency would help prevent the transmission of the disease; 180 (43.4%) thought the State of Emergency was not implemented thoroughly as planned. Additionally, 300 (72.3%) of the participants thought that the lockdown was an ideal measure to contain the disease in their community (Table 3).
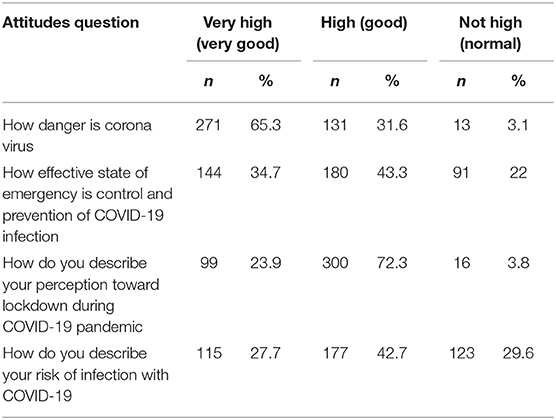
Table 3. Frequency of respondent's attitudes on coronavirus, Dire Dawa administration, Eastern Ethiopia, May, 2020 (N = 415).
A total of eight questions were used to assess the COVID-19 prevention practices of the participants, with 346 (83.4%) participants saying that they stopped going to crowded places and 230 (55.4%) used face masks if they had to go to a crowded place. Similarly, 301 (72.5%) of the participants perceived that they keep social distancing, 399 (96.1%) wash their hands with soap frequently, and 229 (55.2%) stopped shaking hands (Table 4).
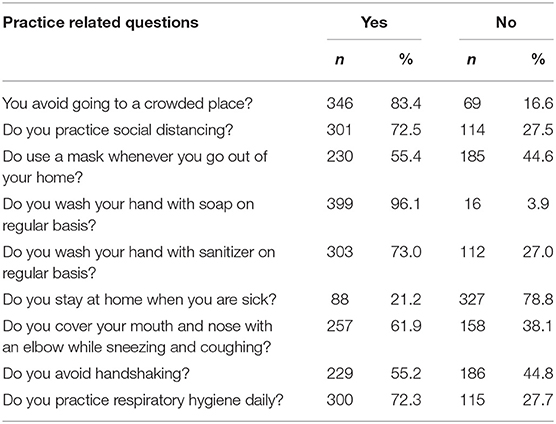
Table 4. Frequency of respondent's practice toward COVID-19, Dire Dawa administration residents, Eastern Ethiopia, May 2020 (N = 415).
Variables such as place of residence, sex, educational level, monthly income, and occupation of participants had a p-value of < 0.2 in the bivariate analysis and were associated with their knowledge about COVID-19. These variables were entered into a multivariate binary logistic regression analysis model. The multivariate analysis showed that the urban residents were five times [AOR 5, 95% CI (3.1.−8.4)] more likely to have adequate knowledge, attitude and practice of study participants is shown in Figure 2 compared with the rural residents. Similarly, the participants who had formal education from registered institutions were 3.1 times [AOR 3.1, CI (1.5–6.7)] more likely to have adequate knowledge than those without formal education (Table 5).
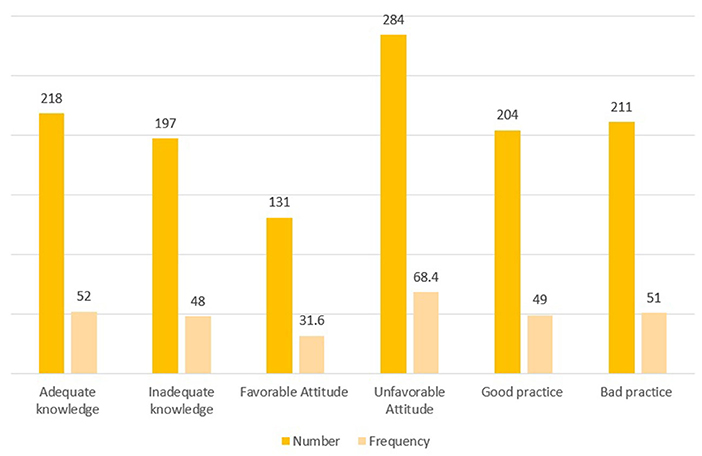
Figure 2. Distribution of knowledge, attitude, and practice toward COVID-19 among the Dire Dawa Administration residents, Eastern Ethiopia, September 2020.
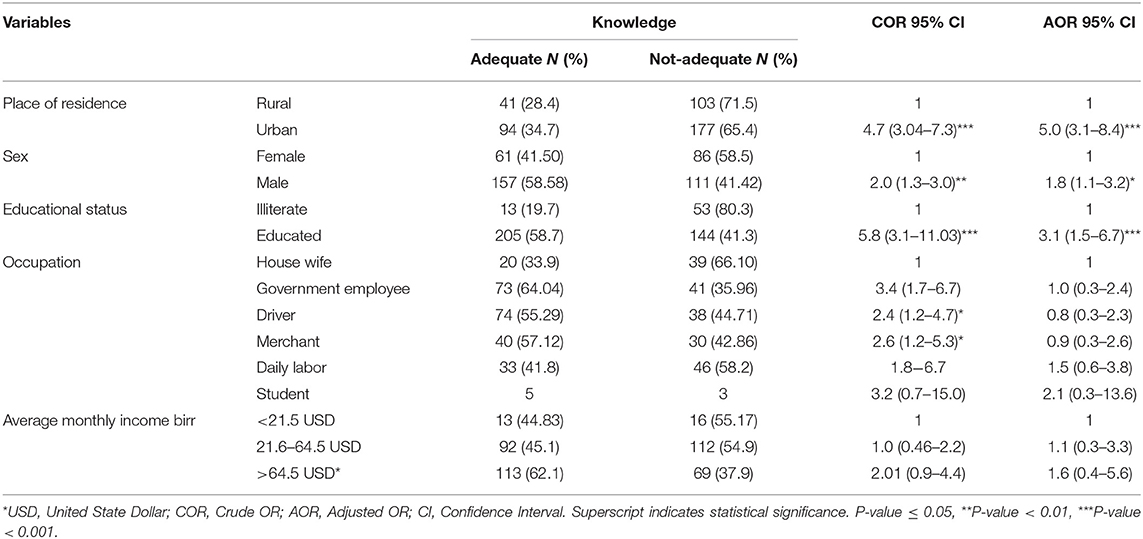
Table 5. Factors associated with knowledge toward COVID-19 among Dire Dawa administration residents, Eastern Ethiopia May 2020.
Variables such as level of knowledge, place of residents, sex, educational status, income, and occupation of the participants were significantly associated with COVID-19 prevention practice in the bivariate analysis. In the multivariate logistic regression model, level of knowledge, attitude, place of residents, sex, educational status, and occupation are significantly associated with COVID-19 prevention practices. Participants who had adequate knowledge were 4.9 times more likely to practice COVID-19 preventive measures compared with those who do not have adequate knowledge. The participants who had a favorable attitude toward COVID-19 were 2-fold likely to practice COVID-19 prevention measures. Men were 60% less likely to practice COVID-19 prevention measures as compared with women (Table 6).
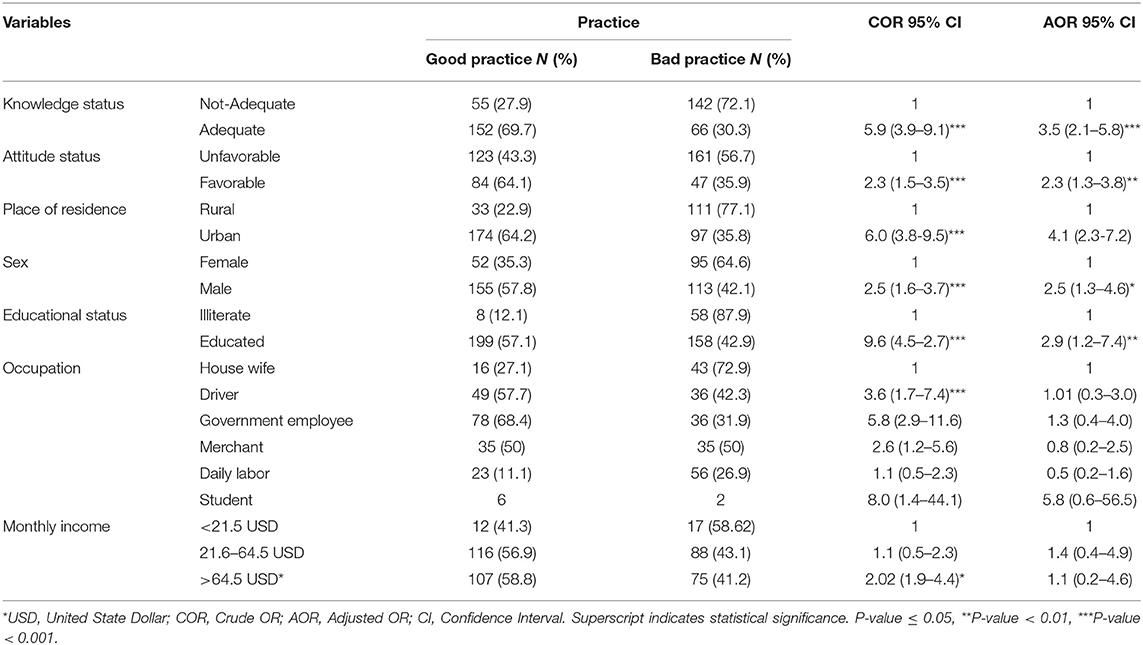
Table 6. Factors associated with practice toward COVID-19 among Dire Dawa administration residents, Eastern Ethiopia, May 2020.
One of the main goals of this study was to investigate the KAP of Dire Dawa residents toward COVID-19. This issue is critical for research to identify the necessary intervention based on the gaps we identified. The study revealed that close to half of the study participants had inadequate knowledge regarding COVID-19; similarly, two-third of the participants had unfavorable attitudes toward COVID-19, and about half had poor practice toward COVID-19 preventive measures.
More than half (54%) of the participants in this study perceived that there was a COVID-19-related stigma in their community; this finding was lower as compared with the finding from a study conducted in Jima Zone which reported 83.3% of stigma toward the disease (13). The observed difference may be due to differences in the study period or demographic characteristics of the study participants. This finding showed that there is an urgent need for an intervention to handle stigma. The WHO emphasized that stigma during such an outbreak demands an urgent intervention (14).
The study revealed that 52% of the study participants have adequate knowledge of COVID-19, and the finding was lower than a previous national-level study in Ethiopia that reported an adequate knowledge of 90% among the participants (15). A possible explanation for this discrepancy could be that the participants of the study were interviewed virtually and such participants could have higher education levels than the current study. Inversely, the current study yielded a higher value compared with a previous study conducted in the Mizan Tepi community, Southern Ethiopia, where 43% of the study participants had adequate knowledge about COVID-19 (8). Comparing our findings with studies conducted outside of Ethiopia, our findings were higher than a study conducted in Bangladesh in which 65% of the participants had inadequate knowledge about COVID-19 (16). This discrepancy may be attributed to the difference in the socio-demographic factors of the study participants.
In this study, 86% of the knowledge of the participants about COVID-19 came from the television as the main source of information, which was in agreement with a previous study conducted in Nigeria (17) but in contrast to a study conducted in Egypt that reported social media as the main source of information (18).
The findings of this study showed that the majority (92%) of the study participants reported that they had regularly used social distancing while some (83 %) of them used frequent hand washing (soap and sanitizer), which are the most effective ways to prevent oneself from COVID-19. A similar finding was reported from a previous study performed in the Jima University teaching hospital in Ethiopia. Similarly, a study conducted in Egypt reported social distancing and proper handwashing as the main ways to protect oneself against coronavirus (19). Furthermore, a study conducted in Italy also considered social distancing as the main defense against coronavirus (20). This study finding showed that the participants who had less educational level were less knowledgeable about coronavirus transmission and prevention. Similar to a study from Southern Ethiopia (21), Egypt (18), and Saudi Arabia (22). However, a study conducted in the Jima University teaching hospital found that education is not associated with the knowledge status of COVID-19 (13).
The findings of this study showed that about one-third of the study participants had a favorable attitude toward coronavirus prevention policy and risk level; this is in line with the study conducted by Bekele D et al. at the national level in Ethiopia (13). However, this result differs from the high level of favorable attitude (92.%) found in southern Ethiopian residents (23). Regarding the trust of the population in the effectiveness of government policies in the prevention and control of the coronavirus, only one-third of the study participants had a favorable attitude; this is similar to a study conducted in Egypt (24) and Nigeria (25), where the participants believe that it was a biological weapon; this may result in valuing the preventive methods less, which is dangerous in controlling the fastest spreading coronavirus.
The findings of this study showed that about half of the study participants had poor practice toward the prevention of coronavirus. This is in line with a study conducted in Addis Zemen Hospital, Northwest Ethiopia (26). However, this finding is higher than the study conducted in Bangladesh where only 19% of the respondents had poor practice toward coronavirus prevention methods (27). Our study revealed that most of the study participants had malpractice toward COVID-19 prevention measures despite their adequate knowledge. For instance, only 61% of participants used a mask daily, although the majority of the respondents reported that they knew the importance of masks. This finding shows that it takes repeated health education to change the behavior of an individual. This study finding showed that being rural residents, the level of education in terms of sociodemographic was associated with the poor practice of coronavirus prevention methods. This finding was consistent with studies done in southern Ethiopia (8), Egypt (24), China (28), and Malaysia (29).
Overall, among the studied demographic characteristics, the place of residence, sex, and education had a significant association with the knowledge and practice of COVID-19 transmission and preventive measures. However, the attitudes of the participants did not show significant association with the actual practice. In comparison to this finding, a couple of studies reported that place of residence, educational level, and sex were significantly associated with knowledge status (18, 23, 28), and another study showed the association of sex and educational level (22). Furthermore, previous studies have shown that the place of residents and education status were significantly associated with COVID-19 prevention practices (26). Additionally, significant associations were found between knowledge status and attitude (29). This difference may be due to differences in the population characteristics. In certain areas, there are low levels of early adoption of the new practices while in other geographic areas, people adopt new practices early. In our study, males had a higher level of knowledge and practice toward transmission and prevention methods. This could be explained by the responding tendency of the participants and the statistical allocation of the study participants.
The low level of preventive practices among the participants of this study may reflect the unstable conditions and economic status of the individuals and country as a result of the current coronavirus pandemic. Many government and private-sector employees have lost their jobs nationally and internationally (30, 31), and the pandemic interrupts the healthcare services for other disease conditions (32). The main concern of these people is to provide their families with daily food requirements. As a result, the financial shortage has affected the knowledge and preventive behavior of people against COVID-19. The use of information technology, including digital health solutions, may help build the KAP potential of the community through training, dissemination of up-to-date information about the disease, and exchange of information that can combat misinformation (33–35).
In general, although the COVID-19 KAPs studies in Ethiopia are limited, there is a significant variation in the KAP between the studies, which could be attributed to the differences in the study areas, study population, and the study design followed.
Our findings revealed that there are significant knowledge gaps, unfavorable attitudes, and poor practices toward COVID-19 among the Dire Dawa administration residents in Eastern Ethiopia. Predictor variables including place of residence, sex, and educational level were significantly associated with the knowledge scores. Predictive variables including knowledge score, attitude, place of residence, and educational level were significantly associated with the practice levels. These call for robust community-centered behavioral communication strategies that could bridge the gaps and help prevent and control COVID-19 and other future pandemics in their community.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Dire Dawa University office of the vice president by ad-hoc Committee for Ethical Review of Human Study. The patients/participants provided their written informed consent to participate in this study.
AU participated in all phases of preparation starting from the inception of the project, collection of data, analysis and interpretation of results, and writing of the manuscript. HM contributed to the study design and checklist development during the data collection and writing of the manuscript. TM and MY contributed to the writing of the manuscript. AD contributed to the data collection and analysis. YT participated in the questionnaire development and analysis and manuscript preparation. KA participated in the questionnaire development and data collection. All authors read and approved the final manuscript.
This work was funded by the Dire Dawa University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Dire Dawa University for their commitment and keen motivation to solve the problem of the community during this challenging time. We would also like to thank the Dire Dawa University office of the vice president for research and community engagement affairs for their continuous professional comments. Last but not least, the authors like to thank the Dire Dawa Administration residents for their participation in this research during the COVID-19 pandemic.
1. Worldometer. COVID-19 Coronavirus Pandemic. Worldometer Corona Virus (2020). Available online at: https://www.worldometers.info/coronavirus/ (accessed August 02, 2021).
2. Mohammed H, Oljira L, Roba KT, Yimer G, Fekadu A, Manyazewal T. Containment of COVID-19 in Ethiopia and implications for tuberculosis care and research. Infect Dis Poverty. (2020) 9:1–8. doi: 10.1186/s40249-020-00753-9
3. Zhang C, Jin H, Wen Y, Yin G. Efficacy of COVID-19 treatments: a Bayesian network meta-analysis of randomized controlled trials. Front. Public Health. (2021) 9:729559. doi: 10.3389/fpubh.2021.729559
4. Zikargae MH. COVID-19 in Ethiopia: assessment of how the Ethiopian government has executed administrative actions and managed risk communications and community engagement. Risk Manag Healthc Policy. (2020) 13:2803–10. doi: 10.2147/RMHP.S278234
5. Jafari F, Shahriari M, Sabouhi F, Farsani AK, Babadi ME. Effects of a lifestyle modification program on knowledge, attitude and practice of hypertensive patients with angioplasty: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery. (2016) 4:286–96. Available online at: https://www.ncbi.nlm.nih.gov/pubmed/27713892
6. Baranowski T, Cullen KW, Nicklas T, Thompson D, Baranowski J. Are current health behavioral change models helpful in guiding prevention of weight gain efforts? Obes Res. (2003) 11:23S−43. doi: 10.1038/oby.2003.222
7. Fishbein M, Triandis HC, Kanfer FH, Becker M, Middlestadt SE, Eichler A. Factors influencing behavior and behavior change. Handb Health Psychol. (2001) 3:17. doi: 10.1177/01632780122034966
8. Mechessa DF, Ejeta F, Abebe L, Henok A, Nigussie T, Kebede O, et al. Community's knowledge of COVID-19 and its associated factors in Mizan-Aman Town, Southwest Ethiopia, 2020. Int J Gen Med. (2020) 13:507–13. doi: 10.2147/IJGM.S263665
9. Dires A, Addis SG, Tesema YG. Perceived Efficacy of COVID-19 Prevention Measures and Intention to Use Among Chronic Disease Patients in Northeast Ethiopia, 2020. Research Square (2020). doi: 10.21203/rs.3.rs-73649/v1
10. Central Statistical Agency F. Population Projections for Ethiopia 2007-2037. Addis Ababa: Population Census Commission (2013). p. 188. Report No.: 01. Available online at: https://www.statsethiopia.gov.et/wp-content/uploads/2019/05/ICPS-Population-Projection-2007-2037-produced-in-2012.pdf.
11. Degu G, Tessema F. Biostatistics Lecture Note for Health Science Students. (2005). p. 275. Available online at: https://www.cartercenter.org/resources/pdfs/health/ephti/library/lecture-notes/env-health-science-students/ln-biostat-hss-final.pdf (accessed Feb 12, 2021).
12. Wolka E, Zema Z, Worku M, Tafesse K, Anjulo AA, Takiso KT, et al. Awareness towards corona virus disease (COVID-19) and its prevention methods in selected sites in Wolaita Zone, Southern Ethiopia: a quick, exploratory, operational assessment. Risk Manag Healthc Policy. (2020) 13:2301–8. doi: 10.2147/RMHP.S266292
13. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS ONE. (2020) 15:e0233744. doi: 10.1371/journal.pone.0233744
14. World Health Organization. A Guide to Preventing and Addressing Social Stigma Associated With COVID-19. COVID-19: Risk Communication and Community Engagement (2020). Available online at: https://www.who.int/publications/m/item/a-guide-to-preventing-and-addressing-social-stigma-associated-with-covid-19 (accessed Oct 12, 2020).
15. Bekele D, Tolossa T, Tsegaye R, Teshome W. The knowledge and practice towards COVID-19 pandemic prevention among residents of Ethiopia. An online cross-sectional study. PLoS ONE. (2021) 16:e0234585. doi: 10.1371/journal.pone.0234585
16. Paul A, Sikdar D, Hossain MM, Amin MR, Deeba F, Mahanta J, et al. Knowledge, attitudes, and practices toward the novel coronavirus among Bangladeshis: implications for mitigation measures. PLoS ONE. (2020) 15:e0238492. doi: 10.1371/journal.pone.0238492
17. Anikwe CC, Ogah CO, Anikwe IH, Okorochukwu BC, Ikeoha CC. Coronavirus disease 2019: knowledge, attitude, and practice of pregnant women in a tertiary hospital in Abakaliki, southeast Nigeria. Int J Gynecol Obstet. (2020) 151:197–202. doi: 10.1002/ijgo.13293
18. Abdelhafiz AS, Mohammed Z, Ibrahim ME, Ziady HH, Alorabi M, Ayyad M, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. (2020) 45:881–90. doi: 10.1007/s10900-020-00827-7
19. Hager E, Odetokun IA, Bolarinwa O, Zainab A, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 coronavirus pandemic: a bi-national survey in Africa. PLoS ONE. (2020) 15:e0236918. doi: 10.1371/journal.pone.0236918
20. Gallè F, Sabella EA, Da Molin G, De Giglio O, Caggiano G, Di Onofrio V, et al. Understanding knowledge and behaviors related to COVID−19 epidemic in Italian undergraduate students: the EPICO study. Int J Environ Res Public Health. (2020) 17:3481. doi: 10.3390/ijerph17103481
21. Andarge E, Fikadu T, Temesgen R, Shegaze M, Feleke T, Haile F, et al. Intention and practice on personal preventive measures against the COVID-19 pandemic among adults with chronic conditions in Southern Ethiopia: a survey using the theory of planned behavior. J Multidiscip Healthc. (2020) 13:1863–77. doi: 10.2147/JMDH.S284707
22. Ali M, Uddin Z, Banik PC, Hegazy FA, Zaman S, Ambia ASM, et al. Knowledge, attitude, practice and fear of COVID-19: a cross-cultural study. medRxiv. (2020). doi: 10.1101/2020.05.26.20113233
23. Mola S, Aweke Z, Jemal B, Hussen R, Hailu S, Neme D, et al. Magnitude and associated factors for attitude and practice toward COVID-19 and its prevention among the residents of gedeo zone, Southern Ethiopia: a community-based cross-sectional study. Risk Manag Healthc Policy. (2021) 14:253–62. doi: 10.2147/RMHP.S277904
24. Wahed WYA, Hefzy EM, Ahmed MI, Hamed NS. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J Community Health. (2020) 45:1242–51. doi: 10.1007/s10900-020-00882-0
25. Reuben RC, Danladi MM, Saleh DA, Ejembi PE. Knowledge, attitudes and practices towards COVID-19: an epidemiological survey in North-Central Nigeria. J Community Health. (2020) 46:457–70. doi: 10.1007/s10900-020-00881-1
26. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. (2020) 13:1949–60. doi: 10.2147/IDR.S258736
27. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS ONE. (2020) 15:e0239254. doi: 10.1371/journal.pone.0239254
28. Yue S, Zhang J, Cao M, Chen B. Knowledge, attitudes and practices of COVID-19 among urban and rural residents in China: a cross-sectional study. J Community Health. (2020) 46:1–6. doi: 10.1007/s10900-020-00877-x
29. Mohamad EM, Azlan AA, Hamzah MR, Tham JS, Ayub SH. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. medRxiv. (2020). doi: 10.1371/journal.pone.0233668
30. Wieser C, Ambel AA, Bundervoet T, Haile A. Monitoring COVID-19 Impacts on Households in Ethiopia. The World Bank (2020). doi: 10.1596/33824
31. Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus and COVID-19 pandemic: a review. Int J Surg. (2020) 78:185–93. doi: 10.1016/j.ijsu.2020.04.018
32. Manyazewal T, Woldeamanuel Y, Blumberg HM, Fekadu A, Marconi VC. The fight to end tuberculosis must not be forgotten in the COVID-19 outbreak. Nat Med. (2020) 26:811–2. doi: 10.1038/s41591-020-0917-1
33. Tilahun B, Gashu KD, Mekonnen ZA, Endehabtu BF, Angaw DA. Mapping the role of digital health technologies in prevention and control of COVID-19 pandemic: review of the literature. Yearb Med Inform. (2021) 30:26–37. doi: 10.1055/s-0041-1726505
34. Manyazewal T, Woldeamanuel Y, Blumberg HM, Fekadu A, Marconi VC. The potential use of digital health technologies in the African context: a systematic review of evidence from Ethiopia. NPJ Digit Med. (2021) 4:125. doi: 10.1038/s41746-021-00487-4
Keywords: coronavirus disease 2019 (COVID-19), SARS-CoV-2, knowledge, attitude, practice, community
Citation: Umer A, Abdella K, Tekle Y, Debebe A, Manyazewal T, Yuya M and Mohammed H (2021) Community Engagement in the Fight Against COVID-19: Knowledge, Attitude, and Prevention Practices Among Dire Dawa Residents, Eastern Ethiopia. Front. Public Health 9:753867. doi: 10.3389/fpubh.2021.753867
Received: 19 August 2021; Accepted: 07 October 2021;
Published: 30 November 2021.
Edited by:
Argaw Ambelu, Jimma University, EthiopiaCopyright © 2021 Umer, Abdella, Tekle, Debebe, Manyazewal, Yuya and Mohammed. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdurezak Umer, ZGFnYWFiZHUyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.