 Yu Guo
Yu Guo Tingshuai Ge
Tingshuai Ge Li Mei
Li Mei Lina Wang
Lina Wang Jingbo Li
Jingbo Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 17 November 2021
Sec. Aging and Public Health
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.745073
This article is part of the Research Topic Aging and Health in China View all 21 articles
Although many studies have suggested that widowhood is related to worse health conditions among older adults, few have examined the mediation effects of social support between widowhood and health. Employing mediation analysis to a sample of data from the 2014 wave of China Longitudinal Aging Social Survey (CLASS), this study examined the mediation effects of social support, including emotional support, instrumental support, and companionship, in the widowhood-health association among older adults. The results indicated that the negative effect of widowhood on older adults' health was in part attributable to decreased emotional support and companionship. Specifically, emotional support exerted a significant role in the widowhood-mental health association, and companionship exerted a significant role in widowhood-physical health and widowhood-mental health associations. In the subsample analysis, the mediation effects were only significant among female older adults, and among rural older adults. Our findings highlight the importance of emotional support and companionship in maintaining health among widowed older adults and strategies should pay more attention to female and rural widowed older adults.
The loss of a spouse is one of the most painful and stressful events faced by older adults, as well as an inevitable role transition (1–3). Surviving spouses must bear the grief of losing a partner who provides daily support and companionship (4, 5). This may have adverse effects on mental and physical health (6–9). Even if widowhood is universal for all older adults, its impact on health varies according to gender, cultural norms, and social structure (10, 11).
A recent study indicates that widowhood alone may not lead to depression in older adults, but those who are widowed and socially isolated have an increased risk of depression (11). Social support seems to be a potential mediator in the pathway from widowhood to health. Lots of research has proved that social support as an important protective factor for mental and physical health, can lower the mortality risk, prevent depression, and maintain good physical health among older adults. However, social support tends to shrink with age, particularly after the death of a spouse who may be the primary support provider (12, 13). Currently, we know little about the role of social support and its subtypes in the relationship between widowhood and health. Besides, considering the characteristics of social support formed by different social structures and cultural norms are different (11, 12), it is necessary to explore the role of support in the pathway from widowhood to health, under the background of urban-rural dual structure and rigid gender division.
Therefore, using the 2014 wave of China Longitudinal Aging Social Survey (CLASS), this paper aimed to examine: (1) whether the relationship between widowhood and the health status of older adults is mediated by social support, especially the different types of social support; (2) whether the mediation effects of social support vary according to gender and rural-urban areas. Below, we first introduced the literature review, which provides an overview of the relationship between widowhood, social support, and health status, and a brief introduction of the Chinese context. Second, the data and methods section outlines the sample adopted, the measurement of variables, and the analytic strategy. Third, the results section demonstrates the role of social support in the widowhood-health relationship, including gender and rural-urban specific findings. Finally, the discussion and conclusions section compares the findings to the existing literature and considers the contribution to the existing knowledge base. And the limitations of the study and suggestions for further research are also considered.
Many studies have shown that the health of older adults tends to deteriorate after losing a spouse (14–16). According to the “marriage protection effect” hypothesis, marriage can promote good health through support for healthy behaviors (17). For example, spouses can motivate or encourage each other to quit smoking, engage in physical activities, and maintain a healthy diet, all of which are important for somatic health (18). On the other hand, marriage can also promote good health due to the available companionship, economic, and material resources (19, 20). A study by Emanuele reported that co-residency of couples provides companionship, better financial status, and health care resources (21).
The association and the mechanisms between widowhood and health seem not the same for all age groups (5, 10, 22). It is more detrimental to be bereaved at a younger age than it is to be widowed later in life (10). Widowhood, for example, raises the risk of death in older people, but the link is weaker for those aged 75 and above (22). Based on a sample of 75 years old and blow, Golden et al. (23) found that a higher prevalence of depression in widows with a higher prevalence of loneliness and isolation. While Forster et al. (24) found that widowhood alone is not necessarily related, only the oldest widowers, those socially isolated, face an increased risk of depressive symptoms.
Further studies also suggest this protection effect differs by gender. Nonetheless, the findings are mixed. For example, several studies hold that men are perceived to gain more health benefits from marriage than women (6, 25), and thus men are always more vulnerable during the transition to widowhood (26, 27). While some other scholars believe that in the context of patriarchy, such as in China, women gain more health benefits from marriage due to gender inequality (11, 28). Because women tend to experience disadvantages in labor markets and face a greater risk of poverty than men, staying in marriage allows women to enjoy better living conditions and health benefits. Thus, women are more negatively affected and are more likely to suffer from poor health after being widowed (29).
An abundance of research has shown that widowhood is linked to a decrease in social support (23, 30–32). Widowhood means the loss of primary support from the deceased spouse. More importantly, with the death of a spouse, relatives, and friends who relied on the spouse to maintain close relationships gradually move away, and the support from their relatives and social networks gradually decline (5, 33), resulting in less social support for the older adults (5). Furthermore, widowhood also leads to poor health status among older adults, creates barriers to social participation and maintaining social connections, and results in changes in social networks and less social support (34). Although some research focused on marital status, and found that widowers received less support than their coupled counterparts (14, 29), little has differentiated the types of social support, such as emotional and instrumental support (29).
Further research suggests that the change in social support for widowed older adults differs by gender. That is, for husbands, widowhood means the loss of the wives' companionship and daily care. And for wives, widowhood means a decline in financial and practical support more than in companionship and daily care. Meanwhile, in marriage, husbands tend to benefit from their wives' network of social support, whereby men might experience difficulty in maintaining relationships with relatives and friends after becoming widowed (35–37).
Social support refers to the actual or perceived availability of resources from the individual's social networks (38), and it has been proven to have a significant positive association with health throughout one's lifespan (39–41). Social support can be classified into emotional support (e.g., providing empathetic understanding and warm care, talking about problems), instrumental support (e.g., entailing help with household tasks or financial aid through goods or services), and companionship (e.g., daily meetings and contact) (42–44). Instrumental support refers to tangible help, such as providing goods or services. Emotional support implies psychological help, entails talking about problems, privacy, and providing advice, and companionship focused on the accompanying of a variety of daily activities (43, 44).
Different types of social support may exert different protective effects on health. Most researchers are interested in emotional and instrumental support and hold it strongly associated with overall health and well-being (42), and it can reduce the risk of dementia and mortality (45, 46), help older adults stay healthy and relieve their psychological stress and burden (13, 47). There are fewer concerns about companionship support, however, they are often supportive in their own right (48, 49). Some researchers focus on the influence of social contacts on health and show significant and meaningful associations between contact frequency and health outcomes (50). Companionship means daily meeting and spending time together, which further influences health status by affecting the mood, attitude, and cognition of widowed older adults (51).
Men and women may receive different types and levels of social support, which may result in different outcomes in health (52). For example, a study found that men benefit from social support in terms of improved mental health, while women benefit from social support in terms of improved physical health (53). Another study on marital loss discovered that perceived social support has a moderate and significant effect on marital transition in men but not in women (29).
China has a large population of widowed older adults. The number of widowed older adults in China has continued to increase since the country transitioned into an aging society in 2000. According to recent survey data, 27.9% of the population aged 65 and older in China are widowed (16.0% for men and 38.6% for women), accounting for a large share of the global population of widowed older adults (2, 54).
Family orientation and gender division are rooted in Chinese society and culture. Family members, especially spouses, are always the primary provider of support. This situation is particularly typical in rural China, where it is characterized as “hollowing,” that is, young people go out to work, leaving the elderly parents to live alone and support each other. Therefore, widowhood may deal a heavier blow to the elderly in China than in western countries. Besides, the Chinese culture is characterized by patrilocality, patrilineality, and patriarchy, in which wives depend heavily on their husbands (55). In such a context, the death of the spouse, who is the most essential and longest-standing family member with older adults, can generate an even more adverse effect on the health of China, and this impact may have gender differences.
Moreover, there is a long-standing urban-rural dual system in China which has in some ways created a marked difference in social networks (56, 57) and medical resources (58, 59). This too could pose a mechanism affecting the health status of widowed older adults. Besides, the social security system in China is less developed and inadequate to provide comprehensive protection for widowed older adults (60), especially in rural areas.
Based on the overview of previous studies, although many studies have examined the relationship between widowhood and health, few have explored whether social support, as well as subtypes, play a mediating role in the relationship between widowhood and health, and the potential gender and urban-rural differences. Our study aims to examine the role of social support in the widowhood-health association of older adults and provide gender and rural-urban-specific analysis. Understanding this can inform policymakers to take more effective measures to help bereaved older adults adjust to life after widowhood and improve their health, which is essential for healthy aging.
The data used in this study was from the China Longitudinal Aging Social Survey of 2014 (CLASS). CLASS is a nationwide, continuous, large-scale social survey project conducted by the Renmin University of China in 2014. Applying the multi-stage stratified probability sampling method and face-to-face interview, CLASS covered 462 villages or communities across 29 provinces, a total of 11,511 participants aged 60 and above in China (excluding Hong Kong, Taiwan, Macau, Hainan, Xinjiang, and Tibet). The data collection was approved by the Ethics Committee of Renmin University of China, and each participant was informed of the purpose of this survey. The participation of each participant in the study was voluntary, and they were assured that their privacy would be strictly protected. Given the purpose of this study that examined the mediating role of social support between widowhood and older adults' health status, all participants who had never been married or divorced were excluded. Additionally, we excluded participants who did not complete the mental health questionnaire due to cognitive impairment (61, 62). Finally, participants with missing values in the variables of interest were excluded. The final analysis sample includes 7,647 participants, among whom 28% were widowed, 46% were women, and 45% lived in rural areas.
Health status, which usually includes mental health and physical health, is a crucial indicator of successful aging (63, 64). For mental health, it was measured using the abbreviated 12-item Center for Epidemiologic Studies Depression scale (CES-D) (65). This instrument is widely used to measure the mental health of older and widowed adults (66–68). The scale includes three questions on positive affect (feeling happy, enjoying life, feeling pleasure), two questions on negative affect (feeling lonely, upset), five questions on marginalization (feeling useless, having nothing to do, unaccompanied, isolated, and neglected) and two questions on somatic symptoms (poor appetite, trouble sleeping). Each item was scored on a scale (0 = most time; 1 = sometimes; 2 = hardly ever), suggesting the frequency of the symptom they experienced last week (the positive items were reverse coded). The sum score ranged from 0 to 24, with higher scores indicating better mental health (Cronbach's α = 0.756).
For physical health, it was assessed by using 10 basic items of the Activities of Daily Living scale (ADL): cleaning, dressing, bathing, self-feeding, controlling bowel and urine, toileting, transferring from bed to chair, indoor transferring, and climbing stairs. Each item was rated on a 3-point scale based on the individual's ability to perform the activities (0 = unable; 1 = with help; 2 = on my own). Higher final sum scores (range = 0–20) are associated with better physical health (Cronbach's α = 0.887).
According to the purpose of the study, we focused on older adults whose marital status is widowed or married with a spouse (non-widowed). Widowhood status was measured by asking the participants' current marital status, and widowhood status was coded as 1 if widowed; otherwise, coded as 0.
Social support was measured using the Lubben Social Network Scale (LSNS), a 6-item scale assessing the availability of social support from friends, relatives, and neighbors. The scale estimates the number of people to talk about privacy, help in need, and contact or meet, using items such as “How many families/relatives do you feel comfortable talking about private matters with?” “How many families/relatives are available to you when you need them?”, and “How many families/relatives do you see or contact at least once a month.” And then the same set of questions were prompted in regards to their relationship with friends. According to the previous research using CLASS data and the scores assigned by the CLASS questionnaire: none (0), one person (1), two persons (2), three to four persons (3), five to eight persons (5), and nine persons and above (9). We added up the scores for each question for each type of support and created a variable whose values ranged from 0 to 54 (69) (Cronbach's α = 0.778). Further, we use the total number of friends, relatives, and neighbors who can talk, help and meet to measure the emotional, instrumental and companionship support. Each subtype of social support ranges from 0 to 18. A higher value indicates stronger perceived social support.
Many covariates were controlled in this study based on prior research (70, 71), including age (60–74 = 0, 75 and above = 1), gender (male = 0, female = 1), ethnicity (Han = 0, minority = 1), hukou type (agricultural = 0, non-agricultural = 1), education level (primary and below = 0, junior high = 1, secondary = 2, university and above = 3), whether with religion (no = 0, yes = 1), participation in community activities (policing patrols, caring for other older adults, environmental protection, mediating disputes, etc.) (no = 0, yes = 1) and living with someone (no = 0, yes = 1).
We used SPSS Macro PROCESS to test the mediation effect of social support in the relationship between widowhood and health among older adults. PROCESS adopts a bias-corrected percentile bootstrap method which is one of the most valid and robust methods for testing mediation effects. Results obtained using this procedure have a higher likelihood of being devoid of Type I error and also estimated more accurate confidence intervals (72–74). An indirect effect is considered significant when the confidence interval does not include a zero.
Below we first described the characteristics of the variable used in this study by adults' widowhood status. Mediation analysis was conducted to examine the mediation effect of social support between widowhood and older adults' health status in the total, male-female subsample, and rural-urban subsample. We conducted a causal mediation analysis to test the reliability of the results. The mediation effect of social support calculates using a sequential approach proposed by Hick and Tingley (75). Following Robins and Greenland (76) and Pearl (77), this method calculates the average of the mediation effects between the actual outcome and counterfactual outcomes to estimate the indirect effects. This causal mediation analysis was performed using STATA 15.1.
Descriptive and chi-square test results between widowed and non-widowed participants are shown in Table 1. Numerical variables were reported as mean ± standard deviation (SD). Categorical variables were reported as proportions (%). As shown in Table 1, there are significant differences in health status and social support between non-widowed and widowed older adults. Specifically, widowed older adults have poorer mental and physical health status, and receive less emotional, instrumental, and companionship support.
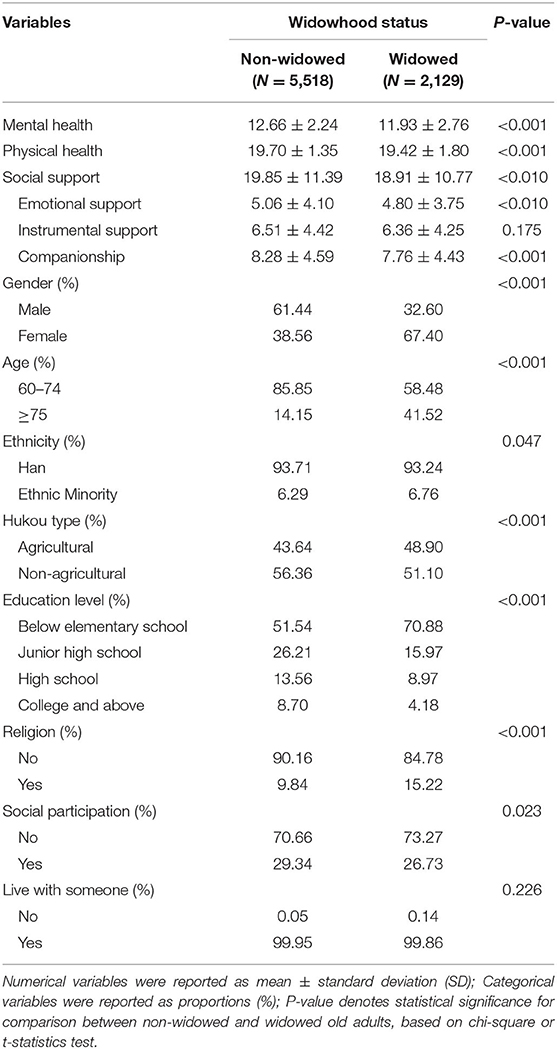
Table 1. Descriptive statistics for widowed vs. non-widowed participants (N = 7,647).
We further follow the procedure of mediation effects analysis proposed by Zhao et al. (72) and refer to the bootstrap test for mediation effects proposed by Preacher and Hayes (73, 78), with 5,000 bootstrap samples to obtain the bias-corrected 95% confidence intervals for the total indirect effect and the specific indirect effects.
Figure 1 shows the results for mediation effects of social support between widowhood status and health status after controlling for socio-demographic characteristics. It can be seen that the coefficient of widowhood on both mental and physical health is reduced after the inclusion of social support. Widowhood has a significant and inverse relationship with social support, that is, older adults perceive less social support in widowhood (β = −0.7111, p < 0.05). Social support did exert a significant but small role in the relationship between widowhood and mental health [β = −0.0325, CI (−0.0610, −0.0049)] as well as physical health [β = −0.0065, CI (−0.0126, −0.0009)]. While it implies that widowhood reduces social support and further affects health.
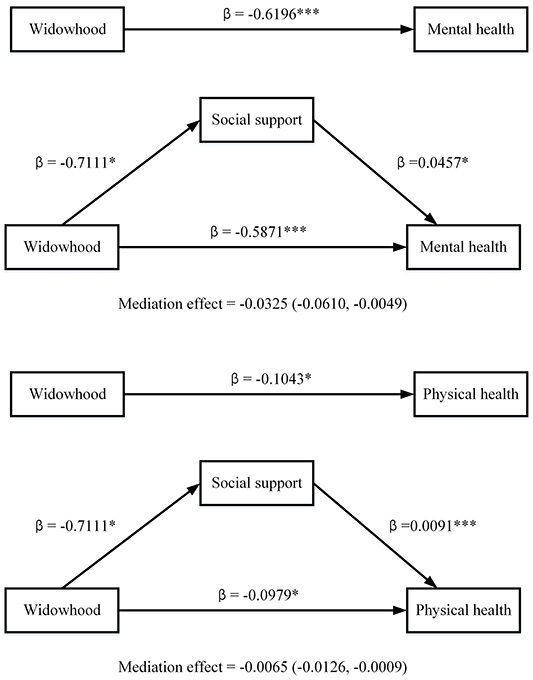
Figure 1. Mediating effects of social support in the association between widowhood and health (N = 7,647). Adjusting for gender, age, ethnicity, hukou, education, religion, social participation, and living arrangement; * p < 0.05, *** p < 0.001; Confidence intervals do not cross zero means the relationship is significant.
Further analyses evaluate the subtypes of social support as mediators in the pathways from widowhood to health (see Table 2). The results revealed detective small mediation effects through emotional support and companionship for mental health [emotional support: β = −0.0076, CI (−0.0161, −0.0004); companionship: β = −0.0191, CI (−0.0338, −0.0063)]. For physical health, companionship was exerted as a significant mediator. However, the effects were also small [companionship: β = −0.009, CI (−0.0163, −0.0029)]. The direct effect of widowhood on mental and physical health was still significant, indicating that social support plays a partial mediating role. Partial mediation does not mean that the data results are not perfect, but implies that it is not the only relationship path.
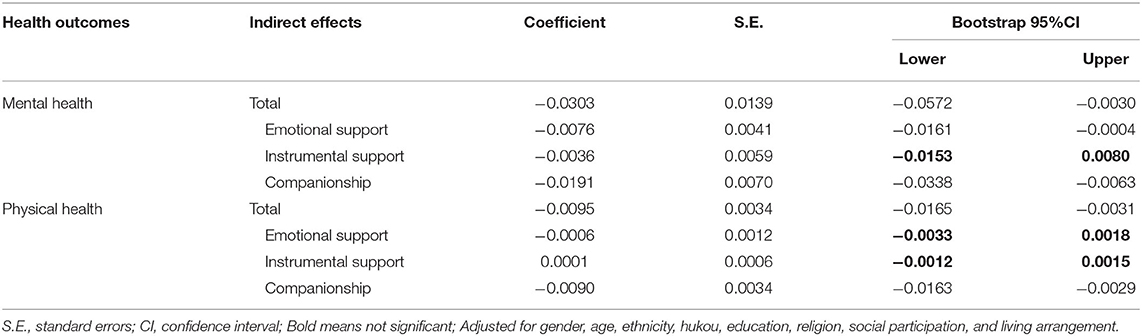
Table 2. Mediation effects of the subtypes of social support in the association between widowhood and health status in the whole sample (N = 7,647).
Then we conducted another set of analyses for different gender and rural-urban subsamples, reviewing the different role of social support in it. Significant mediation effects were only found in women and rural older adults. For women (see in Table 3), instrumental support and companionship have significant mediated effects in the relationship between widowhood and mental health [instrumental support: β = −0.0106, CI (−0.0243, −0.001); companionship: β = −0.0239, CI (−0.0419, −0.0087)]. Companionship significantly mediated the relationship between widowhood and physical health [companionship: β = −0.0172, CI (−0.0306, −0.0071)]. For males (see in Table 4), however, the mediating effect of social support was not significant because the impact of widowhood on social support was not significant.
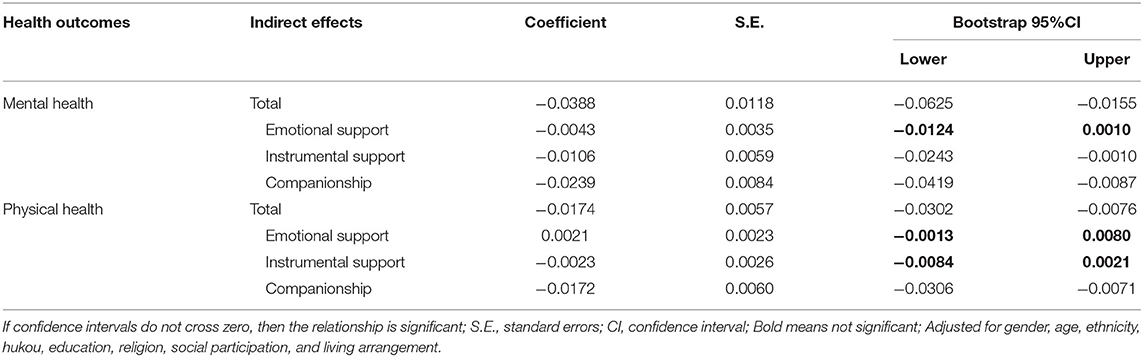
Table 3. Mediation effects of the subtypes of social support in the association between widowhood and health status in the female subsample (N = 4,084).
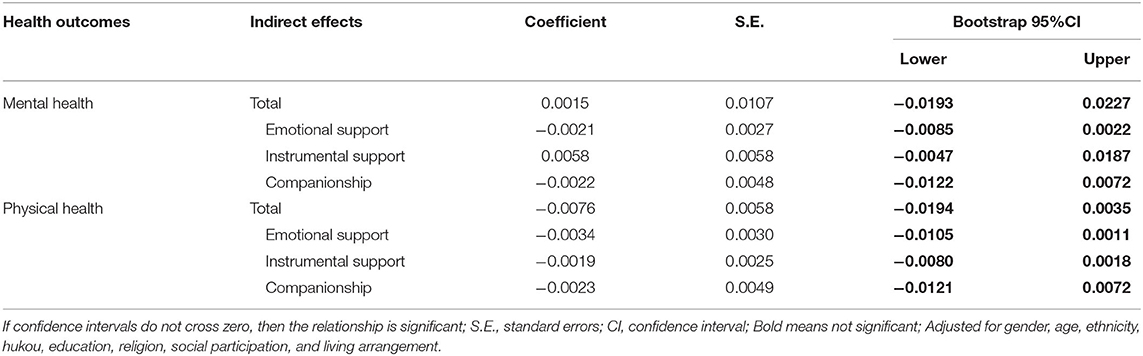
Table 4. Mediation effects of the subtypes of social support in the association between widowhood and health status in the male subsample (N = 3,563).
For rural older adults (see in Table 5), the mediating effect of companionship in the pathways from widowhood to mental (β = −0.0175, CI (−0.0345, −0.0044)] and physical health was significant [physical heath: β = −0.0079, CI (−0.0173, −0.0012)]. For urban older adults (see in Table 6), the mediating effect of social support was not significant.
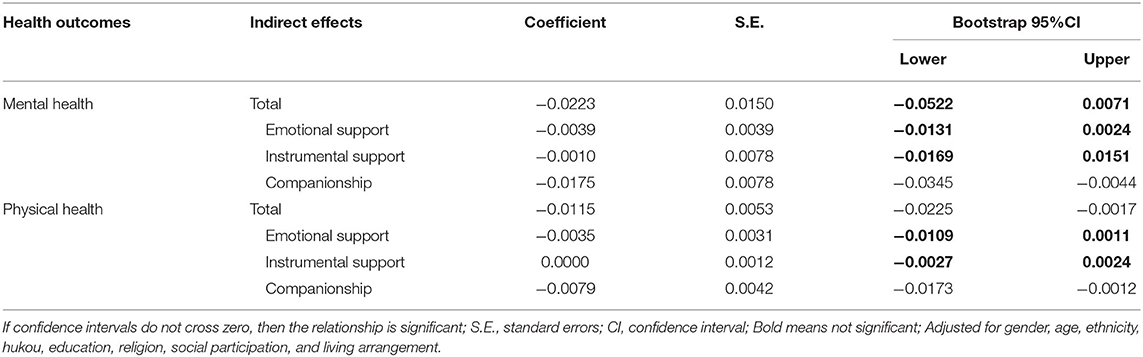
Table 5. Mediation effects of the subtypes of social support in the association between widowhood and health status in the rural subsample (N = 3,449).
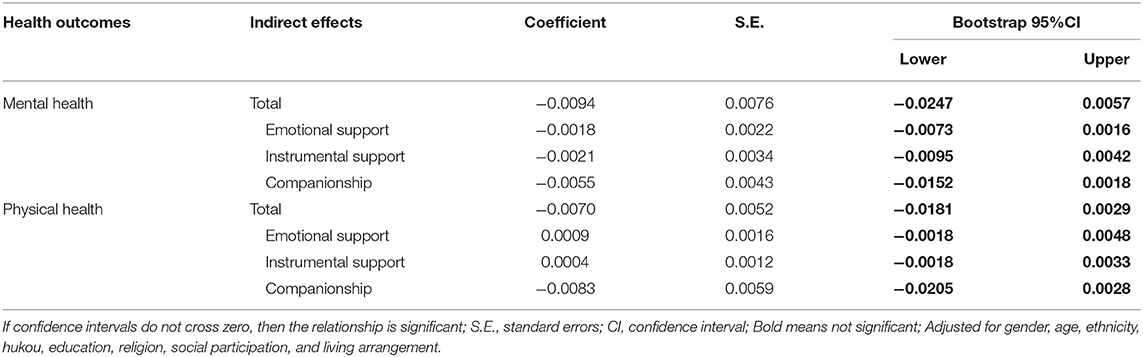
Table 6. Mediation effects of the subtypes of social support in the association between widowhood and health status in the urban subsample (N = 4,198).
Table 7 shows the results of causal mediation analysis. Becoming widowed was significantly associated with a mean score reduction in mental and physical health. When emotional support and companionship were modeled as mediators, the estimated indirect effect was significant, indicating the indirect effect through emotional support and companionship can explain the change in mental health and physical health. This is consistent with the findings of our main analysis.
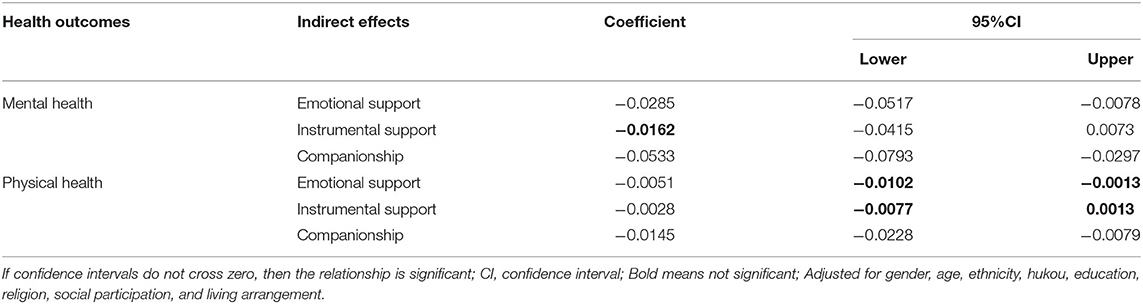
Table 7. Causal mediation effects of the subtypes of social support in the association between widowhood and health status in the whole sample (N = 7,467).
Using data from the 2014 wave of China Longitudinal Aging Social Survey, this study examined the mediation effects of social support, as well as different types including emotional support, instrumental support, and companionship, on the association between widowhood and older adults' health status. It was found that emotional support and companionship exerted a mediation effect on the influence of widowhood and health status. It indicates that older adults perceive significantly less emotional support and companionship after widowhood, leading to poorer mental health and physical health. Furthermore, women and rural older adults are more likely to be affected by the reduced emotional support and companionship caused by widowhood.
This study found that social support is an essential path through which widowhood is negatively associated with the health of old adults. It is consistent with other findings suggestive of the fact that social support explains part of the effects of widowhood on health (66, 79–81). Specifically, emotional support and companionship play a significant role in the relationship between widowhood and mental health as well as physical health. However, the contribution of social support here is small, as has also been found in other research exploring the mechanism of health outcomes (82–84). But this kind of small mediating role does exist, especially the mediating effect of emotional support and companionship.
Emotional support assumes a partial mediating role in the relationship between widowhood and mental health. It suggests that the negative effect of widowhood on the mental health of older adults is partly due to the reduced emotional support from family, relatives, and friends. This is consistent with previous studies which have shown that emotional support may be linked to widowhood and mental health (66, 85). And support is most helpful for widowed older adults to have the opportunity to freely express themselves (86). For older adults, a spouse is the main person to share private thoughts, boredom, depression. However, if a spouse who plays such an important role becomes deceased, it may create a void and, in the long run, may affect psychological health. And after the death of a spouse, older adults may be overwhelmed with grief and nostalgia for their spouse. For example, they will close themselves off and no longer share their hearts with others. This finding underscores the fact that emotional support is key in ameliorating the harmful effects of widowhood among older adults. Also, that older adults need communication and care to alleviate the intense psychological toll of widowhood.
Companionship plays an indispensable role in the pathway from widowhood to health outcomes. Companionship partially mediates the relationship between widowhood and health. That is, the negative association of widowhood with the mental and physical health of older adults is due to the decreased social interaction with family, relatives, and friends. Older people with close relationships tend to engage more in physical activities, have better dietary behavior, and have better access to information that may be beneficial to health (87, 88). However, the shrunken social network that is likely to characterize widowhood in older adults may be detrimental to health. Specifically, besides the void created when a spousal intimate relationship once relied upon is no longer available, widowed older adults may develop negative emotions like depression, pessimism, guilt, or fear of becoming a burden unto others. This may culminate in an unwillingness to interact with others or seek help. Such alienation amplifies the feelings of loneliness and loss, which may, in turn, impact physical functioning as well as both mental and physical health (89).
After taking gender into account, the mediation role of social support is only significant for women. This is consistent with some previous studies. Using data from Korea, Jeon found that social ties better explained the effect of widowhood on depression in women than in men (66). This phenomenon may be explained by the fact that with the transition to widowhood, women are more sensitive to such changes and tend to experience broader changes in social networks (90, 91). Furthermore, in a strongly patriarchal society such as China, women in marriage rely heavily on their husbands' status, power, and social resources, and are more affected by the changes caused by widowhood (92–94). In contrast, compared to women, elderly males have smaller social networks and are less likely to initiate or engage in social outdoor activities (52). Thus, widowhood has little effect on changes in social network size for elderly males, and the mediating role of social support is not significant either.
The mediating role of social support was only significant among rural older adults rather than urban older adults. That is, companionship significantly mediated the relationship between widowhood and mental as well as physical health in rural older adults. This may occur due to the disparities in the conception of marriage and the availability of social support between rural and urban areas (10, 95). In rural China, multigenerational cohabitation is very common, and social relationships are still dominated by family or clan; therefore, widowhood is more affected by changes in this network (56). While in urban areas, older adults have a wider social network and more social security resources, such as community-based care and scientific spiritual comfort. In addition, there are elderly colleges sponsored by the government and the community, to provide older residents with health information and creative enlightenment, as well as a place to meet new friends (96). As a result, the elderly have more opportunities to engage in social activities. All these may serve as a potential resource for social support, compensating for the decrease in social support resulting from the death of a spouse. Moreover, although it is seldom to hold multigenerational families in urban China, older adults tend to cohabitate with their children after being widowed, in order to provide care and nurturing for their grandchildren. This may provide a sense of belonging and continued engagement in family functions (97).
Our results did not find a significant difference in instrumental support between widowed and non-widowed older adults, and instrumental support did not play a mediating role in the relationship between widowhood and health status. Indeed, influenced by the Confucian ideology, the young generation should support the elderly, ensuring they are well-fed and clothed. Although this kind of support is mainly focused on material support and is always less mandatory in the aspects of spiritual, psychological care, and affection (98, 99), it does not change due to widowhood. So the mediating role of instrumental support is not significant.
This study still has several limitations to this study, which highlight the need for future research to better understand the connection between widowhood and health. First, analyses are limited by using self-report measures of mental and physical health scales, and they may differ when using objective assessments. Besides, we use the limitation of activities as a measure of physical health. While ADLs are an important component of health status, addressing functional status, other key components of health status in older adults include perceived health status, cognitive status, pain, and perceived quality of life, which need further research. Second, although we used a large sample size, it is cross-sectional data. This study only established a correlation but cannot make a causal inference. Further studies are needed to identify the causal mechanism of widowhood's effects on health based on longitudinal data. Thirdly, we only evaluated the partial mediation effects between widowhood and health status, and the effects of the mediator are small. Therefore, we urge some caution in interpreting our results. And there may likely be a case of missed variables that needs further research. For example, previous studies indicate that different sources and structures (relatives, friends, community, government agencies, etc.) of social support may differ in their functions (100–102). Thus, more work needs to be done to explore the role of social support in this association. Finally, it is also a limitation that CLASS doesn't provide other important contextual information about widowhood, such as time since the death of the spouse, age at the time of spouse's death, widowed person's perceived closeness to the spouse, or size of support system before widowhood. This limits our ability to meaningfully interpret the findings. Further research is needed.
Despite these limitations, our study extends the body of literature by providing evidence as to how widowhood may have deleterious effects on health, and how it differs across gender and urban vs. more remote residential areas. This study proposed that emotional support and companionship could potentially mediate the extent to which widowhood affects health. The evidence also suggests that it is only among rural and older women that social support plays a significant role in the association between widowhood and health. It underscores the evidence that emotional support and companionship may be associated with measures that improve the impact of widowhood on the health of older adults, particularly women and rural older adults.
Publicly available datasets were analyzed in this study. This data can be found here: http://class.ruc.edu.cn/.
The studies involving human participants were reviewed and approved by the Ethics Committee of Renmin University of China. The patients/participants provided their written informed consent to participate in this study.
YG and TG designed the study, performed the statistical analysis, and drafted the manuscript. LM, LW, and JL collaborated with the study and revised the manuscript. All authors have given approval to the final version for publication.
This work was supported by a Major Project of National Social Science Foundation of China (21ZDA103) and a National Social Science Foundation of China (18BRK012).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.745073/full#supplementary-material
CLASS, The China Longitudinal Aging Social Survey; CES-D, Center for Epidemiological Studies Depression Scale; ADL, activities of daily living; S.E., Standard errors; CI, confidence interval.
3. Stroebe M, Schut H, Boerner K. Models of Coping with Bereavement: An Updated Overview. Estud Psicol-Madrid. (2017) 38:582–607. doi: 10.1080/02109395.2017.1340055
5. Isherwood LM, King DS, Luszcz MA. Widowhood in the fourth age: support exchange, relationships and social participation. Ageing Soc. (2017) 37:188–212. doi: 10.1017/S0144686X15001166
6. Jadhav A, Weir D. Widowhood and depression in a cross-national perspective: evidence from the United States, Europe, Korea, and China. J Gerontol B-Psychol. (2018) 73:E143–E53. doi: 10.1093/geronb/gbx021
7. Kristiansen CB, Kjaer JN, Hjorth P, Andersen K, Prina AM. The association of time since spousal loss and depression in widowhood: a systematic review and meta-analysis. Soc Psych Psych Epid. (2019) 54:781–92. doi: 10.1007/s00127-019-01680-3
8. van den Brink CL, Tijhuis M, van den Bos GAM, Giampaoli S, Kivinen P, Nissinen A, et al. Effect of widowhood on disability onset in elderly men from three European countries. J Am Geriatr Soc. (2004) 52:353–8. doi: 10.1111/j.1532-5415.2004.52105.x
9. Vable AM, Subramanian SV, Rist PM, Glymour MM. Does the “Widowhood Effect” precede spousal bereavement? Results from a nationally representative sample of older adults. Am J Geriat Psychiat. (2015) 23:283–92. doi: 10.1016/j.jagp.2014.05.004
10. Hu LC. Marital status and self-rated health in china: a longitudinal analysis. Popul Res Policy Rev. (2020) 40:499–531. doi: 10.1007/s11113-020-09593-9
11. Burns RA, Browning CJ, Kendig HL. Examining the 16-year trajectories of mental health and wellbeing through the transition into widowhood. Int Psychogeriatr. (2015) 27:1979–86. doi: 10.1017/S1041610215000472
12. Li YW, Chi I, Krochalk PC, Xu L. Widowhood, family support, and self-rated health among older adults in China. Int J Soc Welf. (2011) 20:S72–85. doi: 10.1111/j.1468-2397.2011.00818.x
13. Sullivan C, Infurna FJ. The multidimensional nature of social support and engagement in contributing to adjustment following spousal loss. Aging Ment Health. (2020) 24:857–69. doi: 10.1080/13607863.2018.1555695
14. Manvelian A, Sbarra DA. Marital status, close relationships, and all-cause mortality: results from a 10-year study of nationally representative older adults. Psychosom Med. (2020) 82:384–92. doi: 10.1097/PSY.0000000000000798
15. Vala CH, Lorentzon M, Sundh V, Johansson H, Lewerin C, Sten S, et al. Increased risk for hip fracture after death of a spouse-further support for bereavement frailty? Osteoporosis Int. (2020) 31:485–92. doi: 10.1007/s00198-019-05242-w
16. van Boekel LC, Cloin JCM, Luijkx KG. Community-dwelling and recently widowed older adults: effects of spousal loss on psychological well-being, perceived quality of life, and health-care costs. Int J Aging Hum Dev. (2021) 92:65–82. doi: 10.1177/0091415019871204
17. Verbrugge LM. Gender and health: an update on hypotheses and evidence. J Health Soc Behav. (1985) 26:156–82. doi: 10.2307/2136750
18. Rendall MS, Weden MM, Favreault MM, Waldron H. The protective effect of marriage for survival: a review and update. Demography. (2011) 48:481–506. doi: 10.1007/s13524-011-0032-5
20. Hu YR, Goldman N. Mortality differentials by marital status: an international comparison. Demography. (1990) 27:233–50. doi: 10.2307/2061451
21. Emanuele S, Lucia G, Claudia G, Silvia G, Marzia B, Antonio C, et al. Marital and cohabitation status as predictors of mortality: a 10-year follow-up of an Italian elderly cohort. Soc Sci Med. (2008) 67:1456–64. doi: 10.1016/j.socscimed.2008.06.026
22. Blomgren J, Martikainen P, Grundy E, Koskinen S. Marital history 1971-91 and mortality 1991-2004 in England & Wales and Finland. J Epidemiol Commun H. (2012) 66:30–6. doi: 10.1136/jech.2010.110635
23. Jeannette Golden, Rona'n M., Conroy, Irene Bruce, Denihan A, Greene E, Kirby M, et al. Loneliness, social support networks, mood and wellbeing in community-dwelling elderly. Int J Geriatr Psych. (2009) 24:694–700. doi: 10.1002/gps.2181
24. Forster F, Luppa M, Pabst A, Heser K, Kleineidam L, Fuchs A, et al. The role of social isolation and the development of depression. a comparison of the widowed and married oldest old in Germany. Int J Env Res Pub He. (2021) 18:1–12. doi: 10.3390/ijerph18136986
25. de Vries B, Utz R, Caserta M, Lund D. Friend and family contact and support in early widowhood. J Gerontol B-Psychol. (2014) 69:75–84. doi: 10.1093/geronb/gbt078
26. Umberson D, Wortman CB, Kessler RC. Widowhood and depression-explaining long-term gender differences in vulnerability. J Health Soc Behav. (1992) 33:10–24. doi: 10.2307/2136854
27. Williams K, Umberson D. Marital status, marital transitions, and health: a gendered life course perspective. J Health Soc Behav. (2004) 45:81–98. doi: 10.1177/002214650404500106
28. Perrig-Chiello P, Spahni S, Höpflinger F, Carr D. Cohort and gender differences in psychosocial adjustment to later-life widowhood. J Gerontol Series B. (2015) 71:765–74. doi: 10.1093/geronb/gbv004
29. Hewitt B, Turrell G, Giskes K. Marital loss, mental health and the role of perceived social support: findings from six waves of an Australian population based panel study. J Epidemiol Commun H. (2012) 66:308–14. doi: 10.1136/jech.2009.104893
30. Sasson I, Umberson DJ. Widowhood and depression: new light on gender differences, selection, and psychological adjustment. J Gerontol B. (2014) 69:135–45. doi: 10.1093/geronb/gbt058
31. Williams BR, Sawyer P, Allman RM. Wearing the garment of widowhood: variations in time since spousal loss among community-dwelling older adults. J Women Aging. (2012) 24:126–39. doi: 10.1080/08952841.2012.639660
32. Holt-Lunstad J. The potential public health relevance of social isolation and loneliness: prevalence, epidemiology, and risk factors. Public Policy Aging Rep. (2017) 27:127–30. doi: 10.1093/ppar/prx030
33. Donnelly EA, Hinterlong JE. Changes in social participation and volunteer activity among recently widowed older adults. Gerontol. (2010) 50:158–69. doi: 10.1093/geront/gnp103
34. Cornwell B, Schumm LP, Laumann EO, Kim J, Kim YJ. Assessment of social network change in a national longitudinal survey. J Gerontol B. (2014) 69:S75–82. doi: 10.1093/geronb/gbu037
35. Okabayashi H, Liang J, Krause N, Akiyama H, Sugisawa H. Mental health among older adults in Japan: do sources of social support and negative interaction make a difference? Soc Sci Med. (2004) 59:2259–70. doi: 10.1016/j.socscimed.2004.02.024
36. Arai A, Ishida K, Tomimori M, Katsumata Y, Grove JS, Tamashiro H. Association between lifestyle activity and depressed mood among home-dwelling older people: a community-based study in Japan. Aging Ment Health. (2007) 11:547–55. doi: 10.1080/13607860601086553
37. Sugihara Y, Sugisawa H, Shibata H, Harada K. Productive roles, gender, and depressive symptoms: evidence from a national longitudinal study of late-middle-aged Japanese. J Gerontol B-Psychol. (2008) 63:227–34. doi: 10.1093/geronb/63.4.P227
38. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
39. Duboz P, Boëtsch G, Gueye L, Macia E. Selfrated health in Senegal: a comparison between urban and rural areas. PLoS ONE. (2017) 12:1–16. doi: 10.1371/journal.pone.0184416
40. Khalid A, Dawood S. Social support, self-efficacy, cognitive coping and psychological distress in infertile women. Arch Gynecol Obstetr. (2020) 30:423–30. doi: 10.1007/s00404-020-05614-2
41. White S, Foster R, Marks J, Morshead R, Goldsmith L, Barlow S, et al. The effectiveness of one-to-one peer support in mental health services: a systematic review and meta-analysis. BMC Psychiatry. (2020) 20:1–20. doi: 10.1186/s12888-020-02923-3
42. House JS, Landis KR, Umberson D. Social relationships and health. Science. (1988) 241:540–4. doi: 10.1126/science.3399889
43. D. Alio J. J., Okiror J. G., Agea, Matsiko FB, Ekere W. Influence of social networks and social support on credit utilization in the savings and credit cooperatives in Soroti District, Uganda. J Agr Extens Rural Dev. (2018) 10:54–60. doi: 10.5897/JAERD2017.0877
44. Wang S, Yang XI. A social support networks and quality of life of rural men in a context of marriage squeeze in China. Am J Men's Health. (2018) 12:706–19. doi: 10.1177/1557988317753263
45. Salinas J, Beiser A, Himali JJ, Satizabal CL, Aparicio HJ, Weinstein G, et al. Associations between social relationship measures, serum brain-derived neurotrophic factor, and risk of stroke and dementia. Alzheimer's Dementia. (2017) 3:229–37. doi: 10.1016/j.trci.2017.03.001
46. National Academies of Sciences Engineering and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System. Washington, DC: National Academies of Sciences, Engineering, and Medicine (2020).
47. Wortman CB, Silver RC. Successful mastery of bereavement and widowhood: a life-course perspective. In: Baltes PB, Baltes MM, editors. Successful Aging: Perspectives from the Behavioral Sciences. New York, NY: Cambridge University Press (1990) 225–64. doi: 10.1017/CBO9780511665684.010
48. Fischer CS. To Dwell among Friends: Personal Networks in Town and City. Chicago, IL: University of Chicago Press (1982).
49. Wills TA. Supportive Functions of Interpersonal Relationships. In: Syme CSL, editor. Social Support and Health. New York, NY: Academic Press (1985). p. 61–82.
50. Teo AR, Choi H, Andrea SB, Valenstein M, Newsom JT, Dobscha SK, et al. Does mode of contact with different types of social relationships predict depression in older adults? Evidence from a Nationally Representative Survey. J Am Geriatr Soc. (2015) 63:2014–22. doi: 10.1111/jgs.13667
51. Debra U, Robert C, Corinne R. Social relationships and health behavior across life course. Ann Rev Sociol. (2010) 36:139–57. doi: 10.1146/annurev-soc-070308-120011
52. Kneavel M. Relationship between gender, stress, and quality of social support. Psychol Rep. (2020) 124:1481–501. doi: 10.1177/0033294120939844
53. Lee CYS, Dik BJ. Associations among stress, gender, sources of social support, and health in emerging adults. Stress Health. (2017) 33:378–88. doi: 10.1002/smi.2722
55. Thornton A, Lin HS. Social Change and the Family in Taiwan. Chicago, IL: University of Chicago Press (1994).
56. Dong XQ, Simon MA. Health and aging in a Chinese population: urban and rural disparities. Geriatr Gerontol Int. (2010) 10:85–93. doi: 10.1111/j.1447-0594.2009.00563.x
57. Nzabona A, Ntozi J, Rutaremwa G. Loneliness among older persons in Uganda: examining social, economic and demographic risk factors. Ageing Soc. (2016) 36:860–88. doi: 10.1017/S0144686X15000112
58. Zhang YL, Zhou ZL, Gao JM, Wang D, Zhang Q, Zhou ZY, et al. Health-related quality of life and its influencing factors for patients with hypertension: evidence from the urban and rural areas of Shaanxi Province, China. BMC Health Serv Res. (2016) 16:277. doi: 10.1186/s12913-016-1536-x
59. Zhang CC, Lei XY, Strauss J, Zhao YH. Health insurance and health care among the mid-aged and older Chinese: evidence from the national baseline survey of Charls. Health Econ. (2017) 26:431–49. doi: 10.1002/hec.3322
60. Phillips DR, Feng Z. Challenges for the aging family in the People's Republic of China. Canad J Aging. (2015) 3:290–304. doi: 10.1017/S0714980815000203
61. Wang J, Chen T, Han B. Does co-residence with adult children associate with better psychological well-being among the oldest old in China? Aging Ment Health. (2014) 18:232–9. doi: 10.1080/13607863.2013.837143
62. Chen HL, Chi I, Liu RT. Hospital utilization among Chinese older adults: patterns and predictors. J Aging Health. (2019) 31:1454–78. doi: 10.1177/0898264318780546
63. Freund AM, Baltes PB. Selection, optimization, and compensation as strategies of life management: correlations with subjective indicators of successful aging. Psychol Aging. (1998) 13:531–43. doi: 10.1037/0882-7974.13.4.531
64. Cecilia SM, Francisco Jos'e EO. Training mental health peer support training facilitators: a qualitative, participatory evaluation. Int J Ment Health Nu. (2021) 30:261–73. doi: 10.1111/inm.12781
65. Radloff LS. The Ces-D scale: a self-report depression scale for research in the general population. Appl Psychol Measur. (1977) 1:385–401. doi: 10.1177/014662167700100306
66. Jeon GS, Jang SN, Kim DS, Cho SI. Widowhood and depressive symptoms among korean elders: the role of social ties. J Gerontol B-Psychol. (2013) 68:963–73. doi: 10.1093/geronb/gbt084
67. Fastame MC, Manca C, Penna MP, Lucangeli D, Hitchcott PK. Numeracy skills and self-reported mental health in people aging well. Psychiat Quart. (2019) 90:629–35. doi: 10.1007/s11126-019-09655-y
68. Deborah C. Mental health of older widows and widowers: which coping strategies are most protective. Pubmed. (2020) 24:291–9. doi: 10.1080/13607863.2018.1531381
69. Shi C, Hu B. Preferences for formal social care in rural and urban China: evidence from a national survey. J Gerontol Soc Work. (2020) 63:19–40. doi: 10.1080/01634372.2019.1709246
70. Zeng Y, George LK. Population ageing and old-age insurance in China. In: Dannefer D, Phillipson C, editors. The Sage Handbook of Social Gerontology. Los Angeles, CA: SAGE (2010). p. 421.
71. Standridge SH, Dunlap R, Kleiber DA, Aday RH. Widowhood and leisure: an exploration of leisure's role in coping and finding a new self. J Leisure Res. (2020) 51:1–18. doi: 10.1080/00222216.2020.1844553
72. Zhao XS, Lynch JG, Chen Q. Reconsidering Baron and Kenny: myths and truths about mediation analysis. J Consumer Res. (2010) 37:197–206. doi: 10.1086/651257
73. Hayes AF. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. New York, NY: The Guilford Press (2013).
74. Ren Q, Treiman DJ. Living arrangements of the elderly in china and consequences for their emotional well-being. Chinese Sociol Rev. (2015) 47:255–86. doi: 10.1080/21620555.2015.1032162
75. Hick R, Tingley D. Causal mediation analysis. Stata J. (2011) 11:605–19. doi: 10.1177/1536867X1201100407
76. Robins JM, Greenland S. Identifiability and exchangeability for direct and indirect effects. Epidemiology. (1992) 3:143–55. doi: 10.1097/00001648-199203000-00013
77. Pearl J. Direct and indirect effects. In: Proceedings of the Seventeenth Conference in Uncertainty in Artificial Intelligence. San Francisco: Morgan Kaufmann (2001).
78. Preacher kJ, Hayes AF. Spss and Sas procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instr Comp. (2004) 36:717–31. doi: 10.3758/BF03206553
79. van Grootheest DS, Beekman ATF, van Groenou MIB, Deeg DJH. Sex differences in depression after widowhood. do men suffer more? Soc Psych Psych Epid. (1999) 34:391–8. doi: 10.1007/s001270050160
80. Cairney J, Corna LM, Veldhuizen S, Kurdyak P, Streiner DL. The social epidemiology of affective and anxiety disorders in later life in Canada. Canad J Psychiatry. (2008) 53:104–11. doi: 10.1177/070674370805300205
81. Momtaz YA, Hamid TA, Yahaya N, Ibrahim R. Widowhood and psychological well-being among older Malaysians mediating effect of social network. Indian J Soc Work. (2009) 70:375–90.
82. Power JEM, Lawlor BA, Kee F. Social support mediates the relationships between extraversion, neuroticism, and cognitive function in older adults. Public Health. (2017) 147:144–52. doi: 10.1016/j.puhe.2017.02.015
83. Mao XP, Zhang LW, Liu YR. Stressors and subjective well-being among Chinese older adults: uncovering the buffering roles of tangible support patterns. J Cross Cult Psychol. (2021) 52:78–98. doi: 10.1177/0022022120977042
84. Lin CY, Namdar P, Griffiths MD, Pakpour AH. Mediated roles of generalized trust and perceived social support in the effects of problematic social media use on mental health: a cross-sectional study. Health Expect. (2020) 24:165–73. doi: 10.1111/hex.13169
85. Zhang BS, Li J. Gender and marital status differences in depressive symptoms among elderly adults: the roles of family support and friend support. Aging Ment Health. (2011) 15:844–54. doi: 10.1080/13607863.2011.569481
86. Merz EM, Gierveld JD. Childhood memories, family ties, sibling support and loneliness in ever-widowed older adults: quantitative and qualitative results. Ageing Soc. (2016) 36:534–61. doi: 10.1017/S0144686X14001329
87. Frongillo EA, Rauschenbach BS, Roe DA, Williamson DF. Characteristics related to elderly persons' not eating for one or more days: implications for meal programs. Am J Public Health. (1992) 82:600–2. doi: 10.2105/AJPH.82.4.600
88. Watt RG, Heilmann A, Sabbah W, Newton T, Chandola T, Aida J, et al. Social relationships and health related behaviors among older us adults. BMC Public Health. (2014) 14:1–11. doi: 10.1186/1471-2458-14-533
89. Cacioppo J, Hawkley L, Crawford L. Loneliness and health: potential mechanisms. Psychosomatic Med. (2002) 64:407–17. doi: 10.1097/00006842-200205000-00005
90. Morgan DL, March SJ. The impact of life events on networks of personal relationships - a comparison of widowhood and caring for a spouse with Alzheimers-disease. J Soc Pers Relat. (1992) 9:563–84. doi: 10.1177/0265407592094006
91. Uchino BN, Cacioppo JT, KiecoltGlaser JK. The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychol Bull. (1996) 119:488–531. doi: 10.1037/0033-2909.119.3.488
92. Krochalk PC, Li YW, Chi I. Widowhood and self-rated health among Chinese elders: the effect of economic condition. Australas J Ageing. (2008) 27:26–32. doi: 10.1111/j.1741-6612.2007.00269.x
93. Sargeson S. Why women own less, and why it matters more in rural china's urban transformation. China Persp. (2012) 4:35–42. doi: 10.4000/chinaperspectives.6025
94. Perkins JM, Lee HY, James KS, Oh J, Krishna A, Heo J, et al. Marital status, widowhood duration, gender and health outcomes: a cross-sectional study among older adults in India. Bmc Public Health. (2016) 16:1032. doi: 10.1186/s12889-016-3682-9
95. Guo M, Chi I, Silverstein M. Intergenerational support and depression among Chinese older adults: do gender and widowhood make a difference? Ageing Soc. (2017) 37:695–724. doi: 10.1017/S0144686X15001403
96. Global Times. China's ‘Elderly Colleges’ Teach Senior Citizens How to Stay Hip China. (2019). Available online at: https://www.globaltimes.cn/content/1139496.shtml (Accessed October 22, 2021).
97. Tiedt AD. The gender gap in depressive symptoms among japanese elders: evaluating social support and health as mediating factors. J Cross-Cult Gerontol. (2010) 25:239–56. doi: 10.1007/s10823-010-9122-x
98. Cheng Y, Xi J, Rosenberg M, Gao S. Intergenerational differences in social support for the community-living elderly in Beijing, China. Health Sci Rep. (2018) 1:e96. doi: 10.1002/hsr2.96
99. Bai X, Lai D, Liu C. Personal care expectations: photovoices of Chinese ageing adults in Hong Kong. Health Social Care. (2020) 28:1071–81. doi: 10.1111/hsc.12940
100. Tiedt AD, Saito Y, Crimmins EM. Depressive symptoms, transitions to widowhood and informal support from adult children among older women and men in Japan. Res Aging. (2016) 38:619–42. doi: 10.1177/0164027515595442
101. Huang JL, Jiang ZY, Zhang T, Wang L, Chu YM, Shen M, et al. Which matters more for medication adherence among disabled people in Shanghai, China: family support or primary health care? J Health Care Org Provis Finan. (2019) 56:1–10. doi: 10.1177/0046958019883175
Keywords: widowhood, social support, health, mediation effects, older adults
Citation: Guo Y, Ge T, Mei L, Wang L and Li J (2021) Widowhood and Health Status Among Chinese Older Adults: The Mediation Effects of Different Types of Support. Front. Public Health 9:745073. doi: 10.3389/fpubh.2021.745073
Received: 21 July 2021; Accepted: 25 October 2021;
Published: 17 November 2021.
Edited by:
Qiushi Feng, National University of Singapore, SingaporeReviewed by:
Jon Barrenetxea, Duke-NUS Medical School, SingaporeCopyright © 2021 Guo, Ge, Mei, Wang and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tingshuai Ge, YmFjY2FfZ3RzQDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.