 Faizus Sazzad
Faizus Sazzad V. Priya Rajan1,3
V. Priya Rajan1,3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 15 December 2021
Sec. Public Health Policy
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.743748
Strong leadership in public sector innovation can empower governments to address community challenges in new ways in light of the challenges posed by the global coronavirus pandemic. Coronavirus management policy, pandemic responses, needs, and options are reflected in various Asian countries in respective published literature, but a summarized synthesis is not available. Using a systematic review approach (PRISMA), this study has analyzed the role of leadership in public sector innovation in COVID-19 management and synthesized 23 articles from 23 different Asian countries. In the light of available data, public sector innovation (PSI) and the role played by the leadership of each country' have been found to be largely inter-dependent. The current review provides a cross-section of the ongoing nature of the pandemic, as management responses and trend data in the countries are still emerging or evolving. Additionally, our study contributes a current state report regarding the barriers facing the leadership of Asian countries in mitigating the global pandemic through PSI. Our study found that a strong political leadership presence combined with a technocratic approach and a highly-skilled public sector workforce, could lead to more tremendous success in managing the outbreak. Furthermore, religious leadership was also found to have a potentially significant role in COVID-19 management strategies.
Asia was the first region to be affected by the global pandemic of the Coronavirus (COVID-19), particularly countries in East and Southeast Asia which saw rapid growth in the number of confirmed cases and deaths when COVID-19 broke out in early 2020. The ensuing economic downturn caused by global trade disruptions, cessation of tourism, and regional containment measures brought on socio-economic challenges, which eventually forced some countries to take the initiative and adopt innovative measures in their overall policy responses for COVID-19 management (1, 2).
The purpose of this article is to examine the role of leadership in public sector innovation (PSI), specifically in addressing the challenges in public health management of the global COVID-19 outbreak from 2020 using a systematic review. This evaluation is based on a systemic review of scholarly studies of the leadership role in the various PSI adopted in 23 Asian countries to manage their respective COVID-19 outbreaks. This article provides a “state-of-art” summary of the PSI impact, categorized leadership role, and policy responses employed in Asian countries during the global pandemic.
PSI can be defined as novel services, technologies, organizational structures, management approaches, processes, or policies adopted by government agencies to address specific challenges confronting the organization, nation, or society (3–5). Leadership has been acknowledged as one of the most important factors influencing the success or failure of PSI (6, 7). Leadership in PSI can take the form of top-down innovation initiated by executive leadership and bottom-up innovation started by civil servants on the ground (8, 9). Particularly in a significant or national crisis, PSI tends to be “led by politicians” in response to crises (10). The COVID-19 pandemic is a prime example of a national crisis, and evaluating the management responses across different countries presents an opportunity to understand how effective leadership can drive PSI. This review explores these challenges for leaders and decision-makers and evaluates the generalizability of the leadership role in PSI processes across Asian nations.
The rest of the article is organized as follows: The first section will explain the rationale and context of the research. Section methods will provide information about methods, such as search strategy, which is a systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) method. Section results will report results, and section discussion will discuss the findings along with implications, limitations, and future research directions. Finally, this article ends with a conclusion. The main finding of this article is that leadership styles can influence the level of innovation adopted and the success or failure of the strategic response. More research in this area, particularly on religious leadership as a source of innovation, could be helpful. The statistical calculation may not reflect the impact of PSI and leadership role in the short term, and long-term impact is yet to be achieved, as the COVID-19 situation is continuously evolving.
Much has been written since 2020 about the responses to COVID-19 across different countries (1, 2, 11). The novelty of the virus presented unknown and evolving challenges that continue to test the effectiveness of governments across the world in adopting containment and management strategies (11). Beyond the public health perspective, the national responses can thus offer insight into how top-down leadership (e.g., politicians, political appointees, or senior-level management) can directly influence the effectiveness of public administration responses. Although country cases and small-scale comparisons between a few countries have been published (12, 13), much of the literature published to date has focused on individual country-based studies, or small-scale studies involving a few selected countries, as mentioned above.
This current state of the literature could be attributed to the recency of the COVID-19 outbreak, as well as the continually evolving responses as countries grappled with unprecedented demand on their processes and problem-solving capabilities. Hence, this article's contribution to the current literature offers a systematic review of the government responses to COVID-19 management across countries. In addition, the value of systematic research has been noted as it provides reproducible, transparent, and standardized techniques to identify pertinent studies (14, 15).
The systematic review in this article focuses on scholarly publications analyzing leadership roles in PSI within Asia specifically. The two factors underpinning this rationale are the geographical point of origin of COVID-19 and the region's relative level of preparedness. Firstly, as Asia was the origin of the outbreak, the first transmissions within and beyond national borders were recorded in Asia (16). As such, Asian nations were among the first to have their governance and administrative capacity tested. Taiwan and Hong Kong, for example, were the first to send fact-finding missions to Wuhan in China to understand the potential public health risk. Not surprisingly, the first confirmed transmissions beyond China's borders were recorded in Asian countries, namely Thailand and Japan (17).
Therefore, it stands to reason that Asian governments were among the first nations to design, adopt, or refine their administrations' responses to address the early outbreak. Secondly, while all countries had to grapple with the unprecedented scale and nature of the COVID-19 epidemic, those in Asia had some prior experience in dealing with a broadly similar outbreak about 18 years earlier, during the SARS outbreak in 2003 (18). At that time, countries outside Asia had limited or no exposure and minimal cases. However, Asian countries, especially those in East Asia, had a higher degree of exposure, both in the number of cases and deaths. As such, the governments in Asia had put in place more processes in readiness for a potential new outbreak in the future. A systematic review of the studies on Asian governments' responses in harnessing PSI through leadership would thus be able to deepen the current understanding of how leadership can drive adequate PSI in managing this COVID-19 challenge.
Traditional approaches to the typology of leadership as a source of innovation within an organization present two broad types: bottom-up vs. top-down innovations (9). Bottom-up innovations typically arise from employees or work units at lower rungs of public sector organizations as they seek to improve aspects of their work processes. By contrast, top-down innovations are driven by politicians, political appointees, or senior-level management. In addition, they are “often associated with changes of government, new mandates or large-scale initiatives, and can involve a combination of new policy goals and frameworks that are sometimes associated with contemporary ideologies, as well as new concepts of services and service delivery” (p. 794) (19). The context always matters for the effects of leadership on PSI (9, 19, 20).
In the case of COVID-19, the nature and scale of the crisis mean that top-down leadership to drive innovation appears imperative. Both leadership and innovation are urgently required public sector-wide, within a short span of time. However, in a VUCA world (Volatile, Uncertain, Complex, Ambiguous) (20), the binary opposites of top-down vs. bottom-up leadership to drive innovation may be less applicable. Instead, the concept of horizontal leadership has been proposed (21) as a more appropriate response to innovation and problem-solving. Ansell et al. suggest that when dealing with such turbulent problems (i.e., VUCA problems) as the COVID-19 crisis, leaders need to drive “horizontal collaboration between professional groups and sectors, allowing the situation or task to set the team” (21) and lead people for whom there is “no formal leadership responsibility” [ibid]. Beyond seeking expert advice, leaders driving innovation to deal with VUCA problems will have to “accept cognitive dissonance and imperfect solutions, build alliances, learn from experience, adapt to new circumstances, and look for next practice” instead of seeking a “non-existing best practice” (pp. 955–956) (21).
The systematic review and the meta-analysis illustrates the feasible relationships among PSI and leadership in COVID-19 management. To affirm these relationships, published literature has been reviewed to get the potential answers to the following questions:
R.Q. 1: Was PSI adopted to manage COVID-19 in Asian countries?
R.Q. 2: Did leadership have an impact on nations' COVID-19 management strategies and approaches? If so, how?
The influence of leadership on the COVID-19 management was identified in Asian countries' policy responses from published articles in business forums (22). The findings from these articles and published literature have led to the presumption that PSI has been adopted in some Asian countries to mitigate the adverse effects of COVID-19.
A systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) standard (23). We conducted electronic searches on Embase, Web of Science, Medline (via PubMed) database records from the date of inception to 31st May 2021. A repetitive and exhaustive combination of the “Emtree Headings” were used at Embase database, Web of Science database, and PubMed database with MeSH headings. An additional search for scholarly articles in Google Scholar and selective search to Public administration journals via Wiley Online Library, SAGE journals, and Emerald publishing journals were performed to authenticate the primary search.
A repetitive and exhaustive combination of the following “Emtree Headings” were used at Embase database: “public health service” /exp AND (“coronavirus disease 2019” /exp OR “2019 novel coronavirus disease” OR “2019 novel coronavirus epidemic” OR “2019 novel coronavirus infection” OR “2019-ncov disease” OR “2019-ncov infection” OR “covid' OR “covid 19” OR “covid 19 induced pneumonia” OR “covid 2019” OR “covid-10” OR “covid-19” OR “covid-19 induced pneumonia” OR “covid-19 pneumonia” OR “covid19” OR “sars coronavirus 2 infection” OR “sars coronavirus 2 pneumonia” OR “sars-cov-2 disease” OR “sars-cov-2 infection” OR “sars-cov-2 pneumonia” OR “sars-cov2 disease” OR “sars-cov2 infection” OR “sarscov2 disease” OR “sarscov2 infection” OR “wuhan coronavirus disease” OR “wuhan coronavirus infection” OR “coronavirus disease 2” OR “coronavirus disease 2010” OR “coronavirus disease 2019” OR “coronavirus disease 2019 pneumonia” OR “coronavirus disease-19” OR “coronavirus infection 2019” OR “ncov 2019 disease” OR “ncov 2019 infection” OR “new coronavirus pneumonia” OR “novel coronavirus 2019 disease” OR “novel coronavirus 2019 infection” OR “novel coronavirus disease 2019” OR “novel coronavirus infected pneumonia” OR “novel coronavirus infection 2019” OR “novel coronavirus pneumonia” OR “paucisymptomatic coronavirus disease 2019” OR “severe acute respiratory syndrome 2” OR “severe acute respiratory syndrome 2 pneumonia” OR “severe acute respiratory syndrome cov-2 infection” OR “severe acute respiratory syndrome coronavirus 2 infection” OR “severe acute respiratory syndrome coronavirus 2019 infection”).
The Web of science database searched for “COVID” AND “Leadership” in public service with all linked databased namely Web of science core collection, BIOSIS previewes, Current contents connects, KCI-Korean Journal database, Russian science citation index, SciELO citation index and Zoological records. On the PubMed database, a repetitive and exhaustive combination of the following “Medical Subject Headings” (MeSH) search terms were used: (“Leadership”[Majr]) AND (“COVID-19”[Mesh] AND “SARS-CoV-2”[Mesh]). Additional search for scholarly articles in Google Scholar and selective search to Public administration journals via Wiley Online library, SAGE journals and Emerald publishing journals were performed to authenticate the primary search.
The unit of analysis in this study is at the country or national government level. We have included the published articles mentioning the government's role in COVID-19 pandemic management only if published in English. The role of leadership was a subject to ascertain via “topic,” “title,” and “abstract” review during the enrolment process. The inclusion criteria included the reviews of COVID-19 management and were restricted to Asian countries and regions. As Asia was the center of this disaster's first-situation-report, it is rational to investigate the Asian countries' responses to mitigate/control the large-scale effects. Additionally, multiple articles from the same country or a province of a country have been excluded as they would not reflect different leadership roles in the same population and may produce “synergistic inclusion” bias, and may lead to a “confounding” effect. National policy statements/papers were also excluded as they depict large-scale management plans of the particular country and remain beyond the scope of judgment due to a lack of comparative outcome analysis. It is also not unexpected to have government expressions of hopeful aspirations in the policy statement that may not be materialized in reality and which we believe in many cases were superseded anyway by the uncontrollable COVID-19 destructive effects.
Similarly, policy reports published by different government authorities were excluded for two reasons; firstly, these reports contain many domains beyond the scope of analysis of this review. Secondly, not all countries have published their COVID-19 policy reports, and they may have reflected the government achievements only. The smaller-scale case comparisons, especially between two nations or a few, remain out of the inclusion in this article, as these papers have already described a comparison. Hence they may induce directive business and have a confounding effect if added. However, we took the opportunity to review those papers and have cited them in this article whenever relevant. Media reports, critic papers, opinions, and reviews published in “online domains” were excluded from this manuscript as the validity and authenticity of the data could not be ascertained. Furthermore, for studies published from the same country or region, only those with more recent data were included. “Innovation” in this domain was not an active search criterion set by the authors, rather a fruitful concomitant outcome. We have included all public sector innovations implemented for COVID-19 management from an Asian perspective.
The extracted citations were screened and assessed by the authors using reference manager software EndNote X9 independently for inclusion. The articles were first screened by their titles and abstracts, where criteria were purposely broad to include all relevant studies. Second stage review for studies that have made it through the first stage, or cases where a decision cannot be made, full-text reviews were performed on articles to confirm the relevance. To ascertain the conformity of the included studies, expert opinion was sought from one university in Asia. The final inclusion was guided, and an additional search was made to improve the sensitivity, where we have used citation chasing in Google Scholar and public administration publishing houses (via online). Further data was sought by manual search using the backward snowballing method.
All the included studies were observational studies, with the majority reporting the leadership role of the respective countries in managing the COVID-19 disaster. As illustrated in chapter 11 of the Cochrane handbook of reviews (24), GRADEpro was used to evaluate the quality of evidence in the included studies (Table 1). In addition, all included studies were assessed for the specific outcome relating to the leadership role in COVID-19 management, namely, availability of an effective public sector administration of the country, formation of a national committee, crisis denial at early stage, digital surveillance, public sector innovation (PSI), community awareness level and role of scientific/physician's recommendation for disaster management.
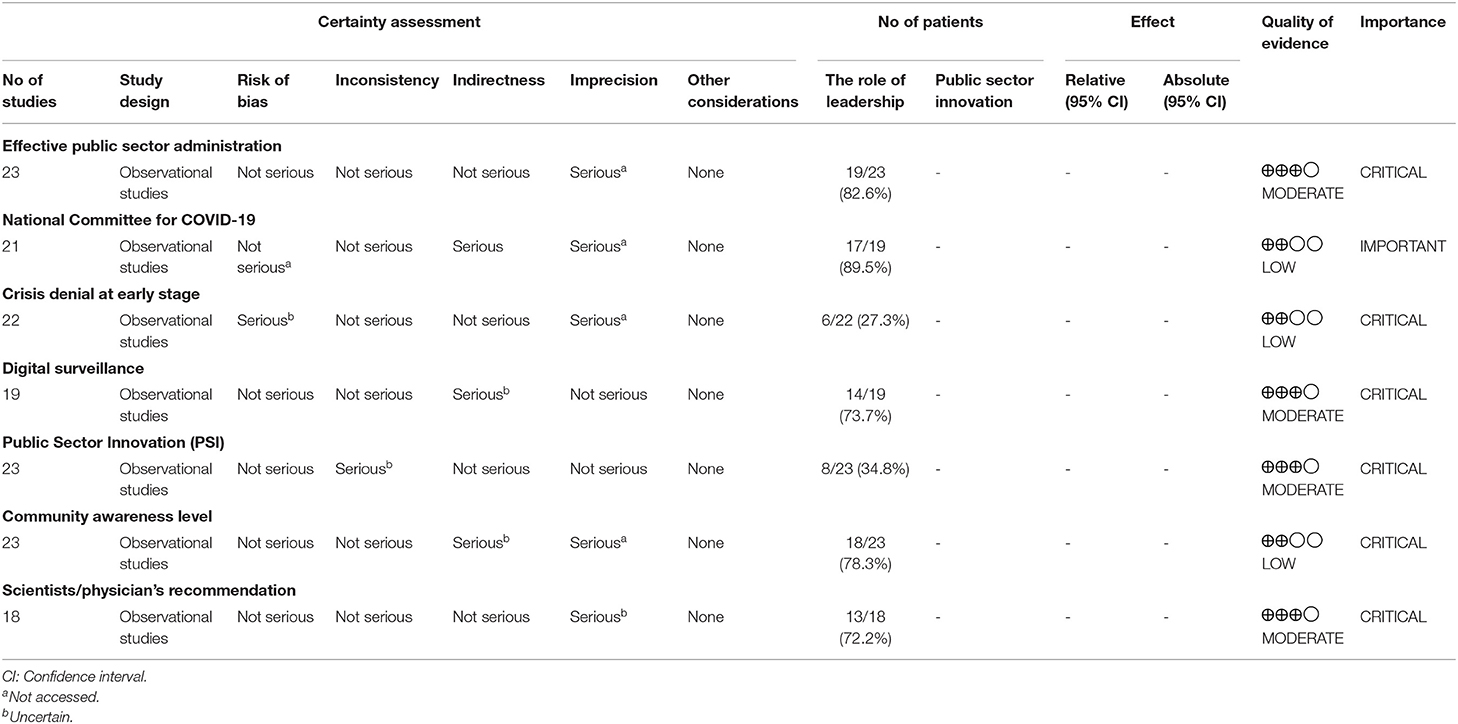
Table 1. Assessment of the quality of the included evidence.
Authors abstracted details of the study characteristics, article information, essential policy information, leadership role assessment, and outcome and impact of COVID-19. Additionally, PSI in different countries was ascertained with their impact in diagnosing confirmed COVID-19 cases, number of death due to COVID-19, and vaccinated population till date were measured. Finally, the forest plots were generated utilizing the Review Manager 5 software (RevMan 5.4) (25).
Depending on the nature of the outcomes extracted from the journals, they were categorized either under dichotomous or continuous data type to generate effect measures in the form of risk ratio (RR) and mean difference (MD), respectively. The effect measures were calculated using the inverse variance method. The data were pooled into either a “random effects” or “fixed effects” model based on the I2 value. When there was high heterogeneity (I2 > 75%), a random effect model was utilized to account for statistical variability across studies.
Our systematic search revealed a total of 2,671 articles in the initial search. Two papers were retrieved from alternative sources after re-review. With duplicates removal, 1,335 articles remained for review. Based on title and abstract scrutiny, irrelevant publications that did not satisfy our inclusion criteria were not considered, leaving 151 articles for full-text review. Following the full-text assessment of these articles, 23 manuscripts remained for final review (Figure 1). Eight PSI have been identified within the included series (Table 2).
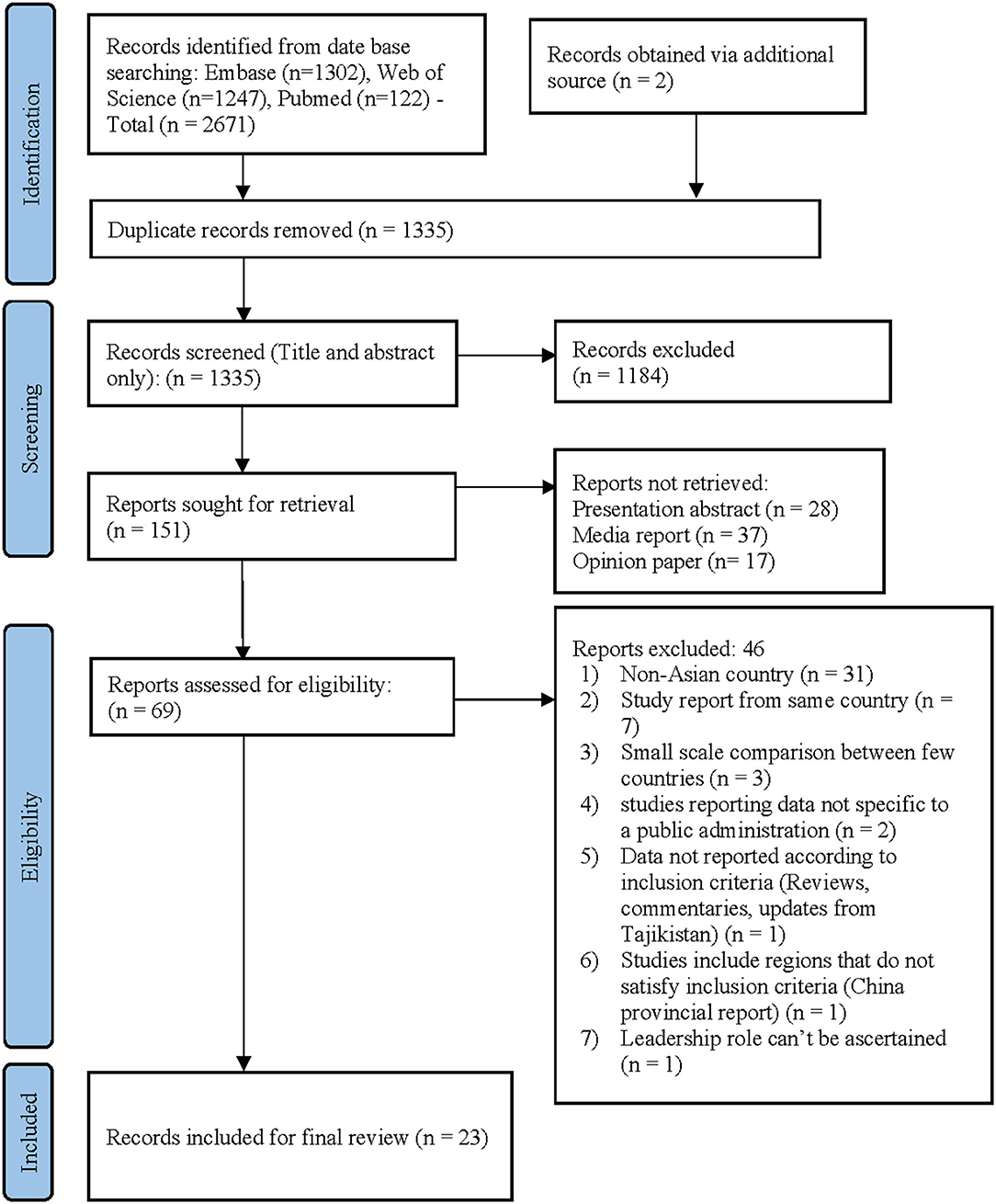
Figure 1. PRISMA Flow diagram. PRISMA chart illustrating our process of obtaining the 23 included articles.
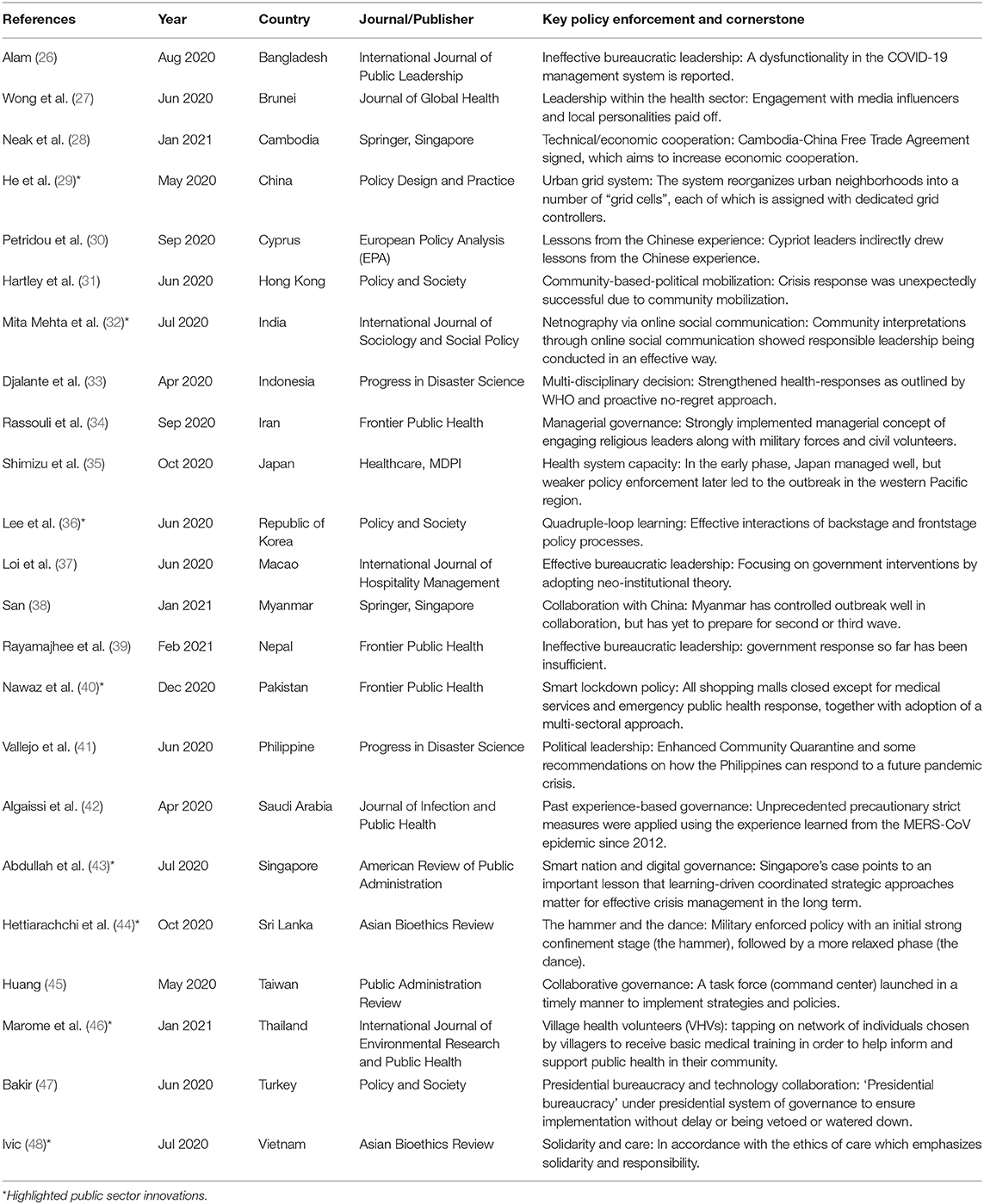
Table 2. Characteristics of the included studies with key policy enforcement and cornerstones of COVID-19 management.
The authors assessed all the included text for their risk of bias and quality of evidence by using RevMan 5.4. The risk of bias of each study was evaluated according to guidelines in chapter 8 of the Cochrane handbook of reviews (49). The overall risk of bias has been assessed for all articles, but keeping the PSI within the primary focus of the RoB has been summarized in Figure 2. As seen from Table 1 and Figure 2, the selection bias for each study was critical/substantial, which we believe can be credited to the type of study itself, the majority being observational studies and case studies describing one particular country or region. Despite this, the overall risk of bias for all the studies was classed as low/moderate. Therefore, the evidence provided by these studies was still of acceptable quality.
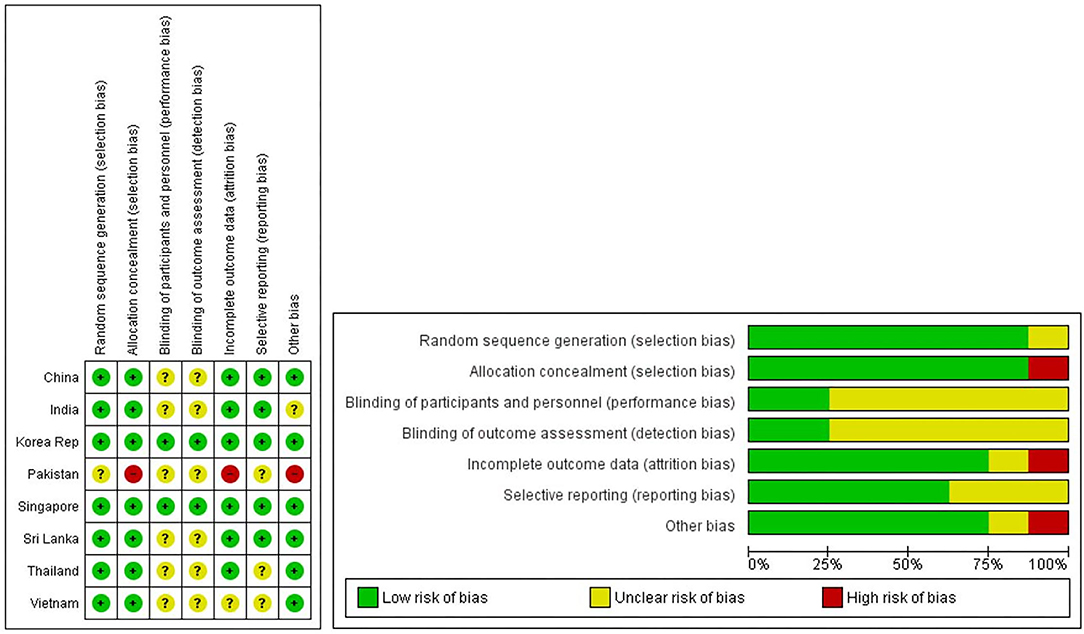
Figure 2. Risk of bias graphs for selected studies with PSI. This figure shows review of authors' judgements about each risk of bias item presented as percentages across all included studies. Random sequence generation were marked high due to selection bias.
Twenty-three eligible articles (26–48) were included for final review on 31st May 2021, summarized in Table 2. As discussed earlier, all the included articles were observational studies of COVID-19 management strategies adopted by the respective governments of Asian countries. The PRISMA statement flowchart shown in Figure 1 highlights the aforementioned screening process. PRISMA chart illustrates our process of obtaining the 23 included articles. With 1,184 irrelevant records excluded based on their titles and abstracts, we reviewed the full texts of 69 articles, of which 46 were excluded, and finally, 23 articles remained for inclusion in our study. Additionally, among the included articles we identified eight papers (29, 32, 36, 40, 43, 44, 46, 48) stated “innovation” to the public sector for this disaster management.
Asian countries are vastly diverse, both in terms of geographic distribution and population size. Despite having many dissimilarities, the COVID-19 pandemic has placed unforeseen demands on the leaders of all these nations. The potential impact of COVID-19 also has tremendous implications based on the population size. As per global population data from the 2019 Revision of World Population Prospects of U.N. shows the largest population is in China (~1.38 B) with India (~1.36 B), Indonesia (~270 M), and Bangladesh (~162 M) in top ten. Hence, the impact of having a strong and effective public administration is very much warranted. Our review shows 82.6% of the included countries had an effective public administration (Table 1) with a few exceptions, namely Bangladesh (26) and Nepal (39), which were not effective; Hong Kong (31) was relatively slow; Pakistan (40) and Saudi Arabia (42) was not known from the reports.
89.1% of the included countries had formed a national committee dedicated to COVID-19 management with multiple government authorities was directly in charge. The exceptions were India (32) and Turkey (47), where the Prime Minister and President of the respective governments were directly involved. Interestingly, there was an initial crisis denial among some countries such as Indonesia (33). The report suggests that the Indonesian government was misled by the initial “nil” incidence reported by the absence of scientific validation, after which once noticed, mitigating efforts were made through by an early presidential decree. Most of the countries reported early effective border control, Home Quarantine, or Isolation of any form. However, people did not adhere to the non-strict lockdown in Bangladesh (26), and the government was slow and reactive in the case of Hong Kong (31). Conversely, Thailand (46) was criticized by the people for an extended lockdown despite having nil community cases.
The case of Singapore (43) showed a success story by tapping on pre-existing infrastructure of “digital governance” to implement new measures such as contact tracing; in contrast, some other countries did not implement contact tracing. At the same time, non-compliance with government directives seemed to be an influential factor and has been reflected in some communities in both positive and negative ways. For example, Hong Kong (31) responded with a community-based political mobilization, while the government was reported to have a sluggish initial response. The overall effect in Asian countries is summarized in Table 3.
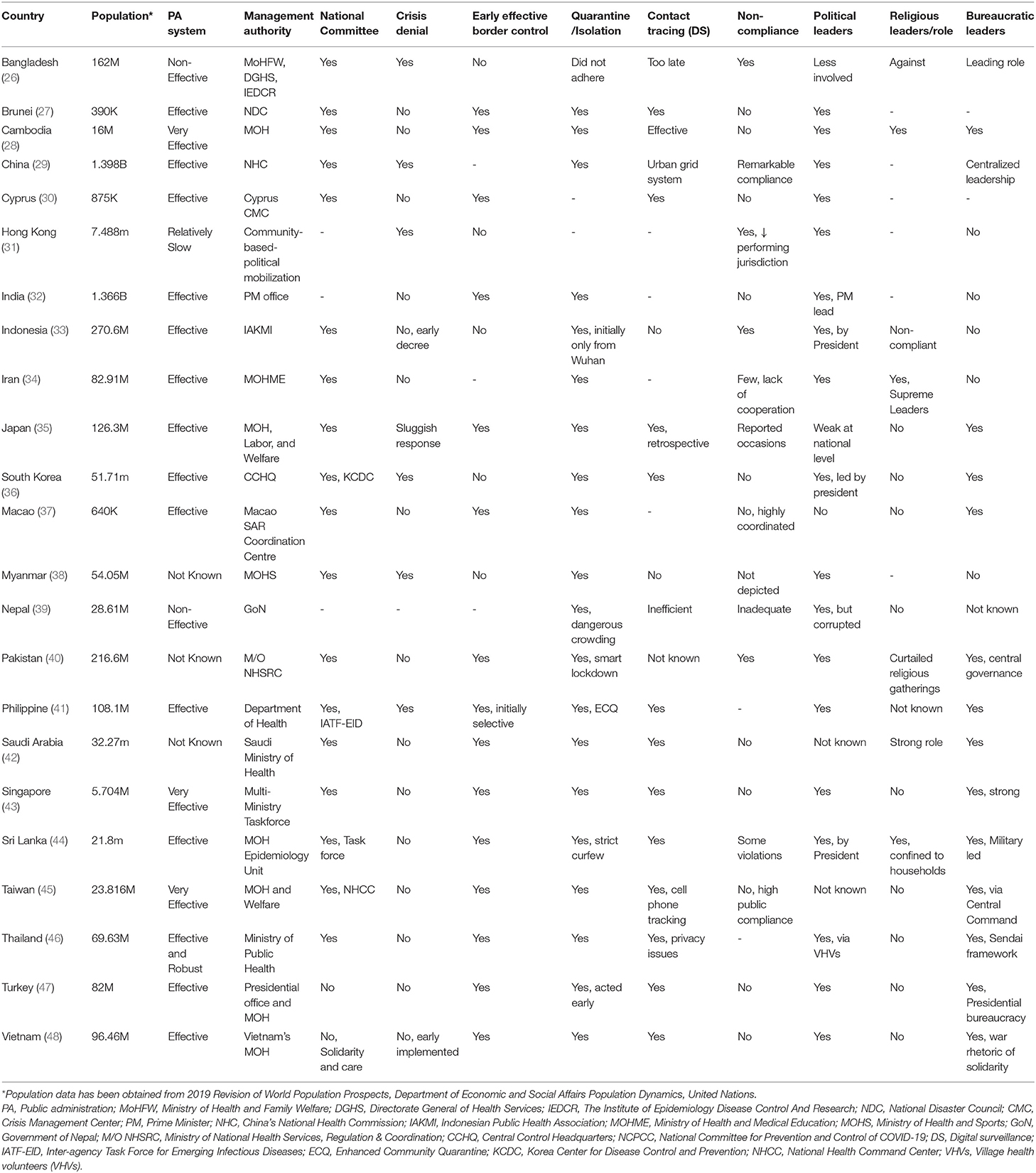
Table 3. Asian countries' responses in COVID-19 management reflecting the role of leadership.
Data abstracted from WHO's COVID-19 response are summarized in Figure 3 (50), showing the number of confirmed cases and the number of deaths due to COVID-19 as reported by the respective countries. In addition, a meta-analysis of the outcome was carried out using RevMan 5.4 software to assess the overall effect in selected countries with PSI (29, 32, 36, 40, 43, 44, 46, 48).
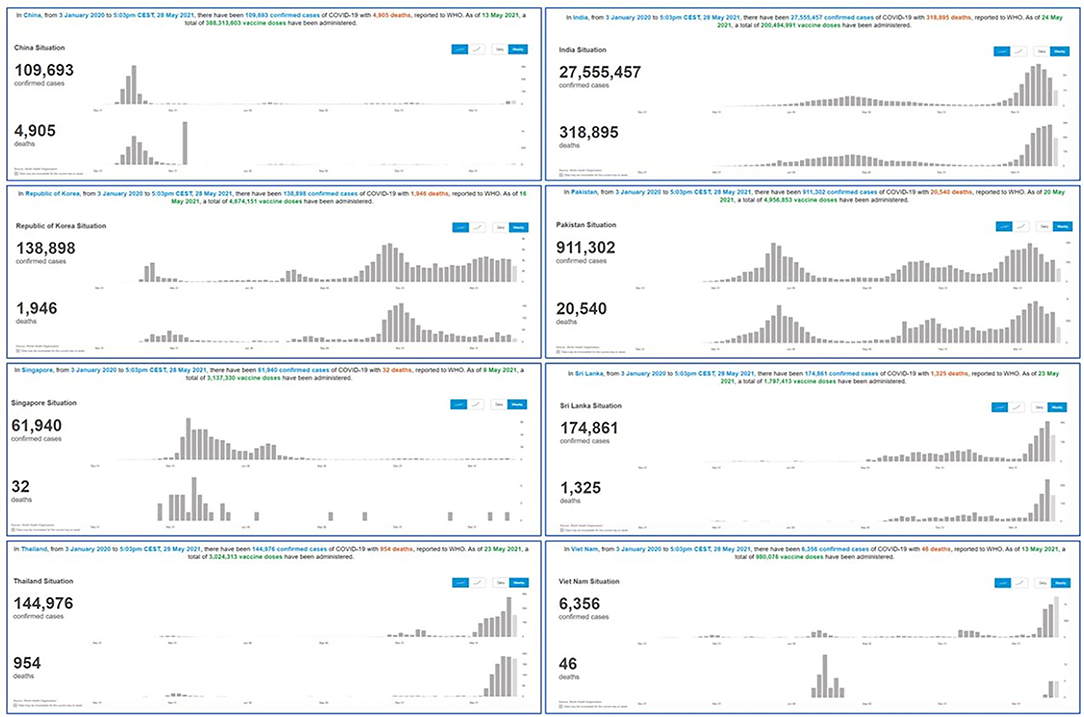
Figure 3. Summary of COVID-19 outcomes in PSI implemented Asian countries. WHO's dashboard of COVID-19 (50) related outcomes from January 2020 till 31st May 2021 reflecting the total number of confirmed COVID-19 cases and total number of death due to COVID-19 is Asian countries (China, India, Republic of Korea, Pakistan, Singapore, Srilanka, Thailand and Vietnam). The histogram showing the changes of outcome over the period of estimate.
The weighted mean comparison in the Cochran-Mantel-Haenszel model in random sequence generation showed that the total number of deaths in PSI implemented countries was still significantly higher when compared with a total number of confirmed COVID-19 cases (Figure 4A). However, the statistical heterogeneity of the data across countries was high. Therefore, the results of this outcome need to be interpreted with caution, with further exploration of the exact cause of heterogeneity.
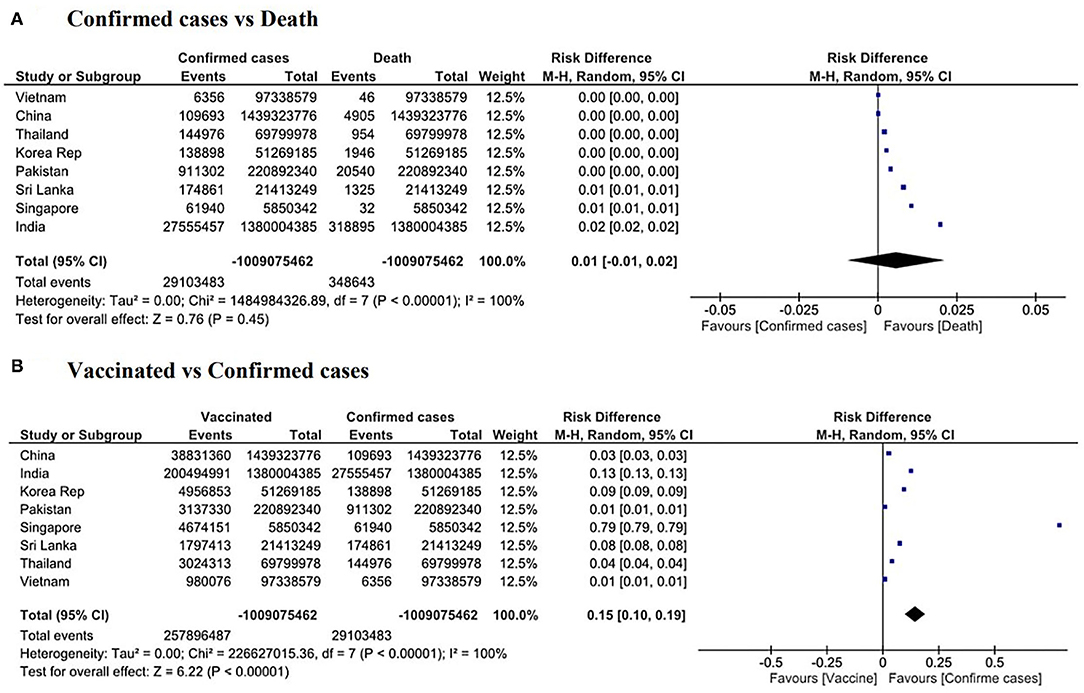
Figure 4. Meta-analysis of COVID-19 outcome in PSI implemented countries. Forest plots showing (A) Total confirmed cases vs. total number of death due to COVID-19. There is significant overall higher death in this cohort, (B) Overall significant number of confirmed cases when compared to vaccinated population in PSI implemented Asian countries.
Forest plot for vaccinated population compared with the total number of confirmed cases in the PSI implemented Asian countries also suggests the overall weighted mean is not in favor of the vaccination program in these countries (Figure 4B). As heterogeneity is persistent, and the I2 index is significantly higher, these results may be due to multifactorial data variation, and two or more subgroups of studies can also cause this high heterogeneity to have a different actual effect.
The study of the eight countries with leadership in PSI being cited revealed a range of different types of innovations (Table 2). The strategic response was categorized as a PSI as long as the innovation was new to the organization or country (4, 5, 19). Hence, for example, contact tracing apps could be considered an innovation in Thailand because this is a novel approach, which was then used to leverage its existing network of Village Health Volunteers (VHVs). Similarly, the approach adopted in Vietnam of tackling the pandemic using the language of war and emphasizing the patriotic duty of citizens to adhere to the strict lockdown was a novel strategy while at the same time leveraging the country's experience of collaboration and solidarity in the face of war.
Undoubtedly, this global pandemic is hard to control, and even though many measures have been taken, overall success is yet to be achieved. However, the leadership of some countries made little effort at the initial stage of the COVID-19 outbreak, whether by downplaying the severity of the pandemic, disregarding the importance of having a national committee, or by not having early effective border control or other safety measures. Eight Asian countries had adopted PSI to combat the global pandemic, namely China (29), India (32), Republic of Korea (36), Pakistan (40), Singapore (43), Srilanka (44), Thailand (46), and Vietnam (48). All these countries' political leaders were directly involved in the decision-making process. While the overall outcome in terms of cases and deaths is not yet satisfactory as the outbreak is still ongoing and evolving, interestingly, citizens' response varies, based on the leadership's response in managing the crisis.
Among the included countries, it could be observed that the countries that exercised only political leadership (32, 33) or weak political leadership, faced greater challenges in managing their respective outbreaks. India, for example, adopted a strong transformational leadership style, whereby the leadership aims to inspire a shared vision resulting in innovative and intrinsically motivated followers or subordinates (21). In India's case, the Prime Minister personally led all major communications and came to be seen as the face of the administration's efforts. However, the weak technocratic infrastructure and excessive bureaucratic obstacles in implementing swift measures stymied India's initial progress. Elsewhere, countries like Bangladesh (26) and Japan (35) faced challenges in adopting practical measures in the face of absent, weak, or belated political leadership.
Bureaucratic leadership appeared to have some early success in managing the outbreak. For example, the presidential bureaucracy in Turkey (47) was a known factor behind the country's early pandemic control (47), while a military-led bureaucratic enforcement in Sri Lanka (44) also led to initial success. Both countries, however, suffered a later loss of control over the pandemic. In contrast, countries such as China (29), the Republic of Korea (36), and Singapore (43), where the political leadership was combined with strong technocracy or bureaucracy, saw more significant and sustained success in controlling their outbreaks. Such countries were able to combine a strong political leadership presence with a highly technocratic style and leverage a highly-skilled bureaucracy in the public sector to implement the evolving strategies. To varying degrees, horizontal leadership can be seen at play, in Singapore and the Republic of Korea, with strong collaboration between expert groups and the public sector and allowing the problem or task to define the team. For example, in the Republic of Korea, some of the most innovative responses (such as drive-through testing centers) arose from input or feedback from expert groups or citizens, ultimately allowing the country to be one of the few that have successfully managed their outbreak without imposing national lockdowns.
At the time of writing, the leadership of countries such as Singapore (43) and Vietnam (48) were able to win the confidence of their citizens. In contrast, Indian leaders were blamed for the last surge of the pandemic (51), as they engaged in packed outdoor rallies for election campaigns and allowed religious festivals to be held with millions of attendees (51). It is evident that consistent and sustained messaging by the leadership regarding pandemic management strategies plays a key role in sustaining public confidence. In India's case, the challenges of implementing management strategies are made more complex by several factors. Firstly, the immense and diverse population places constraints on implementation and consistency of approach across all states. In contrast, countries like Singapore and the Republic of Korea are better able to maintain a consistent approach with their relatively smaller population sizes (about 6 million in Singapore and 51 million in the Republic of Korea). Secondly, there is a relatively lower level of public trust in the quality of governance in India, when compared to countries like Singapore and the Republic of Korea. These three countries' relative performance has been reflected in the annual Worldwide Governance Indicators issued by the World Bank (52). Lower levels of public trust in governance can undermine efforts to manage novel or unprecedented situations such as the COVID-19 pandemic.
In terms of religious leadership, the religious leaders from Iran, Saudi Arabia, and Sri Lanka (34, 42, 44) supported the COVID-19 regulations adopted by their respective governments. Saudi Arabia (42) deferred the Haj pilgrimage and set other historical exceptions, while Sri Lankan religious leaders endorsed the government's household confinement measures (44). In contrast, where the spiritual leadership was at odds with the administration (as in Indonesia), the mixed messaging and contradictory signals compounded the government's challenges in managing the outbreak. Elsewhere, the religious leaders in Bangladesh were against the COVID-19 measures (26), and the Pakistan government allowed religious gatherings (40), both of which seemed detrimental for managing the outbreak.
Overall, it can be seen that leadership styles can influence the level of innovation adopted and the success or failure of the strategic response. More research in this area, particularly on religious leadership as a source of innovation, could be helpful. Although many existing studies analyzed the impact of various sources of innovation, such as politicians, senior executives, supervisors, employees, citizens, industry stakeholders, or universities (7–9, 53, 54), it is not known how religious leadership functions as a source of innovation and how spiritual leadership impacts different organizational (e.g., performance) and national outcomes (e.g., economic development). Thus, this study provides significant contributions to the literature on leadership and PSI while demonstrating that top-down leadership is common and effective and religious leaders can also affect policy implementation and success at the national level.
A number of Asian countries were found to have adopted and implemented PSI for COVID-19 management. In China, the urban grid system (29) reflects a command structure of bureaucratic mobilization. Many aspects of crisis governance are unique and found have embedded in Chinese socio-economic culture. The netnographic study of the Indian community evaluated the prime minister's leadership and the “Janata curfew” (a form of social confinement), showing that the leadership had “relational intelligence” as they aimed to echo a similar style and voice to have a better control via the central command (32). However, after some initial success, the central leadership reported the control measures as “badly-mishandled” (51).
The quadruple-loop learning model was used to explain how the Korean government could effectively tame COVID-19 in the initial stage (36). The study concluded that the Korean government successfully responded to the COVID-19 crisis based on organizational learning theory, despite the fact that the clinical outcomes were non-resonating at the later stage of the pandemic. Interestingly, Pakistan adopted a “Smart lockdown” policy to mitigate the COVID-19 spread (50), but were never been able to bring down the number of confirmed cases and deaths. The policy's failings were rooted in poor socio-economic considerations, and government effort ultimately appeared to be ineffective (55). Nevertheless, Pakistan managed to take practical steps in the vaccination program and develop a native solution, “Pak-Vac,” with the help of China (56).
Elsewhere, multiple global authorities have lauded Singapore's success story, and the government's management strategies have been described in many publications (57). The government, having a bureaucratic culture, coordinated strategic approaches tapping on the earlier groundwork of building a smart nation with adopted policy (43). Meanwhile, in Sri Lanka, the Hammer and the Dance policy was initially enforced strictly by the military and police, leading to early and initial success; later, however, the “Dance” phase appeared to be mismatched (44), leading to rising cases. Village health volunteers (VHVs) in Thailand (46) and Solidary & Care plan by Vietnam (48) showed a similar pattern.
In most countries studied, it would appear that the initial success rate in terms of COVID-19 related confirmed cases, deaths, and vaccinations could not be sustained at the point of writing. The differentiation between countries whose leaders that adopted PSI-based measures, and those adopting non-PSI measures was also not always clear. For example, based on the percentage population that had vaccinations administered, countries with leadership in PSI registered between 0.1% (Vietnam) to 1.5% (Pakistan), 3.4% (Sri Lanka), 7.5% (Republic of Korea), and 34.9% (Singapore). Conversely, among countries where the studies did not cite leadership in PSI, vaccination rates ranged from 16.6% (Hong Kong) to 6.4% (Japan) and 2.3% (Myanmar). Similarly, the number of confirmed cases vs. deaths also presents inconclusive data between countries citing leadership in PSI and those that did not. For example, India, which maintained somewhat low numbers relative to population size for about 1 year, experienced escalated numbers of both categories from March 2021. Singapore too, which initially had low figures, entered an escalated phase a few months into 2020.
The relationship between leadership as a source of innovation in the public sector and the rates of deaths and vaccinations in this study is therefore inconclusive. Hence, while the answer to RQ1 may be partially affirmative, as 34.8% of the included countries adopted leadership in PSI (Table 1), the answer to RQ2 is not conclusive. Accordingly, the beneficial effects of PSI, and leadership in PSI, respectively, to manage the COVID-19 outbreak cannot be answered definitively. The reasons for this are manifold: most importantly, the ongoing nature of the COVID-19 outbreak makes it more challenging to pinpoint the most effective management strategies when management responses and trend data in the countries are continually evolving (58). Future systematic review after the outbreak stabilizes could shed further light on the overall impact of leadership in PSI to manage the response. Secondly, as a complex multifactorial crisis, it is challenging to identify a direct causal relationship between a few specific variables, such as the effects of leadership in PSI and the rates of confirmed cases vs. deaths and vaccinations.
Finally, the challenges that government leaders and public sector managers have faced during COVID-19 are enormous and complex. Both government leaders and the public sector continue to address problems mainly related to human resources management. For example, managers can create the conditions for employees to work in a safe and healthy environment while assessing who can work remotely. In other words, managers need to identify essential tasks, such as whether employees have to come to the job. In addition, organizations need to be more flexible and encourage work from home to those employees who are most at risk such as who have prior medical conditions and who are elderly. While doing so, workspaces can be redesigned to make sure that there are physical distances across employees and there is sufficient fresh air. Overall, what matters most for organizations is employees' well-being (9, 59–62). Investigating the effects of COVID-19 on organizations and employees, Raghavan et al. (63) find that telework and digital adoptions are two trends in COVID-19. They provide four recommendations to organizations: “improve remote work infrastructure for employees,” “use digital tools to improve communication and workflow within organizations,” “Deploy additional resources at the organizational level for digital transformation,” and “Collaborate with technology firms and academic institutions to enhance the digital skills of employees and overcome the digital divide.” [pp.11–12]. Thus, government leaders and public managers can also implement these recommendations.
Last but not least, the statistical calculation may not reflect the impact of PSI and leadership role in the short term, and long-term impact is yet to be achieved, although it has shown the initiatives taken by the leaders, perspectives of governance, and measures for COVID-19 management. Early recognition of the problem, early effective border control, avoiding crisis denial at the early stage, leveraging existing experience, digital access to information, and ensuring compliance to the government directives are found to have a strong influence in pandemic management.
Firstly, the systematic review is confined to studies published on Asian countries' management of the COVID-19 outbreak. Further research into a systematic review of global reflections on the role of leadership in PSI to manage the epidemic would be helpful. In particular, as the outbreak spread rapidly across Europe and North America, further research in this area would add to the understanding of the role and impact of leadership in PSI adopted to manage the COVID-19 outbreak. Secondly, the findings of this study are preliminary due to the ongoing nature of the epidemic, where management responses and trend data in the countries are still emerging or evolving. A future systematic review after the episode could shed further light on the overall impact of leadership in PSI to manage the response. Thirdly, this study has explicitly focused on the context of the COVID-19 outbreak. An area for further research could include other contexts of turbulent problems to deepen understanding of the impact of leadership in PSI in response to such issues. Another major limitation of the current study is that PSI is not adopted in all Asian countries, limiting adequate statistical calculation. A further comparison of countries that implemented PSI, and countries that did not, could add rational values but was beyond the scope of this manuscript. Finally, the meta-synthesis did not appear significant in terms of COVID-19 management and reflected short-term outcomes. A long-term impact of the leadership role and identified PSI in the respective countries would be a potential subject for future research.
The COVID-19 outbreak is still evolving, and the current review provides a cross-section of the ongoing nature of the pandemic, where management responses and trend data in the countries are still emerging or evolving. Public sector innovation applied by a few Asian countries faced mixed reactions, and overall success is yet to be achieved. Nevertheless, a decisive leadership role, early recognition of the problem, early effective border control, avoiding crisis denial at the early stage, leveraging existing experience, digital access to information, and ensuring compliance to government directives are the cornerstones to successful management of the crisis.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
FS and VR: conceptualization, validation, formal analysis, resources, data curation, and writing—original draft preparation. FS, VR, and MD: methodology. FS: software, visualization, and project administration. VR and MD: writing—review and editing. MD: supervision. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to express special gratitude to Zhu Lin from the Lee Kuan Yew School of Public Policy, NUS.
COVID-19, Corona Virus Disease 2019; PSI, Public Sector Innovation; SARS, Severe Acute Respiratory Syndrome; VUCA, Volatile, Uncertain, Complex, Ambiguous; RQ, Research Question; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses; QOE, Quality of Evidence; RR, Risk Ratio; MD, Mean Difference; ROB, Risk of Bias; UN, United Nations; WHO, World Health Organization; VHV, Village Health Volunteers.
1. Hope MD, Raptis CA, Shah A, Hammer MM, Henry TS. A role for C.T. in COVID-19? What data really tell us so far. Lancet. (2020) 395:1189–90. doi: 10.1016/S0140-6736(20)30728-5
2. Meijer A, Webster CWR. The COVID-19-crisis and the information polity: an overview of responses and discussions in twenty-one countries from six continents. Inf Polity. (2020) 25:243–74. doi: 10.3233/IP-200006
3. Bekkers V, Edelenbos J, Steijn B. Linking Innovation to the Public Sector: Contexts, Concepts and Challenges. In: Bekkers V, Edelenbos J, Steijn B., editors. Innovation in the Public Sector. IIAS Series: Governance and Public Management. London: Palgrave Macmillan (2011). doi: 10.1057/9780230307520
4. Demircioglu MA. The effects of organizational and demographic context for innovation implementation in public organizations. Public Manage Rev. (2020) 22:1852–75. doi: 10.1080/14719037.2019.1668467
5. Vivona R, Demircioglu MA, Raghavan A. (2020). Innovation and Innovativeness for the Public Servant of the Future: What, Why, How, Where, and When. In H. Sullivan & H. Dickinson (Eds.), The Palgrave Handbook of the Public Servant. Switzerland: Springer. doi: 10.1007/978-3-030-03008-7_34-1
6. Chan IYS, Liu AMM, Fellows R. Role of leadership in fostering an innovation climate in construction firms. J Manage Eng. (2014) 30:1–7. doi: 10.1061/(ASCE)ME.1943-5479.0000271
7. Orazi DC, Turrini A, Valotti G. Public sector leadership: new perspectives for research and practice. Int Rev Adm Sci. (2013) 79:486–504. doi: 10.1177/0020852313489945
8. OECD (2017) Fostering Innovation in the Public Sector, OECD Publishing Paris. http://dx.doi.org/10.1787/9789264270879-en doi: 10.1787/9789264270879-en
9. Demircioglu MA. Sources of innovation, autonomy, and employee job satisfaction in public organizations. Public Perform Manage Rev. (2021) 44:155–86. doi: 10.1080/15309576.2020.1820350
10. Lægreid P, Roses PG, Verhoest K. Explaining the innovative culture and activities of state agencies. Organ Stud. (2011) 32:1321–47. doi: 10.1177/0170840611416744
11. Alanezi F, Aljahdali A, Alyousef SM, Alrashed H, Mushcab H, Al-Thani B, et al. Comparative study on the strategies adopted by the United Kingdom, India, China, Italy, and Saudi Arabia to contain the spread of the COVID-19 pandemic. J Healthc Leadersh. (2020) 12:117–31. doi: 10.2147/JHL.S266491
12. Summers DJ, Cheng DHY, Lin PHH, Barnard DLT, Kvalsvig DA, Wilson PN, et al. Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic. Lancet Reg Health West Pac. (2020) 4:100044. doi: 10.1016/j.lanwpc.2020.100044
13. An BY, Tang S-Y. Lessons from COVID-19 responses in East Asia: institutional infrastructure and enduring policy instruments. Am Rev Public Adm. (2020) 50:790–800. doi: 10.1177/0275074020943707
14. Cinar E, Trott P, Simms C. A systematic review of barriers to public sector innovation process. Public Manage Rev. (2019) 21:264–90. doi: 10.1080/14719037.2018.1473477
15. Page MJ, Moher D. Evaluations of the uptake and impact of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement and extensions: a scoping review. Syst Rev. (2017) 6:263. doi: 10.1186/s13643-017-0663-8
16. Mallapaty S. The scientists investigating the pandemic's origins. Nature. (2020) 588:208. doi: 10.1038/d41586-020-03402-1
17. Okada P, Buathong R, Phuygun S, Thanadachakul T, Parnmen S, Wongboot W, et al. Early transmission patterns of coronavirus disease 2019 (COVID-19) in travelers from Wuhan to Thailand, January 2020. Euro Surveill. (2020) 25:2000097. doi: 10.2807/1560-7917.ES.2020.25.8.2000097
18. Capano G, Howlett M, Jarvis DS, Ramesh M, Goyal N. Mobilizing policy (In) capacity to fight COVID-19: understanding variations in state responses. Policy Soc. (2020) 39:285–308. doi: 10.1080/14494035.2020.1787628
19. Arundel A, Bloch C, Ferguson B. Advancing innovation in the public sector: aligning innovation measurement with policy goals. Res Policy. (2019) 48:789–98. doi: 10.1016/j.respol.2018.12.001
20. Demircioglu MA, Van der Wal Z. Leadership and innovation: what's the story? The relationship between leadership support level and innovation target. Public Manage Rev. (2021) 1–23. doi: 10.1080/14719037.2021.1900348
21. Ansell C, Sorenson E, Torfing J. The COVID-19 pandemic as a game changer for public administration and leadership? The need for robust governance responses to turbulent problems. Public Manage Rev. 23:949–60. doi: 10.1080/14719037.2020.1820272
22. Baker JR, Howe CK. Leadership in a Time of Crisis: Asian Businesses Respond to COVID-19. Asian Business Council. September (2020). Available online at: https://asiabusinesscouncil.org/2020/10/28/leadership-in-a-time-of-crisis-asian-businesses-respond-to-covid-19/
23. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9, W64. doi: 10.7326/0003-4819-151-4-200908180-00135
24. Higgins JP, Green S.R. Assessing risk of bias in included studies. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1. 0 (2011). Available online at: https://handbook-5-1.cochrane.org/
25. Review Manager (RevMan) [Computer program]. Version 5.4. Copenhagen: the Nordic Cochrane Centre, The Cochrane Collaboration, (2014). Available online at: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download
26. Alam MA. Leading in the shadows: understanding administrative leadership in the context of COVID-19 pandemic management in Bangladesh. Int J Public Leadersh. (2021) 17:95–107. doi: 10.1108/IJPL-06-2020-0050
27. Wong J, Koh WC, Alikhan MF, Abdul Aziz ABZ, Naing L. Responding to COVID-19 in Brunei Darussalam: lessons for small countries. J Glob Health. (2020) 10:010363. doi: 10.7189/jogh.10.010363
28. Neak C, Sok S. Cambodia's Response to COVID-19 and Its Impacts on Cambodia–China Relations. In: Peng N. (eds) The Reshaping of China-Southeast Asia Relations in Light of the COVID-19 Pandemic. Springer, Singapore. doi: 10.1007/978-981-33-4416-7_4
29. He AJ, Shi Y, Liu H. Crisis governance, Chinese style: distinctive features of China's response to the Covid-19 pandemic. Policy Des Pract. (2020) 3:242–58. doi: 10.1080/25741292.2020.1799911
30. Petridou E, Zahariadis N, Ceccoli S. Averting institutional disasters? Drawing lessons from China to inform the Cypriot response to the COVID-19 pandemic. Eur Policy Anal. (2020). 6:318–27. doi: 10.1002/epa2.1090
31. Hartley K, Darryl S, Jarvis L. Policymaking in a low-trust state: legitimacy, state capacity, and responses to COVID-19 in Hong Kong. Policy Soc. (2020) 39:403–23. doi: 10.1080/14494035.2020.1783791
32. Mehta M, Sarvaiya H, Chandani A. Community engagement through responsible leadership in managing pandemic: insight from India using netnography. Int J Sociol Soc Policy. (2020). doi: 10.1108/IJSSP-06-2020-0214
33. Djalante R, Lassa J, Setiamarga D, Sudjatma A, Indrawan M, Haryanto B, et al. Review and analysis of current responses to COVID-19 in Indonesia: period of January to March 2020. Prog Disaster Sci. (2020) 6:100091. doi: 10.1016/j.pdisas.2020.100091
34. Rassouli M, Ashrafizadeh H, Shirinabadi Farahani A, Akbari ME. COVID-19 management in Iran as one of the most affected countries in the world: advantages and weaknesses. Front Public Health. (2020) 8:510. doi: 10.3389/fpubh.2020.00510
35. Shimizu K, Negrita M. Lessons learned from Japan's response to the first wave of COVID-19: a content analysis. Healthcare. (2020) 8:426. doi: 10.3390/healthcare8040426
36. Lee S, Hwang C, Jae Moon M. Policy learning and crisis policy-making: quadruple-loop learning and COVID-19 responses in South Korea. Policy Soc. (2020) 39:363–81. doi: 10.1080/14494035.2020.1785195
37. Loi KI, Lei WS, Lourenço F. Understanding the reactions of government and gaming concessionaires on COVID-19 through the neo-institutional theory - The case of Macao. Int J Hosp Manag. (2021) 94:102755. doi: 10.1016/j.ijhm.2020.102755
38. San M. Myanmar's Response to COVID-19 and Its Impacts on China–Myanmar Relations. In: Peng N. (eds) The Reshaping of China-Southeast Asia Relations in Light of the COVID-19 Pandemic. Springer, Singapore. doi: 10.1007/978-981-33-4416-7_6
39. Rayamajhee B, Pokhrel A, Syangtan G, Khadka S, Lama B, Rawal LB, et al. How well the government of Nepal is responding to COVID-19? An experience from a resource-limited country to confront unprecedented pandemic. Front Public Health. (2021) 9:597808. doi: 10.3389/fpubh.2021.597808
40. Nawaz A, Su X, Barkat MQ, Asghar S, Asad A, Basit F, et al. Epidemic spread and its management through governance and leadership response influencing the arising challenges around COVID-19 in Pakistan-A lesson learnt for low income countries with limited resource. Front Public Health. (2020) 8:573431. doi: 10.3389/fpubh.2020.573431
41. Vallejo BM, Ong RAC. Policy responses and government science advice for the COVID 19 pandemic in the Philippines: January to April 2020. Prog Disaster Sci. (2020) 7:100115. doi: 10.1016/j.pdisas.2020.100115
42. Algaissi AA, Alharbi NK, Hassanain M, Hashem AM. Preparedness and response to COVID-19 in Saudi Arabia: building on MERS experience. J Infect Public Health. (2020) 13:834–8. doi: 10.1016/j.jiph.2020.04.016
43. Abdullah WJ, Kim S. Singapore's responses to the COVID-19 outbreak: a critical assessment. Am Rev Public Adm. (2020) 50:770–6. doi: 10.1177/0275074020942454
44. Hettiarachchi D, Noordeen N, Gamakaranage C, Somarathne EARBD, Jayasinghe S. Ethical responses to the COVID-19 pandemic-lessons from Sri Lanka. Asian Bioeth Rev. (2020) 13:1–9. doi: 10.1007/s41649-020-00153-z
45. Huang IY. Fighting COVID-19 through government initiatives and collaborative governance: the Taiwan experience. Public Adm Rev. (2020) 80:665–70. doi: 10.1111/puar.13239
46. Marome W, Shaw R. COVID-19 response in Thailand and its implications on future preparedness. Int J Environ Res Public Health. (2021) 18:1089. doi: 10.3390/ijerph18031089
47. Bakir C. The Turkish state's responses to existential COVID-19 crisis. Policy Soc. (2020) 39: 424–41. doi: 10.1080/14494035.2020.1783786
48. Ivic S. Vietnam's response to the COVID-19 outbreak. Asian Bioeth Rev. (2020) 12:1–7. doi: 10.1007/s41649-020-00134-2
49. Sterne JAC, Higgins JPT, Reeves BC. on behalf of the development group for ACROBAT-NRSI. A Cochrane risk of bias assessment tool: for non-randomized studies of interventions (ACROBATNRSI), Version 1.0.0, 24 September (2014). Available online at: http:// http://www.bristol.ac.uk/population-health-sciences/centres/cresyda/barr/riskofbias/robins-i/acrobat-nrsi/ (accessed: Sep 1, 2019)
50. World Health Organisation (WHO) (2020). WHO Timeline: COVID-19. Available online at: https://www.who.int/news/item/29-06-2020-covidtimeline
51. Ganguly S, Chin D, King EJ, Fonseca EM, Mercado SV, Greer SL. World's worst pandemic leaders: 5 presidents and prime ministers who badly mishandled COVID-19. The Conversation. May (2021). Available online at: https://theconversation.com/worlds-worst-pandemic-leaders-5-presidents-and-prime-ministers-who-badly-mishandled-covid-19-159787
52. Daniel K, Kraay A, Mastruzzi M. The Worldwide Governance Indicators: Methodology and Analytical Issues (September 2010). World Bank Policy Research Working Paper No. 5430, Available online at: https://ssrn.com/abstract=1682130
53. Arundel A, Casali L, Hollanders H. How European public sector agencies innovate: The use of bottom-up, policy-dependent and knowledge-scanning innovation methods. Res Policy. (2015) 44:1271–82. doi: 10.1016/j.respol.2015.04.007
54. Demircioglu MA, Audretsch DB. Public sector innovation: the effect of universities. J Technol Transf. (2019) 44:596–614. doi: 10.1007/s10961-017-9636-2
55. Waris A, Atta UK, Ali M, Asmat A, Baset A. COVID-19 outbreak: current scenario of Pakistan. New Microbes New Infect. (2020) 35:100681. doi: 10.1016/j.nmni.2020.100681
56. Sultan F. Pakistan develops home made anti-COVID-19 vaccine 'PakVac' with help of China. The Economic Times. Jan (2021). Available online at: https://economictimes.indiatimes.com/news/international/world-news/pakistan-develops-home-made-anti-covid-19-vaccine-pakvac-with-help-of-china/articleshow/83153406.cms
57. Arfi Bambani Amri. Singapore's strategy to overcome COVID-19 threat. Anadolu Agency, Asia-Pacific. December (2020). Available online at: https://www.aa.com.tr/en/asia-pacific/opinion-singapore-s-strategy-to-overcome-covid-19-threat/2085896
58. Xiao Y, Torok ME. Taking the right measures to control COVID-19. Lancet Infect Dis. (2020) 20:523–4. doi: 10.1016/S1473-3099(20)30152-3
59. Baptiste NR. Tightening the link between employee wellbeing at work and performance: a new dimension for HRM. Manage Decis. (2008) 46:284–309. doi: 10.1108/00251740810854168
60. Grant AM, Christianson MK, Price RH. Happiness, health, or relationships? Managerial practices and employee well-being tradeoffs. Acad Manag Perspect. (2007). 21:51–63. doi: 10.5465/amp.2007.26421238
61. Lahat L, Ofek D. Emotional well-being among public employees: a comparative perspective. Rev Public Pers Adm. (2020). doi: 10.1177/0734371X20939642
62. Oksa R, Saari T, Kaakinen M, Oksanen A. The motivations for and well-being implications of social M61edia use at work among millennials and members of former generations. Int J Environ Res Public Health. (2021) 18:803. doi: 10.3390/ijerph18020803
Keywords: coronavirus, COVID-19, pandemic, leadership, public sector, innovation, policy
Citation: Sazzad F, Rajan VP and Demircioglu MA (2021) The Role of Leadership in Public Sector Innovation: A Systematic Review and Meta-Analysis of the Management of COVID-19 in Asian Countries. Front. Public Health 9:743748. doi: 10.3389/fpubh.2021.743748
Received: 19 July 2021; Accepted: 24 November 2021;
Published: 15 December 2021.
Edited by:
Alexandra P. Leader, Eastern Virginia Medical School, United StatesReviewed by:
Frederick Ato Armah, University of Cape Coast, GhanaCopyright © 2021 Sazzad, Rajan and Demircioglu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Faizus Sazzad, ZTA2Nzc4NjhAdS5udXMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.