 Md. Tanzilul Amin
Md. Tanzilul Amin Mahmud Hasan
Mahmud Hasan N. M. Mahmudul Alam Bhuiya
N. M. Mahmudul Alam Bhuiya
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 29 September 2021
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.738352
This article is part of the Research TopicCOVID-19: Integrating Artificial Intelligence, Data Science, Mathematics, Medicine and Public Health, Epidemiology, Neuroscience, and Biomedical Science in Pandemic ManagementView all 95 articles
Objective: This study aimed to assess the prevalence, onset, and duration of COVID-19 associated symptoms, hospitalization, and recovery time from the infection in Bangladesh.
Methods: A retrospective study was designed adopting the snowball sampling technique (n = 439). The association of gender, age, and comorbidity on COVID-19 associated complications was determined using chi-square and binary logistic regression analysis (p < 0.05).
Result: Fever, exhaustion, cough, loss of taste, sore throat, body ache, and hair-loss were prevalent among more than 50% of the participants and developed within fourth days in above 90% of the patients. Shortness of breath was significantly higher in males (χ2 = 5.671; OR 1.641). Significant comorbidity association on the shortness of breath (χ2 = 40.119; OR 2.564), vomiting (χ2 = 4.422; OR 1.018), and loss of speech (χ2 = 17.299; OR 3.430) was observed. Patients (>40 years) exerted higher association in shortness of breath (χ2 = 24.083; OR 2.901). Age and comorbidity were significantly associated with COVID-19 associated hospitalization (χ2 = 16.890 and χ2 = 23.638, respectively) and recovery time (χ2 = 12.870 and χ2 = 26.924, respectively).
Conclusion: The study suggests that the hospitalization rate increased for older (>40 years) and comorbid patients. Comorbid patients demonstrated higher susceptibility to have shortness of breath, vomiting, loss of speech, and confusion, whereas male patients showed significant increase in the prevalence of sore throat, loss of smell, and vomiting compared to female patients.
In late December 2019, a small number of inexplicable respiratory infections were recorded in Wuhan, Hubei province, China. It has clinical similarities to viral pneumonia and Prevention Research Centers, Centers for Disease Control (CDC) experts determined that pneumonia was caused by a novel β-coronavirus (1, 2). Afterward, WHO relabeled the name of this virus as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) suggested by the Coronavirus Study Group of the International Committee on Taxonomy of Viruses (ICTV), and the disease was termed as coronavirus disease 2019 or simply COVID-19 (3). Although no animal source has been confirmed yet, due to the similarity in genomic features, it is postulated that bat or pangolin may work as a reservoir of SARS-CoV-2 (4). On Mar 11, 2020, WHO stated the COVID-19 outbreak as a global pandemic as reported cases reach 200,000 people, with over 8,000 people died due to the complications related to COVID-19 in over 160 countries (5, 6). The number of confirmed cases increases every day, exerting a wide variety of symptoms in the infected persons. SARS-CoV-2 has now spread to more than 213 countries worldwide.
Coronaviruses are a broad family of viruses that cause respiratory disorders, which diagnosis varies from the common cold to more severe disorders such as Middle East Respiratory Syndrome (MERS), Severe Acute Respiratory Syndrome (SARS), and COVID-19 (7). The symptoms of coronaviruses infections include cough, fever, diarrhea, chest pain, fatigue, body ache, sore throat, rhinorrhea, tachypnea, dyspnea (7, 8). The presence of glycoprotein spikes on the envelope of this RNA virus gives it a classic crown-like look under an electron microscope (9). This group of viruses is zoonotic, meaning they can be transmitted between animals and people (10–12). Coronaviruses are classified into four genera, one of which is α-/β-/γ-/δ-coronavirus. The α- and β-coronaviruses are both capable of infecting mammals, while γ- and δ-coronaviruses are more commonly found in birds (13). Six coronaviruses had long been described as human-susceptible viruses. Among them, α-coronavirus HCoV-229E and HCoV-NL63 bear low pathogenicity, and β-CoVs HCoV-HKU1 and HCoV-OC43 cause moderate respiratory symptoms, identical to a common cold. On the other hand, the other known β-CoVs, SARS-CoV and MERS-CoV could result in a severe and potentially fatal respiratory illness (14, 15). The disease is generally known to be transmitted between animals and humans through sneezing, coughing, touching or shaking hands, and contacting a surface or object and the incubation period ranges from 2 to 14 days (9, 14). The infection has been predicted by a loss of smell and taste in addition to other symptoms (16, 17). The prevalence of gastrointestinal symptoms before fever and difficulty in breathing was also reported in a previous study (18). COVID-19 has caused millions of people to be hospitalized around the world, with symptoms including fever, dry cough, exhaustion, diarrhea, breathing problem, headache, nausea, and vomiting (19). After 60 days, just 13% of people in Italy were completely free of COVID-19 symptoms, with 55% reporting three or more persistent symptoms and 32% reporting one or two residual symptoms (20). Similarly, COVID-19 patients who suffered from chronic symptoms exhibited a lower life expectancy after 2–3 weeks of infection in the United States (21).
COVID-19 associated symptoms and complications may vary from person to person. COVID-19 has a wide range of frequency and severity, which is believed to be influenced by various biological, cultural, and economic factors. Many of those who died had other advanced age, hypertension, diabetes, or cardiovascular disease that impaired their immune systems (14). According to previous clinical investigations, females are less likely to be infected and have lower cytokine production than previous clinical investigations (22). African and Asian races have a higher chance of acquiring COVID-19 than Caucasian people; Asians may also have a higher chance of hospitalization and mortality (23).
In Bangladesh, the first documented incidence was reported on Mar 08, 2020 (24). Infection rates remained low until the end of March, following which a significant surge in infected cases occurred that persisted till June 2020 (25, 26). The number of new COVID-19 infection cases, COVID-19-related deaths, recovery from COVID-19, and the number of Real-Time Reverse Transcription Polymerase Chain Reaction (RT-PCR) tests conducted in Bangladesh is illustrated in Figure 1. There has been very limited information regarding the COVID-19 symptoms and associated consequences among the patient of Bangladesh. In this study, we were focused on assessing the prevalence, onset, and duration of the severity of the symptoms and recovery time in the study participants. We also tried to determine the impact of different factors such as gender, age, and comorbidity on hospitalization, recovery time as well as the prevalence of the COVID-19 associated symptoms.
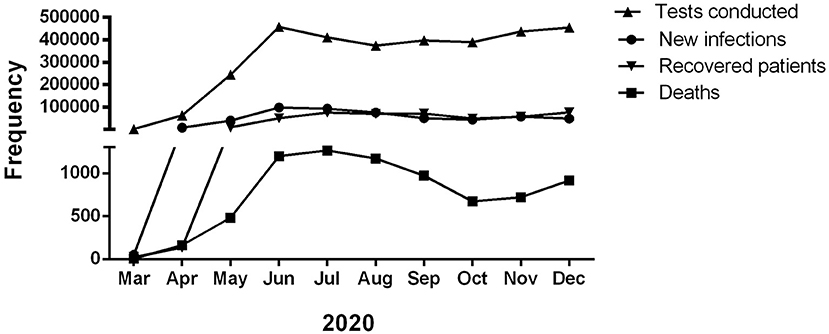
Figure 1. Month-wise total number of COVID-19 patients, death, recovered, and RT-PCR test conducted in Bangladesh in 2020 (Ref: DGHS, Bangladesh).
A cross-sectional study design using “Google Form” was adopted to assess the prevalence of COVID-19-related symptoms among the patients of Bangladesh during the outbreak of COVID-19. Data were collected from Sept 08, 2020, to Nov 08, 2020. At that time, it was not feasible to conduct community-based surveys due to the countrywide lockdown implemented by the government (27, 28). This self-reported retrospective study was conducted using a standardized questionnaire. Only those infected with coronavirus between Mar 08, 2020, and Aug 08, 2020, had their infection verified by RT-PCR test and then recovered from the condition- were included in the study.
The online link was circulated by the Exponential Non-Discriminative snowballing method (29, 30). An online-based advertisement campaign was designed to recruit participants for this online survey who suffered and eventually recovered from COVID-19 (31). Participants residing in Bangladesh were randomly selected, and none of them were related to any study. We covered the people who use social media platforms (e.g., Facebook and LinkedIn) to collect information for this study. People receiving the message were requested to participate in the survey and forward the link to their close contacts infected by this coronavirus. Participants whose age was 18 years old or above were allowed to participate in this study. A total of 453 complete responses were received in this survey who agreed to take part. Of these, six responses were also omitted due to incomplete data. In addition, answers from the participants having COVID-19 like symptoms but not performing the RT-PCR test- were also excluded. Finally, a total of 439 responses were considered for final data analysis.
The survey consisted of 23 questions. Except for two unstructured, open-ended questions, all of the questions were closed-ended. The questionnaire has four domains. The first one collected the demographic details of the participants. The second domain was constructed to contain participants' infection date, RT-PCR test information (to ascertain the infection and recovery from the disease), treatment, hospitalization and recovery time, and other comorbidity histories. The questions of the third and fourth domains were designed to measure the onset and duration of the symptoms, respectively. A set of nineteen symptoms was included in the questionnaire to check the symptoms' prevalence, onset, and duration. In addition, participants were allowed to report any other symptoms that were not mentioned in the questionnaire through an open-ended question. The history of other chronic diseases was also recorded. The questions were constructed in English to understand the scientific terminologies better, whereas a Bengali (most participants' mother tongue) translation was also provided. A forward-backward translation process was followed for the finalization of the questionnaire.
The data from the “Google Form” was initially extracted in.xlsx format. Participants who disagreed with using their information, those who did not complete an RT-PCR test to confirm infection, and incomplete responses were then deleted from this study. After that, the data was converted to.sav format for further statistical analysis. Descriptive statistics (frequency, percentages, and means) were used to examine the participants' responses and demographic distribution. Participants were divided into different groups for further analysis based on gender (male-female), age (aging ≤40 years old and aging >40 years old), and comorbidity (other chronic disease(s)-no other disease(s) during the infection) based on other relevant conditions (32, 33). The Pearson's chi-squared test followed by binary logistic regression analysis was applied to determine the association of different predictors in the prevalence of the symptoms. Statistical significance was defined when p < 0.05. All statistical tests were performed using STATA 12.0 and IBM SPSS 23.0 version.
The current study was carried out following the Helsinki declaration changed in 2014 and the checklist for reporting internet e-surveys (CHERRIES) (34, 35). The study was reviewed and approved by The Jagannath University Research Cell, Dhaka, Bangladesh (File no.- JnURes-001/2020). The objectives, potential benefits, risks, and the confidentiality of given responses were communicated with participants before starting the online survey. Participants also received an option to provide their consent to use their provided information for further analysis in the study.
The final analysis consisted of 439 respondents where 69% (n = 303) were male, and 31% (n = 136) were female (Table 1). The participants' ages ranged from 18 years to above 60 years. About 42% (n = 183) participants aged from 18 to 30 years followed by 31% (n = 135) people aged from 31 to 40 years. Although respondents were from all divisions of Bangladesh, the highest response rate was from Barishal Division (49%, n = 215), whereas the lowest was from the Rangpur division (0.7%, n = 3). The division wise participant information is illustrated in Supplementary Figure 1.
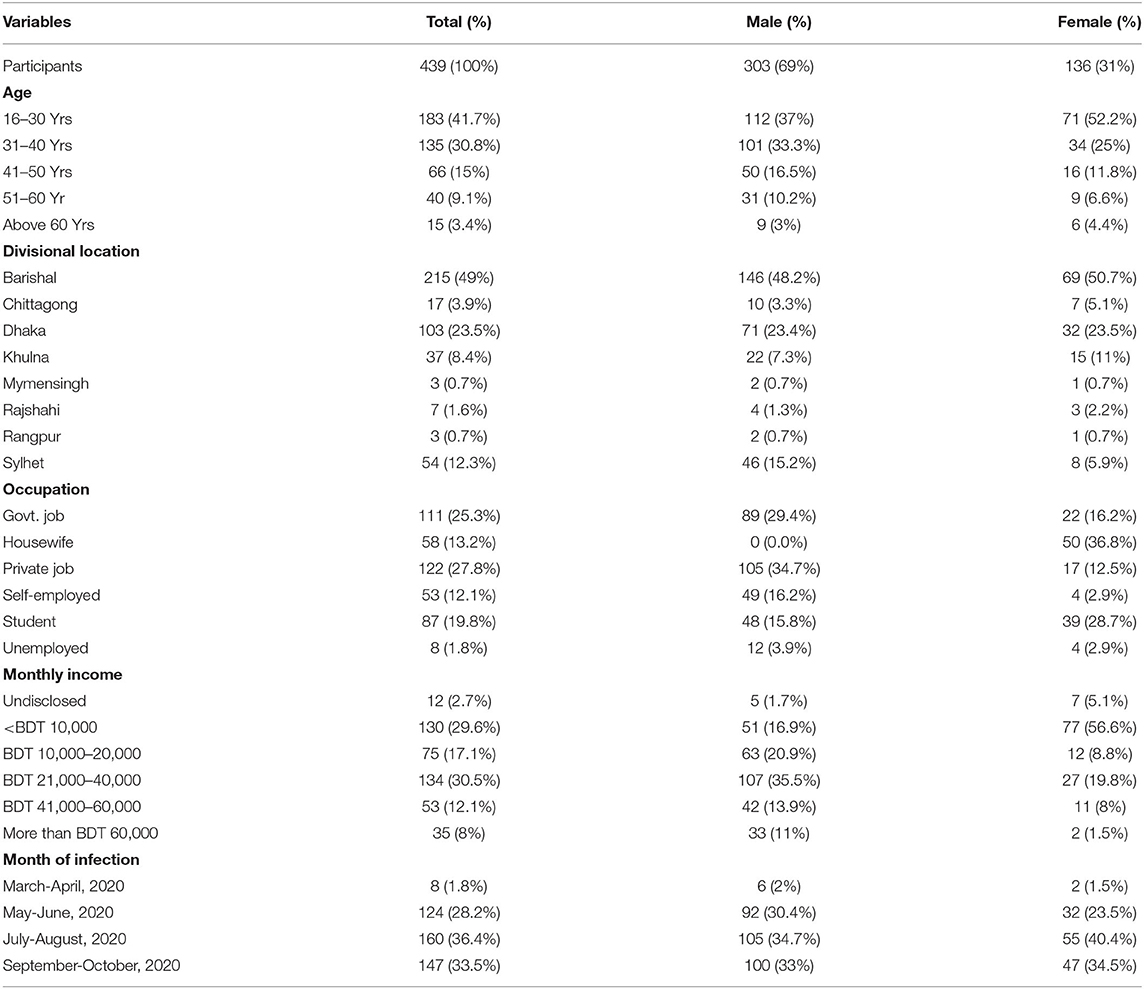
Table 1. Demographic distribution of the participants, Bangladesh, 2020.
Out of all the participants, 44.5% were students, and most non-student participants had a baccalaureate degree. There was a larger response among those with higher secondary education and graduates. The majority of the respondents (more than 70%) work in the private sector, whereas some were government job holders (25.28%) healthcare professionals and mostly worked or did Private Job holder or business (39.86) in a crowded place, 19.81% were students, and 18 % of the respondents reported that a relative, colleagues or a neighbor had been diagnosed with COVID-19.
One-third (29.6%, n = 130) of respondents' monthly income was below 10,000 BDT (117.81 USD), whereas another one-third (30.5%, n = 134) of respondent's monthly income was between 21,000 BDT to 40,000 BDT (247.41 USD to 471.27 USD). The exchange rate was considered 1 USD = 84.8775 (average of day's lowest and day's highest, data obtained from www.bb.org.bd/econdata/exchangerate.php on June 25th, 2021). Monthly income of above 60,000 BDT (706.9 USD) consist of 8% (n = 35), where 2.7% (n = 12) did not disclose the information (Table 1).
The prevalence and severity of the COVID-19 associated symptoms tend to be impacted by comorbidities. Therefore, participants were asked to report any chronic disease(s) they had been suffering from. Among 439 participants, 26.19% of participants (a total of 115 participants, among them 76 male and 39 female) reported that they had been suffering from different chronic diseases(s) or comorbidities (single or multiple chronic diseases) before being infected by the coronavirus, such as asthma, chronic obstructive pulmonary disease (COPD), diabetes, hypertension, stroke, heart attack, other heart diseases, kidney disease, allergy, arthritis, liver disease, and obesity. The self-reported comorbidities were later categorized as Lung disease (asthma, COPD, and other respiratory problems), diabetes, cardiac disease (hypertension, stroke, heart attack, and other heart diseases), and miscellaneous (kidney disease, allergy, rhinitis, liver disease, and obesity). 18.67% of total participants (n = 82) had cardiac disease, 6.83% (n = 30) had diabetes, 5% (n = 22) had lung disease, and the rest of the comorbid participants (2.96%, n = 13) were suffering from miscellaneous chronic conditions.
The obtained result found that COVID-19-related complications led to the admission of 13% of participants to the hospital (Table 2). Comorbid patients were more prone to be hospitalized due to COVID-19 associated complications. Significant association in gender (χ2 = 12.870, p = 0.000) and comorbidity (χ2 = 26.924, p = 0.000) was also found in hospitalization due to COVID-19 associated complications.
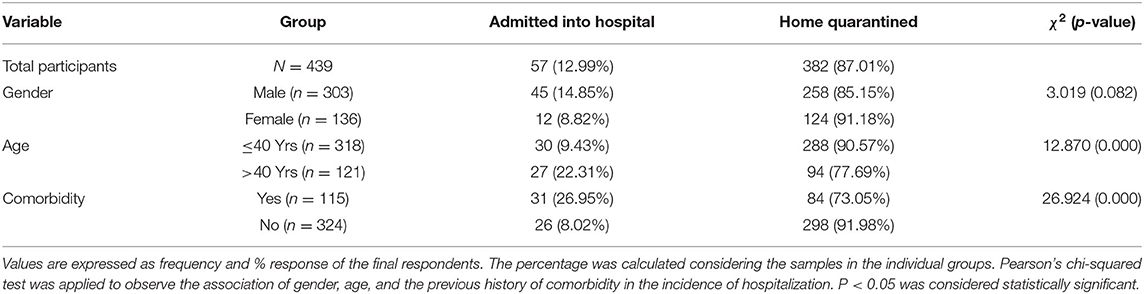
Table 2. Hospitalization due to COVID-19 associated complications, Bangladesh, 2020.
Table 3 shows the prevalence of COVID-19-related symptoms. Table 4 depicts how male gender, older age (>40 years), and comorbidity were associated (odds ratio) with the prevalence of these symptoms among the participants. Fever (93.60%), exhaustion (88.80%), and cough (70.80%) were the most prevalent symptoms reported by the participants. Loss of taste, sore throat, body ache, and hair loss were common among more than 50%. Nearly half of the respondents (49.70%) complained about the loss of smell due to the infection. Significant gender association was observed in sore throat (χ2 = 4.210; p = 0.040), loss of smell (χ2 = 5.671; p = 0.017), and vomiting (χ2 = 4.724; p = 0.030). The findings revealed that gender and comorbidities also had an impact on the characteristics of COVID-19-related symptoms. Older adults (>40 years) were significantly associated with shortness of breath (χ2 = 24.083; p = 0.000) and hair loss (χ2 = 38.887; p = 0.000). A significant difference was observed in the group based on comorbidity in shortness of breath (χ2 = 40.119; p = 0.000), vomiting (χ2 = 4.442; p = 0.035), confusion (χ2 = 15.558; p = 0.000), Loss of speech (χ2 = 17.299; p = 0.000) and hair loss (χ2 = 20.212; p = 0.000). Male patients showed 1.641 times higher odds (95% CI 1.090–2.472) of having the symptom of loss of smell than the female patients. Patients over 40 years old were significantly associated with shortness of breath [OR = 2.901 (95% CI 1.881–4.476)]. According to the findings, comorbidity was also found to be substantially linked with the prevalence of shortness of breath [OR = 4.042; (95% CI 2.564–6.374)], vomiting [OR = 1.689; (95% CI 1.018–2.802)], loss of speech [OR = 3.430 (1.944–6.053)], and Confusion [OR = 2.746 (95% CI 1.686–4.476)].
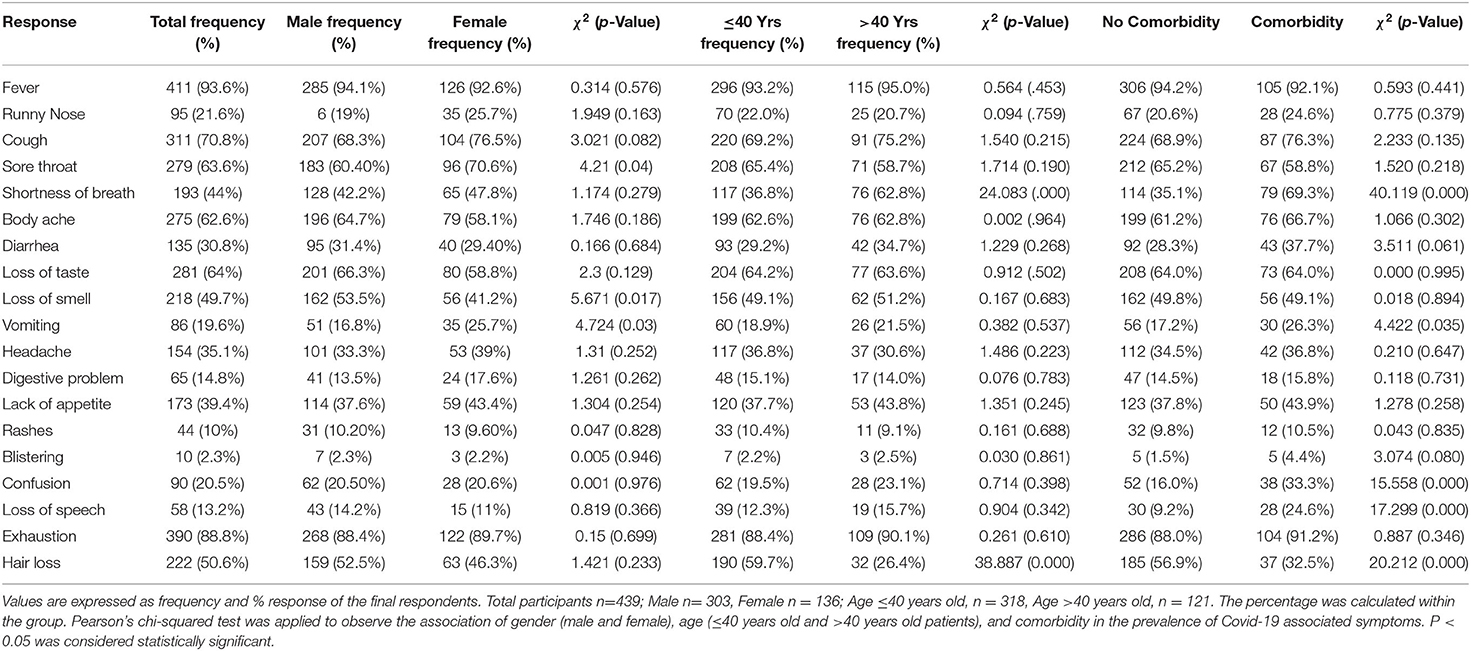
Table 3. Prevalence of the Covid-19 associated symptoms among the participants, Bangladesh, 2020.
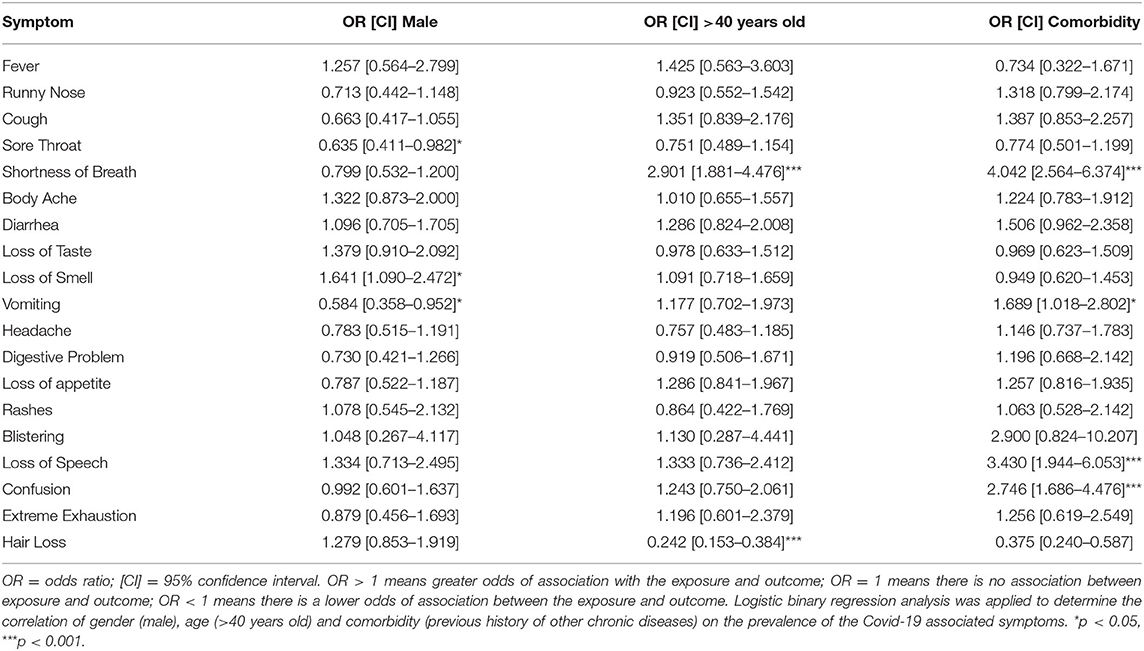
Table 4. Odds Ratios of Covid-19 associated symptoms, Bangladesh, 2020.
The onset and duration of COVID-19 related symptoms are described in Table 5 and Table 6, respectively. In brief, the most common symptom in COVID-19 patients was fever (93.6%, n = 411), which lasted for 1–4 days for most of the patients (77.4%, n = 340). The second most common symptom was exhaustion, reported in 89.8% (n = 390) patients and lasted for 11–14 days for 50% of the patients who have the symptom. Other accompanying symptoms were cough, body ache, loss of taste, loss of smell, lack of appetite, and headache, whereas more than 100 patients were affected by those symptoms. Out of all the symptoms we reported, exhaustion, sore throat, shortness of breath, body ache, vomiting, headache, digestive problems, lack of appetite, blistering, Confusion, and/or loss of speech were developed in some patients 14th days of infection. Interestingly, the onset of blistering was after 14th days for 20% of patients (n = 2). However, all the symptoms persisted in some patients for more than 14 days, whereas 33% (n = 127) exhibited exhaustion for more than 14 days. Similarly, Confusion occurred for more than 14 days in 27% of patients (n = 22).
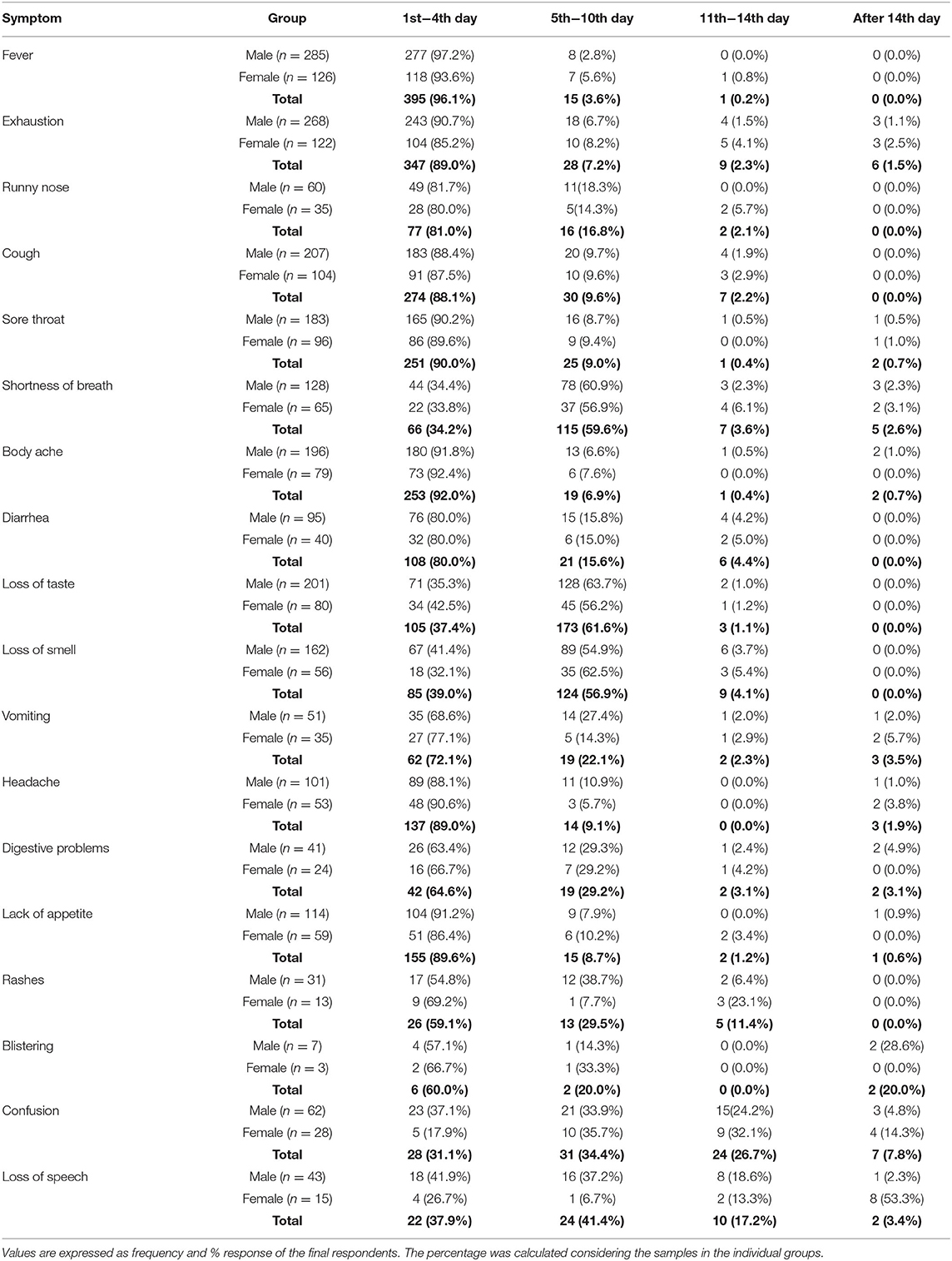
Table 5. Onset of COVID-19-associated symptoms in the patients, Bangladesh, 2020.
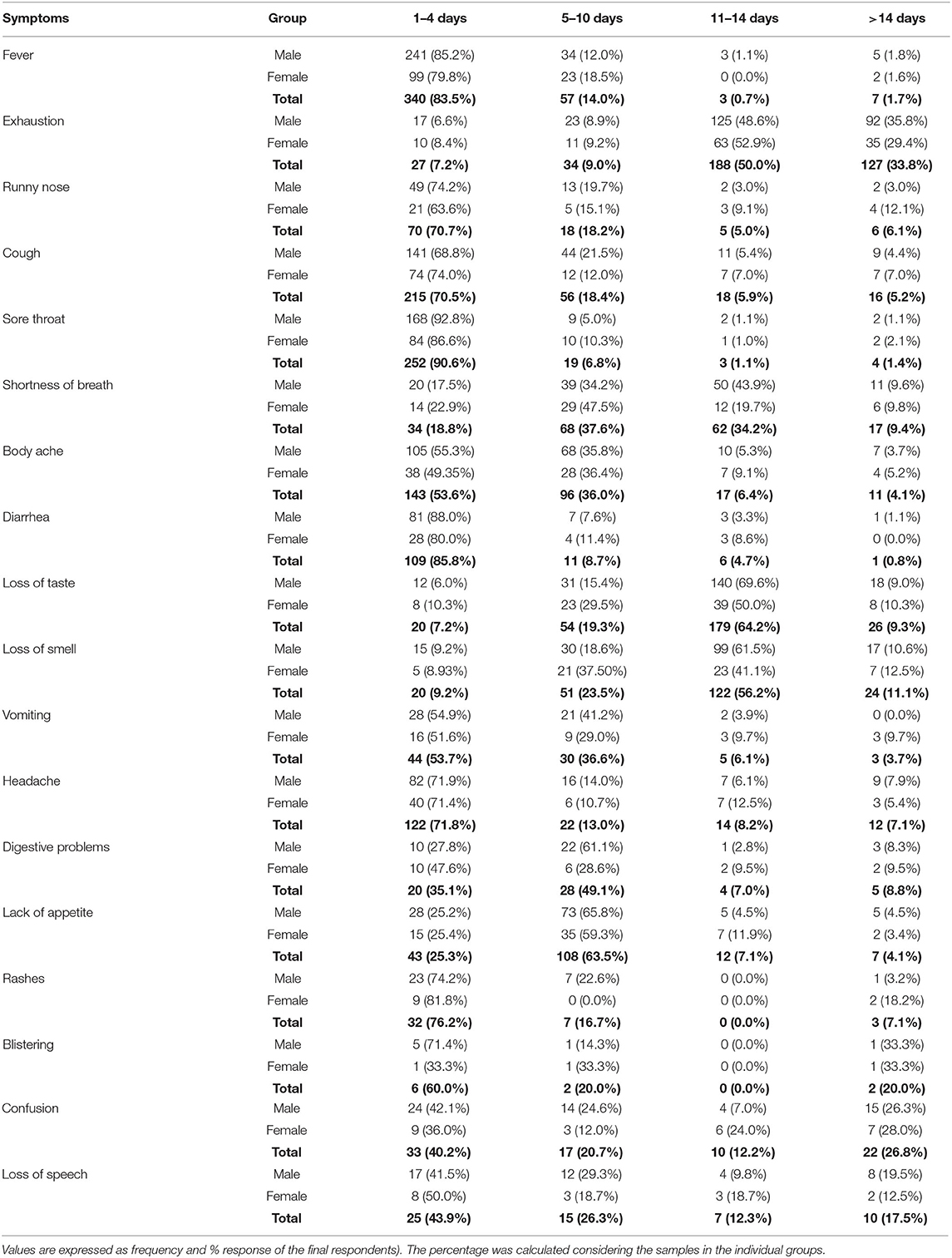
Table 6. Duration of the COVID-19-associated symptoms of the patients, Bangladesh, 2020.
In various patients, the time it takes to get a coronavirus infection negative by RT-PCR test may differ from the time it takes to recover from all symptoms. The duration required to get rid of all the COVID-19 associated symptoms was also assessed in this study and illustrated in Table 7. More than 53% of patients were recovered from all COVID-19 related symptoms within 8 to 14 days. However, most patients older than 40 years (45.5%) required 15–21 days to recover from the symptoms. Significant differences in the groups of age (χ2 = 16.890; p = 0.005) and comorbidity (χ2 = 23.638; p = 0.040) was observed in time required for the complete symptomatic recovery.
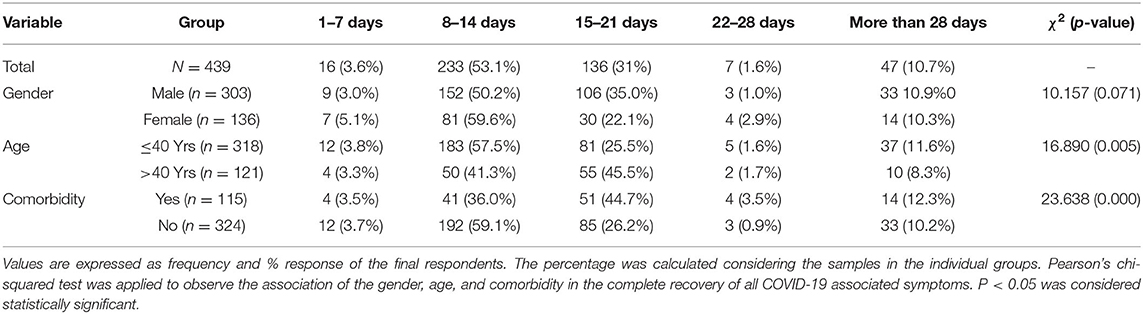
Table 7. Days required for symptomatic recovery in both male and female patients, Bangladesh, 2020.
In the last 20 years, several respiratory-related viral diseases such as SARS-CoV, H1N1 influenza, and MERS-CoV epidemics outbroke (36). Although previous coronaviruses, SARS-CoV and MERS-CoV, exhibited a high death rate, 9.6, and 35%, respectively, SARS-CoV-2 was declared as pandemic because of its high contagiousness and global spreading (36).
This study was conducted on 439 people in Bangladesh who recovered from COVID-19 at least 1 month before participating. Conforming to the first COVID-19 patient detection in Bangladesh, the survey includes the patients who got infected between March 2020 to September 2020. Our study found that most participants got infected from May-June, which matches the data obtained from the Directorate General of Health Services (DGHS) (Figure 1). Only 8 (1.8%) respondents got infected between March and April, suggesting that the virus took about 2 months to widespread. Most patients were between the ages above 40 years, and the male patient rate was 74.38%.
When we try to assess the relationship between hospitalization rate and predictors such as gender, age, or comorbidity, we found elderly patients had a significantly high hospitalization rate (22.31 vs. 9.43%), and 26.95% of patients with comorbidity were hospitalized compared to the patients (8.02%) who were hospitalized without any comorbid condition. The data suggest that age and comorbid conditions play a significant role in the severity of COVID-19. A recent study also found that the elder patients group (median age 69) had a long time of illness onset to hospitalization compared to the younger patients group (median age 40) (37). The study conducted in rural US patients found that hospitalized patients had a higher comorbidity burden (38). However, one of the major drawbacks of this cross-sectional study is determining the disease conditions. Since most were treated at home, we excluded some symptoms such as pneumonia because of a complicated diagnosis. Another limitation could include the lack of mortality data since we did not include deceased patients.
Next, we conducted a chi-square test to study the role of gender, age, and comorbidity in the prevalence of the Covid-19 associated symptoms. Out of all the symptoms we have tested, we found gender is a risk factor for sore throat and loss of smell, whereas aging and comorbidity could be a risk factors for shortness of breath and hair loss. Furthermore, we found a difference in symptomatic prevalence for vomiting, confusion, and loss of speech between the comorbid patients and the patients without any second disease. Further, odd ratios were calculated to assess the high risk of certain groups in the gender, age, and comorbidity predictors. Male patients showed a high-risk factor for the loss of smell symptom, whereas elderly patients had higher risk factors in developing shortness of breath than ≤40 years of age. Four symptoms such as shortness of breath, vomiting, loss of speech, confusion demonstrated high prevalence in comorbid patients.
One plausible reason for the gender differences could be due to hormonal differences. Female has shown higher incidence rate than male; however, female age between 20 s and 70 s exhibited lower incidence rate than similar age of male. The study suggests that estrogen may play a protective role with the other susceptible factors by inhibiting the entry of the SARS-CoV-2 virus into the host cells (39). Another important susceptible factor is age. A study conducted in 5,484 case contacts found that only 18.1% of participants developed symptoms below age 20, whereas 64.6% of participants demonstrated symptoms above age 80 (40). Chronic illnesses including hypertension, respiratory disease, kidney disease, diabetes, and cancer are considered underlying conditions that put people at greater risk with COVID-19. Hence we have included comorbid conditions (such as lung disease, cardiac disease, diabetes, and miscellaneous) to find their impacts on the symptoms. The study found that patients with comorbid disease/diseases had increased hospitalization rates and longer extended recovery periods. A retrospective study also described that aging and comorbid diseases possess higher severity and mortality in COVID-19 and SARS patients (41). Studies also found that patients with diabetes, heart disease, and other comorbidities had an increased risk of severity (42, 43). Similar to other studies, we also found comorbidity is a prime risk factor for COVID-19 patients in Bangladesh.
The most prevalent symptom in the COVID-19 patient was fever followed by exhaustion, cough, loss of taste, sore throat, and body ache. In general, all the symptoms showed up within 10 days of infection. However, 20% of patients who developed blistering demonstrated onset after 14th days of disease. While the incidence rate is low and the actual mechanism is still unknown, it is possible that angiotensin-converting enzyme-2 (ACE-2) available under the skin may play a role in the dermatological manifestation of SARS-CoV-2 virus can enter through ACE-2 receptors (44). Furthermore, some other neurological symptoms such as Confusion and loss of speech were also developed after the 14th day of infection. Neurological symptoms were found in 36.4% of patients in a previous study conducted in 214 patients (45). Another study conducted in France found that more than two-thirds of the cases demonstrated altered consciousness, including agitation and Confusion (46). Although SARS-CoV-2 can induce neurological damage, the exact mechanism is yet to be discovered. It is postulated that the virus can disseminate through the cribriform plate and olfactory bulb; and damage the capillary endothelium to induce brain injury (45). A preclinical study showed that the SARS virus could cause neuronal loss through transneuronal spreading from the olfactory bulb in K18-hACE2 mice (47). Hence, several reasons such as viral encephalitis, metabolic perturbation, infectious, toxic encephalopathy, seizures with post-ictal Confusion, and stroke could be the underlying reason behind neurological symptoms (46).
While most symptoms persisted for 1 to 10 days, some symptoms such as extreme exhaustion (33%), loss of smell (11%), loss of speech, blistering (20%), and confusion (27%) persisted for more than 14 days. While it is not clear why the onset and duration of symptoms vary from patient to patient, studies suggest that low interferon response in some patients could be the possible underlying mechanism of severity (48, 49). Nevertheless, the onset and duration data also match the study conducted by Lauer et al., where they analyzed 181 cases from outside Hubei province, China, and found the onset of symptoms for SARS-CoV-2 is ~5 days, and 101 out of every 10,000 cases developed symptoms after 14 days of monitoring or quarantine (50).
This study demonstrates the prevalent symptoms in COVID-19 patients affected from March 2020 to September 2020 in Bangladesh. To date, there are limited data available for the prevalence of symptoms in COVID-19 patients in Bangladesh. This study found that older (>40 years old) and comorbid patients required more hospitalization due to the COVID-19 associated complications, where comorbid patients were more susceptible to have shortness of breath, vomiting, loss of speech, and confusion. In regards of gender difference, the prevalence of sore throat, loss of smell, and vomiting were significantly higher in the male patient. Age and comorbidity also played a crucial role in the duration required to recover from all the COVID-19 associated symptoms. Since this study is highly relevant to the clinical outcomes of COVID-19, the data on different predictors such as age, gender, and comorbidity observed can provide valuable insight into the management of COVID-19 symptoms and can also lead to the understanding of disease progression.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Jagannath University Research Cell. The patients/participants provided their written informed consent to participate in this study.
MA, MH, and TA conceptualized the study, analyzed the data, developed the methods and materials, and wrote the manuscript. MA and TA conducted the study. MH and TA edited the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.738352/full#supplementary-material
1. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. (2020) 395:497–506. doi: 10.1016/S0140-6736(20)30183-5
2. McIntosh K, Hirsch MS, Bloom A. Coronavirus disease 2019 (COVID-19). UpToDate Hirsch MS Bloom. (2020) 5:1–1.
3. WHO Announces Simple Easy-to-Say Labels for SARS-CoV-2 Variants of Interest and Concern. Available online at: https://www.who.int/news/item/31-05-2021-who-announces-simple-easy-to-say-labels-for-sars-cov-2-variants-of-interest-and-concern (accessed October 07, 2021).
4. Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF. The proximal origin of SARS-CoV-2. Nat Med. (2020) 26:450–2. doi: 10.1038/s41591-020-0820-9
5. Baloch S, Baloch MA, Zheng T, Pei X. The coronavirus disease 2019 (COVID-19) pandemic. Tohoku J Exp Med. (2020) 250:271–8. doi: 10.1620/tjem.250.271
6. Spinelli A, Pellino G. COVID-19 pandemic: perspectives on an unfolding crisis. J Br Surg. (2020) 107:785–7. doi: 10.1002/bjs.11627
7. Zhang S, Tuo J, Huang X, Zhu X, Zhang D, Zhou K, et al. Epidemiology characteristics of human coronaviruses in patients with respiratory infection symptoms and phylogenetic analysis of HCoV-OC43 during 2010-2015 in Guangzhou. PLoS ONE. (2018) 13:e0191789. doi: 10.1371/journal.pone.0191789
8. Li J, Chen Z, Nie Y, Ma Y, Guo Q, Dai X. Identification of symptoms prognostic of COVID-19 severity: multivariate data analysis of a case series in Henan Province. J Med Internet Res. (2020) 22:e19636. doi: 10.2196/19636
9. Di Gennaro F, Pizzol D, Marotta C, Antunes M, Racalbuto V, Veronese N, et al. Coronavirus diseases (COVID-19) current status and future perspectives: a narrative review. Int J Environ Res Public Health. (2020) 17:2690. doi: 10.3390/ijerph17082690
10. Mackenzie JS, Smith DW. COVID-19: a novel zoonotic disease caused by a coronavirus from China: what we know and what we don't. Microbiol Aust. (2020) MA20013. doi: 10.1071/MA20013. [Epub ahead of print].
11. Hafeez A, Ahmad S, Siddqui SA, Ahmad M, Mishra S. A review of COVID-19 (Coronavirus Disease-2019) diagnosis, treatments and prevention. EJMO. (2020) 4:116–25. doi: 10.14744/ejmo.2020.90853
12. Perlman S, Netland J. Coronaviruses post-SARS: update on replication and pathogenesis. Nat Rev Microbiol. (2009) 7:439–50. doi: 10.1038/nrmicro2147
13. Hu H, Jung K, Wang Q, Saif LJ, Vlasova AN. Development of a one-step RT-PCR assay for detection of pancoronaviruses (α-, β-, γ-, and δ-coronaviruses) using newly designed degenerate primers for porcine and avianfecal samples. J Virol Methods. (2018) 256:116–22. doi: 10.1016/j.jviromet.2018.02.021
14. Budholiya P, Ali AW, Gunwan D, Sahil S, Tyagi CK, Sharma H. COVID-19: a global pandemic of 21st Century. J Drug Deliv Ther. (2020) 10(3-s):311–21. doi: 10.22270/jddt.v10i3-s.4088
15. He X, Lau EH, Wu P, Deng X, Wang J, Hao X, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. (2020) 26:672–5. doi: 10.1038/s41591-020-0869-5
16. Lechien JR, Chiesa-Estomba CM, Hans S, Barillari MR, Jouffe L, Saussez S. Loss of smell and taste in 2013 European patients with mild to moderate COVID-19. Ann Intern Med. (2020) 173:672–5. doi: 10.7326/M20-2428
17. Menni C, Valdes AM, Freidin MB, Sudre CH, Nguyen LH, Drew DA, et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat Med. (2020) 26:1037–40. doi: 10.1038/s41591-020-0916-2
18. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. (2020) 323:1061–9. doi: 10.1001/jama.2020.1585
19. Li L, Huang T, Wang Y, Wang Z, Liang Y, Huang T, et al. COVID-19 patients' clinical characteristics, discharge rate, and fatality rate of meta-analysis. J Med Virol. (2020) 92:577–83. doi: 10.1002/jmv.25757
20. Carfì A, Bernabei R, Landi F. Persistent symptoms in patients after acute COVID-19. Jama. (2020) 324:603–5. doi: 10.1001/jama.2020.12603
21. Tenforde MW, Kim SS, Lindsell CJ, Rose EB, Shapiro NI, Files DC, et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network—United States, March–June 2020. Morb Mortal Wkly Rep. (2020) 69:993. doi: 10.15585/mmwr.mm6930e1
22. Kopel J, Perisetti A, Roghani A, Aziz M, Gajendran M, Goyal H. Racial and gender-based differences in COVID-19. Front Public Health. (2020) 8:418. doi: 10.3389/fpubh.2020.00418
23. Sze S, Pan D, Nevill CR, Gray LJ, Martin CA, Nazareth J, et al. Ethnicity and clinical outcomes in COVID-19: a systematic review and meta-analysis. EClin Med. (2020) 29–30:100630. doi: 10.1016/j.eclinm.2020.100630
24. World Health O. Novel Coronavirus (2019-nCoV): Situation Report, 11 (Geneva) (2020). Retrieved from: https://apps.who.int/iris/handle/10665/330776
25. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS ONE. (2020) 15:e0239254. doi: 10.1371/journal.pone.0239254
26. Islam MS, Potenza MN, van Os J. Posttraumatic stress disorder during the COVID-19 pandemic: upcoming challenges in Bangladesh and preventive strategies. Int J Soc Psychiatry. (2020) 67:205–6. doi: 10.1177/0020764020954469
27. Bhattacharjee A. Epidemiology and clinical course of asymptomatic COVID-19 infection. Sch J App Med Sci. (2021) 2:194–8. doi: 10.36347/sjams.2021.v09i02.004
28. Khan MAS, Debnath S, Islam MS, Zaman S, Ambia N-E, Barshan AD, et al. Mental health of young people amidst COVID-19 pandemic in Bangladesh. Heliyon. (2021) 7:e07173. doi: 10.1016/j.heliyon.2021.e07173
29. Biernacki P, Waldorf D. Snowball sampling: problems and techniques of chain referral sampling. Soc Meth Res. (1981) 10:141–63. doi: 10.1177/004912418101000205
31. Hosen I, Pakpour AH, Sakib N, Hussain N, Al Mamun F, Mamun MA. Knowledge and preventive behaviors regarding COVID-19 in Bangladesh: a nationwide distribution. PLoS ONE. (2021) 16:e0251151. doi: 10.1371/journal.pone.0251151
32. Islam M, Islam US, Mosaddek ASM, Potenza MN, Pardhan S. Treatment, persistent symptoms, and depression in people infected with COVID-19 in Bangladesh. Int J Environ Res Public Health. (2021) 18:1453. doi: 10.3390/ijerph18041453
33. Wang Y, Di Y, Ye J, Wei W. Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID-19) in some regions of China. Psychol Health Med. (2021) 26:13–22. doi: 10.1080/13548506.2020.1746817
34. Association GA of the WM. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. (2014) 81:14–8.
35. Bryson GL, Turgeon AF, Choi PT. The science of opinion: survey methods in research. Can J Anesth Can Anesth. (2012) 59:736–42. doi: 10.1007/s12630-012-9727-3
36. Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19). In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing (2021).
37. Deng Y, Liu W, Liu K, Fang Y-Y, Shang J, Zhou L, et al. Clinical characteristics of fatal and recovered cases of coronavirus disease 2019 in Wuhan, China: a retrospective study. Chin Med J. (2020) 133:1261–7. doi: 10.1097/CM9.0000000000000824
38. Shah P, Owens J, Franklin J, Mehta A, Heymann W, Sewell W, et al. Demographics, comorbidities and outcomes in hospitalized Covid-19 patients in rural southwest Georgia. Ann Med. (2020) 52:354–60. doi: 10.1080/07853890.2020.1791356
39. O'Brien J, Du KY, Peng C. Incidence, clinical features, and outcomes of COVID-19 in Canada: impact of sex and age. J Ovarian Res. (2020) 13:1–12. doi: 10.1186/s13048-020-00734-4
40. Poletti P, Tirani M, Cereda D, Trentini F, Guzzetta G, Sabatino G, et al. Association of age with likelihood of developing symptoms and critical disease among close contacts exposed to patients with confirmed sars-cov-2 infection in italy. JAMA Netw Open. (2021) 4:e211085. doi: 10.1001/jamanetworkopen.2021.1085
41. Jin J-M, Bai P, He W, Wu F, Liu X-F, Han D-M, et al. Gender differences in patients with COVID-19: focus on severity and mortality. Front Public Health. (2020) 8:152. doi: 10.3389/fpubh.2020.00152
42. Henry BM, de Oliveira MHS, Benoit J, Lippi G. Gastrointestinal symptoms associated with severity of coronavirus disease 2019 (COVID-19): a pooled analysis. Intern Emerg Med. (2020) 15:857–9. doi: 10.1007/s11739-020-02329-9
43. Sanyaolu A, Okorie C, Marinkovic A, Patidar R, Younis K, Desai P, et al. Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med. (2020) 2:1–8. doi: 10.1007/s42399-020-00363-4
44. Gottlieb M, Long B. Dermatologic manifestations and complications of COVID-19. Am J Emerg Med. (2020) 38:1715–21. doi: 10.1016/j.ajem.2020.06.011
45. Montalvan V, Lee J, Bueso T, De Toledo J, Rivas K. Neurological manifestations of COVID-19 and other coronavirus infections: a systematic review. Clin Neurol Neurosurg. (2020) 194:105921. doi: 10.1016/j.clineuro.2020.105921
46. Lahiri D, Ardila A. COVID-19 pandemic: a neurological perspective. Cureus. (2020) 12:e7889. doi: 10.7759/cureus.7889
47. Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S. Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol. (2008) 82:7264–75. doi: 10.1128/JVI.00737-08
48. Acharya D, Liu G, Gack MU. Dysregulation of type I interferon responses in COVID-19. Nat Rev Immunol. (2020) 20:397–8. doi: 10.1038/s41577-020-0346-x
49. Salman AA, Waheed MH, Ali-Abdulsahib AA, Atwan ZW. Low type I interferon response in COVID-19 patients: interferon response may be a potential treatment for COVID-19. Biomed Rep. (2021) 14:1–5. doi: 10.3892/br.2021.1419
Keywords: COVID-19, SARS-CoV-2, COVID-19 symptoms, corona, flu, symptoms, fever, cold
Citation: Amin MT, Hasan M and Bhuiya NMMA (2021) Prevalence of Covid-19 Associated Symptoms, Their Onset and Duration, and Variations Among Different Groups of Patients in Bangladesh. Front. Public Health 9:738352. doi: 10.3389/fpubh.2021.738352
Received: 08 July 2021; Accepted: 30 August 2021;
Published: 29 September 2021.
Edited by:
Reza Lashgari, Shahid Beheshti University, IranReviewed by:
Pritom Chowdhury, Tea Research Association, IndiaCopyright © 2021 Amin, Hasan and Bhuiya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: N. M. Mahmudul Alam Bhuiya, bWFobXVkdWxAcGhhcm0uam51LmFjLmJk
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.