 Monica Elisa Meneses-La-Riva
Monica Elisa Meneses-La-Riva Josefina Amanda Suyo-Vega
Josefina Amanda Suyo-Vega Víctor Hugo Fernández-Bedoya
Víctor Hugo Fernández-Bedoya- 1School of Nursing, Universidad César Vallejo, Lima, Peru
- 2School of Education, Universidad César Vallejo, Lima, Peru
- 3School of Management, Universidad César Vallejo, Lima, Peru
Nowadays, humanized care is an essential component in the field of health because the professional work of nursing seeks to provide quality services to patients who are suffering and fear illness or the dying process. Nurses recognize the need to incorporate humanized care into their daily work, as supported by Jean Watson, who states that caring entails establishing an adequate nurse–patient therapeutic relationship, where health education is a tool that promotes self-care in the patient, family, and community. The main objective of this work was to find scientific evidence on humanized care from the perspectives of nurses and hospitalized patients. To meet those research objectives, an exploratory systematic review of articles published in high-quality scientific journals from 2016 to 2020 using the PRISMA methodology in the Scopus and Scielo databases was conducted, yielding 26 studies that were analyzed. The findings show that nurses and patients perceive the need to remove the barriers that limit the advancement of humanized care in hospital institutions because they urgently demand that health professionals in all settings, especially critical ones, strengthen their humanizing role by sharing cordial, empathetic health experiences, and respecting their customs and beliefs during the hospitalization process. As a conclusion of the findings, the nurse–patient professionals agree that health personnel training is critical to providing humanized attention with quality in the hospital context, emphasizing that professional training should develop in practice soft skills, communication, safety environment, and human values.
Introduction
The humanization of care is an essential element to achieve the promotion of well-being during the processes of care within health systems because the hospital environment is immersed in an imbalance of emotions resulting from the suffering and anxiety endured by the sick person and the family (1, 2).
Promoting humanized care during the daily work of health professionals implies promoting the universality of the right to health as an essential element and where there should be no distinction of any kind (3). This should be developed as an integral formation of every nursing student in the university classrooms (4, 5).
The humanization of health services seeks to raise the quality of care at the administrative and assistance levels, for comprehensive care and without financial difficulties throughout the life of the patient (6–8).
The essence of nursing care is founded on Jean Watson's (9–12) theory, which states that care necessitates a way of being able to interact and connect with the patient and the family, with the goal of providing an environment of excellence, comfort, and safety, with high competencies, skills, and conditions to achieve holistic care (13).
Some authors agree that the conceptualization of care, the essential art of nursing, is to care for the most primitive act that a human being performs to effectively become, this being, a being in relation to another who invokes it in an ethical and philosophical foundation (14–19). Humanized care represents an enlightening guide and support to the practice for its benefit in cultivating a conscience of care and the establishment of a strong and sustainable therapeutic relationship. Therefore, care represents the work of nursing, based on humanistic values in order to meet the needs of patients and improve their quality of life (20, 21).
Care, as the essence of professional nursing practice, necessitates that professionals know how to act with ethical commitment, foster relationships of understanding, empathy, and respect, and prioritize actions to provide timely responses to difficulties, because humanized care, to be meaningful, must be based on the reciprocity of professionals in the face of health problems (22–24). However, no one is unaware that health services are seen as stressful and overcrowded places for patients, which causes emotional exhaustion in professionals as a result of work overload and lack of resources, which makes care management a current challenge for health professionals, especially for nurses (25, 26).
On the other hand, the dynamics of action of nursing professionals is to provide comprehensive care from the practice of learned scientific knowledge and their own experience, with the objective that the patient achieves physical, psychosocial, and spiritual well-being (27); since care has ethical bases, originates autonomy, and creates confidence and security (28).
In reference to the problematic reality, it can still be seen that nurses still govern their work in a technical–scientific and somewhat mechanized manner, often disregarding the human aspect, which alienates the patient and damages interpersonal relationships (29). In this regard, the humanized care approach conceives that “the other human being” in front of us, expects humanized care, being necessary that professionals have the appropriate qualities, which should be generated during academic training (30).
There are some studies that sought to systematize the evidence of the perception of humanized care received by patients or delivered by nurses throughout the world. Some cases can be reviewed in (31–33).
A systematic review was carried out in Chile on humanized care in patients with limited therapeutic effort focused on adults in intensive care in Ibero-America. The authors found 23 articles from the databases PubMed, Epistemonikos, Web of Science, Scielo, Elsevier, and added information from other electronic sources such as End-of-Life Journal and Journal of Medical Ethics. The main conclusion of the study was the determination that the nursing professional is aware of the diversity of roles he or she fulfills when attending to a patient, but when applying humanized care, the relationship between patient, family, and medical team is evidenced, communication being a priority agent for the knowledge of the needs of the patient (34).
Likewise, a systematic review on humanized care in children was carried out in Italy, analyzing scientific evidence published in the PubMed and Scopus databases. Only 28 records met the inclusion criteria, and it was concluded that humanized care is elementary for pediatric hospital global management, being necessary to continue research to strengthen child-centered research (31).
In Spain, the results of a systematic review on the humanized care of the neonate and the family were disclosed. The search was done in PubMed, Cochrane, CINHAL, Scopus, and Google Scholar databases. Thirteen peer-reviewed scientific articles were found that met the inclusion criteria, whose conclusions suggest the promotion of family participation through the modification of health policies such as the daily and permanent attention of the nurse and their constant communication (33).
Currently, health institutions show an urgent need to strengthen the right and guarantee accessibility to health services with a human face. Thus, humanized care is a way to raise the quality of health services provided by health professionals, especially nurses, who must create a safe environment, with dignified treatment for the patient, family, and community. The satisfaction experienced by patients and families in health institutions is important to strengthen trust, quality of services in a safe environment to ensure holistic care in each individual, taking into account a moral commitment, through values of respect for the dignity of life, contributing to improve the quality of life of people (13).
To complement the findings identified by the authors previously developed, it was deemed convenient to carry out a systematic review on humanized care in hospitalized patients, compiling evidence published in Spanish in the Scopus and Scielo databases.
Materials and Methods
The study was an exploratory systematic review (35). We searched for evidence seeking to meet the research objectives in the Scopus and Scielo databases published in the years 2016–2020 in Spanish and Portuguese. The searches detailed in Table 1 were performed.
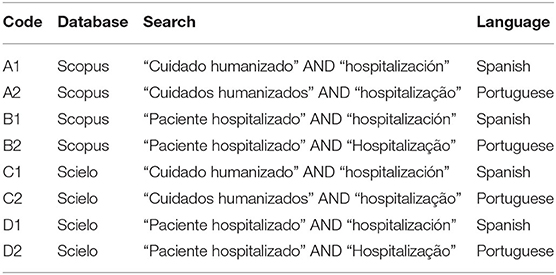
Table 1. Searches.
The initial search of the Scopus and Scielo databases yielded 74 records. During their exploration, 32 articles were identified that were neither downloadable nor visible, which were withdrawn from the study, resulting in a subtotal of 42 accessible records. The application of filters according to the inclusion and exclusion criteria resulted in 30 eligible records, of which four records were removed due to duplicity. The final result included 26 records. Having all the information collected, we proceeded according to the research question: What is the scientific evidence on humanized care from the point of view of nurse–patients in a hospital context?
To meet the objectives, the database was exhaustively reviewed and to categorize them, the titles, abstracts, and contents of each document were evaluated, extracting the data from the preselected and selected studies, to finally present the conclusions after analyzing and interpreting them. That said, the preferred reporting items for systematic review and meta-analyses (PRISMA) flow chart (36) was used for its presentation, which is detailed in Figure 1.
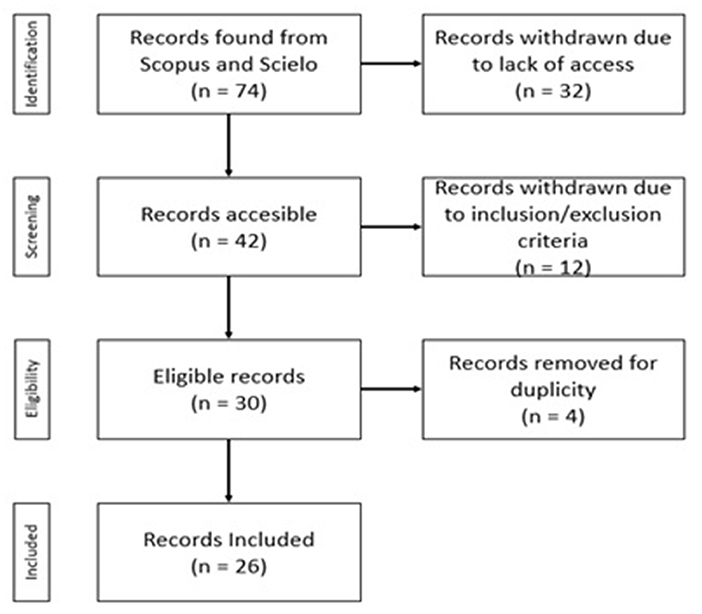
Figure 1. PRISMA flow chart.
Results
The 26 reorder identified were carefully reviewed and systematized and are shown in Table 2.
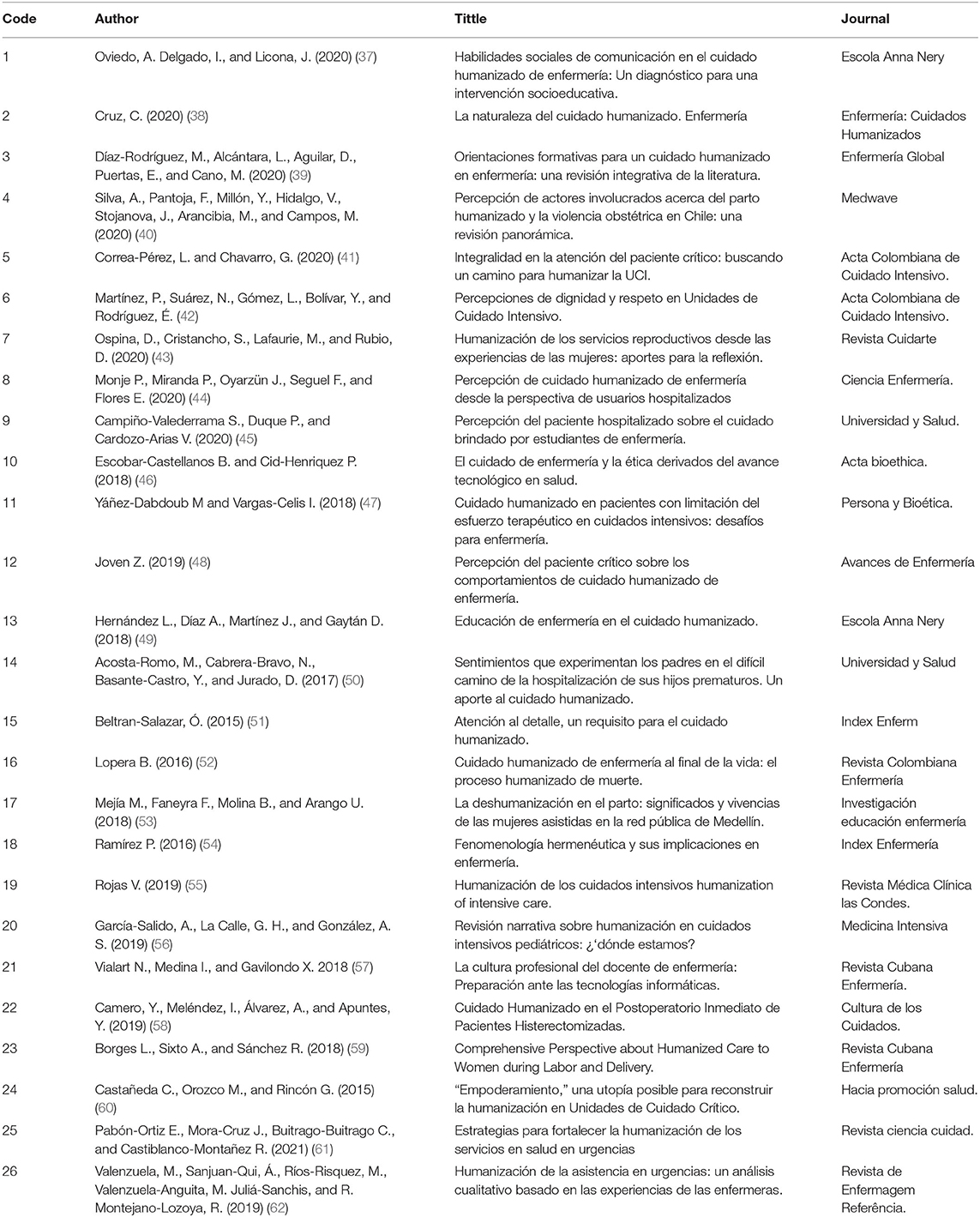
Table 2. Records identified.
A more detailed analysis by the authors identified relevant data for each of the records, such as the country where the study was carried out, the methodology applied, the results, and the conclusions reached. This is detailed in Table 3.
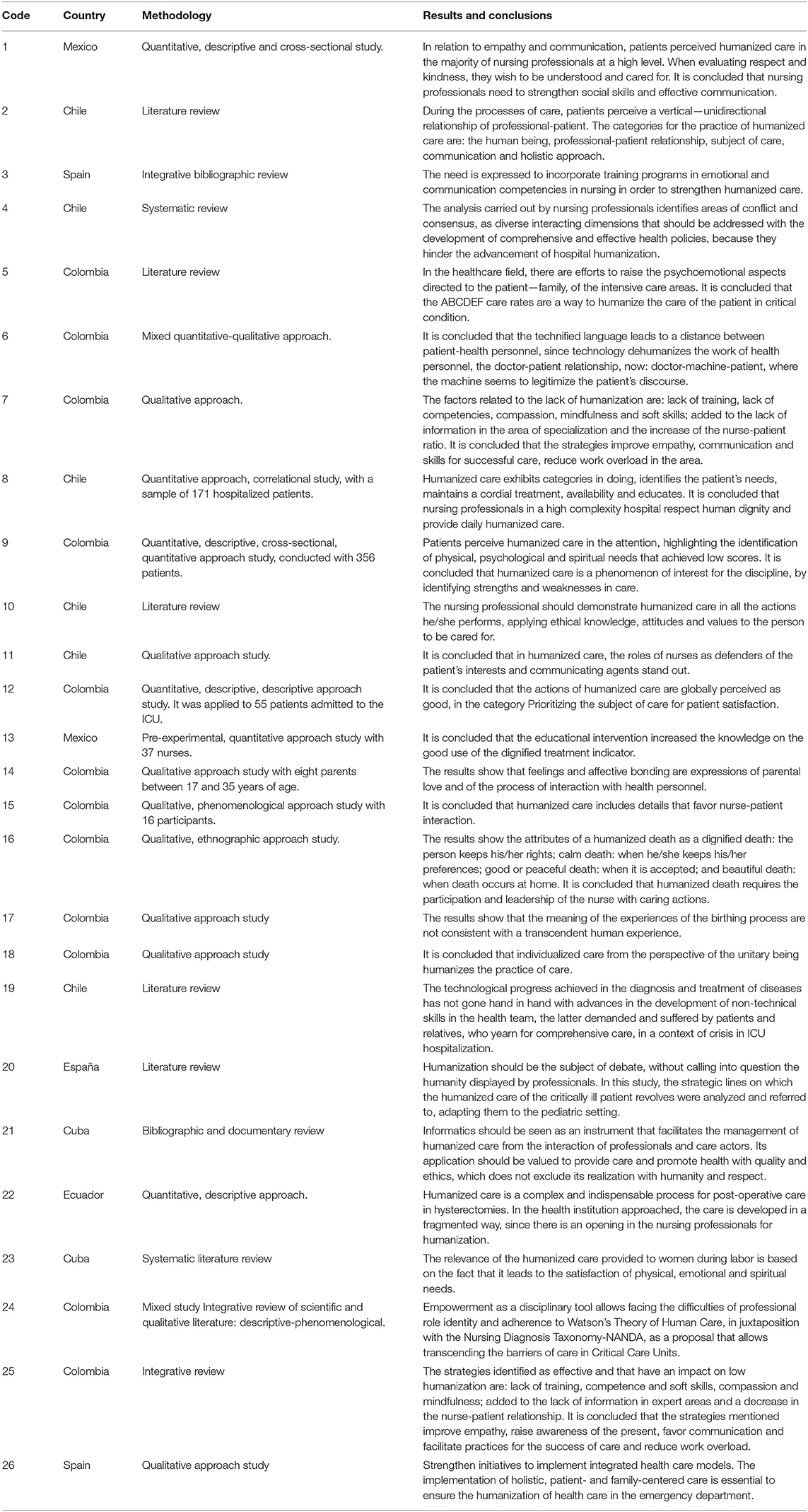
Table 3. Details of the studies.
Discussion
Articles pertaining to humanized care from the point of view of nurses–patients in a hospital context were found in the two databases. The articles were selected according to the objectives of the search, obtaining a total of 26 articles from six countries (Spain, Chile, Mexico, Cuba, Ecuador, and Colombia), which were quantitative (6), qualitative (9), mixed (1), and systematic review (10), which were critically analyzed to meet the objectives of the study.
Humanized nursing care is a unique way of caring within the health system, where the patient is offered a safe environment and protection of their human dignity, which sustains the care over time, educates to promote health and harmony in body, mind, and soul, based on a relationship of trust. Likewise, humanized nursing care attends to the human and therapeutic needs of the patient in his or her health–disease condition (13, 54).
The evidence suggests that from the perception of nurses–patients, the topic leads to discussing and reflecting on the complexity that humanized care implies, from dignified treatment to the application of institutional policies, for which the commitment of all social actors is required to assist in humanizing health institutions. Expressions that are perceived by nurse–patients in the hospital context are detailed.
Elimination of the Constraints of the Delivery of Humanized Care
Prieto Martínez et al. (42) state that patients and family members perceive limitations in humanized care related to the technified language that causes distance and distrust, and in health personnel they perceive a greater interest in technological equipment, diagnoses, and disease evolution, which brings with it a feeling of disinterest in the person and a lack of compassion in front of the suffering, and pain experienced by the person and the family.
Also, Ospina Vanegas et al. (43) point out that health professionals show a lack of soft and social skills, which makes it difficult for them to achieve adequate interpersonal relationships, especially in critical situations experienced by patients (21, 24). In fact, the health problems faced by patients lead to strict changes in their lifestyle, which generates emotional and even existential crises, with some physical limitations to carrying out their daily activities.
In this sense, health professionals assume critical behavior due to the same health situation experienced by patients, and the strict pressures to comply with medical indications generates insecurity, fear, and apprehension, resulting in distancing for interpersonal relationships and even little freedom to express doubts about emerging health scenarios, turning them into simple listeners, which hinders the achievement of joint goals designed by the nursing staff.
In relation to the infrastructure of health services, in some cases these do not meet the needs of patients as they do not protect privacy, do not provide comfort, and there is no waiting room for family members, among others. In addition, the lack of institutional policies does not allow promoting behavioral change of professionals within health institutions, who continue to label the patient with a bed number, a diagnosis, name of the disease, among others; who currently demand health services based on the right, with the freedom to make complaints or complaints in the institutions for mistreatment, misinformation, lack of medicines or disinterest in the health situation, among others.
Cruz C. argues that the hegemony of the medical paradigm wields a vertical-unidirectional relationship between the professional and the patient, where decision making is an obstacle to the joint work between health professionals–patient and family. However, the management of hospital services from a patient-centered vision favors the quality of health services with a sense of accessibility, social inclusion, and health for all from a humanizing vision (42). Likewise, Diaz Rodríguez et al. (39) report that deficiencies in professional training limit the competencies and soft skills of professionals, who are unable to deal with situations of emotional imbalance experienced by the patient during the care process.
In short, the various limitations in hospital systems affect management, block the expectations of patients and relatives, and the continuity of health care with the various phenomena experienced by the sick person and which are linked to suffering due to the disease itself and to treatment-care, because care is a service that requires faith, hope, and love. Considering that caring is an art and a science, it turns the service into a moment of transcendent gratitude.
Humanizing Nursing Role in Hospital Services, Especially in Critical Areas
According to international studies, participation and leadership of nurses in care actions are critical to supporting quality standards because of their role in defending the rights of the patient and acting as communication agents of care (46). According to Oviedo et al. (37), humanizing behavior creates a calm and confident environment for the health scenario that is being experienced, an affirmation that can be validated when patients yearn within the care attention process to establish affective bonds of trust with details of cordiality, kind treatment, active listening, empathy, solidarity, and respect for customs and beliefs (37, 48, 51).
According to Silva et al. (40), nursing professionals have to deal with highly complex services, most of whom respect human dignity by providing humanized care on a daily basis. However, these critical areas necessitate a high level of specialization and emotional skills from professionals to respond to the needs of the patient and family who live in a state of uncertainty due to the same situation or health condition of the patient. So professionals must be trained to deal with such situations from the standpoint of ethical knowledge of care (40).
In this regard, it is necessary to implement and strengthen professional and technical competencies and soft skills in nurses of critical services: emergency, post-operative, intensive care unit, pediatrics, maternity, oncology, among others, to provide holistic care focusing on the physical, psychological, and spiritual dimensions, among others (41, 45, 55, 56).
On the other hand, in the case of maternity services, women express the various emotions they experience in adapting to a new way of life. It should be noted that the process of childbirth is important for a woman, but it requires humanized care, where the health personnel can identify her needs, offer her cordial treatment, be available, and educate her so that she can deal with her own self-care and in the management of the integral care of her child (53).
In relation to areas where there is a high mortality rate, health professionals should generally have the appropriate competencies to address bereavement situations and care for a dignified death (52). Likewise, Correa-Pérez and Chavarro (41) state that nurses should make great efforts to train themselves in addressing the psychoemotional aspects of patients so that they can achieve relationships of trust that allow them to raise the quality of the services provided by the nurse.
Indicators That Favor the Implementation of Humanized Care
Humanized care includes the nurse–patient–family relationship, which strengthens the work performance and productivity levels of nurses who perform not only procedural activities, but also provide information and emotional, spiritual, and educational support, which raises the quality indicators in the care processes, safe environment, promotion of self-care, health education, and reduction of operating costs during the health care process, thus ensuring the sustainability of health care over time. Continuous training of care actors should promote the use of the dignified treatment indicator (49, 57).
Strategy and Innovation for a Path of Humanization
It is necessary to identify and prioritize health needs to assume the practice of human care for patients, considering the different human dimensions: physical, psychological, spiritual, among others; with the purpose of maintaining a predisposition to provide continuous care, promote dignified and cordial treatment, and motivate a safe environment that favors the process of care based on values (45). Caring requires the development of skills and the meeting of knowledge because it requires the capacity for active listening, kind response, and constant training to achieve the path to humanization.
During the outcome of care practice, nurses adhere to the Jean Watson theory to transcend in their work and achieve a balance of theoretical and practical approach that generates confidence during the health care process. Strengthening the soft skills of health professionals enables them to adequately increase interpersonal relationships that will support the psychological emotional aspects of patients, as well as maintain education and ongoing training of the patient and family (39, 41, 50).
Finally, humanized care is a way of life that the nursing professional assumes in order to identify the needs, expectations, and health demands of patients and family members who require professional nursing care. As a result, it is critical that the patient perceives highly qualified personnel with whom he or she can maintain trust bonds throughout the health-disease process, taking into account the patient's disposition, commitment, cordiality, kindness, simple language, and availability of care. However, it is necessary that institutional policies are applied to generate spaces for analysis to achieve quality indicators, according to international standards that consider humanized care as an essential right in the hospital context (58–62).
Conclusion
This systematic review evidences the knowledge gap regarding the development and/or construction of care models on humanized care in public and private institutions worldwide, a limitation that should become a worldwide challenge for the application of humanizing policies and models for practice and that should be linked to the professional practice of health personnel, especially nursing professionals, highlighting the prioritization of the basic needs of patients who should receive humanizing care that responds to social changes.
Since nursing professionals lack competencies and soft and social skills, patients are put in danger because they are not cared for in a comprehensive, quality, and warm manner.
It should be noted that care should reinforce the sense of trust to respond to their basic therapeutic needs based on an authentic safe care approach to the production of assistive care, which is an art that requires a willingness to care and share feelings and emotions during the interpersonal and transpersonal relationship between the caregiver and the patient.
Data Availability Statement
The systematic review was carried out using scientific articles available in the open access databases Redalyc and Scielo.
Author Contributions
All authors listed have equally contributed to the work and approved it for publication.
Funding
This study was carried out and funded by the Universidad César Vallejo, within the framework of the work plan outlined in RVI N° 052-2019-VI-UCV.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Velasco Bueno JM, La Calle GH. Humanizing intensive care: from theory to practice. Crit Care Nurs Clin North Am. (2020) 32:135–47. doi: 10.1016/j.cnc.2020.02.001
2. Riley BH, White J, Graham S, Alexandrov A. Traditional/restrictive vs. patient-centered intensive care unit visitation: perceptions of patients' family members, physicians, and nurses. Am J Crit Care. (2014) 23:316–24. doi: 10.4037/ajcc2014980
3. Chochinov HM. Dignity in care: time to take action. J Pain Symptom Manage. (2013) 46:756–9. doi: 10.1016/j.jpainsymman.2013.08.004
4. Fernández Trinidad M, González Pascual JL, Rodríguez García M. Perception of caring among nursing students: results from a cross-sectional survey. Nurse Educ Today. (2019) 83:104196. doi: 10.1016/j.nedt.2019.08.014
5. Rosser EA, Scammell J, Heaslip V, White S, Phillips J, Cooper K, et al. Caring values in undergraduate nurse students: a qualitative longtitudinal study. Nurse Educ Today. (2019) 77:65–70. doi: 10.1016/j.nedt.2019.03.011
6. Setoodegan E, Gholamzadeh S, Rakhshan M, Peiravi H. Nurses' lived experiences of professional autonomy in Iran. Int J Nurs Sci. (2019) 6:315–21. doi: 10.1016/j.ijnss.2019.05.002
7. Keramidou I, Triantafyllopoulos L. The impact of the financial crisis and austerity policies on the service quality of public hospitals in Greece. Health Policy (New York). (2018) 122:352–8. doi: 10.1016/j.healthpol.2017.12.008
8. Husson O, Huijgens PC, van der Graaf WTA. Psychosocial challenges and health-related quality of life of adolescents and young adults with hematologic malignancies. Blood. (2018) 132:385–92. doi: 10.1182/blood-2017-11-778555
9. Watson J, Smith MC. Caring science and the science of unitary human beings: a trans-theoretical discourse for nursing knowledge development. J Adv Nurs. (2002) 37:452–61. doi: 10.1046/j.1365-2648.2002.02112.x
10. Watson J, Foster R. The attending nurse caring model®: integrating theory, evidence and advanced caring-healing therapeutics for transforming professional practice. J Clin Nurs. (2003) 12:360–5. doi: 10.1046/j.1365-2702.2003.00774.x
11. Watson J. The theory of human caring: retrospective and prospective. Nurs Sci Q. (1997) 10:49–52. doi: 10.1177/089431849701000114
12. Watson J. Caring theory as an ethical guide to administrative and clinical practices. JONA's Healthc Law Ethics Regul. (2006) 8:87–93. doi: 10.1097/00128488-200607000-00008
13. Guerrero-Ramirez R, Meneses-La-Riva M, De-la-Cruz-Ruiz M. Cuidado humanizado de enfermería según la teoría de Jean Watson, servicio de medicina del Hospital Daniel Alcides Carrión. Lima- Callao, 2015. Rev enferm Hered. (2015) 9:127–36. doi: 10.20453/renh.v9i2.3017
14. Freed PE, McLaughlin DE. Promoting cultures of thinking: transforming nursing education to transform nursing practice. Creat Nurs. (2013) 19:174–81. doi: 10.1891/1078-4535.19.4.174
15. Palos GR. Care, compassion, and communication in professional nursing: art, science, or both. Clin J Oncol Nurs. (2014) 18:247–8. doi: 10.1188/14.CJON.247-248
16. Carroll K. Highlighting collaboration in living the art of nursing. Nurs Sci Q. (2019) 32:283–5. doi: 10.1177/0894318419864333
17. Henry D. Rediscovering the art of nursing to enhance nursing practice. Nurs Sci Q. (2018) 31:47–54. doi: 10.1177/0894318417741117
18. Robinson SG. True presence: practicing the art of nursing. Nursing (Lond). (2014) 44:44–5. doi: 10.1097/01.NURSE.0000444533.58704.e5
19. Kostovich CT, Clementi PS. Nursing presence: putting the art of nursing back into hospital orientation. J Nurses Prof Dev. (2014) 30:70–5. doi: 10.1097/NND.0000000000000045
20. Patistea E, Siamanta H. A literature review of patients' compared with nurses' perceptions of caring: implications for practice and research. J Prof Nurs. (1999) 15:302–12. doi: 10.1016/S8755-7223(99)80056-8
21. Erkus G, Dinc L. Turkish nurses' perceptions of professional values. J Prof Nurs. (2018) 34:226–32. doi: 10.1016/j.profnurs.2017.07.011
22. Heikkinen E, Isola A. Student nurses' experiences and perceptions of envy in one nurse education environment in Finland. Nurse Educ Today. (2004) 24:160–8. doi: 10.1016/j.nedt.2003.11.004
23. Carr G. Changes in nurse education: being a nurse teacher. Nurse Educ Today. (2007) 27:893–9. doi: 10.1016/j.nedt.2006.12.006
24. Kenny G. The origins of current nurse education policy and its implication for nurse educators. Nurse Educ Today. (2004) 24:84–90. doi: 10.1016/j.nedt.2003.09.001
25. Elder E, Johnston ANB, Wallis M, Crilly J. The demoralisation of nurses and medical doctors working in the emergency department: a qualitative descriptive study. Int Emerg Nurs. (2020) 52:100841. doi: 10.1016/j.ienj.2020.100841
26. Wolf LA, Delao AM, Perhats C, Clark PR, Edwards C, Frankenberger WD. Traumatic stress in emergency nurses: does your work environment feel like a war zone? Int Emerg Nurs. (2020) 52:100895. doi: 10.1016/j.ienj.2020.100895
27. Suhonen R, Stolt M, Habermann M, Hjaltadottir I, Vryonides S, Tonnessen S. et al. Ethical elements in priority setting in nursing care: a scoping review. Int J Nurs Stud. (2018) 88:25–42. doi: 10.1016/j.ijnurstu.2018.08.006
28. Stutzer K, Rodriguez AM. Moral resilience for critical care nurses. Crit Care Nurs Clin North Am. (2020) 32:383–93. doi: 10.1016/j.cnc.2020.05.002
29. Luchsinger JS, Jones J, McFarland AK, Kissler K. Examining nurse/patient relationships in care coordination: a qualitative metasynthesis. Appl Nurs Res. (2019) 49:41–9. doi: 10.1016/j.apnr.2019.07.006
30. Christopher R, de Tantillo L, Watson J. Academic caring pedagogy, presence, and Communitas in nursing education during the COVID-19 pandemic. Nurs Outlook. (2020) 68:822–9. doi: 10.1016/j.outlook.2020.08.006
31. Tripodi M, Siano MA, Mandato C, De Anseris AGE, Quitadamo P, Guercio Nuzio S. et al. Humanization interventions in general pediatric wards: a systematic review. Eur J Pediatr. (2019) 178:607–22. doi: 10.1007/s00431-019-03370-3
32. Agulles Simo P. Cooperation with Evil, the Theory of Action and the Contraception Mandate. Pers y Bioética. (2018) 22:55–68. doi: 10.5294/pebi.2018.22.1.5
33. Gómez-Cantarino S, García-Valdivieso I, Dios-Aguado M, Yáñez-Araque B, Gallego BM, Moncunill-Martínez E. Nursing perspective of the humanized care of the neonate and family: a systematic review. Children. (2021) 8:35. doi: 10.3390/children8010035
34. Yáñez-Duamante C, Oliva-Figueroa I, Catalán-Verdugo G, Moreno-Doña A. “Other” educative space and ecological knowledge: exchange and collaborative consumption trade fairs in Chile. Estud pedag.ption. (2019) 45:123–35. doi: 10.4067/S0718-07052019000100123
35. Petticrew M, Roberts H. Systematic Reviews in the Social Sciences: A Practical Guide. Oxford: Blackwell (2006). doi: 10.1002/9780470754887
36. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
37. Oviedo AD, Delgado IAV, Licona JFM. Habilidades sociales de comunicación en el cuidado humanizado de enfermería: Un diagnóstico para una intervención socioeducativa. Esc Anna Nery. (2020) 24:1–7. doi: 10.1590/2177-9465-ean-2019-0238
38. Cruz C. La naturaleza del cuidado humanizado the nature of humanized care A natureza do cuidado humanizado Escuela de Enfermería, Universidad Santo Tomás. Chile Introduccid; En el siguiente artuient se presenta una reflexiae sobre la naturaleza del cuidado ejer. Enfermerza Cuid Humaniz. (2020) 9:21–32. doi: 10.22235/ech.v9i1.2146
39. Diaz Rodríguez M, Alcántara Rubio L, Aguilar Garcia D, Puertas Cristobal E, Cano Valero M. Orientaciones formativas para un cuidado humanizado en enfermería: una revisión integrativa de la literatura. Enfermerra Glob. (2020) 19:640–72. doi: 10.6018/eglobal.392321
40. Silva A, Pantoja F, Millón Y, Hidalgo V, Stojanova J, Arancibia M, et al. Stakeholders' perceptions of humanized birth practices and obstetric violence in Chile: a scoping review. Medwave. (2020) 20:e8047. doi: 10.5867/medwave.2020.09.8047
41. Correa-Pérez L, Chavarro GA. Integralidad en la atención del paciente crítico: buscando un camino para humanizar la UCI. Acta Colomb Cuid Intensivo. (2021) 21:77–82. doi: 10.1016/j.acci.2020.04.004
42. Prieto Martínez P, Rodríguez Suárez N, Gómez Gómez L, Cárdenas Bolívar Y, Celis Rodríguez É. Percepciones de dignidad y respeto en Unidades de Cuidado Intensivo. Acta Colomb Cuid Intensivo. (2020) 20:77–85. doi: 10.1016/j.acci.2020.01.005
43. Ospina Vanegas DP, Cristancho Gómez SM, Lafaurie Villamil MM, Rubio León DC. Humanización de los servicios reproductivos desde las experiencias de las mujeres: aportes para la reflexión. Rev Cuid. (2020) 11:564–8. doi: 10.15649/cuidarte.1005
44. Pablo Monje V, Paulina Miranda C, Jéssica Oyarzún G, Fredy Seguel P, Elizabeth Flores G. Perception of humanized nursing care by hospitalized users. Cienc y Enferm. (2018) 24:1–10. doi: 10.4067/S0717-95532018000100205
45. Campiño-Valederrama SM, Duque PA, Cardozo-Arias VH. Percepción del paciente hospitalizado sobre el cuidado brindado por estudiantes de enfermería. Univ y Salud. (2019) 21:215–25. doi: 10.22267/rus.192103.158
46. Escobar Castellanos B, Cid Henriquez P. El cuidado de enfermería y la ética derivados del avance tecnológico en salud. Acta Bioeth. (2018) 24:39–46. doi: 10.4067/S1726-569X2018000100039
47. Yañez-Dabdoub M, Vargas Celus IE. Cuidado humanizado en pacientes con limitación del esfuerzo terapéutico en cuidados intensivos, desafíos para enfermería. Pers y Biosrmer. (2018) 22:55–68. doi: 10.5294/pebi.2018.21.1.5
48. Joven ZM, Guáqueta Parada SR. Percepción del paciente crítico sobre los comportamientos de cuidado humanizado de enfermería. Av en Enfermerdo. (2019) 37:65–74. doi: 10.15446/av.enferm.v37n1.65646
49. Hernández Terrazas LE, Díaz Oviedo A, Martínez Licona JF, Gaytan Hernandez D. Nursing education in humanized care. Esc Anna Nery. (2018) 22:1–5. doi: 10.1590/2177-9465-ean-2017-0275
50. Acosta Romo MF, Cabrera Bravo N, Basante Castro YDR, Jurado DM. Sentimientos que experimentan los padres en el difícil camino de la hospitalización de sus hijos prematuros. Un aporte al cuidado humanizado. Univ y Salud. (2017) 19:17. doi: 10.22267/rus.171901.65
51. Beltrán-Salazar O. Atención al detalle, un requisito para el cuidado humanizado. Index de enfermerdo. (2015) 24:49–53. doi: 10.4321/S1132-12962015000100011
52. Lopera MA. Cuidado humanizado de enfermería al final Humanized care to the patient at the end of life. Colomb Enferm. (2016) 13:16–25. doi: 10.18270/.v13i11.1898
53. Merino CMM, Zapata LF, Berrio DPM, Urrea JDA. Dehumanization during delivery: meanings and experiences of women cared for in the Medellín Public Network. Investig y Educ en Enferm. (2018) 36:e03. doi: 10.17533/udea.iee.v36n1e03
55. Rojas V. Humanización De Los Cuidados intensivos. Rev Mevens Clvensi Las Condes. (2019) 30:120–5. doi: 10.1016/j.rmclc.2019.03.005
56. García-Salido A, Heras la Calle G, Serrano González A. Narrative review of pediatric critical care humanization: where we are? Med Intensiva. (2019) 43:290–8. doi: 10.1016/j.medine.2018.01.015
57. Vialart Vidal N, Medina González I, Gavilondo Mariño X. La cultura profesional del docente de enfermería: preparación ante las tecnologías informáticas. Rev Cubana Enferm. (2018) 34:433–41.
58. Solórzano YC, Mogollón IM, Gonzalez AÁ, Guerrero JA. Humanized care in the immediate postoperative period of hysterectomized patients. Cult los Cuid. (2019) 23:360–73. doi: 10.14198/cuid.2018.54.31
59. Borges Damas L, Sixto Pérez A, Sánchez Machado R. Concepción integral del cuidado humanizado a la mujer durante el trabajo de parto y parto. Rev Cubana Enferm. (2018) 34:723–34.
60. Castañeda C, Orozco M, Rincón G. “Empoderamiento”, Una Utopía Posible Para Reconstruir La Humanización En Unidades De Cuidado Crítico. Hacia la Promocisc la Salud. (2015) 20:13–34. doi: 10.17151/hpsal.2015.20.1.2
61. Pabón-Ortíz EM, Mora-Cruz JV-D, Castiblanco-Montañez RA, Buitrago-Buitrago CY. Estrategias para fortalecer la humanización de los servicios en salud en urgencias. Rev Cienc y Cuid. (2021) 18:94–104. doi: 10.22463/17949831.2512
62. Anguita MV, Sanjuan-Quiles Á, Ríos-Risquez MI, Valenzuela-Anguita MC, Juliá-Sanchis R, Montejano-Lozoya R. Humanização dos cuidados de saúde no serviço de urgência: análise qualitativa baseada nas experiências dos enfermeiros / Humanization of healthcare at the emergency department: a qualitative analysis based on nurses' experiences / Humanización de la asistencia en urgencias: un análisis cualitativo basado en las experiencias de las enfermeras. Rev Enferm Ref. (2019) serIV:59–68. doi: 10.12707/RIV19030
Keywords: humanized care, nurse, patient, perspective, hospital, systematic review
Citation: Meneses-La-Riva ME, Suyo-Vega JA and Fernández-Bedoya VH (2021) Humanized Care From the Nurse–Patient Perspective in a Hospital Setting: A Systematic Review of Experiences Disclosed in Spanish and Portuguese Scientific Articles. Front. Public Health 9:737506. doi: 10.3389/fpubh.2021.737506
Received: 12 August 2021; Accepted: 25 October 2021;
Published: 03 December 2021.
Edited by:
Kenia Lara Silva, Federal University of Minas Gerais, BrazilReviewed by:
Maricelys Jimenez Barrera, Pontificia Universidad Católica del Ecuador, EcuadorMaría Teresa Cabanillas Chavez, Universidad Peruana Unión, Peru
Copyright © 2021 Meneses-La-Riva, Suyo-Vega and Fernández-Bedoya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Víctor Hugo Fernández-Bedoya, dmZlcm5hbmRlemJAdWN2LmVkdS5wZQ==