
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 15 December 2021
Sec. Public Health Education and Promotion
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.735902
This article is part of the Research TopicPromising Strategies for Vaccine Messages: The message and the sourceView all 6 articles
 Lovely Jain1†
Lovely Jain1† Jatina Vij1†
Jatina Vij1† Prakasini Satapathy2
Prakasini Satapathy2 Venkatesan Chakrapani3
Venkatesan Chakrapani3 Binod Patro4
Binod Patro4 Sitanshu Sekhar Kar5
Sitanshu Sekhar Kar5 Ritesh Singh6
Ritesh Singh6 Star Pala7
Star Pala7 Lalit Sankhe8
Lalit Sankhe8 Bhavesh Modi9
Bhavesh Modi9 Surya Bali10
Surya Bali10 Neeti Rustagi11
Neeti Rustagi11 Vineeth Rajagopal1
Vineeth Rajagopal1 Tanvi Kiran1
Tanvi Kiran1 Kapil Goel1*
Kapil Goel1* Arun Kumar Aggarwal1
Arun Kumar Aggarwal1 Madhu Gupta1
Madhu Gupta1 Bijaya Kumar Padhi1*
Bijaya Kumar Padhi1*Background: Students act as messengers in delivering effective messages for better uptake of health-promoting behavior. Understanding their knowledge about coronavirus disease 2019 (COVID-19), intentions to use the COVID-19 vaccine, and its associated factors will help develop promising strategies in vaccine promotion concerning the current COVID-19 pandemic.
Methods: A cross-sectional online survey was carried out among students in the healthcare and non-healthcare sectors to assess their intentions to get vaccinated against the COVID-19. A non-probability snowball sampling technique was used to recruit study participants (N = 655) through social media platforms and emails. Study participants were recruited across the country, including six major geographical regions (Eastern, Western, Northern, Southern, North-east, and Central) in India between November 2020 and January 2021 before the introduction of the COVID-19 vaccine. Descriptive statistics were used to present the sociodemographic, and vaccine-related behaviors of the study participants. Key determinants that likely predict vaccine acceptance among students were modeled using logistic regression analysis. For each analysis, p < 0.05 was considered significant.
Results: A total of 655 students were recruited, 323 from healthcare and 332 from non-healthcare sectors, to assess their intentions to receive the COVID-19 vaccine. Of the 655 students, 63.8% expressed intentions to receive the COVID-19 vaccine. The acceptance was higher among non-healthcare students (54.07 vs. 45.93%). At the time of the study, 27.8% of the students indicated that they had been exposed to a confirmed COVID-19 patient. A vast majority (93.4%) of the students knew about the COVID-19 virus, and most (89.3%) of them were aware of the development of a COVID-19 vaccine. The history of vaccine hesitancy was found to be low (17.1%). Only one-third (33.4%) of the students showed concern about contracting COVID-19. Trust in the healthcare system [adjusted odds ratio (aOR): 4.13; (95% CI: 2.83–6.04), p < 0.00] and trust in domestic vaccines [aOR: 1.46; (95% CI: 1.02–2.08), p < 0.05] emerged as the significant predictors of student's intention to get vaccinated. Higher acceptance for vaccine was observed among students in the non-healthcare [aOR: 1.982; 95% CI: 1.334–2.946, p < 0.00].
Conclusion: This study shows that the Indian college students had relatively high levels of positive intentions to receive COVID-19 vaccines, although about one-third were not sure or unwilling to receive the vaccine, highlighting possible vaccine hesitancy. Informational campaigns and other strategies to address vaccine hesitancy are needed to promote uptake of COVID-19 vaccines.
The coronavirus disease 2019 (COVID-19) pandemic has continued to affect multiple domains of human lives since its emergence at theend of 2019 (1). The increasing cases of COVID-19 had an adverse effect on all spheres of life, the economy, and the environment during the lockdown period (2). On 30 January 2020, the World Health Organization (WHO) declared an outbreak, a Public Health Emergency of International Concern (3). The COVID-19 pandemic has significantly affected the lives of college students physically, academically, financially, and psychologically (4). To prevent widespread transmission of the COVID-19 virus among college staff and the young adult population, higher-education institutions across the country have rapidly switched from in-person to online learning (5). Growing attention has been paid to vaccinate high-risk populations to control the COVID-19 pandemic. Young adults and students are critical populations for the vaccination campaign and could act as messengers in delivering effective messages for better uptake of vaccines among their families and communities (6). Students in the healthcare sector are considered to have high-risk exposures to COVID-19 and have been given priority in vaccine allocations (6). In India, the COVID-19 vaccine was introduced in a phased manner with the first phase focused on healthcare workers, frontline workers, and populations at high risk as part of concerned control measures (7). Covishield (Serum Institute of India) and Covaxin (Bharat Biotech) were the two vaccines approved for restricted emergency use (8, 9). However, at the time of the study, acceptance of these vaccines remained skeptical, with safety (10) and efficacy (11) as major concerns. Students and younger populations seemed to play an important role in determining vaccine acceptance in the community, with contrasting effects in different countries (12), but information on the same was lacking in India.
Vaccine hesitancy was a significant issue even before the COVID-19 pandemic (13). The WHO considered this phenomenon as one of the top ten threats in global health in 2019. The available evidence seems to show that the intention to get vaccinated against COVID-19 is lower among younger adults and young people (14). Younger individuals may believe that COVID-19 poses a less serious threat to themselves than to other age groups (15). To attain complete protection from the COVID-19 viruses, the vaccines need to be widely accepted by all subgroups of the populations, including youth (16). In the United States of America (USA), though it reported the highest number of confirmed cases of COVID-19 in 2020, only half of the medical students expressed willingness to participate in a vaccine trial and about 23% were hesitant to get vaccination (17). Similarly, only 35% of the medical students in Egypt (18), 45% of nursing students in Europe (19), and 52.8% of college students in New Jersey, USA, indicated their intention to receive COVID-19 vaccine (4). Although, a majority (86.1%) of the university students in Italy were willing to receive COVID-19 vaccine (20). Numerous studies reported that lack of trust in healthcare and/or health officials are common barriers to vaccination (21–23). However, there is a lack of such information from India on the prevalence of vaccination intentions and the reasons for such intentions among students in India.
Given that students could play an essential role in the global vaccination campaign by influencing the vaccination intentions of their families and communities, their perception and acceptance of COVID-19 vaccines, including factors associated with those intentions, need to be investigated. Accordingly, we conducted a study to assess the intention to receive the COVID-19 vaccine and predictors of uptake among students in India. The findings from this study could help policymakers to prioritize strategies for effective interventions to promote vaccination among college students.
A cross-sectional study was conducted among college students including healthcare and non-healthcare sectors across India. The survey was conducted between November 2020 and January 2021 during the “first wave” and before the introduction of COVID-19 vaccines in India. Students (N = 655) were recruited from an online survey via a self-reported questionnaire through social media, like WhatsApp, Facebook, and Twitter. Thus, primarily a convenient sampling technique was used. Further, the snowball sampling technique was used for enlisting additional participants, where the invited participants were requested to pass on the invitations to their peers. The minimum required sample size was estimated to be 576 with a 50% acceptance rate, 5% absolute precision, and 95% confidence level. The design effect was kept at 1.5. We recruited a total of 655 students of which 323 students were from healthcare and 332 students were from non-healthcare sectors. Participants aged 18 years or above who are currently living in India were included in the study. An online informed consent was obtained from all the participants before the survey. Only those provided the informed consent were taken to the questionnaire web page to initiate the survey.
The questionnaire was informed by a literature review of similar studies (24, 25). The survey assessed various domains, such as (1) previous immunization behaviors; (2) perception of vaccines; (3) current knowledge about COVID-19 and personal experiences about COVID-19; and (4) sociodemographic characteristics, including age, sex, marital status, educational status, family size and income, social status, religion, caste, and residence. Some of the key questions that were asked include whether “they ever refused a vaccine for themselves or a child considering it as useless or dangerous”; “if they ever postponed a vaccine recommended by the physician” for assessing the general perception toward vaccine; “before the interview if they were aware of the COVID-19 virus that is currently circulating in the community”; “Is there currently any vaccine being prepared for the pandemic Coronavirus strain”; “do you have any history of staying or traveling with confirmed COVID-19 patient”; and “how concern are you that your family member will be infected with COVID-19 virus,” for estimating the current knowledge and personal experience about COVID-19.
Descriptive analysis was conducted for socio-demographic characteristics of the responses to the survey. The age variable was categorized into three groups: 18–25, 26–35, and above 35 years. Gender was coded as a binary variable (male and female). Marital status was grouped into two categories (married and single). The educational status was categorized into three groups (postgraduate, graduate, and high school/diploma). Five response options were provided to family monthly income < INR 5,000 (about USD 71), 5,000–10,000, 11,000–20,000, 21,000–50,000, and >50,000. The geographical region of India was grouped into six categories (East, West, North, South, Central, and North-east), and the place of residence was categorized into urban vs. rural. “Yes” and “no” options were used for categorizing responses to certain questions, such as previous immunization behavior, perception of vaccines, awareness about COVID-19, and personal experience concerning COVID-19. In addition, they were asked “How concerned you are that you or someone in your family will be infected with COVID-19 virus?” and the responses were recorded in a three-point Likert scale (very concerned, somewhat concerned, and not at all concerned). “Do you have trust in the healthcare system to manage the current situation related to COVID-19?” was categorized into very likely, somewhat likely, and not at all. Bivariate analysis was conducted between all variables with the dependent variable of interest. Multiple logistic regression analysis was conducted to examine the association between the students receiving the COVID-19 vaccine with their sociodemographic and vaccination behaviors. A p < 0.05 was considered significant. Data analysis was conducted using Stata 15 software (STATA Corporation, College Station, TX, USA).
The study was approved by the Institutional Research Ethics Committee of the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India. All participants provided informed consent. Steps were taken to ensure confidentiality and privacy of the information provided by the participants, and only de-identified data were used.
A total of 655 students participated in the study, with 49.3% from healthcare sectors and 50.6% from non-healthcare sectors. Of these 655 students, 42.8 and 22.4% belonged to the Northern and Eastern parts of India, respectively. Around 43.2% were graduates, and 41.1% were postgraduate students. About half of the students were in the age group of 18–25 years (54.0%). About three-fifths (61.9%) were women and 68.5% were unmarried. A majority (79.7%) of students belonged to middle socioeconomic status, with (41.0%) reporting a family monthly income of >INR 50,000 (about USD 710) (Table 1).
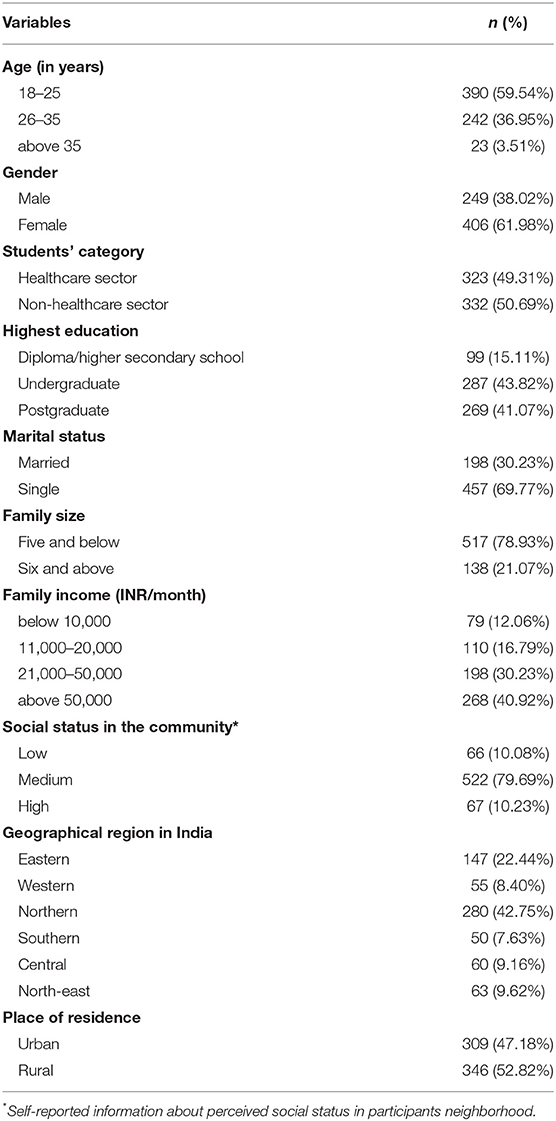
Table 1. Socio-demographic characteristics of the study participants (N = 655).
Most (93.4%) of the participants were aware that the COVID-19 virus was circulating in the community; 89.3% of the students were aware that a “COVID-19 vaccine” was being prepared. About a little less than two-thirds (64.5%) of the students reported having trust in the healthcare system of India, and a little more than half (56.0%) reported having confidence in domestic vaccines. About 27.7% of students reported having had a history of travel or contact with a confirmed COVID-19 patient. Only one-third (33.4%) of the students were concerned about contracting the COVID-19 virus. A large proportion of students (82.9%) did not have any history of vaccine hesitancy (Table 2). A majority (89.3%) of the students knew that COVID-19 vaccines were being developed, had trust in the healthcare system (64.5%) and domestic vaccines (56.0%). Only about one-third (33.4%) perceived themselves at risk of contracting Coronavirus infection (Table 2).
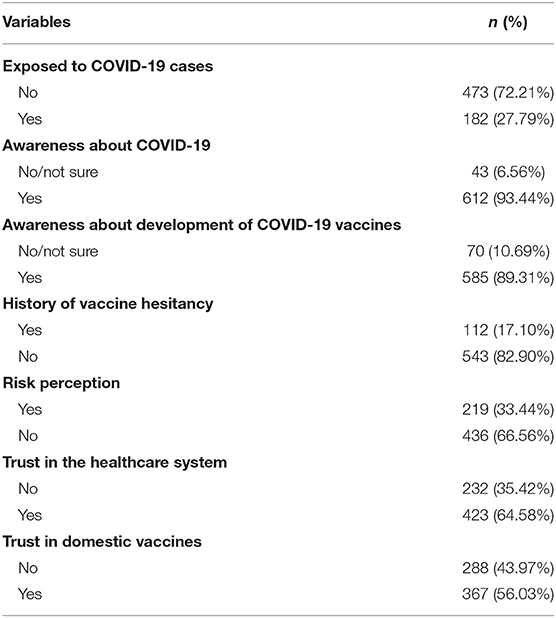
Table 2. Descriptive statistics on knowledge, risk perception, trust on the healthcare system, and perception toward domestic COVID-19 vaccine among the study participants (N = 655).
In bivariate analysis, intention to receive COVID-19 vaccine seems to be slightly higher among non-healthcare sector students than among healthcare sector students (68.1 vs. 59.4%, p = 0.02), higher among unmarried students when compared to those who were single (33.9 vs. 66.0%), and higher among postgraduate (42.8%) and undergraduate students (40.1%) when compared to diploma/higher secondary students (Table 3). Knowledge about the development of the COVID-19 vaccine, risk perception, trust in the healthcare system, and trust in the domestic vaccine was found to be independently associated with vaccine intention among students (Table 4).
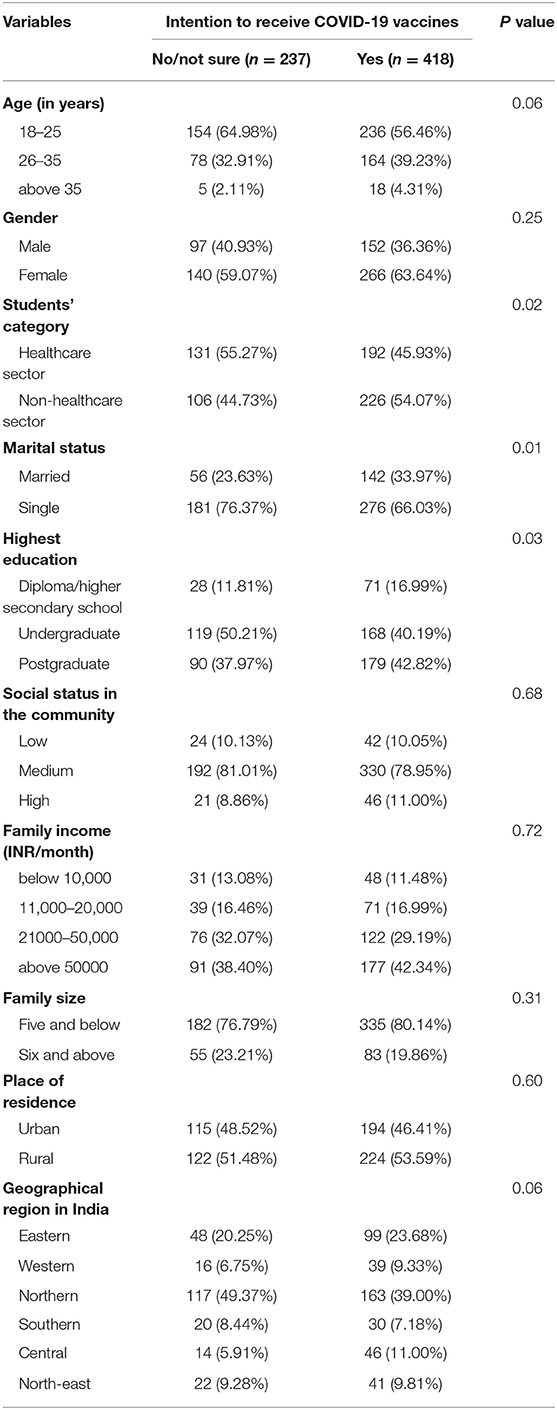
Table 3. Bivariate analysis between sociodemographics and intention to receive COVID-19 vaccines among the study participants (N = 655).
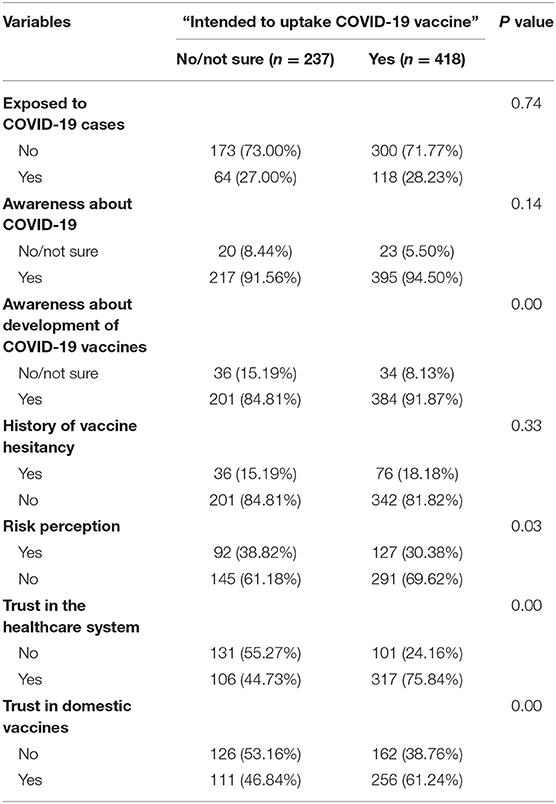
Table 4. Bivariate analysis between vaccine behavior, risk perception, and intention to receive COVID-19 vaccines among the study participants (N = 655).
Table 5 shows a multivariable logistic regression analysis of the factors influencing the COVID-19 vaccine uptake among students. We found that those who trusted the healthcare system (vs. those who did not trust) (aOR = 4.13, 95% CI: 2.83–6.04, p < 0.001), and those who had confidence in domestic vaccines (vs. those who did not have confidence) (aOR = 1.46, 95 % CI: 1.02–2.08, p = 0.03) had higher odds of reporting willingness to receive COVID-19 vaccines.
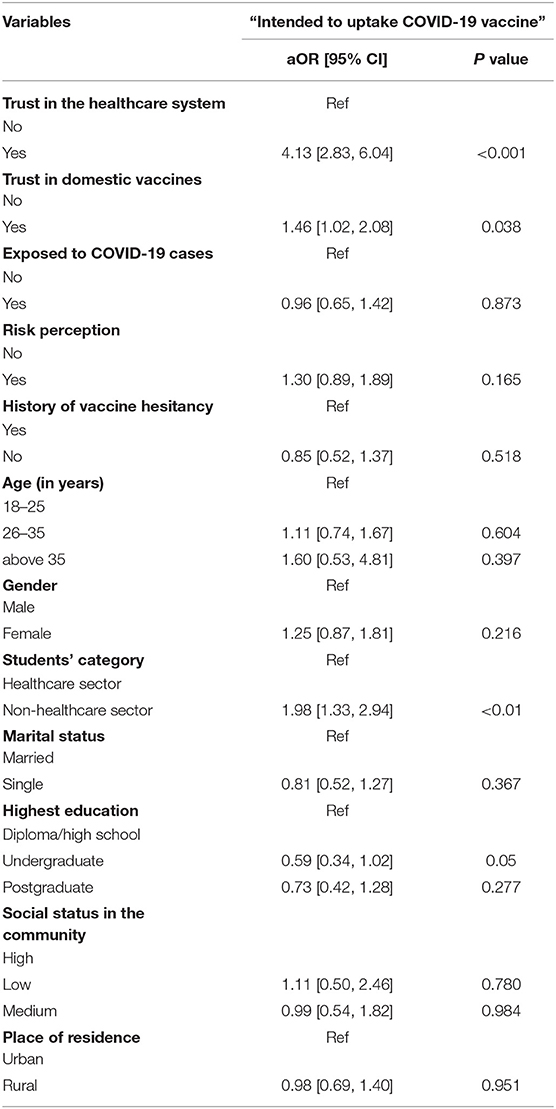
Table 5. Multivariable logistic regression analysis of the influencing factors on the COVID-19 vaccine uptake among study participants (N = 655).
Studies on COVID-19 in India have described the effect of COVID-19 on medical education (26), the relationship between COVID-19 and the suicidal tendency among healthcare professionals and students (27, 28) and COVID-19-related anxiety among students (29, 30). However, none have reported uptake of COVID-19 vaccine among students, especially those in the healthcare sector. This study is one of the first studies that examined the willingness of hypothetical vaccine for COVID-19 among students in India.
Our findings indicate a relatively good level of willingness (63.8%) among the healthcare and non-healthcare sectors to receive COVID-19 vaccines. However, the low or lack of intention to vaccinate among one-third of the sample in this study indicate vaccine hesitancy that needs to be tackled. Our findings are in line with the percentages of students (35–52.8%) who reported willingness to receive the COVID-19 vaccine in European countries and the USA (4, 18). In this study, we also found that the students in the non-healthcare sector were more willing to receive COVID-19 vaccines (54.0%) than those in the healthcare sector (45.9%). We also found that trust in the healthcare system and domestic vaccines was related to intention to receive COVID-19 vaccines. This finding of ours is similar to a survey conducted among college students in South Carolina, where 73.9% of students trust healthcare authorities, and that trust was significantly associated with COVID-19 vaccine acceptance (31). While this study found high levels of trust in domestic vaccines and their association with COVID-19 vaccine acceptance, a study conducted in China reported that imported vaccine was preferred over domestic vaccine (32). Concerning the risk perception for COVID-19 infection, in this study, the participants reported a lower risk perception of getting infected, possibly reflecting an optimism bias, our expectations (low risk of infection) are better than reality (actual risk of infection) (15, 33).
In multivariable analysis, age, gender, and education were not significantly associated with vaccine acceptance. This finding contrasts with the results of other studies conducted in Portugal (23) and Indonesia (34), where vaccine acceptance was significantly associated with education and marital status, respectively; a lower intention to be vaccinated against COVID-19 among women was also reported (35). Perceived adverse events of the COVID-19 vaccine could be a possible reason for hesitancy, as highlighted by various studies among university students and the general population (18, 31). Studies have shown that adverse events and poor vaccine efficacy could be possible reasons for vaccination hesitancy among medical students (36). Studies among other populations too have reported several reasons for hesitancy toward COVID-19 vaccines, including side-effects of the vaccine (37), speed of development of the vaccine (38), uncertainty about the effectiveness (39), and effective duration of the vaccine, and medical mistrust (40).
Students are considered as trusted influencers and ambassadors for vaccine promotion (41). Vaccine hesitancy among students, especially those in the healthcare sector, and other priority groups has potentially negative consequences to themselves and may influence vaccine acceptance among the general population (42). For example, one study reported that vaccinated healthcare providers were more likely to recommend vaccination to their patients (41).
This study has several limitations. First, being a cross-sectional study, the predictors of vaccine acceptance may not be causal and may only reflect potential associations through unknown mechanisms. However, the identified significant predictors are in line with the potential mechanisms of vaccine acceptance documented in the literature. Nevertheless, the intention to receive COVID-19 vaccines may vary over time and structural contexts. Second, the study used convenient and snowball sampling to recruit participants, and thus the results may not be generalizable to all students of healthcare and non-healthcare sectors. Third, an online self-administered questionnaire form was used instead of a face-to-face interview, with potential bias in reporting; however, studies in the health field have shown that there may not be a difference between a self-administered and interviewer-administered questionnaire (43, 44). The reasons for the refusal or low willingness to receive COVID-19 vaccines need further investigation, possibly using qualitative or mixed methods approaches. Despite these limitations, this study provides critical information on the factors that impact the acceptance of COVID-19 vaccination among college students in India. Furthermore, the data presented in this study could act as a piece of baseline information for future comparisons, i.e., how the intention to vaccinate varied over time.
In this study, we found suboptimal levels of willingness to receive COVID-19 vaccines, with nearly one-third not sure or willing to receive a vaccine, indicating high levels of potential vaccine hesitancy. Trust in the healthcare system, including vaccine safety and effectiveness, was a significant factor for COVID-19 vaccine acceptance among students. It is pertinent to design an evidence-based strategy to promote the uptake of vaccination among students, which could include informational campaigns that address vaccine hesitancy. In addition, strategies demonstrating the effectiveness and safety of the vaccine will be essential when rolling out the COVID-19 vaccination programs and those strategies will certainly have implications beyond the COVID-19 pandemic.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Institutional Research Ethics Committee of Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh, India. The patients/participants provided their written informed consent to participate in this study.
BP, LJ, MG, and AA conceptualized the study and designed the tools. BP, LJ, JV, PS, VC, BP, SK, RS, SP, SB, NR, VR, TK, KG, BM, LS, MG, and AA conducted the study at the national level and collected the data. BP and LJ analyzed the data. LJ drafted the introduction. BP drafted the methods and results. LJ and VC drafted the discussion. MG and AA provided guidance, particularly related to the strategy and recommendations. All authors reviewed drafts, provided edits, and approved the final submission.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to acknowledge the study participants for their time and contributions to the study.
COVID-19, Coronavirus disease-2019; WHO, World Health Organization.
1. Crayne MP. The traumatic impact of job loss and job search in the aftermath of COVID-19. Psychol Trauma. (2020) 12: S180–2. doi: 10.1037/tra0000852
2. Ghosh A, Nundy S, Mallick TK. How India is dealing with COVID-19 pandemic. Sensors Int. (2020) 1:100021. doi: 10.1016/j.sintl.2020.100021
3. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3. doi: 10.1038/s41586-020-2012-7
4. Kecojevic A, Basch CH, Sullivan M, Chen YT, Davi NK. COVID-19 vaccination and intention to vaccinate among a sample of college students in New Jersey. J Community Health. (2021) 46:1059–68. doi: 10.1007/s10900-021-00992-3
5. Gewin V. Five tips for moving teaching online as COVID-19 takes hold. Nature. (2020) 580:295–6. doi: 10.1038/d41586-020-00896-7
6. Qiao S, Tam CC, Li X. Risk exposures, risk perceptions, negative attitudes toward general vaccination, and COVID-19 vaccine acceptance among college students in South Carolina. medRxiv [Preprint]. (2020). doi: 10.1101/2020.11.26.20239483
7. Ministry of Health Family Welfare. Covid-19 Vacccines Operational Guidelines. Government of India (2021). Retrieved from: https://main.mohfw.gov.in/newshighlights-31 (accesesed October 10, 2021).
8. Sah R, Shrestha S, Mehta R, Sah SK, Rabaan AA, Dhama K, et al. AZD1222 (Covishield) vaccination for COVID-19: experiences, challenges, and solutions in Nepal. Travel Med Infect Dis. (2021) 40:101989. doi: 10.1016/j.tmaid.2021.101989
9. Ministry of Health Famiy Welfare. COVID-19 Vaccine Rollout. Available online at: https://www.pib.gov.in/PressReleasePage.aspx?PRID=1689180 (accessed May 24, 2021).
10. Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S, et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med. (2020) 383:2603–15. doi: 10.1056/NEJMoa2034577
11. Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, Grinsztejn B, et al. Safety and efficacy of single-dose Ad26.COV2.S vaccine against Covid-19. N Engl J Med. (2021) 384:2187–201. doi: 10.1056/NEJMoa2101544
12. Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. (2021) 27:225–8. doi: 10.1038/s41591-020-1124-9
13. Dubé E, Vivion M, MacDonald NE. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact and implications. Expert Rev Vaccines. (2015) 14:99–117. doi: 10.1586/14760584.2015.964212
14. Barnard M, George P, Perryman ML, Wolff LA. Human papillomavirus (HPV) vaccine knowledge, attitudes, and uptake in college students: Implications from the Precaution Adoption Process Model. PLoS ONE. (2017) 12:e0182266. doi: 10.1371/journal.pone.0182266
15. Wise T, Zbozinek TD, Michelini G, Hagan CC, Mobbs D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R Soc Open Sci. (2020) 7:200742. doi: 10.1098/rsos.200742
16. Schaffer DeRoo S, Pudalov NJ, Fu LY. Planning for a COVID-19 vaccination program. JAMA. (2020) 323:2458. doi: 10.1001/jama.2020.8711
17. Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health. (2021) 43:445–9. doi: 10.1093/pubmed/fdaa230
18. Saied SM, Saied EM, Kabbash IA, Abdo SAE. Vaccine hesitancy: beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J Med Virol. (2021) 93:4280–91. doi: 10.1002/jmv.26910
19. Patelarou E, Galanis P, Mechili EA, Argyriadi A, Argyriadis A, Asimakopoulou E, et al. Factors influencing nursing students' intention to accept COVID-19 vaccination: a pooled analysis of seven European countries. Nurse Educ Today. (2021) 104:105010. doi: 10.1016/j.nedt.2021.105010
20. Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. (2020) 35:781–3. doi: 10.1007/s10654-020-00670-z
21. AL-Mohaithef M, Padhi BK, Ennaceur S. Socio-demographics correlate of COVID-19 vaccine hesitancy during the second wave of COVID-19 pandemic: a cross-sectional web-based survey in Saudi Arabia. Front Public Health. (2021) 9:698106. doi: 10.3389/fpubh.2021.698106
22. Al-Mohaithef M, Padhi BK. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. J Multidiscip Healthc. (2020) 13:1657–63. doi: 10.2147/JMDH.S276771
23. Soares P, Rocha JV, Moniz M, Gama A, Laires PA, Pedro AR, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccines. (2021) 9:300. doi: 10.3390/vaccines9030300
24. Karafillakis E, Dinca I, Apfel F, Cecconi S, Wurz A, Takacs J, et al. Vaccine hesitancy among healthcare workers in Europe: a qualitative study. Vaccine. (2016) 34:5013–20. doi: 10.1016/j.vaccine.2016.08.029
25. Roberts JR, Thompson D, Rogacki B, Hale JJ, Jacobson RM, Opel DJ, et al. Vaccine hesitancy among parents of adolescents and its association with vaccine uptake. Vaccine. (2015) 33:1748–55. doi: 10.1016/j.vaccine.2015.01.068
26. Gupta S, Dabas A, Swarnim S, Mishra D. Medical education during COVID-19 associated lockdown: Faculty and students' perspective. Med J Armed Forces India. (2021) 77(Suppl. 1):S79–84. doi: 10.1016/j.mjafi.2020.12.008
27. Jahan I, Ullah I, Griffiths MD, Mamun MA. COVID-19 suicide and its causative factors among the healthcare professionals: Case study evidence from press reports. Perspect Psychiatr Care. (2021) 57:1707–11. doi: 10.1111/ppc.12739
28. Lathabhavan R, Griffiths M. First case of student suicide in India due to the COVID-19 education crisis: a brief report and preventive measures. Asian J Psychiatr. (2020) 53:102202. doi: 10.1016/j.ajp.2020.102202
29. Kochuvilayil T, Fernandez RS, Moxham LJ, Lord H, Alomari A, Hunt L, et al. COVID-19: Knowledge, anxiety, academic concerns and preventative behaviours among Australian and Indian undergraduate nursing students: a cross-sectional study. J Clin Nurs. (2021) 30:882891. doi: 10.1111/jocn.15634
30. Hazarika M, Das S, Bhandari SS, Sharma P. The psychological impact of the COVID-19 pandemic and associated risk factors during the initial stage among the general population in India. Open J Psychiatry Allied Sci. (2021) 12:31–5. doi: 10.5958/2394-2061.2021.00009.4
31. Qiao S, Friedman DB, Tam CC, Zeng C, Li X. Vaccine acceptance among college students in South Carolina: do information sources and trust in information make a difference? medRxiv [Preprint]. (2020). doi: 10.1101/2020.12.02.20242982
32. Dong D, Xu RH, Wong EL, Hung C, Feng D, Feng Z, et al. Public preference for COVID-19 vaccines in China: a discrete choice experiment. Heal Expect. (2020) 23:1543–78. doi: 10.1111/hex.13140
34. Faturohman T, Kengsiswoyo GAN, Harapan H, Zailani S, Rahadi RA, Arief NN. Factors influencing COVID-19 vaccine acceptance in Indonesia: an adoption of technology acceptance model. F1000Research. (2021) 10:476. doi: 10.12688/f1000research.53506.1
35. Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. Lancet Reg Health Eur. (2021) 1:100012. doi: 10.1016/j.lanepe.2020.100012
36. Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. (2021) 397:99–111. doi: 10.1016/S0140-6736(20)32661-1
37. Riad A, Pokorná A, Attia S, Klugarová J, Koščík M, Klugar M. Prevalence of COVID-19 vaccine side effects among healthcare workers in the Czech Republic. J Clin Med. (2021) 10:1428. doi: 10.3390/jcm10071428
38. Callaway E. The race for coronavirus vaccines: a graphical guide. Nature. (2020) 580:576–7. doi: 10.1038/d41586-020-01221-y
39. Wagner AL, Huang Z, Ren J, Laffoon M, Ji M, Pinckney LC, et al. Vaccine hesitancy and concerns about vaccine safety and effectiveness in Shanghai, China. Am J Prev Med. (2021) 60(1 Suppl. 1):S77–86. doi: 10.1016/j.amepre.2020.09.003
40. Thiagarajan K. Covid-19: India is at centre of global vaccine manufacturing, but opacity threatens public trust. BMJ. (2021) 372:n196. doi: 10.1136/bmj.n196
41. Paterson P, Meurice F, Stanberry LR, Glismann S, Rosenthal SL, Larson HJ. Vaccine hesitancy and healthcare providers. Vaccine. (2016) 34:6700–6. doi: 10.1016/j.vaccine.2016.10.042
42. World Health Organization. Covid-19 Weekly Epidemiological Update. (2021). Retrieved from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19 (accesesed June 1, 2021).
43. Lozano F, Lobos JM, March JR, Carrasco E, Barros MB, González-Porras JR. Self-administered versus interview-based questionnaires among patients with intermittent claudication: do they give different results? A cross-sectional study.Med J. (2016) 134:63–9. doi: 10.1590/1516-3180.2015.01733009
Keywords: COVID-19, students, vaccine hesitancy, vaccine uptake, vaccine intention, first wave
Citation: Jain L, Vij J, Satapathy P, Chakrapani V, Patro B, Kar SS, Singh R, Pala S, Sankhe L, Modi B, Bali S, Rustagi N, Rajagopal V, Kiran T, Goel K, Aggarwal AK, Gupta M and Padhi BK (2021) Factors Influencing COVID-19 Vaccination Intentions Among College Students: A Cross-Sectional Study in India. Front. Public Health 9:735902. doi: 10.3389/fpubh.2021.735902
Received: 03 July 2021; Accepted: 11 November 2021;
Published: 15 December 2021.
Edited by:
Bridget Kelly, RTI International, United StatesReviewed by:
Larry Kenith Olsen, Logan University, United StatesCopyright © 2021 Jain, Vij, Satapathy, Chakrapani, Patro, Kar, Singh, Pala, Sankhe, Modi, Bali, Rustagi, Rajagopal, Kiran, Goel, Aggarwal, Gupta and Padhi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bijaya Kumar Padhi, YmtwYWRoaUBnbWFpbC5jb20=; Kapil Goel, ZHJrYXBpbDEyQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.