 Hujie Wang1*
Hujie Wang1* Martina Buljac-Samardzic1
Martina Buljac-Samardzic1 Wenxing Wang1
Wenxing Wang1 Jeroen van Wijngaarden1
Jeroen van Wijngaarden1 Shasha Yuan2
Shasha Yuan2 Joris van de Klundert1,3
Joris van de Klundert1,3- 1Erasmus School of Health Policy and Management, Erasmus University Rotterdam, Rotterdam, Netherlands
- 2Institute of Medical Information and Library, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
- 3Prince Mohammad Bin Salman College of Business and Entrepreneurship, King Abdullah Economic City, Saudi Arabia
Background and Objective: Improving quality of care is one of the primary goals in current Chinese hospital reforms. Teamwork can play an essential role. Characteristics of teamwork and interventions for improving teamwork in hospitals have been widely studied. However, most of these studies are from a Western context; evidence from China is scarce. Because of the contextual differences between China and Western countries, empirical evidence on teamwork from Western hospitals may have limited validity in China. This systematic review aims to advance the evidence base and understanding of teamwork in Chinese hospitals.
Methods: Both English (i.e., Embase, Medline, and Web of Science) and Chinese databases (i.e., CNKI, CQVIP, and Wanfang) were searched for relevant articles until February 6, 2020. We included the studies that empirically researched teamwork in Chinese hospitals. Studies were excluded if they (1) were not conducted in hospitals in Mainland China, (2) did not research teamwork on team interventions, (3) were not empirical, (4) were not written in English or Chinese, (5) were not published in peer-reviewed journals, and (6) were not conducted in teams that provide direct patient care. Both deductive and inductive approaches were used to analyze data. The Mixed Methods Appraisal Tool (MMAT) was used to assess their methodological quality.
Results: A total of 70 articles (i.e., 39 English articles and 31 Chinese articles) were included. The results are presented in two main categories: Teamwork components and Team interventions. The evidence regarding the relationships among inputs, processes, and outcomes is scarce and mostly inconclusive. The only conclusive evidence shows that females perceive better team processes than males. Similar types of training and tools were introduced as can be found in Western literature, all showing positive effects. In line with the Chinese health reforms, many of the intervention studies regard the introduction of multidisciplinary teams (MDTs). The evidence on the implementation of MDTs reveals that they have led to lower complication rates, shorter hospital stays, higher diagnosis accuracy, efficiency improvement, and a variety of better disease-specific clinical outcomes. Evidence on the effect on patient survival is inconclusive.
Conclusion: The Chinese studies on teamwork components mainly focus on the input-process relationship. The evidence provided on this relationship is, however, mostly inconclusive. The intervention studies in Chinese hospitals predominantly focus on patient outcomes rather than organizational and employee outcomes. The introduction of training, tools, and MDTs generally shows promising results. The evidence from primary hospitals and rural areas, which are prioritized in the health reforms, is especially scarce. Advancing the evidence base on teamwork, especially in primary hospitals and rural areas, is needed and can inform policy and management to promote the health reform implementation.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020175069, identifier CRD42020175069.
Introduction
Improving the quality of hospital care has been one of the primary goals of the Chinese national health reforms since 2009 (1). In recent years, the Chinese government has been making efforts to explore strategies to reach this goal. In Western countries, facilitating interdisciplinary communication, collaboration, and teamwork are emphasized in many quality improvement strategies for hospital care (2, 3). The World Bank and the World Health Organization have also recommended China to enhance teamwork within medical teams of hospitals as a managerial practice to promote the delivery of high-quality hospital care (4). However, a systematic scientific understanding of teamwork and its relationship to the quality of hospital care in China is lacking.
Teamwork significantly impacts the quality and safety of care. Failure in teamwork can result in (preventable) medical errors and adverse events (5–8), while improving teamwork is beneficial for the quality of care (9, 10). Numerous literature reviews have considered teamwork and the improvement of teamwork in hospitals (11–14). Some reviews focus on characteristics that are important for teamwork and team performance. For instance, Mickan and Rodger summarize the characteristics of an effective team in hospitals (e.g., suitable leadership, trust, coordination, and communication) and suggest finding a balance between organizational structure and team processes (11). Lemieux-Charles and McGuire have developed an Integrated (Health Care) Team Effectiveness Model (ITEM), showing the relation between team characteristics, team processes, psycho-social traits, and team performance (12). Other reviews focus on interventions to improve teamwork in hospitals. For example, Buljac-Samardzic et al. present an overview of team interventions (i.e., training, tools, (re)design, and program) to improve team effectiveness (13), and Hughes et al. show a positive impact of team training on trainees' reactions to training, learning outcomes, behaviors, and organizational and patient outcomes (14). A solid body of evidence on teamwork in hospitals exists. With few exceptions, however, the studies included in these reviews are from Western countries. For example, only one study from Buljac-Samardzic et al. (13) review is conducted in Mainland China.
Cultural differences between China and Western countries may influence people's behaviors in a team. For instance, Chinese people emphasize collectivism and are more likely to avoid conflict to preserve harmony within their teams, while people from Western countries prefer individualistic values and are prone to debate with their teammates when disagreement emerges (15, 16). Tjosvold et al. (17) provide empirical evidence showing that collectivism has a positive effect on constructive controversy, which in turn positively influences the performance of teams in Chinese factories. Hui et al. (18) provide evidence of the positive relationship between collectivism and team performance. These examples suggest that teams in Chinese hospitals function differently from those in Western hospitals, which may subsequently translate into differences regarding characteristics of teamwork and the effectiveness of interventions. In other words, the empirical evidence on teamwork from Western hospital settings may have limited validity in a Chinese setting. With the aim to advance the scientific evidence base and understanding of teamwork in Chinese hospitals, we conducted a systematic review to address the following research question: What is the present empirically based knowledge on teamwork in Chinese hospitals?
Methodology
This systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (19, 20). The review protocol was registered in PROSPERO (No. CRD42020175069).
Search Strategy
English and Chinese databases were searched for published articles, not restraining the year of publication. A medical librarian from the Erasmus Medical Center developed the English query, which consisted of keywords that combined three areas: (1) teamwork or team interventions (e.g., teamwork, team performance, team effectiveness, multidisciplinary team, and team training); (2) hospital setting (e.g., hospital and healthcare); and (3) China (i.e., China, Chinese, and the names of the 31 administrative regions in Mainland China). This query was searched in Embase, Medline and Web of Science on February 6, 2020. A Chinese medical librarian assisted in translating the English query and finalizing the Chinese query (both the English and Chinese queries are shown in Supplementary File 1). The Chinese databases CNKI, CQVIP, and Wanfang were searched for articles until February 6, 2020. Finally, 1,533 records were retrieved after all the duplicates deleted: 996 from English databases and 537 from Chinese databases.
Inclusion and Exclusion Criteria
Based on the research question, we aimed at including studies that empirically researched teamwork in Chinese hospitals. The following exclusion criteria were established: (1) studies that were not conducted in hospitals located in Mainland China; (2) studies that do not provide information about teamwork or team interventions; (3) non-empirical studies, such as editorial letters and literature reviews; (4) articles that are not written in English or Chinese; (5) articles that are not published in peer-reviewed journals, such as conference papers and dissertations; and (6) studies conducted in departments that do not provide direct patient care, such as pharmacy, laboratory, administration, logistics and information technology.
Selection Process
There were two stages of selecting articles. Each stage consisted of an English and a Chinese part. Firstly, the titles and abstracts retrieved from both the English and Chinese databases were independently screened by two researchers according to the above-mentioned exclusion criteria. In case of disagreement between the two researchers, consensus would be reached through discussion. In case of any doubt, it was transferred to the second stage. This first stage resulted in a selection of 363 articles (from the 1,533): 264 from English databases and 99 from Chinese databases. Surprisingly, 123 out of the 264 articles with English titles and abstracts are actually written in Chinese. Hence, the numbers of articles written in English and Chinese were adjusted to 141 and 222, respectively. Secondly, the full texts of the 363 articles were independently reviewed by the same researchers of the first stage. In case of disagreement, a third researcher would settle it. Finally, 70 articles (i.e., 39 English articles and 31 Chinese articles) were included for data synthesis. Figure 1 shows the screening and reviewing process based on the PRISMA Flow Diagram (20).
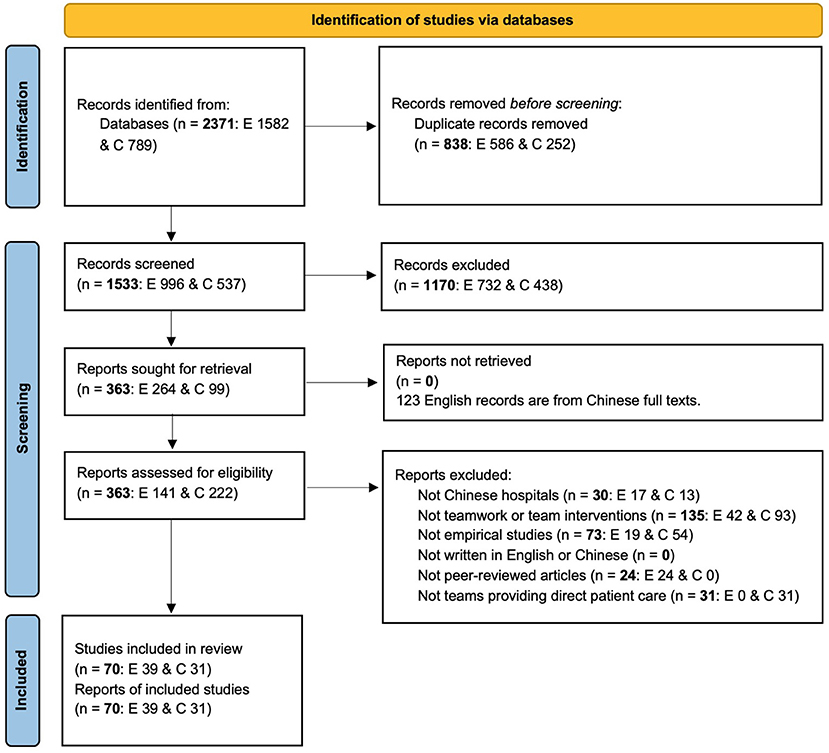
Figure 1. PRISMA flow diagram. E, English; C, Chinese.
Data Synthesis
The conducted analysis combined deductive and inductive elements and consisted of four steps.
As a first step, we extracted data from the included articles in terms of author (year), research aim, setting, administrative regions, research methods, time period, main focus of teams considered, team interventions considered (if any), findings related to teamwork (if any), other findings, potentially relevant information from the discussion section, interpretation specifically relevant to the Chinese context, and conclusion. These data fields were selected to systematically extract all information relevant to our research question. In this step, the data from the Chinese articles were translated into English.
The second step combined deductive and inductive approaches to create primary result categories (21). The classical (Western) reviews (12, 13, 22, 23) served as deductive starting points for the categorization process. We used the categories of the ITEM model, which describes team inputs, processes, and outcomes in health care, as well as their interrelations (12). In addition, we included categories identified by systematic reviews on teamwork components (i.e., inputs, processes, and outcomes) in intensive care and chronic care (22, 23).
Combining the categorization in these reviews (deduction) with an initial inductive analysis of the data collected, we identified the input element “team composition” as a first primary category and added articles that research the composition of teams in hospitals to this primary category.
Buljac-Samardzic et al. summarize the interventions implemented in health care teams and categorize the interventions as training, tools, (re)design, and program (13). The second primary category “team interventions” was established based on this review and consisted of articles reporting on interventions on teams in hospitals.
Two additional primary categories were inductively formed to classify the remaining articles. The category “describing teamwork” included descriptive studies reporting on teamwork via questionnaires, interviews, or both. The category “the influence of teamwork on performance” consisted of articles addressing the influence of teamwork on team performances.
In the third step, these primary categories were repeatedly adjusted based on discussions among all authors. The category “team interventions” remained unchanged, while “team composition” was divided into two parts. The first part was composed of studies that actually examine the relationship between the three teamwork components (i.e., inputs, processes, and outcomes) (12, 22, 23). Articles in the primary categories “describing teamwork” and “the influence of teamwork on performance” also research the three teamwork components and the relationships between them. Therefore, these two primary categories were merged with the first “team composition” category, forming a new category “teamwork components” (see also 12, 22, 23). The second part of “team composition” consisted of studies that research interventions on team composition (i.e., (re)design and program) and was added to the category “team interventions.” These adjustments resulted in the two final categories “teamwork components” and “team interventions.”
In step four, the two categories were further divided into several subcategories according to the theoretical frameworks and reviews mentioned above (12, 13, 22, 23). The first category “teamwork components” was divided into processes, relationship between inputs and processes, relationship between inputs and outcomes, and relationship between processes and outcomes based on the teamwork theoretical models (12, 22, 23). The second category “team interventions” included training, tools, (re)design and program, in accordance with the categorization of Buljac-Samardzic et al. (13) review. Table 1 shows the categorization of results and the number of articles per category and subcategory.
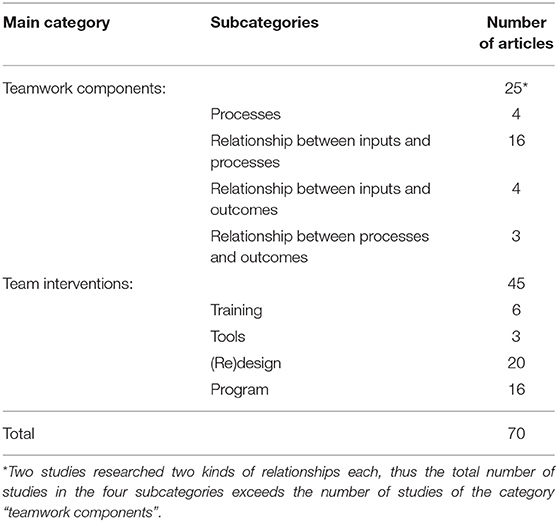
Table 1. Categorization of results.
Quality Assessment
The Mixed Methods Appraisal Tool (MMAT) was used to assess the methodological quality of the included studies (24). The quality score of a study, ranging from 0 to 5, was the number of criteria a study met. All the studies were divided into high quality (scoring 4 or 5) and low quality (scoring 3 or less) studies (25).
Results
Overall Findings
Most studies in the first category address relationships across the three components of the input-process-outcome framework. The second category describes the specific interventions implemented and their effects on outcomes. More than 70% of the studies were conducted in tertiary hospitals. With one exception, all studies were situated in urban hospitals. In the following paragraphs, we summarize the main findings of the review. Supplementary Tables 1, 2 provide a complete overview of the results.
Based on the MMAT scores, the majority of the studies (60 out of 70 studies) are of high methodological quality, while the other ten studies are of low quality in the research design. The quality of research design of each study is also shown in both Supplementary Tables 1, 2.
Teamwork Components
Processes
Collaboration is one of the process elements of the ITEM model (12) and, two out of the four studies in this subcategory focus on collaboration (26, 27). Sharing the same goal is one of the strategies that facilitate the collaboration within a team (26), while lack of common ground is a barrier to the collaboration between healthcare professionals (27). The other two studies measure team processes with two well-known patient safety culture questionnaires: the Hospital Survey on Patient Safety Culture (HSOPSC) (i.e., “teamwork within units,” “teamwork across units,” and “communication openness”) and the Safety Attitudes Questionnaire (SAQ) (i.e., “teamwork climate”) (28–31). One of these two studies compare results between Chinese and US hospitals, showing significantly higher scores of “teamwork within units” and “teamwork across units” but significantly lower scores of “communication openness” in the Chinese hospital (29).
Relationship Between Inputs and Processes
Sixteen studies explore the relationship between inputs and processes (32–47). The majority of the articles in this subcategory are based on HSOPSC and SAQ (10 out of 16) (33, 35–37, 39, 40, 42, 44–46). The input “gender” is found to influence team processes. Female staff perceive significantly better “communication openness” (42), “teamwork within units” (46), and “teamwork climate” (45) than male staff. The relationship between the input “profession” and team processes is inconclusive, although profession is researched the most in these studies. Two HSOPSC studies show that nurses score “communication openness” significantly higher than doctors (37, 42), while two other HSOPSC studies find no significant differences between the ratings of doctors and nurses (36, 46). Two SAQ studies find that doctors evaluate “teamwork climate” significantly more positively than nurses (35, 45).
Mixed results are also found in terms of education level and age. Staff with a degree higher than bachelor score “communication openness” (42) and “teamwork across units” (46) significantly higher but “teamwork climate” significantly lower than those with an education level lower than bachelor (35, 45). Staff younger than 25 years report significantly higher scores for “teamwork climate” than those older than 50 years in one study (45) but the opposite is found in another study (35). Besides, two HSOPSC studies compare the results between China and the US without testing significance, showing that overall Chinese healthcare professionals score higher in the three process related composites than their counterparts in the US (37, 42), except for “teamwork across units” in one study (42).
Five out of the six remaining studies investigate the input-process relationship via other questionnaires (32, 34, 38, 41, 47). Similar to the findings of the previous HSOPSC and SAQ studies, female doctors perceive significantly better team interaction (e.g., communication, coordination, and mutual help) than male doctors (47). Profession, department, and age also influence healthcare professionals' ratings on team processes. The overall teamwork scores of internal medicine nurses are significantly lower than those of surgical nurses (34, 38). However, internal medicine doctors score team interaction significantly higher than surgeons (47). Staff younger than 30 years perceive better overall teamwork than those older than 30 years in one study (38) but score team cohesion significantly lower than those between 40 and 50 years old in another study (41). In addition, cultural values are considered to affect team processes (43). Feminine traits (e.g., friendship, enthusiasm, and patience) are shown to be beneficial to communication; collectivism facilitates the mutual support, while a clique culture hinders it.
Relationship Between Inputs and Outcomes
Four studies examine the correlation between inputs and outcomes (48–51). Disciplinary diversity shows positive effects on team performance (i.e., the number of team consultations) (50). Tenure and team size are found to influence team outcomes. Staff working between 16 and 30 years perceive significantly worse job satisfaction than other staff (49), while nurses working more than 20 years report significantly more adverse events than those working less than 20 years (51). Adding additional members to a stable surgical team increases the surgical procedure time (48).
Relationship Between Processes and Outcomes
Three studies investigate the process-outcome relationship (47, 51, 52). Teamwork is a positive predictor to nurses' adverse events reporting (51) but is negatively related to nurses' willingness to make plans for their retirement (52). All the six factors of team interaction (i.e., communication, coordination, mutual help, team goals, work norms, and cohesion and conflict resolution) are inversely related to physicians' burn-out (47).
Team Interventions
Training
Training as a team intervention focuses on enhancing inputs and team processes, consequently resulting in improved outcomes. Most studies on training evaluate simulation-based training. Simulation, the core of simulation-based training, refers to “a technique to replace or amplify real-patient experiences with guided experiences, artificially contrived, that evokes or replicates substantial aspects of the real world in a fully interactive manner” (53). All the five studies on simulation-based training are conducted in emergency settings (e.g., trauma care, pediatric septic shock, cardiac surgeries, and advanced cardiac life support) (54–58). The forms of simulated scenarios include mannequins (55), simulators (56), and animals (58). Two studies find the inputs (e.g., surgical skills and emergency skills) significantly improved after the training (57, 58), while two other studies observe significantly better outcomes (e.g., task complete compliance and work efficiency) in the simulation group, compared to the non-simulation group (56) or pre-intervention group (54). One study concludes that licensed perfusionists score communication and coordination higher than the trainees in a cardiac surgery simulation scenario, without testing significance (55). In addition to the studies on simulation-based training, there is one study on TeamSTEPPS (i.e., Team Strategies and Tools to Enhance Performance and Patient Safety). TeamSTEPPS is a training system aiming at improving healthcare professionals' teamwork and communication skills (inputs), facilitating information sharing, resolving conflicts (processes), and finally providing better patient care (outcomes) (59). This study on TeamSTEPPS presents descriptive results that more healthcare professionals rate their communication skills as good after the training (60).
Tools
Tools in this subcategory refer to SBAR (i.e., Situation-Background-Assessment-Recommendation tool) and checklists, both aiming at optimizing the team processes. SBAR is a structured template used to facilitate the communication between team members (61). Two studies have evaluated SBAR and show significantly better patients' and healthcare professionals' satisfaction, and a significant decrease in the incidence of adverse events (62, 63). Moreover, one of these two studies also shows higher work efficiency (62). A checklist is a list of actions to be done in a hospital setting, with the goal of avoiding any steps being forgotten (64). Yuan et al. (65) have implemented a self-developed electronic checklist for multidisciplinary team meetings and report significantly higher working efficiency and diagnosis accuracy and lower hospital stay but no significant change in terms of the incidence of complications.
(Re)Design
(Re)design is defined as constructing or revising the input characteristics and/or the processes of a medical team within hospitals.
Multidisciplinary teams (MDTs) are the main focus of most studies in this subcategory (18 out of 20 studies) (66–83). An MDT is a team consisting of healthcare professionals from different disciplines that work together to provide better patient care (84). Five studies describe or evaluate the effects of establishing MDTs (revising the inputs) in cancer (66, 67, 80), trauma (82), and stroke care (78). Significantly higher diagnosis accuracy and lower incidence of complications and hospital stay are reported in these studies (66, 80, 82). Eight studies implement MDTs with clarified roles and responsibilities of team members (defining the inputs) (69–73, 75, 77, 81), which results in significantly higher quality of life and patients' satisfaction and lower incidence of complications. The other five studies on MDT consider the standardization and optimization of the working procedures of MDTs (optimizing team processes) through a pathway of care (79), a new procedure (68, 76, 83) or re-organizing multidisciplinary meetings (74). The results of these studies are significantly higher overall survival rate, shorter hospital stay, less complications, and better disease-specific clinical outcomes. In addition to the outcomes reported above, two studies present mixed results regarding hospitalization costs (68, 76), and two other studies find no significant changes in mortality rate (76, 82). Moreover, four out of the eighteen studies only summarize the outcomes after the (re)design, without controls (70, 71, 78, 83).
Of the remaining two studies, one clarifies roles and responsibilities of a non-MDT (85) and reports significantly higher nursing quality and patients' satisfaction. The other study optimizes the working procedures of medical teams via a novel team performance appraisal system (86). Per capita performance and healthcare professionals' satisfaction are significantly higher, but the overall patients' satisfaction is significantly lower in the experiment group compared to those in the control group.
Program
A fixed component of programs is (re)design, which is combined with training, a tool, or both. MDTs are also involved in 7 out of the 16 studies on program (87–93). Nine studies combine (re)design with training on technical skills (inputs) (87–89, 94–99). The outcomes are significantly higher patients' satisfaction, nursing quality, and working efficiency, and lower incidence of medical errors. Notable, two studies show lower incidence of complications and higher work efficiency, without testing significance (97, 99). Four studies evaluate programs that combine (re)design with rounds (90–93), a structured tool referring to a group of healthcare professionals meeting around a patient to discuss the patient's condition (13). Three out of these four studies present significantly lower incidence of complication and hospital stay and decreased depression scores (90–92), while one study only summarizes the results (93). Lastly, three studies introduce programs in which all the three types of interventions are combined for postoperative care (100, 101) or cancer pain care (102). One study reports a reduction in complications and no significant change in recovery time (100). Another study shows significant pain reduction (102), while the third study reports a sustainable significantly increase in the teamwork score (101).
Discussion
This systematic review presents an overview of research on teamwork in Chinese hospitals. We first summarize the findings of the relationships among the three teamwork components (i.e., inputs, processes, and outcomes) and then list the evidence on interventions to improve teamwork and achieve better team outcomes. As more than 70% of the studies were conducted in tertiary hospitals and nearly all the studied hospitals are in urban areas, the evidence base on primary and secondary hospitals and hospitals in rural areas is very limited.
More than half of the studies that research teamwork components focus on the relationship between inputs (e.g., age, gender, profession, education level, and department) and processes (e.g., teamwork within units, teamwork across units, and teamwork climate). This relationship has received little attention in Western literature so far (12, 103).
Despite the relatively large number of studies on the input-process relationship included in our review, the evidence synthesis is inhibited by the heterogeneity of variables used, the mixed results, and the primary research goals that are not focused on this relationship. The only conclusive evidence that can be synthesized from the review findings is that females perceived better team processes (i.e., communication openness, teamwork within units, teamwork climate, and team interaction) than males. This may be explained by the differences in personality traits between females and males. Females have been reported to be more agreeable than males, which means that females are more willing to cooperate and maintain harmony (104, 105). The evidence on the relationships between other inputs and processes is inconclusive.
Six studies research the input-outcome relationships, process-outcome relationships, or both (47–52). These studies, however, focus on different input, process, and outcome variables, which makes it difficult to synthesize the results across studies. One study shows a positive correlation between disciplinary diversity (input) and the number of team consultations (outcome) (50). Another study shows that better team interaction as a process variable (e.g., communication, coordination, and cohesion) is associated with less burn-out (outcome), suggesting a positive influence of team interaction on team performance (47). These results are in line with Lemieux-Charles and McGuire's review that most of the inputs (e.g., disciplinary diversity) and processes (e.g., communication, coordination, and cohesion) have positive correlations with team outcomes (12). Altogether, however, the evidence on the input-outcome and process-outcome relationships is still scarce. More studies are needed to strengthen the evidence on the relationships of outcomes with processes and inputs.
The studied trainings and tools correspond to those mentioned in Western literature (13). The three studies on efficiency all present evidence of improvement (54, 56, 62). Moreover, two studies on SBAR report higher patients' satisfaction (62, 63), and two studies report improved technical skills as an effect of training (57, 58). These results are in line with the findings of Buljac-Samardzic et al. (13) that most trainings and tools result in improvements in team performance. However, the evidence base on training and tools identified in our review is still small.
As was the case for the studies on team components, many team intervention studies regard multidisciplinary teams. The World Bank and the World Health Organization have recommended forming MDTs to promote people-centered integrated care and the quality of care, both of which play important roles in the Chinese health reforms (4). Correspondingly, there has been much research emphasis on MDT implementation in Chinese hospitals, which contrasts with the findings of Buljac-Samardzic et al. (13) review on team interventions. We find consistent evidence that MDTs are associated with reduced complication rates and length of hospital stays, and improved efficiency and diagnostic accuracy (66, 75–77, 79, 88–91). Nine of the MDT studies present better disease-specific clinical outcomes for different conditions (67–69, 73, 75, 80, 81, 87, 92). These findings support the positive effects of MDTs, which is in line with the findings of Western MDT studies (106, 107).
The evidence on the effects of MDT implementation on survival is inconclusive. Three studies report higher survival rates (67, 74, 80), while two other studies find no significant change in mortality rates after MDT implementation (76, 82). This inconclusive finding may be explained by the different severity, treatment, and prognosis of the diseases researched in these studies.
Kirkpatrick (108) divides the team training evaluation into four levels: reactions (e.g., people's reactions and feedbacks to the intervention), learning (e.g., knowledge and skills learnt), behavior (e.g., participants' behavioral change at work), and results (e.g., patient outcomes and organizational outcomes). Based on these four levels, the majority of the included intervention studies in our review focus on patient outcomes which belong to the fourth level (i.e., results). However, studies in Western reviews commonly regard the first three levels (i.e., reactions, learning, and behavior) and organizational outcomes which are a part of the fourth level (13). This difference may be due to the different research aims of Chinese and Western studies and different research interests of researchers from China and Western countries.
Advocating harmony and collectivism are typical Chinese cultural values, which differ from Western countries (15, 16). Three studies comparing the results between China and the US show higher scores on “teamwork within units” in Chinese hospitals but mixed results on “teamwork across units” and “communication openness” (29, 37, 42), proposing the value attached to the harmony in the Chinese culture as an explanation. Another Chinese cultural trait, collectivism, is reported to promote mutual support (43). These findings and inferences form first evidence on teamwork in China in relation to cultural differences with Western countries.
Limitation
This review has several limitations. Firstly, books and gray literature were not included. Secondly, the translation of the query from English to Chinese may have led to missing results in Chinese databases. With the assistance of a Chinese librarian, the two queries have been made as equivalent as possible. Thirdly, because of publication bias, intervention studies which have not produced desired results may have been underreported. Finally, although we assessed the methodological quality, the included studies are heterogenous, making it difficult to synthesize the evidence. This limits the certainty of evidence of our findings.
Implications for Future Research
Firstly, patient outcomes have been predominant in the teamwork research in China, while important team outcomes such as healthcare professionals' satisfaction and well-being have received little attention. The team outcomes deserve future research to advance the evidence base on team performance, as is conducive to designing, selecting, and assessing team interventions.
Secondly, the evidence base on the relationships among the three teamwork components deserves strengthening. The included studies seldomly aim to investigate these relationships, causing the evidence on the relationships among inputs, processes, and outcomes to be largely inconclusive. More appropriately designed studies addressing these relationships are called for, as they will also promote the understanding of interventions on inputs (e.g., the introduction of MDTs) related to processes and subsequently to organizational outcomes and patient outcomes.
Lastly, it is important to recognize that China is a large country with considerably variety across provinces (109). The impact of this variety of contexts (e.g., different cultures) on teamwork and team performance is largely unexplored. Most studies are from tertiary hospitals in urban China. Due to the contextual differences, it cannot be assumed that this evidence has validity in lower-level hospitals and rural areas. In view of the priority attached to improving primary care and rural healthcare in the Chinese health reforms (110), valid evidence for primary hospitals and rural China is urgently called for.
Conclusion
The Chinese studies on teamwork components mainly focus on the input-process relationship. The evidence provided on this relationship is, however, mostly inconclusive. The intervention studies in Chinese hospitals predominantly focus on patient outcomes rather than organizational and employee outcomes. The introduction of training, tools, and MDTs generally shows promising results. The evidence from primary hospitals and rural areas, which are prioritized in the health reforms, is especially scarce. Advancing the evidence base on teamwork, especially in primary hospitals and rural areas, is needed and can inform policy and management to promote the health reform implementation.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author Contributions
SY provided support in finalizing the Chinese search query. HW and MB-S screened the English titles and abstracts. HW and WW screened the Chinese titles and abstracts. HW, MB-S, and JK reviewed the English full texts. HW, WW, and SY reviewed the Chinese full texts. HW, MB-S, JW, and JK analyzed the data and categorized the results together. HW initiated the draft of the manuscript and revised it based on the inputs of MB-S, JW, and JK. All authors read and approved the final manuscript.
Funding
This work was supported by China Scholarship Council (No. 201906160092; receiver: HW). This funder has no role in the study design, data collection and analysis, interpretation of data, and writing the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the librarian Wichor Bramer from Erasmus Medical Center, Erasmus University Rotterdam for his support in searching in English databases for this systematic review. We also thank the librarian Gusta Drenthe from Erasmus University Rotterdam for her suggestions on finding full texts.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2021.735754/full#supplementary-material
Supplementary File 1. English and Chinese search queries.
Supplementary File 2. PRISMA 2020 checklist.
Supplementary File 3. PRISMA 2020 abstract checklist.
Supplementary File 4. MMAT assessment.
Supplementary Table 1. Summary of results (teamwork component).
Supplementary Table 2. Summary of results (team interventions).
Abbreviations
MMAT, Mixed Methods Appraisal Tool; MDTs, multidisciplinary teams; ITEM, Integrated (Health Care) Team Effectiveness Model; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis; HSOPSC, Hospital Survey on Patient Safety Culture; SAQ, Safety Attitudes Questionnaire; TeamSTEPPS, Team Strategies and Tools to Enhance Performance and Patient Safety; SBAR, Situation-Background-Assessment-Recommendation.
References
1. The Central People's Government of the People's Republic of China. [Opinions of the CPC Central Committee and the State Council on Deepening the Healthcare System Reform] (2009). Available online at: http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm (accessed April 1, 2021).
2. Hughes RG. Tools and strategies for quality improvement and patient safety. In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville, MD: Agency for Healthcare Research and Quality (US) (2008). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK2682/?report=classic (accessed April 1, 2021).
3. Scott I. What are the most effective strategies for improving quality and safety of health care? Intern Med J. (2009) 39:389–400. doi: 10.1111/j.1445-5994.2008.01798.x
4. World Bank, World Health Organization. Healthy China: Deepening Health Reform in China: Building High-Quality and Value-Based Service Delivery. Washington, DC: World Bank Group (2019). p. 387. Available online at: http://documents.worldbank.org/curated/en/690791553844042874/Deepening-Health-Reform-in-China-Building-High-Quality-and-Value-Based-Service-Delivery (accessed April 1, 2021).
5. Spath PL, editor. Error Reduction in Health Care: A Systems Approach to Improving Patient Safety. 2nd ed. Hoboken, NJ: John Wiley & Sons (2011). p. 416.
6. Suresh G, Horbar JD, Plsek P, Gray J, Edwards WH, Shiono PH, et al. Voluntary anonymous reporting of medical errors for neonatal intensive care. Pediatrics. (2004) 113:1609–18. doi: 10.1542/peds.113.6.1609
7. El-Dawlatly AA, Takrouri MS, Thalaj A, Khalaf M, Hussein WR, El-Bakry A. Critical incident reports in adults: an analytical study in a teaching hospital. Middle East J Anaesthesiol. (2004) 17:1045–54.
8. Pronovost PJ, Thompson DA, Holzmueller CG, Lubomski LH, Dorman T, Dickman F, et al. Toward learning from patient safety reporting systems. J Crit Care. (2006) 21:305–15. doi: 10.1016/j.jcrc.2006.07.001
9. Kohn LT, Corrigan JM, Donaldson MS, editors. To Err is Human: Building A Safer Health System. Washington, DC: National Academies Press (2000). p. 312.
10. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. (2009) 53:143–51. doi: 10.1111/j.1399-6576.2008.01717.x
11. Mickan S, Rodger S. Characteristics of effective teams: a literature review. Aust Health Rev. (2000) 23:201–8. doi: 10.1071/AH000201
12. Lemieux-Charles L, McGuire WL. What do we know about health care team effectiveness? A review of the literature. Med Care Res Rev. (2006) 63:263–300. doi: 10.1177/1077558706287003
13. Buljac-Samardzic M, Doekhie KD, van Wijngaarden JD. Interventions to improve team effectiveness within health care: a systematic review of the past decade. Hum Resour Health. (2020) 18:2. doi: 10.1186/s12960-019-0411-3
14. Hughes AM, Gregory ME, Joseph DL, Sonesh SC, Marlow SL, Lacerenza CN, et al. Saving lives: a meta-analysis of team training in healthcare. J Appl Psychol. (2016) 101:1266–304. doi: 10.1037/apl0000120
15. Meyer E. The Culture Map: Breaking Through the Invisible Boundaries of Global Business. New York, NY: PublicAffairs (2014). p. 288.
16. Hofstede Insights. Country Comparison. (2021). Available online at: https://www.hofstede-insights.com/country-comparison/ (accessed April 1, 2021).
17. Tjosvold D, Law KS, Sun HF. Collectivistic and individualistic values: their effects on group dynamics and productivity in China. Group Decis Negot. (2003) 12:243–63. doi: 10.1023/A:1023383200180
18. Hui C, Wong A, Tjosvold D. Turnover intention and performance in China: the role of positive affectivity, Chinese values, perceived organizational support and constructive controversy. J Occup Organ Psychol. (2007) 80:735–51. doi: 10.1348/096317906X171037
19. Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
21. Azungah T. Qualitative research: deductive and inductive approaches to data analysis. Qual Res J. (2018) 18:383–400. doi: 10.1108/QRJ-D-18-00035
22. Dietz AS, Pronovost PJ, Mendez-Tellez PA, Wyskiel R, Marsteller JA, Thompson DA, et al. A systematic review of teamwork in the intensive care unit: what do we know about teamwork, team tasks, and improvement strategies? J Crit Care. (2014) 29:908–14. doi: 10.1016/j.jcrc.2014.05.025
23. Korner M, Butof S, Muller C, Zimmermann L, Becker S, Bengel J. Interprofessional teamwork and team interventions in chronic care: a systematic review. J Interprof Care. (2016) 30:15–28. doi: 10.3109/13561820.2015.1051616
24. Hong QN, Fabregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, et al. The Mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. (2018) 34:285–91. doi: 10.3233/EFI-180221
25. Charette M, McKenna LG, Deschenes MF, Ha L, Merisier S, Lavoie P. New graduate nurses' clinical competence: a mixed methods systematic review. J Adv Nurs. (2020) 76:2810–29. doi: 10.1111/jan.14487
26. Hu Y, Broome M. Interprofessional collaborative team development in China: a grounded theory study. J Nurs Manag. (2019) 27:1075–83. doi: 10.1111/jonm.12775
27. Zhou L, Nunes MB. Identifying knowledge sharing barriers in the collaboration of traditional and western medicine professionals in Chinese hospitals: a case study. J Librariansh Inf Sci. (2012) 44:238–48. doi: 10.1177/0961000611434758
28. Cui Y, Xi X, Zhang J, Feng J, Deng X, Li A, et al. The safety attitudes questionnaire in Chinese: psychometric properties and benchmarking data of the safety culture in Beijing hospitals. BMC Health Serv Res. (2017) 17:590. doi: 10.1186/s12913-017-2543-2
29. Zhong X, Song Y, Dennis C, Slovensky DJ, Wei LY, Chen J. Patient safety culture in Peking university cancer hospital in China: baseline assessment and comparative analysis for quality improvement. BMC Health Serv Res. (2019) 19:1008. doi: 10.1186/s12913-019-4837-z
30. Agency for Healthcare Research and Quality. Surveys on Patient Safety Culture (SOPS) Hospital Survey. (2021). Available online at: https://www.ahrq.gov/sops/surveys/hospital/index.html (accessed April 1, 2021).
31. Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. (2006) 6:44. doi: 10.1186/1472-6963-6-44
32. Chu J, Mao J, Xi M, Cao H. [Investigation on the status quo of creating team atmosphere in the construction of hospital safety culture]. Heilongjiang Yi Yao Ke Xue. (2014) 37:77–8.
33. Feng X, Bobay K, Krejci JW, McCormick BL. Factors associated with nurses' perceptions of patient safety culture in China: a cross-sectional survey study. J Evid Based Med. (2012) 5:50–6. doi: 10.1111/j.1756-5391.2012.01177.x
34. Jia E, Zhou Y, Yan X, Liao J, Feng F, Zhang J. [Situation of nursing teamwork in a class III grade A hospital of Shanghai Municipality]. Zhongguo Xian Dai Hu Li Za Zhi. (2017) 23:2853–8. doi: 10.3760/cma.j.issn.1674-2907.2017.22.007
35. Jiang K, Tian L, Yan C, Li Y, Fang H, Peihang S, et al. A cross-sectional survey on patient safety culture in secondary hospitals of Northeast China. PLoS ONE. (2019) 14:e0213055. doi: 10.1371/journal.pone.0213055
36. Liu C, Liu W, Wang Y, Zhang Z, Wang P. Patient safety culture in China: a case study in an outpatient setting in Beijing. BMJ Qual Saf. (2014) 23:556–64. doi: 10.1136/bmjqs-2013-002172
37. Nie Y, Mao X, Cui H, He S, Li J, Zhang M. Hospital survey on patient safety culture in China. BMC Health Serv Res. (2013) 13:228. doi: 10.1186/1472-6963-13-228
38. Song C, Wang G, Wu H. [Investigation on cooperation status of nursing teamwork in third-grade hospitals in Wuhan city]. Hu Li Yan Jiu. (2014) 28:405–8. doi: 10.3969/j.issn.1009-6493.2014.04.008
39. Wang M. Tao H. How does patient safety culture in the surgical departments compare to the rest of the county hospitals in Xiaogan City of China? Int J Environ Res Public Health. (2017) 14:1123. doi: 10.3390/ijerph14101123
40. Wang S, Lin Z, Cheng D. [The status quo and influential factors of nurses' perceptions of patient safety culture]. Jiangsu Yi Yao. (2016) 42:1630–2. doi: 10.19460/j.cnki.0253-3685.2016.14.038
41. Xie Y, Xu X. [Private hospital medical process of virtual team members impact on the analysis of differences]. Zhonghua Yi Xue Za Zhi. (2011) 91:1973–6. doi: 10.3760/cma.j.issn.0376-2491.2011.28.010
42. Xu XP, Deng DN, Gu YH, Ng CS, Cai X, Xu J, et al. Changing patient safety culture in China: a case study of an experimental Chinese hospital from a comparative perspective. Risk Manag Healthc Policy. (2018) 11:83–98. doi: 10.2147/RMHP.S151902
43. Hai-ping Y, Wei-ying Z, You-qing P, Yun-ying H, chi C, Yang-yang L, et al. Emergency medical staff's perceptions on cultural value difference-based teamwork issues: a phenomenological study in China. J Nurs Manag. (2020) 28:24–34. doi: 10.1111/jonm.12854
44. Zhang F, Tian L, Shang X, Li X, Xue R, Cheng S. Exploring relationships between first-line nurse manager's safety attitudes and safety factors in Henan, China. J Nurs Manag. (2018) 26:314–20. doi: 10.1111/jonm.12549
45. Zhao C, Chang Q, Zhang X, Wu Q, Wu N, He J, et al. Evaluation of safety attitudes of hospitals and the effects of demographic factors on safety attitudes: a psychometric validation of the safety attitudes and safety climate questionnaire. BMC Health Serv Res. (2019) 19:836. doi: 10.1186/s12913-019-4682-0
46. Zhao X, Liu W, Wang Y, Zhang L. Survey and analysis of patient safety culture in a county hospital. Fam Med Community Health. (2017) 5:299–310. doi: 10.15212/FMCH.2017.0137
47. Song W, Li H, Ding N, Zhao W, Shi L, Wen D. Psychometrics properties of the team interaction scale and influencing factors of team interaction of tertiary hospital physicians in China: a cross-sectional study. BMJ Open. (2019) 9:e026162. doi: 10.1136/bmjopen-2018-026162
48. He W, Ni S, Chen G, Jiang X, Zheng B. The composition of surgical teams in the operating room and its impact on surgical team performance in China. Surg Endosc. (2014) 28:1473–8. doi: 10.1007/s00464-013-3318-4
49. Liu JA, Wang Q, Lu ZX. Job satisfaction and its modeling among township health center employees: a quantitative study in poor rural China. BMC Health Serv Res. (2010) 10:115. doi: 10.1186/1472-6963-10-115
50. Liu X, Chen M, Li J, Ma L. How to manage diversity and enhance team performance: evidence from online doctor teams in China. Int J Environ Res Public Health. (2020) 17:48. doi: 10.3390/ijerph17010048
51. Hong S, Li Q. The reasons for Chinese nursing staff to report adverse events: a questionnaire survey. J Nurs Manag. (2017) 25:231–9. doi: 10.1111/jonm.12461
52. Liu PC, Zhang HH, Zhang ML, Ying J, Shi Y, Wang SQ, et al. Retirement planning and work-related variables in Chinese older nurses: a cross-sectional study. J Nurs Manag. (2018) 26:180–91. doi: 10.1111/jonm.12532
53. Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, et al. Training and simulation for patient safety. BMJ Qual Saf. (2010) 19:i34–43. doi: 10.1136/qshc.2009.038562
54. Hong Y, Cai X. Effect of team training on efficiency of trauma care in a Chinese hospital. J Int Med Res. (2018) 46:357–67. doi: 10.1177/0300060517717401
55. Liu T, Qin Z, Luo M, Tan ZX, Xiong JY, Gu GJ, et al. Assessment of three methods for removing massive air in a cardiopulmonary bypass circuit: simulation-based multi-discipline training in West China Hospital. Perfusion. (2019) 34:203–10. doi: 10.1177/0267659118806120
56. Qian J, Wang Y, Zhang Y, Zhu X, Rong Q, Wei H, et al. survey of the first-hour basic care tasks of severe sepsis and septic shock in pediatric patients and an evaluation of medical simulation on improving the compliance of the tasks. J Emerg Med. (2016) 50:239–45. doi: 10.1016/j.jemermed.2015.05.040
57. Xie X, Zhong J, Zhang Y, Zhou Z, Chen M, Tan W, et al. [The implementation and effect of the team training model of advanced cardiac life support]. Zhonghua Hu Li Jiao Yu. (2011) 8:483–5. doi: 10.3761/j.issn.1672-9234.2011.11.001
58. Zhang LF, Feng HB, Yu ZG, Jing S, Wan F. Surgical training improves performance in minimally invasive left ventricular assist device implantation without cardiopulmonary bypass. J Surg Educ. (2018) 75:195–9. doi: 10.1016/j.jsurg.2017.06.029
59. Agency for Healthcare Research Quality. About TeamSTEPPS. (2019). Available online at: https://www.ahrq.gov/teamstepps/about-teamstepps/index.html (accessed April 1, 2021).
60. Sun X, Luo X, Kang B, Zhu Y, Xu Z, Chen Y, et al. [The introduction and practice of team strategies & tools to enhance performance & patient safety in a hospital]. Zhongguo Wei Sheng Zi Yuan. (2016) 19: 221–5. doi: 10.13688/j.cnki.chr.2016.15371
61. Institute for Healthcare Improvement. SBAR Communication Technique. (2021). Available online at: http://www.ihi.org/Topics/SBARCommunicationTechnique/Pages/default.aspx (accessed April 1, 2021).
62. Wen L, Hu X, Ren G, Yi L. [Application effect of elaborative SBAR communication mode in hospital surgical teams]. Zhonghua Xian Dai Hu Li Za Zhi. (2017) 23:3461–4. doi: 10.3760/cma.j.issn.1674-2907.2017.27.006
63. Yang X, Mo W, Xiang H, Xie X, Long L. [Application of standardized communication mode in interventional ward]. Jie Ru Fang She Xue Za Zhi. (2019) 28:296–9. doi: 10.3969/j.issn.1008-794X.2019.03.019
64. Agency for Healthcare Research Quality. Checklists. (2019). Available online at: https://psnet.ahrq.gov/primer/checklists (accessed April 1, 2021).
65. Yuan Y, Ye J, Ren Y, Dai W, Peng J, Cai S, et al. The efficiency of electronic list-based multidisciplinary team meetings in management of gastrointestinal malignancy: a single-center experience in Southern China. World J Surg Oncol. (2018) 16:146. doi: 10.1186/s12957-018-1443-1
66. Chen Y, Guo C, Zhang Q, Shen Y, Li Y, Li X, et al. Patients with pancreatic cystic neoplasms can benefit from management of multidisciplinary team: experience from a Chinese academic centre. Pancreatology. (2018) 18:799–804. doi: 10.1016/j.pan.2018.07.010
67. Du CZ, Li J, Cai Y, Sun YS, Xue WC, Gu J. Effect of multidisciplinary team treatment on outcomes of patients with gastrointestinal malignancy. World J Gastroenterol. (2011) 17:2013–8. doi: 10.3748/wjg.v17.i15.2013
68. Xue L, Zhang J, Shen H, Hou Y, Ai L, Cui X. [The application of rapid rehabilitation model of multidisciplinary cooperation in cesarean section and the evaluation of health economics]. Zhonghua Yi Xue Za Zhi. (2019) 99:3335–9. doi: 10.3760/cma.j.issn.0376-2491.2019.42.012
69. He Z, Han Z, Gao F, Liu G, Zhu S, Wang L. [Model of community comprehensive intervention: influence on treatment effectiveness of hypertension patients]. Zhongguo Quan Ke Yi Xue. (2014) 17:192–4. doi: 10.3969/j.issn.1007-9572.2014.02.021
70. Li W, Hao N, Liu W, An D, Yan B, Li J, et al. The experience of the multidisciplinary team in epilepsy management from a resource-limited country. Epilepsia Open. (2019) 4:85–91. doi: 10.1002/epi4.12290
71. Li W, Tong Z, Quan Z, Zhao Y, Yu W, Ye X, et al. [Treatment experience of severe acute pancreatitis on 1033 cases]. Zhonghua Wai Ke Za Zhi. (2009) 47:1472–82. doi: 10.3760/cma.j.issn.0529-5815.2009.19.009
72. Lin H, Pan H. [The effect of team-based community health service mode on mobility maternal care]. Zhejiang Yu Fang Yi Xue. (2013) 25:69–70. doi: 10.19485/j.cnki.issn1007-0931.2013.04.029
73. Liu Q, Zhao S, Zheng X, Zhao L, Li J, Tian Y. [The effect of multidisciplinary collaborative respiratory rehabilitation treatment on pneumoconiosis patients]. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2009) 27:670–2. doi: 10.3760/cma.j.issn.1001-9391.2009.11.010
74. Lu J, Jiang Y, Qian M, Lv L, Ying X. The improved effects of a multidisciplinary team on the survival of breast cancer patients: experiences from China. Int J Environ Res Public Health. (2020) 17:277. doi: 10.3390/ijerph17010277
75. Luo Y, Huang Y, Chen X, Meng G, Zhang Y. Effects of multidisciplinary team care based on 5e's renal rehabilitation for peritoneal dialysis patients in guangxi zhuang autonomous region of China: a randomized controlled trial. Blood Purif. (2019) 48:115–23. doi: 10.1159/000496823
76. Rui Y, Qiu X, Zou J, Xie T, Ma B, Lu P, et al. [Clinical application of multidisciplinary team co-management in geriatric hip fractures]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. (2019) 33:1276–82. doi: 10.7507/1002-1892.201905017
77. Wang J, Guo S. [The impact of team management nursing on the hospital-community rehabilitation effects and negative emotions of patients after renal cancer surgery]. Hu Li Shi Jian Yu Yan Jiu. (2018) 15:136–8. doi: 10.3969/j.issn.1672-9676.2018.08.057
78. Wu D, Chen Y. [The impact of establishing a stroke center treatment team on improving the treatment performance of stroke patients]. Zhejiang Chuang Shang Wai Ke. (2016) 21:500–1. doi: 10.3969/j.issn.1009-7147.2016.03.048
79. Wu X, Tian M, Zhang J, Yang M, Gong X, Liu Y, et al. The effect of a multidisciplinary co-management program for the older hip fracture patients in Beijing: a “pre-and post-” retrospective study. Arch Osteoporos. (2019) 14:43. doi: 10.1007/s11657-019-0594-1
80. Ye YJ, Shen ZL, Sun XT, Wang ZF, Shen DH, Liu HJ, et al. Impact of multidisciplinary team working on the management of colorectal cancer. Chin Med J. (2012) 125:172–7.
81. Zhang L, Geng S, Qian L, Ye S, Wang X, Lu G, et al. Multidisciplinary care in patients with systemic lupus erythematosus: a randomized controlled trial in China. Int J Clin Pharm. (2019) 41:1247–55. doi: 10.1007/s11096-019-00870-y
82. Zhang S, Tang M, Ma J, Yang J, Qin X, Jin W, et al. Thoracic trauma: a descriptive review of 4168 consecutive cases in East China. Medicine. (2019) 98:e14993. doi: 10.1097/MD.0000000000014993
83. Zhao M, Guo X, Song Z, Liang G, Wang Z. [The clinical analysis of the hospital informatization and multidisciplinary team treatment for patients with severe craniofacial wounds]. Chuang Shang Yu Ji Wei Zhong Bing Yi Xue. (2014) 2:234–6. doi: 10.16048/j.cnki.tccm.2014.04.013
84. Taberna M, Moncayo FG, Jane-Salas E, Antonio M, Arribas L, Vilajosana E, et al. The multidisciplinary team (MDT) approach and quality of care. Front Oncol. (2020) 10:85. doi: 10.3389/fonc.2020.00085
85. Zhu B, Cai R, Bi Y, Mei Y. [Effects of team cooperation combined with risk prevention on nosocomial infection in emergency children]. Zhongguo Yi Yuan Gan Ran Xue Za Zhi. (2018) 28:1900–3. doi: 10.11816/cn.ni.2018-171849
86. Xiao L, Huang R, Chen B. [Effect of team performance appraisal program for community health service centers]. Zhongguo Quan Ke Yi Xue. (2015) 18:3781–6. doi: 10.3969/j.issn.1007-9572.2015.31.004
87. Chen H, Chen F, Shu X, Huang X, Peng F, Tu P, et al. [The impact of the team management mode in a secondary hospital on treating effect of diabetic patients]. Zhongguo Yi Yao Zhi Nan. (2011) 9:166–7. doi: 10.15912/j.cnki.gocm.2011.14.145
88. Chen Q, Chai Y, Hu L, Zhu L, Pei L, Wu X. [Preliminary study on the effect of multiple disciplinary team model nursing team on treatment of patients with multiple trauma in emergency department]. Zhonghua Xian Dai Hu Li Za Zhi. (2019) 25:4472–5. doi: 10.3760/cma.j.issn.1674-2907.2019.34.015
89. Di L, Wu H, Zhu R, Li Y, Wu X, Xie R, et al. Multi-disciplinary team for early gastric cancer diagnosis improves the detection rate of early gastric cancer. BMC Gastroenterol. (2017) 17:147. doi: 10.1186/s12876-017-0711-9
90. Jiang Y, Han H, Chen F, Lin S, Guo R, Chen X, et al. Impact of an innovative multidisciplinary team model on the management of spontaneous intracerebral hemorrhage in West China. Neurosurg Q. (2015) 25:488–94. doi: 10.1097/WNQ.0000000000000106
91. Wang C, Chang Y, Zheng Y, Wang Z, Li Y, Yang Y, Wang Q. [Application of multidisciplinary doctor-nurse collaboration team on the perioperation management of geriatric hip fractures]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. (2019) 33:1283–6. doi: 10.7507/1002-1892.201805068
92. Yue T, Tang Y, Wang X, Wang J, Chen L, Chen H, et al. [The role of integrated psychological intervention group mode in rescue of August 8th Jiuzhaigou Earthquake in a comprehensive hospital]. Zhongguo Ji Jiu Fu Su Yu Zai Hai Yi Xue Za Zhi. (2019) 14:252–5. doi: 10.3969/j.issn.1673-6966.2019.03.016
93. Zhou X, Qiu F, Wan D, Sun S, Yao G, Liu Y, et al. Nutrition support for critically ill patients in China: role of the pharmacist. Asia Pac J Clin Nutr. (2019) 28:246–51. doi: 10.6133/apjcn.201906_28(2)0.0006
94. Kong J, Wu Z. [The effect of team management mode in emergency nursing management]. Shenzhen Zhong Xi Yi Jie He Za Zhi. (2016) 26:185–6. doi: 10.16458/j.cnki.1007-0893.2016.23.096
95. Liu Q, Wan J. [The application of quality control circle in improving the coordination ability of batch cataract surgery]. Shi Yong Yi Ji Za Zhi. (2015) 22:1364–5.
96. Shang Y. [Analyzing the application effect of diabetic specialized nursing team in diabetes management in a hospital]. Jian Kang Da Shi Ye. (2019) 9:279. doi: 10.3969/j.issn.1005-0019.2019.09.450
97. Xing H, Fang F, Chen L, Yao H. [Exploration of intravenous infusion team operation and management model in large general hospitals]. Hu Li Yan Jiu. (2013) 27:4075–6. doi: 10.3969/j.issn.1009-6493.2013.35.059
98. Xiong Z, Yuan L, He L, Zhu H, Ma L, Yang X, et al. [The effect of blood glucose management team in large comprehensive hospitals over inpatient in abnormal dysglycemia in non-endocrinology departments]. Zhongguo Quan Ke Yi Xue. (2015) 18:443–5. doi: 10.3969/j.issn.1007-9572.2015.04.022
99. Xu H, Cao G, Yao J, He W, Guo J. [Enhancing night and holiday team building in a specialized hospital]. Jiangsu Wei Sheng Shi Ye Guan Li. (2017) 28:173–4. doi: 10.3969/j.issn.1005-7803.2017.06.063
100. Xu W, Huang Y, Bai J, Varughese AM. A quality improvement project to reduce postoperative adverse respiratory events and increase safety in the postanesthesia care unit of a pediatric institution. Pediatr Anesth. (2019) 29:200–10. doi: 10.1111/pan.13534
101. Yang JG, Zhang J. Improving the postoperative handover process in the intensive care unit of a tertiary teaching hospital. J Clin Nurs. (2016) 25:1062–72. doi: 10.1111/jocn.13115
102. Wu L. [Exploring the practical effect of cancer pain nursing team in a comprehensive hospital in pain management of geriatric cancer patients]. Zhongguo Yi Yao Zhi Nan. (2015) 13:269–70. doi: 10.15912/j.cnki.gocm.2015.26.215
103. Schmutz JB, Meier LL, Manser T. How effective is teamwork really? the relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open. (2019) 9:e028280. doi: 10.1136/bmjopen-2018-028280
104. Costa Jr PT, Terracciano A, McCrae RR. Gender differences in personality traits across cultures: robust and surprising findings. J Pers Soc Psychol. (2001) 81:322. doi: 10.1037/0022-3514.81.2.322
105. Weisberg YJ, DeYoung CG, Hirsh JB. Gender differences in personality across the ten aspects of the big five. Front Psychol. (2011) 2:178. doi: 10.3389/fpsyg.2011.00178
106. Gentene AJ, Guido MR, Woolf B, Dalhover A, Boesken TA, Mueller EW, et al. Multidisciplinary team utilizing pharmacists in multimodal, bundled care reduce chronic obstructive pulmonary disease hospital readmission rates. J Pharm Pract. (2021) 34:110–6. doi: 10.1177/0897190019889440
107. Ju M, Wang SC, Syed S, Agrawal D, Porembka MR. Multidisciplinary teams improve gastric cancer treatment efficiency at a large safety net hospital. Ann Surg Oncol. (2020) 27:645–50. doi: 10.1245/s10434-019-08037-9
108. Kirkpatrick Partners. The New World Kirkpatrick Model. (2021). Available online at: https://www.kirkpatrickpartners.com/Our-Philosophy/The-New-World-Kirkpatrick-Model (accessed April 1, 2021).
109. Kwon JW. Does China have more than one culture? Asia Pac J Manag. (2012) 29:79–102. doi: 10.1007/s10490-010-9191-y
Keywords: teamwork, team performance, team intervention, multidisciplinary team, Chinese hospitals
Citation: Wang H, Buljac-Samardzic M, Wang W, van Wijngaarden J, Yuan S and van de Klundert J (2021) What Do We Know About Teamwork in Chinese Hospitals? A Systematic Review. Front. Public Health 9:735754. doi: 10.3389/fpubh.2021.735754
Received: 03 July 2021; Accepted: 15 November 2021;
Published: 17 December 2021.
Edited by:
Saturnino Luz, University of Edinburgh, United KingdomReviewed by:
Bridget T. Kane, Karlstad University, SwedenSissel Eikeland Husebø, University of Stavanger, Norway
Copyright © 2021 Wang, Buljac-Samardzic, Wang, van Wijngaarden, Yuan and van de Klundert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hujie Wang, d2FuZ0Blc2hwbS5ldXIubmw=