
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 November 2021
Sec. Public Health Education and Promotion
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.731272
This article is part of the Research Topic One Health, Environmental Health, Global Health, and Inclusive Governance: What can we do? View all 12 articles
 Ariba Abbasi1†
Ariba Abbasi1† Khuram Shahzad1
Khuram Shahzad1 Rana Muhammad Kamran Shabbir2†
Rana Muhammad Kamran Shabbir2† Muhammad Sohail Afzal2
Muhammad Sohail Afzal2 Hamza Zahid3Talha Zahid4
Hamza Zahid3Talha Zahid4 Haroon Ahmed1*
Haroon Ahmed1* Jianping Cao5,6,7,8*
Jianping Cao5,6,7,8*Background: Loose bowels is a clinical sign of gastrointestinal transport channel proteins, channels, and physical and chemical boundaries being harmed, prompting issues of water and electrolyte transport in the intestinal system. It is still considered as a major reason for emergency visits to hospitals in low-middle income countries. Zinc is a suitable treatment along with ORS for diarrhea. KAP surveys are usually conducted to collect information about general or specific topics of a particular population. The objective of this study was to investigate the knowledge, attitude, practices (KAP), and one health perspective regarding diarrhea among the participants from urban and rural populations of Rawalpindi and Islamabad, Pakistan.
Methods: Data was collected by conducting a survey among residents of twin cities over a period of 6 months (from July 2020 to December 2020). The questionnaire compromised socio-demographic features and the degree of KAP with respect to diarrhea management and control. One way ANOVA tests were applied to observe the demographic relationship and various factors influencing knowledge, attitude, practices, and one health perspective about diarrhea.
Results: A total of 338 subjects participated in the study. Female subjects were in the majority with 63% while the rest were male. A majority of the participants were between 15–25 years of age and 79.6% participants were un-married. The leading ethnic group was Punjabi with 52.7%; the lowest ethnic group were of Sindhi ethnicity with 8.6%. Age has a significant association with respect to knowledge and attitude. Religion has a significant association with respect to knowledge, practices, and one health, while education/qualification has an association with knowledge. The rest of the variables found no association with each other.
Conclusion: It is concluded from the recent study that most residents of the twin cities of Pakistan knew about diarrhea and had a good attitude and practices toward it. Age, religion, and education have different roles regarding different diseases in the population of Pakistan. The current study has its limitations as well. Parts of the study were conducted in the capital of Pakistan which is more developed as compared to other areas of Pakistan. It would be better to explore the remote areas of Pakistan where basic amenities of life such as education, wealth, and unemployment are not available. It is important to create more awareness among community members. They should be aware how dangerous these viruses and bacteria can be. Other parts of Pakistan should also be explored for better understanding that will help in making a nationwide health policy.
Diarrhea is characterized as three or more loose or liquid stools passing through each day or more frequently than usual for the person. For the most part, loose bowels is a clinical sign of gastrointestinal transport channel proteins, channels, and physical and chemical boundaries being harmed, prompting issues of water and electrolyte transport in the intestinal system (1). With advancements in technology and the medical field, the mortality rate associated with diarrhea has reduced but it is still considered as a major reason for pediatric emergency visits in hospitals, particularly in low-income countries in Asia and Africa (2). The common cause for diarrhea is a variety of bacteria, viruses, and fungus (3). Due to poor hygiene, infection spreads by infected food or drink or from individual to individual. Diarrhea is a condition that is both preventable and treatable. Diarrhea fluid deficiency has fatal consequences and is the leading cause of malnutrition (4). It causes 1.3 million (M) deaths per year and is also a widespread health problem in the world (5).
The treatment of Diarrheal illness as per the World Health Organization (WHO) is Zinc supplementation along with ORS, which has emerged as a potent approach to treating Diarrhea (6). To meet the challenges of prevention of diarrhea, an effective public health program is needed which should include supplies of safe drinking water, zinc supplementation prevention/early correction of dehydration, ultraviolet purification filter plants, and advice on boiling of water at household level (7). Diarrhea can also be treated by Rehydration with intravenous fluids, Nutrient-rich foods including breast milk, and by giving a nutritious diet to children when they are well (8).
An expert consultation identified several barriers in reducing childhood diarrhea–related mortality (9). These included: the absence of national coordination within ministries and other stakeholders to deliver interventions, insufficient financial resources, inadequate training and support for health workers, poor systems for monitoring and assessing key programmatic indicators, and sporadic availability of key commodities. However, care–seeking behaviors by families, and their belief systems around diarrheal diseases, were not identified as possible barriers, although these are well-described in the literature (10).
WHO and UNICEF launched a comprehensive Diarrhea control plan in 2009 (11). Global Action Plan for Diarrhea has an ambitious goal of ending preventable childhood deaths by 2025, and to achieve that, it provides a set of priorities and interventions to scale-up progress at a country level (12). Integrated Global Action Plan for Diarrhea introduces a cohesive approach to ending preventable Diarrhea deaths. But to reach every child would require scaling-up and targeting of interventions known to prevent and control Diarrhea. Enabling this vision requires coordination and collaboration from child-health-related programs, parents, communities, community health workers (CHWs), civil society, and the private sector. Pakistan follows the WHO guidelines and policies in this regard (13).
A KAP survey is usually conducted to collect information on the knowledge, attitudes, and practices about general and/or specific topics of a particular population. KAP surveys can identify needs, problems, and barriers to help plan and implement interventions (14). It deepens the understanding of commonly known information, attitudes, and factors that influence behavior. KAP studies help in assessing and identifying communication processes and sources important for program implementation and effectiveness. It also helps to set program priorities and make program decisions (11).
There is a scarcity of data regarding the KAPs of diarrhea in the Pakistani community, so the present study was designed to assess demographic attributes of knowledge, attitude, and practices and to establish one health perspective toward diarrhea among residents of Rawalpindi and Islamabad, Pakistan.
The study was carried out in universities of the twin cities: the capital Islamabad and Rawalpindi. The terrain consists of plains and mountains in the metropolitan area of Islamabad and Rawalpindi, whose total area exceeds 1,175 m. In general, three general physiographic zones trend east-northeast. In the mountainous terrain of the Margalla Hills lies the northern part of the metropolitan area. Rawalpindi, famed for its ancient Buddhist heritage, is situated on the Pothohar Plateau.
Simple random sampling was considered throughout this study and the university students and adjoining areas within the university were considered in the population, by following the (15), for the Demographic variables such as age, gender are categorical data. To assess the correct sample size formula was used. The margin of error is set to 0.05, the estimate of variance is set at 0.50, and the t-value is fixed at 1.65, which resulted in a 264-sample size. However, to overcome the non-response, initially, we set 369 sample sizes, and 31 did not provide a response. Hence, the final sample size of this study is 338 students. The study was done between July and December 2020. The proforma for data collection was designed after a thorough literature survey (4, 16, 17) and consisted of 57 questions. The questionnaire was divided into five main parts. The first part consists of 13 questions that were about the demography. The second part was about the knowledge, with 24 questions. The third, fourth, and fifth parts were about the attitude, practices, and one health with four, eight, and eight questions, respectively.
The participants were briefed about the survey purposes and written informed consent was collected from the participants. Data was entered into an MS excel spread sheet and a database was established. Statistical evaluation was executed by using Jamovi version 1.6.7. One way ANOVA tests were applied to observe the scores of various factors e.g., knowledge, attitude, practices, and one health across demographic variables regarding diarrhea.
A total of 338 subjects participated in the study. Most of the participants were female with 63.0%, and the rest were male. Most of the participants (72.2%) were between the ages of 15–25, followed by 26–35, 36–45, and below 15 age groups. Based on ethnic groups, most of the participants were Punjabi with 52.7%, followed by Islamabadis/Islamabadians, Kashmiri, and Sindhi. Of the participants, 96.2% were Muslims while 3.8% were non-Muslims. Based on education, 43.5% participants were undergraduate students followed by graduate and intermediate. A majority (46.4%) of the income group earned below 10,000 Rs followed by participants with incomes above 30,000 Rs. monthly. A majority (70.1%) of participants were of urban origin while 29.9% were from rural backgrounds (Table 1).
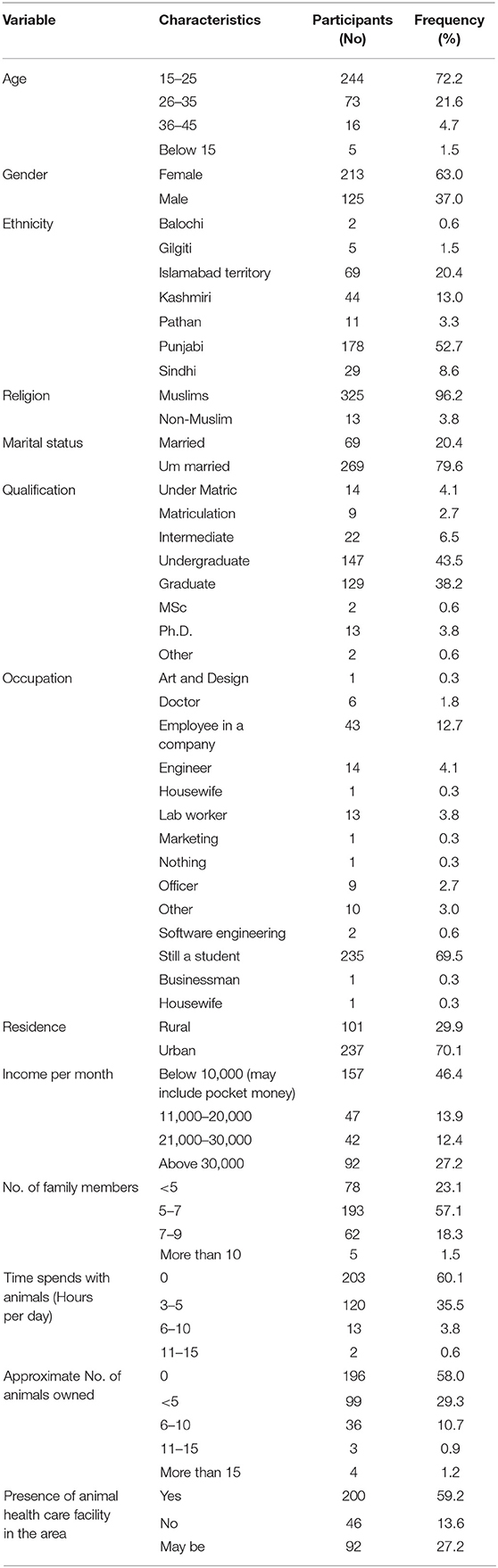
Table 1. Socio demographic background of the participants.
Regarding knowledge about diarrhea, 75.1% of the participants knew that microorganisms were a cause of diarrhea. 52.7% of the participants knew about the microorganisms which were the cause of diarrhea and 43.5% of the respondents were aware that diarrhea is caused due to the rotavirus/norovirus or campylobacter. 50.3% of the participants knew what gastroenteritis is while 40.8% of the participants thought that gastroenteritis was an inflammation of the stomach and small intestine; 11.8% thought it was swelling of the stomach and 47.3% had no idea about the definition of gastroenteritis. 60.9% of the respondents were aware about the early symptoms of the disease while 9.5% were unaware. 69.8% of the subjects considered diarrhea to be a dangerous disease, while 47% considered it a disease that lasted for 1 week. 73% think that babies can have diarrhea, 45.3% considered weight loss to be a result of diarrhea, and 41.4% considered lethargy to be a symptom. 71.6% agreed that animals can also get diarrhea, 58.3% think that animal feces could be responsible for spreading diarrhea, and 64.2% believed that diarrhea can cause bleeding in organisms. 71.6% believed that diarrhea affects blood pressure, 92.6% responded that it may be responsible for dehydration, 54.1% believed that diarrhea can affect the baby during pregnancy, 56.8% believe in death due to this, and 55.3% considered ORS as an effective treatment for this disease. 41.4% agreed that a vaccine is available for this disease, 59.6% believed that undercooked food is responsible for diarrhea, and 83.7% believe contaminated water is a source of transmission of disease. 84.6% of the participants considered contaminated food and water a risk factor of diarrhea; 4.1% did not consider them as a risk factor and 11.2% were not sure about it. 48.2% of the participants had suffered with diarrhea while the rest of the participants had not suffered with this disease (Table 2).
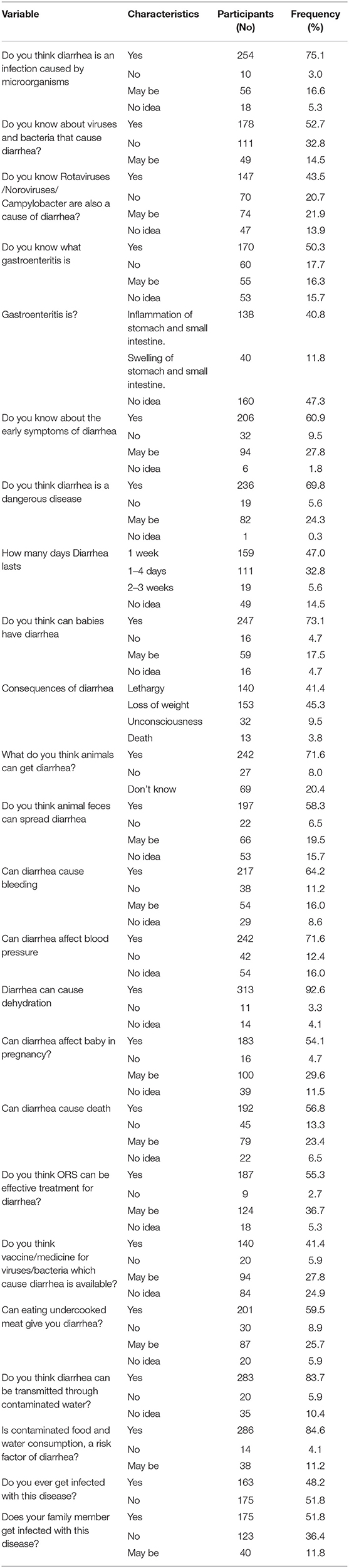
Table 2. Knowledge toward diarrhea of participants in the study.
With respect to attitude questions, 84.6% of the participants considered visiting the doctor if they had diarrhea while 4.1% said they would not visit doctor and 11.2% were not sure about visiting. 82.5% believed that avoiding dipping their hand in a vessel could prevent diarrhea. 75.1% believed that use of filtered or boiled water should be used for consumption to avoid diarrhea and 35.2% believed that it can be transmitted form one person to another; 30.8% do not believe this and the rest of the respondents had no idea or were not sure about this (Table 3).
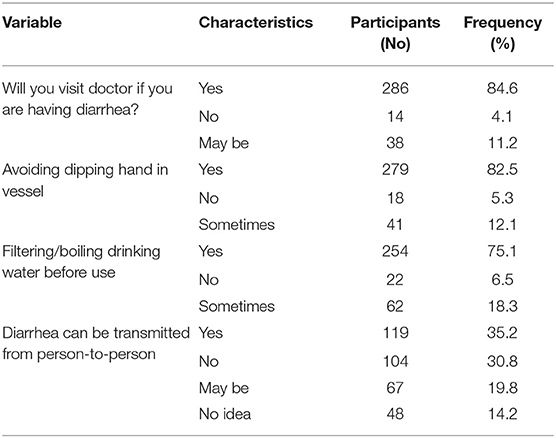
Table 3. Attitude toward diarrhea of participants in the study.
Regarding practices, 61.8% avoided the formation of ice from tap water while 7.4% had not used tap water for ice and 30.8% sometimes used tap water for ice at home. 87.9% considered that closing the lids of drinking water sources can prevent diarrhea. 86.7% of the participants washed their hands before cooking, eating, or after defecation, while 3.0% of responses were negative and 10.4% sometime washed their hands. 78.4% of the participants mentioned regular cleaning of drinking water vessels while 5.6% said they did not clean them regularly and 16.0% cleaned vessels but not always. 90.2% of the subjects mentioned washing fruits and vegetables before use while 1.2% thought it was not necessary to wash them and 8.6% of participants sometimes washed fruits and vegetables before use. 88.2% wash their hands before feeding their children while 9.5% practice this sometimes. 81.4% practice the proper disposal of refuse material while 74% respondents visit the doctor immediately when they encounter diarrhea (Table 4).
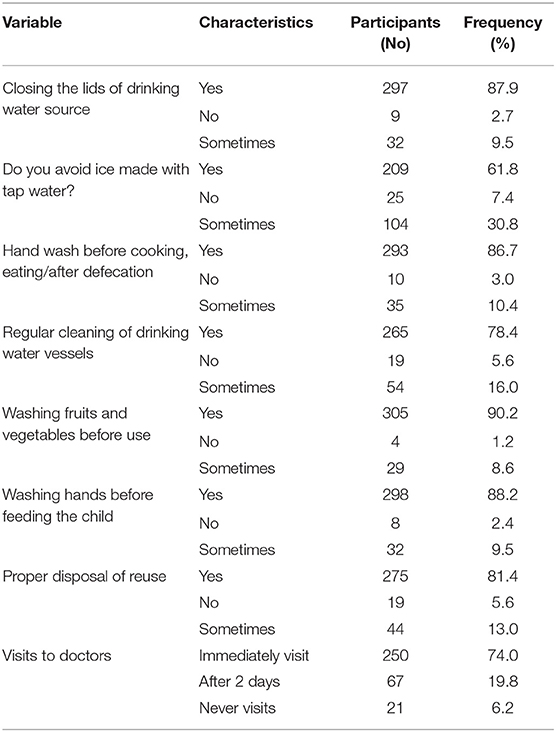
Table 4. Practices toward diarrhea of participants in the study.
Regarding one health perspective, 85.8% of the participants knew that human health is associated with the environment while 2.1% negated it and 10.4% were not sure about it. 58.3% of the participants knew about zoonosis while 41.7% had no knowledge about it. 55.6% of the participants considered that diarrhea can be transmitted through animals while 10.4% thought it cannot be transmitted through animals and 16.6% were not sure about that. 63.6% of the participants knew about one health while 36.4% participants had no idea about one health. 33.7% of the participants mentioned that risk of diarrhea was associated with a specific age while 43.2% negated the statement and 14.8% were not sure about that. Almost more than 90% believed that there is a need for proper disposal and sewage systems, 94.1% considered that there is need for public awareness regarding this disease, and 94.1% considered that there must be awareness of complications of untreated prolonged infection (Table 5).
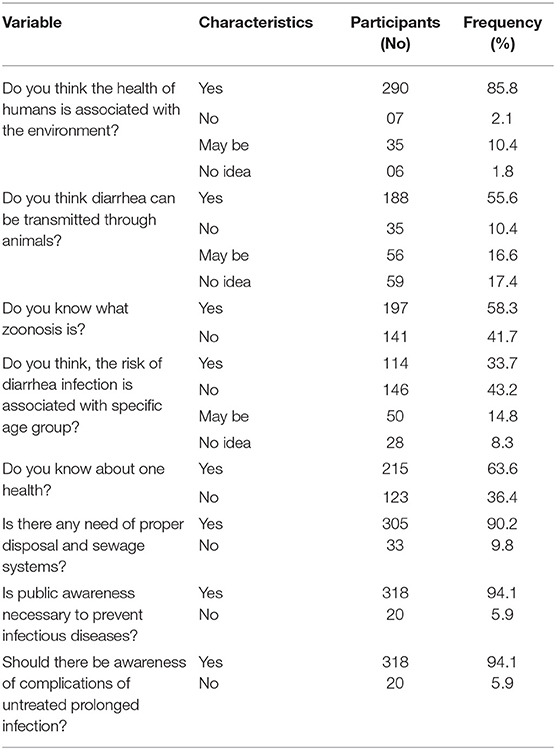
Table 5. One-health toward diarrhea of participants in the study.
One-way ANOVA was applied to establish the relationship between dependent and independent variables. Six independent variables (age, gender, ethnicity, qualification, religion, and marital status) and four dependent variables (knowledge, attitude, practices, and one health) were taken to check their scores across all dependent and independent variables. Age and ethnicity have significant association with respect to knowledge. Religion has significant association with respect to one health while education/qualification has an association with knowledge. The rest of the variables found no association with each other (Table 6).
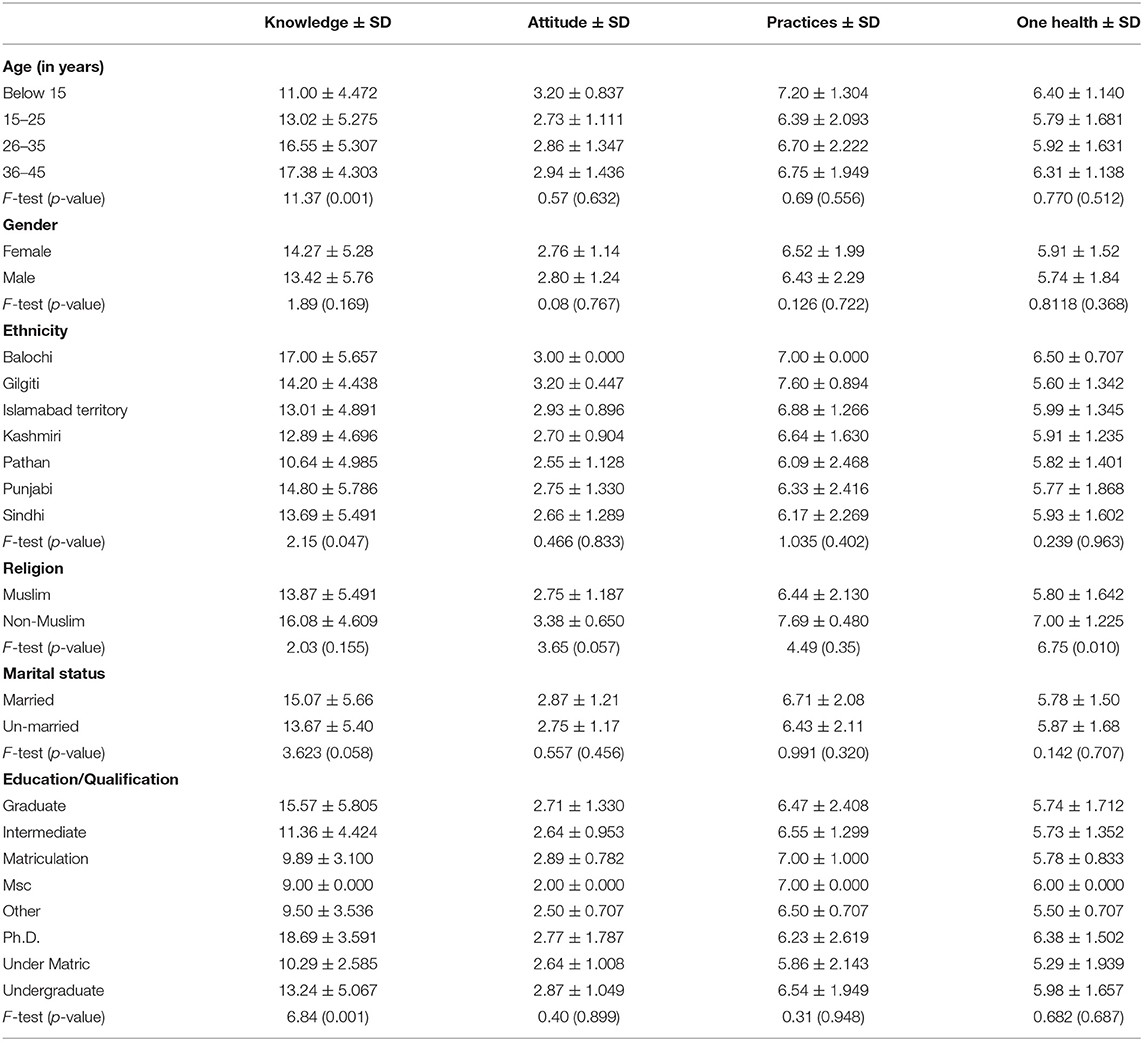
Table 6. Demographic variables across KAPs and one health using one-ANOVA.
The study has assessed the knowledge, attitude, practices, and one health perspective regarding diarrhea among residents of Rawalpindi/Islamabad (twin cities) of Pakistan. 83.7% of the participants were aware that diarrhea spread through contaminated water. A similar kind of study was reported from Karachi where 17% considered polluted water as a cause of diarrhea (4). One study from India reported that 55% of mothers were aware of causes of diarrhea (16). The current study was conducted among residents of twin cities where the literacy rate is highest in Pakistan. The higher literacy rate could be related to the increased knowledge about diarrhea. The contrary results from the Karachi study could be due to the limitation of the Karachi study, which was only conducted among the mothers of children under the age of 5 years (4).
Lethargy is considered as the main consequence of diarrhea. 41.4% of the participants considered lethargy a consequence of diarrhea. Similar kinds of observations were reported from Karachi; 71% of mothers said that diarrhea causes lethargy (4). Our results also showed that most of the study participants had a favorable attitude regarding diarrhea. The study showed that 55.3% of participants thought that ORS was an effective treatment for diarrhea. The same was observed in the National Family Health Survey which found that only 27% of participants use ORS in management (17). In another study from Pakistan, it was reported that 74% of mothers considered ORS as enough of a treatment for diarrhea (18).
The present study also revealed that 56.8% of the participants considered diarrhea to be a dangerous disease which can lead to the death of a person. The same observation was reported in a study from India where 81.7% people considered diarrhea a dangerous disease which can lead to death (18).
The current study reports that 81.4% of participants disposed of refuse material properly. A similar kind of study was reported from India which illustrates that 30.5% of participants disposed of waste material properly (18). The high rate of properly disposed material could be associated with higher literacy levels and people awareness in the advanced cities of Pakistan, while the low ratio from India is associated with the low literacy level in the study duration that was conducted two decades earlier (18).
According to the present survey, 86.7% of the participants washed their hands before cooking, eating, and after defecation. One study of a similar type showed that only 60% and 30% practiced handwashing after defecation and before handling of food, respectively (16). In another study from Karachi, it was reported that 62% of mothers understand the different preventive strategies such as washing hands and keeping the room and the child clean as far as diarrhea prevention was concerned (4).
Statistical analysis showed that age is associated significantly with knowledge and attitude. This may mean that knowledge and attitudes vary with age. Furthermore, knowledge, practices, and one health were associated with religion significantly. This may mean that religion has a major influence on the current knowledge, practices, and one health. Education was also found to be associated with knowledge. The rest of the parameters have no significant association with one another. Our results were in line with a KAPS study from Pakistan (19) and is contrary to the study by Khan et al. (20), suggesting that every disease has their own demographic attributes.
It is concluded from this study that most residents of the twin cities of Pakistan knew about diarrhea and had a good attitude and practices toward it. Age, religion, and education have different roles regarding different diseases in the population of Pakistan. The current study has its limitations as well. Parts of the study was conducted in the capital of Pakistan which is more developed as compared to other areas of Pakistan. It would be better to explore the remote areas of Pakistan where basic amenities of life such as education, wealth, and employment are not available. To raise awareness among those people, we should convey our messages by means of social media, seminars, and motivational talks. In addition to all these things, education, basic amenities, and health facilities should be provided across Pakistan.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by ERB of COMSATS University Islamabad under CUI/Bio/ERB/2021/50 approval number. The patients/participants provided their written informed consent to participate in this study.
AA collected the data. RS and AA wrote the paper. MA and HZ performed the statistical analysis. The study was designed and supervised by KS and HA. RS, HA, TZ, and JC critically revised the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the National Natural Science Foundation of China (No. 81772225 to JC), the Laboratory of Parasite and Vector Biology, National Health Commission of People's Republic of China (No. WSBKFKT2017-01 to AA), and the Fifth Round of Three-Year Public Health Action Plan of Shanghai (No. GWV-10.1-XK13 to JC). The funders had no role in the study design, the data collection and analysis, the decision to publish, or the preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Chu C, Rotondo-Trivette S, Michail S. Chronic diarrhea. Curr. Prob. Pediatr. Ad. (2020) 50:100841. doi: 10.1016/j.cppeds.2020.100841
2. Nataro JP. Diarrhea among children in developing countries. Adv. Exp. Med. Biol. (2013) 764:73–80. doi: 10.1007/978-1-4614-4726-9_5
3. Li Y, Xia S, Jiang X, Feng C, Gong S, Ma J, et al. Gut microbiota and diarrhea: an updated review. Front. Cell. Infect. Microbiol. (2021) 11:625210. doi: 10.3389/fcimb.2021.625210
4. Mumtaz Y, Zafar M, Mumtaz Z. Knowledge attitude practices of mothers about diarrhea in children under 5 years. J. Dow. Univ. Health. Sci. (2014) 8:3–6.
5. Troeger C, Forouzanfar M, Rao PC, Khalil I, Brown A, Reiner RC Jr., et al. Estimates of global, regional, national morbidity. mortality, and aetiologies of diarrhoeal diseases: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. (2017) 17:909–48. doi: 10.1016/S1473-3099(17)30276-1
6. Clasen T, Wolf-Peter S, Tamer R, Ian R, Sandy C. Interventions to improve water quality for preventing diarrhoea: systematic review meta-analysis. Bio. Med. J. (2007) 334:782. doi: 10.1136/bmj.39118.489931.BE
7. Borapich D, Warsh M, Borapich D, Warsh M. Improving child health in Cambodia: social marketing of diarrhea treatment kit, results of a pilot project. Cases Pub. Heal. Commun. Mark. (2010) 4:4–22.
8. Santosham M, Chandran A, Fitzwater S, Fischer-Walker C, Baqui AH, et al. Progress and barriers for the control of diarrhoeal disease. Lancet. (2010) 376:63–7. doi: 10.1016/S0140-6736(10)60356-X
9. Gill CJ, Young M, Schroder K, Carvajal–Velez L, McNabb M, Aboubaker, et al. Bottlenecks, barriers, and solutions: results from multicountry consultations focused on reduction of childhood pneumonia and diarrhoea deaths. Lancet. (2013) 381:1487–98. doi: 10.1016/S0140-6736(13)60314-1
10. Shaikh BT, Hatcher J. (2005). Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health (Oxf). 27:49–54. doi: 10.1093/pubmed/fdh207
11. World Health Assembly. Resolution 64.18. Cholera: mechanism for control and prevention. In Sixty-Fourth World Health Assembly (Geneva: World Health Organization) 2011.
12. Huang W, Yao Y, Long Q, Yang X, Sun W, Liu C, et al. Immunization against multidrug-resistant Acinetobacter baumannii effectively protects mice in both Pneumonia and sepsis models. PLoS ONE. (2014) 9:e100727. doi: 10.1371/journal.pone.0100727
13. World Health Organization UNICEF. Ending preventable child deaths from Pneumonia and diarrhoea by 2025: The integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD). Geneva: World Health Organization (2013).
14. Médecins sans Frontières. Mass vaccination campaign using oral cholera vaccine during an outbreak in Guinea—Boffa and Forecariah Report. Médecins sans Frontières, Geneva, Switzerland (2012).
15. Kotrlik JW, Higgins CC (2001). Organizational research: determining appropriate sample size in survey research appropriate sample size in survey research. Inf. Technol. Learn. Perform. 19:43.
16. Sunanda G, Ramaiah D, Sadiq MM, Narayana G. Impact of structured educational program on maternal knowledge, attitude, and practice toward diarrhea management in children <5 years age in Anantapur District. CHRISMED J. Health. Res. (2017) 4:186–93. doi: 10.4103/cjhr.cjhr_121_16
17. Masiha SA, Khalid A, Malik B, Shah SMA. (2015). Oral rehydration therapy-knowledge, attitude and practice (KAP) survey of Pakistani mothers. SJRMC. 19:51–4.
18. Bhatia V, Swami HM, Bhatia M, Bhatia SP. (1999). Attitude practices regarding diarrhoea in rural community in Chandigarh. Indian J. Pediatr. 66:499–503. doi: 10.1007/BF02727156
19. Afzal MS, Khan A, Qureshi UUR, Saleem S, Saqib MAN, Shabbir MK, et al. Community-based assessment of knowledge, attitude, practices and risk factors regarding COVID-19 among Pakistanis residents during a recent outbreak: a cross-sectional survey. J Community Health. (2021) 46:476–86. doi: 10.1007/s10900-020-00875-z
Keywords: knowledge, attitude, practices, bacteria, viruses, pathogens and diarrhea
Citation: Abbasi A, Shahzad K, Shabbir RMK, Afzal MS, Zahid H, Zahid T, Ahmed H and Cao J (2021) Demographic Attributes of Knowledge, Attitude, Practices, and One Health Perspective Regarding Diarrhea in Pakistan. Front. Public Health 9:731272. doi: 10.3389/fpubh.2021.731272
Received: 26 June 2021; Accepted: 04 October 2021;
Published: 18 November 2021.
Edited by:
Ulrich Laaser, Bielefeld University, GermanyReviewed by:
Abdul Hameed, Innovative Development Strategies Pvt. Ltd, PakistanCopyright © 2021 Abbasi, Shahzad, Shabbir, Afzal, Zahid, Zahid, Ahmed and Cao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianping Cao, Y2FvanBAeWFob28uY29t; Haroon Ahmed, aGFyb29uYWhtYWQxMkB5YWhvby5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.