
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 26 November 2021
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 9 - 2021 | https://doi.org/10.3389/fpubh.2021.728690
 Juan Luis Delgado-Gallegos1
Juan Luis Delgado-Gallegos1 Gerardo R. Padilla-Rivas1Erika Zúñiga-Violante2Gener Avilés-Rodríguez3Daniel Arellanos-Soto1Lilia Julieta Gastelum-Arias1Héctor Franco Villareal4
Gerardo R. Padilla-Rivas1Erika Zúñiga-Violante2Gener Avilés-Rodríguez3Daniel Arellanos-Soto1Lilia Julieta Gastelum-Arias1Héctor Franco Villareal4 María de los Ángeles Cosío-León5
María de los Ángeles Cosío-León5 Gerardo Salvador Romo-Cardenas6
Gerardo Salvador Romo-Cardenas6 María G. Moreno-Treviño7
María G. Moreno-Treviño7 Jorge E. Moreno-Cuevas7*
Jorge E. Moreno-Cuevas7* Jose Francisco Islas1*
Jose Francisco Islas1*Mexico has become one of the most highly affected countries by coronavirus disease 2019 (COVID-19) pandemic in Latin America. Therefore, efficient vaccination programs are needed to address COVID-19 pandemic. Although recent advances around the world have made it possible to develop vaccines in record time, there has been increasing fear and misinformation around the vaccines. Hence, understanding vaccine hesitancy is imperative for modeling successful vaccination strategies. In this study, we analyzed the attitude and perceptions toward COVID-19 vaccination, in a Mexican population (n = 1,512), using the proposed COVID-19 Vaccine Acceptance and Hesitancy Questionnaire (COV-AHQ) (Cronbach's alpha > 0.8), which evaluates a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parent toward vaccination of children; furthermore, a section including sociodemographic variables was included. According to the results of this study, the statistical correlation analysis of the general vaccination posture seems to correlate significantly (p < 0.05) with a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, hesitancy of parent toward vaccination of children, willingness to get COVID-19 vaccine, previous influenza vaccination, perception of the vaccine that could help the economy of country, occupation, gender, age, and participants actively researching COVID-19 vaccine information. An in-depth analysis assisted by binary logistic regression concluded that the young adult population around ages 18–34 years are the most likely to get vaccinated. This posture seems to be highly influenced by a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parents toward vaccination of children. While their own personal religious beliefs and economic status, the level of education does not seem to have an effect on the willingness to get vaccinated neither did having a previous COVID-19 diagnosis or even knowing someone with a positive COVID-19 diagnosis. Health authorities and policymakers could use the results of this study to aid in modeling vaccination programs and strategies and identify population groups with high vaccine hesitancy prevalence and assess significant public health issues.
The highly infectious severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), which gives rise to coronavirus disease 2019 (COVID-19) (1), has through its tenure infected over 106 million people worldwide, while claiming the lives of over 2.3 million (2). According to the John Hopkins Coronavirus Resource Center, the highest hit countries by total cases are the US, Brazil, and UK (top 5%), but if we rank by death rate, Mexico is placed among the top ranks (top 1%) with about 9% death rate or case-fatality ratio, closely followed by Peru, Panama, Brazil, Colombia, and Ecuador, all of which are Latin American countries, with similar or slightly lower case-fatality ratio (2, 3).
Interestingly, healthcare system of Mexico has been a top priority for the country, leading to excellent results even in times of political and financial hardships (4). Regrettably, due to many factors such as the rise in overall healthcare cost and the need to reallocate assets, over time healthcare system of Mexico became fragmented with ill-equipped and understaffed hospitals (5), a paramount problem when trying to combat the current epidemic. It is important to mention that Mexico is a country where more than a quarter of adults develop hypertension and cardiovascular disease and close to 15% have diabetes, as all of these comorbidities might aggravate the condition of a patient infected with COVID-19 (2, 6–9).
Recent technological advances have made possible the acceleration of COVID-19 vaccines design and production. Currently, Mexico is in the last stages of clinical protocol evaluations; hence, Mexico is awaiting the approval of several vaccines for their use in the population (1, 10). Despite successful mass vaccination scenarios recorded throughout history such as polio and smallpox (11, 12), distrust in newly developed vaccines has grown, as there are many myths and misinformation around them (11, 13), Therefore, all the vaccination strategies should take into consideration factors associated with acceptance of the population. “What if I do not want to get a shot?,” “Do I fear adverse effects?;” recently, a multinational survey showed that of 13,426 people from 19 countries, 28.5% reported that they would not apply the vaccine (14). Although side effects associated with vaccination are generally mild, for example, pain and/or bleeding at the application site and temporary general malaise, some serious side effects reported are Guillain-Barré syndrome, febrile seizures, intussusception, coagulopathies, or anaphylaxis (11). Despite measures to counteract mistrust and misinformation around vaccination, these efforts have been frequently ineffective (12). To overcome this, authorities need a proactive approach in order to strengthen vaccination culture, leading with accurate scientific information and emphasizing the importance of vaccines in preventing life-threatening diseases (11, 12). A study by Timmis et al. determined a set of potential attributes in pro of acceptance of applying the vaccine: (1) High incidence of cases prevented per year, (2) Cost-effectiveness, (3) Being disease of high mortality, and (4) Risk of morbidity and mortality (15). Therefore, it is important for the sanitary authorities to strengthen the messages about the positive benefits of taking the vaccine in the general population.
We made a questionnaire based on the Adapted Covid Stress Scales and Vaccine Hesitancy Scales to determine how and which factors play crucial roles in the overall hesitancy of taking the vaccine (16–19). In this study, we look at four major sections as they related to a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parents toward vaccination of children. We also looked at the sociodemographic profile to determine how all these variables correlate. The overall purpose is to understand the levels of acceptance of vaccination against COVID-19 in Mexico and how different variables affect the perception of this event.
This study proposes the application of COVID-19 Vaccine Acceptance and Hesitancy Questionnaire (COV-AHQ), designed by the authors based on the Adapted COVID-19 Stress Scale (ACSS) (16, 17) and the Vaccine Hesitancy Scale (VHS) (18). We wrote our questionnaire using MS Forms (Microsoft Corporation, Redwood, Washington, United States) and applied it remotely through a web link, as seen in Table 1. We distributed this test to the general population in Mexico through electronic means such as social media groups: Facebook, Twitter, Reddit, and directed e-mail. We applied the questionnaire throughout the period from December 2020 to February 2021 before the beginning of the vaccination program in Mexico (20).
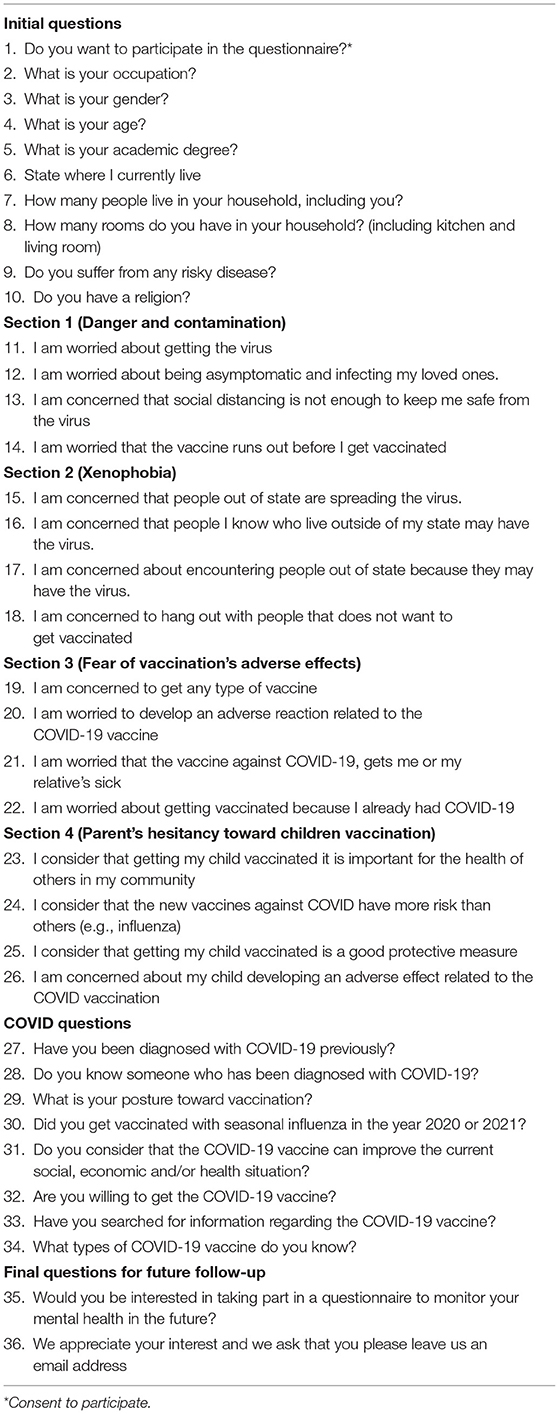
Table 1. COVID-19 Vaccine Acceptance and Hesitancy Questionnaire (COV-AHQ).
In order to calculate the sample size needed, we used the classical method by Lwanga and Lemershow (1991) for a finite population. For Mexico, it accounts for using a total population for 130 million as input (21). Additionally, we used a z-value of 1.96 (confidence level of 97.5%) and an expected p-value of 0.04 (expected percentage of cases) based on official data. The resulting value was an expected n of 1475.15.
All the subjects acknowledged being >18 years old and gave their consent for inclusion before participating in this study. We used a Likert scale format with increasing point values to further classify according to scores (16, 22). We calculated all the statistical correlation analyses using IBM-SPSS Statistics for Windows, version 23.0 (IBM Corporation, Armonk, New York, USA) with the Pearson's chi-squared test and an R ratio of 0.05. We calculated the frequency of answers in relation to categories and other sociodemographic variables. We then correlated the answers to the number of points in each section. Section 1 evaluated a mild perception of danger and contamination with respect to COVID-19, Section 2 evaluated a moderate perception of xenophobia generated throughout COVID-19 quarantine, and Section 3 evaluated fear of adverse effects of COVID-19 vaccination. Finally, Section 4 evaluated hesitancy of parents toward vaccination of children (18). We classified the resulting scores for Sections 1 to 4 and their ranges according to the following scales: absent 0 to 4, mild 5 to 8, moderate 9 to 12, and severe 13 to 16. These classifications evaluate the impact each individual section has on the daily life of participant. Where on one end, absent describes a negligible effect of the section on the participant, to severe where the section highly influences the daily decisions of participants. Other studied items were respect to different sociodemographic and vaccination variables such as occupation, gender, age, practice of religion, education level, total of habitants in household, total number of rooms in household, disease/comorbidity, knowing someone positive for COVID-19, attitude toward vaccination, previous influenza vaccination for 2020–2021 season, consideration of COVID-19 vaccine as a mean of turning a positive tide on the current socioeconomic situation of the country, willingness to receive COVID-19 vaccination, participants actively researching COVID-19 vaccine information, and their willingness to continue participating in follow-up questionnaires. To ensure integrity of the questionnaire, we consulted a group of experts to perform and evaluate pertinence and clarity tests. The calculated Cronbach's alpha (>0.8) represented good internal consistency. To identify the factors, which would have the most impact on the overall perception of acceptance among the participants, we used binary logistic regression analysis. This model was based on using the demographic factors and the studied sections as a whole (a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parents toward vaccination of children associated with willingness) to correlate them to the willingness to get vaccinated. We then introduced these selected factors and sections into a backward stepwise (likelihood ratio) method. Finally, we used to quantify the associations between factors and sections and willingness to vaccine unstandardized regression coefficients (ß) and odds ratios (ORs) and their 95% CIs.
Given the extent COVID-19 pandemic has affected the country (2, 17, 23) and how recent advances in technology have moved forward interconnectivity (23–25), we opted to use electronic means to implement our questionnaire, as this becomes both a permissible way to distribute to the general population and to follow preventive measures such as social distancing. As earlier stated, we used direct email invitation and posting links to the questionnaire in popular social media platforms used by the public. Obtaining 1,512 participants, from which 1,481 (97.9%) participants accepted to participate in this study, while 31 (2.1%) participants declined. We should note that throughout the questionnaire, it did not require participants to answer all the questions to advance. We present the general sociodemographic information for all the consenting participants in Table 2. Out of the initial sociodemographic assessment, the most representative results showed the following information: for gender, there was a slight majority of females (57.9%). The most frequent age range reported was 25 to 34 years (28.6%). The most common occupation status was students (20.2%). sixty-eighth percentage of participants reported practicing a religion, while 55% of participants reported having a bachelor's degree. Interestingly, the most common household occupancy was of four people (27.2%) and the most regular reported house size was of >4 rooms (61.7%). As expected, 30.3% of the participants reported having at least one comorbidity obesity being the highest in frequency (61.1%), followed by cardiovascular diseases (27.6%) and diabetes (14.2%). Forty-Six percentage of participants reported having children. Meanwhile, 82.3% of participants reported not having a previous diagnosis of COVID-19, while 95.7% of participants reported knowing at least someone with COVID-19 diagnosis. Remarkably, 80.2% of participants reported a positive posture toward vaccination. An interesting observation was that 48.7% of participants reported their shoot for influenza in the 2020–2021 season. Unsurprisingly, 86.2% of participants agreed that COVID-19 vaccine will help to advance the economic situation of the country, while 87.8% of participants reported a willingness to get the vaccine against COVID-19. Finally, 73.1% of participants reported actively looking for COVID-19 vaccine-related information.
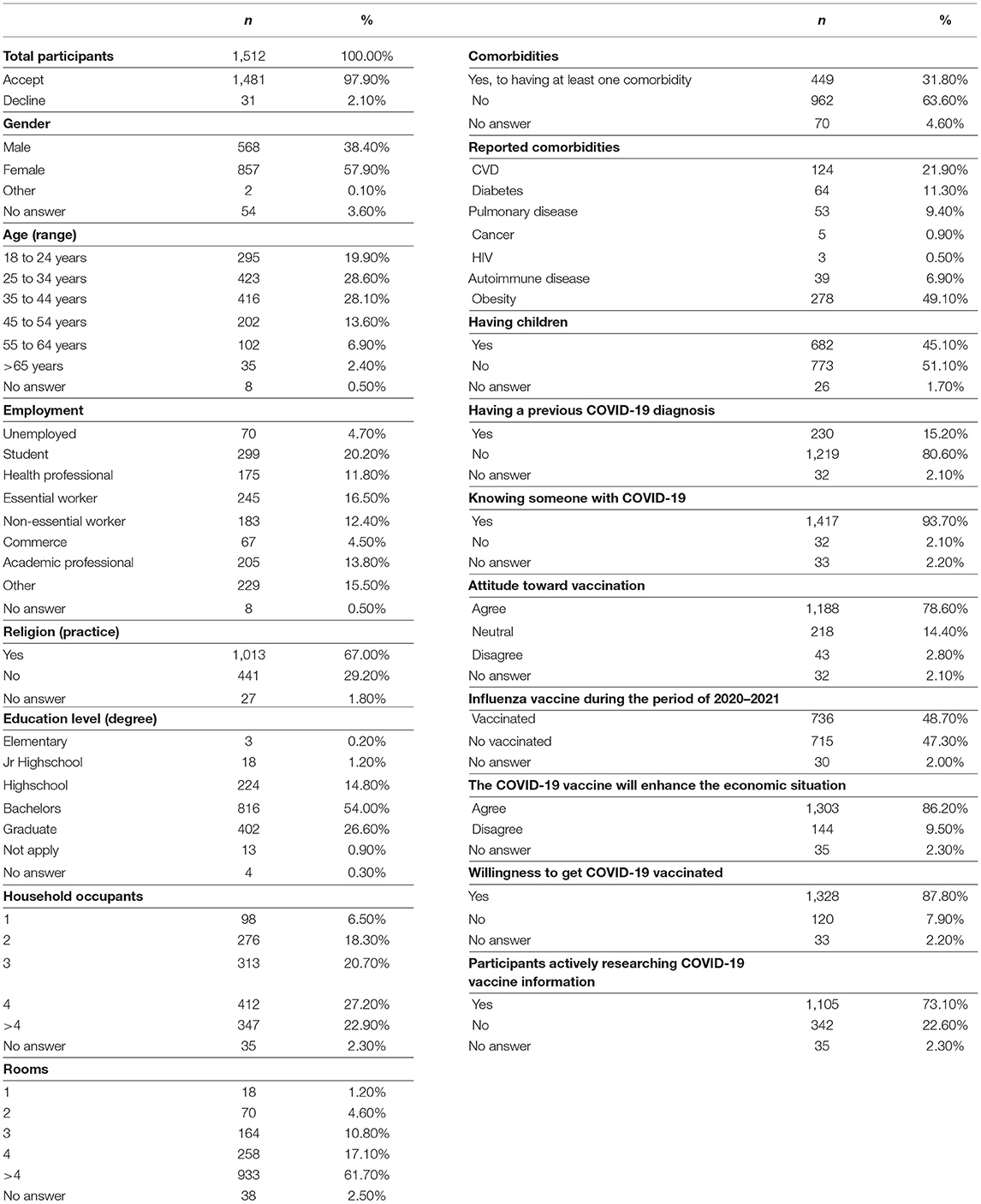
Table 2. Social demographic profiles of participants.
Next, we evaluated the four sections of the questionnaire and correlated them with all the variables studied (sociodemographic and COVID-19-related questions) and results are seen in Table 3. From these results, the most relevant classifications were: occupation showed statistical relevance to Section 2 (moderate), Section 3 (absent), and Section 4 (absent) all with a p < 0.001. Gender showed statistical relevance to Section 3 (absent) and Section 4 (absent) all with a p < 0.001. Age showed statistical relevance to Section 1 (mild) (p < 0.005), Section 2 (moderate) (p < 0.001), Section 3 (absent) (p < 0.010), and Section 4 (absent) (p < 0.001). For religion, Section 3 (absent) and Section 4 (absent) showed statistical relevance with a p < 0.001. Education level showed statistical relevance to Section 3 (absent) (p < 0.001). Household occupants showed statistical relevance to Section 4 (absent) (p < 0.001). Meanwhile, the total number of rooms only showed relevance to Section 4 (absent) (p < 0.002). Interestingly, participants having at least only one comorbidity showed relevance to Section 1 (mild) (p < 0.016) and Section 4 (absent) (p < 0.001). A previous COVID-19 diagnosis was statistically relevant only to Section 3 (absent) (p < 0.001). Knowing someone with COVID-19 diagnosis showed statistical relevance to Section 4 (absent) (p < 0.001). General posture toward vaccination applied to Section 1 (mild), Section 2 (moderate), Section 3 (absent), and Section 4 (moderate) all with a p < 0.001. Getting influenza vaccination for the 2020–2021 season was statistically relevant to Section 1 (mild) (p < 0.001), Section 2 (moderate) (p < 0.007), and Section 3 (absent) (p < 0.001). Considering that COVID-19 vaccine will help to boost the economic situation of country, it showed statistical relevance to Section 1 (mild), Section 2 (moderate), Section 3 (absent), and Section 4 (moderate) all with a p < 0.001. Willingness to get COVID-19 vaccinated showed statistical relevance to Section 1 (mild), Section 2 (moderate), Section 3 (absent), and Section 4 (moderate) all with a p < 0.001. Participants actively researching COVID-19 vaccine information was statistically relevant to Section 1 (mild) (p < 0.011), Section 3 (absent) (p < 0.001), and Section 4 (moderate) (p < 0.016). A previous COVID-19 diagnosis was only relevant to Section 3 (absent) (p < 0.001). We further correlated all the variables studied among themselves (Table 4). We asked if the participant was actively searching for information about the vaccines. Most of the research conducted was about Pfizer, Sputnik V, Moderna, and AstraZeneca vaccines, as seen in Figure 1. Finally, using the SPSS® software, we did binary logistic regression analysis and results are shown in Table 5. The algorithm plucked in a stepwise manner and demographic variables did not influence the outcome of willingness to get vaccinated. Results showed that in the age groups from 18 to 24 years (p < 0.001, OR: 8.36) and in the age groups from 25 to 34 years (p < 0.019, OR: 2.36), the only demographic variables influencing the willingness to get vaccinated. Within the four studied sections, particular categories participated in the willingness to get vaccinated: a mild perception of danger and contamination with respect to COVID-19: mild (p < 0.001, OR: 4.60), moderate (p < 0.001, OR: 24.50), and severe (p < 0.001, OR: 48.41); a moderate perception of xenophobia generated throughout COVID-19 quarantine: absent (p < 0.001, OR: 0.16) and mild (p < 0.045, OR: 0.52); fear of adverse effects of COVID-19 vaccination: absent (p < 0.001, OR: 141.70), mild (p < 0.001, OR: 23.39), and moderate (p < 0.018, OR: 3.40); and hesitancy of parents toward vaccination of children: absent (p < 0.001, OR: 0.16), mild (p < 0.001, OR: 0.07), and moderate (p < 0.004, OR: 0.20).
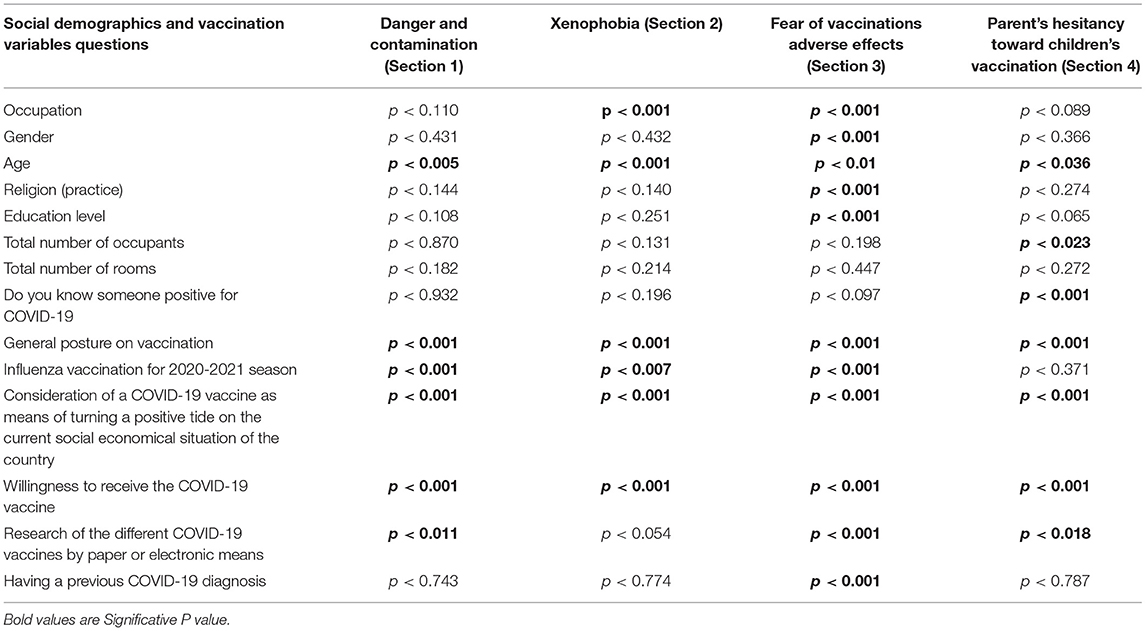
Table 3. Statistical correlation (p-values) for social demographics and coronavirus disease 2019 (COVID-19)-related questions and sections (1–4).
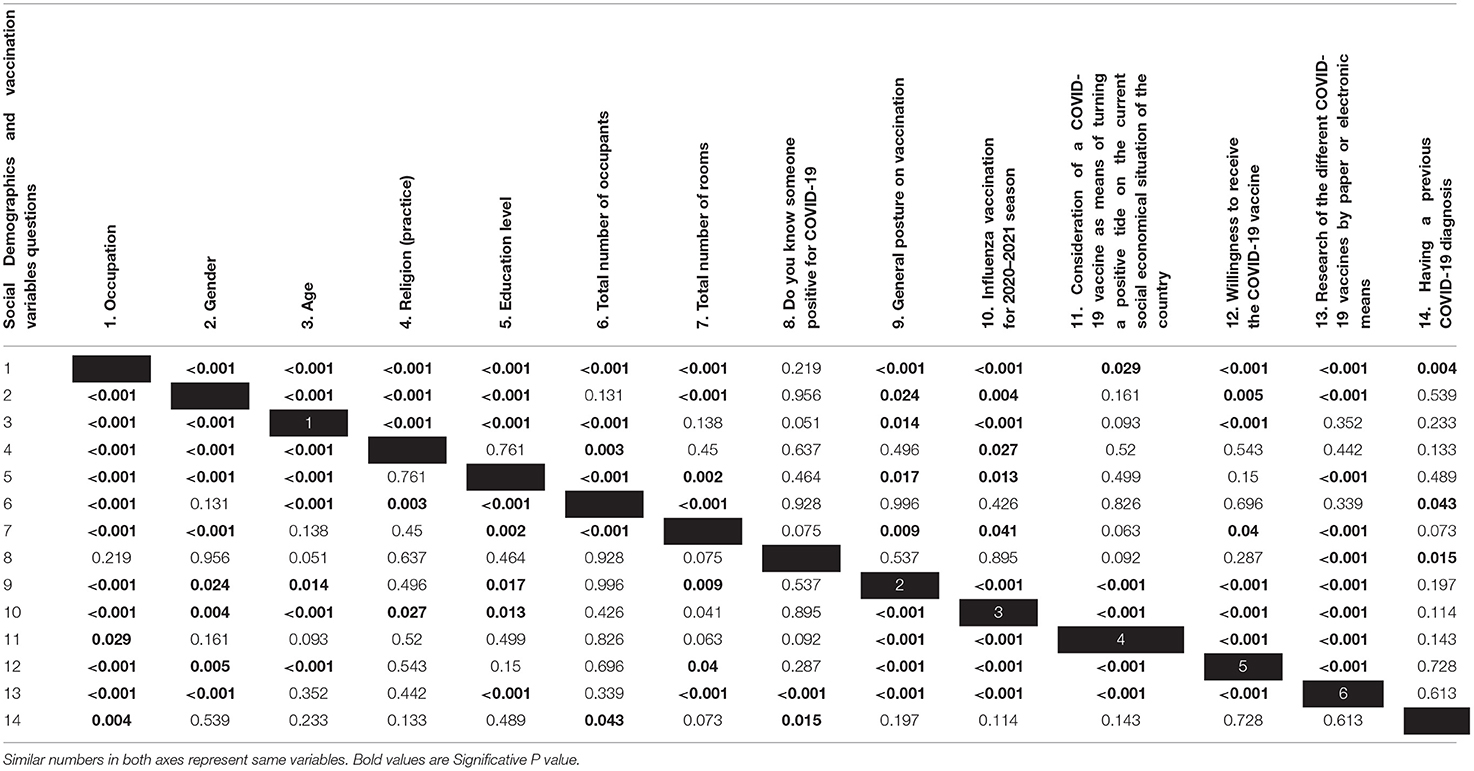
Table 4. Statistical correlation (p-values) among all the social demographics and COVID-19-related questions.
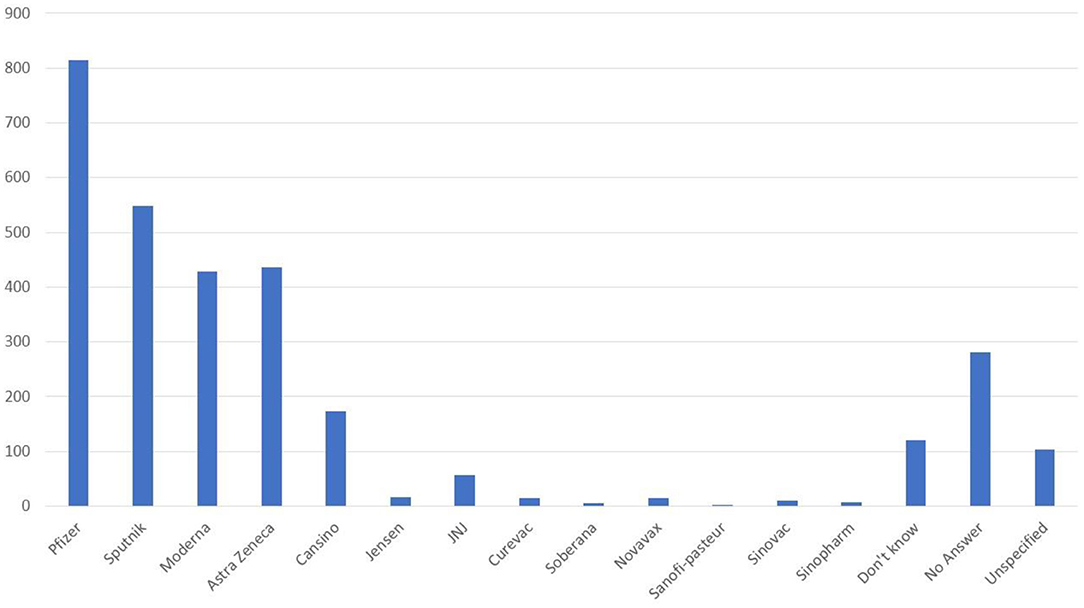
Figure 1. Frequency counts as the most researched coronavirus disease 2019 (COVID-19) vaccines brands.
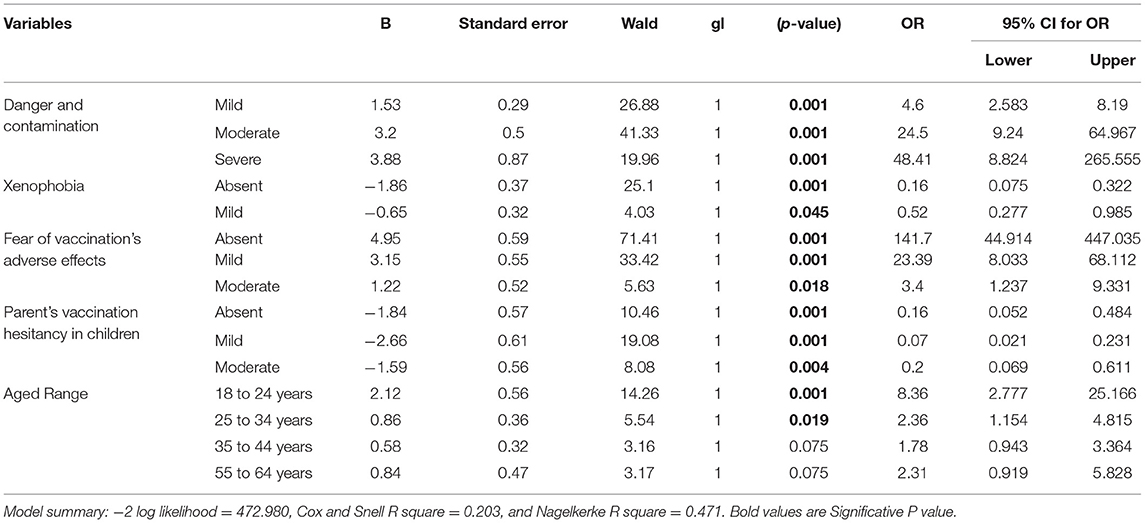
Table 5. Results of binary logistic regression analysis on demographic factors and sections significantly associated with willingness to get vaccinated.
The WHO stated in the last year that vaccinations effectively save millions of lives every year; they recognize that vaccination programs are “one of the world's most successful and cost-effective health interventions,” which prevent over 2 million deaths every year.
In Mexico, influenza vaccination has proven to be effective, albeit there are still several declared cases, it continues well controlled in the overall population (4, 26). Even now with COVID-19 pandemic, we registered that almost 50% of the surveyed population got vaccinated for influenza, even considering the potential risks of going to a health center amid COVID-19 pandemic (27). This seems to fair with what other researcher had observed back in 2020 when a survey by Forbes concluded that there was a massive increase in the demand for influenza vaccine, as this might protect against notable effects of COVID-19 (28). The results in this study suggest that the general population in Mexico has a good vaccination culture, as 78.6% agreed to have a positive posture toward vaccination. Occupations, such as essential workers, students, and healthcare professionals, showed to have a good affinity toward the idea of vaccination. A recent study showed that those involved in the care of patients with COVID-19 had higher levels of vaccination acceptance than those not directly attend patients with COVID-19 positive (29).
Over the course of the past year, the perception toward vaccination may have potentially changed. Currently, the mortality rate in Mexico is around 9% (2, 3) and 95.7% of participants admitted knowing someone diagnosed with COVID-19, while 15.5% of participants had a previous COVID-19 diagnosis. Therefore, a potential preventive measure such as a vaccine would ease at least partially the overall stress felt by the general population. It is easy to assume that a portion of the participants have had contact with a patient that passed away or that has been in a delicate state because of COVID-19. This idea of potential change toward positive views in vaccination is further supported by the results of the questionnaire sections evaluating the different aspects toward fear and contamination and xenophobia related to COVID-19 in Sections 1 and 2 of the questionnaire. Our binary logistic regression analysis further weighed in favor of Section 1 as the OR for moderate: 24.50 and severe: 48.41. Binary logistic regression analysis also showed that Section 3 had a highly important contribution as being absent had an OR of 141.70, with mild contributing with an OR of 23.39; this is interesting as precisely the fear of adverse effects of COVID-19 vaccination correlated with the willingness to get COVID-19 vaccinated. Over 49% of participants scored in the absent category. Thus, affecting the overall desire to get vaccinated as 87.8% of the population showed an interest to get COVID-19 vaccine and 73.1% of participants are actively looking for information with respect to COVID-19 vaccine. Nearly half of the participants (48.7%) got vaccinated against seasonal influenza during the 2020–2021 period; potentially, the rest might not have gotten the vaccine out of fear of getting infected when going to a healthcare center (27). However, a newly realized study among nursing professionals showed that COVID-19 vaccination intention directly relates to a previous influenza vaccination, where the most important associated factors were young age, confidence, and collective responsibility (30). By comparison, we can draw similarities with the general population in Mexico, where the influenza vaccination rate grew over 2019 above 300% (28), as there is an overall positive approval rate toward getting vaccinated. In our result section, we see several correlations among variables related to hesitancy and the four general sections, which evaluate the sense of a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parents toward vaccination of children.
Researchers have recently described factors associated with a decline in vaccination such as exposure to other people while being in line to get vaccinated against COVID-19 as one of the major concerns, as individuals might get infected and possibly spread the virus (27). Also, concerns about safety and effectiveness of the vaccine are noted in the literature and doubts toward the vaccines approval derived from their rapid development, delayed side effects presentation, and misinformation about COVID-19 vaccination on social media (31). Religious beliefs pose interesting perspectives. On one hand, religion seems to have a protective measure against stress related to COVID-19 quarantine and in most cases, it does not correlate toward the application of the vaccine (32). Another variable studied was cohabitation, which did not show any correlations toward protective measures or toward a positive attitude about receiving the vaccine. Patients that have high risk of comorbidities show a more aggressive presentation of the disease. In this study, we found that having any level of education seems to have a positive attitude toward vaccination and less fear toward COVID-19 vaccine. Females showed a significant correlation between variables with respect to a positive attitude toward COVID-19 vaccination. In addition, females seem to show more fear toward a possible adverse reaction. A study by Larson et al. found that these same trends applying similar survey in 2016 (33).
Coronavirus disease 2019 has set an unprecedented stress on the economy of world, as of March 2020 prediction for each additional month of quarantine would cost 2.5–3% of gross domestic product (GDP) and have a high impact on several countries (34). Given the economic crisis that the quarantine has set in Mexico among all the sectors, 86.2% of participants agreed that the application of COVID-19 vaccine will enhance the economic situation. This perspective is an important posture for the overall sentiment within the country, as the positive perception of the vaccines assisting the economy, potentially helps people cope with the overall economic stress generated during the quarantine, and finally seeing a light at the end of the tunnel.
Because of COVID-19 quarantine and at the time of the social distancing restrictions, we applied the questionnaire throughout a digital platform (Microsoft Forms). We could consider this as a limitation as it is unsupervised in-person, particularly during the quarantine, remote evaluations provide a safe alternative, albeit relying on the inclination of participant to answer. Currently, online surveys have been used by several groups, particularly in COVID-19 pandemic, to gather public or particular selected group information (17, 23, 35–37). As stated elsewhere in the manuscript, we distributed the questionnaire either by direct email invitation (we further asked participants to send to other colleagues or acquaintances the link to the questionnaire) or by popular social media platforms. However, this poses the problem of not being able to know the number of potential subjects to whom the questionnaire was available, hence not being able to calculate a participation rate. In addition, full completion of the questionnaire of participant was optional, as we believe that this might deter some from continuing. Our group distributes well among age groups, gender, types of employments, and other social demographic aspects as seen in Table 2.
Even though COVID-19 vaccine has been associated with much uncertainty and misinformation around it, slowly but surely it is helping the world get through the quarantine. The development of new vaccines might save thousands of lives and eventually offset the balance of case-fatality ratio. Studies determining the factors required for acceptance of the vaccine or other important treatments are of the utmost importance, when trying to understand the behavioral patterns of a population, as many social and cultural factors can play crucial roles in the level of success of a preventive campaign such as that of a vaccination program.
In this study, we analyzed the attitude and perceptions toward vaccination, using the proposed COV-AHQ (with the calculated Cronbach's alpha >0.8). According to the binary logistics correlation analysis, the general vaccination posture seems to correlate significantly (p < 0.05) with a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, hesitancy of parents toward vaccination of children, willingness to get COVID-19 vaccine, previous influenza vaccination, perception of the vaccine that could help the economy of country, occupation, gender, age, and participants actively researching COVID-19 vaccine information. A more in-depth analysis assisted by binary logistic regression analysis concluded that the young adult population around 18–34 years are the most likely to get vaccinated. This posture seems to be highly influenced by a mild perception of danger and contamination with respect to COVID-19, a moderate perception of xenophobia generated throughout COVID-19 quarantine, fear of adverse effects of COVID-19 vaccination, and hesitancy of parents toward vaccination of children. Their own personal religious beliefs, economic status (indirectly measured by household occupancy and total number of rooms), and the level of education do not seem to have an effect and having a previous COVID-19 diagnosis or even knowing someone with a positive COVID-19 diagnosis.
Given that young adults are the motor of the workforce in the country, actions to help with vaccination efforts should include flexible scheduling in vaccination campaign to address availability of different work shifts. Other positive actions that can be taken are enhancing company policies and measures toward employee vaccination such as providing transport for employees to vaccination sites or pay leave for vaccination purposes. Ideally, authorities should incentivize positive and proactive information campaigns directed at this population.
Current efforts by the government to vaccinate the population are being focused initially on at-risk groups, followed by a staggered vaccination divided in age groups. Our recommendation after these initial efforts to provide vaccination the entire population would be now to focus on a more community-based accessibility including local pharmacies and medical offices/hospitals as potential vaccination sites. In this second effort, we can expect a reduction in wait times, travel and expenses, exposure to harsh climate, and other inconveniences, making it more comfortable and accessible for the rest of the population to get vaccinated.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comite de Etica, Hospital La Misión, Monterrey Nuevo León. The patients/participants provided their written informed consent to participate in this study.
JD-G and JI conceptualized and supervised the study, contributed to the overall design of the survey experiment, analysis and interpretation of the data, and wrote the first draft of the manuscript. GP-R, GR-C, HF, MC-L, and MM-T contributed to the overall design of the survey experiment, designed the discrete choice experiment, and contributed to the analysis and statistic interpretation of the data. EZ-V, GA-R, DA-S, LG-A, and JM-C contributed to the discussion of public health implications and helped to shape the overall interpretation. All the authors had access to all the data in this study and had final responsibility for the decision to submit for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sohrabi C, Alsafi Z, Neill NO, Khan M, Kerwan A. World health organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. (2020) 76:71–6. doi: 10.1016/j.ijsu.2020.02.034
2. Bello-Chavolla O, Bahena-López J, Antonio-Villa N, Vargas-Vázquez A, González-Díaz A, Márquez-Salinas A, et al. Predicting mortality due to SARS-CoV-2: a mechanistic score relating obesity and diabetes to COVID-19 outcomes in Mexico Omar. J Clin Endocrinol Metab. (2020) 105:1–13. doi: 10.1210/clinem/dgaa346
3. John Hopkins Coronavirus Resource Center. Mortality Rate. John Hopkins University (2021). Available online at: https://coronavirus.jhu.edu/data/mortality (accessed Feb 8, 2021)
4. Cordova-Villalobos JA, Macias AE, Hernandez-Avila M, Dominguez-Cherit G, Lopez-Gatell H, Alpuche-Aranda C, et al. The 2009 pandemic in Mexico: experience and lessons regarding national preparedness policies for seasonal and epidemic influenza. Gac Med Mex. (2017) 153:102–10.
5. Sierra-Madero JG, Belaunzaran-Zamudio PF, Crabtree-Ramírez B, Magis-Rodriguez C. Mexico's fragmented health system as a barrier to HIV care. Lancet HIV. (2019) 6:e74–5. doi: 10.1016/S2352-3018(18)30356-4
6. Forouzanfar MH, Afshin A, Alexander LT, Biryukov S, Brauer M, Cercy K, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. (2016) 388:1659–724. doi: 10.1016/S0140-6736(16)31679-8
7. Campos-Nonato I, Hernandez-Barrera L, Pedroza-Tobias A, Medina C, Barquera S. Vista de hipertensión arterial en adultos mexicanos_ prevalencia, diagnóstico y tipo de tratamiento. Ensanut MC 2016. Salud Publiva Mex. (2018) 60:233–43. doi: 10.21149/8813
8. Campos-Nonato I, Ramírez-Villalobos M, Flores-Coria A, Valdez A, Monterrubio-Flores E. Prevalence of previously diagnosed diabetes and glycemic control strategies in Mexican adults: ENSANUT-2016. PLoS ONE. (2020) 15:e0230752. doi: 10.1371/journal.pone.0230752
9. Suárez V, Suarez Quezada M, Oros Ruiz S, Ronquillo De Jesús E. Epidemiología de COVID-19 en México: del 27 de febrero al 30 de abril de 2020. Rev Clínica Española. (2020)1–9. doi: 10.1016/j.rce.2020.05.007
10. Sharif A, Aloui C, Yarovaya L. COVID-19 pandemic, oil prices, stock market, geopolitical risk and policy uncertainty nexus in the US economy: fresh evidence from the waveletbased approach. Int Rev Financ Anal. (2020) 70:101496. doi: 10.1016/j.irfa.2020.101496
11. Spencer JP, Trondsen Pawlowski RH, Thomas S. Vaccine adverse events: separating myth from reality. Am Fam Physician. (2017) 95:786–94.
12. Pluviano S, Watt C, Della Sala S. Misinformation lingers in memory: Failure of three pro-vaccination strategies. PLoS ONE. (2017) 12:e0181640. doi: 10.1371/journal.pone.0181640
13. Feleszko W, Lewulis P, Czarnecki A, Waszkiewicz P. Flattening the curve of covid-19 vaccine rejection—an international overview. Vaccines. (2021) 9:1–8. doi: 10.3390/vaccines9010044
14. Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. (2020) 27:225–8. doi: 10.1038/s41591-020-1124-9
15. Timmis JK, Rigat F, Rappuoli R. Core values for vaccine evaluation. Vaccine. (2017) 35:57–62. doi: 10.1016/j.vaccine.2016.11.034
16. Padilla-Rivas GR, Delgado-Gallegos JL, Montemayor-Garza RDJ, Franco-Villareal H, Coiser-León MDLÁ, Avilés-Rodriguez G, et al. Dataset of the adapted COVID STRESS SCALES for healthcare professionals of the Northeast region of Mexico. Data Br. (2021) 34:106733. doi: 10.1016/j.dib.2021.106733
17. Delgado-Gallegos JL, Montemayor-Garza RJ, Padilla-Rivas GR, Franco-Villareal H, Islas JF. Prevalence of stress in healthcare professionals during the covid-19 pandemic in Northeast Mexico: a remote, fast survey evaluation, using an adapted covid-19 stress scales. Int J Environ Res Public Health. (2020) 17:7624. doi: 10.3390/ijerph17207624
18. Shapiro GK, Tatar O, Dube E, Amsel R, Knauper B, Naz A, et al. The vaccine hesitancy scale: psychometric properties and validation. Vaccine. (2018) 36:660–7. doi: 10.1016/j.vaccine.2017.12.043
19. Taylor S, Landry CA, Paluszek MM, Fergus TA, McKay D, Asmundson GJG. Development and initial validation of the COVID stress scales. J Anxiety Disord. (2020) 72:102232. doi: 10.1016/j.janxdis.2020.102232
20. Gobierno de Mexico. Vacunación COVID coronavirus. Secr Salud. (2021). Available online at: https://coronavirus.gob.mx/
21. Lwange SK, Lemershow S. Sample Size determination in Health Studies: A Practical Manual. World Health Organization. (1991). Available online at: https://apps.who.int/iris/handle/10665/40062
22. Marsden PV, Wright JD. Handbook of Survey Research. 2nd ed. Bingley: Emerald Publishing Limited. (2010).
23. Delgado-Gallegos JL, Padilla-Rivas GR, Zuñiga-Violante E, Avilés-Rodriguez G, Arellanos-Soto D, Franco Villareal H, et al. Teaching anxiety, stress and resilience during the COVID-19 pandemic: evaluating the vulnerability of academic professionals in Mexico through the adapted COVID-19 stress scales. Front Public Heal. (2021) 9:669057. doi: 10.3389/fpubh.2021.669057
24. Press A. Mexico Starts School Year Using TV, Radio and the Internet. Washington Post. (2020). Available online at: https://www.washingtonpost.com/lifestyle/kidspost/mexico-starts-school-year-using-tv-radio-and-the-internet/2020/08/24/aad3e60a-d5ba-11ea-aff6-220dd3a14741_story.html
25. Sánchez M, Martínez A, Torres R, de Agüero M, Hernández A, Benavides M, et al. Retos educativos durante la pandemia de COVID-19: una encuesta a profesores de la UNAM. Rev Digit Univ. (2020) 21:1–24. doi: 10.22201/codeic.16076079e.2020.v21n3.a12
26. Hernández-Ávila M, Alpuche-Aranda CM. Mexico: lessons learned from the 2009 pandemic that help us fight COVID-19. Healthc Manag Forum. (2020) 33:158–63. doi: 10.1177/0840470420921542
27. Coustasse A, Kimble C, Maxik K. COVID-19 and vaccine hesitancy: a challenge the United states must overcome. J Ambul Care Manage. (2021) 44:71–5. doi: 10.1097/JAC.0000000000000360
28. Forbes. Detectan Aumento de 300% en la Demanda de Vacuna Contra Influenza. Forbes / Actual. (2020). Available online at: https://www.forbes.com.mx/noticias-aumento-300-demanda-vacuna-influenza/ (accessed March 21, 2021).
29. Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. (2020) 35:775–9. doi: 10.1007/s10654-020-00671-y
30. Kwok KO Li K-K, Wei WI, Tang A, Wong SYS, Lee SS. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: a survey. Int J Nurs Stud. (2021) 114:103854. doi: 10.1016/j.ijnurstu.2020.103854
31. Puri N, Coomes EA, Haghbayan H, Gunaratne K. Social media and vaccine hesitancy: new updates for the era of COVID-19 and globalized infectious diseases. Hum Vaccin Immunother. (2020) 16:2586–93. doi: 10.1080/21645515.2020.1780846
32. Times NY. Religious Objections to the Measles Vaccine? Get the Shots, Faith Leaders Say New York Times. (2019). Available online at: https://www.nytimes.com/2019/04/26/health/measles-vaccination-jews-muslims-catholics.html (accessed January 2, 2021).
33. Larson HJ, de Figueiredo A, Xiahong Z, Schulz WS, Verger P, Johnston IG, et al. The state of vaccine confidence 2016: global insights through a 67-country survey. EBioMedicine. (2016) 12:295–301. doi: 10.1016/j.ebiom.2016.08.042
34. Fernandes N. Economic Effects of Coronavirus Outbreak (COVID-19) on the World Economy. SSRN Electron J. (2020) 1–33. doi: 10.2139/ssrn.3557504
35. Park CL, Russell BS, Fendrich M, Finkelstein-Fox L, Hutchison M, Becker J. Americans' COVID-19 stress, coping, and adherence to CDC guidelines. J Gen Intern Med. (2020) 35:2296–303. doi: 10.1007/s11606-020-05898-9
36. Sharma R, Tikka SK. COVID-19 online surveys need to follow standards and guidelines: comment on “Does COVID-19 pandemic affect sexual behaviour? a cross-sectional, cross-national online survey” and “binge watching behavior during COVID 19 pandemic: a cross-sectional, cross-national online survey.” Psychiatry Res. (2020) 290:113173. doi: 10.1016/j.psychres.2020.113173
Keywords: COVID-19 vaccine hesitancy in Mexico, COVID-19 vaccine Latin-America, COVID-19 vaccine awareness, COVID-19 vaccination attitude, COVID-19 vaccine acceptance
Citation: Delgado-Gallegos JL, Padilla-Rivas GR, Zúñiga-Violante E, Avilés-Rodríguez G, Arellanos-Soto D, Gastelum-Arias LJ, Franco Villareal H, Cosío-León MdlÁ, Romo-Cardenas GS, Moreno-Treviño MG, Moreno-Cuevas JE and Islas JF (2021) Determinants of COVID-19 Vaccine Hesitancy: A Cross-Sectional Study on a Mexican Population Using an Online Questionnaire (COV-AHQ). Front. Public Health 9:728690. doi: 10.3389/fpubh.2021.728690
Received: 29 June 2021; Accepted: 27 October 2021;
Published: 26 November 2021.
Edited by:
Malaisamy Muniyandi, National Institute of Research in Tuberculosis (ICMR), IndiaReviewed by:
Charles J. Vukotich Jr, University of Pittsburgh, United StatesCopyright © 2021 Delgado-Gallegos, Padilla-Rivas, Zúñiga-Violante, Avilés-Rodríguez, Arellanos-Soto, Gastelum-Arias, Franco Villareal, Cosío-León, Romo-Cardenas, Moreno-Treviño, Moreno-Cuevas and Islas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge E. Moreno-Cuevas, am9yZ2VlLm1vcmVub0B1ZGVtLmVkdQ==; Jose Francisco Islas, amlzbGFzLm1lMDExN0B1YW5sLmVkdS5teA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.