 Jordane Boudesseul
Jordane Boudesseul Oulmann Zerhouni
Oulmann Zerhouni Allie Harbert3
Allie Harbert3 Clio Rubinos
Clio Rubinos- 1Facultad de Psicología, Instituto de Investigación Científica, Universidad de Lima, Lima, Peru
- 2University Paris Nanterre, Nanterre, France
- 3School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
- 4Department of Neurology, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
Despite the massive distribution of different vaccines globally, the current pandemic has revealed the crucial need for an efficient treatment against COVID-19. Meta-analyses have historically been extremely useful to determine treatment efficacy but recent debates about the use of hydroxychloroquine for COVID-19 patients resulted in contradictory meta-analytical results. Different factors during the COVID-19 pandemic have impacted key features of conducting a good meta-analysis. Some meta-analyses did not evaluate or treat substantial heterogeneity (I2 > 75%); others did not include additional analysis for publication bias; none checked for evidence of p–hacking in the primary studies nor used recent methods (i.e., p-curve or p-uniform) to estimate the average population-size effect. These inconsistencies may contribute to contradictory results in the research evaluating COVID-19 treatments. A prominent example of this is the use of hydroxychloroquine, where some studies reported a large positive effect, whereas others indicated no significant effect or even increased mortality when hydroxychloroquine was used with the antibiotic azithromycin. In this paper, we first recall the benefits and fundamental steps of good quality meta-analysis. Then, we examine various meta-analyses on hydroxychloroquine treatments for COVID-19 patients that led to contradictory results and causes for this discrepancy. We then highlight recent tools that contribute to evaluate publication bias and p-hacking (i.e., p-curve, p-uniform) and conclude by making technical recommendations that meta-analyses should follow even during extreme global events such as a pandemic.
Background
The 2020 COVID-19 pandemic has highlighted the urgent need for the development and administration of a new treatment for COVID-19. Despite the rollout of several different vaccines globally, the need to find treatment remains essential given the uncertainty and shortcomings with equal distribution of vaccines and vaccine availability. Meta-analyses have historically been used to establish the existence, size, and confidence of therapeutic effects or causes of particular diseases.
Meta-analysis is an important tool to determine the effectiveness of COVID-19 treatments, but it is essential that the strength of evidence be maintained by adhering to all components of the methodology. Various factors during the COVID-19 pandemic, including time pressure, have resulted in alterations and omissions of key aspects of meta-analysis that lower the quality of evidence. Some meta-analyses did not evaluate publication bias, nor treat substantial heterogeneity (I2 > 75%); none checked for evidence of p–hacking in the primary studies nor used recent techniques (i.e., p-curve or p-uniform) to estimate average population-size effect. Journals greatly favor publishing significant findings in comparison to non-significant findings, resulting in publication bias which can overestimate effect sizes (the strength of the relationship between two variables). These discrepancies may contribute to opposing results in the research evaluating COVID-19 treatments. A prominent example of this is the use of hydroxychloroquine (HCQ), where some studies reported a large protective effect, whereas others indicated no significant effect or even increased mortality when HCQ was administered with the antibiotic azithromycin.
In this paper, we first highlight the benefits and fundamental steps of meta-analytical studies. Then, we analyze examples of meta-analyses of HCQ treatments for COVID-19 patients that led to contradictory results and causes for this discrepancy. We conclude by making recommendations that meta-analyses should follow even during extreme global events such as a pandemic (see Table 1).
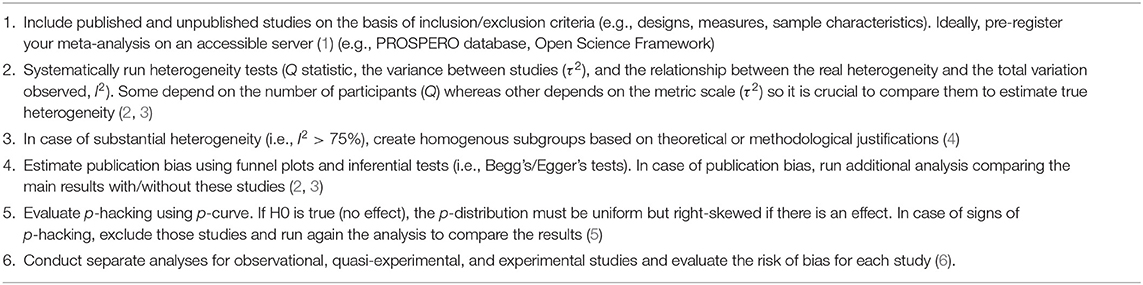
Table 1. General recommendations for meta-analysis of clinical studies.
Methods
Meta-Analysis: Principles and Procedures
Meta-analysis involves a set of statistical techniques to synthesize effect sizes of several studies on the same phenomenon (2, 3). Several benefits are expected from clinical meta-analyses:
• Identify, screen, select, and include studies based on systematic reviews of the literature (i.e., as recommend by the PRISMA Statement) (7).
• Compute the mean effect sizes across different studies (i.e., the average effect of a particular treatment on a specific condition).
• Evaluate the level of heterogeneity (i.e., the amount of variation in the outcomes detected by the different studies).
• Determine the impact of publication bias (i.e., the lack of publication of negative trials and underrepresentation of unpublished data, can lead to overestimated effect sizes).
• Run meta-regressions and subgroup analyses to control for the effects of studies' characteristics (e.g., design, procedure, measures) and sample (e.g., age/gender, BMI, clinical history).
Meta-analyses begins by identifying, screening, and evaluating potentially relevant studies, and ultimately collecting data from included studies and evaluating their quality (through PRISMA, for instance) (7). The mean and variance of the estimates is collected from every included study to compute a global weighted mean based on the inverse variance (2, 3). Some recent meta-analyses on the effect of HCQ in COVID-19 patients have omitted basic practices to assess publication bias (8), resulting in massive untreated heterogeneity (8) (i.e., I2 > 80%) or meta-analyzed small sets of studies [k ≤ 3 implying low statistical power (9)]. None used recent tools to evaluate p-hacking and recent techniques for assessing the publication bias, possibly leading to an overall biased representation of the population-size effect.
Gathering the Studies
The first step in conducting a meta-analysis is to search the literature for studies investigating a specific predefined question and using predetermined inclusion and exclusion criteria based on theoretical or methodological criteria (7) to determine eligibility. Several methods exist to assess and correct for publication bias among a set of studies (e.g., Egger or PET-PEESE tests, p-uniform, p-curve) (5, 10). A general issue is that studies likely differ significantly in design (e.g., randomized controlled trial vs. observational studies) and the specific questions they investigate (e.g., viral load, shedding, mortality/ICU events, mild symptoms). For instance, investigators must decide whether observational or quasi-experimental studies should be included alongside experimental studies. The lack of randomization inherent to observational or quasi-experimental studies is problematic as they are at risk of bias by uncontrolled confounding variables (11).
Recent advances in techniques question the reliance on estimates presented in the original studies for meta-analysis due to significant limitations (12). Systematic reviews and meta-analyses that use individual patient data (IPD) suggest collecting, validating, and reanalyzing the raw data from all clinical trials included in the meta-analysis. Following COCHRANE recommendations, IPD meta-analyses offer a multidisciplinary and cross-cultural perspective that decreases cultural and professional biases. IPD analyses also enable better assessment of moderator variable impact and improves statistical power (13). Integrating contextual variables helps ensure main effects are not explained by sample or country characteristics (or any other contextual factors). Limitations of including such variables are potential collinearity with other variables or insufficient precision in the measure. Although there are several advantages of conducting IPD meta-analyses, it also requires significant organization and coordination that can be challenging.
Statistical Power
A major strength of meta-analysis is the relatively high statistical power associated with compiling several studies (i.e., independent RCTs may have few participants per group limiting their statistical power). The median number of studies in the Cochrane Database for Systematic Reviews is six, according to Borenstein et al. (2). This is a serious concern considering that (1) subgroup analysis and meta-regressions are routine procedures that require high levels of statistical power, and (2) many meta-analyses have high heterogeneity (I2 > 75%), which negatively affects precision and thus statistical power. For example, the statistical power to detect a small effect size (d = 0.2) with 25 participants per group in 6 different studies using a random-effects model with moderate heterogeneity (I2 = 50%) and a 5% of type I error is only 26.7% (https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/power-calculator-tool.html).
Assessing Heterogeneity
The objective of meta-analysis is not simply to calculate an average weighted effect estimate but also to make sense of the pattern of effects. An intervention that consistently reduces the risk of mortality by 30% in numerous studies is different from an intervention that reduces the risk of mortality by 30% on average, with a risk reduction ranging from 10 to 80% across studies. We must determine the true variance to provide different perspectives on the dispersion of the results based on the Q statistic, the variance between studies (τ2), and the relationship between the real heterogeneity and the observed total variation (I2).
Publication Bias
Publication bias affects both researchers conducting meta-analyses and physicians searching for primary studies in a database. If the missing studies are a random subset of all studies, excluding them will result in less evidence, wider confidence intervals, and lower statistical power, but will not have a systematic influence on the effect size (2). However, whenever there are systematic differences in unpublished and published studies included in the meta-analysis, the weighted effect sizes are biased (e.g., a lack of studies reporting non-significant effects of HCQ in COVID-19 patients). Dickersin (14) found that statistically significant results are more likely to be published than non-significant findings, and thus when published studies are combined together, they may lead to overestimated effects. Also, for any given sample size, the result is more likely to be statistically significant if the effect size is large. Studies with inflated estimate effects are expected to be reported in the literature more frequently as a result (i.e., the first studies on HCQ likely reported large effects). This trend has the potential to produce large biases both on effect size estimates and significance testing (15).
Different techniques have been developed to detect publication bias (16). A widely used method—the funnel plot—consists of plotting effect sizes against their standard errors or precisions (the inverse of standard errors). A skewed funnel plot is usually an indication of the presence of publication bias. However, subjective visual examination as well as coding of the outcome, the choice of the metric, and the choice of the weight on the vertical axis all impact the appearance of the plot (17). Inferential tests such as Egger's regression test regress the standardized effect size on the corresponding precisions (the inverse of the within-study variance). Although widely used, the Egger test may suffer from an inflated type I error rate or low statistical power in certain conditions (16, 17).
Results
Hydroxychloroquine and COVID-19 Meta-Analysis
HCQ and chloroquine (CQ) have been used for decades to manage and treat malaria and several autoimmune conditions. At the beginning of the pandemic, preliminary studies (18–20) suggested that HCQ might have a positive effect on the treatment of COVID-19 patients. This led the U.S. Food and Drug Administration (FDA) to issue an emergency-use (EUA) authorization on March 28, 2020 allowing for HCQ sulfate and CQ phosphate to be donated to the Strategic National Stockpile for use in hospitalized COVID-19 patients. Given its multiple antiviral effects, it is plausible that HCQ could be beneficial in COVID-19 patients (21). In vitro data have shown that HCQ/CQ blocks viral infection by inhibiting virus/cell fusion through increasing endosomal pH (22) and by reducing the production of inflammatory cytokines (23–25). Shortly after the EUA of HCQ/CQ, a group in France published a study describing viral load reduction/cure with HCQ (20). However, this study included a small sample size, was non-randomized, only reported viral load as an outcome, and excluded the most severely ill patients from the analysis. Numerous meta-analyses have already been published on the use of HCQ in COVID-19 patients, with some indicating a large protective effect for HCQ (8), and others reporting no effect (9) or increased mortality when HCQ was used with the antibiotic azithromycin (AZ) (26) (see a complete Table of HCQ/CQ meta-analysis and their bias on Table 2).
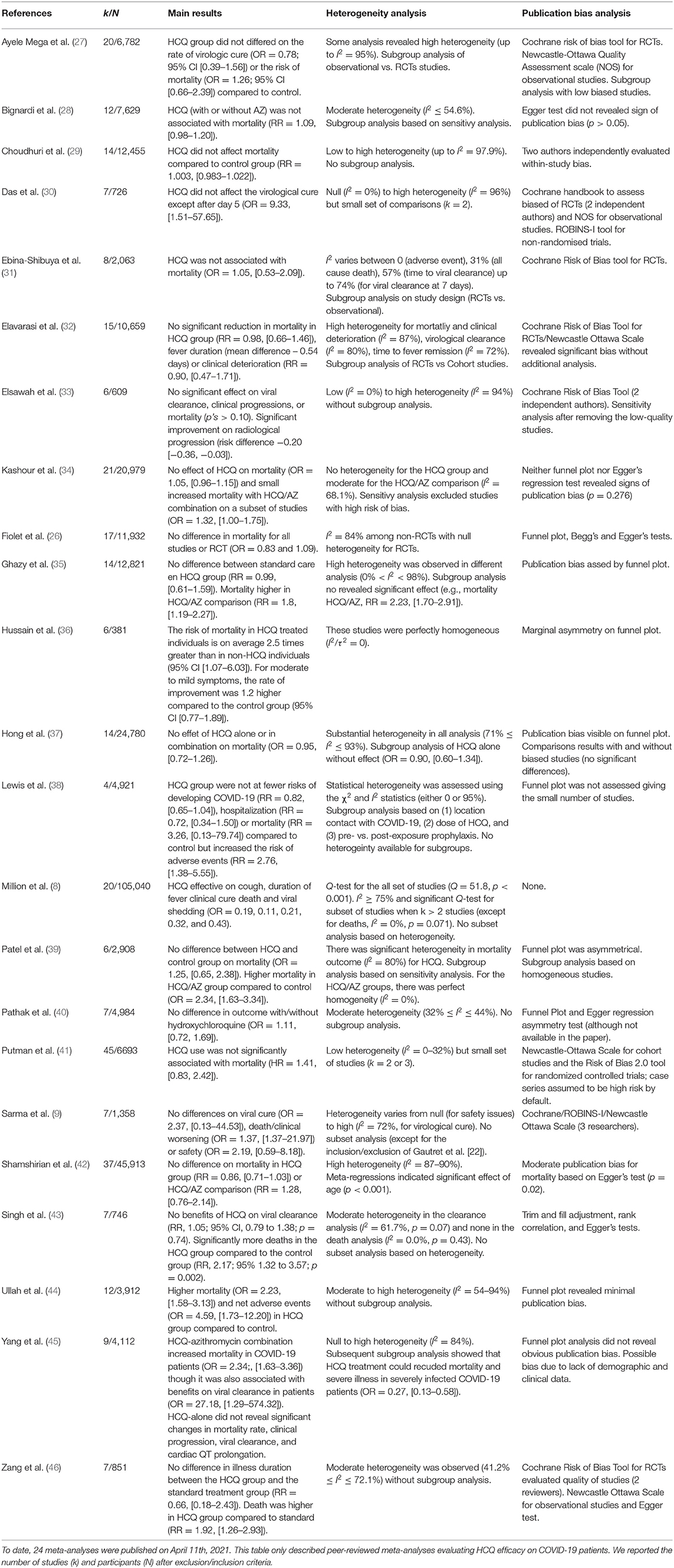
Table 2. Meta-analysis on the efficacy of hydroxychloroquine on COVID-19 patients published in peer-reviewed journals.
Some Examples of Questionable Research Practices in Meta-Analysis Suggesting No-Effect or Effects of HCQ
Million et al. (8) published a meta-analysis containing 20 studies involving 105,040 patients of which 19,270 had been on chloroquine derivatives and found a positive effect of the drug on mortality and symptoms associated with COVID-19. On the other hand, Fiolet et al. (26) did not find any effect of HCQ/AZ in a meta-analysis of 29 studies including 11,932 patients. In both meta-analyses, the authors found large heterogeneity among the included studies (I2 = 75% and I2 = 83%), which suggests the presence of confounders not being accounted for across studies, and neither study performed subgroup analysis to better explore the high heterogeneity. Study selection was problematic in both studies. For instance, Million and colleagues did not publish a flow diagram with the different phases of a systematic review as recommended by the PRISMA Statement (7). Several items, fundamental in the method of the PRISMA protocol, were not followed such as review protocol registration, detailed study selection criteria, data collection process, risk of bias within and across studies, and additional analyses. Million et al. (8) grouped “clinical” studies together (studies that had direct access to patients) and “observational big data” studies together (that may present conflicts of interest and show no effect of HCQ) instead of doing meta-regressions based on study designs (i.e., RCT vs. observational study). Fiolet et al. (26) excluded several studies because of critical risk of bias (i.e., lack of statistical information and the assignment of treatment, unknown timing between measures and confounders) with HCQ and AZ combination therapy (47–49).
Outcome selection is concerning, as Million et al. (8) reported positive effects on the duration of symptoms such as cough, fever, and clinical care with analysis of 1 to 7 small sample size studies (50). In Fiolet's et al. meta-analysis (26), the type of estimate used for effect sizes was inconsistent and not clearly reported. They did not make a distinction between Risk Ratios (RR), which are usually used in cohort studies, and Hazard Ratios (HR) and Odds Ratios (OR), which are used in case-control studies. This can influence the analysis because OR tend to overestimate effects compared to RR when the selected outcome occurs frequently (51). In both meta-analyses, the selection of included studies, the degree of heterogeneity in these analyses, and the calculations of effect sizes make the veracity of the estimates uncertain. Many of the meta-analyses published had low statistical power, untreated heterogeneity and none used tools to evaluate potential risks of p-hacking (13, 27–46, 52).
Discussion
A Proposal for Conducting Meta-Analyses in Clinical Research
As discussed above, one potential bias in meta-analyses is “selection bias,” which may lead to inaccurate estimation of effect sizes. An important question is whether to incorporate unpublished pre-print studies, especially when the field has limited studies and there is urgency for reliable data. An argument against this approach could be that unpublished studies might not be as rigorous as published studies. From this point of view, unpublished studies should not be included in meta-analyses because the inclusion of poorly conducted research also introduces bias. However, having access to published and unpublished studies helps decide which studies to include in a meta-analysis based on a priori inclusion criteria [through pre-registered meta-analyses for instance (1), see Table 2].
Readers typically focus on the forest plot, which depicts the quantitative effects and level of uncertainty for each study included in the meta-analysis. Forest plots are great tools to visually assess heterogeneity (coupled with quantitative index such as I2 or Q-test) and pooled results (53). However, forest plots do not address publication bias and thus can mislead readers's conclusion if not presented with additional information such as a funnel plot.
One of the most widely used tools to assess publication bias is plotting the effect sizes for each study against an indicator for the precision to which each study estimated the effect size. In funnel-plots, studies will be plotted near the average effect size, while studies with low precision (e.g., small sample) will have effect estimates distributed on either side of the average effect, creating a funnel-shaped plot.
Although funnel plots are a widely used and reliable way to evaluate publication bias, another useful tool is the p-curve (5). The p-curve plots a proportion of observed p-values for each value of p in a set of studies. Because true effects are more likely to have smaller values of p (e.g., “p < 0.01”) than values around the arbitrary significant threshold of p < 0.05, a flat p-curve or a p-curve indicating a higher proportion of p-values between 0.04 and 0.05 is more likely to be an indicator of questionable research practices, sometimes referred to as p-hacking. Van Assen et al. (4) propose the use of another tool, p-uniform, to estimate population effect size in the presence of small to moderate heterogeneity (I2 < 50%).
Conducting sub-group analyses for observational, quasi-experimental, and experimental studies will also help evaluate the risk of bias of each study design (6). In cases of substantial heterogeneity, researchers can generate a homogenous group of studies based on theoretical or methodological criteria and then use the p-curve and p-uniform to estimate the average population effect sizes for each subgroup analysis (4). Additional tools can be useful to determine publication bias. For instance, selection models can adjust for suspected selective publication; Rosenthal's fail-safe N is used to estimate the number of unpublished studies necessary to overturn the significant results and Copas sensitivity approach uses regression models to evaluate publication bias (54).
The fact that statistically significant results are more likely to be published than non-significant results is a major source of publication bias. Additional sources of potential bias that should be addressed when possible include pipeline bias (non-significant results take longer to publish than significant results), subjective reporting bias (selective reporting of the results), duplicate reporting bias (results published in multiple sources), and language bias (non-native English speakers tend to publish non-significant findings in their native tongue) (54).
Conclusion
Tensions over the use of HCQ for COVID-19 patients have unfortunately led some authors to disregard basic meta-analytical protocols. Concern over the quality of studies included in meta-analyses has also emerged in a recent comparative psychological study between meta-analytical findings and registered replication studies. The authors found that meta-analytical effect sizes significantly differed from the replication effect sizes for 12 of the 15 meta-replication pairs, and meta-analytic effect sizes were almost three times larger than the replication effect sizes (15). These inconsistencies call for caution when running and interpreting meta-analyses of new clinical studies.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
JB and OZ contributed to the original idea and wrote the original manuscript. JB, OZ, and CR analyzed the relevant literature and updated the manuscript. JB, OZ, CR, and AH were all contributor in writing the final manuscript. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AZ, Azithromycin; COVID-19, Coronavirus disease 2019; CQ, Chloroquine; EUA, Emergency-use authorization; FDA, Food and Drug Administration; HCQ, Hydroxychloroquine; HR, Hazard ratio; ICU, Intensive care unit; IPD, Individual patient data; OR, Odd ratio; PRISMA, Preferred reporting items for systematic reviews and meta-analyses; RCT, Randomized controlled trial; RR, Risk ratio.
References
1. Quintana DS. From pre-registration to publication: a non-technical primer for conducting a meta-analysis to synthesize correlational data. Front Psychol. (2015) 6:1549. doi: 10.3389/fpsyg.2015.01549
2. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to Meta-Analysis. New York, NY: John Wiley & Sons (2009). doi: 10.1002/9780470743386
4. Van Assen MA, van Aer R, Wicherts JM. Meta-analysis using effect size distributions of only statistically significant studies. Psychol Methods. (2015) 20:293–309. doi: 10.1037/met0000025
5. Simonsohn U, Nelson LD, Simmons JP. P-curve: a key to the file-drawer. J Exp Psychol Gen. (2014) 143:534–47. doi: 10.1037/a0033242
6. Higgins JP Altman DG Sterne JA On behalf of the Cochrane Statistical Methods Group and the Cochrane Bias Methods Group. Chapter 8: Assessing risk of bias in included studies. Cochrane Handb Syst Rev Intervent. (2011) 2008:187–241. doi: 10.1002/9780470712184.ch8
7. Moher D, Liberati A, Tetzlaff J, Altman DG, Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
8. Million M, Gautret P, Colson P, Roussel Y, Dubourg G, Chabriere E, et al. Clinical efficacy of chloroquine derivatives in COVID-19 infection: comparative meta-analysis between the big data and the real world. New Micro New Infect. (2020) 38:100709. doi: 10.1016/j.nmni.2020.100709
9. Sarma P, Kaur H, Kumar H, Mahendru D, Avti P, Bhattacharyya A, et al. Virological and clinical cure in COVID-19 patients treated with hydroxychloroquine: a systematic review and meta-analysis. J Med Virol. (2020) 92:776–85. doi: 10.1002/jmv.25898
10. van Aert RC, Wicherts JM, van Assen MA. Conducting meta-analyses based on p values: reservations and recommendations for applying p-uniform and p-curve. Persp Psych Sci. (2016) 11:713–29. doi: 10.1177/1745691616650874
11. Shapiro S. Meta-analysis/Shmeta-analysis. Am J Epidem. (1994) 140:771–8. doi: 10.1093/oxfordjournals.aje.a117324
12. Stewart LA, Tierney JF. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval Health Prof. (2002) 25:76–97. doi: 10.1177/0163278702025001006
13. Karyotaki E, Riper H, Twisk J, Hoogendoorn A, Kleiboer A, Mira A, et al. Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms a meta-analysis of individual participant data. JAMA Psychiatry. (2017) 74:351–59. doi: 10.1001/jamapsychiatry.2017.0044
14. Dickersin K. Publication bias: recognizing the problem, understanding its origins and scope, and preventing harm. In: Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments. New York, NY (2005). p. 11–33. doi: 10.1002/0470870168.ch2
15. Kvarven A, Strømland E, Johannesson M. Comparing meta-analyses and preregistered multiple-laboratory replication projects. Nat Hum Behav. (2020) 4:423–34. doi: 10.1038/s41562-019-0787-z
16. Lin L, Chu H. Quantifying publication bias in meta-analysis. Biometrics. (2018) 3:785–94. doi: 10.1111/biom.12817
17. Lau J, Ioannidis JP, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot. BMJ. (2006) 333:597–600. doi: 10.1136/bmj.333.7568.597
18. Zhai P, Ding Y, Wu X, Long J, Zhong Y, Li Y. The epidemiology, diagnosis and treatment of COVID-19. Int J Antimicrob Agents. (2020) 55:1–13. doi: 10.1016/j.ijantimicag.2020.105955
19. Ferner RE, Aronson JK. Chloroquine and hydroxychloroquine in covid-19. BMJ. (2020) 369:m1432. doi: 10.1136/bmj.m1432
20. Gautret P, Lagier JC, Parola P, Meddeb L, Mailhe M, Doudier B, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. (2020) 56:1–6. doi: 10.1016/j.ijantimicag.2020.105949
21. Devaux CA, Rolain JM, Colson P, Raoult D. New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19? Int J Antimicro Agents. (2020) 55:1–6. doi: 10.1016/j.ijantimicag.2020.105938
22. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. (2020) 30:269–71. doi: 10.1038/s41422-020-0282-0
23. Ballabio A, Bonifacino JS. Lysosomes as dynamic regulators of cell and organismal homeostasis. Nat Rev Mol Cell Bio. (2020) 21:101–18. doi: 10.1038/s41580-019-0185-4
24. Mauthe M, Orhon I, Rocchi C, Zhou X, Luhr M, Hijlkema KJ, et al. Chloroquine inhibits autophagic flux by decreasing autophagosome-lysosome fusion. Autophagy. (2018) 14:1435–55. doi: 10.1080/15548627.2018.1474314
25. Van den Borne BE, Dijkmans BA, De Rooij HH, Le Cessie S, Verweij CL. Chloroquine and hydroxychloroquine equally affect tumor necrosis factor-alpha, interleukin 6, and interferon-gamma production by peripheral blood mononuclear cells. J Rheumatol. (1997) 24:55–60.
26. Fiolet T, Guihur A, Rebeaud ME, Mulot M, Peiffer-Smadja N, Mahamat-Saleh Y. Effect of hydroxychloroquine with or without azithromycin on the mortality of COVID-19 patients: a systematic review and meta-analysis. Clin Micro Infect. (2020) 27:19–27. doi: 10.1016/j.cmi.2020.08.022
27. Ayele Mega T, Feyissa TM, Dessalegn Bosho D, Kumela Goro K, Zeleke Negera G. The outcome of hydroxychloroquine in patients treated for COVID-19: systematic review and meta-analysis. Can Res J. (2020) 2020:4312519. doi: 10.1155/2020/4312519
28. Bignardi PR, Vengrus CS, Aquino BM, Cerci Neto A. Use of hydroxychloroquine and chloroquine in patients with COVID-19: a meta-analysis of randomized clinical trials. Pathog Glob Health. (2021) 115:139–50. doi: 10.1080/20477724.2021.1884807
29. Choudhuri AH, Duggal S, Ahuja B, Biswas PS. The efficacy and safety of hydroxychloroquine (HCQ) in treatment of COVID19–a systematic review and meta-analysis. Ind J Med Microbiol. (2021) 39:159–70. doi: 10.1016/j.ijmmb.2021.03.002
30. Das RR, Behera B, Mishra B, Naik SS. Effect of chloroquine and hydroxychloroquine on COVID-19 virological outcomes: an updated meta-analysis. Indian J Med Microbiol. (2020) 38:265–72. doi: 10.4103/ijmm.IJMM_20_330
31. Ebina-Shibuya R, Namkoong H, Horita N, Kato H, Hara Y, Kobayashi N, et al. Hydroxychloroquine and chloroquine for treatment of coronavirus disease 19 (COVID-19): a systematic review and meta-analysis of randomized and non-randomized controlled trials. J Thorac Dis. (2021) 1:202–12. doi: 10.21037/jtd-20-2022
32. Elavarasi A, Prasad M, Seth T, Sahoo RK, Madan K, Nischal N, et al. Chloroquine and hydroxychloroquine for the treatment of COVID-19: a systematic review and meta-analysis. J Gen Intern Med. (2020) 35:3308–14. doi: 10.1007/s11606-020-06146-w
33. Elsawah HK, Elsokary MA, Elrazzaz MG, Elshafie AH. Hydroxychloroquine for treatment of nonsevere COVID-19 patients: systematic review and meta-analysis of controlled clinical trials. J Med Virol. (2021) 93:1265–75. doi: 10.1002/jmv.26442
34. Kashour Z, Riaz M, Garbati MA, AlDosary O, Tlayjeh H, Gerberi D, et al. Efficacy of chloroquine or hydroxychloroquine in COVID-19 patients: a systematic review and meta-analysis. J Antimicrob Chemother. (2021) 76:30–42. doi: 10.1093/jac/dkaa403
35. Ghazy RM, Almaghraby A, Shaaban R, Kamal A, Beshir H, Moursi A, et al. A systematic review and meta-analysis on chloroquine and hydroxychloroquine as monotherapy or combined with azithromycin in COVID-19 treatment. Sci Rep. (2020) 10:22139. doi: 10.1038/s41598-020-77748-x
36. Hussain N, Chung E, Heyl JJ, Hussain B, Oh MC, Pinon C, et al. A meta-analysis on the effects of hydroxychloroquine on COVID-19. Cureus. (2020) 12:1–17. doi: 10.7759/cureus.10005
37. Hong TS, Gonzalez J, Nahass RG, Brunetti L. Impact of hydroxychloroquine on mortality in hospitalized patients with COVID-19: systematic review and meta-analysis. Pharmacy. (2020) 8:208. doi: 10.3390/pharmacy8040208
38. Lewis K, Chaudhuri D, Alshamsi F, Carayannopoulos L, Dearness K, Chagla Z, et al. The efficacy and safety of hydroxychloroquine for COVID-19 prophylaxis: a systematic review and meta-analysis of randomized trials. PLoS ONE. (2021) 16:e0244778. doi: 10.1371/journal.pone.0244778
39. Patel TK, Barvaliya M, Kevadiya BD, Patel PB, Bhalla HL. Does adding of hydroxychloroquine to the standard care provide any benefit in reducing the mortality among COVID-19 patients?: a systematic review. J Neuroimmune Pharmacol. (2020) 15:350–8. doi: 10.1007/s11481-020-09930-x
40. Pathak SK, Salunke DAA, Thivari DP, Pandey A, Nandy DK, Harish VK, et al. No benefit of hydroxychloroquine in COVID-19: results of systematic review and meta-analysis of randomized controlled trials. Diabetes Metab Syndr. (2020) 14:1673–80. doi: 10.1016/j.dsx.2020.08.033
41. Putman M, Chock YP, Tam H, Kim AH, Sattui SE, Berenbaum F, et al. Antirheumatic disease therapies for the treatment of COVID-19: a systematic review and meta-analysis. Arthritis Rheumatol. (2021) 73:36–47. doi: 10.1002/art.41469
42. Shamshirian A, Hessami A, Heydari K, Alizadeh-Navaei R, Ebrahimzadeh MA, Yip GW, et al. The role of hydroxychloroquine in COVID-19 treatment: a systematic review and meta-analysis. Ann Acad Med Singap. (2020) 49:789–800. doi: 10.47102/annals-acadmedsg.2020370
43. Singh AK, Singh A, Singh R, Misra A. Hydroxychloroquine in patients with COVID-19: a systematic review and meta-analysis. Diabetes Metab Syndr. (2020) 14:589–96. doi: 10.1016/j.dsx.2020.05.017
44. Ullah W, Abdullah HM, Roomi S, Sattar Y, Almas T, Gowda SN, et al. Safety and efficacy of hydroxychloroquine in COVID-19: a systematic review and meta-analysis. J Clin Med Res. (2020) 12:483–91. doi: 10.14740/jocmr4233
45. Yang TH, Chou CY, Yang YF, Chien CS, Yarmishyn AA, Yang TY, et al. Systematic review and meta-analysis of the effectiveness and safety of hydroxychloroquine in treating COVID-19 patients. J Chin Med Assoc. (2021) 84:233–41. doi: 10.1097/JCMA.0000000000000425
46. Zang Y, Han X, He M, Shi J, Li Y. Hydroxychloroquine use and progression or prognosis of COVID-19: a systematic review and meta-analysis. Naunyn Schmiedebergs Arch Pharmacol. (2020) 4:775–82. doi: 10.1007/s00210-020-01964-5
47. Davido B, Boussaid G, Vaugier I, Lansaman T, Bouchand F, Lawrence C, et al. Impact of medical care, including use of anti-infective agents, on prognosis of COVID-19 hospitalized patients over time. Int J Antimicro Agents. (2020) 56:1–9. doi: 10.1016/j.ijantimicag.2020.106129
48. Di Castelnuovo A, Costanzo S, Antinori A, Berselli N, Blandi L, Bruno R, et al. Use of hydroxychloroquine in hospitalised COVID-19 patients is associated with reduced mortality: findings from the observational multicentre Italian CORIST study. Euro J Intern Med. (2020) 82:38–47. doi: 10.1016/j.ejim.2020.08.019
49. Catteau L, Dauby N, Montourcy M, Bottieau E, Hautekiet J, Goetghebeur E, et al. Low-dose hydroxychloroquine therapy and mortality in hospitalised patients with COVID-19: a nationwide observational study of 8075 participants. Int J Antimicro Agents. (2020) 56:1–8. doi: 10.1016/j.ijantimicag.2020.106144
50. Button KS, Ioannidis JPA, Mokrysz C, Nosek BA, Flint J, Robinson ESJ, et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neuro. (2013) 14:365–76. doi: 10.1038/nrn3475
51. Magagnoli J, Narendran S, Pereira F, Cummings TH, Hardin JW, Sutton SS, et al. Outcomes of hydroxychloroquine usage in United States veterans hospitalized with Covid-19. Med. (2020) 1:114–27. doi: 10.1016/j.medj.2020.06.001
52. Cortegiani A, Ingoglia G, Ippolito M, Giarratano A, Einav S. AUpdate I. A systematic review on the efficacy and safety of chloroquine/hydroxychloroquine for COVID-19. J Crit Care. (2020) 57:279–83. doi: 10.1016/j.jcrc.2020.03.005
53. Ioannidis JP, Patsopoulos NA, Rothstein HR. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ. (2008) 336:1413–5. doi: 10.1136/bmj.a117
Keywords: COVID−19, meta-analysis, heterogeneity, publication bias, hydroxychloroquine
Citation: Boudesseul J, Zerhouni O, Harbert A and Rubinos C (2021) Keeping Meta-Analyses Hygienic During the COVID-19 Pandemic. Front. Public Health 9:722458. doi: 10.3389/fpubh.2021.722458
Received: 08 June 2021; Accepted: 01 September 2021;
Published: 29 September 2021.
Edited by:
Andreia Silva Costa, ISAMB & ESEL, PortugalReviewed by:
Jacques Oosthuizen, Edith Cowan University, AustraliaAndree Kurniawan, University of Pelita Harapan, Indonesia
Copyright © 2021 Boudesseul, Zerhouni, Harbert and Rubinos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jordane Boudesseul, am1qLmJvdWRlc3NldWxAZ21haWwuY29t